susan barron-hamilton - darling downs & west moreton phn - creating collective impact conditions...
TRANSCRIPT

National Mental Health Conference PIR to PHN Creating Collective Impact Conditions
November 2015

What is involved in facilitating better coordination of clinical services and supports
What does it take to develop sustainable partnerships and build links between sectors and services
How do you build collective ownership and collaborative networks that have tangible outcomes
What is involved in building integrated pathways to support a person transitioning across continuums of care
How do you embed recovery principles – what is involved and how is it done
Finding the answer to DoH Questions!
Collective Impact – What’s that?
Generating collaborative commitment to a common agenda aimed at solving a problem with measurable and sustainable outcome
Agreement Common Agenda
Mutually reinforcing activities – coordinated through a agreed plan of action
Shared Measures
Continuous Communication
Backbone Support
Essential elements
Needs analysis
Find models that can be adopted and amended to fit
ADKAR change management tools
Cynefin Adaptive Leadership Complexity Framework
SWOT analysis
Tactical tools

Intervention Coordination Integration Systems Change
PIR Consortium
PIR Program Manager
Support Facilitators
Action Research Methodology

Psychological stress
Daytime Activity
Company and social connections
Employment/volunteering
Accommodation
CANSAS Top 5 Unmet Needs
Issues register – 128
53 Projects (January 2014)
25 Projects (October 2014)
11 final count
WMO System Reform

Embracing New Frontiers Designing and establishing innovative models Recovery focused Unlocking the Value Its Mobilising Living well as equals Tailored wrap around care Blur the boundaries between formal and informal support Reducing stigma Supporting people to self manage and stay well
People Powered Health
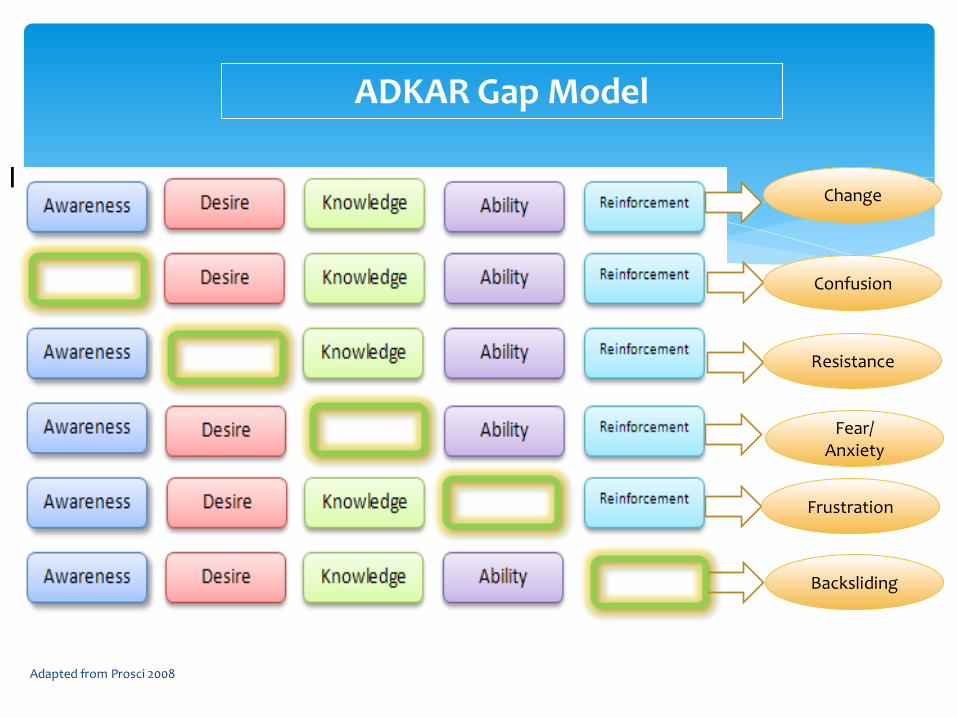
Adapted from Prosci 2008
ADKAR Gap Model
Change
Confusion
Resistance
Fear/ Anxiety
Frustration
Backsliding
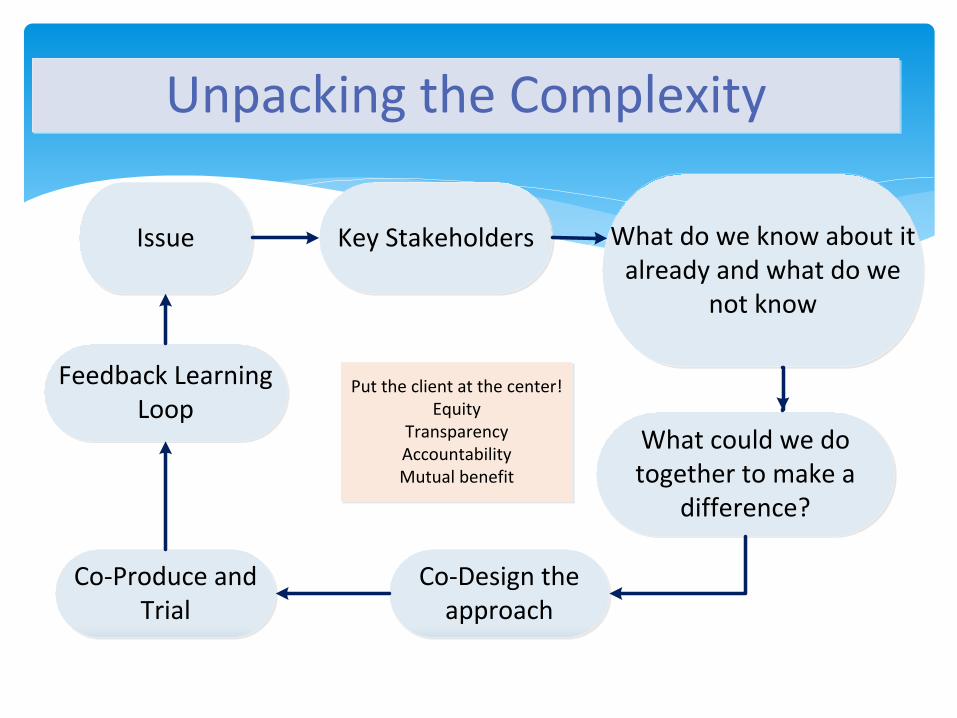
Feedback Learning Loop
Co-Produce and Trial
What could we do together to make a
difference?
Co-Design the approach
Issue
Unpacking the Complexity
Key Stakeholders What do we know about it already and what do we
not know
Put the client at the center!Equity
TransparencyAccountabilityMutual benefit


Good Program Management
Good Project Management
Engagement and communication
Sound Business Intelligence
Emotional Intelligence
Essential skills

Learnings
Seeing the issue from others vantage points Do your learning in the real world and do lots
of it Get off the balcony and get on the dance
floor Be resilient and persistent Develop good political antennae Have patience and pivot fast Be prepared for the life boats to be lowered!
Embrace change and growth Seek Allies and Create a Movement Water goes round the rock – go with the
energy Be open to developing the workforce
Learnings Continued
Big need for innovation in healthcare – never been greater Consumer demands and expectations are rising. Ageing and the advancement of new medical options have led to a growth in healthcare expenditures. A focus on innovation brings together both theory and practice to transform Healthcare Policy and Management in innovative ways which are more effective and efficient This is done on all possible levels, from micro-to-macro-level, from individual organisations to national healthcare systems, from patient relations to the process of caretaking.
The Right Care in the Right Place at the Right Time
Innovation Management

Prevention Defence Line
Corrections /
Police/
justice
Hospital /
Ambulance
Complex / Crisis / Acute Individual Capacity Building / Rehabilitation Prevention Defence Line Living Well
Self Management
NGO Community Orgs -
Wellbeing Centres
Tight Care Coordination
Therapeutic Treatment
Peer Support
Pharmacy
Medication Management
Continuity of Medication
Health Promotion
Primary Prevention
Secondary Prevention
Private Practitioners
ATAPS
Better Access
E-Health
General Practice
Primary Prevention
Secondary Prevention Continuity of Medication
Medication Review
Gate way to integrated
health care
Medical and social
prescribing
Str
on
g C
om
mu
nit
y C
en
tres
(Com
mu
nity C
on
ne
cto
rs in t
he
Ce
ntr
es)
Developing
Workforce
Building Capacity
and Capability
General Practice
Practice Nurses
Mental Health
Workforce
University Schools
Community and
Neighbourhood
Centres (CaNs)
Other
New HR & Workforce
Succession Planning Provisional Practitioners
Social Work
(BSW)
Psychology
Dietetics
Exercise
Physiology
Org Psychology
Community
Development (Dip)
Low cost no cost Human
Resources
Volunteers
Community
Connectors
Sector 3 Sector 2 Sector 1
Transition
Partnerships Common Agenda Agreed Plan of Action Efficiency and Effectiveness Care Coordination System Capacity building Evaluation and Outcome Measured Carer / Consumer Participation
Darling Downs West Moreton Regional Primary Health Network for Living Well
People Helping
People
Volunteers /
Students
Religious
Spiritual
Cultural
Societal
Emotional
Wellbeing
Art / Craft /
Hobby
Activities
No Cost /
Low Cost
Economic
Participation
Developing Integrated Care Pathways (ICPs) and Shared Care Planning - build the Recovery Road across the Living Well Network
Rec
ove
ry
Population Health -
Integrated Ambulatory
Care of Chronic
Conditions (&
Comorbidity)
Mental Health
Aboriginal and Torres
Strait Islander - Closing
the Gap
Overseas Born –
Refugee Health
Cardiovascular
Respiratory Disease
Diabetes
Obesity
Kidney Disease
Drugs of dependency
Domestic Violence
Cancer Control
Aged Care (Veterans)
End of Life Care
Planned
Admission -
elective

Darling Downs and West Moreton PHN Strategic Framework for Transforming Primary Health Care
Our Values – Integrity, Respect, Transparency, Accountability and Learning
Our Priorities – Mental Health (including domestic violence and substance abuse), Aged Care, Aboriginal and Torres Strait
Islander Health, Health Workforce, Population Health (including chronic disease and lifestyle) and E-Health
1:
Acti
ve
su
pp
ort
for
se
lf m
an
ag
em
en
t
2:
Hea
lth
pro
mo
tio
n a
nd
ill
ne
ss
pre
ve
nti
on
3:
Inte
gra
ted
in
ten
siv
e a
mb
ula
tory
ca
re m
an
ag
em
en
t
4:
Inte
gra
ted
so
cia
l an
d e
mo
tio
na
l
we
llb
ein
g m
an
ag
em
en
t
5:
Co
ord
ina
tin
g In
teg
rate
d C
are
Pa
thw
ay
s
6:
Co
nti
nu
ity
of
me
dic
ati
on
ma
na
gem
en
t
7:
Bett
er
pre
pa
rati
on
fo
r p
lan
ned
ho
sp
ita
l a
dm
iss
ion
s
8:
Es
tab
lis
hin
g c
om
mu
nit
y b
as
ed
alt
ern
ati
ve
s t
o a
cc
ide
nt
an
d
em
erg
en
cy
9:
Dev
elo
pin
g t
he
wo
rkfo
rce
10:
Info
rm
ati
on
te
ch
no
log
y –
ch
an
gin
g t
he
he
alt
h c
are c
ult
ure
Our Aim - Right Care, Right Place, Right Time
Our Vision - Seamless healthcare system that fulfils the needs of primary health care providers and our community

Investment: Investment in health innovation lags behind that in other sectors. Separate worlds: Research and practice exists in separate worlds Short–termism: Day–to–day pressures and burdens lean to short–term planning and operational matters Political: political imperative compounds short–term thinking by demanding instant results Access to evidence: vital to demonstrate success and increase the likelihood of role out Knowledge transfer: Even where innovation is actively adopting ideas from elsewhere, the organisational learning during the process of innovating creates a tacit knowledge that cannot simply be bottled up and sold on.
The Right Care in the Right Place at the Right Time
Challenges

Structure and hierarchy: Large organisations have evolved to be self–sustaining – see innovation from outside as a threat Silo mentality: act as barriers to sharing ideas Risk aversion: Staff see innovation as a challenge to the way they work/job roles Rewards: Professionals who deliver a service with a track record of success have little personal incentive to decommission that service and put alternatives in place. Service change: is likely to attract unwelcome attention from service users, local media and politicians. Scrutiny: accountability, clear standards and continuity of service can contribute to the culture of risk aversion rather than embracing it as part of the journey to radically different outcomes.
The Right Care in the Right Place at the Right Time
Challenges

The Right Care in the Right Place at the Right Time
Contact