table rock regional roundup part 2: costly coding · pdf file · 2016-09-29table...
TRANSCRIPT

Table Rock Regional Roundup
Part 2: Costly Coding Errors
and Lessons Learned from
Real Life Audits
Saturday, September 23, 2016

Financial Disclosure
•Sue Vicchrilli, COT, OCS
•Director, Coding and Reimbursement
o Has no financial interests or
relationships to disclose.

Topics
• Types of Audits
o It’s not a matter of if, but when
• ICD-10 Update
• What’s Coming

Types of Audits

Types of Audits: Documentation Review
• All payers conduct audits
o Primary importance
– Physician signature!
– Legibility for paper records
– Physician signature secure for EHR
o Automatic failure and payment recoupment
o 50% or greater = extrapolation

Types of Audits – Diagnosis Reporting
• Medicare Advantage Plans
o Review of Systems data
o Determine costs to care for patients
o More money from CMS
o OIG investigations of “inflating” diagnosis

Types of Audits – Diagnosis Reporting
• Your options:
1. Administrative Burden:
Reduce number of chart requests
Costs – Set up an account
– $ per page by state rule, or
– Lump amount for each chart
2. Allow insurance staff to copy records
Your staff still monitors what they copy/upload

ICD-10 Update

ICD-10 Information Update
• ICD-10 has rules that are not required for payment by the payer.o Code first underlying disease
o Excludes1 edits
o Injury and trauma “how” codes may only be required by Workers Comp – who doesn’t have to convert to ICD-10!
o Look at LCDs or Ophthalmic Coding Coach/Complete Guide to Retina for ICD-10 to CPT code linkage.

ICD-10 Update
• 368 new ICD-10 codes impacting
ophthalmology effective Oct 1
o Impacts PQRS reporting too
• No due date by which payers must
update their databases; however
• Watch for updates to LCDs.

Laterality to POAG
• Replace the X in 6th position
with 1, 2, 3
• H40.11 Primary open-angle
glaucoma
o H40.111 POAG, right eye
o H40.112 POAG, left eye
o H40.113 POAG, bilateral
Continue staging in 7th
position
1 = mild
2 = moderate
3 = severe
4 = indeterminate

Diabetes Type 1 and Type 2
• What’s new?
o Laterality in the 7th position
Exception E10.9 and E11.9 without
complication has no laterality
o For proliferative retinopathy, identification of
stable PDR,
traction or
rhegmatogenus RD involving macula

Type 1 Diabetes E10Without mention of complication E10.9
With mild non-prolif, with macular edema E10.321
With mild non-prolif, without macular edema E10.329
With moderate non-prolif, with macular edema E10.331
With moderate non-prolif, without macular edema E10.339
With severe non-prolif, with macular edema E10.341
With severe non-prolif, without macular edema E10.349
With prolif retinopathy, with macular edema E10.351
With prolif retinopathy, without macular edema E10.359
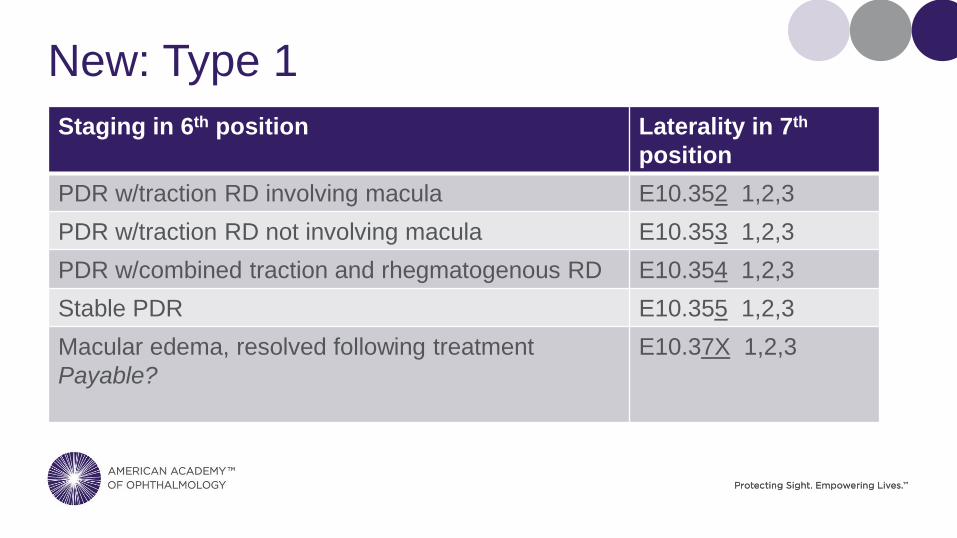
New: Type 1
Staging in 6th position Laterality in 7th
position
PDR w/traction RD involving macula E10.352 1,2,3
PDR w/traction RD not involving macula E10.353 1,2,3
PDR w/combined traction and rhegmatogenous RD E10.354 1,2,3
Stable PDR E10.355 1,2,3
Macular edema, resolved following treatment
Payable?
E10.37X 1,2,3

Type 2 Diabetes E11
Without mention of complication E11.9
With mild non-prolif, with macular edema E11.321
With mild non-prolif, without macular edema E11.329
With moderate non-prolif, with macular edema E11.331
With moderate non-prolif, without macular edema E11.339
With severe non-prolif, with macular edema E11.341
With severe non-prolif, without macular edema E11.349
With prolif retinopathy, with macular edema E11.351
With prolif retinopathy, without macular edema E11.359

New: Type 2
Staging in 6th position Laterality 7th
position
PDR w/traction RD involving macula E11.352 1,2,3
PDR w/traction RD not involving macula E11.353 1,2,3
PDR w/combined traction and rhegmatogenous RD E11.354 1,2,3
Stable PDR E11.355 1,2,3
Macular edema, resolved following treatment
Payable?
E11.37X 1,2,3

PDR & DME Distinct, Parallel Disease Processes
Proliferative
Retinopathy
Diagnosis w/DME Diagnosis
E10.359-
OR E10.351-
Type 1 E10.351-
OR E10.359-
PDR with or without DME
H43.1- PDR, vitreous
hemorrhage
A
N
D
E10.351-
OR E10.359-
with or without DME
E10.355- Stable PDR A
N
D
E10.351-
OR E10.359-
with or without DME
E10.352- PDR w/ TRD inv
the macula
A
N
D
E10.351-
OR E10.359-
with or without DME
E10.353- PDR w/ TRD not
inv the macula
A
N
D
E10.351-
OR E10.359-
with or without DME
E10.354- PDR w/ TRD &
Rheg RD
A
N
D
E10.351-
OR E10.359-
with or without DME

PDR & DME Distinct, Parallel Disease Processes
Proliferative
Retinopathy
Diagnosis w/DME Diagnosis
E11.359-
OR E11.351-
Type 2 E10.351-
OR E10.359-
PDR with or without
DME
H43.1- PDR, vitreous
hemorrhage
A
N
D
E11.351-
OR E11.359-
with or without DME
E11.355- Stable PDR A
N
D
E11.351-
OR E11.359-
with or without DME
E11.352- PDR w/ TRD
inv the macula
A
N
D
E11.351-
OR E11.359-
with or without DME
E11.353- PDR w/ TRD
not inv the
macula
A
N
D
E11.351-
OR E11.359-
with or without DME
E11.354- PDR w/ TRD &
Rheg RD
A
N
D
E11.351-
OR E11.359-
with or without DME

No Diagnosis of Diabetes?
• No diabetes diagnosis but glucose
issues:
o Report R73.09 Abnormal glucose level

Age-Related Macular Degeneration
• Whether wet or dry
o Now specifies eye
In the 6th position

Wet AMD – Part 1
• Exudative (wet) AMD now requires
laterality.
• Location is 6th position.
• H35.321 Nonexudative AMD, right eye
• H35.322 Nonexudative AMD, left eye
• H35.323 Nonexudative AMD, bilateral
Wet AMD – Part 2
• Wet AMD requires a 7th final character:
1 = with active choroidal neovascularization
2 = with inactive choroidal neovascularization
3 = with inactive scar

Wet AMD Example
H35.32 3 1
Exudative age-related macular
degeneration, bilateral, with active
choroidal neovascularization

Dry AMD – Part 1
• Nonexudative (dry) AMD now requires
laterality.
• Location is 6th position.
• H35.311 Nonexudative AMD, right eye
• H35.312 Nonexudative AMD, left eye
• H35.313 Nonexudative AMD, bilateral

Dry AMD – Part 2
• Dry AMD requires 7th final character:
1 = dry stage
2 = intermediate dry stage
3 = advanced atrophic without subfoveal
involvement
4 = advanced atrophic with subfoveal
involvement

Dry AMD Example
H35.31 2 2
Dry AMD
• Nonexudative age-related macular
degeneration, left eye, intermediate dry
stage
Amblyopia
• New codes
H53.041 Amblyopia suspect, right eye
H53.042 Amblyopia suspect, left eye
H53.043 Amblyopia suspect, bilateral

ICD-10 Resources
• www.aao.org/ICD-10
• Webinar recording on new Diabetes,
AMD, BRVO and CRVO
www.aao.org/store
• Ophthalmology specific ICD-10 book
www.aao.org/store
• ICD-10 online www.aao.org/store

ICD-10 Resources
• October 2016 EyeNet Savvy Coder
• Coding Coach book and online
www.aao.org/store
• Complete Guide to Retina Coding
www.aao.org/store
• Questions? Email [email protected]

What’s Coming
Modifier -JW
• Effective Jan 1, 2017 delay from July 1,
2016
o Use the -JW modifier for claims with unused
drugs or biologicals from single use vials or
single use packages that are appropriately
discarded (except those provided under the
Competitive Acquisition Program (CAP) for
Part B drugs and biologicals) and

Modifier -JW
o Document the discarded drug or biological
in the patient's medical record.
Modifier -JW
• Bill the drug
• Bill a second line with modifier –JW
o Indicating the amount of drug wasted

Modifier -JW
• Exception:
o Administered dosage is less than the
billable unit and the increments of dosage
and wastage can’t be broken down
o Just document in medical record

Unilateral Payment for Testing Services
•Ophthalmology is fortunate in that we still have tests that
are payable for the right and left side of the body or
unilateral payment.
o Do not bill for the eye that does not have pathology.
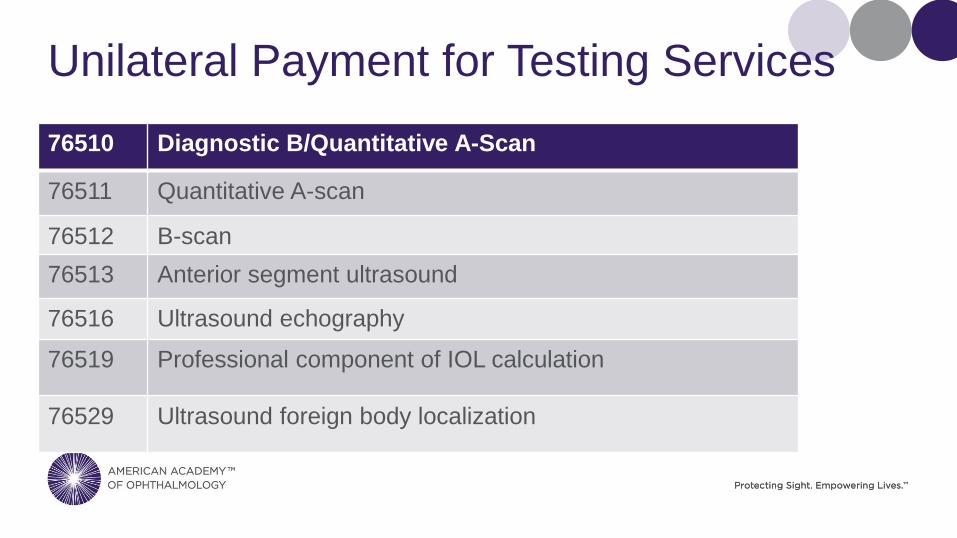
Unilateral Payment for Testing Services
76510 Diagnostic B/Quantitative A-Scan
76511 Quantitative A-scan
76512 B-scan
76513 Anterior segment ultrasound
76516 Ultrasound echography
76519 Professional component of IOL calculation
76529 Ultrasound foreign body localization

Unilateral Payment for Testing Services
92071 Bandage contact lens
92136 Professional component of IOLMaster, Lenstar
92225 Extended ophthalmoscopy
92226 Subsequent ophthalmoscopy
92230 Fluorescein angioscopy
92235 Fluorescein angiography
92240 ICG

Unilateral Payment for Testing Services
•When pathology is in both eyes:
o Some payers require a two line submission with -RT and -LT and a
1 in each unit field.
o Other payers require a single line submission appended with
modifier -50 and a 2 in the unit field.
Make sure payment is correct at 100 percent of the allowable for each
eye.

Payment Update
•RVUs for
o 92235 FA
o 92240 ICG
Based on film and development
How long have you performed digital photography?

Payment Update
•Effective January 1
o Payment for FA and ICG will reflect new RVUs
o Payment will be inherently bilateral

New Code in 2017
•92242 Fluorescein angiography and indocyanine-green
angiography (including multiframe imaging) performed at
the same patient encounter with interpretation and report
•Bilateral

New Code in 2017
•Vignette: 77-year-old female with a history of dry age-
related macular degeneration presents with subretinal
blood and fluid
•Direct supervision

MPPR
•Implemented January 2013
•When multiple tests are performed the same day, same
patient, the lowest technical component allowable on the
second and subsequent tests is reduced by 20 percent.
•Impacts all tests that have a technical component or tests
that can be delegated.

MPPR Case Scenario
•The following are performed on the same day:
o An exam, CPT code 92012
o SCODI CPT code 92133,
o Visual field CPT code 92183,
o Pachymetry CPT code 76514
MPPR Case Scenario
•Payment for this Medicare Part B patient until December
31, 2016 will be:
o 100 percent of the exam
o 100 percent of the visual field
o 80 percent payment of the technical component
92133 $3.24 less
76514 $1.06 less

MPPR Update
•Good News!
•Effective January 1, 2017 the reduction will be less
•CMS identifies impacted CPT codes by appending modifier
-51.

2015 Success?
2016 PQRS/VBM Reporting
2017 MIPS

2015 Reporting Success
• Find out now if you were successful or
not
o www.aao.org/pqrs
o Feedback reports are not available as of
today.
o Appeal process has not be published.

Penalties
• Penalties depend on the size of the
physician practice
o No PQRS or unsuccessful participation?
o 4% penalty for less than 10 physicians
o 6% penalty for 10 or more physicians
Note: if more than 50% of the qualifying
providers fail, practice may be subject to
VBM penalty.

New 2016 PQRS Reporting Option
• Diabetic Retinopathy Measures Group
o Report all 7 measures on 20 cases. Of the
20, at least 11 patients must have Medicare
Part B insurance. The remaining patients
may have Medicare Advantage or
commercial insurance.
o Ages 18-75
o IRIS Registry reporting
Diabetic Retinopathy Measures Group
1. Measure 1 Diabetes: Hemoglobin A1c Poor Control
2. Measure 18 Diabetic Retinopathy: Documentation of Presence or Absence of Macular Edema and
Level of Severity of Retinopathy
3. Measure 19 Diabetic Retinopathy: Communication with the Physician Managing Ongoing Diabetes
Care
4. Measure 117 Diabetes: Eye Exam
5. Measure 130 Documentation of Current Medications in the Medical Record
6. Measure 226 Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
7. Measure 317 Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up
Documented
• Take at least 1 blood pressure to meet measure 317

PQRS Reporting as of Oct 1
• ICD-10 code updates finalized late June.
• CMS is not updating measure diagnosis
for claims or registry
• Many PQRS measures are impacted
o AMD, diabetes, glaucoma
o Impacts last 3 months of reporting
o What about new physicians to your
practice?

Merit-Based Incentive Payment
System (MIPS)

MIPS
• A consolidation of PQRS, VBM and MU
• How we report in 2017 impacts 2019
payments for:
o Medicare Part B
o Medicare as a Secondary Payer
o Railroad Medicare


Exclusions
• See fewer than 100 Medicare patients
o AND bill less than $10,000 in charges
• Newly enrolled in Medicare during the
reporting year

AMA compares penalty risks for 2019
Prior Law 2019 Adjustment
PQRS -2%
MU -5%
VBM -4% or more*
Total penalty risk -11 or more*
Bonus potential
(VBM only)
Unknown
(budget neutral)
*VBM was in effect for 3 years before
MACRA passed, and penalty risk was
increased in each of these years.
There were no ceilings or floors on
penalties and bonuses; only a budget
neutrality requirement.

MIPS
• Four components
Quality
(PQRS)
Resource
Use
(VBM)
Advancing
Care
Information
(ACI)
(MU)
Clinical
Practice
Improvement
Activities
(CPIA)

Quality
• Formerly known as PQRS
• 50% of score
• Report via IRIS Registry or claims
o 6 measures including
1 cross-cutting measure and
1 outcome measure
o Can receive partial credit if unable to report 6
measures and at least 1 cross-cutting measure

Quality Measures
• Unspecified diagnosis codes
o Are valid ICD-10 code, but
o Not payable ICD-10 codes
o Will still be included in measures specifications
o Like ICD-10 for Ophthalmology book
Identified by strikethrough

Quality
• IRIS Registry = 90% on all patients
• Claims = 80% of all Medicare Part B
patients

Resource Use
• Formerly known as value based modifier
• 10% of score
• Costs
• No need to submit separate data.
o CMS will determine resource use through
administrative claims.

Advancing Care Information
• Formerly known as Meaningful Use
• 25% of score
• Answer yes or no
o No specific threshold
• Receive credit:
o ½ credit: Report on every measure at least one patient or
yes/no
o ½ credit: How many additional patients you can get to report

Clinical Practice Improvement Activities
• 15% of score
• 94 CPIAs are proposed by CMS
o Each will be assigned a point system
High 20 points
Medium 10 points
Must achieve 60 points during 90-day
reporting period

Question
• Can I get a neutral score or even a
bonus score without EHR?

Answer
• Based on the proposed rule, it would
depend on what final composite score is
and how it compares to the benchmark.
• With ACI accounting for 25% you will
begin with 75/100.

Answer
• Your final composite score would be
compared against the benchmark, and
payment adjustment determined by how
far you fall from the benchmark.

Answer
• If your composite score is lower than the
benchmark, you’ll earn a penalty.
• If your composite score is equal to the
benchmark, you’ll be neutral.
• If your composite score is higher than
the benchmark, you’ll be eligible for a
bonus.

New: 2017 Pick Your Pace
• Released September 8, 2016
• First year of performance, CMS will allow
physicians multiple options for
participation.
• Final rule (published date?) will provide
more detail as to applicable measures,
guidelines, etc.

New: Pick Your Pace
• #1 To avoid the negative payment
adjustment
o Submission of some quality payment data
after January 1, 2017
o Allows you to get more comfortable with the
program and enable you to perform fully in
2018.

New: Pick Your Pace
• #2 Potential qualification for small bonus
payment
o Reporting for part of 2017- not yet defined.
o Participate in quality measures, use of
technology and improvement activities

New: Pick Your Pace
• #3 Potential qualification for modest
bonus payment
o Reporting period is full calendar year of
2017.
o Participate in quality measures, use of
technology and improvement activities

New: Pick Your Pace
• #4 Qualification for 5 percent bonus
o Advanced Alternative Payment Model
(APM)
o Most ophthalmologists will not qualify for
this option.
o For those participating in a payment model
such as Medicare Shared Savings Track 2
or 3

IRIS Registry
• Not too late for 2016 assistance.
• Reporting does not have to be done in
real time.
• Accuracy
• www.aao.org/irisregistry

Pele
Success is no accident.
It is hard work, perseverance, learning,
studying, sacrifice, and most of all, a
love of what you are doing.
