surviving sepsis campaign learn - baylorcme.org · bslmc launched a surviving sepsis working group...
TRANSCRIPT

Sepsis e‐Learn: Module 1
1
Surviving Sepsis Campaign “Sepsis” e‐learn ‐Module 1
Situation & Background
Learning ObjectivesModule 1
Understand…
• The impact sepsis has on patient mortality and healthcare costs.
• The importance of improving the identification and treatment of sepsis at BSLMC.
• The plan at BSLMC is to improve all sepsis outcomes.

Sepsis e‐Learn: Module 1
2
1.6 million cases in US hospitals per year
800 deaths occur due to severe sepsis and septic shock daily in
the US
One of the top 10 causes of disease‐related death
Cost > $20 BILLION per year
SEPSISin USA
(CDC, 2016)(Sepsis Alliance)
Source: Torio CM, Andrews RM. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011. HCUP Statistical Brief No. 160. Rockville, MD: Agency for Healthcare Research and Quality; August 2013. http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb160.pdf.
Source 1: Hall MJ, Williams SN, DeFrances CJ, Golosinskiy A. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief No. 62. Atlanta, GA: National Center for Health Statistics; June 2011. https://www.cdc.gov/nchs/data/databriefs/db62.pdf.Source 2: Wood KA, Angus DC. Pharmacoeconomic implications of new therapies in sepsis. PharmacoEconomics. 2004;22(14):895‐906.Source 3: New Jersey Sepsis Learning Action Collaborative. Toolkit for Post‐Acute Care Settings: To Save Lives: Early Identification–Early Treatment. Princeton, NJ: Health Research and Educational Trust of New Jersey; 2015. http://www.njha.com/media/328416/NJSepsisLACToolkitPost‐AcuteCareSettings.pdf.

Sepsis e‐Learn: Module 1
3
Source 4: Hall MJ, Williams SN, DeFrances CJ, Golosinskiy A. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief No. 62. Atlanta, GA: National Center for Health Statistics; June 2011. https://www.cdc.gov/nchs/data/databriefs/db62.pdf.
Sepsis ‐ Situation
BSLMC is no exception. In 2015 and 2016, 3060 patients were diagnosed with sepsis, severe sepsis, or septic shock; 572 of
these patients expired.
Source: Internal Data, Baylor St. Luke's Medical Center Sepsis Initiative.

Sepsis e‐Learn: Module 1
4
•“Life‐threatening organ dysfunction caused by a dysregulated host response to infection”.
(Singer, Deutschman, et al., 2016, pg. 805)
•“Life‐threatening condition that arises when the body’s response to an infection injures its own tissues and organs”.
(Singer, Deutschman, et al., 2016, pg. 805)
What is “SEPSIS ”?
Source: Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis‐3). JAMA. 2016 Feb 23;315(8):801‐810.
8
Sepsis – Background
BSLMC launched a Surviving Sepsis Working group in 2015 to improve sepsis related outcomes. The work group has built an early detection program and treatment tools for sepsis from the SSC bundles that additionally promote compliance with the CMS
quality metrics for sepsis care.

Sepsis e‐Learn: Module 1
5
• The Surviving Sepsis Campaign (SSC) is a partnership of the European Society of Intensive Care Medicine and the Society of Critical Care Medicine formed in 2002 to promote advances in sepsis care, in order to improve outcomes.
• The SSC has created evidence based “bundles” of care for early recognition and treatment of sepsis, severe sepsis and septic shock. These bundles are grouped by timing of interventions into three hour and six hour bundles.
• A large landmark international study (62 countries) showed that use of these bundles decreased severe sepsis and septic shock mortality by 40 %.1
Source 1: Rhodes A, Phillips G, Beale R, et al. The Surviving Sepsis Campaign bundles and outcome: results from the International Multicentre Prevalence Study on Sepsis (the IMPreSS study). Intensive Care Med. 2015 Sep;41(9):1620‐1628. DOI: 10.1007/s00134‐015‐3906‐y.
The SIRS criteria reflect inflammation.
Infection
Steps in Recognizing “SEPSIS ”?
BSLMS sepsis working group / CMS bundles based upon SSC (still in effect) definitions of SIRS, sepsis, severe sepsis, and septic shock

Sepsis e‐Learn: Module 1
6
The Future……Revised Sepsis Definitions……
Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis‐3) JAMA 2016Society of Critical Care Medicine and European Society of Intensive Care Medicine
New definition emphasizes host of patient response to infection not so much as SIRS but as organ dysfunction due to SIRS that is harmful.
Source: Antonelli M, DeBacker D, Dorman T, et al, Surviving Sepsis Campaign Responds to Sepsis‐3. March 1 2016. Available at: http://www.survivingsepsis.org/SiteCollectionDocuments/SSC‐Statements‐Sepsis‐Definitions‐3‐2016.pdf.
As the extent and severity of sepsis related syndromes is so significant, and the Surviving Sepsis Campaign bundles so effective in treatment of sepsis, that CMS began requiring hospitals to report compliance with the Surviving Sepsis Campaign three and six hour bundles for sepsis syndromes.

Sepsis e‐Learn: Module 1
7
“Minutes Saves Lives!”
“We encourage the implementation of international sepsis guidelines to enable healthcare workers to recognize sepsis earlier, and treat it more effectively.”Global Alliance for
Sepsis 2016
Source: Daniels R. Surviving the first hours in sepsis: getting the basics right (an intensivist's perspective), J Antimicrob Chemother. 2011 Apr;66 Suppl 2:ii11‐ii23. DOI: 10.1093/jac/dkq515.
“If sepsis is recognized and treated within the first hour, the chanceof survival is over 80%. Widespread effective early‐recognition and treatment systems are critical to increasing sepsis survival rates” “For every hour of delay in recognition and treatment of sepsis, mortality goes up 7.6 %.” (World Sepsis Day, 2016).
Sepsis Fact –
At BSLMC sepsis mortality rate is almost 150% less if recognized and treated early.
Diagnosed & Treated late
Recognized & Treated early
Source: Internal Data (Premier), Baylor St. Luke's Medical Center Sepsis Initiative.

Sepsis e‐Learn: Module 1
8
Two Most Important Factors in Decreasing Sepsis Mortality
Early Recognition
RN/MD
Timely screening & Assessment in the
ED
Acute Care Units
ICU
Early Intervention
MD/RN
Timely & appropriate medical treatment utilizing the
“Sepsis Order Set “
with accurate documentation with “Sepsis Notes 1 & 2 “
Early RecognitionThe screening/assessment process vary slightly depending on the location of the patient...
ED
1. Triage Sepsis Screen
If positive…
2. RN Delegated Lab Orders
Lactic Acid, Glucose, CMP, CBC
If positive…
3. Secondary Sepsis Screen
If positive…
4. MD Intervention
Acute Care Units
1. qSOFA/qShift Sepsis Screen &/or
Electronic SIRS Best Practice Alert (BPA)
If positive…
2. RN Delegated Lab Orders
Lactic Acid, Glucose, CMP, CBC
If positive…
3. Secondary Sepsis Screen
(Rapid Response Team)
If positive…
4. MD Intervention
ICU
1. Electronic SIRS Best Practice Alert (BPA)
If positive…
2. Secondary Sepsis Screen
(ICU RN)
If positive…
3. MD Intervention
Sepsis e‐Learn: Module 1
9
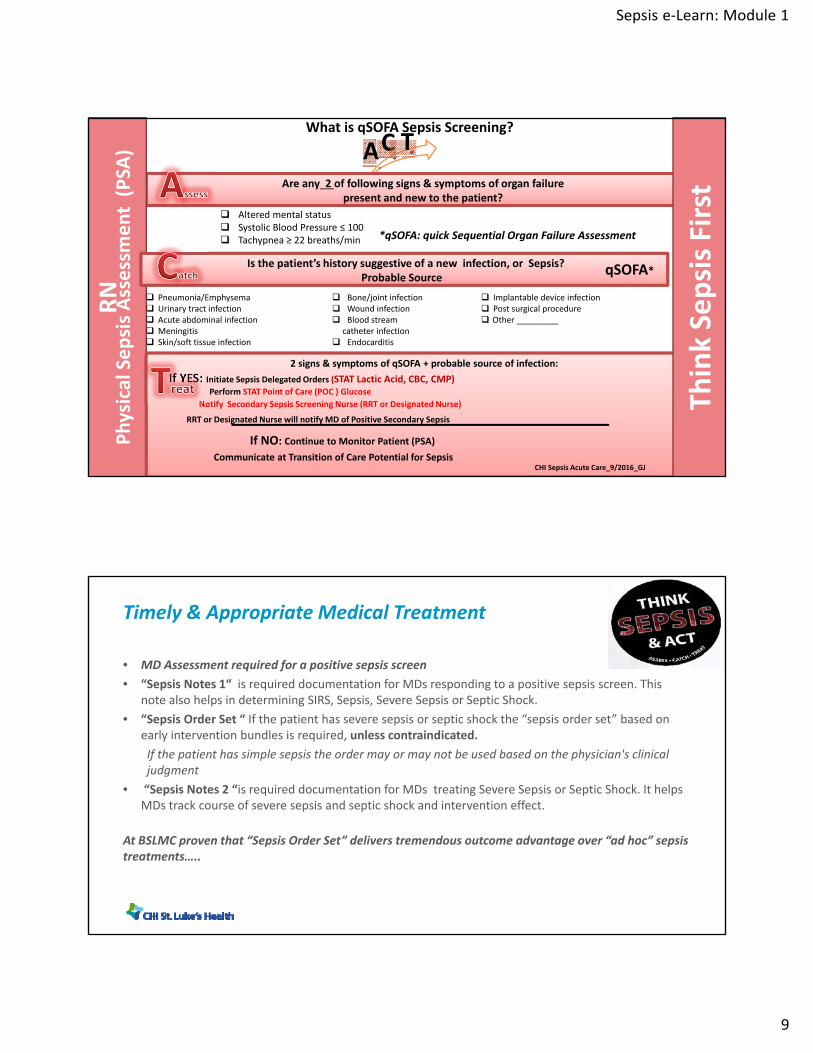
AC T
Are any 2 of following signs & symptoms of organ failurepresent and new to the patient?
RN
Physical Sepsis Assessment (PSA
)
Pneumonia/Emphysema Urinary tract infection Acute abdominal infection Meningitis Skin/soft tissue infection
Bone/joint infection Wound infection Blood stream
catheter infection Endocarditis
Implantable device infection Post surgical procedure Other _________
Altered mental status Systolic Blood Pressure ≤ 100 Tachypnea ≥ 22 breaths/min
2 signs & symptoms of qSOFA + probable source of infection:
If YES: Initiate Sepsis Delegated Orders (STAT Lactic Acid, CBC, CMP)Perform STAT Point of Care (POC ) Glucose
Notify Secondary Sepsis Screening Nurse (RRT or Designated Nurse)
RRT or Designated Nurse will notify MD of Positive Secondary Sepsis
If NO: Continue to Monitor Patient (PSA)
Communicate at Transition of Care Potential for Sepsis
ThinkSepsis First
Is the patient’s history suggestive of a new infection, or Sepsis?Probable Source
qSOFA*
CHI Sepsis Acute Care_9/2016_GJ
*qSOFA: quick Sequential Organ Failure Assessment
What is qSOFA Sepsis Screening?
Timely & Appropriate Medical Treatment
• MD Assessment required for a positive sepsis screen
• “Sepsis Notes 1“ is required documentation for MDs responding to a positive sepsis screen. This note also helps in determining SIRS, Sepsis, Severe Sepsis or Septic Shock.
• “Sepsis Order Set “ If the patient has severe sepsis or septic shock the “sepsis order set” based on early intervention bundles is required, unless contraindicated.
If the patient has simple sepsis the order may or may not be used based on the physician's clinical judgment
• “Sepsis Notes 2 “is required documentation for MDs treating Severe Sepsis or Septic Shock. It helps MDs track course of severe sepsis and septic shock and intervention effect.
At BSLMC proven that “Sepsis Order Set” delivers tremendous outcome advantage over “ad hoc” sepsis treatments…..

Sepsis e‐Learn: Module 1
10
Sepsis – 2014 SummaryPulmonary Section Meeting3/11/2015
John Sabo RN RRTCHI St. Luke’s Health – Baylor St. Luke’s Medical Center
Treated with Order Set Treated without Order Set
Expired 3 20
n 51 53
51 53
320
Order Set Utilization & Sepsis Mortality
5.9 %Mortality
37.7 %Mortality
Fact: A study at BSLMC demonstrated a marked decrease in mortality when the order set was utilized properly (all component of the 3 hour sepsis bundle).
Source: Ike C, Freibott P, Myers K, et al. Impact of order set utilization for the treatment of patients with severe sepsis and septic shock. Crit Care Med. 2015 Dec;43:12(Suppl):267. Abstract 1061.
34%
14%
20%23%
47%50%
46%43%
26%
38%
31%35% 34%
30.2%
34.4%
26.3%
35.0%
32.5%
20.6% 20.2%
36.1%
26.3%
37.5%
30.9%29.4%
34.7%
0%
10%
20%
30%
40%
50%
60%
2015 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Severe Sepsis/Septic Shock Mortality& Order Set Utilization
Order Set Utilization (%) Severe Sepsis & Septic Shock Mortality (%)
Fact: Statistics demonstrate at BSLMC the months with the lowest Severe Sepsis & Septic Shock mortality were when the order set was utilized the most.
Source: Internal Data, Baylor St. Luke’s Medical Center Sepsis Initiative.

Sepsis e‐Learn: Module 1
11
n = 34
By the way, an interesting fact:The Sepsis Order Set is only utilized 30% of the time.
The following chart indicates why MDs at BSLMC do not use the order set…
Source: Internal Data, Baylor St. Luke's Medical Center Sepsis Initiative.
Sepsis – What has been done to decrease mortalityImproved Sepsis Assessment & recognition
“Doing the Right Things at the Right Time”
Assessment & Recognition
1. Improved ED Triage process with documentation & delegated orders.
2. Improve the current electronic “Best Practice Alert” (BPA).
3. Improved Acute Care Sepsis Screening with Q Shift Sepsis Assessment.

Sepsis e‐Learn: Module 1
12
Intervention
Tools & Processes to improve MD Sepsis Documentation
Tools & Processes to increase MD Sepsis Order Set Utilization
Sepsis – What has been done to decrease mortalityImproved Sepsis Interventions
“Doing the Right Things at the Right Time”
At the March 2016 the Medical Executive Committee (MEC) motioned, seconded & carried to require the utilization of the Sepsis Notes & Sepsis Order Set in appropriate patients……
Dynamic Sepsis Assessment and InterventionCritical
“Sepsis is a highly dynamic process, especially at onset. It requires ongoing assessment of severity, organ dysfunction, intervention effect, and stepwise escalation or de‐escalation of care.”
Ivor Douglas MD, co‐chair Surviving Sepsis Campaign Writing Committee at BSLMC 11/16/2016
Sepsis e‐Learn: Module 1
13
End module 1