systems of care for st-segment–elevation myocardial...
TRANSCRIPT

Systems of Care for ST-Segment–Elevation MyocardialInfarction: A Report From the American Heart
Association’s Mission: LifelineJames G. Jollis, MD; Christopher B. Granger, MD; Timothy D. Henry, MD; Elliott M. Antman, MD;
Peter B. Berger, MD; Peter H. Moyer, MD, MPH; Franklin D. Pratt, MD; Ivan C. Rokos, MD;Anna R. Acuna; Mayme Lou Roettig, RN, MSN; Alice K. Jacobs, MD
Background—National guidelines call for participation in systems to rapidly diagnose and treat ST-segment–elevationmyocardial infarction (STEMI). In order to characterize currently implemented STEMI reperfusion systems and identifypractices common to system organization, the American Heart Association surveyed existing systems throughout theUnited States.
Methods and Results—A STEMI system was defined as an integrated group of separate entities focused on reperfusiontherapy for STEMI within a geographic region that included at least 1 hospital that performs percutaneous coronaryintervention and at least 1 emergency medical service agency. Systems meeting this definition were invited to participatein a survey of 42 questions based on expert panel opinion and knowledge of existing systems. Data were collectedthrough the American Heart Association Mission: Lifeline website.
Between April 2008 and January 2010, 381 unique systems involving 899 percutaneous coronary intervention hospitals in47 states responded to the survey, of which 255 systems (67%) involved urban regions. The predominant fundingsources for STEMI systems were percutaneous coronary intervention hospitals (n�320, 84%) and /or cardiologypractices (n�88, 23%). Predominant system characteristics identified by the survey included: STEMI patient acceptanceat percutaneous coronary intervention hospital regardless of bed availability (N�346, 97%); single phone call activationof catheterization laboratory (N�335, 92%); emergency department physician activation of laboratory withoutcardiology consultation (N�318, 87%); data registry participation (N�311, 84%); and prehospital activation of thelaboratory through emergency department notification without cardiology notification (N�297, 78%). The mostcommon barriers to system implementation were hospital (n�139, 37%) and cardiology group competition (n�81,21%) and emergency medical services transport and finances (n�99, 26%).
Conclusions—This survey broadly describes the organizational characteristics of collaborative efforts by hospitalsand emergency medical services to provide timely reperfusion in the United States. These findings serve as abenchmark for existing systems and should help guide healthcare teams in the process of organizing care forpatients with STEMI. (Circ Cardiovasc Qual Outcomes. 2012;5:00-00.)
Key Words: delivery of health care � multi-institutional systems � myocardial infarction � myocardial reperfusion
For more than 2 decades, medical evidence has shownrapid coronary reperfusion reduces mortality in patients
with ST-segment–elevation myocardial infarction (STEMI).1–3
Moreover, it has been increasingly clear that percutaneouscoronary intervention (PCI) is the preferred method of rep-erfusion if it can be performed in a timely manner.4,5 Yet,reperfusion therapy continues to be administered too slowly,
particularly in patients undergoing hospital transfer forprimary PCI.6,7 In order to provide primary PCI morerapidly, many medical centers have begun to coordinate carebeyond the traditional boundaries of a hospital.8–12 By im-plementing reperfusion strategies that incorporate the patientwith STEMI’s first and subsequent medical contacts, includ-ing emergency medical service (EMS) transport between
Received July 12, 2011; accepted April 12, 2012.From Duke University Medical Center, Durham, NC (J.G.J., C.B.G.); Minneapolis Heart Institute Foundation, Minneapolis, MN (T.D.H.); Brigham
and Women’s Hospital, Boston, MA (E.M.A.); Geisinger Health System, Danville, PA (P.B.B.); Boston Emergency Medical Services, Boston, MA(P.H.M.); Los Angeles County Fire Department, Los Angeles, CA (F.D.P.); University of California, Los Angeles (UCLA)-Olive View Medical Center,David Geffen School of Medicine at UCLA (I.C.R.); American Heart Association, Dallas, TX (A.R.A.); Duke Clinical Research Institute, Durham, NC(M.L.R.); Boston Medical Center, Boston, MA (A.K.J.).
Guest Editor for this article was Brahmajee K. Nallamothu, MD. The Editors had no role in the evaluation of the article or the decision about itsacceptance.
The online-only Data Supplement is available at http://circgenetics.ahajournals.org/lookup/suppl/doi:10.1161/CIRCGENETICS.111.964668/-/DC1.Correspondence to James G. Jollis, MD, Professor of Medicine and Radiology, Room 3347 Duke South Hospital, Box 3254 DUMC, Durham, NC
27710. E-mail [email protected]© 2012 American Heart Association, Inc.
Circ Cardiovasc Qual Outcomes is available at http://circoutcomes.ahajournals.org DOI: 10.1161/CIRCOUTCOMES.111.964668
1
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from

hospitals, delays in achieving reperfusion have been greatlyreduced, and enthusiasm for developing systems of care hasemerged.13–15 Based on the existing delays to reperfusion, thebarriers to timely treatment, and the success of early modelSTEMI systems,16 the American Heart Association (AHA)embarked on Mission: Lifeline, an initiative to improve thequality of care and outcomes for patients with STEMI and toimprove the healthcare system readiness and response toSTEMI. An important focus of Mission: Lifeline is to increasethe number of patients with timely access to primary PCI.17–18
In order to characterize currently implemented STEMIreperfusion systems and identify practices common to systemorganization and potential best practices, the AHA surveyedexisting systems throughout the United States.
WHAT IS KNOWN
● Coronary reperfusion can be greatly accelerated bycoordinated care between hospitals and emergencymedical services in a region.
WHAT THE STUDY ADDS
● In a large national survey, several processes werecommonly implemented, including accepting pa-tients at a PCI hospital regardless of bed availability,single phone call activation of catheterization labo-ratory, emergency department physician activationof a laboratory without cardiology consultation, na-tional data registry participation, and prehospitalactivation of the catheterization laboratory by para-medics and transferring physicians.
● The most commonly reported barriers to systemimplementation were hospital and cardiology groupcompetition and EMS transport and finances.
MethodsWe developed a 42-question survey based on expert panel opinionand knowledge of existing systems (online-only Supplemental DataAppendix A). Survey questions focused on processes of care for the
diagnosis, system activation, and treatment of STEMI. The surveyalso examined resource allocation, financial considerations, and themost significant barriers to implementing systematic care. Surveydata were collected through the AHA website (Register Your System)(online-only Supplemental Data Appendix A). In addition to postingthe survey on the website, registration of existing STEMI networkswas encouraged at local, regional, and national meetings involvingthe treatment of STEMI and by the AHA staff of 8 regional affiliatescovering all 50 states. The survey was initially made available inApril 2008, and responses through January 2010 were analyzed. Thesurvey took approximately 60 minutes to complete and was deployedusing online survey software (Vovici Corporation). For the majorityof questions, multiple responses were allowed. For the purposes ofthis survey, a STEMI system was defined as an integrated group ofseparate entities focused on reperfusion therapy for STEMI within ageographic region that included at least 1 hospital that performs PCIand at least 1 EMS agency.
In order to avoid double counting, all new system submissionswere reviewed on a monthly basis. Any system that did not meet thesystem definition based on their responses was not included in thedata. Duplicate responses were identified using 1 of 2 methods: 1)the regional AHA office reported a duplicate; or 2) the response wasfrom the same individual, agency, and address. Systems that hadmultiple submissions were contacted by an AHA staff member toverify which submission should be kept in the systems database. Toconsider the representativeness of the survey, responses were cate-gorized by state and as a function of the number of PCI hospitals.
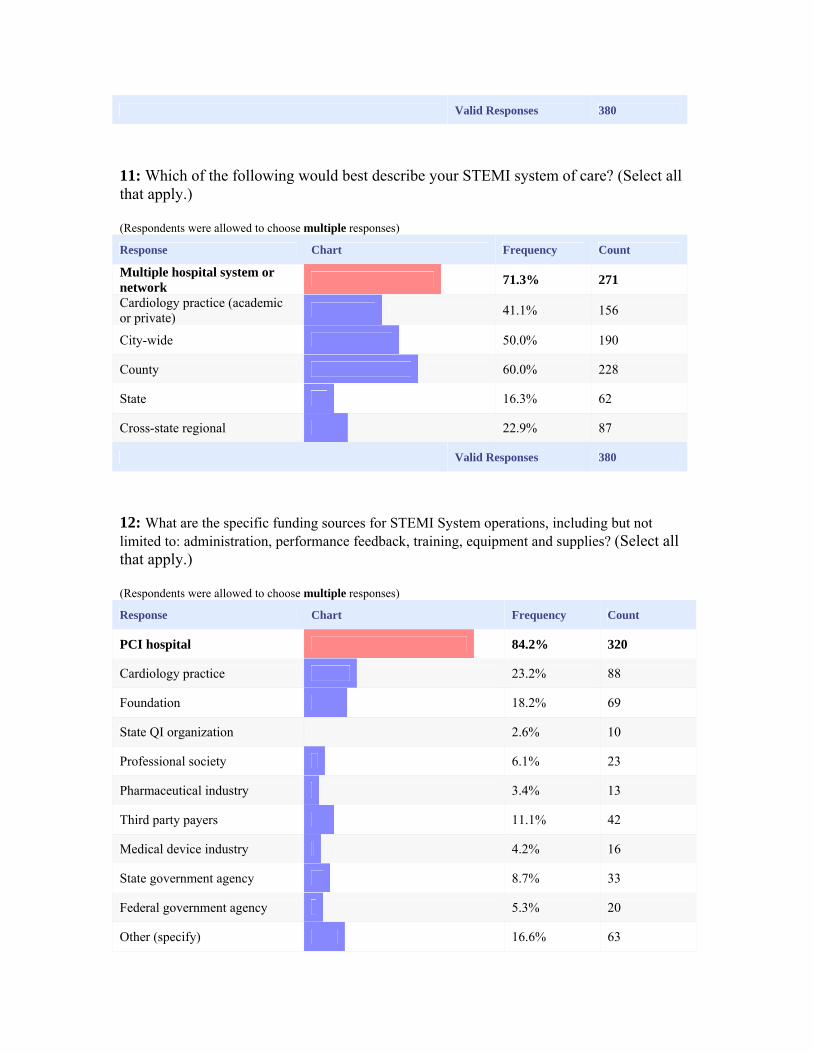
ResultsA total of 381 unique systems involving 899 PCI hospitalsfrom 47 states responded to the survey (Figure 1A and 1B andonline-only Supplemental Data Appendix B). Of these sys-tems, 202 involved a single PCI hospital, 150 encompassed 2to 5 PCI hospitals, and 29 included �5 PCI hospitals(online-only Supplemental Data Appendix C). The systemsidentified affiliations with 3539 non-PCI hospitals, some ofwhich may have been counted by more than 1 system. Froma geographic perspective, 279 (74%) involved rural regions,and 255 (67%) involved urban regions; 228 (60%) werecounty-based; 190 (50%), city-based; 620 (16%), state-based,and 87 (23%) crossed state lines. The predominant fundingsources for STEMI systems are shown in Figure 2. A broadarray of groups provided STEMI system oversight, includingcardiology, emergency medicine, emergency departments(ED), hospital and catheterization laboratory administration,
Figure 1. A, Mission: Lifeline: Registered STEMI systems by state. B, Mission Lifeline: STEMI systems coverage.
2 Circ Cardiovasc Qual Outcomes July 2012
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from

nursing, EMS, and cardiology quality improvement personnel(Figure 3).
EMS OrganizationA number of survey questions involved EMS organizationand protocols. Most systems responded to potential STEMIcalls using a combination of paramedic and lower levelemergency medical technician-staffed ambulances (N�237,62%), while 115 systems (30%) had only basic orintermediate-level emergency medical technician-staffed ve-hicles, and 249 systems (66%) included helicopter transport.More than one half of systems (N�209, 55%) reported theavailability of 12-lead electrocardiograms (ECGs) in theirvehicles, and it was available in some but not all for anadditional 155 (41%) systems. The ability to transmit ECGsto the receiving hospitals for all ambulances was available in132 (35%) of systems, and an additional 135 systems (36%)could transmit ECGs in some ambulances. The most com-monly reported methods of ECG interpretation were trans-mission to a hospital (N�184, 68%), paramedic interpreta-tion (N�170, 63%), and computer interpretation (N�92,34%). When a prehospital ECG revealed a STEMI, thecatheterization laboratory was activated through ED notifica-tion without the involvement of cardiology for 297 systems(78%); 72 systems (19%) involved a cardiologist for activa-tion; and 58 systems (15%) enabled an emergency medicaltechnician to directly activate the laboratory. The EMSperformance measures routinely tracked and reviewed areshown in Figure 4. The most commonly reported frequenciesof laboratory cancellation were �10% (N�202, 54%), 10%to 24% (N�79, 21%), and �25% (N�14, 4%). Two hundred
and twenty seven (61%) systems reported that protocols werein place to allow for diversion to a PCI hospital for patientsdiagnosed with a STEMI by a prehospital ECG. Most of theseprotocols were implemented independent of legislation(N�186, 82%); while 41 systems (18%) indicated thatdestination protocols were supported by legislation. Seventyseven systems (21%) reported the use of prehospital fibrino-lysis (sometimes, 52 systems; routinely, 25 systems).
PCI HospitalsRegarding PCI hospitals involved in the STEMI systems, 346(97%) accepted STEMI patients regardless of bed availabil-ity, 335 (92%) could activate the catheterization laboratorywith a single call, 318 (87%) permitted emergency physiciansto activate the laboratory without cardiology consultation,and 311 (84%) participated in a data registry. The mostfrequently reported registries were National CardiovascularData Registry (NCDR) Cath PCI (N�201, 61%), NCDRAcute Coronary Treatment and Intervention Outcomes Net-work (ACTION) (N�114, 35%), Get With The Guidelines(N�89, 27%), and local or program-specific registries(N�72, 22%). Common performance measures at the PCIhospital are shown in Figure 5. Most systems providedfeedback on performance to the ED at the PCI hospital(N�318, 84%) and to emergency medical personnel(N�285, 75%), and 175 systems (46%) provided feedback tothe referring hospital ED. The most common time frame forfeedback was 24 hours to 1 week (N�173, 46%), with 135systems (36%) providing monthly feedback and 133 systems(35%) providing feedback within 24 hours.
Figure 2. Predominate funding sources.
Figure 3. Organizations that provide oversight.
Figure 4. EMS performance measures routinely tracked.
Figure 5. Hospital performance measures routinely tracked.
Jollis et al Systems of Care for STEMI 3
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from

Reperfusion StrategyThe most frequent reperfusion strategy employed by non-PCIhospitals involved a mixed strategy employing both fibrino-lysis and PCI (N�198, 52%); 135 systems (36%) predomi-nantly referred for a PCI strategy, and 69 systems (18%)involved a fibrinolysis strategy. Among patients treated withfibrinolysis, 256 systems (81%) transferred these patients onan emergency basis to PCI hospitals, 35 systems (11%)routinely transferred patients on a nonurgent basis, and 24systems (8%) did not routinely transfer fibrinolysis patientsunless their clinical condition necessitated it later. For pa-tients requiring transport to PCI hospitals, local EMS wasused by 241 systems (63%), air transport by 168 systems(44%), and mobile intensive care unit sent by the PCI hospitalfor 48 systems (13%). Reperfusion protocols for non-PCIhospitals included standardized protocols specifying adjunc-tive anticoagulation (N�244, 78%), transfer by the sameEMS unit that brought the patient to the non-PCI hospital(N�136, 36%), avoidance of intravenous infusions (N�73,19%), and reduced-dose fibrinolysis before transfer for PCI(N�25, 7%).
Barriers to System ImplementationThe final question about barriers to the optimal functioning ofthe STEMI system allowed respondents to choose �1 re-sponse and to identify additional barriers not listed among thepossible responses provided. The most common barriers werehospital competition (N�139, 37%), EMS transport andfinances (N�99, 26%), competition between cardiologygroups (N�81, 21%), lack of data collection and feedback(N�68, 18%), lack of infrastructure support and funding(N�59, 16%), and lack of bed availability (N�59, 16%).Additional responses, many of which included free text, arelisted in the online-only Supplemental Data Appendix.
DiscussionRecognizing the importance of regional coordination of EMSand hospitals for the rapid diagnosis and treatment of STEMI,the 2009 update of the American College of Cardiology/AHASTEMI Guidelines added a new Class I recommendation that“each community should develop a STEMI system of care.”14
This report presents the first national survey of STEMIsystems, examining implementation from multiple perspec-tives, including funding, data, and specific EMS and hospitalprotocols. Respondents identified the widespread applicationof a number of interventions likely to improve treatmenttimes, including direct activation of the catheterization labo-ratory by paramedics and emergency physicians, destinationor hospital bypass protocols, interhospital transfer protocols,data collection using national data instruments, and timelyfeedback to healthcare providers involved in STEMI care.The survey also revealed common barriers to regional STEMIcare with competition, EMS finances, and data collectionbeing the predominant challenges. These findings shouldassist ongoing efforts to organize regional care by identifyingcommon approaches to systematic problems and by definingthose challenges most frequently shared by systems thatwarrant the greatest investment of additional resources.Moreover, those systems registered with Mission: Lifeline are
now part of a STEMI system community that may share newinformation, resources, and best practices through the AHA’ssocial network (http://mlcommunity.heart.org).
A number of interesting themes emerged from the inquiry.By far, the most frequent source of funding for STEMIsystems was the PCI hospitals. Additional funding wasderived from a broad array of industry, government, andfoundation sources. As PCI hospitals have a mandate fromthe Center for Medicare & Medicaid Services to providetimely reperfusion and report their results publicly, thesehospitals have additional incentive to improve the speed ofcoronary reperfusion19,20; however, the Center for Medicare& Medicaid Services mandate does not entirely explain thefinding, as patients transferred from other hospitals to PCIhospitals are excluded from the measures. PCI hospitals haveincentives to support the development of STEMI systemsabove and beyond improving the quality of care, whichinclude increasing catheterization laboratory volume and tobe recognized as an exceptional regional facility in theprovision of cardiac care. It is interesting that so few systemsidentified payers as a source of support. The financialinterests of health insurers are not limited to a single hospitalor physicians group. Potentially, payers have much to gainfrom more coordinated and rapid treatment of patients withSTEMI, including better outcomes for their beneficiariesmanifested as fewer complications, shorter hospitalizationsand lower use of medical care after discharge.21 Greater payersupport for STEMI systems will likely require additionalevidence to build a business case for coordinated rapidcoronary reperfusion.
More than half of the STEMI systems reported the avail-ability of ECGs in emergency medical vehicles, with approx-imately two-thirds having the capability to transmit ECGs insome or all of their ambulances. The predominant method forEMS to activate the catheterization laboratory involved com-munication with the receiving ED, while some systemspermitted emergency medical technicians to directly activatethe laboratory team. Most importantly, the survey identifiedcontinued opportunities to improve STEMI care, particularlyby establishing protocols for early laboratory activation forall patients with the prehospital diagnosis of STEMI, as wellas by expanding the 12-lead ECG capability on ambulances.According to this survey, STEMI protocols can be establishedwithout the need for legislation for the majority of systems.
For hospitals lacking PCI facilities, �one half reported theuse of a mixed strategy of fibrinolysis and PCI while anadditional third relied on a transfer for a PCI strategy. Patientstreated with fibrinolysis were urgently transferred to PCI-capable hospitals for most STEMI systems, indicating thatprovisions for rapid transfer represent an important compo-nent for STEMI treatment, even in the systems initiallyrelying on fibrinolysis. This approach is consistent withrandomized trials and current guidelines supporting transferof higher-risk patients treated with fibrinolysis.14,22,23 LocalEMS transfer was more commonly reported than air trans-port, likely a function of distances between facilities amongthe systems surveyed. The fact that only 8% of non-PCIcapable hospitals do not routinely transfer patients afterfibrinolytic therapy provides important insight into the role of
4 Circ Cardiovasc Qual Outcomes July 2012
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
the PCI center for the vast majority of patients with STEMI,even those presenting to non-PCI centers.
Commonly reported barriers to STEMI systems includedcompetition between hospitals and physician groups, funding,and data collection. Medical care in the United States istraditionally organized by hospitals, physician practices, andEMS. These reported barriers reflect deficiencies of ourhealthcare system in providing adequate support to allow forcoordinated patient care among these entities. In particular,fiscal horizons that end at the hospital or ambulance door maynot allocate adequate funds for STEMI systems. Furthermore,in this traditional model, competition between hospitals andphysician groups discourages collaboration in a joint andsystematic fashion.
The lack of support for the development of STEMI systemsmay be remedied through a number of approaches. As above,public reporting of performance measures that extend beyondtraditional borders, such as first medical contact to reperfu-sion, will provide an incentive to hospitals and EMS tocollaborate. Support for STEMI systems may also be encour-aged by involving entities with medical and fiscal responsi-bilities that span multiple hospitals, physician groups, andEMS such as large payers and government agencies. It hasbeen suggested that the most attractive proposition for pay-ment reform would be to create a single prospective paymentthat covers care from first medical contact to interhospitaltransfer, if appropriate, that would allow EMS and bothhospitals to share gains resulting from the coordination ofpatient care and that would remove the inefficiencies inherentin the payment system.24 Finally, collaborative systems maybe fostered by private or public foundations wishing to havea measurable effect on one of the leading causes of death.
LimitationsThe most significant limitation of this survey is likely relatedto our definition of a system requiring at least 2 hospitals and1 EMS agency. By giving equal weight to responses regard-less of system size, the responses of larger systems involvinglarger numbers of EMS and hospitals are underrepresented inour cumulative approach. If larger systems substantiallydiffered from smaller systems according to processes of care,resources, and barriers, our survey responses may not ade-quately reflect issues in these larger systems. A secondlimitation of our methods involves the framing of surveyquestions. Although our questions were derived from anexpert panel familiar with STEMI system issues and weincluded some open-ended queries, it is possible that signif-icant issues in implementation were not identified owing to alack of questions pertaining to such issues. A third limitationof our technique involves our reliance on voluntary partici-pation and self reporting. Biases may have been introducedby selecting respondents more likely to participate in asystem survey and by the provision of answers that were notfully reflective of the corresponding system. The 381 re-sponding systems, including 899 hospitals with PCI facilities,representing approximately 66% of the 1355 hospitals iden-tified as having PCI facilities according to the AmericanHospital Association.25 A final limitation involves our ques-tion concerning systematic use of prehospital fibrinolysis.
The 21% rate appears high compared with practical experi-ence, and we believe that some respondents possibly misin-terpreted this question to include fibrinolysis administered ata transferring hospital.
In conclusion, this survey of 381 STEMI systems broadlydescribes the organizational characteristics of collaborativeefforts by hospitals and EMS to provide timely reperfusion inthe United States. We identified a number of commonapproaches to STEMI diagnosis and coronary reperfusion,and we identified major barriers that must be overcome inorder to implement systematic care. These findings serve as abenchmark to existing systems and to regions in the processof organizing care for STEMI patients and provide a foun-dation for the ongoing implementation of Mission: Lifelineacross the country.
DisclosuresThe following authors report conflicts of interest: James G. Jollis,MD: Medtronic Foundation, Sanofi-aventis, and Philips; ChristopherB. Granger, MD: AstraZeneca, Boehringer Ingelheim, Bristol-MyersSquibb, GlaxoSmithKline, Novartis, Otsuka, Roche, Sanofi-aventis,The Medicines Company, and Astellas Pharma; and Elliott M.Antman, MD: Merck & Co., Bristol-Myers Squibb PharmaceuticalResearch Institute, Sanofi-aventis, Millennium Pharmaceuticals,AstraZenaca Pharmaceuticals, CV Therapeutics, Inotek Pharmaceu-ticals Corporation, Eli Lilly and Company, Schering-Plough Re-search Institute, Bayer Healthcare LLC, Sanofi-Synthelabo Recher-che, GlaxoSmithKline, Beckman Coulter, Inc., Biosite Incorporated,Roche Diagnostics Corporation, Pfizer, Accumetrics, and NovartisPharmaceuticals. The other authors report no conflicts.
References1. Gruppo Italiano per lo Studio della Streptochinasi nell’Infarto Miocardico
(GISSI). Effectiveness of intravenous thrombolytic treatment in acutemyocardial infarction. Gruppo Italiano per lo Studio della Streptochinasinell’Infarto Miocardico (GISSI). Lancet. 1986;1:397–402.
2. ISIS-2 (Second International Study of Infarct Survival) CollaborativeGroup. Randomised trial of intravenous streptokinase, oral aspirin, both,or neither among 17 187 cases of suspected acute myocardial infarction:ISIS-2 (Second International Study of Infarct Survival) CollaborativeGroup. Lancet. 1988;2:349–360.
3. Rathore SS, Curtis JP, Chen J, Wang Y, Nallamothu BK, Epstein AJ,Krumholz HM. Association of door-to-balloon time and mortality inpatients admitted to hospital with ST elevation myocardial infarction:national cohort study. BMJ. 2009;338:b1807.
4. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenousthrombolytic therapy for acute myocardial infarction: a quantitativereview of 23 randomised trials. Lancet. 2003;361:13–20.
5. Dalby M, Bouzamondo A, Lechat P, Montalescot G. Transfer for primaryangioplasty versus immediate thrombolysis in acute myocardial infarc-tion: a meta-analysis. Circulation. 2003;108:1809–1814.
6. Nallamothu BK, Bates ER, Herrin J, Wang Y, Bradley EH, KrumholzHM; NRMI Investigators. Times to treatment in transfer patientsundergoing primary percutaneous coronary intervention in the UnitedStates: National Registry of Myocardial Infarction (NRMI)-3/4 analysis.Circulation. 2005;111:761–767.
7. Chakrabarti A, Krumholz HM, Wang Y, Rumsfeld JS, Nallamothu BK;National Cardiovascular Data Registry. Time-to-reperfusion in patientsundergoing interhospital transfer for primary percutaneous coronaryintervention in the U.S: an analysis of 2005 and 2006 data from theNational Cardiovascular Data Registry. J Am Coll Cardiol. 2008;51:2442–2443.
8. Henry TD, Sharkey SW, Burke MN, Chavez IJ, Graham KJ, Henry CR,Lips DL, Madison JD, Menssen KM, Mooney MR, Newell MC, PedersenWR, Poulose AK, Traverse JH, Unger BT, Wang YL, Larson DM. Aregional system to provide timely access to percutaneous coronary inter-vention for ST-elevation myocardial infarction. Circulation. 2007;116:721–728.
Jollis et al Systems of Care for STEMI 5
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from

9. Le May MR, So DY, Dionne R, Glover CA, Froeschl MP, Wells GA,Davies RF, Sherrard HL, Maloney J, Marquis JF, O’Brien ER, Trickett J,Poirier P, Ryan SC, Ha A, Joseph PG, Labinaz M. A citywide protocol forprimary PCI in ST-segment elevation myocardial infarction. N EnglJ Med. 2008;358:231–240.
10. Ting HH, Rihal CS, Gersh BJ, Haro LH, Bjerke CM, Lennon RJ, Lim CC,Bresnahan JF, Jaffe AS, Holmes DR, Bell MR. Regional systems of careto optimize timeliness of reperfusion therapy for ST-elevation myocardialinfarction: the Mayo Clinic STEMI Protocol. Circulation. 2007;116:729–736.
11. Jollis JG, Roettig ML, Aluko AO, Anstrom KJ, Applegate RJ, Babb JD,Berger PB, Bohle DJ, Fletcher SM, Garvey JL, Hathaway WR, HoekstraJW, Kelly RV, Maddox WT Jr, Shiber JR, Valeri FS, Watling BA,Wilson BH, Granger CB. Implementation of a statewide system forcoronary reperfusion for ST-segment elevation myocardial infarction.JAMA. 2007;298:2371–2380.
12. Aguirre FV, Varghese JJ, Kelley MP, Lam W, Lucore CL, Gill JB, Page L,Turner L, Davis C, Mikell FL; Stat Heart Investigators. Rural interhospitaltransfer of ST-elevation myocardial infarction patients for percutaneouscoronary revascularization: the Stat Heart Program. Circulation. 2008;117:1145–1152.
13. Jacobs AK, Antman EM, Ellrodt G, Faxon DP, Gregory T, Mensah GA,Moyer P, Ornato J, Peterson ED, Sadwin L, Smith SC; American HeartAssociation’s Acute Myocardial Infarction Advisory Working Group.Recommendation to develop strategies to increase the number ofST-segment-elevation myocardial infarction patients with timely accessto primary percutaneous coronary intervention. Circulation. 2006;113:2152–2163.
14. Henry TD, Atkins JM, Cunningham MS, Francis GS, Groh WJ, HongRA, Kern KB, Larson DM, Ohman EM, Ornato JP, Peberdy MA,Rosenberg MJ, Weaver WD. ST-segment elevation myocardial infarc-tion: recommendations on triage of patients to heart attack centers: is ittime for a national policy for the treatment of ST-segment elevationmyocardial infarction? J Am Coll Cardiol. 2006;47:1339–1345.
15. Kushner FG, Hand M, Smith SC Jr, King SB III, Anderson JL, AntmanEM, Bailey SR, Bates ER, Blankenship JC, Casey DE Jr, Green LA,Hochman JS, Jacobs AK, Krumholz HM, Morrison DA, Ornato JP, PearleDL, Peterson ED, Sloan MA, Whitlow PL, Williams DO. ACC/AHAguidelines for the management of patients with ST-elevation myocardial
infarction–executive summary: a report of the American College ofCardiology/American Heart Association Task Force on PracticeGuidelines. Circulation. 2009;120:2271–2306.
16. Rokos IC, Larson DM, Henry TD, Koenig WJ, Eckstein M, French WJ,Granger CB, Roe MT. Rationale for establishing regional ST-elevationmyocardial infarction receiving center (SRC) networks. Am Heart J.2006;152:661–667.
17. Jacobs AK, Antman EM, Faxon DP, Gregory T, Solis P. Development ofsystems of care for ST-elevation myocardial infarction patients: executivesummary. Circulation. 2007;116:217–230.
18. American Heart Association. Mission: Lifeline. http://www.heart.org/HEARTORG/HealthcareResearch/MissionLifelineHomePage/Mission-Lifeline-Home-Page_UCM_305495_SubHomePage.jsp. AccessedFebruary 22, 2010.
19. Centers for Medicare & Medicaid Services and the Joint Commission,Specification Manual for National Inpatient Hospital Quality Measures.Version 3.0, March 31, 2009.
20. Hibbard JH, Stockard J, Tusler M. Hospital performance reports: impacton quality, market share, and reputation. Health Affairs. 2005;24:1150–1160.
21. Concannon TW, Kent DM, Normand SL, Newhouse JP, Griffith JL,Cohen, Beshansky JR, Wong JB, Aversano T, Selker HP. Comparativeeffectiveness of STEMI regionalization strategies. Circ Cardiovasc QualOutcomes. 2010;3:506–513.
22. Cantor WJ, Fitchett D, Borgundvaag B, Ducas J, Heffernan M, CohenEA, Morrison LJ, Langer A, Dzavik V, Mehta SR, Lazzam C, SchwartzB, Casanova A, Goodman SG. Routine early angioplasty after fibrinolysisfor acute myocardial infarction. N Engl J Med. 2009;360:2705–2718.
23. Di Mario C, Dudek D, Piscione F, Mielecki W, Savonitto S, Murena E,Dimopoulos K, Manari A, Gaspardone A, Ochala A, Zmudka K,Bolognese L, Steg PG, Flather M; CARESS-in-AMI (CombinedAbciximab RE-teplase Stent Study in Acute Myocardial Infarction)Investigators. Immediate angioplasty versus standard therapy with rescueangioplasty after thrombolysis in the Combined Abciximab REteplaseStent Study in Acute Myocardial Infarction (CARESS-in-AMI). Lancet.2008;371:559–568.
24. Solis P, Amsterdam EA, Bufalino V, Drew BJ, Jacobs AK. Developmentof systems of care for ST-elevation myocardial infarction patients: policyrecommendations. Circulation. 2007;116:e73–e76.
25. American Hospital Association. Hospital statistics. 2010 ed. Chicago.
6 Circ Cardiovasc Qual Outcomes July 2012
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from

Alice K. JacobsPeter H. Moyer, Franklin D. Pratt, Ivan C. Rokos, Anna R. Acuña, Mayme Lou Roettig and
James G. Jollis, Christopher B. Granger, Timothy D. Henry, Elliott M. Antman, Peter B. Berger,Mission: LifelineAmerican Heart Association's
Elevation Myocardial Infarction: A Report From the−Systems of Care for ST-Segment
Print ISSN: 1941-7705. Online ISSN: 1941-7713 Copyright © 2012 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Circulation: Cardiovascular Quality and Outcomes
published online May 22, 2012;Circ Cardiovasc Qual Outcomes.
http://circoutcomes.ahajournals.org/content/early/2012/05/22/CIRCOUTCOMES.111.964668World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circoutcomes.ahajournals.org/content/suppl/2012/05/22/CIRCOUTCOMES.111.964668.DC1Data Supplement (unedited) at:
http://circoutcomes.ahajournals.org//subscriptions/
at: is onlineCirculation: Cardiovascular Quality and Outcomes Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theCirculation: Cardiovascular Quality and Outcomesin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from

Appendix A. STEMI System On-line Questionnaire
STEMI SYSTEM OF CARE QUESTIONNAIRE
Are you already a part of a STEMI System of Care? Or, are you involved in an effort considering implementing a STEMI System of Care? If so, please take the time to fill out the STEMI System assessment questionnaire and let the AHA know about your initiative. This questionnaire should be filled out on behalf of your overall STEMI system, not just your individual institution. Don’t forget to search the Mission: Lifeline STEMI Systems Directory to see if your system is already registered with Mission: Lifeline. Part A: Contact Information 1. Describe the current status of your STEMI System.
System in place System being planned (The system oversight group is in place and planning has begun) System being considered (The development of the system is currently being debated)
2. Are you willing to have your STEMI System listed in the Mission: Lifeline STEMI Systems Directory?
Yes No
3. Name of STEMI System (Please indicate how you would want it to be listed in the Mission: Lifeline STEMI Systems Directory): 4. Name and contact information (Name, Address, City, State, Zip, Phone, e-mail) of individual completing the questionnaire: 5a. Are you also the system Champion?
Yes No
5b. Name and contact info for STEMI System Champion. Click here if this person is the same as person completing the questionnaire. 2a. Name, Address, City, State, Zip, Phone, e-mail

6a. Is the System Champion willing to be the contact person listed in the Mission: Lifeline STEMI Systems Directory?
Yes No
6b. Occupation of System Champion(s): (Check all that apply) Cardiologist ED physician Other physician Nurse EMT/paramedic Hospital/health care administrator Other: 6c. What organization is the System Champion(s) affiliated with? (Check all that apply): PCI hospital Non-PCI hospital EMS Other: 7. Enter the zip codes that are covered in your STEMI system of care. 8. Is there a website for your system that you want listed in the Mission: Lifeline STEMI Systems Directory? If so, please provide the website url.
Yes, the website is: ____________________________________ No
Part B: STEMI Initiative General Information (The next three questions are formatted as a grid in the survey) Indicate how the following organizations are involved, if at all, in the STEMI initiative: 9a. Partnered in the STEMI initiative. (Check all that apply) Local or state government Local American Heart Association American College of Cardiology Chapter Hospital// cardiology QI personnel Hospital administration Cath lab administration Emergency medicine Emergency Medical Services Nursing Air transport system Third party payers Other:

9b. Work with, sponsor or endorse the lead and/or governing organizations. (Check all that apply) Local or state government Local American Heart Association American College of Cardiology Chapter Hospital/ cardiology QI personnel Hospital administration Cath lab administration Emergency medicine Emergency Medical Services Nursing Air transport system Third party payers Other: 9c. Represented on the governing body that provides oversight. (Check all that apply) Local or state government Local American Heart Association American College of Cardiology Chapter Hospital/ ED/ cardiology QI personnel Hospital administration Cath lab administration Emergency medicine Emergency Medical Services Nursing Air transport system Third party payers Other: 10. Describe the system coverage, specifically EMS transport range. (Check all that apply) Rural Suburban Urban 11. Which of the following would best describe your STEMI System? (Check all that apply) Multiple hospital system Cardiology practice (academic or private) City-wide County State Cross-state regional 12. What are the specific funding sources for the STEMI System operations, including but not limited to: administration, performance feedback, training, equipment and supplies? (Select all that apply) PCI hospital

Cardiology practice Foundation State QI organization Professional society Pharmaceutical industry Third party payers Medical device industry State government agency Federal government agency Other (specify) Part C: EMS Assessment 13. Describe the specific EMS/Ambulance transport vehicles involved in your STEMI System. (Check all that apply) EMT or BLS only ambulance Paramedic or other ALS only ambulance EMT/Paramedic combination Helicopter transport 14. How many EMS programs work with your STEMI System? Ground: N= Air: N= 15. Does your STEMI System have pre-hospital 12-lead ECGs available in EMS vehicles? Yes Yes, but not in all ambulances No (skip to Q20)
16. Does your STEMI System transmit pre-hospital 12-lead information to the receiving hospital? Yes No In some ambulances yes and in some no. 17. How is the pre-hospital 12-lead ECG information transmitted and/or interpreted ? (Check all that apply) ECG read by paramedic and interpretation called by phone
ECG read by computer algorithm and called by phone
ECG transmitted to hospital by wireless or satellite phone
ECG transmitted to hospital by other device (i.e. fax)
18. Does your EMS system track and review any of the following performance measures? Check all that apply.
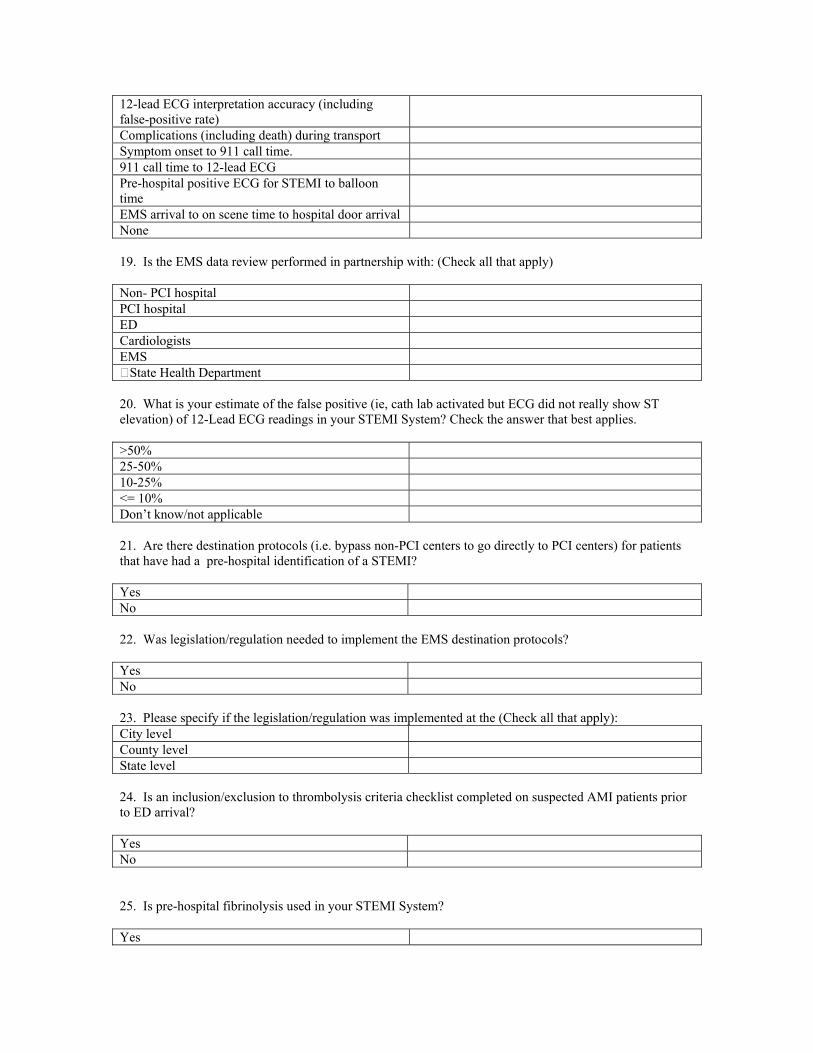
12-lead ECG interpretation accuracy (including false-positive rate)
Complications (including death) during transport Symptom onset to 911 call time. 911 call time to 12-lead ECG Pre-hospital positive ECG for STEMI to balloon time
EMS arrival to on scene time to hospital door arrival None
19. Is the EMS data review performed in partnership with: (Check all that apply) Non- PCI hospital PCI hospital ED Cardiologists EMS State Health Department 20. What is your estimate of the false positive (ie, cath lab activated but ECG did not really show ST elevation) of 12-Lead ECG readings in your STEMI System? Check the answer that best applies. >50% 25-50% 10-25% <= 10% Don’t know/not applicable 21. Are there destination protocols (i.e. bypass non-PCI centers to go directly to PCI centers) for patients that have had a pre-hospital identification of a STEMI? Yes No 22. Was legislation/regulation needed to implement the EMS destination protocols? Yes No 23. Please specify if the legislation/regulation was implemented at the (Check all that apply): City level County level State level 24. Is an inclusion/exclusion to thrombolysis criteria checklist completed on suspected AMI patients prior to ED arrival? Yes No
25. Is pre-hospital fibrinolysis used in your STEMI System? Yes

No Sometimes
26a. What type of inter-facility ambulance service is used to transport STEMI patients between non-PCI and PCI hospitals? (Check all that apply) Ground Air 911 activation is used None 26b. If ground, is a private ambulance service used? Yes No Not Applicable
26c. Is there an expected response time for the private service? Yes No 26d. If 911 is used: is 911 used as a primary protocol is 911 used as a back up if a private service cannot meet response times
Not applicable Part D: Participating Hospital System Assessment 27. What is the total number of hospitals in your system? Hospitals perform primary PCI? N= Hospitals are not PCI-capable? N=
28. Do you have a single call activation number to activate the STEMI Team/Cath Lab in your STEMI System? Yes No Not Sure
29. Please describe the pre-hospital and hospital department interaction when a patient either calls 911 or presents to a hospital. (Check all that apply) Pre-hospital/EMS Activation: EMS identifies STEMI and: Activates STEMI Team/Cath Lab Alerts ED & ED activates STEMI Team/Cath Lab (without consulting cardiologist or determining if patient has cardiologist)

Alerts ED & Cardiologist activates STEMI Team/Cath Lab
Other: 30. Hospital / ED Activation
Emergency Department staff:
Activates STEMI Team/Cath Lab (without cardiologist Consultation)
Calls Cardiologists prior to activation of STEMI team
Other: 31a. Do the hospitals in the system participate in a data registry program? Yes No 31b. In which data registry programs do the hospitals utilize? Check all that apply. ACTION Registry- GWTG Local/program specific NCDR Cath PCI Other: Other: 31c. Do hospitals in your system track and review any of the following performance measures? (Check all that apply) Hospital times:
Median arrival time for interventional cardiologist and staff at lab
Time to reperfusion: Door to balloon or door to needle
Time to reperfusion for transfer patients: 1st door to balloon
Time from door-in to door-out for transfer
Time from 1st medical contact (i.e. 1st ECG and/or EMS arrival) to reperfusion
Time from patient EMS summons to EMS arrival
% of patients eligible for reperfusion who receive it
Incidence of vascular complications Angiographic Success: % of stented lesions with angiographic success
Procedure Success: % of procedures with angiographic success and no death, MI or emergent/salvage CBG during admission
In hospital mortality 30-day risk adjusted mortality Major Adverse Cardiac Events (MACE)
32. Please categorize data feedback of performance and patient outcomes, including door to balloon times. (Check all that apply)
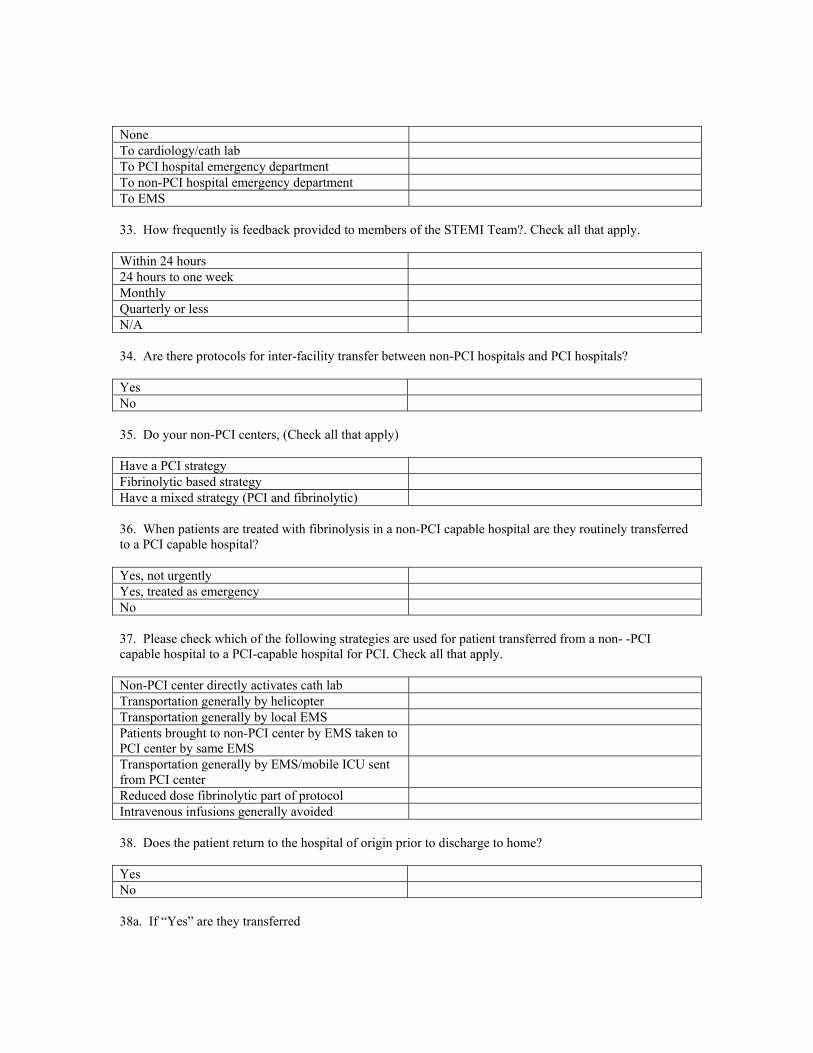
None To cardiology/cath lab To PCI hospital emergency department To non-PCI hospital emergency department To EMS 33. How frequently is feedback provided to members of the STEMI Team?. Check all that apply. Within 24 hours 24 hours to one week Monthly Quarterly or less N/A 34. Are there protocols for inter-facility transfer between non-PCI hospitals and PCI hospitals? Yes No
35. Do your non-PCI centers, (Check all that apply) Have a PCI strategy Fibrinolytic based strategy Have a mixed strategy (PCI and fibrinolytic) 36. When patients are treated with fibrinolysis in a non-PCI capable hospital are they routinely transferred to a PCI capable hospital? Yes, not urgently Yes, treated as emergency No
37. Please check which of the following strategies are used for patient transferred from a non- -PCI capable hospital to a PCI-capable hospital for PCI. Check all that apply. Non-PCI center directly activates cath lab Transportation generally by helicopter Transportation generally by local EMS Patients brought to non-PCI center by EMS taken to PCI center by same EMS
Transportation generally by EMS/mobile ICU sent from PCI center
Reduced dose fibrinolytic part of protocol Intravenous infusions generally avoided
38. Does the patient return to the hospital of origin prior to discharge to home? Yes No
38a. If “Yes” are they transferred

between 24 hrs. to 48 hrs. >48 hrs when the patient is stable 39. Do your PCI capable hospitals accept STEMI transfers regardless of hospital bed availability? Yes No 40a. Do your PCI capable hospitals include a standardized protocol for adjunctive therapy (antiplatelet, antithrombin, etc)? Yes No 40b. Do your non-PCI capable hospitals include a standardized protocol for adjunctive therapy (antiplatelet, antithrombin, etc)? Yes No

41. Does your system use the following six (6) ACC’s D2B Alliance evidence-based strategies?
1. ED physician activates the cath lab
2. One call activates the cath lab
3. Cath lab team ready in 20 – 30 minutes
4. Prompt data feedback
5. Senior management commitment
6. Team-based approach
42. Which of the following barriers has your STEMI system encountered? (Check all that apply) Bed availability Infrastructure support/funding Non-PCI hospital finances EMS/transport finances Cardiology group competition Hospital competition Lack of data collection/ feedback to systems EMS organization EMTALA regulations Receiving hospital on diversion Lack of leadership/identified champion Limited availability of interventional cardiologists Other Other Any additional comments or suggestions would be greatly appreciated.

Appendix B. Responses (Hospital identifiers removed)
STEMI System of Care Questionnaire
Date: 1/13/2010
Number of Responses Analyzed: 381
1: STEMI status: Describe the current status of your STEMI System. (Respondents could only choose a single response)
Response Chart Frequency Count
System in place 100.0% 381
System being planned (The system oversight group is in place and planning has begun)
0.0% 0
System being considered (The development of the system is currently being debated)
0.0% 0
Valid Responses 381
9a: Indicate how the following organizations are involved, if at all, in the STEMI initiative. (Partnered in the STEMI Initiative)
Yes No Total
Cardiology Count 349 8 357
Emergency medicine
Count 356 5 361
Emergency Medical Services
Count 356 4 360
Nursing Count 344 13 357
Primary care Count 153 156 309
EMS Count 353 8 361
Hospital/ED/ Count 356 4 360
Cardiology QI personnel
Count 319 24 343
Hospital administration
Count 340 11 351
Cath lab administration
Count 348 5 353

Air transport system
Count 218 108 326
Local or state government
Count 106 185 291
Local American Heart Association
Count 157 152 309
American College of Cardiology Chapter
Count 120 176 296
Third party payers Count 51 222 273
Total Count 3926 1081 5007
9b: Indicate how the following organizations are involved, if at all, in the STEMI initiative. (Work with/sponsor/endorse the lead/governing organizations)
Yes No Total
Cardiology Count 238 28 266
Emergency medicine
Count 231 30 261
Emergency Medical Services
Count 232 29 261
Nursing Count 207 43 250
Primary care Count 96 145 241
EMS Count 221 37 258
Hospital/ED/ Count 228 28 256
Cardiology QI personnel
Count 210 40 250
Hospital administration
Count 229 31 260
Cath lab administration
Count 224 34 258
Air transport system
Count 146 106 252
Local or state government
Count 91 152 243
Local American Heart Association
Count 118 126 244
American College of Cardiology Chapter
Count 86 158 244
Third party payers Count 42 194 236
Total Count 2599 1181 3780

9c: Indicate how the following organizations are involved, if at all, in the STEMI initiative. (Represented on the governing body that provides oversight)
Yes No Total
Cardiology Count 245 30 275
Emergency medicine
Count 241 31 272
Emergency Medical Services
Count 214 44 258
Nursing Count 214 43 257
Primary care Count 75 154 229
EMS Count 201 54 255
Hospital/ED/ Count 234 24 258
Cardiology QI personnel
Count 204 52 256
Hospital administration
Count 223 44 267
Cath lab administration
Count 223 40 263
Air transport system
Count 95 141 236
Local or state government
Count 48 175 223
Local American Heart Association
Count 45 182 227
American College of Cardiology Chapter
Count 34 189 223
Third party payers Count 21 204 225
Total Count 2317 1407 3724
10: Describe the system coverage, specifically EMS transport range. (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
Rural 73.4% 279
Suburban 72.9% 277
Urban 67.1% 255
Valid Responses 380
11: Which of the following would best describe your STEMI system of care? (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
Multiple hospital system or network
71.3% 271
Cardiology practice (academic or private)
41.1% 156
City-wide 50.0% 190
County 60.0% 228
State 16.3% 62
Cross-state regional 22.9% 87
Valid Responses 380
12: What are the specific funding sources for STEMI System operations, including but not limited to: administration, performance feedback, training, equipment and supplies? (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
PCI hospital 84.2% 320
Cardiology practice 23.2% 88
Foundation 18.2% 69
State QI organization 2.6% 10
Professional society 6.1% 23
Pharmaceutical industry 3.4% 13
Third party payers 11.1% 42
Medical device industry 4.2% 16
State government agency 8.7% 33
Federal government agency 5.3% 20
Other (specify) 16.6% 63

Valid Responses 380
13: Describe the specific EMS/Ambulance transport vehicles involved in your STEMI System. (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
EMT only or BLS only ambulance
30.3% 115
Paramedic or other ALS only ambulance combination
62.4% 237
EMT/Paramedic combination 82.6% 314
Helicopter transport 65.5% 249
Valid Responses 380
15: Does your STEMI System have pre-hospital 12-lead ECGs available in EMS vehicles? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 55.1% 209
Yes, but not in all ambulances 40.9% 155
No 4.0% 15
Not Answered 1
Valid Responses 379
16: Does your STEMI System transmit pre-hospital 12-lead information to the receiving hospital? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 35.0% 132
No 29.2% 110
In some ambulances yes and in some no
35.8% 135
Not Answered 3

Valid Responses 377
17: How is the pre-hospital 12-lead ECG information transmitted and/or interpreted? (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
ECG read by paramedic and interpretation called by phone
62.5% 170
ECG read by computer algorithm and called by phone
33.8% 92
ECG transmitted to hospital by wireless or satellite phone
67.6% 184
ECG transmitted to hospital by other device (i.e. fax)
48.2% 131
Valid Responses 272
Total Responses 272
18: Does your EMS system track and review any of the following performance measures? (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
12-lead ECG interpretation accuracy (including false-positive rate)
64.2% 244
Complications (including death) during transport
64.5% 245
Symptom onset to 911 call time 45.3% 172
911 call time to 12-lead ECG 48.2% 183
Pre-hospital positive ECG for STEMI to balloon time
65.0% 247
EMS arrival to on scene time to hospital door arrival
71.8% 273
Valid Responses 380
19: Is the EMS data review performed in partnership with: (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count

Non-PCI hospital 29.7% 113
PCI hospital 77.1% 293
ED 67.4% 256
Cardiologists 55.0% 209
EMS 73.9% 281
State Health Department 5.5% 21
Valid Responses 380
20: What is your estimate of the false positive (i.e. cath lab activated but ECG did not really show ST elevation) of 12-lead ECG readings in your STEMI System? (Select the answer that best applies.) (Respondents could only choose a single response)
Response Chart Frequency Count
Greater than 50% 0.8% 3
25-50% 3.8% 14
10-24% 21.2% 79
Less than 10% 54.3% 202
Don't know/not applicable 19.9% 74
Not Answered 8
Valid Responses 372
21: Are there destination protocols (i.e. bypass non-PCI centers to go directly to PCI centers) for patients that have had a pre-hospital identification of a STEMI? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 60.9% 227
No 39.1% 146
Not Answered 7
Valid Responses 373

22: Was legislation/regulation needed to implement the EMS destination protocols? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 18.1% 41
No 81.9% 186
Not Answered 19
Valid Responses 227
23: Please specify if the legislation/regulation was implemented at the: (select all that apply) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
City level 18.2% 10
County level 40.0% 22
State level 40.0% 22
Valid Responses 55
24: Is an inclusion/exclusion criteria checklist completed on suspected AMI patients prior to ED arrival? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 37.9% 141
No 62.1% 231
Not Answered 8
Valid Responses 372
25: Is pre-hospital fibrinolysis used in your STEMI System? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 6.6% 25

No 79.6% 301
Sometimes 13.8% 52
Not Answered 2
Valid Responses 378
26a: What type of inter-facility ambulance service is used to transport STEMI patients between non-PCI and PCI hospitals? (Check all that apply) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
Ground 92.1% 350
Air 67.9% 258
911 activation is used 33.4% 127
Valid Responses 380
26b: If ground, is a private ambulance service used? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 54.1% 196
No 37.3% 135
Not Applicable 8.6% 31
Not Answered 18
Valid Responses 362
26c: Is there an expected response time for the private service? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 73.7% 146
No 26.3% 52
Not Answered 29
Valid Responses 198
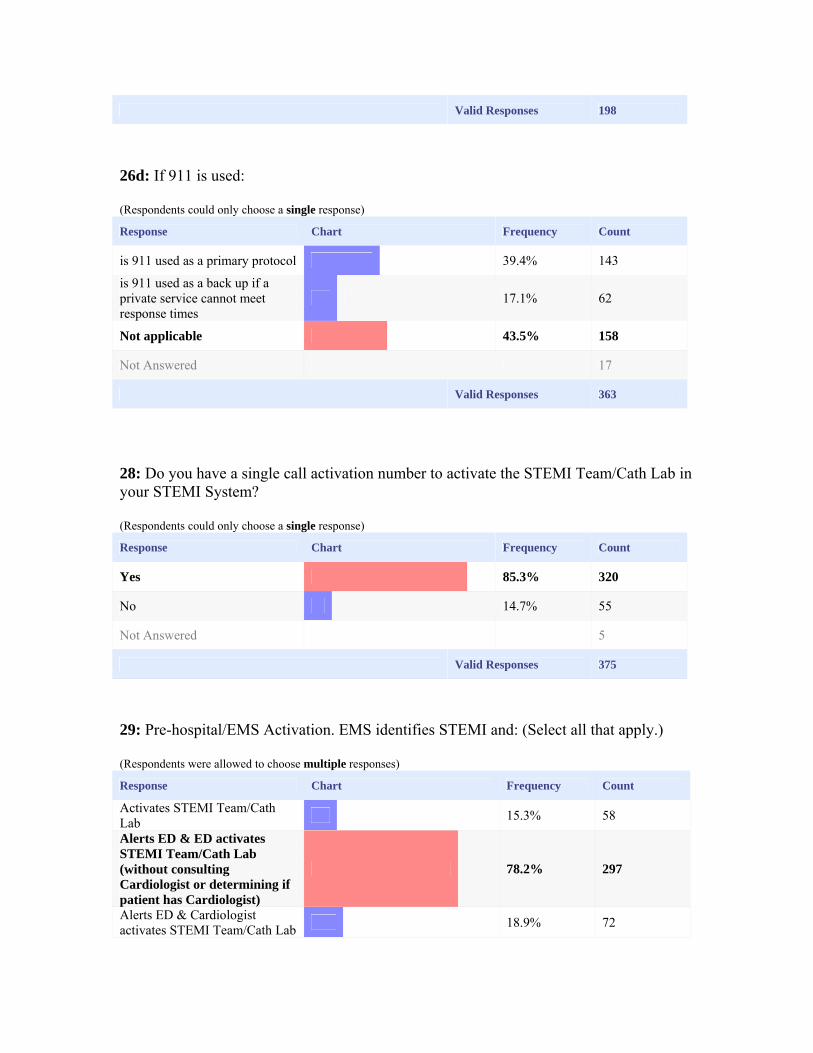
26d: If 911 is used: (Respondents could only choose a single response)
Response Chart Frequency Count
is 911 used as a primary protocol 39.4% 143
is 911 used as a back up if a private service cannot meet response times
17.1% 62
Not applicable 43.5% 158
Not Answered 17
Valid Responses 363
28: Do you have a single call activation number to activate the STEMI Team/Cath Lab in your STEMI System? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 85.3% 320
No 14.7% 55
Not Answered 5
Valid Responses 375
29: Pre-hospital/EMS Activation. EMS identifies STEMI and: (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
Activates STEMI Team/Cath Lab
15.3% 58
Alerts ED & ED activates STEMI Team/Cath Lab (without consulting Cardiologist or determining if patient has Cardiologist)
78.2% 297
Alerts ED & Cardiologist activates STEMI Team/Cath Lab
18.9% 72

Other (specify) 6.6% 25
Valid Responses 380
30: Hospital/ED Activation: Emergency Department staff: (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
Activates STEMI Team/Cath Lab (without Cardiologist consultation)
83.2% 316
Calls Cardiologist prior to activation of STEMI team
21.3% 81
Other (specify) 5.0% 19
Valid Responses 380
31a: Do your hospitals in the system participate in a data registry program? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 83.8% 311
No 16.2% 60
Not Answered 9
Valid Responses 371
31b: Which data registry programs do the hospitals utilize? (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
ACTION 34.8% 114
GWTG-CAD 27.1% 89
Local/program specific 22.0% 72
NCDR Cath PCI 61.3% 201
Other (specify) 30.5% 100
Other (specify) 7.3% 24

Valid Responses 328
31c: Do hospitals in your system track and review any of the following performance measures? (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
(Hospital time) Median arrival time for interventional cardiologist and staff at lab
77.6% 295
(Hospital time) Time to reperfusion: door to balloon or door to needle
94.5% 359
(Hospital time) Time to reperfusion for transfer patients: 1st door to balloon
76.6% 291
(Hospital time) Time from door-in to door-out for transfer
56.1% 213
Time from 1st medical contact (i.e. 1st ECG and/or EMS arrival) to reperfusion
67.6% 257
Time from patient EMS summons to EMS arrival
39.5% 150
% of patients eligible for reperfusion who receive it
47.9% 182
Incidence of vascular complications
74.7% 284
Angiographic success: % of stented lesions with angiographic success
70.3% 267
Valid Responses 380
32: Please categorize data feedback of performance and patient outcomes, including door to balloon times. (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
None 2.6% 10
To cardiology/cath lab 86.3% 328
To PCI hospital emergency department
83.7% 318
To non-PCI hospital emergency department
46.1% 175
To EMS 75.0% 285

Valid Responses 380
33: How frequently is feedback provided to members of the STEMI Team? (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
Within 24 hours 35.0% 133
24 hours to one week 45.5% 173
Monthly 35.5% 135
Quarterly or less 21.6% 82
Not applicable 2.9% 11
Valid Responses 380
34: Are there protocols for inter-facility transfer between non-PCI hospitals and PCI hospitals? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 71.8% 255
No 28.2% 100
Not Answered 25
Valid Responses 355
35: Do your non-PCI centers: (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
Have a PCI strategy 35.5% 135
Fibrinolytic based strategy 18.2% 69
Have a mixed strategy (PCI and fibrinolytic)
52.1% 198
Valid Responses 380

36: When patients are treated with fibrinolysis in a non-PCI capable hospital, are they routinely transferred to a PCI-capable hospital? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes, not urgently 11.1% 35
Yes, treated as emergency 81.3% 256
No 7.6% 24
Not Answered 65
Valid Responses 315
37: Please check which of the following strategies are used for patients transferred from a non-PCI capable hospital to a PCI-capable hospital for PCI. (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count
Non-PCI center directly activates cath lab
31.8% 121
Transportation generally by helicopter
44.2% 168
Transportation generally by local EMS
63.4% 241
Patients brought to non-PCI center by EMS taken to PCI center by same EMS
35.8% 136
Transportation generally by EMS/mobile ICU sent from PCI center
12.6% 48
Reduced dose fibrinolytic part of protocol
6.6% 25
Intravenous infusions generally avoided
19.2% 73
Valid Responses 380
38: Does the patient return to the hospital of origin prior to discharge to home? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 2.1% 7

No 97.9% 326
Not Answered 47
Valid Responses 333
38a: Are they transferred: (Respondents could only choose a single response)
Response Chart Frequency Count
Between 24 hours to 48 hours 36.4% 4
More than 48 hours 9.1% 1
When the patient is stable 54.5% 6
Not Answered 46
Valid Responses 11
39: Do your PCI-capable hospitals accept STEMI transfers regardless of hospital bed availability? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 96.9% 346
No 3.1% 11
Not Answered 23
Valid Responses 357
40a: Do your PCI-capable hospitals include a standardized protocol for adjunctive therapy (antiplatelet, antithrombin, etc.)? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 92.4% 326
No 7.6% 27
Not Answered 27

Valid Responses 353
40b: Do your non-PCI capable hospitals include a standardized protocol for adjunctive therapy (antiplatelet, antithrombin, etc.)? (Respondents could only choose a single response)
Response Chart Frequency Count
Yes 77.5% 244
No 22.5% 71
Not Answered 65
Valid Responses 315
41: Does your system use the following six (6) ACC's D2B Alliance evidence-based strategies?
Yes No Partially Total
ED physician activates the cath lab
Count 318 18 30 366
One call activates the cath lab
Count 335 11 18 364
Cath lab team ready in 20-30 minutes
Count 352 4 10 366
Prompt data feedback
Count 322 5 33 360
Senior management commitment
Count 354 2 6 362
Team-based approach
Count 360 2 1 363
Total Count 2041 42 98 2181
42: Which of the following barriers has your STEMI system encountered? (Select all that apply.) (Respondents were allowed to choose multiple responses)
Response Chart Frequency Count

Bed availability 15.5% 59
Infrastructure support/funding 15.5% 59
Non-PCI hospital finances 10.3% 39
EMS/transport finances 26.1% 99
Cardiology group competition 21.3% 81
Hospital competition 36.6% 139
Lack of data collection/feedback to systems
17.9% 68
EMS organization 13.9% 53
EMTALA regulations 6.6% 25
Receiving hospital on diversion 5.8% 22
Lack of leadership/identified champion
2.9% 11
Limited availability of interventional cardiologists
6.3% 24
Other (specify) 15.3% 58
Other (specify) 2.4% 9
Valid Responses 380
Other responses: 7: What are the specific funding sources for STEMI System operations, including but not limited to: administration, performance feedback, training, equipment and supplies? (Select all that apply.) Response County government County government agency public parish hospital Local (County) Gov. Agency data coordinating center pro bono County government donations, operating expenses Cardiac PHO Grant, initially Fire Based EMS City and County Taxes Not sure how to answer, as there is no funding for the System per se County EMS; EMS providers local government agency Local Government

County, Private ambulance EMS County Health Services, EMS Agency County EMS Municipality and Grants non-PCI hospital County EMS Agency, local fire departments and private ambulance providers (see above) EMS Municipality of Anchorage County Government Local Government Fire / EMS Departments City govt None city government EMS System, Fire Department Our EMS ESD local government Local Government RACE Cooperative agreement RACE grant Hospital Hospital District County Government, AHA EMS Agency Individual Hospitals JCAHO (core measures), Society of Chest Pain Centers none grants donations, operating expenses Hospital EMS Agency County EMS, Berkshire Medical Center PCI referral center non-PCI facilities, regional EMS providers EMS private donations county budget grant funded EMS 25: Pre-hospital/EMS Activation. EMS identifies STEMI and: (Select all that apply.) Response Hospital determines policy alert ED only notification is in house ED varies between PCI facilities
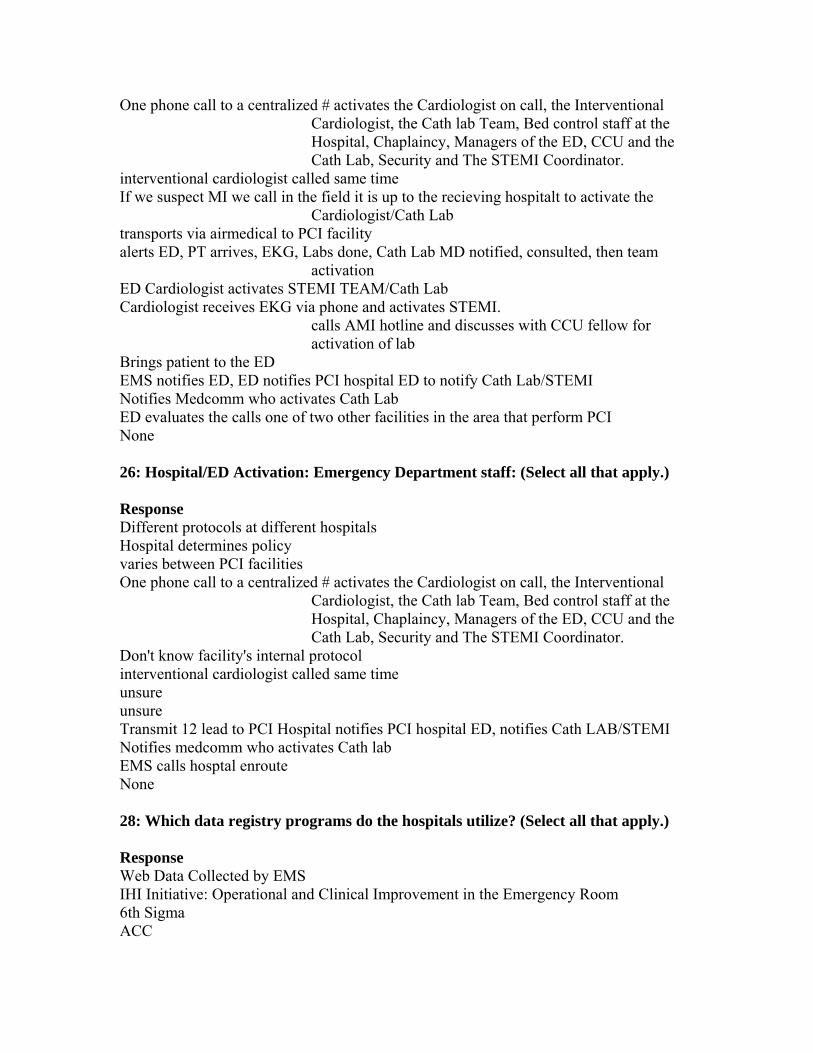
One phone call to a centralized # activates the Cardiologist on call, the Interventional Cardiologist, the Cath lab Team, Bed control staff at the Hospital, Chaplaincy, Managers of the ED, CCU and the Cath Lab, Security and The STEMI Coordinator.
interventional cardiologist called same time If we suspect MI we call in the field it is up to the recieving hospitalt to activate the
Cardiologist/Cath Lab transports via airmedical to PCI facility alerts ED, PT arrives, EKG, Labs done, Cath Lab MD notified, consulted, then team
activation ED Cardiologist activates STEMI TEAM/Cath Lab Cardiologist receives EKG via phone and activates STEMI.
calls AMI hotline and discusses with CCU fellow for activation of lab
Brings patient to the ED EMS notifies ED, ED notifies PCI hospital ED to notify Cath Lab/STEMI Notifies Medcomm who activates Cath Lab ED evaluates the calls one of two other facilities in the area that perform PCI None 26: Hospital/ED Activation: Emergency Department staff: (Select all that apply.) Response Different protocols at different hospitals Hospital determines policy varies between PCI facilities One phone call to a centralized # activates the Cardiologist on call, the Interventional
Cardiologist, the Cath lab Team, Bed control staff at the Hospital, Chaplaincy, Managers of the ED, CCU and the Cath Lab, Security and The STEMI Coordinator.
Don't know facility's internal protocol interventional cardiologist called same time unsure unsure Transmit 12 lead to PCI Hospital notifies PCI hospital ED, notifies Cath LAB/STEMI Notifies medcomm who activates Cath lab EMS calls hosptal enroute None 28: Which data registry programs do the hospitals utilize? (Select all that apply.) Response Web Data Collected by EMS IHI Initiative: Operational and Clinical Improvement in the Emergency Room 6th Sigma ACC
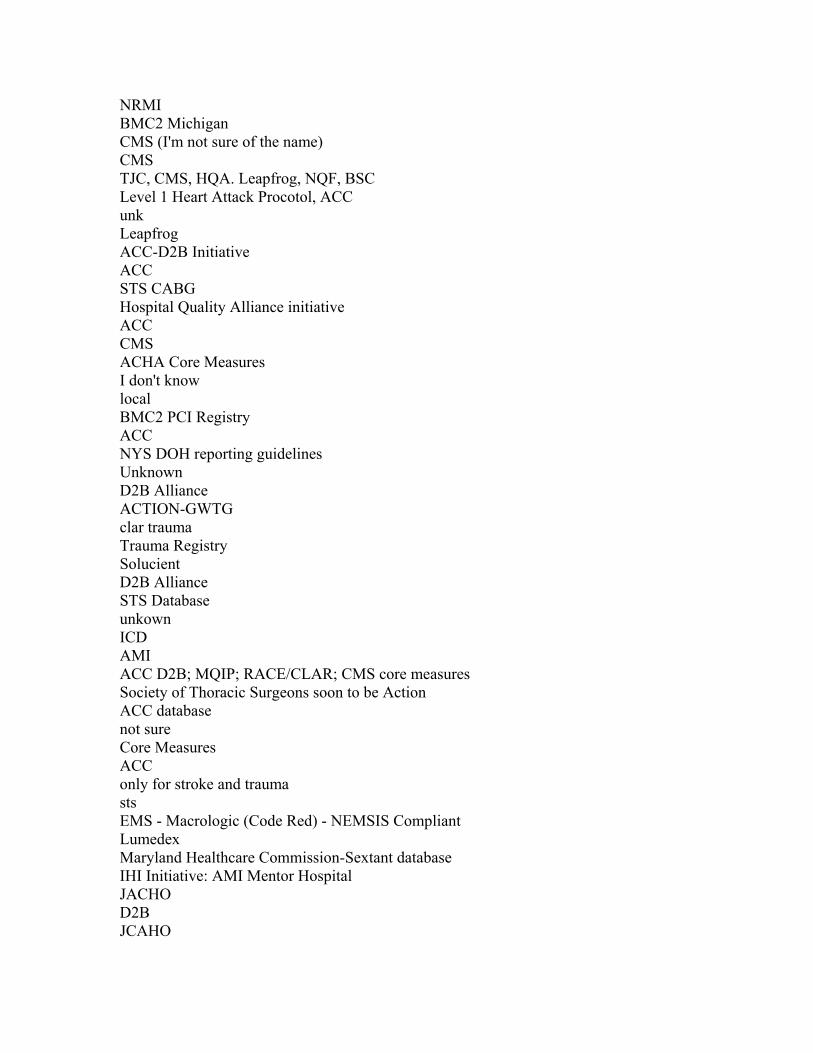
NRMI BMC2 Michigan CMS (I'm not sure of the name) CMS TJC, CMS, HQA. Leapfrog, NQF, BSC Level 1 Heart Attack Procotol, ACC unk Leapfrog ACC-D2B Initiative ACC STS CABG Hospital Quality Alliance initiative ACC CMS ACHA Core Measures I don't know local BMC2 PCI Registry ACC NYS DOH reporting guidelines Unknown D2B Alliance ACTION-GWTG clar trauma Trauma Registry Solucient D2B Alliance STS Database unkown ICD AMI ACC D2B; MQIP; RACE/CLAR; CMS core measures Society of Thoracic Surgeons soon to be Action ACC database not sure Core Measures ACC only for stroke and trauma sts EMS - Macrologic (Code Red) - NEMSIS Compliant Lumedex Maryland Healthcare Commission-Sextant database IHI Initiative: AMI Mentor Hospital JACHO D2B JCAHO

Pinpoint Compliance for Quality Measures Centers for Medicare and Medicaid/Joint Commission data reporting JCAHO HQI - AMI (CMS) STS WCHQ – state CMS 42: Which of the following barriers has your STEMI system encountered? (Select all that apply.) Response False Positive Rate non-interventional cardiologist assessment EKG transmission We encountered many barriers and worked through them at a local level Cardiologist are not interested in doing primary PCI for patients at non PCI center If adverse weather conditions preclude flying, ground transport is arranged time and availability of staff at non PCI centers technology linkage between many independent organizations physician protocol compliance some reluctance from one cardiology group to standardize one-call activation Multiple
STEMI's at the same time Just getting started working wit the local PCI hospital, the previous cardiologist did not want to work with EMS. Consistency in data collection/feedback to systems Enough people dedicated to data collection ED staff buy in vendor ability to provide equipment for transmissions Labor individual cardiologist and group practice patterns EMS availability throughout area difficulty finding transport, Lack of EMS education to recognize STEMI State regulations regarding EMS hospital destinations Need for Atomic Clocks patients with cardiologists at different centers Education of EMS, local hospitals Lack of resources to provide consistent feedback and loop closure Weather delays Non-PCI Hospital bypasses the closest PCI hospital to stay within their system. This
results in delays for the patient EMS transportatin from non PCI facilities lenghty call backs by receiving PCI capable Hospital none of the above EKG transmission Rural area
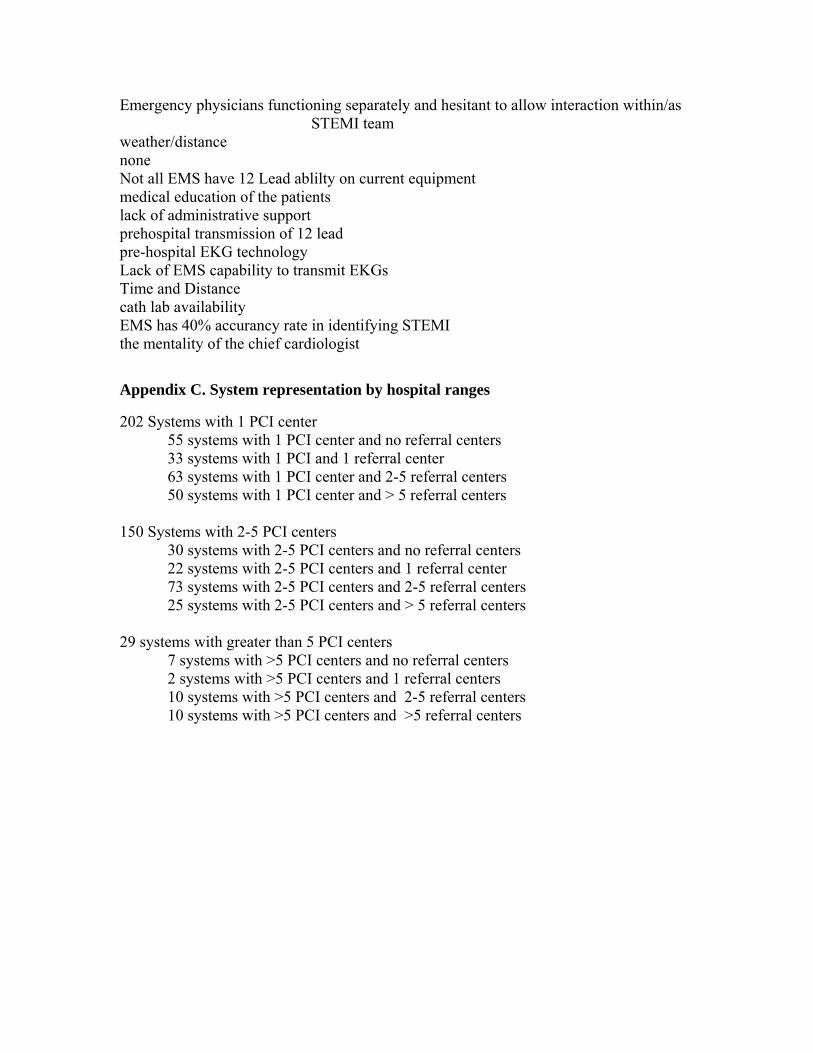
Emergency physicians functioning separately and hesitant to allow interaction within/as STEMI team
weather/distance none Not all EMS have 12 Lead ablilty on current equipment medical education of the patients lack of administrative support prehospital transmission of 12 lead pre-hospital EKG technology Lack of EMS capability to transmit EKGs Time and Distance cath lab availability EMS has 40% accurancy rate in identifying STEMI the mentality of the chief cardiologist
Appendix C. System representation by hospital ranges
202 Systems with 1 PCI center 55 systems with 1 PCI center and no referral centers 33 systems with 1 PCI and 1 referral center 63 systems with 1 PCI center and 2-5 referral centers 50 systems with 1 PCI center and > 5 referral centers 150 Systems with 2-5 PCI centers 30 systems with 2-5 PCI centers and no referral centers 22 systems with 2-5 PCI centers and 1 referral center 73 systems with 2-5 PCI centers and 2-5 referral centers 25 systems with 2-5 PCI centers and > 5 referral centers 29 systems with greater than 5 PCI centers 7 systems with >5 PCI centers and no referral centers 2 systems with >5 PCI centers and 1 referral centers 10 systems with >5 PCI centers and 2-5 referral centers 10 systems with >5 PCI centers and >5 referral centers