causes and treatment of wegener’s granulomatosis alicia yu yifan (emily) hu grace tang jessica wu...
TRANSCRIPT

Causes and Treatment of Wegener’s granulomatosisAlicia YuYifan (Emily) HuGrace TangJessica Wu
PHM142 October 20, 2015
PHM142 Fall 2015Coordinator: Dr. Jeffrey HendersonInstructor: Dr. David Hampson

Case Study
A 45 year-old male goes to the physician, complaining of nasal congestion, cough, chest discomfort and dyspnea. He thinks it is just a common cold, but also reports finding bloody nasal discharge, and experiences painful swelling in his lower eyelid. The physician orders a blood and urine test.
Case Study: Laboratory Results
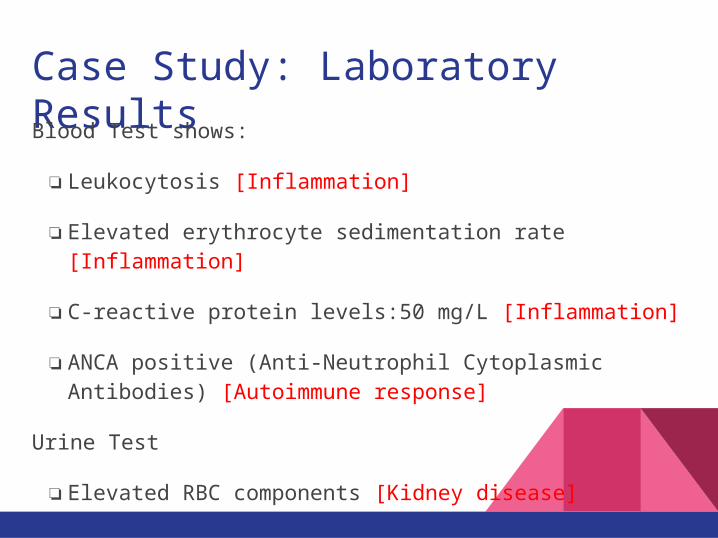
Blood Test shows:
❏Leukocytosis [Inflammation]
❏Elevated erythrocyte sedimentation rate [Inflammation]
❏C-reactive protein levels:50 mg/L [Inflammation]
❏ANCA positive (Anti-Neutrophil Cytoplasmic Antibodies) [Autoimmune response]
Urine Test
❏Elevated RBC components [Kidney disease]

What is Wegener’s Granulomatosis?❏ a.k.a. granulomatosis with polyangiitis (GPA).
❏ An uncommon systemic disorder that causes inflammation of blood vessels.
❏ This inflammation is accompanied by granuloma formation which restricts the supply of blood to various organs.
❏ GPA is characterized by an close association with ANCA (anti-neutrophil cytoplasm antibody) targeted against PR3 (proteinase 3).
❏ About 80-90% of patients with GPA are ANCA-positive.
❏ The levels of PR3-ANCA is highly specific for GPA and thus is a valuable tool for the diagnosis of this disease.
❏ Today, our knowledge pertaining the cause and pathogenesis of GPA are still incomplete. The clue to the initiating event in GPA is considered to be a combination of environmental and genetic factors.

Infected Organs and Symptoms❏ The major sites of infection usually involve the upper and lower respiratory tracts and
kidneys. The symptoms at these infected sites include:
recurrent infections of the nose
❏ sinus pain and inflammation
❏ mucosal thickening
❏ cough
❏ shortness of breath
❏ chest pain
❏ blood in urine
❏ During active disease, patient may have other non-specific symptoms such as weight loss, joint pain, skin sores, malaise, eye swelling, and some forms of hearing loss.
Diagnosis
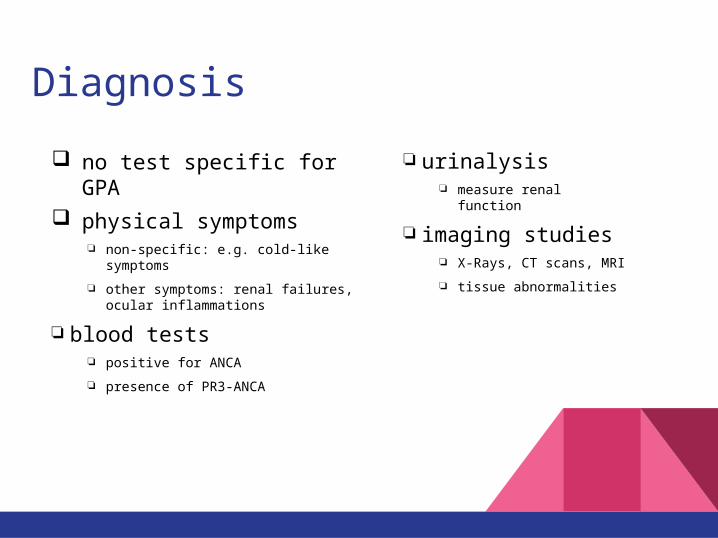
❏ urinalysis ❏ measure renal function
❏ imaging studies❏ X-Rays, CT scans, MRI
❏ tissue abnormalities
no test specific for GPA
physical symptoms❏ non-specific: e.g. cold-like symptoms
❏ other symptoms: renal failures, ocular inflammations
❏ blood tests❏ positive for ANCA
❏ presence of PR3-ANCA

Pathogenesis
❏ Dual morphology - necrotizing vasculitis and extravascular granulomatous inflammation
❏ Usually starts as granulomatous disease before it converts to systemic autoimmune vasculitis
Hypotheses regarding the pathogenesis of GPA concentrate on PR3-ANCA, TNF-alpha, neutrophils, T and B cells in granuloma formation and induction of vasculitis.



Pathogenesis - proposed mechanismsSome in vitro and in vivo studies support the concept that PR3-ANCA and TNF-alpha interaction activate neutrophil granulocytes, thereby inducing subsequent endothelial damage in blood vessels and further leukocyte recruitment resulting in vasculitis.

Causes❏ Genetic Factors
❏ MHC:
❏ particularly HLDPB1*0401 - significant risk factor
❏ HLA-DPB4
❏ risk factor for GPA but not for other AAV (anca-associated vasulitis)
❏ Environmental Factors❏ infections
❏ bacterial: Staphylococcus aureus
❏ exposure to inhaled substances
❏ fume and particulate
❏ drugs
❏ evidence suggesting that some drugs may induce ANCA production

Treatment❏Cyclophosphamide (Trade name: Cytoxan)
❏ Anti-cancer and Immunosuppressant
❏Prednisone (Cortisone)
❏ Corticosteroid: prevents inflammation, immunosuppressive
❏Methotrexate (Trade name: Rheumatrex)
❏ Anti-cancer and immunosuppressant
❏Trimethoprim/sulfamethoxazole (Trade name: Bactrim)
❏ Antibiotics to prevent relapse
Treatment: Rituximab❏Trade Name: Rituxan
❏Chimeric monoclonal antibody that binds to CD20 protein, destroying B cells
❏IV administration, 10 mg/mL
❏Used in combination with glucocorticoids
❏Studies found it to be effective in adults patients with refractory GPA
❏Other uses: treatment of Non Hodgkin’s Lymphoma, and Rheumatoid Arthritis

Summary❏Wegener’s granulomatosis, a.k.a. granulomatosis with
polyangiitis (GPA), is an autoimmune disease characterized by granuloma formation-induced inflammation and necrotic vasculitis
❏Undefined etiology and pathogenesis ❏ Risk factors: genetic and environmental❏ Models of pathogenesis have been proposed
❏ inconclusive due to lack of supporting evidence
❏Pathological hallmark: presence of PR3-ANCA❏Treatment: immunosuppressants (eg. Cyclophosphamide,
Prednisone)❏Rituximab : Chimeric monoclonal antibody that binds to
CD20 protein to destroying B cells, found to be effective in refractory cases

ReferencesArning L, Holle JU, Harper L et al. Are there specific genetic risk factors for the different forms of ANCA-associated vasculitis? Ann. Rheum. Dis. 70(4), 707–708 (2011).
CPS [Internet]. Ottawa (ON): Canadian Pharmacists Association; c2015. Rituxin [product monograph]. Available from: http://www.e-therapeutics.ca. Also available in paper copy
from the publisher.
Holle JU, Gross WL, Holl-Ulrich K et al. Prospective long-term follow-up of patients with localised Wegener’s granulomatosis: does it occur as persistent disease stage? Ann.
Rheum. Dis. 69(11), 1934–1939 (2010).
Laudien M, Gadola SD, Podschun R et al. Nasal carriage of Staphylococcus aureus and endonasal activity in Wegener s granulomatosis as compared to rheumatoid arthritis and
chronic rhinosinusitis with nasal polyps. Clin. Exp. Rheumatol. 28(1 Suppl. 57), 51–55 (2010).
Ntatsaki E, Watts RA, Scott DG. Epidemiology of ANCA-associated vasculitis. Rheum. Dis. Clin. North Am. 36(3), 447–461 (2010).
Oristrell, J., Bejarano, G., Jordana, R., Monteagudo, M., Marí, B., Casanovas, A., & Tolosa, C. (2009). Effectiveness of Rituximab in Severe Wegener’s Granulomatosis: Report of
Two Cases and Review of the Literature. The Open Respiratory Medicine Journal, 3, 94–99. http://doi.org/10.2174/1874306400903010094.
Stegeman CA, Tervaert JW, Sluiter WJ, Manson WL, de Jong PE, Kallenberg CG. Association of chronic nasal carriage of Staphylococcus aureus and higher relapse rates in
Wegener granulomatosis. Ann. Intern. Med. 120(1), 12–17 (1994).
Wieczorek S, Holle JU, Epplen JT. Recent progress in the genetics of Wegener’s granulomatosis and Churg-Strauss syndrome. Curr. Opin. Rheumatol. 22(1), 8–14 (2010).
Witko-Sarsat, V., Reuter, N., & Mouthon, L. (2010). Interaction of proteinase 3 with its associated partners: Implications in the pathogenesis of Wegenerʼs granulomatosis. Current
Opinion in Rheumatology, 22(1), 1-7. doi:10.1097/BOR.0b013e3283331594.
Lamprecht, P., Csernok, E., & Gross, W. L. (2006). Effector memory T cells as driving force of granuloma formation and autoimmunity in wegener's granulomatosis. Journal of
Internal Medicine, 260(3), 187-191. doi:10.1111/j.1365-2796.2006.01698.x.
[Untitled photograph of Rituximab Vial ]. Retrieved from http://rheumatoidarthritisnews.com/2015/01/06/rheumatoid-arthritis-drug-rituximab-delays-need-for-re-treatment-from-
disease-flares/.