ten things ped need to know about urology.ppt · 2019-09-26 · nocturnal enuresis: randomized,...
TRANSCRIPT

Ten Things Pediatricians Need to Know About Urology
Tony Khoury MD FRCSC FAAPWalter R. Schmid Professor of Pediatric Urology
Professor, Department of UrologyUniversity of California, Irvine
Head of Pediatric UrologyChildren's Hospital of Orange County
1. Prenatal Hydronephrosis

Antenatal Hydronephrosis Detected by U/S in 1/400 pregnancies
Represents 30% of prenatal anomalies
Postnatal persistence in 50%
VUR26%
Duplex10%
PUV10%
37%
Bilateral15%
Single kidney2%
Unilateral
Antenatal HydronephrosisUltrasound - Prenatal
AP diameter – SFU grading Empty bladder 20 weeks or more
Grade 1 – slight central split
Grade 2 – central split confined to border, normal parenchyma
Grade 3 – wide split, pelvis outside renal border, caliectasis, normal parenchyma
–Grade 4 – large calyces, thin parenchyma»< half contralateral, or <4mm
SFU Consensus
No Calyx
Normal Calyx
Blunted Calyx
Bulging Calyx

Normal Fetal AP diameter
Week MM
16 4 mm
24 6 mm
28 7 mm
40 10 mm
Antenatal HydronephrosisUltrasound - Postnatal
Careful with the interpretation of the newborn US relative dehydration
Cortical echogenicity

Antenatal HydronephrosisUltrasound - Prenatal
Outcomes Grade 1
97% spontaneous resolution 20-30% incidence of VUR (with any degree of prenatal hydronephrosis)
Grade 2 80% spontaneous resolution 10% OR
Grade 3 30% OR
Grade 4 ≈90% OR
AP Diameter as an Indicator for Pyeloplasty

Key points AHN
Majority resolve, early delivery “never” Infections rare VCUG only indicated if ureter dilated or
bladder abnormal No need for Abx Insist on proper radiology interpretation
2. Incontinence
The Poor Bladder
10
CourageKindness
Generosity
IntelligenceWisdom
Creativity
11
12

Normal Bladder Function
Low pressure filling Low pressure storage Perfect continence Periodic voluntary expulsion
(at low pressure) Resist infection
Detrusor Muscle Properties
Contractile properties well suited for either urine storage or release
Smooth Muscle Connective Tissue

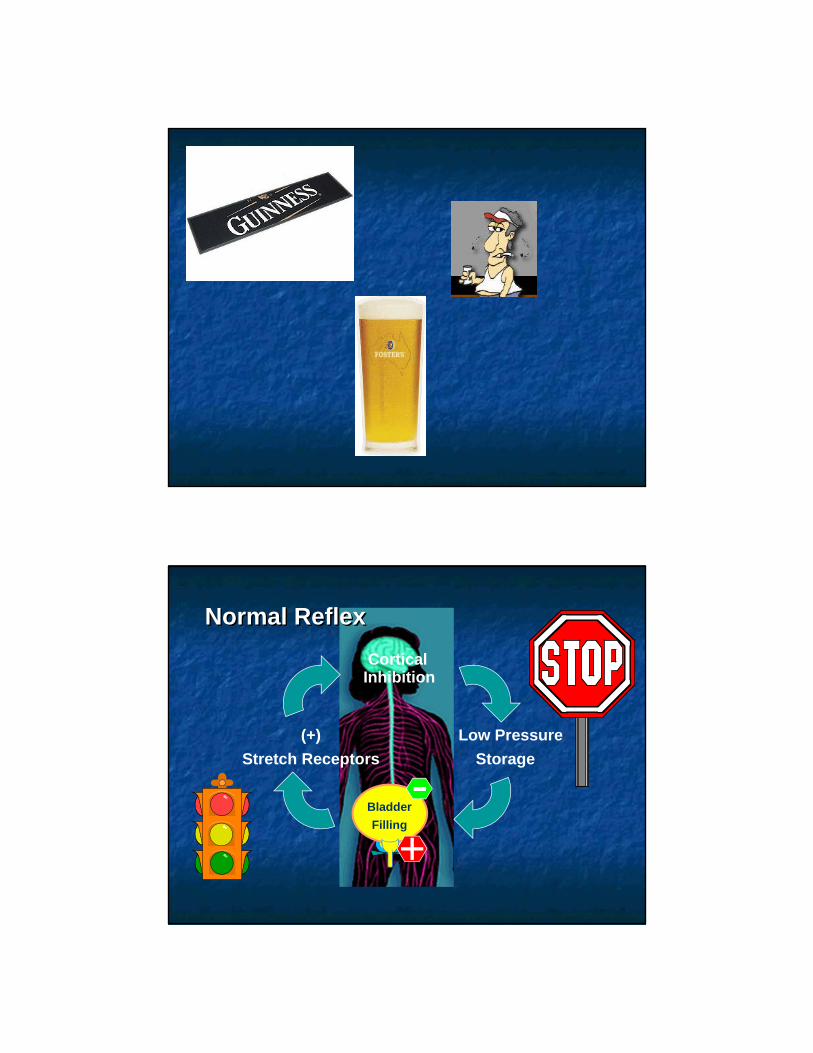
Normal ReflexNormal Reflex
Bladder
Filling
CorticalInhibition
(+)
Stretch Receptors
Low Pressure
Storage
Urethral Control Mechanism
Smooth muscle maintains tone with relatively little expenditure of energyStriated muscle for emergencies
+-
+
Sacralreflex
+
Holding Reflex
Voiding Dysfunction

Wein’s Functional Classification Failure to Store
Because of Bladder Because of Urethra Combined
Failure to Empty Because of Bladder Because of Urethra Combined
+
-
-
+
Diagnostic Studies
Bladder Diary (capacity, urgency, frequency, incontinence)
Uroflow and PVR

Simple Measures to Correct Incontinence
Timed voiding: vibrating alarm Watch Increase water intake Correct constipation
Sensory Urgency
Daytime frequency No Nocturia No incontinence
Self limiting Water Rx Constipation

3. Nocturnal Enuresis
Incidence
80% primary15% resolve / year
5 to 7 million children in the USBoys:Girls 3:1

Hereditary Factors
Norgaard JP, Djurhuus JC, Watanabe H, Stenberg A, Lettgen B. Experience and current status of research into the pathophysiology of nocturnal enuresis. Br J Urol 1997;79:825-35.
Etiology - Dandelions
Anecdotal reports and folk wisdom say children who handle dandelions can end up wetting the bed.
Dandelions are reputed to be a potent diuretic.
English folk names for the plant are "peebeds" and "pissabeds”. In
French dandelions are called pissenlit, which means "urinate
in bed"; likewise "piscialletto", an Italian folkname, and "meacamas" in Spanish.

Pathophysiology
Disturbance atthe
Brainstem Level
Disturbance atthe
Brainstem Level
Nocturnal Polyuria
Nocturnal Polyuria
High Arousal Thresholds
High Arousal Thresholds
Nocturnal DetrusorOveractivity
Nocturnal DetrusorOveractivity
The bedwetting child is regarded as a “deep sleeper”
Supported by Universal parental observation that their enuretic
children are difficult to awaken (Nevéus T, Hetta J, Cnattingius S, Tuvemo T, Läckgren G, Olsson U, Stenberg A (1999) Depth of sleep and sleep habits among enuretic and incontinent children. Acta Paediatr 88:748–752)
Studies on objective arousal thresholds (Wolfish NM, Pivik RT, Busby KA (1997) Elevated sleep arousal thresholds in enuretic boys: clinical implications. Acta Paediatr 86:381–384)
Sleep electroencephalogram (EEG) of enuretic children not different from that of dry children.

NE and Sleep Disturbances
Enuresis may be caused by heavy snoring or sleep apneas due to adenotonsillar hypertrophy.
Possible explanations The constant arousal stimuli from the obstructed
airways causes paradoxically high arousal thresholds The negative intrathoracic pressure causes polyuria
via increased secretion of the atrial natriuretic peptide
Umlauf MG, Chasens ER (2003) Sleep disordered breathing and nocturnal polyuria: nocturia and enuresis. SleepMed Rev 7:403–411
The Marvel of the Hibernating Bear
Urine production Muscle mass Bones Boredom!

Alterations in Vasopressin Secretion and Nocturnal Urine Production
About 50% less urine is normally excreted during the night than during the day.
Due to a circadian rhythm of plasma arginine vasopressin (AVP)
Etiology : ADH
Delay in achieving circadian rise inarginine vasopressin
nocturnal polyuria
overwhelms the bladder

No significant difference in nocturnal urine osmolality
between enuretic and nonenuretic children at any age
Kawauchi and Watanabe (1993)
Nocturnal Polyuria
Weak evidence for presence of true nocturnal polyuria in MSNE
Van Hoeck K, Bael A, Lax H, et al. Urine output rate and maximum volume voided in school-age children with and without nocturnal enuresis. J Pediatr 2007; 151:575–580.
Normal ReflexNormal Reflex
Bladder
Filling
CorticalInhibition
(+)
Stretch Receptors
Low Pressure
Storage
+-

Evaluation
General Child and parent attitude toward NE Confirm that it is PMNE BBD: Bladder Bowel Diary, Uroflow Frequency of NE: number per week and
per night R/O other conditions: DI, CRF, PUV, UTI
Treatment
Remember the Natural History!!

Timing of Treatment
Treatment is rarely successful before Age 7 15% of children are enueretic at age 5
The child needs to be truly motivated for treatment to succeed
Who is more interested in dryness: the parent or the child?
Treatment
Behavioral Interventions Alarms Medications
Important treatment aim is to protect and improve self-esteem.Counsel the parents, warn about psychological damage caused by pressure, shaming, or punishment for a condition the child cannot control

TreatmentBehavioral Interventions
Reducing fluid intake in the evening Reduces incontinence volume Rarely impacts frequency of wetting episodes
Lifting: ineffective Reward System Responsibility to induce motivation

Treatment - Medications
Desmopressin Response
Desmopressin Response
DryDry
Partial ResponsePartial Response
No ResponseNo Response
Desmopressin probably unsuccessful:• If maximum voided volumes <70% of the expected bladder capacity• No nocturnal polyuria (nocturnal urine production less than 130% of the
expected bladder capacity).
Desmopressin + Alarm

Desmopressin + Anticholinergic
Patients with MNE who did not respond to desmopressin alone
Reduction in the number of wet nights compared to desmopressin alone
Austin PF, Ferguson G, Yan Y, et al. Combination therapy with desmopressin and an anticholinergic medication for nonresponders to desmopressin for monosymptomatic nocturnal enuresis: randomized, double-blind, placebocontrolled trial. Pediatrics 2008; 122:1027–1032.
Desmopressin Downside
The therapeutic effect of DDAVP is temporary, and once treatment is stopped 50% to 90% of children relapse and resume their original pattern of wetting (Kahan et al, 1998).

DDAVP
Ideal for Overnight Campsand Sleepovers
Behavior Modification
should be considered the first-line approach to the management of
enuresis

Reward System
StickersRewards
Responsibility Reinforcement

Conditioning Therapy
The Wetness Alarm
Alarm Results
Complete resolution 66% 16% relapse after discontinuation Relapses respond well to retreatment Better with overtreatment
Glazener, C. M., J. H. Evans, et al. (2005). "Alarm interventions for nocturnal enuresis in children." The Cochrane database of systematic reviews(2): CD002911.
4. Catheterizable Continent Channels

Clean Intermittent Catheterization
Urethra Manual Dextrerity Balance Issues
Stoma Mitrofanoff
Mitrofanoff

Catheterizable Conduit
The appendix preferred material for a continent cathetrizable conduit.
55
56

10 Years Later
57
58
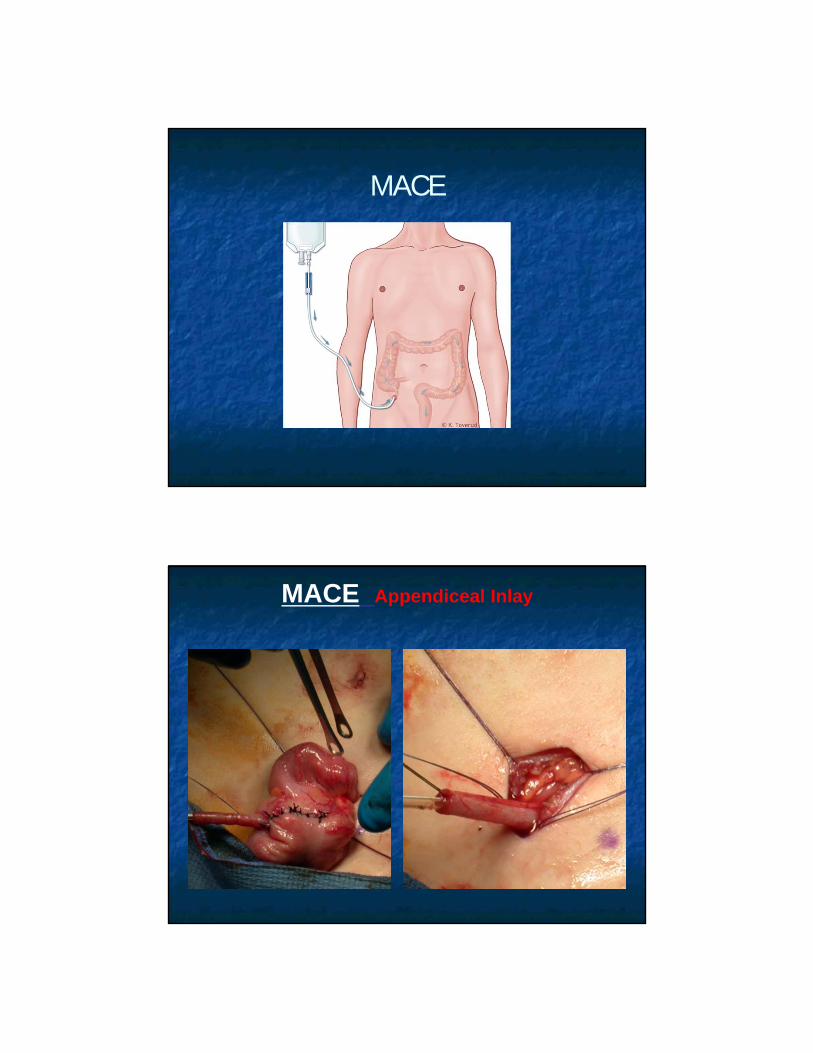
MACE
MACE Appendiceal Inlay
5. UTI
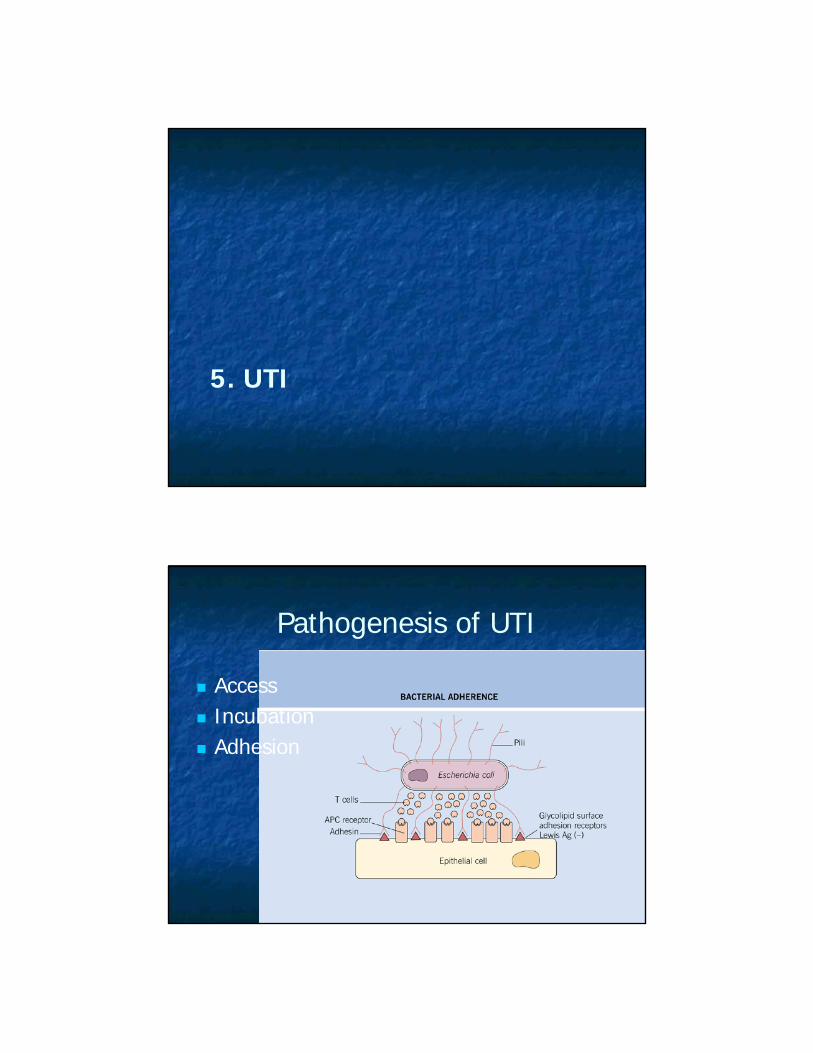
Pathogenesis of UTI
Access Incubation Adhesion

Time Amount Wet / Dry
Evaluation
Review Urine Culture and Analysis Report Elimination Diary & Drinking Habits US FR & PVR

Investigations for UTI
If no Hx of BBD: US VCUG only if US abnormal
HN HU Bladder
Management
Correction of Predisposing Factors Insufficient water intake Infrequent voiding Incomplete bladder emptying Constipation Poor Hygiene, Fecal soiling Voiding into vagina Chemical urethritis

6. VUR
Indications for Surgical Correction of VUR
1990’s
Breakthrough infections
Non resolution after 4 years of Follow-up
Noncompliance with ABP
New renal scars on therapy

AAP Guidelines 2011
Published literature does not provide evidence supporting the benefit of prophylaxis Rec UTI or renal scarring
Therefore why diagnose VUR when the imaging findings would not affect the nature of treatment?

Swedish Reflux Trial
Antibiotic prophylaxis and endoscopic treatment decreased the infection rate in: Children under 2 y with Grade III-IV VUR
Be Selective

Renal Scarring
Outcome scans (at the 2year visit or 3 to 4 months after the child had met treatment failure criteria) showed no significant differences in the incidence of renal scarring 11.9% in the prophylaxis group and 10.2% in the
placebo group (P = 0.55), Severe renal scars (4.0% and 2.6%, respectively; P =
0.37 New renal scars since baseline (8.2% and 8.4%
P=0.94)

Compliance
Parents of 467 of the children (76.9%) reported having administered the study medication at least 75% of the time,
Parents of 517 children (85.2%) reported having administered it at least 50% of the time.
Parents of 91 children in the prophylaxis group and of 76 children in the placebo group discontinued the study medication.
Antimicrobial Resistance
Stool colonization with resistant E. coli was more common in the prophylaxis group than in the placebo group, but the difference was not significant
Among 87 children with a first febrile or symptomatic recurrence with E. coli, the proportion of isolates that were resistant to TMP-SMX was 63% with prophylaxis and 19% with placebo (P<0.001)

How does this reconcile with the AAP Guidelines?
1. CAP does not reduce renal scarring or CKD2. CAP results in a modest reduction in UTIs3. The likelihood of resistant organisms
causing UTI is higher in the group on CAP4. Do the results with SMX-TMP cross over to
other antibiotics?
Bladder and Bowel Dysfunction

Outcome of Antibiotic Prophylaxis Discontinuation in Patients With Persistent Vesicoureteral Reflux Initially Presenting With Febrile Urinary Tract Infection:
Time to Event Analysis Bruno Leslie, Katherine Moore, Joao L. Pippi Salle, Antoine E. Khoury, Anthony Cook, Luis H.P.
Braga, Darius J. Bägli, Armando J. Lorenzo The Journal of Urology - September 2010 (Vol. 184, Issue 3, Pages 1093-1099
I-II
III-V
Outcome of Antibiotic Prophylaxis Discontinuation in Patients With Persistent Vesicoureteral Reflux Initially Presenting With Febrile Urinary Tract Infection:
Time to Event Analysis Bruno Leslie, Katherine Moore, Joao L. Pippi Salle, Antoine E. Khoury, Anthony Cook, Luis H.P.
Braga, Darius J. Bägli, Armando J. Lorenzo The Journal of Urology - September 2010 (Vol. 184, Issue 3, Pages 1093-1099
BBD
No BBD

The Journal of UrologyVolume 184, Issue 3 , Pages 1134-1144,
September 2010
Summary of the AUA Guideline on Management of Primary
Vesicoureteral Reflux in Children
Craig A. Peters, Steven J. Skoog, Billy S. ArantJr., Hillary L. Copp, Jack S. Elder, R. Guy Hudson, Antoine E. Khoury, Armando J.
Lorenzo, Hans G. Pohl, Ellen Shapiro, Warren T. Snodgrass, Mireya Diaz
BBD is associated with more UTIs on CAP BBD is associated with less reflux resolution
at 24 month BBD is associated with reduced success for
endoscopic therapy but not open surgery BBD is associated with increased incidence
of UTI after surgery

Predicting The Risk For Breakthrough Urinary Tract Infections In Patients With
Primary Vesicoureteral Reflux
Guy Hidas, John Billimek , Alexander Nan, Blake Watts, Maryellen Pribish, Soltani Tandis, Elias Wehbi, Irene
McAleer, Gordon McLorie, Sheldon Greenfield, Sherrie H. Kaplan, Antoine E. Khoury
University of California, Children's Hospital of Orange County, Orange, CA, USA
Prevention of Renal Injury
PrenatalOr
Post UTI
Bladder DysfunctionConstipation
Sex Race
AgeInfant
Vs.>5 y
Grade of VUR
Number of Febrile
UTI
Presence of Parenchymal
changes
VUR is a spectrum
Methods
Retrospective Data Review to Construct Risk
Calculator
Prospective Application of Risk Calculator
To evaluate accuracy
Prospective Validation of Risk Model
We tested the risk model on a prospective cohort of 56 patients with VUR followed for two years
Mean probability prediction of BTUTI using the model was 19.5%
21% (12 patients) actually experienced BTUTI
The model also showed good discrimination between positive versus negative BTUTI cases in this prospective sample (AUROC= 0.80).
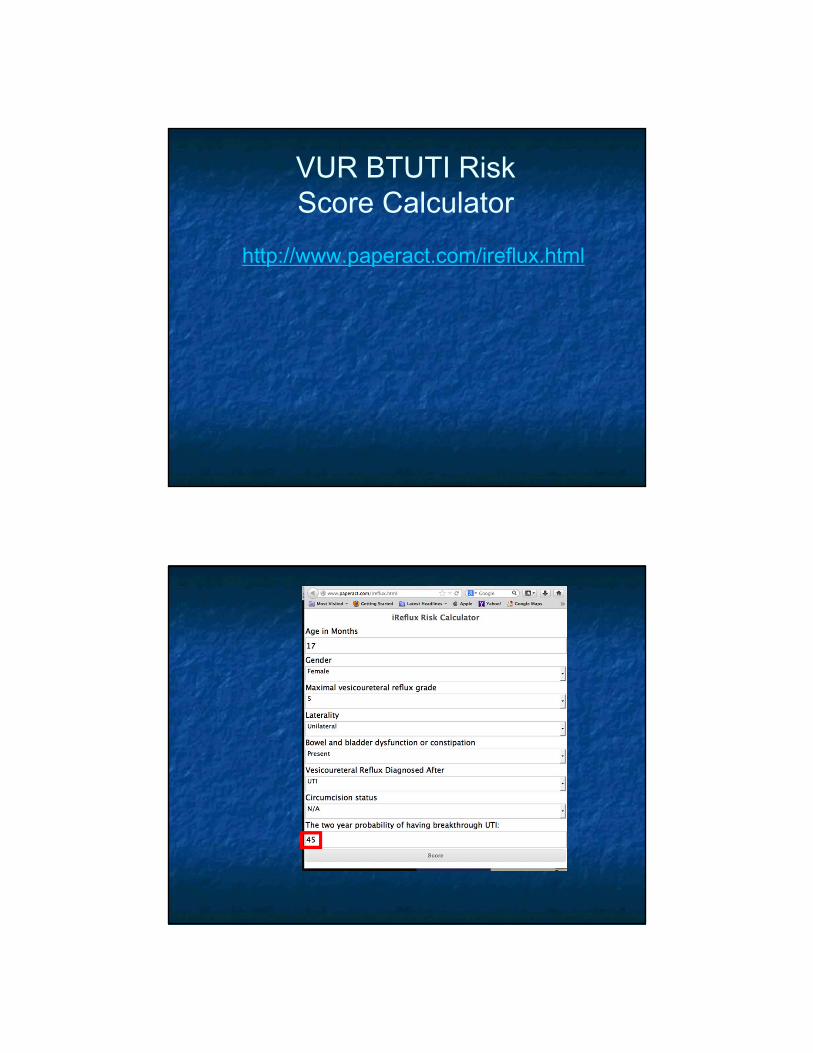
VUR BTUTI RiskScore Calculator
http://www.paperact.com/ireflux.html

Categorical risk stratification
• VUR Grade I-III andNo BBD
• Circumcised MaleLow RiskLow Risk
• VUR Grade I-III and BBD• Uncircumcised Male• VUR Grade IV-V, Female,
Presented as PNH
Intermediate Risk
Intermediate Risk
• VUR Grade IV and V• and Female • and Presented as a UTI
High Risk High Risk
% of PopBUTI Risk
67% 8%
27% 27%
6% 62%
VUR Score
Low Risk: Nothing ± Periodic RBUS
Intermediate Risk: CAP + Periodic RBUS
High Risk: early intervention
Females after puberty????

7. Hematuria
Microscopic Hematuria
Microscopic hematuria is a common finding in children.
In two large population-based studies, 3-4% of unselected school-age children between 6 to 15 years of age had a positive dipstick for blood in a single urine sample
Drops to 1% or less for two or more positive samples. Among the 1 percent of children with two or more positive urines for hematuria, only one-third have persistent hematuria (positive repeat test after six months)

Routine office screening with urinalysis for urinary abnormalities is no longer recommended.
The actual time of onset for microscopic hematuria is often unknown
Microscopic Hematuria
Confirmation of microscopic hematuria after a positive dipstick examination requires a microscopic examination of the urine for the presence of red blood cells and casts.

Glomerular VS. NonglomerularBleeding
Extraglomerular Glomerular
Color (if macroscopic) Red or pinkRed, smoky brown, or "Coca‐Cola"
Clots May be present Absent
Proteinuria Usually absent May be present
RBC morphology Normal Dysmorphic
RBC casts Absent May be present
Thin Basement Membrane Disease
Thin basement membrane disease (TBM), also called benign familial hematuria, is an autosomal dominant condition

Hypercalciuria
Defined in children as a urine calcium/creatinineratio >0.2 (mg/mg) in children older than six years of age,
In studies performed in the United States, the prevalence has ranged from as low as 11 percent in the Northeast to as high as 35 percent in the South.
Association between hypercalciuria and hematuria may be more common in areas where there is a higher prevalence of nephrolithiasis.
Transient hematuria
Urinary tract infection (dysuria and pyuria) Trauma Fever Exercise-induced hematuria
Evaluation
Hx: UTI, Stone, Water intake, Trauma, Menstruation
Remember to examine urethral meatus
Recommendation
Observation of children with asymptomatic microscopic hematuria with normal physical examination.
Extensive diagnostic evaluation reserved only in children with: Proteinuria Hypertension Gross hematuria

Gross Hematuria
0
5
10
15
20
25
30
35
40
0
5
10
15
20
25
30
35
40
Nephrology Urology
Gross Hematuria
Terminal Hematuria = Urethral source Exercise induced AVM Ca:Cr ratio >0.2 (mg/mg) Diet: Water + citrate + Less NaCl Consider an US if persistent Cystoscopy rarely indicated

8. Modern Management of the Undescended Testicle
EpidemiologyAt birth:
3-4% of full-term male infants
25-45% of pre-term male infants
At 6 and 12 months:
1% of full-term males
10% of pre-term male infants
10-25% are bilateral

Testicular AscentWell documented in the literatureVarious theories on the etiology:
Patent processus (found in 25-47% at surgery) Spasticity of cremasteric reflex Relative cranial migration due to linear growth
Similar abnormalities of germ cell development have been observed
Barthold and Gonzalez; J Urology 2003
Retractile testicle
Can be manipulated into the scrotum and stays
there for an undefined period of time
Most commonly seen at 5 yrs of age
Hyperactive cremasteric reflex
Should be monitored annually until puberty
7-33% “progress” to cryptorchidism

Physical examination
Warm, relaxed environment
Sweep fingers from internal ring to external ring
Facilitated by use of lubricant
Try supine first, then in a seated, cross-legged position
What is the Role of Imaging?
None

Ultrasound vs. Physical ExamTasian and Copp; Pediatrics 2011 Systematic review and meta-analysis 12 studies (591 testes) US has sensitivity of 45% and specificity of 78%
Conclusion – US does not reliably localize nonpalpable testes and does not rule out an intraabdominal testis.
No change in surgical management based on ultrasound findings!
Bilateral Non-palpable Testes Karyotype and endocrine evaluation
particularly when associated with hypospadias
Surgical exploration still required!
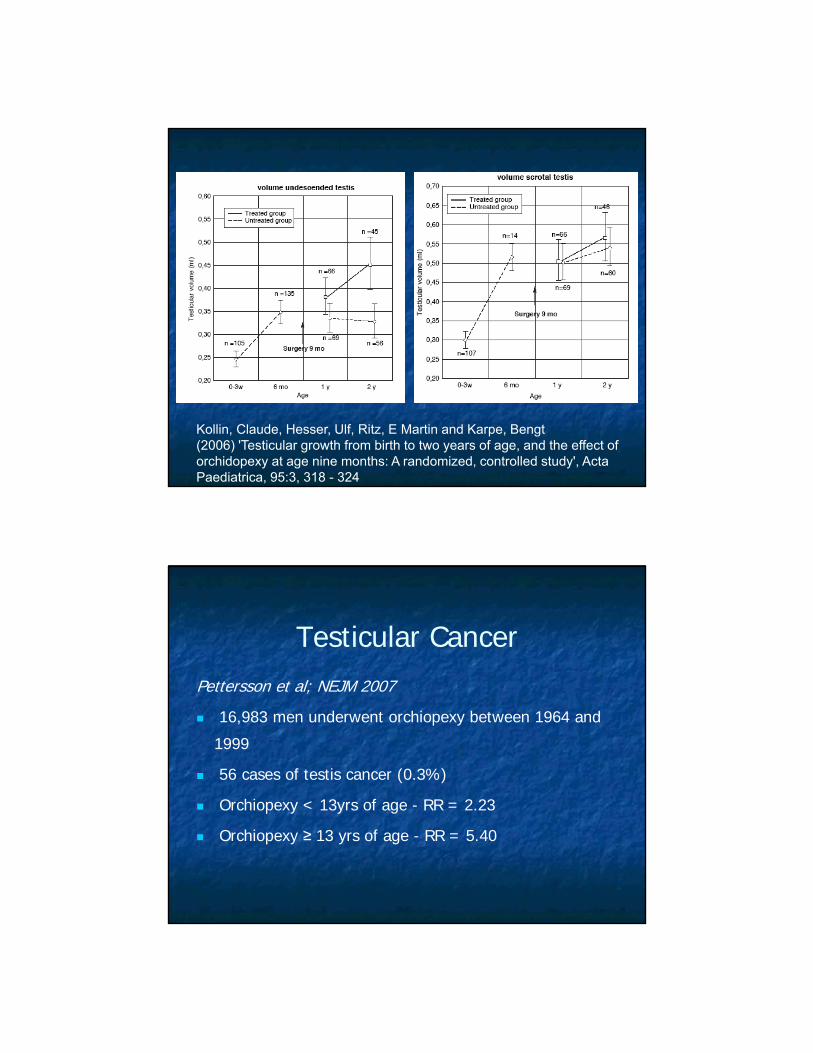
Kollin, Claude, Hesser, Ulf, Ritz, E Martin and Karpe, Bengt(2006) 'Testicular growth from birth to two years of age, and the effect of orchidopexy at age nine months: A randomized, controlled study', Acta Paediatrica, 95:3, 318 - 324
Testicular CancerPettersson et al; NEJM 2007
16,983 men underwent orchiopexy between 1964 and
1999
56 cases of testis cancer (0.3%)
Orchiopexy < 13yrs of age - RR = 2.23
Orchiopexy ≥ 13 yrs of age - RR = 5.40

Testicular Cancer Educate parents
Most common cancer
among men age 15-35yrs
Recommend testicular self-
exams starting in
adolescence
Take home messages Imaging is unnecessary
Normal paternity rates in unilateral cryptorchidism; decreased rates in bilateral
Ideal age for surgery is 6-12 months
Testicular self-exams starting in adolescence

9. DSD
Gender Assignment
4 components of psychosexual development gender identity gender role sexual identity sexual orientation.
Factors Influencing Psychosexual Development
Exposure to androgens Sex chromosomes Compliance Brain structure Social circumstance Family dynamics.
Gender Assignment
3 important factors Expected gender identity Sexual function Fertility potential

Other factors that may be considered include genital appearance gonadal malignant potential need for gonadectomy surgical options prenatal androgen exposure views of the family cultural practices.
The external masculinization score (EMS) has been used to aid this process. (Ahmed SF, Khwaja O and Hughes IA: The role of a clinical score in the assessment of ambiguous genitalia. BJU Int. 85: 120-4,) 2000.
Influence of Sex Hormones on the Developing Brain
Prenatal exposure contributes to gender identity
Current recommendation: genetic males be reared as male micropenis penile agenesis 46,XY males with PAIS 5-alpha reductase deficiency.

The majority of patients with 46,XX CAH and 46,XY CAIS patients identify as female
despite exposure to elevated androgen levels during fetal life.
It is recommended these patients are gender assigned as female
CAH: Prenatal DEX Treatment
Family History Start at 6-7 week of pregnancy Females only (7/8 fetuses treated unnecessarily)

Cell-free Fetal DNA Testing
Cell-free fetal DNA testing, a noninvasive prenatal screening of fetal DNA in maternal circulation, can provide early sex identification and genotyping without amniocentesis or chorionic villus sampling, and thus decreases unnecessary prenatal CAH dexamethasone therapy.
Feminizing Genitoplasty
vaginoplasty clitoroplasty Labioplasty Skin

Buccal mucosa graft
Hypospadias Reconstruction

10. Prepuce
Function of the prepuce
Protection of the glans

Infant “Smegma”
Penile pearls
Penile abscess
Penile cysts
Penile mass
Penile calcifications•Desquamated cells•Helps separation
Infants
XQ-tips
Irrigation
Antiseptics

Phimosis
Physiologic phimosisBy 3 years of age, 90% of foreskins are retractable,
less than 1% of males have phimosis by 17 years of age.
Early forceful retraction is not recommended
"Iatrogenic" Phimosis

Management of Physiologic Phimosis
Steroid + Gentle retraction 95% success Gentle retraction alone 45% success
(p<0.001)
Indications for Circumcision
MedicalSocial
Religious
Hygiene
Cosmetic
• Penile and cervical cancer • Sexually transmitted diseases• Phimosis and lessening of the
risk of balanitis.