survival and follow-up after pacemaker implantation: a comparison of patients with sick sinus...
TRANSCRIPT

Survival and Follow-up After PacemakerImplantation: A Comparison of Patients WithSick Sinus Syndrome, Complete Heart Block,and Atrial Fibrillation
ECKHARD ALT. REINHARD VOLKER. ALEXANDER WIRTZFELD,and KURT ULMFrom the L Medical Clinic, and Institute of Statistics and Epidemiology.Technical University of Munich, Munich. W. Germany
ALT, E., ET AL.: Survival and follow-up after pacemaker implantation: A comparison of patieuts withsick sinus syndrome, complete heart block, and atrial flbrillation. The number of patients receivingcardiac pacemakers for sick sinus syndrome (SSSJ has increased considerably in recent years. The literaturehas suggested Ihat patients with sick sinus syndrome have a shorter life expectancy with pacemakertherapy than patients with total heart block or atrial fibriilation. We studied the survivnl rate of 1,049patients with complete heart block, 592 with sick sinus syndrome and 447 with atrial ftbrillation. After 10years we found a survival rate of 54.5% for patients paced for SSS, 34.4% for those with complete heartblock, and 24.7% for those with atrial jibrillation (statistical significance: SSS—heart block: p < 0.05: SSS—atria/ fibrillation: p < 0.01; heart block—atrial jibrillation: NS}. Considering the calculated survival ratesof a comparable normal population (i.e., 56.5%; 41.2%; 47.8%), ihe differences in survival expectancy areeven more pronounced (SSS-normaJ: NS, heart block-norrnal p <0.05; atrial/ibrillation-normal: p < 0.05).For patients with sick sinus syndrome, the life expectancy parallels that of the general population, whilethat of patients with complete heart block or atrial fibrillation have a life expectancy thai is considerablylower. (PACE, Vol. 8, November-December, 1Q85]
survival with pacing, complications, sick sinus syndrome
Introduction
The indications for pacemaker therapy havechanged considerably during recent years. Whilein 1968 patients with sick sinus syndrome com-prised only 5% of those treated with permanentpacemakers at the Technical University of Mu-nich, in 1984 the number increased to 43%. In theUnited States, the percentage of patients with sicksinus syndrome amounts to 50% of the entirepacemaker population.'"'
Reasons for this increase in the types of indi-cations for pacing include the evolution of pace-maker therapy from a life-saving measure, to one
Address fnr reprints: Dr. Eckhard Alt. I. Medical Clinic. TUMunich. Ismaninger Str. 22. aooo Munich 80. W. Germany.
Received April 30, 1985: revision received |uly 15. 1985; ac-cepted |uly 17. 1985.
aimed at improving the quality of life,̂ ^ Parallelto this development, the improved surgical tech-nique reduced the risks of surgery even for elderlypatients; new technology led to a considerable re-duction of the size and weight of the pacemaker.Improved preoperative diagnostic possibilities,such as Holter ECG monitoring, have uncoveredfar more rhythm disturbances and patients withsick sinus syndrome than were suspected by sim-ple ECG recordings."* Because of the steadily risingnumber of pacemaker implantations, the percent-age of patients with sick sinus syndrome is of spe-cial interest.
Differences exist in the literature concerning theprognosis for SSS patients, and life-expectancystudies were only approximations.^"^ The greatestdiscrepancies have been found in studies not usingcumulative survival analysis.'""''' In particular, arelatively poor prognosis was found in small groupswith other serious diseases.'•* Obviously, the over-
PACE. Vol. 8 November-December 849
ALT. ET AL.
Indication
Heart BlockSick Sinus SyndromeAtrial FibrillationOther
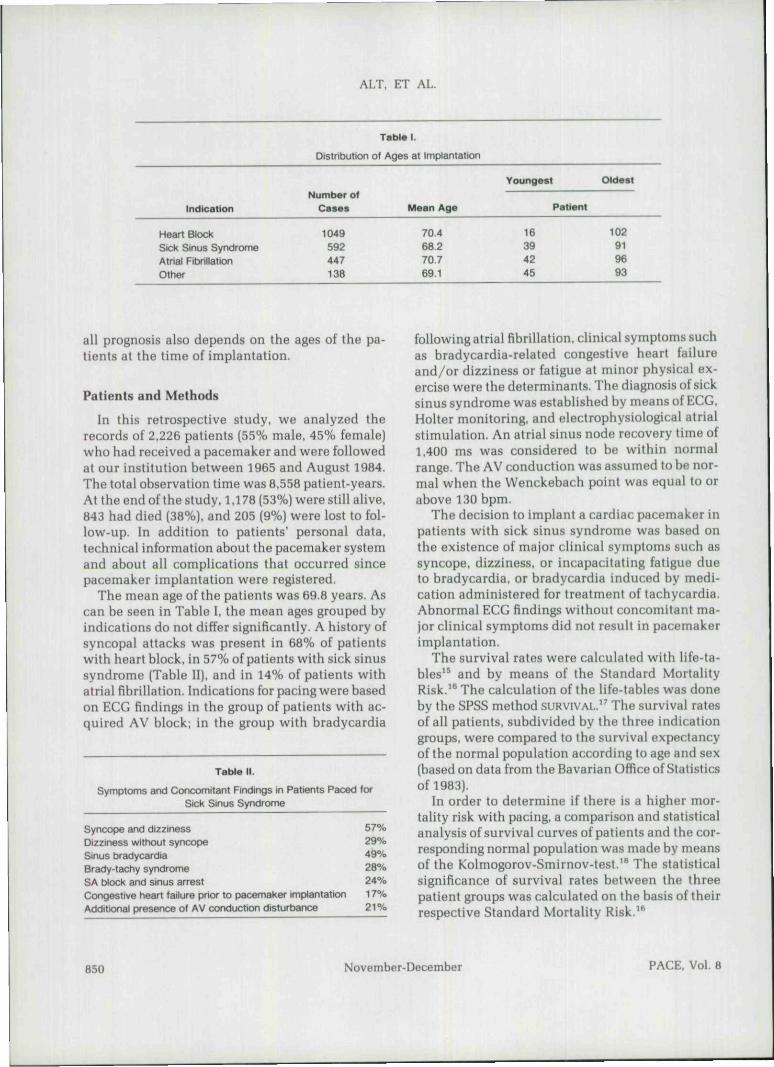
Table 1.
Distribution of Ages at Implantation
Number olCases
1049592447138
Mean Age
70.468.270.769.1
Youngest
Patient
16394245
Oldest
102919693
all prognosis also depends on the ages of the pa-tients at the time of implantation.
Patients and Methods
In this retrospective study, we analyzed therecords of 2,226 patients [55% male. 45% female)who had received a pacemaker and were followedat our institution between 1965 and August 1984.The total observation time was 8,558 patient-years.At the end of the study, 1.178 (53%) were still alive,843 had died (38%). and 205 (9%) were lost to fol-low-up. In addition to patients' personal data,technical information about the pacemaker systemand about all complications that occurred sincepacemaker implantation were registered.
The mean age of the patients was 69.8 years. Ascan be seen in Table 1. the mean ages grouped hyindications do not differ significantly. A history ofsyncopal attacks was present in 68% of patientswith heart block, in 57% of patients with sick sinussyndrome (Table II), and in 14% of patients withalrial fibrillation. Indications for pacing were basedon ECG findings in the group of patients with ac-quired AV block; in the group with bradycardia
Table II.
Symptoms and Concomitant Findings in Patients Paced lorSick Sinus Syndrome
Syncope and dizziness 57%Dizziness without syncc^w 29%Sinus bradycardia 49%Brady-tachy syndrome 28%SA block and sinus arrest 24%Congestive heart failure prior to pacemaker implantation 17%Additional presence of AV conduction disturbance 2 1 %
following atrial fibrillation, clinical symptoms suchas bradycardia-related congestive heart failureand/or dizziness or fatigue at minor physical ex-ercise were the determinants. The diagnosis of sicksinus syndrome was established by means of ECG,Holter monitoring, and electrophysiological atrialstimulation. An atrial sinus node recovery time of1.400 ms was considered to be within normalrange. The AV conduction was assumed to be nor-mal when the Wenckebach point was equal to orabove 130 bpm.
The decision to implant a cardiac pacemaker inpatients with sick sinus syndrome was based onthe existence of major clinical symptoms such assyncope, dizziness, or incapacitating fatigue dueto bradycardia, or bradycardia induced by medi-cation administered for treatment of tachycardia.Abnormal ECG findings without concomitant ma-jor clinical symptoms did not result in pacemakerimplantation.
The survival rates were calculated with life-ta-bles^^ and by means of the Standard MortalityRisk.'* The calculation of the life-tables was doneby the SPSS method SURVIVAL." The survival ratesof all patients, subdivided by the three indicationgroups, were compared to the survival expectancyof the normal population according to age and sex(based on data from the Bavarian Office of Statisticsof 1983).
In order to determine if there is a higher mor-tality risk with pacing, a comparison and statisticalanalysis of survival curves of patients and the cor-responding normal population was made by meansof the Kolmogorov-Smirnov-test."* The statisticalsignificance of survival rates between the threepatient groups was calculated on the basis of theirrespective Standard Mortality Risk.'*
850 November-December PACE, Vol. 8

SURVIVAL AFTER PACER IMPLANTATION
Table III.
Survival Rate (percentage) of 2.226 Pacemaker Patients Grouped According to Indications and Compared to theUnpaced (termed 'normal") Population.
Years after Afl Patients sss Heart Block Atrial FibrillationHacemaKerImplantation
356
10
Paced
70.157.043435.0
Normal
80.168.353.144.4
Paced
77.Z67.860.054.5
Normal
82.873.062.356.5
Paced
69.556.242,934.4
Normal
78-966.850.641.1
Paced
66.550.833.827.7
Normal
79.567.353.747.8
Results
Tahle III shows the survival rates of all 2,226pacemaker patients. After three years, the entirepactimaker group had a lower survival rate (70.1%)than the expected survival rate of the normal pop-ulation (80.1%). In the follow-up extending up to10 years after pacemaker implantation, the sur-vival rate for the entire group of pacemaker pa-tients was equal to that of the normal population.
After 10 years, 35% of the pacemaker patients and44% of the normal population are still alive (TahleIII). By grouping the survival rates according toindications for pacing, it is evident that patientswith sick sinus syndrome have the best survivalrate over the follow-up period of 10 years; thosewith complete heart block have a higher survivalthan those with atrial fibrillation (Fig. 1). The ac-tual survival rates after 10 years were 54.5% forpatients with sick sinus syndrome, 34.4% for pa-
O Sick Sinus SyndromeD Heart - Block
Atrial Fibrillation
6 7 8 9Years after implantation
10
Figure 1. Survival rate after pacemaker implantation o/palients with sick sinus syndrome, heartblock. (Htd nirin/ fibrillation.
PACE. Vol. 8 November-December 851

ALT. ET AL.
tients with complete heart block, and 24.7% forpatients with bradyarrhythmias.
To avoid misleading results when comparingnon-homogeneous groups of widely varying ageand sex. a comparison of life expectancies in thisstudy was done based upon the difference of themean of the expectancies of the individual mem-bers within these groups compared to their cal-culated "normal" survival.
By the end of 10 years with a pacemaker, pa-tients with sick sinus syndrome have nearly thesame life expectancy as the normal population,that is 54.5% for pacemaker patients compared to56.5% for the normal population. The SSS patientsalso have the longest survival of the paced groupsstudied. This difference is not significant (Fig. 2).Patients paced for complete heart block have a34.4% survival rate compared to 41.2% for thenormal population (p < 0.05). It should be noted(Fig. 3) that the greatest difference in survivalcurves between paced patients and the normalpopulation occurs mainly during the first threeyears after implantation. After that, the curves arealmost parallel. Patients with atrial fibrillation (Fig.
4) have the lowest life expectancy in comparisonto the normal population after the 10-year follow-up period (p < 0.05). The survival rate of patientspaced for bradycardia following atrial fibrillationreveals a 10-year survival of only 24.7%. whereasthe calculated survival for the normal populationis 47.8% for this period of time.
The complication rate of pacing must be con-sidered when assessing the benefit of a greatersurvival expectancy with pacing. Based on allnoted complications subsequent to pacing, weplotted the survival curve for all patients both withand without complications and compared it to thegroup free of complications (Fig. 5). Since the com-plications in all the 2,226 patients were evenlydistributed among the three groups of 1 patient,this curve can he considered representative for anyone of the groups. As shown in Figure 5. there isa notable difference between 35.0% cumulativesurvival rate for all patients compared to an 11.5%survival rate for only those patients that were freeof any complications. The difference of more than20% between the two curves represents compli-cations that accumulated over the 10-year period.
i 30
O 20
10
0
Q Sick Sinus SyndromeO Normal Population
-I 1 1 1 r"6 7 8 9 10
Years after ImplantationFigure 2. Survival rate after pacemaker implantation of patients with sick sinus syndrome com-pared to their mean individual life expectancies adjusted to the age and sex for normal populolion.
852 November-December PACE. Vol. 8

SURVIVAL AFTER PACER IMPLANTATION
a Heart BlockO Normal Population
41.2
p<0,05
0 1 2 3 4 5 6 7 6 9Years after Implantation
Figure 3. Survival rate after pacemaker implantation of patients ivith heart block compared totheir mean individual life expectancies adjusted to the age and sex for normal population.
100D Atrial FibrillationO Normal Population
p<0,05
O
0 1 2 3 4 5 6 7 89Years after Implantation
Figure 4. Survival rate after pacemaker implantation of patients with atrial /ibrillation comparedto their mean individual life expectancies adjusted to the age and sex for normal population.
PACE. Vol. 8 November-December 853

ALT, ET AL.
100 . O Patients with or without ComplicationsD Patients free of Complications
35.0
pc:0,05
0 1 2 3 4 5 6 7 8 9Years after Implantation
Figure 5. Survival rate of all paced palienls: curves for survival without pacing complicationsand for survival with or withoul complicalions.
Discussion
The present study shows the survival rate ofpacemaker patients with sick sinus syndrome asbeing nearly identical to that of the normal pop-ulation, and as significantly better than those ofpatients with complete heart block or bradycardiafollowing atrial fibrillation. This does not confirmresults of some other reports.^"*^'' The differencemight be explained by the fact that some of thestudies had few patients, with a disproportionatelyhigh number of patients suffering from other se-vere diseases. In one of these studies/** 45% of thepatients had a previous history of valve disease,myocardial infarction, or severe congestive heartfailure, evidently reducing life expectancy.
Our findings and prognosis for paced SSS pa-tients do agree with those of other investiga-tors.^"^" From the literature'^^^ it is known thatthe prognosis of patients with sick sinus syndrome,even without pacing, is rather similar to that ofthe normal population. Therefore, in many casesthe indication for pacemaker therapy in patientswith SSS is established mainly to improve the
quality of life, unlike the situation for patients withcomplete heart block. When indicating permanentpacing for sick sinus syndrome, this fact alsoshould be considered.
When the survival rate of pacemaker patientsas a whole is compared to the individual life ex-pectancy of the normal population (Table III), it isobvious that the highest mortality of paced patientsoccurs during the first few years. In patients withsick sinus syndrome, this effect is less pronouncedthan in patients with complete heart block or bra-dycardia following atrial fibrillation. Survival ofpatients who have sick sinus syndrome or com-plete heart block nearly parallels the slope of thematched population after the third year, while inthe group of patients with bradycardia followingatrial fibrillation, the survival rate of paced pa-tients gets continuously worse when compared totheir matched population.
Of patients with sick sinus syndrome, 17% alsohad congestive heart failure, and 57% had syn-copal attacks prior to pacemaker implantation; inpatients with bradycardia following atrial fibril-lation, the indication for pacing was established
854 November-December PACE. Vol. 8

SURVIVAL AFTER PACER IMPLANTATION
in only 14% due to syncopal attacks. This mightbe an indication of the more serious underlyingmyocardial disease usually found in these patients,which might explain the difference in survival.
In considering the use of permanent pacing, thepossibility of complications should be kept inmind. This is particularly true for patients withsick sinus syndrome, as cardiac pacing is oftenused to relieve incapacitating symptoms rather
than to prolong life.'^ Although complications ofpacemaker therapy can usually be corrected, theyare troublesome for the patient. Therefore, in pa-tients with ECG findings of sick sinus syndromewho have no major clinical symptoms, the benefitsto be achieved from pacing should be carefullyweighed against the possible complications re-sulting from pacing.
References
1. Friedman, H.S.: Are too many permanent pace-makers being implanted? PACE. 4:232. 1981.
2. Kaplan. B.: Sick sinus syndrome. Arch. Inlern. Med.,138:28. 1978.
3. Vaisrub, S.: The not-so-sick sinus. ]AMA, 243:2068.1980.
4. Shaw. D.B,, Kekwick. C.A.: Potential candidatesfor pacemakers: Survey of heart block and sino-atrial disorder (sick sinus syndrome). Br. Heart /..40:99. 1978.
5. Wirtzfeld. A.. Himmler. F.C., Prauer. H.W.. et al.:Atrial and ventricular pacing in patients with thesick sinus syndrome. In C. Meere (Ed.): Proceedingsof the VI"' World Symposium on Cardiac Pacing.Montreal, PACESYMP. 1979. Chap. 15-5.
6. Blomer. H.. Wirtzfeld. A.. Delius, W,. et al.: DasSinusknotensyndrom. Straublng. Perimed Verlag,1977.
7. Aroesty, J.M., Cohen, S.M., Morkin, E,: Bradycar-dia-tachycardia syndrome. Results in twenty-eightpatients treated by combined pharmacologic ther-apy and pacemaker implantation. Chest, 66:257.1974.
8. Breivik. K.. Ohm. O.-f.. Segadal. L.: Sick sinus syn-drome treated with permanent pacemaker in 109patients. Acta Med. Scand.. 206:153. 1979.
9. Hager. W,: Spatergebnisse nach herzschrittmach-erimplantation. Dtsch. Med. Wochenschr.. 99:1345.1974.
10. Hartel. G.. Talvensaari, T.: Treatment of sinoatrialsyndrome with permanent cardiac pacing in 90patients. Acta Med. Scand.. 198:341. 1975.
11. Rettig, G., Schietfer. H.. Doenecke. P., et al.: Lang-zeitprognose bei Schrittmacherpatienten. Herz.Kreislauf.. 7: 10:497. 1975.
12. Rokseth, R., Hatle. L.: Prospective study onthe occurrence and management of chronicsinoatrial disease, with foUow-up. Br. Heart }..36:582. 1974.
13. Wirtzfeld. A,, Himmler, F.Ch.. Blomer. H.: Klin-ische gesichtspunkte bei bradycarden herzrhyth-
musstbrungen. Verh. Dtsch. Ges. Herz. Kreislauf-/orsch.. 47:98. 1981.
14. Wohl, A.M.. Laborde. N,I,, Atkins, J.M.. et al.:Prognosis of patients permanently paced for sicksinus syndrome. Arch. Intern. Med.. 136:406.1976.
15. Cutler. S.J.. Ederer, F.: Maximum utilisation of thelife-table method in analysing survival. /. Chron.Dis., 11:699, 1958.
16. Woolson. R.V.. Tsuang, M.T.. Fleming. ].A.: Amethod for analysing mortality data collected infollow up studies. Meth. In/orm. Med., 17:116.1978.
17. Nie, N.H., Hull. CH,: Statistik-Programm-Systemfur die Sozialwissenschaften. Stuttgart. GustavFischer Verlag. 1980.
18. Fleming. T,R,. O'FoIIon. J.R., O'Brien. P.C: Modi-fied Kolmogorov-Smirnov test procedures with ap-plication to arbitrarily right-censored data. Bio-metrics, 36:607. 1980,
19. van Hemel, N.M.. Schaepkens van Riempst. A.L.E.,Bakema, H,, et al.: Long-term follow-up after pace-maker implantation in sick sinus syndrome. PACE,4:8. 1981.
20. Simonsen, E.: Der natiirliche verlauf des sinus-knoten-syndroms. Vitalext. 2:3, 1981.
21. Escher, D.J.W,, Furman. S., Fisher. ID.: The naturalhistory of the paced patient with sick sinus nodesyndrome as compared with patients with heartblock, PACE. 4:A-43. 1981 (Abstract).
22. Fisher, ].D.. Furman, S.: Pacing in the sick sinussyndrome: Profile and prognosis, PACE, 4:A-45,1981 (Abstract).
23. Nolan, S.P.. Crampton, R.S., McGuire. L.B.. et al.:Factors influencing survival of patients with per-manent cardiac pacemakers. Ann, Surg,, 185:123.1977.
24. Seipel. L., Pietrek. G., Kdrfer. R., et al.: Prognosenach schrittmacherimplantation. Internist, 18:21.1977.
25. Shaw, D.B., Holman, R.R.. Cowers, J.I.: Survival insinoatrial disorder (sick-sinus-syndrome). Br. Med./., 280:139, 1980.
PACE. Vol. 8 November-December 855
