surgery for shoulder instability len funk
TRANSCRIPT

Surgery for Shoulder Instability
Lennard Funk

Rugby Injury• 24 year old
• Semi-Pro Rugby player
• Tackling injury
• Unable to continue
• Mid-season
• Struggling with weights
• Unable to play at same level
Decision Making
1.Does he need surgery?
2.Why?
3.When?
4.How?
5.Recovery Times?

Factors:
1.What is the extent of injury?
2.Time of Season?
3.Return to play with/without surgery?

Bony BankartHAGL
SLAP
Rotator Cuff Tear
Reverse Bankart

Lesions
Major ‘Minor’• Bony Bankart• ALPSA• Rotator Cuff Tear• HAGL
• Undisplaced Labral Tear• Partial Cuff Tear• ACJ Dislocation

L Funk / 2002
Case ExampleAge & Sex: 22yr Male
Semi-Pro Rugby Player
1st Disloc: Rugby Tackle 6 months agorelocated in A&E
Recurrences: 3 recurrences with rugby in ABER relocated each time
Other: Keen to return to rugby, but unable
MR Arthrogram Bony Bankart lesion & HAGL
Traumatic
RecurrentAnterior
Dislocation
Large lesion RepairBony Reconstructions
Polar ITraumatic Structural

Direct
Complex Labral
Bony BankartPTCT
Flexed Fall
Posterior Labral
RHAGL
Try Scorer
BankartSLAP
Rotator Cuff
Tackler
BankartSLAPHAGL
Mechanisms of Injury

Clinical Exam: Instability in Athletes
• True Instability• Dislocation• Subluxation• Apprehension• Large lesions
• Subclinical Instability
• Dead Arm in ABER• Pain in ABER• Clunking• No Apprehension• Smaller lesions


Posterior

Modified O’Brien’s Test (MOB)Wrightington Posterior Instability Test (WPIT)
WPIT - Wrightington Posterior Instability TestOwen, Mackenzie, Boulter, Funk, 2014

MR Arthrogram v. Scope
Sensitivity Specificity Accuracy
SLAP 0.42 0.92 77%
Rotator Cuff Tear
0.50 0.86 83%
Hill Sachs 0.91 0.78 90%
Bankart 0.85 0.83 86%
Karson, Geoghan & Funk, SECEC 2011

Radiologist Locality
• MRA is not 100% sensitive or specific and does not negate arthroscopy.
• The accuracy of MRA to determine the location of a labral tear was low
• There is a lower diagnostic accuracy of posterior than anterior labral lesions
• Accuracy of glenohumeral MRA diagnosis is achieved with increased experience of radiologist within specialist units and regular surgical feedback of cases
• Negative scan results are not absolute and should not preclude investigation with arthroscopy
Karson, Geoghan & Funk, SECEC 2011

• An experienced Shoulder Surgeon better
• Can correlate with clinical context
• Experience of reviewing Scopes & Scans
• Early Surgery:
• Major structural lesions
• Late in Season
• Unable to Return
• Rehab & Return:
• Minor structural lesions
• Early season
Timing of Surgery

Types of Surgery
• Mostly Arthroscopic Direct Repairs
• Latarjet for High-Risk/Revision

Bankart Repair

Latarjet

• Anterior Instability
• Revision surgery (even without bone loss)
• Chronic Bony Bankart (> 3months)
• Any Bony Glenoid Loss
• True dislocation in Front Row forward (Rugby Union)
• Higher level of sports
Latarjet in Athletes

Safe Zone

Post-Op Rehab Phase and Sport specific - Not time based or ‘Accelerated’
Phase 1: (Level 1 Exercises)
Core stability & Scapula control
Proprioceptive exercises (minimal weightbearing below 90 degrees)
Active assisted ROM as comfortable (in 'safe zone' )
Do not force or stretch
No combined abduction & external rotation
Phase 2: (Level 2 Exercises)
Progress active assisted to active ROM as comfortable
Phase 3: (Level 3+ Exercises)
Regain scapula & glenohumeral stability working for shoulder joint control rather than range
Gradually Strengthen
Plyometrics and pertubation training

Creighton et al. CJSM 2010
Our Results
• Arthroscopic Soft-tissue Bankart’s only
• Primary Procedures
• January 2005 - January 2007
• 128 shoulders
• Return to Sport = 4.8 months
• Return to Sport at same level = 84%
• Recurrent Instability = 6% (7/128)

Rugby Results ‘03-’05
Pain Satisfaction (%) Playing at previous level
Pre-op 5 11% 0%
3 months 10 87% 89%
6 months 12 93% 94%
L Funk , K Roney, CJSM, 2007

Return to Play
Repair! Months-post.op!SLAP! 2.6!Ant.*&*SLAP! 3!Post.*&*SLAP! 4!Ant.*Post.*&*SLAP! 5.5!
L Funk , K Roney, CJSM, 2007

Atraumatic Instability
L Funk / 2002
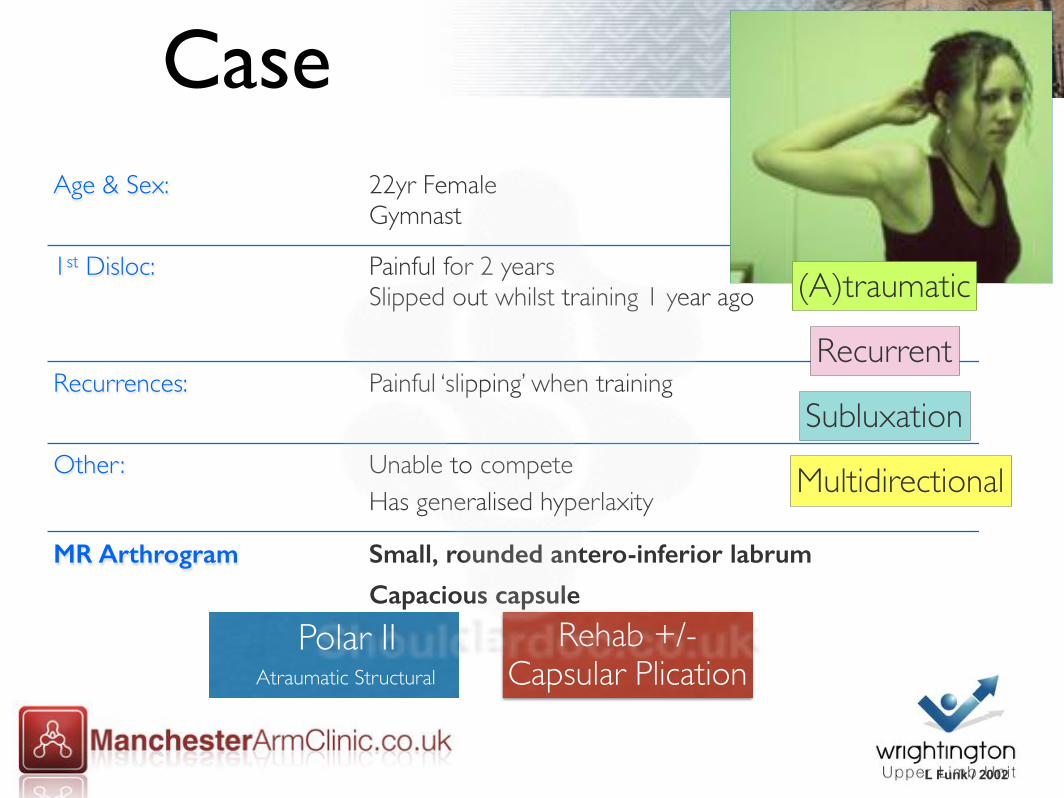
CaseAge & Sex: 22yr Female
Gymnast
1st Disloc: Painful for 2 years Slipped out whilst training 1 year ago
Recurrences: Painful ‘slipping’ when training
Other: Unable to competeHas generalised hyperlaxity
MR Arthrogram Small, rounded antero-inferior labrum
Capacious capsule
(A)traumatic
Multidirectional
Recurrent
Subluxation
Polar IIAtraumatic Structural
Rehab +/-Capsular Plication

Rehab• Optimise:
• Core
• Scapula
• Kinetic Chain
• Psychology

Decision Making

IGHL Hammock

Capsular Plication

Thank You

Thank [email protected]