the 9th topra annual symposium 2012 - human medicines
TRANSCRIPT

4
Regulatory Rapporteur – Vol 9, No 12, December 2012 www.topra.org
this year’s symposium agenda covered a broad spectrum of regulatory developments and updates, from initiatives on scientifi c advice and the centralised procedure to proposals for the new Clinical trial regulation and implementation of the recently introduced EU pharmacovigilance legislation. other important areas discussed in a variety of sessions included moves to tackle counterfeit medicines, the trend for switching from prescription to over-the-counter (otC) products, how to improve access to medicines for patients and how to best deliver information to patients.
To put this agenda in place, the symposium’s Programme Committee comprised members of the Irish Medicines Board (IMB), the European Medicines Agency (EMA), national competent authorities and industry.
Delegates were welcomed to the three-day meeting by TOPRA’s Executive Director, Lynda Wight; Craig McCarthy, Chair of the Symposium Working Party; and Pat O’Mahony, Chief Executive of the Irish Medicines Board.
SESSION 1: Scientifi c advice: an important Strategic activity for all Companies involved in drug development, Especially SmEsReported by Fiona Reekie, Director of Regulatory Intelligence, Europe & Global Emerging Markets, Biogen Idec Ltd
The symposium’s working party chair, Craig mcCarthy, managing director, CamPHarm, France, introduced the opening session. This considered initiatives relating to national scientifi c advice (SA) and the EMA’s Committee for Medicinal Products for Human Use (CHMP) SA, such as joint advice with health technology assessment bodies (HTAs), qualifi cation advice and opinions.
The fi rst speaker, david Wright, Expert Statistical assessor, deputy manager of Statistics Unit and Chair of Sa letters review Group, medicines & Healthcare products regulatory agency (mHra), UK, provided an “Update on National Agency Scientifi c Advice”. The
Human Medicines
toPra’s 9th annual Pharmaceutical Symposium, organised in conjunction with the irish medicines Board, was held in october in dublin, ireland. representatives from the European Commission, regulatory agencies, industry and academia gathered to debate current regulatory issues and discuss future legislative initiatives

5Focus – Pharmaceutical Symposium
acronym s and abbreviationsaPi, Active pharmaceutical ingredient
atmP, Advanced therapy medicinal product
CaP, Centrally authorised product
CESP, Common European Submission Platform
CHmP, Committee for Medicinal Products for Human Use
CmC, Chemistry, manufacturing and controls
Cta, Clinical trial application
Ctd, Common technical document
CtFG, Clinical Trials Facilitation Group
dCP, Decentralised procedure
dP, Drug product
dS, Drug substance
Ema, European Medicines Agency
EPar, European public assessment report
EUrd, European Union reference date
GCP, Good clinical practice
GmP, Good manufacturing practice
GSl, General sales list
Hma, Heads of Medicines Agencies
Hta, Health technology assessment
iCSr, Individual case safety report
imB, Irish Medicines Board
imP, Investigational medicinal product
maa, Marketing authorisation application
maH, Marketing authorisation holder
mHra, Medicines & Healthcare products Regulatory Agency
mrP, Mutual recognition procedure
NiCE, National Institute for Health and Clinical Excellence
Nda, New drug application
Nta, Notice to applicants
otC, Over-the-counter
PaSS, Post-authorisation safety study
Pat, Process analytical technology
Pil, Patient information leafl et
PraC, Pharmacovigilance Risk Assessment Committee
PSa, Parallel scientifi c advice
PSmF, Pharmacovigilance system master fi le
PSUr, Periodic safety update report
Qbd, Quality by design
QPPV, Qualifi ed person for pharmacovigilance
rmS, Reference member state
Sa, Scientifi c advice
SaG, Scientifi c advisory group
SaP, Statistical analysis plan
SaWP, Scientifi c Advice Working Party
SmE, Small to medium-sized enterprise
SmPC, Summary of product characteristics
SoP, Standard operating procedure
SWot, Strengths, weaknesses, opportunities and threats
tHmP, Traditional herbal medicinal product
VHP, Voluntary harmonisation procedure
www.topra.org Regulatory Rapporteur – Vol 9, No 12, December 2012
MHRA holds approximately 250 SA meetings a year, most of which are product-specifi c. The basic fee is based on a 90-minute face-to-face meeting, with the consequence that time is a limiting factor for the number of questions that can be addressed. If the meeting is likely to last longer than 90 minutes, due to the number or complexity of questions raised, then the company will be contacted and given the choice of shortening the list of questions, or attending more than one meeting (with more than one meeting fee charged). In some circumstances, the MHRA will postpone the meeting. For example, if the company fails to provide the briefi ng book ten working days prior to the meeting, or if the questions asked in the fi nal briefi ng book are so diff erent from the original questions that diff erent MHRA expertise is required at the meeting. Follow-up advice should be requested in the same way as the original request was made. To help companies with planning, meetings can be up to a year in advance.
The MHRA will not provide advice on topics that have already been discussed through CHMP SA, as the MHRA will have already provided input into that earlier advice.
The agency also off ers broader-scope advice which follows the same format but can include, for example, questions on methodological issues to investigate new designs/techniques intended to improve drug development. In such cases, due to the more speculative nature of the issues raised, the MHRA does not send written answers to the questions posed.
The MHRA encourages innovation and would like to see more companies asking for broader-scope advice, and Dr Wright further encouraged the audience that, in cases where a company’s senior management may believe that a potential new approach might not be accepted by regulators, the company could request a broader scope meeting to fi nd out what the MHRA’s views on the new approach. There has also not been much uptake for parallel advice with the UK’s National Institute for Health and Clinical Excellence (NICE) – a missed opportunity in Dr Wright’s view – but the pilot continues.
It is important to be aware that the position in an SA written response from the MHRA might be modifi ed from what was discussed in the meeting following review, as regulatory questions may have legal ramifi cations. Companies are always encouraged to submit their own minutes of the meeting to the MHRA.
It is not envisioned that parallel SA from the MHRA and NICE will replace the respective current SA processes at NICE or the MHRA, now or in the future. Interestingly, in this parallel advice process, the majority of the meeting time is given to NICE, which will focus on the key issues for discussion, rather than on the company’s questions (the company itself will only have a short amount of time for presentation of its questions).
Sheila Killalea, irish medicines Board (imB) delegate to the Scientifi c advice Working Party (SaWP), imB, ireland, spoke on “The procedure and advantages of obtaining centralised scientifi c advice via the EMA”, covering new initiatives with SA, including joint advice with HTAs and qualifi cation advice/opinion.
The majority of SA requests are for Phase III programmes (ie, at the end of Phase II) but the CHMP does receive requests for advice in earlier stages of development, which are welcomed. Meetings are used to try to focus on areas that may be contentious. Dr Killalea recommended that companies have a presubmission meeting. She noted that it would be helpful if the briefi ng book includes approaches that the company has tried/considered but rejected, as the CHMP/SAWP does not get sight of these and it helps them to understand the company’s position.

6 Focus – Pharmaceutical Symposium
Sheila Killalea, Irish Medicines Board delegate to the Scientifi c Advice Working Party (SAWP), IMB, Ireland
Regulatory Rapporteur – Vol 9, No 12, December 2012 www.topra.org
The advantage of centralised SA is in obtaining a unifi ed opinion applicable across the EU with input from a large network of experts in a relatively short timeframe, with a positive impact on success on marketing authorisation applications (MAAs).
For the newer procedures available on qualifi cation of “novel methodologies”, it is important to focus on the acceptability of the proposed technology/biomarker developed for a specifi c intended use in the context of pharmaceutical research and development (R&D). This also includes patient-reported outcomes. Qualifi cation advice is confi dential; however, when CHMP provides a Qualifi cation Opinion on the acceptability of a specifi c use of the proposed method (eg, use of a biomarker) in an R&D context (nonclinical or clinical studies), based on the assessment of submitted data, there will be a public consultation and the opinion is published. There is also the option to involve the US FDA in parallel, and this can include joint meetings.
To date, 34 qualifi cation applications have been submitted, ~20 qualifi cation advices completed and six opinions published (four of which were clinical opinions).
The procedures have greater fl exibility and opportunity for dialogue between sponsors and regulators, which can lead to early identifi cation of potential problems and can expedite the path to regulatory acceptance.
The EMA continues to off er parallel HTA/EMA SA, with 16 procedures so far, of which 11 have been fi nalised and fi ve are ongoing in a broad range of disease areas. These have included HTAs and payers from the UK, Sweden, France, Italy, the Netherlands, Spain, Germany and Belgium. To date, six applications have been facilitated through Tapestry Networks and ten independently. The majority involve new mechanisms of action in their respective areas, eg, new monoclonal antibodies, new chemicals and tumour vaccines. Dr Killalea encourages companies to apply very early with nonclinical proof-of-concept data (if
advice is very negative about concept, this in itself can be helpful to companies). In these procedures it is important to consider the varied backgrounds of the many stakeholders and to strike a balance between assumptions and facts.
The outcome of this procedure is the CHMP SA letter with the responses from the regulators; minutes circulated by the company for comments; and sometimes minutes from the HTA participants on the added therapeutic value questions. Although these procedures are relatively novel, they are considered to be enhancing understanding.
The following speaker, ronan donelan, Head of regulatory aff airs EmEa & aNZ, Quintiles, ireland, off ered a strategic view on obtaining SA. Dr Donelan is well positioned to share tips based on his experience of more than 20 national SAs and 12 CHMP SAs. Dr Donelan recommended that companies include milestones in their development plans for when to seek advice.
When introducing a candidate drug to regulators, it is important to be aware that fi rst experiences count. SA can help with decision-making on whether to continue or halt development. It is an opportunity to gain appreciation of an agency’s expectations. Companies should ensure they understand the diff erent SA options and conduct a SWOT (strengths, weaknesses, opportunities and threats) analysis around seeking SA. Dr Donelan advised that companies should target those authorities that will tell them the “good, the bad and the ugly”. National SA, she said, can be a good “practice run” for CHMP SA, but should not create a false sense of security – one agency does not make a CHMP. If in doubt about a programme, it is worth considering national SA fi rst, but some national competent authorities may refuse to give SA and instead advise that CHMP SA is sought. A risk factor for national SA is the potential for fundamental disagreement with the clinical development plan. Any advice received will need to be included in Module 1 of the MAA dossier.
richard Jones, Clinical r&d manager, Cosmo Pharmaceuticals, gave a presentation on the experience of a small to medium-sized enterprise (SME) with both initial national (MHRA) and CHMP SA processes on the same project, and how it helped the development strategy. The briefi ng books submitted for CHMP and MHRA SA packages were essentially the same. Both meetings were informative and invaluable for product development strategy and Phase III protocol development, with clear feedback on special populations. With hindsight, the company questions could have been expanded with more detail to get more valuable advice and extract maximum benefi t, and it might have been benefi cial to submit a detailed draft statistical analysis plan (SAP).
The fi nal speaker for this session, Janice m Soreth, deputy director, Fda Europe offi ce, liaison to Ema, US, updated delegates on EMA/FDA parallel scientifi c advice (PSA). The process and framework has been in place for collaboration on SA between the two agencies for several years, albeit with a rather low uptake by industry initially. Uptake of PSA improved in 2009/2010, when FDA and EMA liaisons were put in place, and this has included companies seeking PSA for earlier development phases and for rare diseases. The most important component of the team, Dr Soreth said, is the assessors being interested and “willing to play”. The FDA and EMA spend time looking at areas of disagreement. Discussions at PSA meetings between FDA/EMA/sponsor do not constitute a fi nal formal outcome; each agency will issue separate responses to the

7Focus – Pharmaceutical Symposium
Janice M Soreth, Deputy Director, FDA Europe Offi ce, Liaison to EMA
www.topra.org Regulatory Rapporteur – Vol 9, No 12, December 2012
company’s questions in line with usual procedures. There is a high level of informal interaction between the EMA and the FDA on SA, even without a formal PSA request. An important diff erence is that, in the FDA, the same group provides SA and subsequently reviews new drug applications (NDAs). The FDA therefore needs to take into consideration whether it can adhere to the timelines of parallel SA, and may on occasion turn down requests because of the timelines. Nevertheless, PSA presents opportunities to exchange views and share expertise to optimise and facilitate global development, meeting both agencies’ requirements (which will ideally be aligned). Furthermore, there many opportunities for informal SA when companies have fi rst approached either the CHMP or the FDA. If a company seeks advice from the FDA, it is worth highlighting that it has already received advice from the CHMP and share that advice, and vice versa.
SESSION 2: Clinical trialsReported by Sarah Roberts, Director, Global Regulatory Consulting, PPD
The second session, chaired by margareth Jorvid, Senior Consultant, methra Uppsala aB/lSm Group, Sweden, discussed recent developments in the regulation of clinical trials. On 17 July 2012, the European Commission adopted the proposal for a Clinical Trials Regulation, which will replace the Clinical Trials Directive 2001/20/EC. The divergent transposition and application of Directive 2001/20/EC across EU member states has led to an unfavourable regulatory framework for clinical research and has contributed to a decrease by 25% of clinical trials conducted between 2007 and 2011. Stefano Soro, Head of Unit d6 medicinal Products, dG SaNCo, European Commission, set the scene by giving an overview of the proposed regulation compared to the current directive. The scope of the regulation is unchanged in that it covers interventional clinical trials with human medicinal products, and does not cover non-interventional (observational) trials or trials without medicinal products (examples include devices and surgery).
The presentation focused the authorisation procedure, “risk-adaptedness” of the regulation, and other aspects. Submission of clinical trial applications (CTAs) under the regulation will be via an EU portal and the documents to be submitted are listed in the Annex to the proposal (although each member state can decide on its preferred language choice). The assessment of the CTA is a two-step process and will result in a single authorisation for the trial per member state (compared with the separate regulatory and ethical approvals currently issued). Initial approval timelines are anticipated to be shorter (41 days for a standard CTA) with assessment of Part I (joint assessment of core documents according to Article 6 of the regulation) and Part II (independent assessment of typically national documents according to Article 7 of the regulation) occurring in parallel. A new category of clinical trials has been included – “low intervention clinical trials” – where the investigational medicinal product (IMP) is authorised, used in accordance with the marketing authorisation or is used as a standard treatment in any of the member states concerned, or where additional diagnostic/monitoring is included in the trial which does not add signifi cant additional risk
to the patients compared with normal clinical practice. For these studies, approval timelines should be as short as 26 days in the proposed regulation.
Other risk-adapted measures have been included in the regulation, such as simplifi ed safety reporting, monitoring adapted to the type of trial, simplifi ed labelling for authorised products and consolidated and simplifi ed rules on the manufacture and import of IMPs. Further improvements included in the regulation include consideration of clinical trials conducted in third countries to ensure the quality of data included in marketing authorisation applications is of the required standard, the national indemnifi cation mechanism, emergency clinical trials, co-sponsorship and inspections and union controls. Hartmut Kraff t, Head of Clinical trials Unit, Paul-Ehrlich-institut (PEi), Germany and Chair of the Clinical trials Facilitation Group (CtFG), provided an update on the voluntary harmonisation procedure (VHP). Year on year the number of VHPs have been increasing and as of October 2012, 94 CTAs have been assessed via the VHP. The average time for approval (before the national authorisation step) is 50 days, with a mean of six member states participating. The spread of geographic location of sponsor companies is interesting, with 86 applications from the US, 29 from Switzerland, 103 from the EU, three from Singapore, one from Canada and one from Israel. There have been 113 substantial amendments processed via VHP with an average assessment time of 20 days. From 2009–Sept 2012, 72.6% of decisions were positive, 13.2% were open, 2.8% were negative, 4.7% had a divergent opinion and 6.6% were withdrawn by the applicant. The majority of applications were at Phase III (53.5%), although a signifi cant number were seen at Phase II (35.5%). Dr Kraff t also discussed the pros and cons of the proposed regulation and concluded that lessons could be learned from the experience gained during the VHP process which could be applied to the new regulation.

8 Focus – Pharmaceutical Symposium
Hartmut Kraff t, Head of Clinical Trials Unit, PEI, and Chair of CTFG
Stefano Soro, Head of Unit D6 Medicinal Products, DG SANCO, European Commission
Regulatory Rapporteur – Vol 9, No 12, December 2012 www.topra.org
daphne Smyth, Senior director regulatory aff airs EU & asia-Pacifi c, iCoN Clinical research, ireland, presented a view from industry outlining experiences of multinational trials to date and examining the potential impact of the proposed regulation on the future of clinical trials in the EU. The VHP for harmonisation, acceptance of core documents, fast review times within certain agencies for Phase I healthy volunteer studies and EudraCT were all praised for working well; however, challenges were noted around ethics committee alignment, local requirement diff erences, divergent timelines and substantial amendment classifi cations. The new regulation with its single submission portal, clear dossier requirements, common defi nition of substantial amendments, risk-adaptedness, centralised safety reporting and clarifi cation on sponsor/co-sponsor requirements was seen as a great advancement over the directive. However, it was noted that there are still some open questions where it is not yet clear on how the regulation will work in reality. These include clarifi cation around the timelines (particularly around the defi nition of ‘additional time’ during the 10 day part II assessment), transition with the VHP, details of the single EU portal and document requirements and EU contact person for non-EU sponsors versus the current legal representative.
Janice Soreth, deputy director, Fda Europe offi ce, liaison to Ema, US, provided insight into a good clinical practice (GCP) initiative, the FDA-EMA GCP Inspection Program. The pilot phase, which ran from Autumn 2009 to Spring 2011, aimed to reduce duplication of inspections. The scope included EMA centrally approved products and FDA products regulated by CDER. The scheme conducted periodic information exchanges on GCP-related information and collaborative inspections, allowing information to be shared on the interpretation of GCP. During the pilot phase, more than 250 documents were exchanged, facilitating improvements in bilateral inspection coverage and decision making. Twenty-three teleconferences were held during the pilot (and are ongoing on a monthly basis) to identify inspection reports of interest and applications pending at both agencies which would provide opportunities for collaboration. Thirteen collaborative inspections were held which promoted the understanding of inspection procedures, a greater harmonisation of the approach to risk-based site selection and avoidance of duplicate inspections. Since the pilot phase has fi nished, FDA/CBER have joined the collaboration and the monthly teleconferences continue, allowing the exchange of information and bilateral training opportunities. These building blocks will hopefully result in a greater confi dence in and mutual acceptance of inspection fi ndings.
SESSION 3: New EU medical device legislationReported by Rosalind Cox, Scientifi c Advisor, NDA Group
Full details of this session can be found in our report on the Medical Devices Symposium, later on in this issue. manfred Kohler, European Commission, directorate General Health and Consumers, Unit Health technology and Cosmetics (SaNCo B 2), discussed the future regulatory framework, covering the key changes proposed and the consequences of these changes. An outline was given of the current position and the next steps in the revision process.
SESSION 4: the role and activities of the irish medicines BoardReported by John Fletcher, Janssen, UK
In addition to licensing and inspection activities for medicinal products, the IMB also now oversees the protection of animals used for scientifi c purposes, as well as the organ donation and transplantation directive.To refl ect its full spectrum of responsibilities, the agency is planning to change its name.
This session, presented by Pat o’mahony, Chief Executive, imB, fi rst described the agency’s mission, which is “to protect and enhance public and animal health through the regulation of medicines, medical devices and healthcare products”. The range of activities in which the IMB is involved includes:l Authorisation of medicinal products for human and veterinary usel Inspection and licensing of manufacturers and wholesalers
(human)l Competent authority for medical devicesl Competent Authority for Blood Directive and for Tissues and Cells
Directivesl Competent Authority for advanced therapiesl Competent Authority for cosmeticsl Approval of human clinical trials and medical device clinical
investigations l pharmacovigilance/vigilancel Sampling and analysisl Enforcement (human)l Overseeing recallsl Issue of export certifi catesl Issue of GMP [good manufacturing practice] certifi catesl International representative functionl Advice to Governmentl Protection of animals used for scientifi c purposes l Organ donation and transplantation directive (this does not relate
to encouraging organ donation but rather to having oversight of the quality systems).As well as the aforementioned activities, the agency also
undertakes international duties and activities such as the European Commission and EMA Scientifi c Committees, Working Parties and Management Board, International Conference on Harmonisation (the IMB was at the recent international summit), Cooperation Agreements, HTA dialogue and EU benchmarking. There is currently

9Focus – Pharmaceutical Symposium
Pat O’Mahony, Chief Executive, Irish Medicines Board
www.topra.org Regulatory Rapporteur – Vol 9, No 12, December 2012
a global network of medicine agencies, of which the IMB is one, that will be visited in the second half of 2013 and audited against set criteria.
Mr O’Mahony then outlined the IMB’s strategic objectives. These were summarised into the following fi ve points:1 To enhance healthcare product safety and patient outcomes by
eff ective risk management and market surveillance2 To deliver clear, relevant and timely communications to patients,
consumers and healthcare professionals3 To improve service delivery within a high quality, risk-based
regulatory framework4 To infl uence legislation and policy development at European and
international levels for the benefi t of public and animal health5 To build future capabilities to meet evolving regulatory
requirements, and scientifi c and technological advances.The session was then concluded with the key challenges and
opportunities faced, such as new science and new therapies, balance of benefi t and risk – a question was raised as to whether the emergence of the EMA’s new pharmacovigilance risk assessment committee (PRAC) would change the landscape on counterfeit products – patient engagement and scarce resources for health budgets.
SESSION 5: Centralised ProcedureReported by Patricia Hurley, Regulatory Aff airs Manager, Global Regulatory Aff airs, PPD
This session, chaired by Brenton James, EU Consultant, covered the key activities, performance and achievements of the CHMP in 2012. It also gave the audience insight into some of the activities in this area undertaken by the IMB.
The opening session by dr Jens Heisterberg, Chief medical offi cer, danish Health and medicines authority, and danish CHmP member, covered several key activities undertaken by the CHMP, including its role in the new pharmacovigilance legislation, advice on using scientifi c advisory groups (SAGs) and its role in arbitration. With the introduction of the new pharmacovigilance legislation eff ective from July 2012 (Regulation (EU) No 1235/2010; Directive 2010/84/EU) and introduction of the PRAC, the concept of a “fresh pair of eyes” with a mandate covers all aspects of risk management of medicines could, in theory, lessen the workload of the CHMP. However, the CHMP’s role in reviewing new applications, SA, input into new guidelines, arbitration, and safety issues post-authorisation (after PRAC recommendation), is more than enough to keep the CHMP operating at maximal capacity. It was noted that with the introduction of the PRAC, there is no change to the structure of the CHMP; there is still one member and one alternate from each EU member state plus Norway and Iceland, up to fi ve co-opted members, but there are still no patient representatives and decisions are still taken by simple majority.
Dr Heisterberg presented on the function of scientifi c advisory groups (SAGs) and how sponsors could take advantage of consulting with SAGs. These groups, created by the CHMP, have expertise on key therapeutic areas and deliver answers on a consultative basis to specifi c questions addressed to them. Rapporteurs (or their representatives) together with the marketing
authorisation holder (MAH)/applicant are invited to SAG meetings, and on occasion and where appropriate, patient groups may also be appointed. A challenge often faced is fi nding experts without confl icts of interest. For sponsors, identifi cation of a potential need for SAG input should be made early in the procedure, and not when CHMP opinion is already split. It is important for sponsors to defi ne specifi c and appropriately worded questions to address to the SAG; in particular, SAGs should not be asked to do the full benefi t–risk assessment.
Dr Heisterberg also commented on the role of the CHMP in arbitration. The committee arbitrates when asked to “solve” disagreements in the mutual recognition procedure (MRP) or the decentralised procedure (DCP). CHMP arbitrations are not very common; in fact, there were only fi ve cases 2011. Typically, most arbitration issues are on bioequivalence.
To conclude his presentation, Dr Heisterberg highlighted some of the key focus areas of the CHMP for the coming year. Namely, (a) collaboration with the PRAC and working together with new pharmacovigilance legislation; (b) improvement of assessment reports and quality of assessment, including more transparency in the assessment of benefi t–risk; (c) focus on geriatric patients, who are still under-represented in clinical trials; (d) improved enforcement of post-authorisation measures; (e) better understanding of GCP fi ndings and their impact on benefi t–risk and (f) adaptive licensing.
The second presentation of this session: “The EMA Centralised Procedure Metrics, Perspectives for the Future, ORGAM DG”, was given by anthony Humphreys, Head of regulatory, Procedural and Committee Support, Ema. Mr Humphreys presented interesting metrics on the number of applications fi led under the optional and mandatory scope of the centralised procedure between January 2010 and September 2012; in terms of novel developments, 11 applications for advanced therapy medicinal products (ATMPs) were accepted under the mandatory scope thus far. In terms of applications fi led as independent self-standing applications (Article 8 (3)), it appears that obtaining SA correlates with positive outcomes, highlighting the importance for companies to seek centralised SA at key strategic milestones during product development. Mr Humphreys also detailed the rapporteurships undertaken by the member states with the UK, Germany and Sweden undertaking in excess of 80 procedures thus far in 2012.

10 Focus – Pharmaceutical Symposium
Anthony Humphreys, Head of Regulatory, Procedural and Committee Support, EMA
Regulatory Rapporteur – Vol 9, No 12, December 2012 www.topra.org
With the introduction of the pharmacovigilance legislation and formation of the PRAC, Mr Humphreys presented the structure of new rapporteur teams that will review new MAAs for centrally authorised products (CAPs) from December 2012. In brief, there will be an appointed CHMP and PRAC rapporteur/co-rapporteur; the PRAC rapporteur position will be open to all PRAC delegates with the selection criteria being the best possible scientifi c expertise and where possible, from a diff erent member state compared to the CHMP rapporteur and co-rapporteur. One of the most important points to note on the assessment of new applications is that initial comments on the risk management plan by the PRAC will be provided to the applicants as part of the Day 120 List of Questions. The CHMP and the PRAC will work to develop and maintain strong links between the two committees; this successful working relationship will be an integral part of the assessment process going forward.
The third and fi nal presentation of this session was given by david lyons, irish medicines Board (imB) and CHmP member, ireland. Dr Lyons presented on the experience of Ireland as rapporteurs and some of the key additional activities undertaken by the IMB. Between January 2003 and October 2012, the IMB had 75 items where they were classifi ed as rapporteur or co-rapporteur in the centralised procedure; these included new active substances, repeat applications, duplicates, line extensions, biological transport media and generics, but excluded variations, re-examinations and referrals. Dr Lyons presented experiences on the re-examination process in which the IMB has been involved. Re-examinations off er an interesting regulatory/scientifi c “laboratory” for examining why applications succeed or fail. The IMB acted as (co)rapporteur from 2001 to 2011 in eight re-examination procedures, in which there were four with positive outcomes (ie, CHMP opinion reversed) and four with negative outcomes. It should be noted that two of the four reversed opinions were negative by consensus or near consensus, and therefore through the re-examination process additional discussions and enthusiasm from SAG and rapporteurs is key. In most re-examinations it is likely not permitted to present new data, so it is necessary to put forward a new angle and rationale as to why a re-examination is deemed necessary and therefore worthy of an opinion to be reversed.
SESSION 6: Self-CareReported by Clare Lavery, Director, Global Regulatory Policy & Intelligence, Janssen Research & Development
This session provided an update on regulatory developments in the EU self-care arena. The session was introduced by Hubertus Cranz, director General of the aESGP, who explained that the self-care arena can be categorised into three distinct areas, namely medicines, food supplements and self-care medical devices. Interest in the self-care sector by politicians and health policy leaders is growing due to economic considerations and the realisation of the social benefi ts of self-medication. Fifty percent of pharmaceutical medicines sold (based on number of packs) are non-prescription products. Given this backdrop, Dr Cranz commented that there is a real need to consider to what extent the regulatory system can facilitate the availability of these medicines and what might be needed by way of improvements in the current system.
Zaide Frias, Head of regulatory aff airs Section, Ema, provided the EMA viewpoint with a presentation entitled: “EMA Update on Progress – Non-prescription Medicines in the Centralised Procedure”. The centralised procedure has been open to non-prescription medicines since 2005 and is the only regulatory procedure where there is a harmonised legal status across the EU for such products.
Eligibility for the centralised procedure is automatic for switches of products that have been authorised via the centralised procedure and is optional according to Article 3(2)(b) of Regulation (EC) No 726/2004 for products that represent signifi cant innovation or for reasons of “interests to patients” at Community level. To date, of the 11 eligibility requests granted, all have been on the grounds of the interests of patients.
Dr Frias mentioned that the CHMP discussions on product switches to non-prescription status are not just scientifi c in nature but are also focused on other aspects, such as national diff erences between the healthcare systems in the member states and the diff erent patient and healthcare professional attitudes. The use of suitable educational and risk management tools, such as product information, is a common topic of discussion at the CHMP, particularly as there is no intervention by a healthcare professional.
Approaches that can be helpful in overcoming the hurdles for product switches include use of benefi t–risk models specifi c for the non-prescription setting and dialogue with pharmacists and patients during development. Companies should aim to show benefi ts additional to “conventional” ones, such as effi cient use of the doctor’s time and rapid patient access.
Dr Frias spoke of the involvement of the PRAC. Its role will include assessment of renewal applications, safety referrals, and post-authorisation safety studies (PASS) for existing switches and assessment of risk management plans, periodic safety update reports (PSURs) and the European Union Reference Date (EURD) list for new switches. Dr Frias noted that the concept of public hearings under the new legislation represents a great opportunity for interaction with healthcare professionals and patients.
Glen Carpenter, Vice President, regulatory aff airs – EmEa, Johnson and Johnson, provided the industry viewpoint on over-the-counter (OTC) product switches. Dr Carpenter advised that there

11Focus – Pharmaceutical Symposium
Zaide Frias, Head of Regulatory Aff airs Section, EMA
www.topra.org Regulatory Rapporteur – Vol 9, No 12, December 2012
is a general trend towards more and more innovative switches by the industry as the “low-hanging fruit” has already gone. This has led to more novel considerations on whether a product is suitable for switching, such as whether patients can adequately self-monitor, whether there is a need for an associated medical device, and the importance of compliance on the particular disease being treated.
Consumers need reassurance that moving products to non-prescription status is not a refl ection of a lack of effi cacy. In this regard, Dr Carpenter commented that the industry could benefi t from more government support in some EU member states to provide this reassurance. The role of the pharmacist is particularly key in ensuring the success of a switched product by educating and advising consumers on the product. Information provided to the consumer, including the packs themselves, should be designed so as to help consumers make the appropriate choices.
Turning to regulatory considerations, Dr Carpenter noted that the role of the clinical overview is absolutely critical in supporting a product switch, bearing in mind that there are often additional factors to be justifi ed which go beyond the more conventional considerations of quality, safety and effi cacy. For example, not all indications are suitable for OTC use, and the indication for the non-prescription product can be diff erent compared with the prescription product. Similarly, the benefi t–risk decision must weigh the benefi ts of easier access against potential harm from unsupervised or inappropriate use.
Regulatory challenges include the diff erences in legal status of medicinal products across the EU, as these refl ect the diff erent member states’ views on conditions of sale. It can be diffi cult to accommodate the national requirements in the framework of the MRP/DCP. Although switching via the national route is relatively straightforward, this can result in disparate end-products in the member states in terms of product labelling. Naming of non-prescription products is also challenging, as the typical expectation is that the invented name cannot be the same as that of the prescription product.
Looking to the future, Dr Carpenter highlighted some of the ongoing eff orts for identifying new areas for switching. Initiatives have been undertaken by the Commission and at member state level to increase the potential for product switches. One such example is the MHRA forum on widening access to medicines via reclassifi cation.
Dr Carpenter concluded by stating that the preoccupation with risk has hampered the progress of product switching. Industry needs to reassure and engage more with patients, doctors and other healthcare professionals on the benefi ts of these products. Encouraging stakeholders to work together will increase the chances of successfully driving the reclassifi cation agenda forward.
dr olive Smyth, imB, provided an overview of the reclassifi cation process in Ireland. Simplifi cation of the application process in 2007 has led to an increase in the number of applications submitted to the IMB, although Dr Smyth commented that there is still room for further improvement.
The IMB determines the legal classifi cation of a product and the method of supply and promotion which, for non-prescription products, is either General Sales List (GSL) or Pharmacy medicine (P). Following changes to the legislation, the legal status of a product in Ireland is now linked to the product itself rather than the substance. The agency maintains a list on its website of the legal classifi cation of all authorised medicines in Ireland.
Concerning the assessment process, Dr Smyth highlighted the
need for a good quality clinical overview. A risk management plan is required for all new national applications, and non-prescription products may require additional risk minimisation measures.
Dr Smyth encouraged applicants to engage in dialogue with the IMB prior to submission and for companies to pay particular attention to the correct legal status and to the benefi t–risk of the product. She also noted the IMB guidance of October 2010, as there are some national-specifi c requirements. Dr Smyth advised companies to introduce the brand name in the patient information early in the procedure. For multi-state applications, she also advised that companies should bring to the attention of the Reference Member State (RMS) any diff erences in non-prescription status in the member states. Dr Smyth welcomed the new pharmacovigilance legislation in the EU, stating that she expects the improved transparency and communication measures will be a positive step for OTC products.
Dr Smyth fi nished her presentation by referencing the IMB Consultative Panel on the Legal Classifi cation of Medicines. This is a new initiative looking at ways to increase patient access to medicines and examining the role of the agency in this process. A public consultation was conducted in 2011 asking stakeholders to provide input on the types of product they would be interested in utilising. Policy guidance is expected in this area.
SESSION 7: availability of medicines: How to Solve the ChallengesReported by Julie Warner, Senior Manager, Regulatory Aff airs, Clovis Oncology
ann o’Connor, director of authorisation and registration, imB, and Helene thybo, Corporate regulatory intelligence Specialist regulatory aff airs & Safety, leo Pharma, denmark, chaired this session, focusing on issues related to the availability of medicines.
Kristin raudsepp, director General, ravimiamet (Estonian agency), Estonia, opened the discussions by providing a considered view on the availability of medicines from a regulator’s perspective. She highlighted the defi nition of problems with availability, ie, when a medicinal product is needed by patients and physicians and could be available for their use, but is either (a) lacking a marketing

12 Focus – Pharmaceutical Symposium
Ann O’Connor, Director of Authorisation and Registration, IMB
Regulatory Rapporteur – Vol 9, No 12, December 2012 www.topra.org
authorisation in the member state; (b) subject to a valid marketing authorisation but is not marketed in the member state; or (c) subject to supply interruptions. Regardless of the reason, the situation in Estonia is apparent: of approximately 95 centrally authorised products, only around 30 are marketed in Estonia. Similarly, for the MRP/DCP, only around one-third of the authorised products are actually marketed. Even though Estonia works diligently in the EU procedures and often takes on the role of (co-) rapporteur for applications, this has not aff ected product availability.
Dr Raudsepp noted that this situation is not limited to Estonia, as highlighted by the results of her survey conducted in 2012. Most EU countries are experiencing problems with availability of medicines, and are actively trying to resolve this by exchanging information to fi nd solutions for physicians and patients. An authorised product may not be marketed owing to the unwillingness of MAHs to take on extra costs (such as pharmacovigilance and scientifi c services) for small markets; the preparation of national language packs/package leafl ets for small markets such as the Baltic States may also be a deterrent. Worryingly, many of the supply shortages aff ect life-saving medicines and oncology products. MAHs do not always comply with the requirement to notify competent authorities two months in advance of an anticipated shortage in supply. Although Directive 2001/83/EC is silent on whether the MAH or the competent authority is responsible for resolving issues around availability, measures thus far to incentivise supply for an MAH (eg, the sunset clause) sometimes result in a product being withdrawn altogether.
Industry has often mentioned that local exemptions from the requirement to provide full packaging/package leafl ets in national languages would be helpful, and the recent revisions to legislation make this a possibility, at least on a temporary basis. Further initiatives (such as the concept of a “Baltic pack”, with review and approval coordinated by one Baltic member state) should also help. Nevertheless, availability issues are a drain on regulators’ resources and MAHs must also take responsibility, with recommendations to have two registered active substance manufacturers, and maintain two months’ drug product supply in stock. Given the price of medicines, it should not solely be companies deciding which patients have access to these. MAHs are also encouraged to propose language packs at the time of the pre-MAA interactions with EU regulators.
maura Kinahan, Pfi zer Healthcare, ireland, then highlighted
product shortages in the US, where fi gures are regularly made available; at present, the majority of drug shortages concern sterile injectable products. In the UK, 29 branded medicines are currently listed as low/no stock, and 90 are similarly categorised in Ireland. These shortages can be caused by manufacturing issues (eg, contamination, lack of active substance), regulatory action, or increased demand (eg, if a competitor product is suddenly unavailable). The consequences of these shortages are far-reaching and aff ect patients (who may at best be underdosed or, at worst, exposed to risk and must cope emotionally with changes to treatment), healthcare professionals, and regulators.
Unfortunately, MAHs often respond to changes in demand over the lifecycle of a product by adjusting manufacturing capacity and, once decreased, it can be diffi cult to increase again quickly to meet demand. However, MAHs can mitigate some supply issues by adequately assessing risks in the supply chain, employing a culture of quality and compliance in manufacturing operations (including distribution and supply), and by prioritising critical care products. To this end, eff ective communication across functions is essential, as is customer communication so that all possible measures can be taken to mitigate supply.
Dr Kinahan noted that there is still scope for further collaboration; namely, harmonisation of label wording to the greatest extent possible would be valuable, as would acceptance of joint pack labels for countries with similar language and content requirements (to overcome diff erences in timelines for implementation of changes etc). Dr Kinahan closed her presentation by reminding delegates that, regardless of the reason for the lack of availability, there is always a patient to consider.
Peter Bachmann, Chair of Cmdh, Head of Unit ‘Cmdh’, department of European and international aff airs, Federal institute for drugs and medical devices (Bfarm), commented on the oligopoly nature of the current market, with industry dominated by a number of companies selling small volume, high cost products. This strategy means they are vulnerable to shortages as they cannot adapt their capacity quickly to meet rapid increases in demand. Many of the products involved require specialist manufacture, and therefore the costs cannot be decreased. As written, Directive 2001/83/EC assumes that enough product is available, which is not always the case. While the Coordination Group for Mutual Recognition and Decentralised Procedures – human (CMDh) can assist, its main role is to exchange information and coordinate assessment of available data on alternative products/manufacturers that could be used in the event of supply shortages. The current EudraMail system covers this well, as do the EU worksharing procedures (for example, the worksharing used for the supply issues with rubber stoppers manufactured by West Pharmaceutical Services). Through these activities, it has become apparent that applications for many products are not harmonised across the EU.
One solution to quickly respond to regulatory supply chain issues could be the use of a “superfast” repeat-use MRP (which requires the concerned member state to confi rm on Day 0 that it has no concerns regarding potential serious risks to public health). This can be completed in one day (followed by the 30-day national step) but requires good communication all round, and obviously means that the concerned member state is “in the driving seat” for the procedure. Dr Bachmann concluded his presentation by noting that a major question for the near future is sustainability of the known active substances/products that are currently used as the backbone for many medical therapies.
A discussion followed during which the speakers and delegates discussed shortages associated with protamine sulphate; the

13Focus – Pharmaceutical Symposium
John Lynch, Director of Compliance, Irish Medicines Board
Helder Mota Filipe, Vice-President of Executive Board, INFARMED – National Authority of Medicines and Health Products, IP Portugal
www.topra.org Regulatory Rapporteur – Vol 9, No 12, December 2012
certifi cation of GMP compliance for active substances manufactured in third countries and the potential impact of this on availability of medicines in the EU. Interestingly, Dr Bachmann noted that at the present time, it is not known how many active substances are authorised in the EU (but that the list of products for human use foreseen in Article 57(2) of Regulation 1235/2010 will help with this). It was also noted that the EMA currently shares information on the shortage of centrally authorised products with the US FDA in an eff ort to establish a useful forum. Finally, Ann O’Connor, as a chair of the session, concluded that supply shortages are not a problem for a single party, but that industry and regulators must work together to put patients fi rst.
SESSION 8: toPra annual review
TOPRA’s Annual Review was presented by Lynda Wight, Patrizia Nestby and David Jeff erys. Coverage of this session will be reported in the TOPRA members’ newsletter, InTouch.
SESSION 9: Falsifi ed medicinesReported by Julie Warner, Senior Manager, Regulatory Aff airs, Clovis Oncology
maria João morais, infarmed, Portugal, and John lynch, director of Compliance, irish medicines Board, jointly chaired a thought-provoking session that strived to highlight awareness of the extent of falsifi ed medicines (fake medicines intended to mimic genuine medicines) and the serious risks these pose to global public health.
Mr Lynch set the scene by providing an overview of the Falsifi ed Medicines Directive (2011/62/EU, coming in to force on 2 January 2013) and the measures it contains to introduce eff ective strategies to combat falsifi ed medicines. There is a perception that the main source of falsifi ed medicines is rooted in internet/online pharmacies; however, many falsifi ed medicines have also entered the legal supply chain, putting many more patients at risk. Historically, regulators did not inspect in-transit areas such as free zones or customs warehouses, but this approach needs to change in today’s challenging environment. In recent years, drugs such as Plavix, Zyprexa and Casodex have all been counterfeited in Asia and these products have entered the legal supply chain globally, meaning thousands of patients are at risk from underdosing and therefore poorly controlled disease, as well as signifi cant safety risks. To combat these problems, the Directive includes four pillars, the fi rst of which focuses on safety features for product packaging: a unique identifi er for each pack (eg, a linear or 2D barcode, or radio frequency identifi er), and tamper-evident seals. Both will be mandatory for prescription-only medicines and not required for OTC products. Responsibility for implementation of these measures and the establishment of a repository to contain information on such safety features lies with the EU Commission, and they will not be in eff ect until January 2017.
The second measure includes requirements for supply chain parties to provide assurance on the quality of the product, including active pharmaceutical ingredient (API) manufacturer
inspections, appropriate GMP for excipients, reporting of suspected falsifi cation to competent authorities, and verifi cation of the status of manufacturers, importers and distributors. Thirdly, APIs must be manufactured to GMP (note that most sites in India and China have not yet been inspected by EU agencies), manufacturers and importers must register with the agency in their member state, and be subject to risk-based inspections. Import controls will also be placed on APIs originating outside the EU. Finally, internet pharmacies will be required to notify member states of their address, website, product off ered for sale, and add an obligatory logo to their website.
david Shore, Pfi zer, ireland, provided probably the most startling talk of the day, challenging the delegates to identify genuine and falsifi ed products. The limited success of this task was not surprising, given that many falsifi ed medicines are virtually indistinguishable from the genuine article, and laboratory testing is the only way to defi nitively identify them. Mr Shore showed some shocking images of falsifi ed medicine production sites and the ingredients they include (including boric acid, leaded road paint, fl oor wax, heavy metals, pesticides and brick dust). Pfi zer itself has seen counterfeit versions of more than 60 of its own medicines, across many therapeutic areas. This organised, global crime is growing, and law enforcement operations such as “Singapore”, “Medi-Fake” and “Pangea” estimate up to a staggering 34 million illegal medicines make their way across Europe’s borders each year. Not all of these are detected and some do reach pharmacies, internet pharmacies and patients; sadly, deaths attributed to counterfeit medicines are starting to emerge. Industry and regulators need to work together globally to identify sources of falsifi ed medicines, raise public awareness and education on the risks and sources of counterfeit medicines, and shape the regulatory environment through lobbying and media campaigns. In short, the issue of counterfeit medicines is a growing global, translational problem that will take global cooperation to address.
Helder mota Filipe, Vice-President of Executive Board, iNFarmEd – National authority of medicines and Health Products, iP Portugal, provided insight into the activities undertaken by Infarmed to coordinate the fi ght against falsifi ed medicines with third countries with Portuguese as the main language (Angola, Cape Verde, Brazil and Mozambique). The project focused mainly on the key areas of alert networks, regulatory dialogue/exchange of information, special advisory groups and specialist workshops. There were, however, a number of cultural diff erences to consider, including the fact that hospital supply in African countries is an informal market, and the risk of falsifi ed medicines is therefore high.

14 Focus – Pharmaceutical Symposium
Avril Daly, CEO, Fighting Blindness, European Patient Forum, IrelandDavid Shore, Pfi zer, Ireland
Regulatory Rapporteur – Vol 9, No 12, December 2012 www.topra.org
Several meetings have been held to date, and the success of these has been greatly helped by involving all stakeholders (each with a single point of contact), harmonising best practice, sharing information and expertise, and having a common language. There were some constraints, however; for example, Angola has a large border, making it more diffi cult to police, much bureaucracy exists, and there was a general desire to have testing laboratories in place prior to the legislation (when it would ideally be the reverse). Based on its experience, Infarmed’s recommendation is for other EU competent authorities to establish similar arrangements with common language countries, so that global networks exist to proactively combat falsifi ed medicines.
avril daly, CEo, Fighting Blindness, European Patient Forum, ireland, closed out the presentations with a patient’s perspective on falsifi ed medicines, stating that all citizens become patients eventually. The internet is a major source of falsifi ed medicines and, in order to address this, we need to fi rst look at why patients buy medicines online (which could include living in a remote area, and lack of mobility, but also many other reasons). However, online purchases deprive the patient of the patient-doctor-pharmacist relationship, which is valuable and needs to be maintained. While the Directive is welcomed, the European Patients’ Forum had wanted it to also include provision for involvement of patient organisations, a safety logo on all medicines, a mechanism to report illegal internet pharmacies, a strong enforcement mechanism, international cooperation and a study of why patients buy online and measures to address this.
Patient organisations are uniquely placed to communicate eff ectively with patients on their diseases and treatments, and are thus a vital resource. Patients need to be empowered through health literacy and to have easily accessible high-quality information to allow them to become involved in the quality and safety of medicines.
SESSION 10: Patient information in 2020Reported by Andrew Germain, Director Regulatory Aff airs, Daiichi-Sankyo Development Ltd
This fi rst session on the last day of the Symposium was chaired by angelika Joos, Head regulatory Policy EU & most of World, mSd (Europe) inc, Belgium, and Jan macdonald, Head of Patient information Quality, mHra. Varied stakeholders have raised concerns around the true usefulness of current “paper” patient
information (PILs) for medicines, which have remained unchanged for many years, and in this session four speakers from academia, industry, regulatory and patient groups provided a perspective of where changes and improvements may lead to in 2020, with important common themes and aspirations.
denis Costello, Web Communications manager, EUrodiS rare diseases, Europe, presented the patient view from an organisation representing over 500 patient groups in the EU. He raised some key questions: Is the information available with medicines good enough? Where do patients obtain information from? Who do patients trust? It was Mr Costello’s view that patients today perceive there to be a lack of accessible and useful medicines information in spite of all medicines being accompanied by written information. Key information which patients actively search for include the correct means of taking the product for optimum eff ect. Many patients search the internet, but report they are directed to predominantly US-based websites and that accurate and reliable information can be very varied. Data show that around 55% of cancer patients, after diagnosis, use the internet to search for information on their condition and medicines available, and that 20% use information from the internet in their decision-making on therapy.
Mr Costello noted the need for those providing information to consider the level of health literacy of the patients they are targeting, so that the information provided truly meets their needs. He discussed the increasing use of social media by patient groups and believes that greater use needs to be made of the electronic space so that patients are more easily able to access the information they need in a timely manner.
He concluded that there is a mismatch between the patient’s desires and the way in which information is prepared and provided to patients in the EU. In thinking towards 2020, Mr Costello envisions a greater need to step away from the written word and make more information available electronically, so that patients searching for information about their disease and its treatment can be more readily engaged.
ann-margaret talberg, mSd and representing liF, Sweden, built on the patient views expressed above and presented fi ndings in Sweden from research by LIF (the trade association for the research-based pharmaceutical industry in Sweden) on how to improve information for patients. In her opening remarks, ms talberg reminded the audience that the core purpose of the statutory information is for the manufacturer to communicate with patients to convey key information for the safe and eff ective use of a product. She pointed out that when patients cannot understand the information provided, meeting regulatory hurdles such as user testing becomes irrelevant.
The research in Sweden evaluated attitudes of patients towards leafl ets and how these could be made more patient-friendly. The study involved patients ranging from 18 to 75 years of age and the fi ndings included:l Doctors and pharmacists are highly trusted as providers of
accurate and useful informationl The internet can be a source of useful information for medicines,
but problems are perceived with the objectivity and credibility of information.Although leafl ets are seen as being relevant to patients and
generally well structured, this contrasts with negative views on poor design and layout, small and dense text and information which is considered to be too long and repetitive.

15Focus – Pharmaceutical Symposium
Jan MacDonald, Head of Patient Information Quality, MHRA
www.topra.org Regulatory Rapporteur – Vol 9, No 12, December 2012
In addressing patients’ aspirations, the research looked at the simplifi cation of patient leafl ets involving a reduction in wording of more than 40%. In the test leafl et, sections were more readily and uniformly structured and the feedback for such revisions was favourable. Even so, the language used in the leafl ets was still considered to be too complex for good understanding.
Ms Talberg highlighted the following key messages in her conclusion: l Patient leafl ets are seen as important and crediblel Target patient audiences have diff ering needsl The simpler design profi led in the research was much better
received than the current standardl Such revised leafl ets still meet the need for information for safety,
effi cacy, utility, usability and security.A complementary perspective was then given by theo raynor,
Professor of Pharmacy Practice, School of Healthcare, University of leeds and luto research, UK, who outlined the learnings from academic research and experience in the UK. He fi rst discussed lessons learned from user testing and how improvements can be achieved now, before turning to consider the goals for 2020 in medicines information. He looked at how patients are served in the information landscape, and the way in which information is provided to healthcare professionals, and where there are current gaps. Academic research continues to show that the concerns expressed by earlier speakers – such as the complexity and length of the information – remain problematic and that patients value information provided by their healthcare professionals. The written word should not be a substitute for the patient-doctor interaction: the views of patients are that personalised information provides greatest satisfaction along with information which sets any risks in the context of their disease.
In looking at the fi ndings from the user testing carried out over the last seven years it was apparent that both the language used and the presentation of the information were critical in patient acceptability. Separately, the free oral opinions expressed in the research regarding general impressions of the patient information provided a rich source of detail on what improvements could be made, but frequently this has not been addressed.
Prof Raynor then considered developments in the templates provided by the European Commission and how these have helped with greater balance in the information provided. Research fi ndings were then presented on patients’ understanding and acceptability of numerical information to convey effi cacy of the medicine. The inclusion of “benefi ts” information can incentivise patients, but Prof Raynor cautioned that the use of numbers can cause its own problems and that many patients struggle to understand numerical data.
With regard to European public assessment reports (EPARs) and their usefulness to the patient, recent research was described which showed that many patients are unaware of EPARs, and that on balance these are not particularly useful and not seen as targeted for the patient. Prof Raynor showed how simple changes to the presentation of the information could achieve greater accessibility and acceptability of the information presented.
Delegates were then asked to consider that the goals for 2020 should be high quality leafl ets that are valued by patients. User testing should be considered as an iterative process to assist with this and not be seen as a regulatory hurdle of a single successful test. To maximise benefi ts, the information made available to patients
should encompass good practice in information design as well as taking account of the available research. Prof Raynor touched on the need to also consider the health literacy of the population and take notice of the all the information provided by participants in the user testing process. He spoke about other collaborative research which is underway, looking at how the use of summary information in leafl ets could better assist in meeting the goals for 2020. He highlighted the new requirement in the recent legislative amendments which asks the European Commission to produce a report on the shortcomings of patient information and determine what changes could be made to improve these.
Co-chair Jan MacDonald gave the fi nal presentation of the session, off ering a regulator’s perspective on future needs. A key theme was for regulators and the pharmaceutical industry to address the acknowledged gap between and an idealised situation and practical reality. There were many points of concurrence with prior speakers:l PILs are seen as too long and repetitive; information hierarchy is
not geared to the patient and text font is too smalll The diversity in patients’ needs are not well represented in current
informationl Poor quality English (for UK leafl ets) does not engage the reader
and causes problems in translation across the Communityl The chance of risk is not set in the context of possible benefi tl In bridging the gap towards 2020, four key ideals were put forward
concerning the quality of the information, the need for it to be targeted, provided in a timely manner and to be balanced. The factors which relate to high quality were set out, and these
principally relate to colloquial language, consistent information and better use of information design principles, as well as helping patients fi nd information from other sources. The use of templates is deemed to be stifl ing innovation.
While it is generally agreed that patients are more likely to relate to personalised information from healthcare professionals, providing targeted information is diffi cult within the current legislation and so communication opportunities are lost.
The information needs of patients vary at diff erent times in their medicine-taking journey and making the information available in advance of prescribing decisions is believed to be important. Concordant decision-making on the appropriate prescription

16 Focus – Pharmaceutical Symposium
Michael Foy, Group Manager – Vigilance, Intelligence and Research, MHRA
Regulatory Rapporteur – Vol 9, No 12, December 2012 www.topra.org
medicine could be enhanced if the information was more accessible. The audience was encouraged to consider developments in “real
time” access to information through media such as smart phones and iPads, and in the possible use of “quick response codes” which could help with the information ideals and take patients to further internet-based information about their disease and its treatment.
SESSION 11: the New Pharmacovigilance legislation – the Experience after implementationReported by Andrew Germain, Director Regulatory Aff airs, Daiichi-Sankyo Development Ltd
Facilitated by Eamonn mcGowran, regulatory aff airs manager/QP for Pharmacovigilance, Newport Pharmaceuticals limited, ireland, and chaired by Joan Gilvarry, imB, ireland, speakers from industry, the MHRA and the IMB gave updates and perspectives of their experiences of the new pharmacovigilance legislation following its introduction in July 2012.
deirdre mcCarthy, director, Customer delivery Europe, lifecycle Safety & infrastructure management, Quintiles, ireland, described
some of the background leading to the new pharmacovigilance legislation in the EU, the main aspects aff ecting industry, and current experience. The aim of the new regulation is to give a more consolidated pharmacovigilance system in the EU and indeed the origins for this started many years ago with the “Fraunhofer Report” on the appraisal of European pharmacovigilance systems, in 2006. Drivers for a new system were the need for simplifi cation, increasing development of monoclonal antibodies and gene therapeutics, the proliferation of large epidemiological and adverse drug report databases, and the increased interest of the EU public. Against this backdrop was also the concerning data that ADRs were the fi fth most common cause of hospital deaths.
The new legislation was adopted by the European Parliament in September 2010, and came into force on 2 July 2012 in the form of a new Directive (2010/84/EU) amending the requirements of Directive 2001/83/EC. Figure 1 details how this change has aff ected regulation and the prior main guidance in EudraLex Volume 9A.
While the full impact of the new legislation is far too broad to cover in a symposium session, some main facets were highlighted, including the new defi nition of ADRs. Directive 2010/84/EU cites:
11. Adverse reaction: A response to a medicinal product which is noxious and unintended. “For the sake of clarity, the defi nition of the term ‘adverse reaction’ should be amended to ensure it covers noxious and unintended eff ects resulting not only from the authorised use of a medicinal product at normal doses, but also from medication errors and usage outside the terms of the marketing authorisation, including the misuse and abuse of the medicinal product” and thus includes occupational exposure.
Reporting convention for all serious suspected adverse reactions that occur in the EU and in third countries is within 15 days.
Ms McCarthy also described key changes as they aff ect the pharmaco-vigilance system Master Files, Quality Systems, patient reporting, literature monitoring, signal detection and periodic safety update reports. She also described how companies are reacting – many standard operating procedures (SOPs) within companies relating to pharmacovigilance and cross-functionally need to change, and medical information teams need to be trained in the new fundamental defi nition for ADRs. Company staff are being trained by the EMA in the XEVMPD [the extended EudraVigilance Medicinal Product Dictionary] system.
michael Foy, Group manager – Vigilance, intelligence and research, mHra, UK, reported on the UK agency experience to date. From the
Figure 1: How the new pharmacovigilance legislation aff ects regulation.
Directive2001/83/EC
Directive2010/84/EU
16 GVP ModulesEudraLex Volume 9A
Regulation (EU)1235/2010
Regulation (EC)726/2004
Centrallyapprovedproducts
Nationallyapprovedproducts
National Regulation National Regulation amended
17Focus – Pharmaceutical Symposium
www.topra.org Regulatory Rapporteur – Vol 9, No 12, December 2012
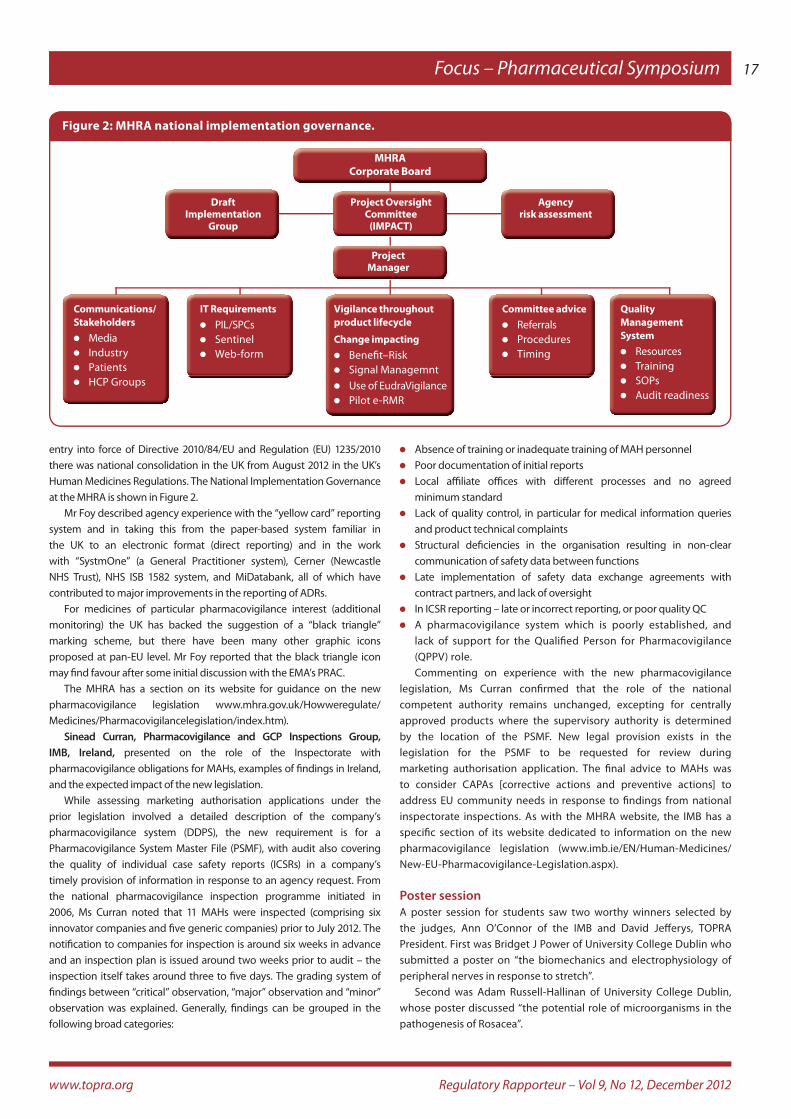
entry into force of Directive 2010/84/EU and Regulation (EU) 1235/2010 there was national consolidation in the UK from August 2012 in the UK’s Human Medicines Regulations. The National Implementation Governance at the MHRA is shown in Figure 2.
Mr Foy described agency experience with the “yellow card” reporting system and in taking this from the paper-based system familiar in the UK to an electronic format (direct reporting) and in the work with “SystmOne” (a General Practitioner system), Cerner (Newcastle NHS Trust), NHS ISB 1582 system, and MiDatabank, all of which have contributed to major improvements in the reporting of ADRs.
For medicines of particular pharmacovigilance interest (additional monitoring) the UK has backed the suggestion of a “black triangle” marking scheme, but there have been many other graphic icons proposed at pan-EU level. Mr Foy reported that the black triangle icon may fi nd favour after some initial discussion with the EMA’s PRAC.
The MHRA has a section on its website for guidance on the new pharmacovigilance legislation www.mhra.gov.uk/Howweregulate/Medicines/Pharmacovigilancelegislation/index.htm).
Sinead Curran, Pharmacovigilance and GCP inspections Group, imB, ireland, presented on the role of the Inspectorate with pharmacovigilance obligations for MAHs, examples of fi ndings in Ireland, and the expected impact of the new legislation.
While assessing marketing authorisation applications under the prior legislation involved a detailed description of the company’s pharmacovigilance system (DDPS), the new requirement is for a Pharmacovigilance System Master File (PSMF), with audit also covering the quality of individual case safety reports (ICSRs) in a company’s timely provision of information in response to an agency request. From the national pharmacovigilance inspection programme initiated in 2006, Ms Curran noted that 11 MAHs were inspected (comprising six innovator companies and fi ve generic companies) prior to July 2012. The notifi cation to companies for inspection is around six weeks in advance and an inspection plan is issued around two weeks prior to audit – the inspection itself takes around three to fi ve days. The grading system of fi ndings between “critical” observation, “major” observation and “minor” observation was explained. Generally, fi ndings can be grouped in the following broad categories:
l Absence of training or inadequate training of MAH personnell Poor documentation of initial reportsl Local affi liate offi ces with diff erent processes and no agreed
minimum standardl Lack of quality control, in particular for medical information queries
and product technical complaintsl Structural defi ciencies in the organisation resulting in non-clear
communication of safety data between functionsl Late implementation of safety data exchange agreements with
contract partners, and lack of oversightl In ICSR reporting – late or incorrect reporting, or poor quality QCl A pharmacovigilance system which is poorly established, and
lack of support for the Qualifi ed Person for Pharmacovigilance (QPPV) role.Commenting on experience with the new pharmacovigilance
legislation, Ms Curran confi rmed that the role of the national competent authority remains unchanged, excepting for centrally approved products where the supervisory authority is determined by the location of the PSMF. New legal provision exists in the legislation for the PSMF to be requested for review during marketing authorisation application. The fi nal advice to MAHs was to consider CAPAs [corrective actions and preventive actions] to address EU community needs in response to fi ndings from national inspectorate inspections. As with the MHRA website, the IMB has a specifi c section of its website dedicated to information on the new pharmacovigilance legislation (www.imb.ie/EN/Human-Medicines/New-EU-Pharmacovigilance-Legislation.aspx).
Poster sessionA poster session for students saw two worthy winners selected by the judges, Ann O’Connor of the IMB and David Jeff erys, TOPRA President. First was Bridget J Power of University College Dublin who submitted a poster on “the biomechanics and electrophysiology of peripheral nerves in response to stretch”.
Second was Adam Russell-Hallinan of University College Dublin, whose poster discussed “the potential role of microorganisms in the pathogenesis of Rosacea”.
MHRACorporate Board
DraftImplementation
Group
Agencyrisk assessment
Project OversightCommittee
(IMPACT)
ProjectManager
Communications/Stakeholdersl Medial Industryl Patientsl HCP Groups
Vigilance throughoutproduct lifecycle
Change impactingl Benefi t–Riskl Signal Managemntl Use of EudraVigilancel Pilot e-RMR
IT Requirementsl PIL/SPCsl Sentinell Web-form
Committee advicel Referralsl Proceduresl Timing
Quality ManagementSysteml Resourcesl Trainingl SOPsl Audit readiness
Figure 2: MHRA national implementation governance.

18 Focus – Pharmaceutical Symposium
Caitriona Fisher, Manager of Chief Executive’s Offi ce/Quality Manager, Irish Medicines Board
Regulatory Rapporteur – Vol 9, No 12, December 2012 www.topra.org
IMB PARALLEL SESSIONS
SESSION 1: Compliance with marketing authorisations
Chaired by Caitriona Fisher, manager of Chief Executive’s offi ce/Quality manager, imB, this session’s focus was on the role of the MAH in ensuring compliance with marketing authorisations.
John lynch, director of Compliance, imB, outlined the agency’s experiences from the inspection of MAH regulatory groups and from its monitoring of compliance with advertising regulations. He provided fi ve strategic recommendations for MAHs. These included the need for clarity around the roles and responsibilities of the regulatory group, manufacturer, sales and marketing and distributor, as well as a clear understanding of process complexity and coupling, a properly designed quality system and linkages to be supported by clear technical agreements.
On advertising, Mr Lynch emphasised the importance of adherence to the summaries of product characteristics (SmPCs) in drawing up prescribing information and of the training given to sales representatives. The need to ensure that any grants/gifts are of low value and are relevant to the practice of medicine was emphasised.
An industry perspective was then given by Natalie Beasley, Senior regulatory aff airs Project Executive, amdipharm, UK, who described her company’s experiences in dealing with MA compliance for multiple products, including those bought in from or divested by other companies. She outlined how to avoid “registration drift” and highlighted:l The need for due diligence around acquisitions of MAsl The challenges presented by the age of the dossierl The types of controls needed for contract manufacturers l The need for appropriate quality systems and knowledge
management to ensure continuity of compliance. During the panel discussion, the audience highlighted the need
for the regulatory group/manufacturer interaction to be two-way and well defi ned. Therefore, the regulatory group needs to be satisfi ed as to the MA compliance systems operated by the manufacturer and vice versa.
SESSION 2: Herbal medicines regulatory Update
This session gave an overview of key issues relating to regulation of traditional herbal medicinal products (THMPs).
mike morris, director Scientifi c aff airs, imB, discussed the classifi cation of herbal and borderline products and the role of the Irish Medicines Board (IMB) Classifi cation Committee in this process. Delegates were told that the borderline area between medicinal products and foods is a complicated issue, particularly for THMPs. The IMB has developed lists of herbal substances acceptable/not acceptable in THMPs as guidance for industry, and this information is available on the IMB website.
Many medicinal herbal products have been marketed as food supplements and this is an area of concern for the IMB. When classifying products, companies are required to take full account of the defi nition of a medicinal product (Article 1 Directive 2001/83/EC, as amended) and should also refer to the published IMB guidance.
The subject of the second presentation, given by Niamh Curran, Pharmaceutical assessor, imB, and anna Cunney, medical offi cer, imB, was key considerations in making a good application for a THMP registration. There are recurrent issues or defi ciencies in the dossiers submitted under the simplifi ed registration scheme. Specifi c areas for concern in the clinical and quality sections of the applications were highlighted in order to provide assistance to companies in preparing new dossiers for submission.
It was emphasised that the quality dossier should contain suffi cient information on the herbal substance and the clinical dossier should contain a detailed expert report and all relevant literature references in the initial application.
lorraine Nolan, distribution manager, imB, gave the fi nal presentation focused on the IMB’s policy on the end of “transitional protection” for THMPs on the market, at the time of coming into force of the regulations. The market surveillance carried out thus far has highlighted areas of non-compliance, at both wholesale and retail level, which include incorrect classifi cation of THMPs as non-medicinal and supply of non-transitionally protected THMPs. Key contributory factors to the non-compliances observed are poor knowledge of the legislative and policy requirements for THMPs and problems with product classifi cation.
The session provided a high level overview of key aspects of the regulatory control of herbal products and emphasised areas which should be considered fully when it is intended to place such products on the market.
SESSION 3: Current developments in Pharmaceutical Preparations
Mike Morris, IMB, chaired this session with its focus on developing an understanding of the most common defi ciencies identifi ed during assessment of the Drug Substance (DS) and Drug Product (DP) sections of MAAs. The discussions were aimed at improving the quality of the Chemistry, Manufacturing, and Controls (CMC) part of MAAs.
The session also aimed to give a brief overview of Quality by Design (QbD)/Process Analytical Technology (PAT) developments and to give a high-level overview of the presentation of CMC sections expected to

19Focus – Pharmaceutical Symposium
www.topra.org Regulatory Rapporteur – Vol 9, No 12, December 2012
be submitted in support of QbD/PAT in an MAA.mirza Catibusic, Senior Pharmaceutical assessor, imB, outlined IMB
experiences from assessment of MAAs, and Sarah Fitzgerald, associate director Global CmC regulatory aff airs, Pfi zer, ireland, gave a practical example of her company’s experience in dealing with PAT submission for a human medicinal product. The key points included:l Details of the most common defi ciencies in the CMC part of an initial
MAA, with recommendations for MAHs on how to address those defi ciencies in an eff ective manner. These included the need to:
l Follow the Notice to Applicants (NtA) – Presentation and format of the dossier – Common Technical Document (CTD)
l Clearly adhere to all relevant and applicable guidelines l Provide a full scientifi c justifi cation if any deviations from the
Guidelines are proposed.l The key and probably major defi ciencies that should be focused on are: l Inadequate defi nition of starting materials l Absence of discussion on the carry-over of impurities/by-products
from key materials in the process l Insuffi cient stability data to support re-test period (DS) or shelf-
life (DP) l Poor validation of analytical methods, with one of the
most common issues being where the stability indicating characteristics of all assay and impurity determination methods are not demonstrated and mass balance is either not adequately addressed or not addressed at all.
l The pharmaceutical development section should be clearly presented and the entire development of the product should be scientifi cally discussed and presented in a logical and transparent way. The fi ndings of the development studies need to be appropriately transferred to all relevant CMC sections. This relates both to DS and DP.
l A high-level overview of regulatory expectations in relation to submission of MAAs that contain full or parts of QbD and PAT was presented. Links to the key guidelines and documents were provided, including ICH guideline Q11 on development and
manufacture of drug substances, and it was noted that the process validation guideline was being revised to include continuous process monitoring/verifi cation. Manufacturers and MAHs are highly encouraged to scientifi cally design product and process performance characteristics to meet specifi c objectives, and not to merely empirically derive them from performance of test batches. Advice may also be requested from the EMA’s PAT Team.A practical industry example of submitting an application with
concepts of PAT attracted particular attention from the audience. The presentation outlined the company’s experience in dealing with a PAT submission for a human medicinal product across the world and emphasised the main points of focus.
SESSION 4: Common European Submission Platform (CESP)
This focused on the HMA project to develop a European submission platform for decentralised, mutual recognition and national procedures and other submission types and its integration within a member state. Presentations were given by Kevin Horan, Business Service Unit manager, imB, and maria Carleton, operations manager, imB, on the project delivered on behalf of the HMA, providing an overview of the business requirements, implementation plan and benefi ts of the system. The IMB outlined its experiences of using the system and the potential savings that may be achieved once fully integrated into its submission process.
Delegates were advised that a pilot project would commence in November 2012 with a number of participating agencies. The pilot will accept “live” submissions from applicants for decentralised, mutual recognition and national procedures, and MAHs are invited to join the pilot at any time. A number of agencies are implementing the system as their main submission platform.
An opportunity to network with colleagues and engage with exhibitors.