targeted therapy: novel caapproaches to cancer treatmentasia4safehandling.org/pdf/narin_targeted...
TRANSCRIPT

1
Targeted Therapy:Novel Approaches to Cancer Treatment
Narin Voravud, M.D.Medical Oncology Unit, Department of Medicine,
Faculty of Medicine, Thai Red Cross Society and King Chulalongkorn Memorial Hospital, Chulalongkorn University
Bangkok, Thailand
The 1st Asia Pacific Oncology Pharmacy Congress(APOPC)
August 5, 2006 Bangkok, Thailand
Targeted Therapy in Oncology
!Cancer is the most common cause of death! Ineffective and incurable treatment in many cancers!Conventional antineoplastic agents lack specificity
causing normal tissue toxicities!Specific, effective, and safer agents
are needed!Progress in molecular oncology defines
specific anticancer targets!Targeted therapy is clinically available
Targeting the Tumor and Its Microenvironment
Endothelial CellCancer Cell
1. Growth factor signaling2. Microtubule dynamics3. Histone acetylation/deacetylation4. DNA replication, transcription, repair5. Metastasis
1
1
43
2
1
1
4
2
5
Tumor Cell Growth / Replication Angiogenesis
Targets of Cancer Therapy
Cell Growth Motility Survival Proliferation Angiogenesis
PP
PP
PDK1,2Growth Factor
Signaling
Gene Transcription DNA Replication and Repair
1
6 3
5
8
9
1011
2Plasma Membrane
Nuclear Membrane
127
4
7
7 1. Growth factors2. Growth factor
receptors3. Adaptor proteins4. Docking
proteins/binding proteins
5. Guanine nucleotide exchange factors
6. Phosphatases and phospholipases
7. Signaling kinases8. Ribosomes9. Transcription
factors10. Histones11. DNA12. Microtubules
Microtubule Dynamics
RNA Translation
Development of Targeted Therapy in Oncology
Agents
RituximabImatinibTrastuzumabGefitinibBevacizumabThalidomideZevalinErlotinibCetuximabSorafenibSunitinib
FDA ApprovalThailand USA
2001 19972001 20012001 19982004 20032005 20042005 19982005 20022005 1998
- 2004- 2005- 2006
Disease
Non-Hodgkin’s lymphomaCML, GISTAdvanced brest cancerAdvanced NSCLCAdvanced colorectal cancerMultiple myelomaNon-Hodgkin’s lymphomaAdvanced NSCLCColorectal cancerRenal cell carcinomaRenal cell carcinoma, Refractory GIST
Why Epidermal Growth Factor and Receptor are Important Targets ?
!Most cancers are epithelial in origin, so called carcinoma.
!Hallmark of cancer is abnormal/uncontrolled growth.!Cancer growth is controlled by growth factors/receptors.!Major growth factor is epidermal growth factor (EGF).!First discovery by John Mendelsohn

2
Growth Factors and Tumor Growth and Metastasis
Tumor effects– metastasis– proliferation– loss of apoptosis– infinite replication– angiogenesis– invasion
Mutations in– HER family – VEGF– MMPs– ras– p53– COX-2
Primary tumor
Hanahan D, Weinberg RA. Cell. 2000;100:57-70.
Metastasis
Autocrinefactors
Receptors
Paracrinefactors
Normalcells
Tumorcell
Hoststromal
epithelium
Biologic Control of Tumor Growth
Incrine
Acrine
Tumors with HER1/EGFR Dysregulation
Salomon DS, Brandt R, Ciardiello F, et al. Crit Rev Oncol Hematol. 1995;19:183-232.Woodburn JR. Pharmacol Ther. 1999;82:241-250.
BreastEsophagus
GastricPancreaticOvarian
CervicalProstate
Bladder
Colorectal
RenalLung
Glioma
Head and neck
The HER Family of Receptors
HER1/EGFRerbB1
HER2erbB2neu
EGFTGF-α
AmphiregulinBetacellulin
HB-EGFEpiregulin Heregulins
NRG2NRG3
HeregulinsBetacellulin
Cysteine-rich
domains
Tyrosine-kinase
domains
HER3erbB3 HER4
erbB4
Ligands:
Salomon D, Brandt R, Ciardiello F, et al. Crit Rev Oncol Hematol. 1995;19:183-232.Woodburn J. Pharmacol Ther. 1999;82:241-250.
Proliferation, invasion, metastasis, angiogenesis, and inhibition of apoptosis
Effects of HER1/EGFR Activation
Src PLCγ GAP Grb2 Shc Nck Vav Grb7 Crk
PKC Ras
JNK AblPI3K Akt
Extracellular
Intracellular Transactivation
MAPK
P P
Woodburn J. Pharmacol Ther. 1999;82:241-250; Lynch TJ, Bell DW, Sordella R, et al. New Engl J Med. 2004;350; Knowlden JM, Hutcheson IR, Jones HE, et al. Endocrinology 2003;144:1032-1044; Chakravarti A, Chakladar A, Delaney MA, et al. Cancer Res. 2002;62:4307-4315.

3
HER1/EGFR and Proliferation
Harari D, Yarden Y. Oncogene. 2000;19:6102-6114.Quon H, Liu FF, Cummings BJ. Head Neck. 2001;23:147-159.
!HER1/EGFR signaling increases cyclin D level
HER1/EGFRdimer
Cyclin DNucleus
Check-point
Cyclin DChromosomesegregation M S
DNAreplication
Promotes G1→S
G1
G2
Geneactivation
G0
l Cyclin D is a critical G1 checkpoint protein
MitogensGrowth factors
Cell–cell contactdifferentiationP P
HER1/EGFR Dysregulation in Tumors
Ligand overproduction(autocrine loop)
Overexpression
Defectiveinternalization or downregulation
P = phosphate
EGFRvII/III
EGFRvI
Mutationsconferring
constitutiveactivation
P P P P P PP P P P P P
De Miguel P, Royuela, Bethencourt R, et al. Cytokine. 1999;11:722-727; Normanno N, Kim N, WenD, et al. Breast Cancer Res Treat. 1995;35:293-297; Lal A, Glazer CA, Martinson HM, et al. Cancer Res. 2002;62:3335-3339; Lynch TJ, Bell DW, Sordella R, et al. New Engl J Med. 2004;350; Paez JG, Janne PA, Lee JC, et al. Science, 29 April 2004 (10.1126/science.1099314); Yang H, Jiang D, Li W, et al. Oncogene 2000;19:1901-1914.
Common Approaches toTargeting HER1/EGFR
Slamon DJ, Leyland-Jones B, Shak S, et al. N Engl J Med. 2001;344:783-792; Mendelsohn J, Baselga J. Oncogene. 2000;19:6550-6565; Noonberg SB, Benz CC. Drugs. 2000;59:753-767; Raymond E, Faivre S, ArmannJP. Drugs. 2000;60(Suppl 1):15-23; Arteaga C. J Clin Oncol. 2001;19:32s-40s; Pedersen MW, Meltom M, Damstrup L, et al. Ann Oncol. 2001;12:745-760.
Anti-HER1/EGFR-blocking antibodies
Anti-ligand-blocking
antibodies
TKinhibitors
Ligand–toxin
conjugatesAntibody–
toxinconjugates
PP P
P
TK inhibitor
↓ Proliferation
↓ Invasion
↓ Metastasis↓ Angiogenesis
↑ Apoptosis
↓ Adhesion
↑ Sensitivity toradiotherapy
HER1/EGFR Inhibitors: Mode of Antitumor Activity
Etessami A, Bourhis J. Drugs Fut. 2000;25:895-899.Moyer J, Barbacci EG, Iwata KK, et al. Cancer Res. 1997;57:4838-4848.Harari PM, Huang SM. Semin Radiat Oncol. 2002;12(Suppl 2):21-26.
Monoclonal antibody
Therapeutic Needs in NSCLC
! Improved survival
! Improved disease-related symptoms/ quality of life
!Better tolerated regimens
!Effective agents for patients not suitable for chemotherapy
!Longer time to disease progression
Rationale for HER1/EGFR as a target for anticancer drug development
! HER1/EGFR is frequently dysregulated in carcinomas
! HER1/EGFR activation initiates a signal transduction cascade that promotes tumour-cell proliferation and survival
! Overexpression/dysregulation of HER1/EGFR is associated with poor prognosis
! Overexpression of HER1/EGFR can transform cells in a ligand-dependent manner
! HER1/EGFR blockade inhibits tumourigenicity
Arteaga C. Semin Oncol 2003;30(Suppl. 7):3–14

4
Treatment Options for Advanced NSCLCTreatment Options for Advanced NSCLC
• cisplatin + paclitaxel• cisplatin + gemcitabine• cisplatin + docetaxel• carboplatin + paclitaxel• cisplatin + vinorelbine
1st line
Standard platinum based regimens
2nd line
3+ line ErlotinibGefitinib
Docetaxel
Pemetrexate (Alimta)
Erlotinib
Erlotinib (TarcevaTM)
! Erlotinib is the first and only HER1/EGFR TKI proven to significantly prolong survival in second and third line NSCLC patients
! Erlotinib is for the treatment of patients with locally advanced or metastatic Non-Small Cell Lung Cancer (NSCLC) after failure of at least one prior chemotherapy regimen
! Erlotinib is not chemotherapy
Erlotinib Structure
O
O
H3C
H3CO
O
NH
N
N
IC50 = 2nM1 Erlotinib binding
Basic Pharmacokinetics of Erlotinib
! Bioavailability of 150mg tablet: 60%! Tmax: 4 hours! Steady-state: 7-8 days! Half-life: 36.2 hours! Plasma protein binding: 92% to 95% ! Metabolization: liver CYP3A4
– Ketoconazole– Enzyme-inducing anti-epileptic drugs
! Excretion: 83% feces
Erlotinib: Simple Once-Daily Dosing! Recommended dose: 150 mg O.D.! 2 dosages of Oral forms (film-coated tablet), 100 and 150 mg! Take 1 tablet one hour before or two hours after meal! Dose modifications
- reduce to 100 mg in case of intolerable skin reactions or diarrhea
! Dose interruption- Erlotinib should be discontinued if ILD is diagnosed
Safety Profiles of Erlotinib
!Rash and diarrhea; mild and moderate grade
! ILD occurred in 0.8% of patients equal to placebo
!Asymptomatic increases in liver transaminases
! Infrequent cases of conjunctivitis, keratitis and
corneal ulceration
Drug Interactions with Erlotinib
!Co-treatment with CYP3A4 inhibitors increases
Erlotinib exposure such as
– ketoconazole, itraconazole, clarithromycin,
indinavir, nelfinavir, nefazodone
!Pre-treatment with CYP3A4 inducers decreases
Erlotinib exposure such as
– rifampicin, phenytoin, carbamazepine

5
Phase III Randomized Study of Erlotinib versus Placebo in Advanced NSCLC Failure to Chemotherapy
RANDOM I Z E
Erlotinib* 150 mg daily
Placebo “150 mg” daily
*2:1 Randomization
Stratified by:CentrePS, 0/1 vs 2/3Response to prior Rx(CR/PR:SD:PD)
Prior regimens, (1 vs 2)
Prior platinum, (Yes vs no)
Primary Endpoint – SurvivalSecondary Endpoint – PFS, Response, Safety, QoL
Phase III Study of Erlotinib vs Placebo in Advanced NSCLC Failure to Chemotherapy
Response Rate (N=638)
N/A15%57%27%N/AN/A
Placebo(N=211)
7.9 mo (95% CI 5.7-10.6)
Response duration18%Inevaluable / Not assessed38%Progression35%Stable disease8%Partial response1%Complete response
Erlotinib(N=427)
Patient characteristics predictive of response to Erlotinib (Study BR.21)
13.0Unknown (23)24.73.87.5
18.94.1
13.96.1
14.4
Erlotinibpatients (%)
(n=427)
No (93)Yes (311)Other (374)Asian (53)Other (218)Adenocarcinoma (209)Male (281)Female (146)
p value*
<0.001Ever smoked**
0.02Ethnicity
<0.001Histology
0.006Gender
*Significance between subgroups**Data collected retrospectivelyIn multiple logistic-regression analyses, only never having smoked (p<0.001) and adenocarcinoma histology (p=0.01) were associated with response
Shepherd F, et al. N Engl J Med 2005;353:123–32
Detection of EGFR Gene Amplification by Fluorescence in situ Hybridization (FISH Scoring)
Disomy
High polysomy
Trisomy
Gene amplificationCappuzzo F, et al. J Natl Cancer InstI 2005;97:643–55
Known HER1/EGFR activating mutations underlyingNSCLC sensitivity to Erlotinib or Gefitinib
Pao W, et al. Proc Natl Acad Sci USA 2004;101:13306–11
Sensitive to GefitinibSensitive to ErlotinibNever treated with TKI
Phase III Study of Erlotinib vs Placebo in Advanced NSCLC Failure to Chemotherapy (Study BR.21)
Overall survival & Progression Free Survival
*HR and p-value adjusted for stratification factors at randomisation + HER1/EGFR status
42.5% improvement in median survival
Surv
ival
dis
trib
utio
n fu
nctio
n
Survival time (months)
ErlotinibTM
Placebo
HR* = 0.73, p<0.001
ErlotinibTM (n=488)
Placebo (n=243)
Median survival (months) 6.7 4.7
1-year survival (%) 31 21
1.00
0.75
0.50
0.25
00 5 10 15 20 25 30
* *Adjusted for stratification factors (except centre) and EGFR status
Perc
enta
ge
0
20
40
60
80
100
0.0488
5.0153
10.052
15.08
___ Erlotinib, _____ Placebo
2.2 mos 1.8 mos*HR 0.61, p <0.0001
Months
Overall Survival Progression Free Survival
6
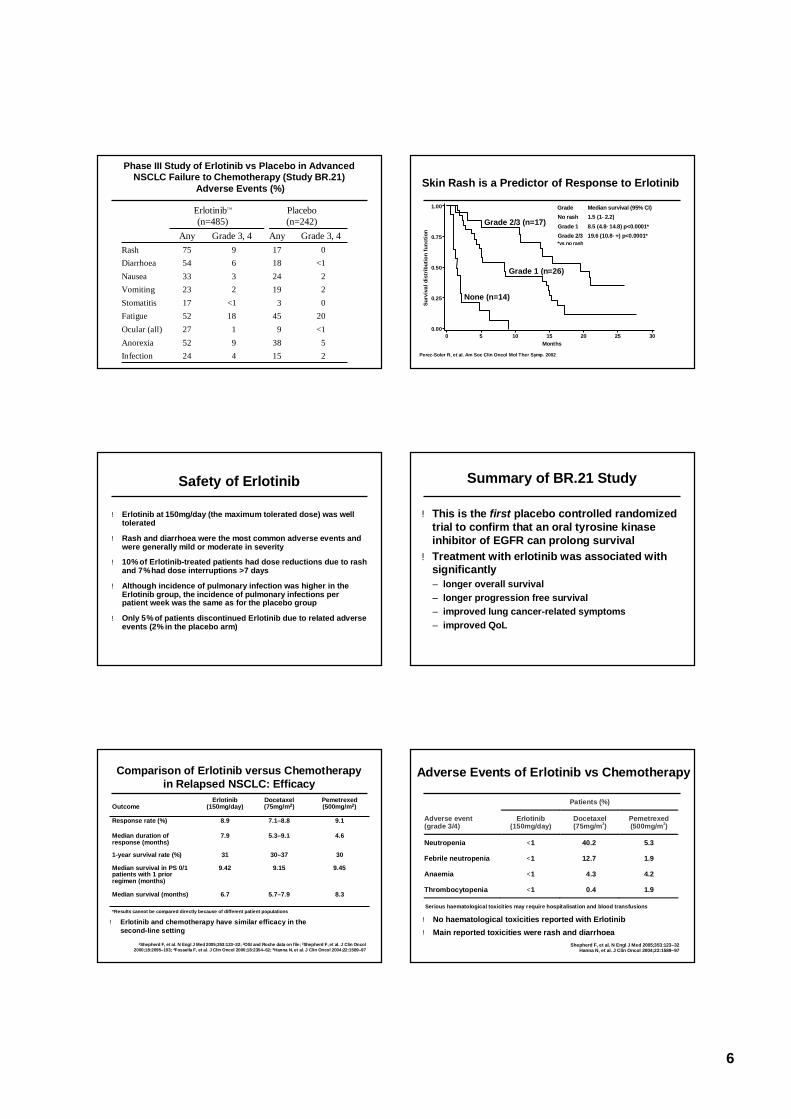
Phase III Study of Erlotinib vs Placebo in Advanced NSCLC Failure to Chemotherapy (Study BR.21)
Adverse Events (%)
538952Anorexia4
118<1
2369
Grade 3, 4
24
27521723335475
Any
ErlotinibTM
(n=485)
03Stomatitis2045Fatigue<19Ocular (all)
2
22
<10
Grade 3, 4
Placebo(n=242)
15Infection
19Vomiting24Nausea18Diarrhoea17Rash
Any
Skin Rash is a Predictor of Response to Erlotinib
Surv
ival
dis
trib
utio
n fu
nctio
n
0.00
0.25
0.50
0.75
1.00
Months0 5 10 15 20 25 30
Grade 2/3 (n=17)
Grade 1 (n=26)
None (n=14)
Grade Median survival (95% CI) No rash 1.5 (1−2.2) Grade 1 8.5 (4.8−14.8) p<0.0001* Grade 2/3 19.6 (10.8−+) p<0.0001* *vs no rash
Perez-Soler R, et al. Am Soc Clin Oncol Mol Ther Symp. 2002
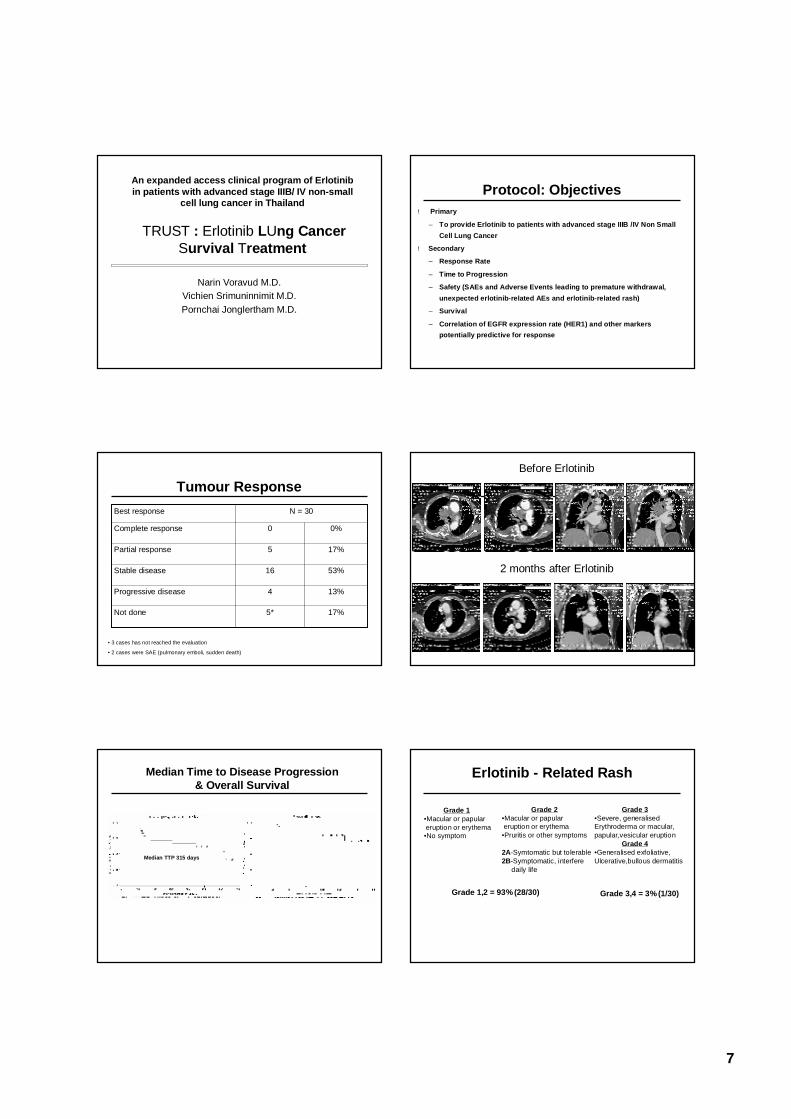
Safety of Erlotinib
! Erlotinib at 150mg/day (the maximum tolerated dose) was well tolerated
! Rash and diarrhoea were the most common adverse events and were generally mild or moderate in severity
! 10% of Erlotinib-treated patients had dose reductions due to rash and 7% had dose interruptions >7 days
! Although incidence of pulmonary infection was higher in the Erlotinib group, the incidence of pulmonary infections per patient week was the same as for the placebo group
! Only 5% of patients discontinued Erlotinib due to related adverse events (2% in the placebo arm)
Summary of BR.21 Study
!This is the first placebo controlled randomized trial to confirm that an oral tyrosine kinase inhibitor of EGFR can prolong survival
!Treatment with erlotinib was associated with significantly– longer overall survival– longer progression free survival– improved lung cancer-related symptoms– improved QoL
Comparison of Erlotinib versus Chemotherapy in Relapsed NSCLC: Efficacy
8.35.7–7.96.7Median survival (months)
9.459.159.42Median survival in PS 0/1 patients with 1 prior regimen (months)
3030–37311-year survival rate (%)
4.65.3–9.17.9Median duration of response (months)
9.17.1–8.88.9Response rate (%)
Pemetrexed(500mg/m2)
Docetaxel (75mg/m2)
Erlotinib (150mg/day)Outcome
1Shepherd F, et al. N Engl J Med 2005;353:123–32; 2OSI and Roche data on file; 3Shepherd F, et al. J Clin Oncol 2000;18:2095–103; 4Fossella F, et al. J Clin Oncol 2000;18:2354–62; 5Hanna N, et al. J Clin Oncol 2004;22:1589–97
*Results cannot be compared directly because of different patient populations
! Erlotinib and chemotherapy have similar efficacy in the second-line setting
Adverse Events of Erlotinib vs Chemotherapy
Shepherd F, et al. N Engl J Med 2005;353:123–32Hanna N, et al. J Clin Oncol 2004;22:1589–97
Serious haematological toxicities may require hospitalisation and blood transfusions
Patients (%)
Adverse event (grade 3/4)
Erlotinib (150mg/day)
Docetaxel (75mg/m2)
Pemetrexed (500mg/m2)
Neutropenia <1 40.2 5.3
Febrile neutropenia <1 12.7 1.9
Anaemia <1 4.3 4.2
Thrombocytopenia <1 0.4 1.9
! No haematological toxicities reported with Erlotinib! Main reported toxicities were rash and diarrhoea
7
An expanded access clinical program of Erlotinib in patients with advanced stage IIIB/ IV non-small
cell lung cancer in Thailand
TRUST : Erlotinib LUng Cancer Survival Treatment
Narin Voravud M.D. Vichien Srimuninnimit M.D. Pornchai Jonglertham M.D.
Protocol: Objectives! Primary
– To provide Erlotinib to patients with advanced stage IIIB /IV Non Small Cell Lung Cancer
! Secondary
– Response Rate
– Time to Progression
– Safety (SAEs and Adverse Events leading to premature withdrawal, unexpected erlotinib-related AEs and erlotinib-related rash)
– Survival
– Correlation of EGFR expression rate (HER1) and other markers potentially predictive for response
Tumour Response
13%4Progressive disease
17%5*Not done
53%16Stable disease
17%5Partial response
0%0Complete response
N = 30Best response
• 3 cases has not reached the evaluation
• 2 cases were SAE (pulmonary emboli, sudden death)
Before Erlotinib
2 months after Erlotinib
Median Time to Disease Progression & Overall Survival
Median TTP 315 days
Erlotinib - Related Rash
Grade 1•Macular or papulareruption or erythema•No symptom
Grade 2•Macular or papulareruption or erythema•Pruritis or other symptoms
2A-Symtomatic but tolerable2B-Symptomatic, interfere
daily life
Grade 3•Severe, generalisedErythroderma or macular,papular,vesicular eruption
Grade 4•Generalised exfoliative, Ulcerative,bullous dermatitis
Grade 1,2 = 93% (28/30) Grade 3,4 = 3% (1/30)

8
Management of Erlotinib-Related Rash
Primary rashTreatment! Topical corticosteroids! Analgesia
Secondary infected rashPrevention! Intranasal mupirocin (apply O.D.)
Treatment! Topical antibiotics (clindamycin)! Oral antibiotics (minocycline)! Topical mupirocin for S.aureus
Recommendations•Emollient cream•Sunscreen•Evaluate 1-2 wks•Prohibit topical retinoids and benzoyl peroxide•Unresponsive -> Dose reduction or interruption
Management of Erlotinib-Related Diarrhoea
! 4 mg Loperamide at onset of symptom! 2 mg Loperamide every 2-4 hrs
Unresponsive to loperamide!Dose reduction or interruption
Phase III studies of Gefitinib (ISEL): Survival
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15Month: 0 2 4 6 8 10 12 14At risk: 1692 1348 876 484 252 103 31
Patie
nts
surv
ivin
g (%
)
1 yr survival
Median (mo)
HR = 0.89 (0.78, 1.03), P = .11N = 1692, deaths = 969Cox analysis, P = .042
22%27%
5.15.6PlaceboGefitinib1.0
0.90.80.70.60.50.40.30.20.10.0
—— Gefitinib------ Placebo
*HR and p-value adjusted for stratification factors at randomisation + HER1/EGFR status
Study BR.21 Overall survival of Erlotinib VS Placebo
42.5% improvement in median survival
Surv
ival
dis
trib
utio
n fu
nctio
n
Survival time (months)
ErlotinibTM
Placebo
HR* = 0.73, p<0.001
TarcevaTM (n=488)
Placebo (n=243)
Median survival (months) 6.7 4.7
1-year survival (%) 31 21
1.00
0.75
0.50
0.25
00 5 10 15 20 25 30
Phase III studies of Erlotinib and Gefitinib: Results
Subset analysis
Overall survival
No survival benefit in adenocarcinoma (HR=0.84,
p=0.089)Suggestion of survival benefit in never-smokers and patients
of Asian origin
Evidence of survival benefit in most subgroups tested,including adenocarcinoma
(HR=0.7, p=0.008)
HR=0.89 (p=0.087)Gefitinib: 5.6 monthsPlacebo: 5.1 months
HR=0.73 (p<0.001)Erlotinib: 6.7 monthsPlacebo: 4.7 months
Gefitinib(n=1692)
Erlotinib(n=731)
1Shepherd FA, et al. N Engl J Med 2005;353:123–322Thatcher N, et al. Lancet 2005;366:1527–37

9
Targeted Therapy in Lung CancerThailand! Erlotinib has approved in 2nd and 3rd line NSCLC treatment.! Gefitinib has approved only in 3rd line NSCLC treatment.
USA! Erlotinib has approved in 2nd and 3rd line NSCLC treatment.! Gefitinib is no longer for new patients.
EMEA! Erlotinib has approved in 2nd and 3rd line NSCLC treatment.! Gefitinib has not approved.
Chromatin Remodeling: Histone Modifications
Targeting Histone Modifying Enzymesin Cancer Treatment
HAT / HDAC and Gene Expression
Growth Factors and the mTOR Pathway
Protein Production
Akt/PKB
4E-BP1
PI3-K
PTEN
S6
S6K1
elF-4E
Growth FactorsIGF-1, EGF, TGFα, VEGF,
etc
Cell Growthand Proliferation
Angiogenesis
mTOR
Oxygen, energy, and nutrients
Ras/RafAbl
ER
!mTOR
– Intracellular protein
– Central controller ofcell growth andproliferation
!mTOR signaling is often deregulated in cancer
!Downstream inhibition of mTOR has potential for
– Antiproliferative effects on tumor cells
– Angiogenesis inhibition
– Enhancement of the effects of chemotherapy
TSC2 TSC1
Ras/Rafpathway kinases
Human Epidermal Growth Factor Receptor-2 (HER-2) Positive Breast Cancer
! 20% of Breast Cancer!Aggressive disease with short survival!Resistance to several chemotherapy!Response to anti HER-2 antibody (Trastuzumab)
Median survival
HER2 positive 3 years
HER2 negative 6–7 years
Slamon DJ et al. Science 1987;235:177–82
!Targets HER2 protein!High affinity (Kd = 0.1 nM) and specificity!95% human, 5% murine
– Decreases potential for immunogenicity
– Increases potential for recruiting immune effectormechanisms
HER2 epitopes recognized by hypervariable murine
antibody fragment
Human IgG-1
Trastuzumab (Herceptin®):Humanized Anti-HER2 Antibody
10
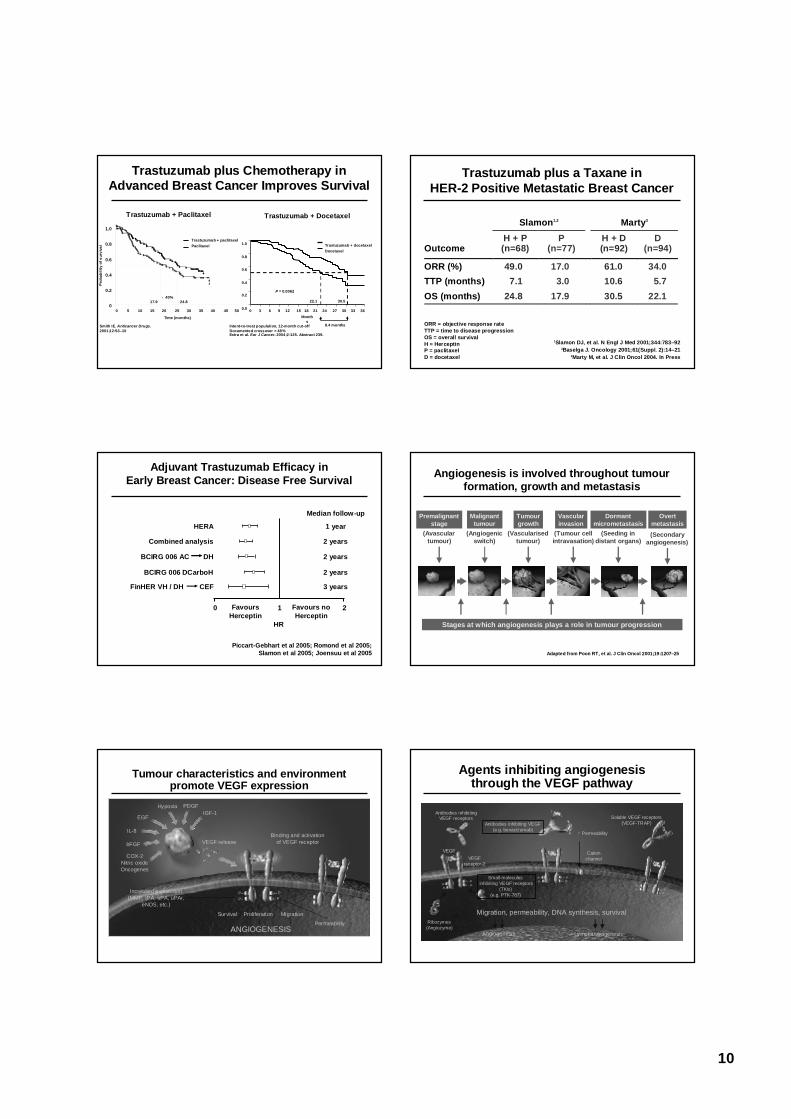
Trastuzumab plus Chemotherapy in Advanced Breast Cancer Improves Survival
Smith IE. Anticancer Drugs.2001;12:S3–10
1.0
0.8
0.6
0.4
0.2
0
Time (months)
0 5 10 15 20 25 30 35 40 45 50
17.9 24.8
Prob
abili
ty o
f sur
viva
l
↑ 40%
Trastuzumab + paclitaxelPaclitaxel
Extra et al. Eur J Cancer. 2004;2:125. Abstract 239.
1.0
36Month
sIntent-to-treat population, 12-month cut-offDocumented crossover = 48%
P = 0.0062
8.4 months
22.1 30.5
Trastuzumab + docetaxelDocetaxel
0.8
0.6
0.4
0.2
0.0 33302724211815129630
Trastuzumab + Paclitaxel Trastuzumab + Docetaxel
Trastuzumab plus a Taxane inHER-2 Positive Metastatic Breast Cancer
1Slamon DJ, et al. N Engl J Med 2001;344:783–922Baselga J. Oncology 2001;61(Suppl. 2):14–21
3Marty M, et al. J Clin Oncol 2004. In Press
Slamon1,2 Marty3
Outcome
H + P (n=68)
P (n=77)
H + D (n=92)
D (n=94)
ORR (%) 49.0 17.0 61.0 34.0
TTP (months) 7.1 3.0 10.6 5.7
OS (months) 24.8 17.9 30.5 22.1
ORR = objective response rateTTP = time to disease progression OS = overall survivalH = HerceptinP = paclitaxelD = docetaxel
Adjuvant Trastuzumab Efficacy in Early Breast Cancer: Disease Free Survival
0 1 2
HERA 1 year
Combined analysis 2 years
Median follow-up
FavoursHerceptin
Favours noHerceptin
HR
BCIRG 006 DCarboH 2 years
2 yearsBCIRG 006 AC DH
FinHER VH / DH CEF 3 years
Piccart-Gebhart et al 2005; Romond et al 2005;Slamon et al 2005; Joensuu et al 2005 Adapted from Poon RT, et al. J Clin Oncol 2001;19:1207–25
Angiogenesis is involved throughout tumour formation, growth and metastasis
Stages at which angiogenesis plays a role in tumour progression
Premalignantstage
Malignanttumour
Tumourgrowth
Vascularinvasion
Dormantmicrometastasis
Overtmetastasis
(Avasculartumour)
(Angiogenicswitch)
(Vascularisedtumour)
(Tumour cellintravasation)
(Seeding indistant organs)
(Secondaryangiogenesis)
Tumour characteristics and environment promote VEGF expression
EGF
Hypoxia PDGF
IL-8
bFGF
COX-2Nitric oxideOncogenes
VEGF releaseBinding and activation
of VEGF receptor
IGF-1
ProliferationSurvival Migration
ANGIOGENESISPermeability
Increased expression(MMP, tPA, uPA, uPAr,
eNOS, etc.)
– P– P
P–P–
Agents inhibiting angiogenesis through the VEGF pathway
VEGFVEGF
receptor-2
Cation channel
↑ Permeability
Antibodies inhibiting VEGF(e.g. bevacizumab)
Antibodies inhibiting VEGF receptors Soluble VEGF receptors
(VEGF-TRAP)
Small-molecules inhibiting VEGF receptors
(TKIs)(e.g. PTK-787)
Ribozymes(Angiozyme)
– P– PP–
P–
– P– P
P–P–
– P– P
P–P–
Migration, permeability, DNA synthesis, survival
LymphangiogenesisAngiogenesis

11
Summary: mechanism of action of anti-VEGF therapy
! Inhibition of VEGF may act against tumours in three ways– regression of existing microvasculature– normalisation of mature vasculature – inhibition of production of new vasculature
EARLY BENEFIT CONTINUED BENEFIT
Regressionof existing microvasculature
Normalisationof surviving microvasculature
Inhibitionof vessel regrowth and neovascularisation
Phase III trial of IFL ± Bevacizumabin metastatic Colorectal Cancer : survival
Median survival (months)IFL + placebo: 15.6 (95% CI: 14.3–17.0) vsIFL + Bevacizumab: 20.3 (95% CI: 18.5–24.2)HR=0.66 (95% CI: 0.54–0.81)p<0.001
CI = confidence intervalHR = hazard ratio
Pro
babi
lity
of s
urvi
val
1.0
0.8
0.6
0.4
0.2
00 10 20 30 40
Survival (months)
IFL + BevacizumabIFL + placebo
15.6 20.3
Hurwitz H, et al. N Engl J Med 2004;350:2335–42
Targeted Therapy in Colorectal Cancer Bevacizumab
Approved Indication! First-line treatment in combination with 5FU-based chemotherapy for
advanced colorectal cancer
Adverse events! Hypertension! Proteinuria! GT perforation, bleeding
Future Perspectives of Targeted Therapy
Narin Voravud, M.D.Medical Oncology Unit, Department of Medicine,
Faculty of Medicine, Thai Red Cross Society and King Chulalongkorn Memorial Hospital, Chulalongkorn University
Bangkok, Thailand
The 1st Asia Pacific Oncology Pharmacy Congress(APOPC)
August 5, 2006 Bangkok, Thailand
Published Randomized Trials of Targeted Therapy in Non-Small Cell Lung Cancer
1Hamilton M, et al. Proc Am Assoc Cancer Res 2005;43 (Abs. 6165)
No benefitPaclitaxel+CarboplatinLonafinibFarnesyltransferase
No benefitPaclitaxel+CarboplatinBMS 275291No benefitPaclitaxel+CarboplatinAG 3340Metalloproteinase
(Ras oncogene)
Benefit in non -
smoker
Paclitaxel+CarboplatinErlotinib(TRIBUTE)
EGFRNo benefitGemcitabine+CisplatinGefitinib
No benefitGemcitabine+CisplatinErlotinib (TALENT)
No benefitPaclitaxel+CarboplatinGefitinibEGFR
OutcomeChemotherapyTargeted AgentTarget
Published Randomized Trials of Targeted Therapy in Non-Small Cell Lung Cancer
1Hamilton M, et al. Proc Am Assoc Cancer Res 2005;43 (Abs. 6165)
↑Survival
↑Response Rate
Paclitaxel+CarboplatinBevacizumabVascular Endothelial
No benefitPaclitaxel+CarboplatinBexaroteneRetinoid X Receptor
↑PFSGrowth Factor
No benefitPaclitaxel+CarboplatinISIS 3521Protein kinase C
OutcomeChemotherapyTargeted AgentTarget
12
Ongoing Randomized Trial of Erlotinib inNon – Small Cell Lung Cancer
Advanced NSCLLTITAN
after platinum-based x 4(N=854)
after platinum-based chemotherapy(N=648)
Advanced NSCLLSATURN
(EGFR+)first-line
Advanced NSCLLOSI-774-203
Adjuvant treatment(N=945)
NSCLC (EGFR+)RADIANT
Second-line(N=650)
Advanced NSCLLBETA
after chemotherapy(N=1150)
Advanced NSCLLATAS
Study
RErlotinib+bevacizumab
Placebo+bevacizumab
RErlotinib+bevacizumab
Erlotinib+Placebo
RErlotinibPlacebo
RErlotinib
Erlotinib
Pemetrexed
R
Docetaxel
chemotherapy x 4+ Erlotinib
RErlotinibPlacebo
First-line phase III trial of Erlotinib sequencing with chemotherapy
! Primary endpoint: survival! Secondary endpoints: QoL, PFS, molecular
assessment! Enrolment planned to start Q1 2006
Gemcitabine + cisplatinsix cycles
Erlotinib150mg/day
Chemotherapy-naïve stage
IIIB/IV NSCLC (n>900)
Gemcitabine + cisplatinsix cycles
Erlotinib150mg/day
PD
PD
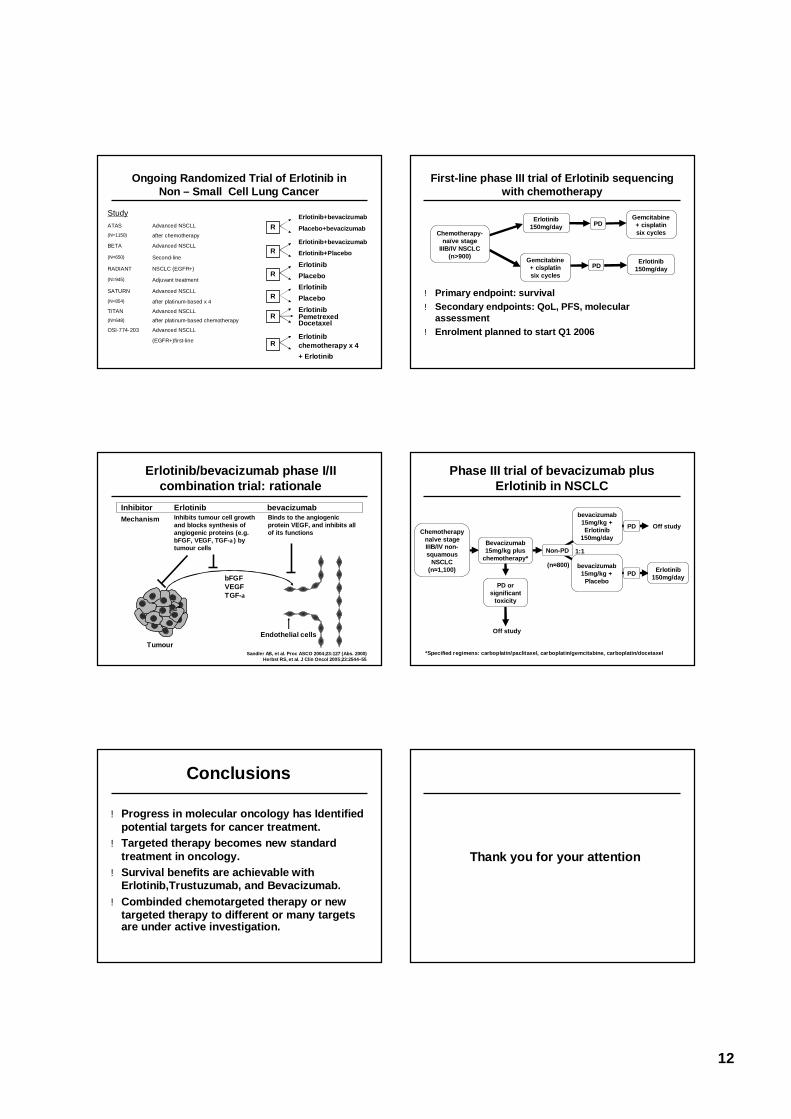
Erlotinib/bevacizumab phase I/II combination trial: rationale
Tumour
Inhibitor Erlotinib bevacizumabMechanism Inhibits tumour cell growth
and blocks synthesis of angiogenic proteins (e.g. bFGF, VEGF, TGF-α) by tumour cells
Binds to the angiogenic protein VEGF, and inhibits all of its functions
bFGFVEGFTGF-α
Endothelial cells
Sandler AB, et al. Proc ASCO 2004;23:127 (Abs. 2000)Herbst RS, et al. J Clin Oncol 2005;23:2544–55
Phase III trial of bevacizumab plus Erlotinib in NSCLC
bevacizumab15mg/kg +
Placebo
Chemotherapy naïve stage IIIB/IV non-squamous
NSCLC (n≈1,100) Erlotinib
150mg/day
Non-PD
*Specified regimens: carboplatin/paclitaxel, carboplatin/gemcitabine, carboplatin/docetaxel
Off study
bevacizumab15mg/kg +Erlotinib
150mg/day
PD
Off study
(n≈800)
PD
1:1Bevacizumab 15mg/kg plus
chemotherapy*
PD or significant
toxicity
Conclusions
!Progress in molecular oncology has Identified potential targets for cancer treatment.
!Targeted therapy becomes new standard treatment in oncology.
!Survival benefits are achievable with Erlotinib,Trustuzumab, and Bevacizumab.
!Combinded chemotargeted therapy or new targeted therapy to different or many targets are under active investigation.
Thank you for your attention