systemic vasculitis 2 dr.. overview ► wegener’s granulomatosis epidemiology clinical features ...
TRANSCRIPT

Systemic vasculitis 2Systemic vasculitis 2
Dr. Dr.

OverviewOverview
►Wegener’s granulomatosisWegener’s granulomatosis EpidemiologyEpidemiology Clinical featuresClinical features PathogenesisPathogenesis DiagnosisDiagnosis TreatmentTreatment PrognosisPrognosis
Wegener’s Wegener’s GranulomatosisGranulomatosis
Wegener’s GranulomatosisWegener’s Granulomatosis
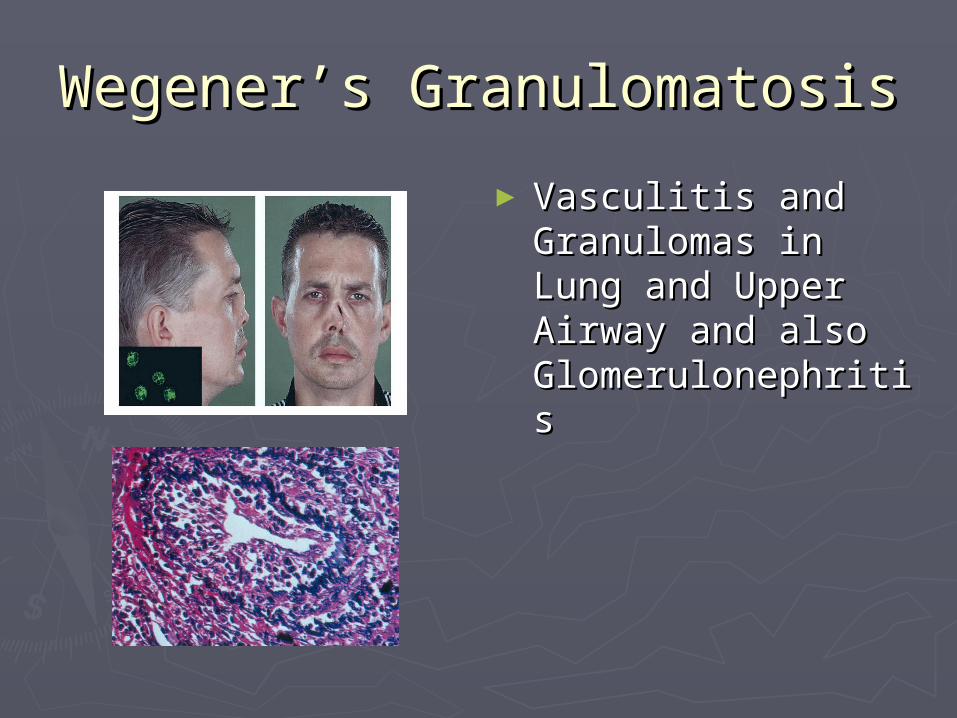
► Vasculitis and Vasculitis and Granulomas in Lung Granulomas in Lung and Upper Airway and Upper Airway and also and also GlomerulonephritisGlomerulonephritis

History of Wegener’sHistory of Wegener’s► In 1931In 1931
Two patients died from prolonged sepsis with Two patients died from prolonged sepsis with inflammation of blood vessels scattered throughout inflammation of blood vessels scattered throughout the bodythe body
► In 1936In 1936 Wegener first described a distinct syndrome in Wegener first described a distinct syndrome in
three patients found to have necrotizing three patients found to have necrotizing granulomas involving the upper and lower granulomas involving the upper and lower respiratory tractrespiratory tract
► In 1954In 1954 Seven more patients described, resulting in Seven more patients described, resulting in
definate criteria definate criteria
Wegener’s granulomatosisWegener’s granulomatosis
►Epidemiology:Epidemiology: Prevalence in US estimated at 3 per Prevalence in US estimated at 3 per
100,000100,000 Male : Female = 1 : 1Male : Female = 1 : 1 80-97% are Caucasian80-97% are Caucasian Mean age at diagnosis: 41-56Mean age at diagnosis: 41-56
DefinitionsDefinitions
►Wegener’s granulomatosis is a Wegener’s granulomatosis is a systemic vasculitis of the medium systemic vasculitis of the medium and small arteries, as well as venules, and small arteries, as well as venules, arterioles and occasionally large arterioles and occasionally large arteriesarteries
► ““Classic” Wegener’s primarily Classic” Wegener’s primarily involves the upper and lower involves the upper and lower respiratory tracts and the kidneysrespiratory tracts and the kidneys
Definitions Definitions (Contd)(Contd)
► ““Limited” form have clinical findings Limited” form have clinical findings isolated to the respiratory tract- can isolated to the respiratory tract- can occur in ¼ of cases, although 80% occur in ¼ of cases, although 80% may go on to develop may go on to develop glomerulonephritisglomerulonephritis
Specifically, pts with limited disease are Specifically, pts with limited disease are younger at disease onset, and more younger at disease onset, and more likely to be womenlikely to be women

The ControversyThe Controversy
►Wegener’s vs PR3-ANCA vasculitisWegener’s vs PR3-ANCA vasculitis Lancet, 22 April 2006Lancet, 22 April 2006 Suggestion that using Wegener’s name Suggestion that using Wegener’s name
“needs balanced discussion within the “needs balanced discussion within the scientific community”scientific community”
Reiter's syndrome-Reiter's syndrome- reactive arthritis reactive arthritis

The Problem with ChangingThe Problem with Changing
►Multiple ANCA+ diseases:Multiple ANCA+ diseases: microscopic polyangiitis (MPA)microscopic polyangiitis (MPA) "renal-limited" vasculitis "renal-limited" vasculitis (pauci-immune (pauci-immune
glomerulonephritis without evidence of extrarenal disease)glomerulonephritis without evidence of extrarenal disease)
Churg-Strauss syndrome (CSS)Churg-Strauss syndrome (CSS) Drug-induced vasculitisDrug-induced vasculitis Goodpasture’sGoodpasture’s Rheumatic disordersRheumatic disorders Autoimmune GI disordersAutoimmune GI disorders CFCF
►Diagnostic Criteria primarily clinicalDiagnostic Criteria primarily clinical

Criteria for ClassificationCriteria for Classification► Nasal or oral inflammationNasal or oral inflammation
Development of painful or painless oral ulcers or purulent or Development of painful or painless oral ulcers or purulent or bloody nasal dischargebloody nasal discharge
► Abnormal chest radiographAbnormal chest radiograph Chest radiograph showing the presence of nodules, fixed Chest radiograph showing the presence of nodules, fixed
infiltrates, or cavitiesinfiltrates, or cavities
► Abnormal Urinary sedimentAbnormal Urinary sediment Microhematuria (>5 red blood cells per high power field) or red Microhematuria (>5 red blood cells per high power field) or red
cell casts in urine sediment cell casts in urine sediment
► Granulomatous inflammation on biopsyGranulomatous inflammation on biopsy Histologic changes showing granulomatous inflammation within Histologic changes showing granulomatous inflammation within
the wall of an artery or in the perivascular or extravascular area the wall of an artery or in the perivascular or extravascular area (artery or arteriole)(artery or arteriole)
* For purposes of classification, a patient shall be said to have Wegener's granulomatosis if at least 2 of these * For purposes of classification, a patient shall be said to have Wegener's granulomatosis if at least 2 of these 4 criteria are present. The presence of any 2 or more criteria yields a sensitivity of 88.2% and a 4 criteria are present. The presence of any 2 or more criteria yields a sensitivity of 88.2% and a specificity of 92.0%specificity of 92.0%

Classic SymptomsClassic Symptoms
►Upper respiratory tract Upper respiratory tract sinuses sinuses NoseNose earsears tracheatrachea
►LungsLungs►KidneysKidneys
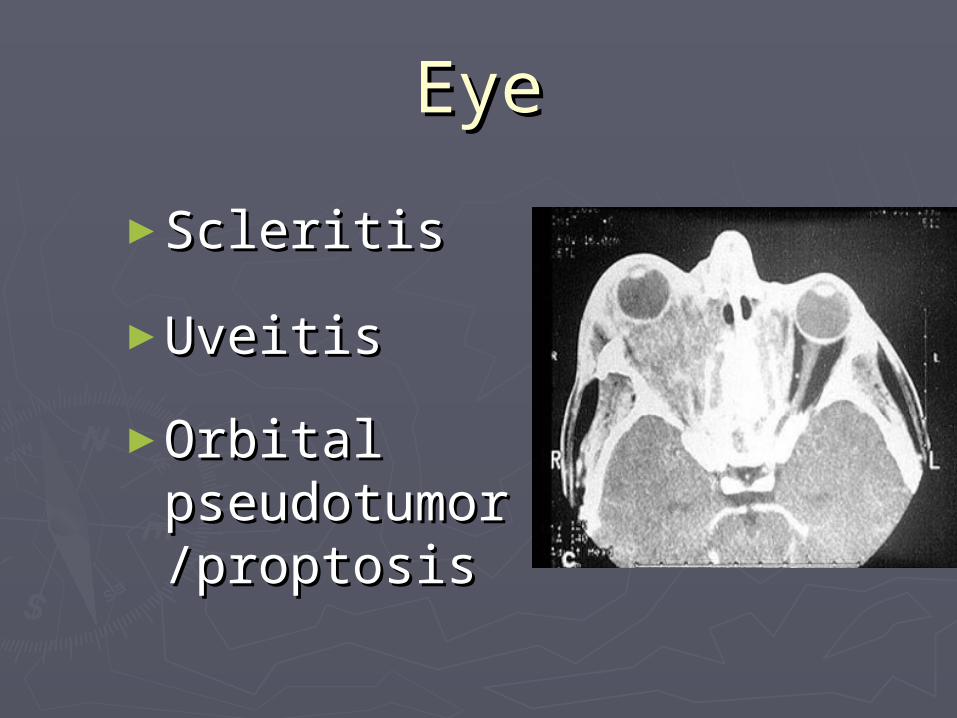
EyeEye
►ScleritisScleritis
►UveitisUveitis
►Orbital Orbital pseudotumopseudotumor /proptosisr /proptosis
Upper Respiratory TractUpper Respiratory TractEarEar
►Ear infections that are slow Ear infections that are slow to resolveto resolve
►Recurrent otitis mediaRecurrent otitis media►Decrease in hearingDecrease in hearing

Upper Respiratory TractUpper Respiratory Tract NoseNose
►Nasal crusting Nasal crusting ►Frequent Frequent
nosebleeds nosebleeds ►Erosion and Erosion and
perforation of perforation of the nasal the nasal septum.septum. The bridge of The bridge of the nose can collapse resulting the nose can collapse resulting
in a “saddle–nose deformity”.in a “saddle–nose deformity”.

Upper Respiratory TractUpper Respiratory Tract Sinuses/TracheaSinuses/Trachea
► SinusesSinuses Chronic sinus Chronic sinus
inflammationinflammation
► TracheaTrachea subglottic stenosissubglottic stenosis
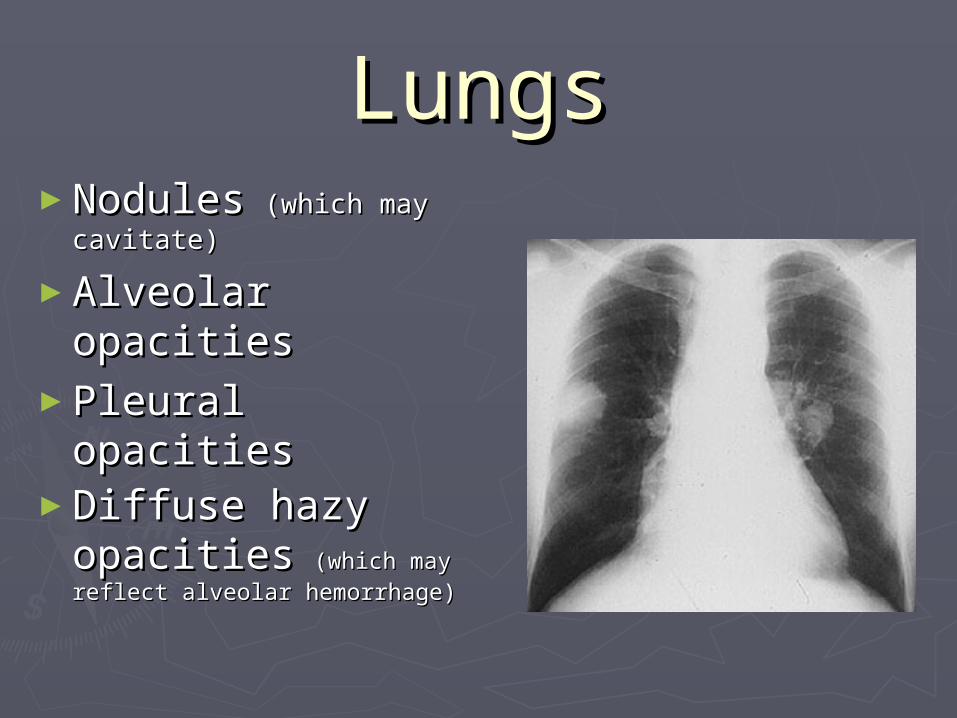
LungsLungs►NodulesNodules (which may (which may
cavitate) cavitate)
►Alveolar Alveolar opacities opacities
►Pleural opacities Pleural opacities ►Diffuse hazy Diffuse hazy
opacitiesopacities (which may (which may reflect alveolar hemorrhage) reflect alveolar hemorrhage)
KidneyKidney►Glomerulonephritis w/ associated Glomerulonephritis w/ associated
hematuria and proteinuriahematuria and proteinuria►Can lead to renal failure if not treated Can lead to renal failure if not treated
aggressively aggressively ►Renal masses (rare)Renal masses (rare)►Active urine sediment: red blood cell Active urine sediment: red blood cell
castscasts

RBC castsRBC casts

SkinSkin► ““palpable purpura” palpable purpura”
most commonmost common
► Raynaud’s Raynaud’s phenomenon—due phenomenon—due to inadequate blood to inadequate blood flow to fingers and flow to fingers and toestoes
► UlcersUlcers
MiscellaneousMiscellaneous
► JointsJointsArthritis can occur, with joint swelling and painArthritis can occur, with joint swelling and pain
►NervesNervesPeripheral nerve involvement leads to Peripheral nerve involvement leads to numbness, tingling, shooting pains in the numbness, tingling, shooting pains in the extremities, and sometimes to weakness in a extremities, and sometimes to weakness in a foot, hand, arm, or leg foot, hand, arm, or leg
►Meninges Meninges ► Prostate glandProstate gland►Genito–urinary tractGenito–urinary tract► Constitutional symptoms of fatigue, low–grade Constitutional symptoms of fatigue, low–grade
fever, and weight lossfever, and weight loss

Incidence of symptomsIncidence of symptoms
SymptomSymptom At OnsetAt Onset TotalTotal► ENT ENT 75%75% 95%95%► Lung Lung 50 50 8585► Joints Joints 30 30 7070► Fever Fever 25 25 5050► Kidney Kidney 20 20 7575► Cough Cough 20 20 5050► Eye Eye 15 15 5050► Skin Skin 15 15 4545► Weight Loss Weight Loss 10 10 3535► Nervous System (Central/Peripheral) 0 Nervous System (Central/Peripheral) 0 10/15 10/15
One-third of patients may be without symptoms at onset of One-third of patients may be without symptoms at onset of diseasedisease

Wegener’s continued. . .Wegener’s continued. . .
► Renal involvement is manifested by acute Renal involvement is manifested by acute renal failure with red cells, red cell and other renal failure with red cells, red cell and other casts , and proteinuriacasts , and proteinuria
► Pts with microscopic polyangitis have a renal Pts with microscopic polyangitis have a renal lesion that is essentially indistinguishable from lesion that is essentially indistinguishable from that of pts with classic Wegener’s, the that of pts with classic Wegener’s, the principle difference is the absence of principle difference is the absence of granulomatosis inflammation, although some granulomatosis inflammation, although some experts consider the presence of any experts consider the presence of any significant upper respiratory tract involvement significant upper respiratory tract involvement to be indicative of Wegener’sto be indicative of Wegener’s

In addition to pulmonary and In addition to pulmonary and renal…renal…
►Upper and lower airways, including Upper and lower airways, including subglottic region or tracheasubglottic region or trachea
► Joints (myalgias, arthralgias, arthritis)Joints (myalgias, arthralgias, arthritis)
►Eyes (conjuctivitis, corneal ulceration, Eyes (conjuctivitis, corneal ulceration, episcleritis/scleritis, optic neuropathy, episcleritis/scleritis, optic neuropathy, nasolacrimal duct obstruction…)nasolacrimal duct obstruction…)
In addition to pulmonary and In addition to pulmonary and renal… renal… (Contd)(Contd)
►Skin (hemorrhagic lesions, Skin (hemorrhagic lesions, palpable purpura)palpable purpura)
►Nervous system(cranial nerve Nervous system(cranial nerve abnormalities)abnormalities)
►GI tract/Heart, lower GUGI tract/Heart, lower GU

Wegener’s GranulomatosisWegener’s Granulomatosis
►About 50% have no About 50% have no lung involvement at lung involvement at presentation. presentation.
• Lung involvement:Lung involvement: InfiltratesInfiltrates NodulesNodules HemoptysisHemoptysis PleuritisPleuritis
• 33% with lung 33% with lung involvement are involvement are asymptomatic.asymptomatic.
• About 80% have no About 80% have no renal involvement at renal involvement at presentation.presentation. Klippel, 1998
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
ENT Lung Kidney
At InitialPresentation
ThroughoutDisease Course
PathogenesisPathogenesisRisk factors and inciting eventsRisk factors and inciting events
►Exact events obscureExact events obscure Infectious—staph?Infectious—staph? Genetic Genetic
►single nucleotide polymorphism in a gene single nucleotide polymorphism in a gene encoding a protein tyrosine phosphatase (PTPN22)encoding a protein tyrosine phosphatase (PTPN22)
►AAT deficiencyAAT deficiency Environmental—inhalational? Environmental—inhalational?
►SilicaSilica►lead lead ►mercurymercury

PathogenesisPathogenesisANCAANCA
►ANCAs may be not only markers for ANCAs may be not only markers for Wegener's granulomatosis and related Wegener's granulomatosis and related disorders, but they may also be actors disorders, but they may also be actors in pathogenesisin pathogenesis
►Neutrophils exposed to cytokines such Neutrophils exposed to cytokines such as TNF, express PR3 & MPO (the as TNF, express PR3 & MPO (the targets for ANCAs)targets for ANCAs) Adding ANCAs to these cytokine-primed Adding ANCAs to these cytokine-primed
neutrophils causes them to generate neutrophils causes them to generate oxygen radicals and release enzymes oxygen radicals and release enzymes capable of damaging blood vesselscapable of damaging blood vessels

Pathogenesis Pathogenesis (Contd)(Contd)
►““Priming” of NeutrophilsPriming” of Neutrophils Exposing PR3 and MPO epitopesExposing PR3 and MPO epitopes
►ANCA bindingANCA binding►Degranulation/ROS Degranulation/ROS
production/neutrophil-endothelial cell production/neutrophil-endothelial cell interactioninteraction
► Increased ANCA = Increased Increased ANCA = Increased degranulation ratedegranulation rate

Pathogenesis Pathogenesis (Contd)(Contd)
► Production of ANCA (anti-neutrophil cytoplasmic Production of ANCA (anti-neutrophil cytoplasmic antibodies) is one of the hallmarks of WG and antibodies) is one of the hallmarks of WG and related forms of vasculitis(Churg-strauss, MPA, related forms of vasculitis(Churg-strauss, MPA, pauciimmune glomerulonephritis, drug –induced).pauciimmune glomerulonephritis, drug –induced).
► ANCA are directed against antigens present within ANCA are directed against antigens present within the primary granules of neutrophils and monocytes, the primary granules of neutrophils and monocytes, and thus produce tissue damage via interactions and thus produce tissue damage via interactions with primed neutrophils and endothelial calls.with primed neutrophils and endothelial calls.
► ~90% of pts with active generalized WG are ANCA ~90% of pts with active generalized WG are ANCA positive, but some do not have ANCA, and those positive, but some do not have ANCA, and those with limited forms of the dz, up to 40% may be with limited forms of the dz, up to 40% may be ANCA negative, thus the absence of ANCA does not ANCA negative, thus the absence of ANCA does not exclude the diagnosis of Wegener’s.exclude the diagnosis of Wegener’s.
Pathogenesis Pathogenesis (Contd)(Contd)
► Most common targeted antigens in WG :Most common targeted antigens in WG : Proteinase 3 (PR3), observed in 70-80% of Proteinase 3 (PR3), observed in 70-80% of
ptspts Myeloperoxidase (MPO)-target in Myeloperoxidase (MPO)-target in
approximately 10%approximately 10% Dual postivity is rare and , and generally Dual postivity is rare and , and generally
indicated the presence of another condition indicated the presence of another condition such as SLEsuch as SLE
~70% of pts with MPA are ANCA positive ~70% of pts with MPA are ANCA positive and most have MPO-ANCA, with only a and most have MPO-ANCA, with only a minority having PR3minority having PR3

►Nasal or oral inflammationNasal or oral inflammation Development of painful or painless oral ulcers or Development of painful or painless oral ulcers or
purulent or bloody nasal dischargepurulent or bloody nasal discharge
►Abnormal chest radiographAbnormal chest radiograph Chest radiograph showing the presence of nodules, Chest radiograph showing the presence of nodules,
fixed infiltrates, or cavitiesfixed infiltrates, or cavities
►Abnormal urinary sedimentAbnormal urinary sediment Microhematuria (>5 red blood cells per high power Microhematuria (>5 red blood cells per high power
field) or red cell casts in urine sediment field) or red cell casts in urine sediment
►Granulomatous inflammation on Granulomatous inflammation on biopsybiopsy Histologic changes showing granulomatous Histologic changes showing granulomatous
inflammation within the wall of an artery or in the inflammation within the wall of an artery or in the perivascular or extravascular area (artery or arteriole)perivascular or extravascular area (artery or arteriole)
Criteria for ClassificationCriteria for ClassificationDiagnosisDiagnosis

Diagnosis Diagnosis (Contd)(Contd)
► American College of Rheumatology –not American College of Rheumatology –not intended to be used in routine clinical practice intended to be used in routine clinical practice and established before ANCA.and established before ANCA.
► Presence of 2 or more yield 88% sensitivity Presence of 2 or more yield 88% sensitivity and 92% specificityand 92% specificity
►Nasal or oral inflammationNasal or oral inflammation►Abnormal chest radiograph (nodules, alveolar Abnormal chest radiograph (nodules, alveolar
opacities)opacities)►Abnormal urine sedimentAbnormal urine sediment►Granulomatous inflammation on biopsy of an Granulomatous inflammation on biopsy of an
artery or perivascular areaartery or perivascular area

Diagnosis Diagnosis (Contd)(Contd)
► Routine Labs-nonspecific- Leukocytosis, thrombocytosis Routine Labs-nonspecific- Leukocytosis, thrombocytosis (>400,000), marked ESR, and normocytic,normochromic (>400,000), marked ESR, and normocytic,normochromic anemia, mildly elevated RFanemia, mildly elevated RF
► ANCA- as previously describedANCA- as previously described► Tissue Biopsy- dx should be confirmed by tissue bx at Tissue Biopsy- dx should be confirmed by tissue bx at
site of active diseasesite of active disease►.Nasopharyngeal bx less invasive, but may not see full .Nasopharyngeal bx less invasive, but may not see full
pathogenesis due to small amount of tissue- acute and pathogenesis due to small amount of tissue- acute and chronic inflammationchronic inflammation
►Renal bx-segmental necrotizing glomerulnephritis w or Renal bx-segmental necrotizing glomerulnephritis w or w/o cresentsw/o cresents
►Skin-leukocytoclastic vasculitis with little or no Skin-leukocytoclastic vasculitis with little or no complement and immunoglobulincomplement and immunoglobulin
►Lung-granulomatous and vasculitisLung-granulomatous and vasculitis

Diagnosis Diagnosis (Contd)(Contd)
► Biopsy specimens showing the triad of vasculitis, Biopsy specimens showing the triad of vasculitis, granulomata, and large areas of necrosis granulomata, and large areas of necrosis SinusesSinuses NoseNose Skin-Skin---leukocytoclastic vasculitis with little or no complement leukocytoclastic vasculitis with little or no complement
and immunoglobulin on immunofluorescence and immunoglobulin on immunofluorescence Kidney-Kidney---segmental necrotizing glomerulonephritis that is segmental necrotizing glomerulonephritis that is
usually pauci-immune on immunofluorescence / EMusually pauci-immune on immunofluorescence / EM Lung--Lung--vasculitis and granulomatous inflammation vasculitis and granulomatous inflammation (Only large sections of lung tissue obtained via (Only large sections of lung tissue obtained via
thoracoscopic or open lung biopsy are likely to show all thoracoscopic or open lung biopsy are likely to show all of the histologic features) of the histologic features)
► Seropositivity for C-ANCAsSeropositivity for C-ANCAs

Antineutrophil cytoplasmic Antineutrophil cytoplasmic antibodies antibodies

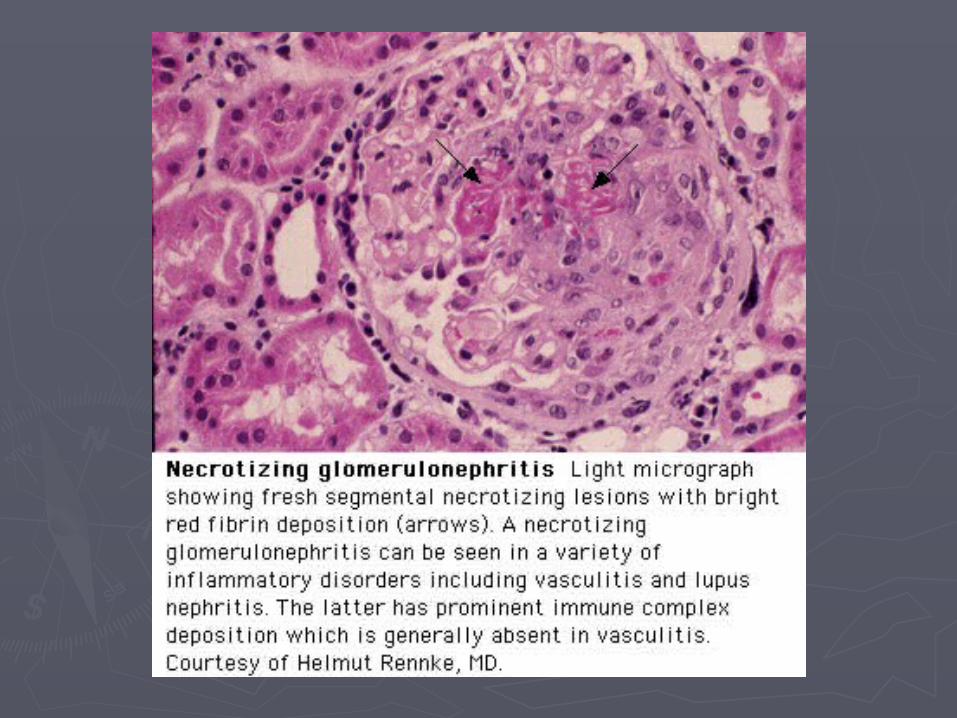
Focal or diffuse necrotizing extracapillary Focal or diffuse necrotizing extracapillary glomerulonephritis is the histological hallmark of glomerulonephritis is the histological hallmark of
ANCA-associated VasculitisANCA-associated Vasculitis
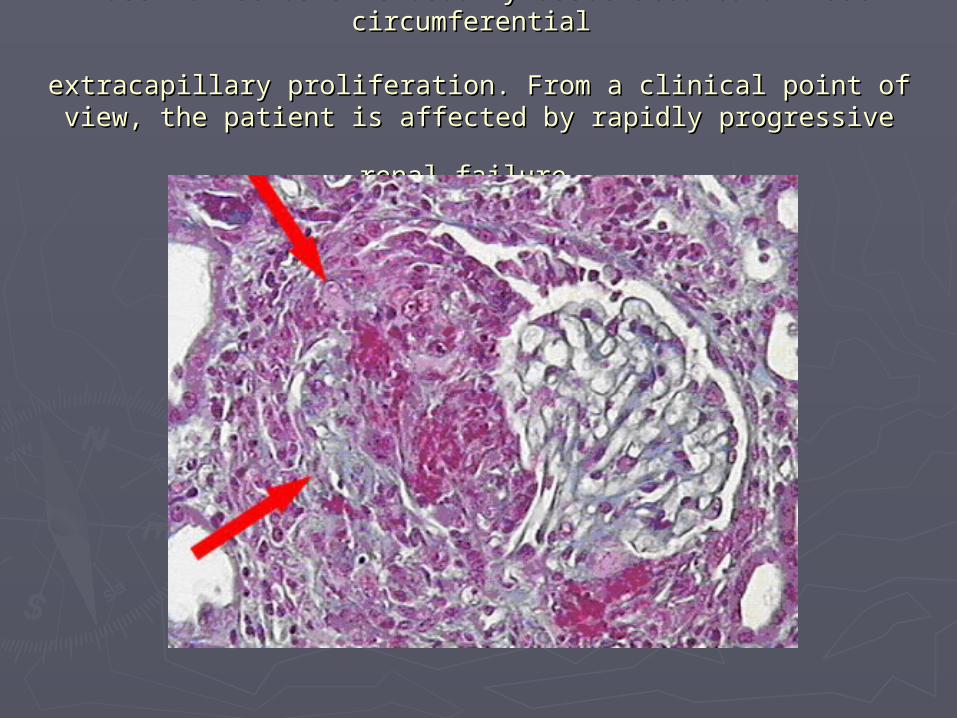
Massive necrosis is usually associated to diffuse circumferential Massive necrosis is usually associated to diffuse circumferential
extracapillary proliferation. From a clinical point of view, the extracapillary proliferation. From a clinical point of view, the
patient is affected by rapidly progressive renal failurepatient is affected by rapidly progressive renal failure..

The biopsy specimen of a lung from a patient with The biopsy specimen of a lung from a patient with Wegener Wegener
granulomatosis showing evidence of vasculitis and granulomatosis showing evidence of vasculitis and
inflammationinflammation

C-ANCA staining pattern of ethanol-fixed C-ANCA staining pattern of ethanol-fixed
normal human neutrophilnormal human neutrophil

ANCAANCA
►~90% of Wegener's cases are ANCA+~90% of Wegener's cases are ANCA+ In limited dz, up to 40% may be ANCA negIn limited dz, up to 40% may be ANCA neg
►80 - 90 % PR3-ANCA 80 - 90 % PR3-ANCA
►Remaining MPO-ANCARemaining MPO-ANCA
Is ANCA sufficient?Is ANCA sufficient?
►Concensus is that tissue dx is Concensus is that tissue dx is necessarynecessary
►Rarely may initiate tx w/o biopsyRarely may initiate tx w/o biopsy
►Should attempt to confirm w/ biopsy Should attempt to confirm w/ biopsy when ablewhen able
TreatmentTreatmentTraditionalTraditional
►PrednisonePrednisone (initiated at 1 mg/kg (initiated at 1 mg/kg daily for 1 to 2 months. then daily for 1 to 2 months. then tapered) tapered)
►CyclophosphamideCyclophosphamide (2mg/kg daily (2mg/kg daily for at least 12 months)for at least 12 months)
►>90% improve and 75% remit >90% improve and 75% remit

Treatment Treatment (Contd)(Contd)
►Many physicians favor use of daily Many physicians favor use of daily oral cyclophosphamide/corticosteroid oral cyclophosphamide/corticosteroid combination therapy in the initial combination therapy in the initial treatment of all pts dx with treatment of all pts dx with Wegener’s, and Wegener’s, and Once remission is induced (which Once remission is induced (which
requires a minimum of 3-6 months for requires a minimum of 3-6 months for most pts), other less toxic most pts), other less toxic immunosuppressives can be employedimmunosuppressives can be employed
Treatment Treatment (Contd)(Contd)
► Use of aggressive immunotherapy is Use of aggressive immunotherapy is justified b/c survival in untreated justified b/c survival in untreated generalized Wegener’s is extremely poor, generalized Wegener’s is extremely poor, with up to 90% of pt’s dying with in 2 yrs with up to 90% of pt’s dying with in 2 yrs from respiratory or renal failure, but from respiratory or renal failure, but mortality is markedly diminished with mortality is markedly diminished with introduction of introduction of cyclophosphamide/corticosteroid therapycyclophosphamide/corticosteroid therapy
Treatment Treatment (Contd)(Contd)
► Response to therapy-partial or complete Response to therapy-partial or complete resolution of inflammatory manifestations, resolution of inflammatory manifestations, such as inactive urine sediment, although such as inactive urine sediment, although renal failure can persistrenal failure can persist
Treatment Treatment (Contd)(Contd)
► IV Cyclophosphamide monthly- lowers the IV Cyclophosphamide monthly- lowers the overall cumulative dose-role is incompletely overall cumulative dose-role is incompletely defined, and both equal and decreased defined, and both equal and decreased efficacy has been described in Wegener’s, efficacy has been described in Wegener’s, which may be due to different pt which may be due to different pt populations in the studies, nonresponders populations in the studies, nonresponders had more severe disease, and those with had more severe disease, and those with incomplete response-switching to oral daily incomplete response-switching to oral daily regimen may induce remissionregimen may induce remission
Treatment Treatment (Contd)(Contd)
►Methotrexate-mild dz, higher relapse rate, Methotrexate-mild dz, higher relapse rate, can’t use in Cr >2.0can’t use in Cr >2.0
► Plasmapharesis-pts with renal dz needing Plasmapharesis-pts with renal dz needing dialysis, pulmonary hemorrhage, or also dialysis, pulmonary hemorrhage, or also with anti-GBMwith anti-GBM
Treatment Treatment (Contd)(Contd)
► In one of largest nonrandomized prospective single In one of largest nonrandomized prospective single center studies, outcomes of 158 pts with Wegener’s center studies, outcomes of 158 pts with Wegener’s treated with varying regimens at NIH were reportedtreated with varying regimens at NIH were reported
► Standard low dose cyclophosphamide plus Standard low dose cyclophosphamide plus prednisone(133), cyclophos alone (8), prednisone(133), cyclophos alone (8), glucocorticoids alone(10), or other cytotoxic agents glucocorticoids alone(10), or other cytotoxic agents plus steroids(6).plus steroids(6).
► Cyclophos administered for a mean of 2 yrs. Cyclophos administered for a mean of 2 yrs.
Treatment Treatment (Contd)(Contd)
► Mean follow up 8 yrs-In cyclophos and steroids:Mean follow up 8 yrs-In cyclophos and steroids: Survival 80%, with deaths due to Wegners, side effects or Survival 80%, with deaths due to Wegners, side effects or
bothboth Significant clinical improvement was observed in more Significant clinical improvement was observed in more
than 90% of pts, with 75% achieving complete remissionthan 90% of pts, with 75% achieving complete remission Among the 98 pts followed for more than 5 yrs, more than Among the 98 pts followed for more than 5 yrs, more than
half experienced remission of greater than 5 yrshalf experienced remission of greater than 5 yrs

Treament Treament (Contd)(Contd)
► So, based on studies, first line is daily oral So, based on studies, first line is daily oral cyclophosphamide/corticosteroid. Cyclophos cyclophosphamide/corticosteroid. Cyclophos at 1.5-2 mg/kg/day, steroid (1mg/kg/day). at 1.5-2 mg/kg/day, steroid (1mg/kg/day).
► IV Cyclophosphamide can be used, not well IV Cyclophosphamide can be used, not well studied, but associated with higher relapse studied, but associated with higher relapse and longer to remissionand longer to remission
► Methotrexate-maybe used in mild disease, or Methotrexate-maybe used in mild disease, or in maintenance, but either way, higher relapse in maintenance, but either way, higher relapse raterate
► Azathioprine-maintence, esp in pts with renal Azathioprine-maintence, esp in pts with renal insuffiencyinsuffiency
► Steroids- no significant benefit in maintenanceSteroids- no significant benefit in maintenance
Treatment Treatment (Contd)(Contd)
►Duration of maintenance therapy- 12-Duration of maintenance therapy- 12-18 months after stable remission18 months after stable remission May need more long term maintenance May need more long term maintenance
esp if ANCA continues to be positiveesp if ANCA continues to be positive
Treatment Treatment (Contd)(Contd)
50% in remission relapse 50% in remission relapse
AND daily cyclophos is very toxicAND daily cyclophos is very toxic
►pancytopenia, pancytopenia, ► infection, infection, ►hemorrhagic cystitishemorrhagic cystitis►bladder cancer (increased 33-fold)bladder cancer (increased 33-fold)► lymphoma (increased 11-fold) lymphoma (increased 11-fold)

Treatment Treatment (Contd)(Contd)
►Monthly IV cyclophosphamideMonthly IV cyclophosphamide -- -- less toxic less toxic but less effectivebut less effective
►Weekly methotrexateWeekly methotrexate -- -- maintains remissionmaintains remission
►Trimethoprim-sulfamethoxazoleTrimethoprim-sulfamethoxazole -- -- controversial (?effective for disease limited to the respiratory tract), controversial (?effective for disease limited to the respiratory tract), reduces the relapse rate reduces the relapse rate
►SteroidsSteroids —prednisone vs solumedrol —prednisone vs solumedrol►PlasmapheresisPlasmapheresis --unproven, awaiting MEPEX trialunproven, awaiting MEPEX trial
Recommended for anti-GBM+, pulm hemmorhage, renal failureRecommended for anti-GBM+, pulm hemmorhage, renal failure
► IVIGIVIG— — recommended in the setting of infection during PLEXrecommended in the setting of infection during PLEX

PrognosisPrognosis
►Overall, the morbidity and mortality Overall, the morbidity and mortality associated with Wegener’s granulomatosis associated with Wegener’s granulomatosis and microscopic polyangiitis, results from and microscopic polyangiitis, results from the combined effects of irreversible organ the combined effects of irreversible organ dysfunction b/c of inflammatory injury dysfunction b/c of inflammatory injury occurring before and the early phase of occurring before and the early phase of effective therapy, consequences of effective therapy, consequences of immunsuppressive therapy, and natural hx immunsuppressive therapy, and natural hx of diseaseof disease

Prognosis Prognosis (Contd)(Contd)
►Morbidity-consequences of therapy Morbidity-consequences of therapy (glucocorticoid toxicity, increased risk of (glucocorticoid toxicity, increased risk of malignancy ie bladder cancer, skin ca, malignancy ie bladder cancer, skin ca, sterility, organ failure); disease related sterility, organ failure); disease related damage (partial hearing loss and persistent damage (partial hearing loss and persistent proteinuria);increased risk of DVT/PE in proteinuria);increased risk of DVT/PE in ANCAANCA
Prognosis Prognosis (Contd)(Contd)
► Renal –ESRD eventually occurs in 20-25% of Renal –ESRD eventually occurs in 20-25% of pts. Poor renal outcome associated with more pts. Poor renal outcome associated with more severe renal dysfunction at presentation, lack severe renal dysfunction at presentation, lack of response to initial treatment,and enhanced of response to initial treatment,and enhanced amount of fibrotic changes on renal bxamount of fibrotic changes on renal bx
► Mortality- Major causes of death are Mortality- Major causes of death are complications of underlying disease and complications of underlying disease and therapy. 90% mortality rate in 2 yrs in therapy. 90% mortality rate in 2 yrs in untreated. Higher mortality in elderly, those untreated. Higher mortality in elderly, those with florid organ failure at presentation.with florid organ failure at presentation.
Prognosis Prognosis (Contd)(Contd)
Poorer outcomes with advanced age, Poorer outcomes with advanced age, severe renal impairment, DAH. severe renal impairment, DAH.
Mortality >75% if untreated with median Mortality >75% if untreated with median survival of 5 months. Drastic survival of 5 months. Drastic improvement since 1970s in mortality.improvement since 1970s in mortality.
Permanent morbidity:Permanent morbidity:• CKD 42%CKD 42%• Hearing Loss 35%Hearing Loss 35%• Nasal Deformity 28%Nasal Deformity 28%• Tracheal Stenosis 13%Tracheal Stenosis 13%• Severe Infection 50% (Treatment)Severe Infection 50% (Treatment)

ConclusionsConclusions
►One of the most frequent pulmonary-One of the most frequent pulmonary-renal syndromesrenal syndromes
►Granuloma’s in upper respiratory tract: Granuloma’s in upper respiratory tract: rhinitis, sinusitis, pharyngits, stomatitis, rhinitis, sinusitis, pharyngits, stomatitis, pulmonary infiltrates (nodules with pulmonary infiltrates (nodules with cavitations) with hemoptoe, respiratory cavitations) with hemoptoe, respiratory insufficiency, diffusion disturbancesinsufficiency, diffusion disturbances
►Most frequently RPGN-crescentic GN Most frequently RPGN-crescentic GN with pauci –immune GNwith pauci –immune GN
► ANCA positive (large majority C-ANCA)ANCA positive (large majority C-ANCA)

► Oral cyclophosphamide 1 - 2 mg/kg BW + Oral cyclophosphamide 1 - 2 mg/kg BW + corticosteroids 0.6 -1 mg/kg BW.corticosteroids 0.6 -1 mg/kg BW.
► I.V. pulse of cyclophosphamide 500 mg/m² every I.V. pulse of cyclophosphamide 500 mg/m² every month for 3 months + corticosteroids- results are month for 3 months + corticosteroids- results are not better?not better?
► Follow ANCA titersFollow ANCA titers► In case of dialysis need, plasmapheresis is to be In case of dialysis need, plasmapheresis is to be
considered, together with pulses of considered, together with pulses of cyclophophamide.cyclophophamide.
► Maintenance therapy: low dose of Maintenance therapy: low dose of cyclophophamide,methotrexatecyclophophamide,methotrexate
for pulmonary or upper respiratory tract for pulmonary or upper respiratory tract manifestations: trimetoprim-sulfamethoxazole manifestations: trimetoprim-sulfamethoxazole
Conclusion Conclusion (Contd)(Contd)
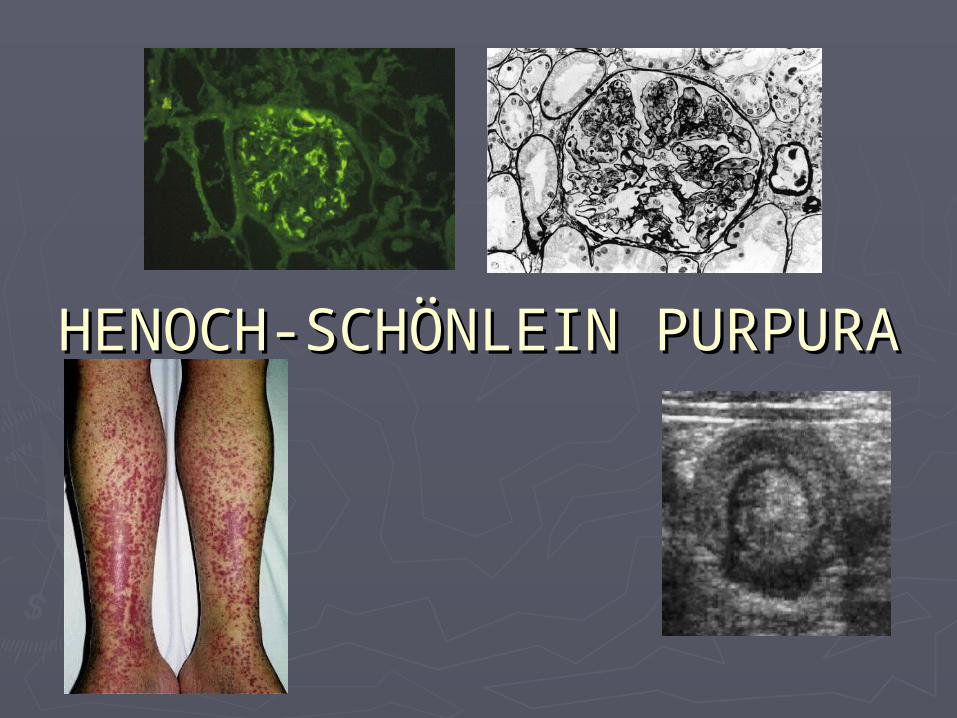
HENOCH-SCHÖNLEIN PURPURAHENOCH-SCHÖNLEIN PURPURA

DEFINITIONDEFINITION
►Also called “anaphylactoid purpura”Also called “anaphylactoid purpura”►HSP is a systemic vasculitic syndrome HSP is a systemic vasculitic syndrome
with:with: Palpable purpuraPalpable purpura ArthralgiasArthralgias GI involvementGI involvement GlomerulonephritisGlomerulonephritis

BACKGROUNDBACKGROUND
►First described in 1801 by William First described in 1801 by William Heberden, a physician in London, who Heberden, a physician in London, who wrote about a case of a 5 year old wrote about a case of a 5 year old boy with hematuria, abdominal pain, boy with hematuria, abdominal pain, joint pains and a skin rash.joint pains and a skin rash.
► In 1837, Johann Schönlein and later in In 1837, Johann Schönlein and later in 1874, Edouard Henoch described 1874, Edouard Henoch described multiple case reports of similar cases. multiple case reports of similar cases. They also showed an association of They also showed an association of an upper respiratory infection an upper respiratory infection preceding development of symptoms. preceding development of symptoms.

EPIDEMIOLOGYEPIDEMIOLOGY
►90% of cases reported in children90% of cases reported in children Peak in children aged 4-7Peak in children aged 4-7
►Male:Female (1.5:1) Male:Female (1.5:1) ►50% follow a URI50% follow a URI►Renal disease is more severe in adultsRenal disease is more severe in adults

PATHOGENESISPATHOGENESIS
►Likely mechanism thought to be an Likely mechanism thought to be an immune-complex mediated disease immune-complex mediated disease with deposits in the glomerular with deposits in the glomerular capillaries, dermal capillaries and GI capillaries, dermal capillaries and GI tract.tract.
►Mesangial deposits of IgA are the Mesangial deposits of IgA are the same as those seen in IgA same as those seen in IgA nephropathy nephropathy
PRECIPITATING ANTIGENSPRECIPITATING ANTIGENS
► INFECTIONSINFECTIONS URIURI MeaslesMeasles RubellaRubella Parvovirus B19Parvovirus B19 MycoplasmaMycoplasma Coxsackie virusCoxsackie virus ToxocaraToxocara AmebiasisAmebiasis SalmonellaSalmonella
C.difficileC.difficile H.pyloriH.pylori AdenovirusAdenovirus LegionellaLegionella TuberculosisTuberculosis MumpsMumps StreptococcusStreptococcus Morganella Morganella
morganiimorganii
PRECIPITATING ANTIGENSPRECIPITATING ANTIGENS
►DrugsDrugs VancomycinVancomycin StreptokinaseStreptokinase RanitidineRanitidine CefuroximeCefuroxime DiclofenacDiclofenac EnalaprilEnalapril CaptoprilCaptopril
PRECIPITATING ANTIGENSPRECIPITATING ANTIGENS
►Other:Other: Food hypersensitivityFood hypersensitivity Cold exposureCold exposure Autosomal recessive Chronic Autosomal recessive Chronic
granulomatous diseasegranulomatous disease Myelodysplastic syndromeMyelodysplastic syndrome Small cell lung cancerSmall cell lung cancer Breast cancerBreast cancer

PATHOLOGIC FEATURESPATHOLOGIC FEATURES
DERMATOLOGIC FINDINGS: DERMATOLOGIC FINDINGS: Leukocytoclastic vasculitis with IgA Leukocytoclastic vasculitis with IgA depositiondeposition
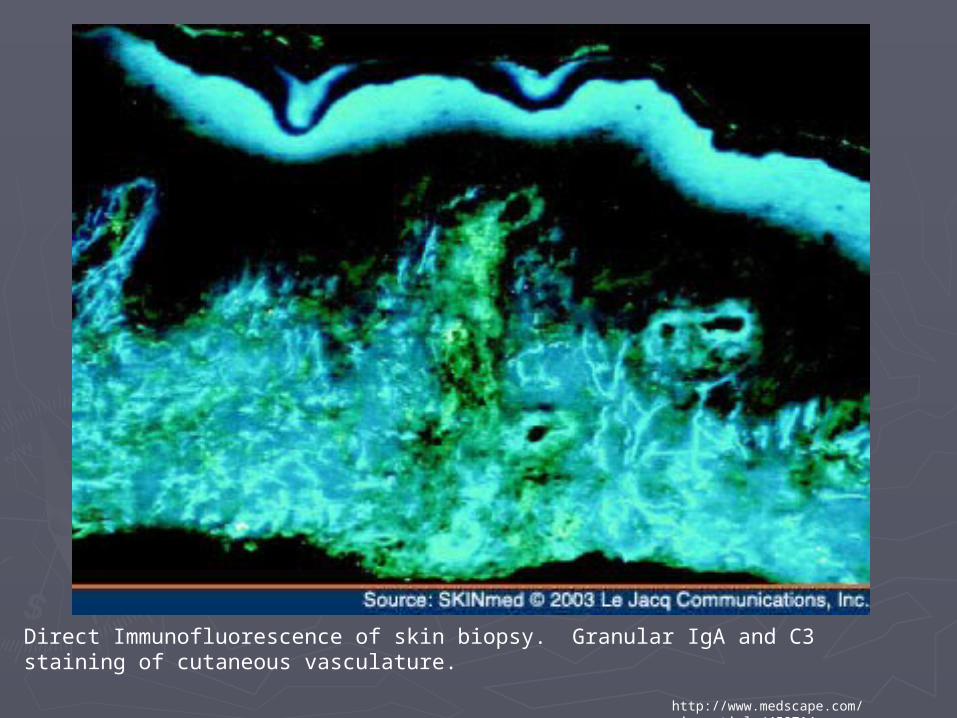
Direct Immunofluorescence of skin biopsy. Granular IgA and C3 staining of cutaneous vasculature.
http://www.medscape.com/viewarticle/459714

H & E stain of skin biopsy showing leukocytoclastic vasculitis with infiltration of neutrophils.
http://www.medscape.com/viewarticle/459714
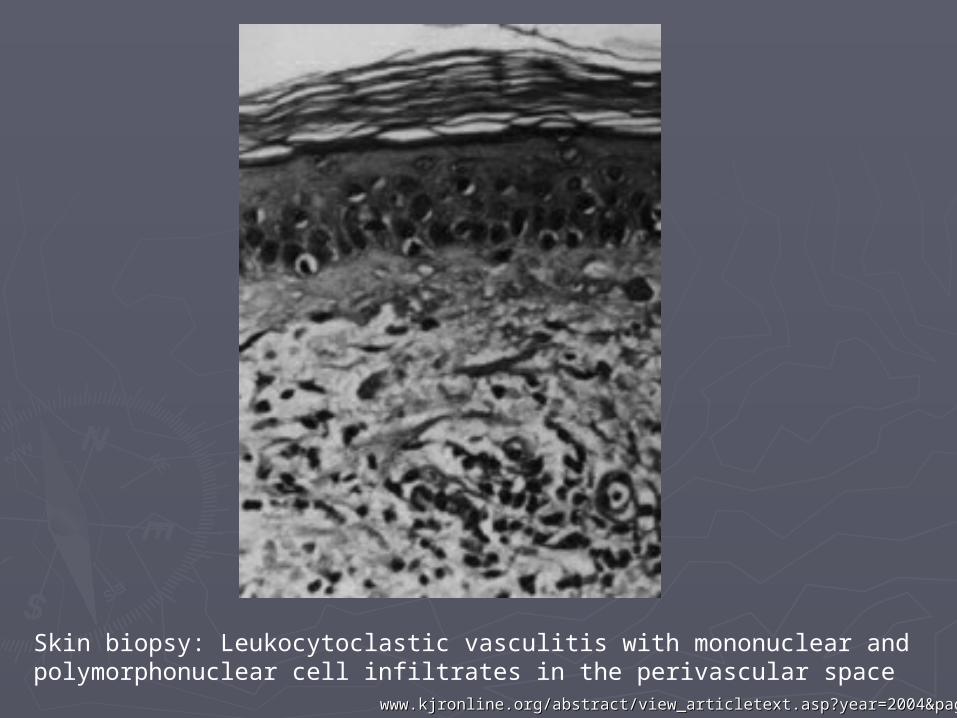
Skin biopsy: Leukocytoclastic vasculitis with mononuclear and polymorphonuclear cell infiltrates in the perivascular space
www.kjronline.org/abstract/view_articletext.asp?year=2004&page=178www.kjronline.org/abstract/view_articletext.asp?year=2004&page=178
PATHOLOGIC FEATURESPATHOLOGIC FEATURES
RENAL FINDINGS: Granular deposits of RENAL FINDINGS: Granular deposits of IgA, mesangioproliferative IgA, mesangioproliferative glomerulonephritis and crescent glomerulonephritis and crescent formation formation

Renal biopsy: sclerosis and fibrous crescents in the glomerulus.
http://www.ndt-educational.org/nagycase.asp

http://www.ndt-educational.org/nagycase.asp
Immunofluorescence: Glomerular deposits of IgAImmunofluorescence: Glomerular deposits of IgA
CLINICAL FEATURESCLINICAL FEATURES
►Tetrad of symptomsTetrad of symptoms Abdominal painAbdominal pain Renal diseaseRenal disease Palpable purpuraPalpable purpura Arthritis/arthralgias – more common in Arthritis/arthralgias – more common in
adults and most common in knees and adults and most common in knees and ankles. Generally self-limitingankles. Generally self-limiting

CLINICAL FEATURESCLINICAL FEATURES
►PALPABLE PURPURA: most commonly PALPABLE PURPURA: most commonly seen on lower extremities and seen on lower extremities and buttocks, however can also been seen buttocks, however can also been seen on the trunk and arms. on the trunk and arms. Lesions begin as erythematous macules Lesions begin as erythematous macules
and progress to purpuric, non-blanching, and progress to purpuric, non-blanching, nonpruritic lesions that may become nonpruritic lesions that may become confluentconfluent
CLINICAL FINDINGSCLINICAL FINDINGS
►GI INVOLVEMENT: more common in GI INVOLVEMENT: more common in children. Symptoms include children. Symptoms include abdominal pain, nausea, vomiting, abdominal pain, nausea, vomiting, diarrhea, constipation or bowel diarrhea, constipation or bowel intussusception. May present with GI intussusception. May present with GI bleeding. bleeding.

CLINICAL FEATURESCLINICAL FEATURES
►RENAL INVOLVEMENT: RENAL INVOLVEMENT: in up to 50% of patientsin up to 50% of patients Usually more rapidly progressive in Usually more rapidly progressive in
adults. Rare in childrenadults. Rare in children May present with hematuriaMay present with hematuria Can have mild glomerulonephritis leading Can have mild glomerulonephritis leading
to microscopic hematuria and can lead to to microscopic hematuria and can lead to a rapidly progressive glomerulonephritis a rapidly progressive glomerulonephritis with RBC castswith RBC casts
Usually resolve spontaneously. Usually resolve spontaneously.

DIAGNOSTIC EVALUATIONDIAGNOSTIC EVALUATION
►May have mild leukocytosisMay have mild leukocytosis►Normal platelet countNormal platelet count►Normal serum complement levelsNormal serum complement levels►Elevated IgA in 50%Elevated IgA in 50%
DIAGNOSISDIAGNOSIS
►Generally a clinical diagnosisGenerally a clinical diagnosis►Skin Biopsy: can be helpful and used Skin Biopsy: can be helpful and used
to confirm IgA and C3 deposits and to confirm IgA and C3 deposits and leukocytoclastic vasculitis. leukocytoclastic vasculitis.
►Renal Biopsy: not usually needed for Renal Biopsy: not usually needed for diagnosis. Will show mesangial IgA diagnosis. Will show mesangial IgA deposits and segmental deposits and segmental glomerulonephritisglomerulonephritis

MANAGEMENTMANAGEMENT
►Usually self-limiting (1-6 weeks)Usually self-limiting (1-6 weeks)►Steroids: Steroids:
may decrease tissue edema, may aid in may decrease tissue edema, may aid in arthralgias and some abdominal painarthralgias and some abdominal pain
Has not been shown to be beneficial in Has not been shown to be beneficial in kidney disease or dermal manifestationskidney disease or dermal manifestations
Does not lessen chance of recurrenceDoes not lessen chance of recurrence Does not shorten duration of diseaseDoes not shorten duration of disease

MANAGEMENTMANAGEMENT
► if rapidly progressive if rapidly progressive glomerulonephritisglomerulonephritis Multidrug regimens with cytotoxic drugs Multidrug regimens with cytotoxic drugs
however not many reports with treatment however not many reports with treatment in adults.in adults.
PlasmaphoresisPlasmaphoresis IVIGIVIG
►Symptomatic management of GI Symptomatic management of GI symptoms and surgical intervention if symptoms and surgical intervention if warranted. warranted.
PROGNOSISPROGNOSIS
►Prognostic factors: Prognostic factors: generally a milder course in children with generally a milder course in children with
shorter duration and fewer recurrences shorter duration and fewer recurrences Proteinuria >1gm/day with worse Proteinuria >1gm/day with worse
prognosis if develop nephrotic syndromeprognosis if develop nephrotic syndrome
►1-5% children progress to ESRD1-5% children progress to ESRD►Recurrence in up to 40% of patientsRecurrence in up to 40% of patients