stroke in patients with aortic...
TRANSCRIPT
1939
The most recent US and European guidelines for treatment of valvular heart disease recommend oral anticoagulation
(OAC) for stroke prophylaxis in all patients with aortic ste-nosis (AS) complicated by atrial fibrillation (AF).1,2 This rec-ommendation differs from nonvalvular AF, where the decision to start OAC is guided by the CHA
2DS
2-VASc (congestive
heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke/transient ischemic attack, vascular disease, age 65–74 years and female sex) risk scheme.3 The guideline discrepancy is based on observational studies indicating that calcific AS is an independent risk factor for stroke,4 which may predict stroke even in the absence of AF.5 However, limited evidence exists on the effectiveness of the CHA
2DS
2-VASc scores in
AS populations, and particularly in less severe AS where data are equivocal with regards to an increased stroke risk per se.6 We hypothesized that calcific AS is associated with the same pathobiology underlying an increase in the CHA
2DS
2-VASc
score and that the latter, therefore, could be particularly use-ful for stratifying risk of stroke in earlier stages of AS. This study was, therefore, undertaken to examine the ability of the CHA
2DS
2-VASc score to predict ischemic stroke in asymp-
tomatic patients with AS with and without coexisting AF. Because risk of new-onset AF and thromboembolism may dif-fer substantially in relation to aortic valve replacement (AVR) with or without coronary artery bypass grafting (CABG), the primary study hypothesis was stratified by AVR with and
Background and Purpose—There are limited data on risk stratification of stroke in aortic stenosis. This study examined predictors of stroke in aortic stenosis, the prognostic implications of stroke, and how aortic valve replacement (AVR) with or without concomitant coronary artery bypass grafting influenced the predicted outcomes.
Methods—Patients with mild-to-moderate aortic stenosis enrolled in the Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) study. Diabetes mellitus, known atherosclerotic disease, and oral anticoagulation were exclusion criteria. Ischemic stroke was the primary end point, and poststroke survival a secondary outcome. Cox models treating AVR as a time-varying covariate were adjusted for atrial fibrillation and congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke/transient ischemic attack, vascular disease, age 65–74 years and female sex (CHA
2DS
2-VASc) scores.
Results—One thousand five hundred nine patients were followed for 4.3±0.8 years (6529 patient-years). Rates of stroke were 5.6 versus 21.8 per 1000 patient-years pre- and post-AVR; 429 (28%) underwent AVR and 139 (9%) died. Atrial fibrillation (hazard ratio [HR], 2.7; 95% confidence interval [CI], 1.1–6.6), CHA
2DS
2-VASc score (HR 1.4 per unit; 95%
CI, 1.1–1.8), diastolic blood pressure (HR, 1.4 per 10 mm Hg; 95% CI, 1.1–1.8), and AVR with concomitant coronary artery bypass grafting (HR, 3.2; 95% CI, 1.4–7.2, all P≤0.026) were independently associated with stroke. Incident stroke predicted death (HR, 8.1; 95% CI, 4.7–14.0; P<0.001).
Conclusions—In patients with aortic stenosis not prescribed oral anticoagulation, atrial fibrillation, AVR with concomitant coronary artery bypass grafting, and CHA
2DS
2-VASc score were the major predictors of stroke. Incident stroke was
strongly associated with mortality.Clinical Trial Registration—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00092677.
(Stroke. 2014;45:1939-1946.)
Key Words: aortic valve stenosis ◼ cardiac surgical procedures ◼ risk factors ◼ stroke
Stroke in Patients With Aortic StenosisThe Simvastatin and Ezetimibe in Aortic Stenosis Study
Anders M. Greve, MD, PhD; Morten Dalsgaard, MD, PhD; Casper N. Bang, MD, PhD; Kenneth Egstrup, MD; Simon Ray, MD; Kurt Boman, MD; Anne B. Rossebø, MD;
Christa Gohlke-Baerwolf, MD; Richard B. Devereux, MD; Lars Køber, MD; Kristian Wachtell, MD, PhD
Received February 28, 2014; final revision received April 18, 2014; accepted April 29, 2014.From the Department of Medicine B, The Heart Center, Rigshospitalet, Copenhagen, Denmark (A.M.G., M.D., C.N.B., L.K.); Department of Cardiology, OUH
Svendborg Sygehus, Denmark (K.E.); Department of Cardiology, Manchester Academic Health Sciences Center, Manchester, United Kingdom (S.R.); Department of Medicine, Institution of Public Health and Clinical Medicine, Umeå University, Skelleftå, Sweden (K.B.); Department of Cardiology, Oslo University Hospital, Ullevål, Oslo, Norway (A.B.R.); Department of Cardiology, Herz-Zentrum Bad Krozingen, Bad Krozingen, Germany (C.G.-B.); Department of Cardiology, Weill Cornell Medical College, New York, NY (R.B.D., K.W.); and Department of Cardiology, Glostrup University Hospital, Copenhagen, Denmark (K.W.).
The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA. 114.005296/-/DC1.
Correspondence to Anders M. Greve, MD, PhD, Department of Medicine, B2142, The Heart Center, Rigshospitalet, 9 Blegdamsvej, DK-2100 Copenhagen, Denmark. E-mail [email protected]
© 2014 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.114.005296
by guest on May 22, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on May 22, 2018
http://stroke.ahajournals.org/D
ownloaded from

1940 Stroke July 2014
without concomitant CABG. A secondary end point was the effect of incident stroke on subsequent all-cause mortality in the operated and nonoperated patients, respectively. Thus, this study examined rates, predictors, and prognostic implications of ischemic stroke before and after AVR during extended fol-low-up in initially low-risk patients with asymptomatic AS not receiving OAC.
MethodsStudy SettingsThe study cohort consisted of participants in the Simvastatin Ezetimibe in Aortic Stenosis (SEAS) study, a multicenter, random-ized, double-blind, placebo-controlled study, investigating whether intensive lipid lowering with simvastatin/ezetimibe combination versus placebo could reduce the need for AVR and risk of cardio-vascular morbidity and mortality in 1873 patients. Inclusion criteria were age 45 to 85 years, asymptomatic mild-moderate AS (defined by the European Society of Cardiology guidelines as echocardio-graphic aortic valve thickening accompanied by Doppler-measured aortic peak flow velocity ≥2.5 and ≤4.0 m/s), and normal left ven-tricular (LV) systolic function.2 The most important exclusion criteria were systolic heart failure, diabetes mellitus, and clinically apparent vascular atherosclerosis. The main outcome including other specif-ics about study design, organization, and clinical measures has been published.7,8
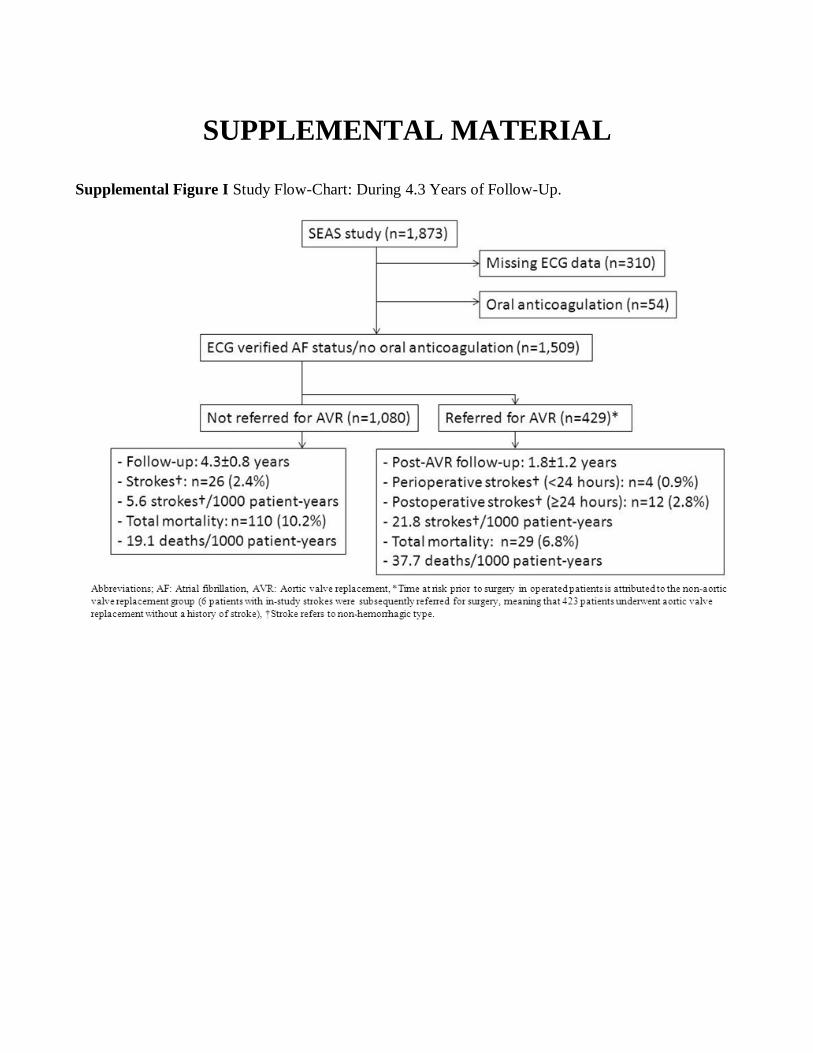
Design and Study PopulationThis study uses post hoc analysis of prospectively collected data from all patients with AF status documented by systematically read base-line ECGs (n=1563) in the SEAS study to examine predictors and prognostic implications of ischemic stroke before and after AVR in initially asymptomatic patients with mild-to-moderate baseline AS not receiving OAC (Figure I in the online-only Data Supplement). Because of exclusion of diabetes mellitus, established vascular ath-erosclerosis, and heart failure, a CHA
2DS
2-VASc score of 4 was by
default the highest value (concomitant hypertension, age ≥75 years and female sex). Informed consent was obtained from each patient, and the SEAS study protocol, covering also this substudy, conforms to the ethical guidelines of the 1975 Declaration of Helsinki as re-flected in a priori approval by the participating countries’ human re-search ethics committees.
ElectrocardiographyECG study protocol reading procedures and reproducibility have been published.9 In short, ECGs were recorded at the local study centers at a paper speed of 25 or 50 mm/s, after which they were sent to the SEAS electrocardiographic corelab at Rigshospitalet, Copenhagen, Denmark. AF (paroxysmal, persistent, or permanent), defined by the standard ECG criteria (Minnesota code 8-3), was determined by a physician blinded to the randomization and all clinical data.10
EchocardiographyEchocardiographic study protocol, reading procedures, and reproduc-ibility have been published.11 In short, transthoracic echocardiograms were read blinded at the SEAS echocardiography core laboratory lo-cated at Haukeland University Hospital in Bergen, Norway. Aortic valve area was calculated by the continuity equation,12 in accordance with recent recommendations,13 averaged over 10 consecutive beats in patients with AF. LV dimensions and wall thicknesses were mea-sured on 2-dimensional images following the American Society of Echocardiography guidelines, and LV mass calculated using an ana-tomically validated formula.14,15 Left atrial volumes were measured in LV end diastole and end systole by the modified Simpons mono-plane method in the apical 4-chamber view.15 Mitral regurgitation was assessed by color Doppler using the previously described 4-point
grading scale, grade ≥2 corresponding to a moderate-to-severe mitral regurgitation.16
Stroke DefinitionsIschemic stroke before and after AVR was classified by an indepen-dent End point Committee, according to an end point manual pre-specified by the SEAS Steering Committee.7 Diagnosis of stroke required evidence of a neurological deficit, usually localized, lasting ≥24 hours or until death (if death occurred <24 hours after onset of neurological symptoms) and confirmation by diagnostic testing (eg, computed tomography or MRI). The clinical characteristics of stroke included the sudden onset of a deficit typically manifested as reduced consciousness, disturbed vision, paresis or paralysis of ≥1 extremi-ties, sensory impairment, speech impairment, central cranial nerve dysfunction, memory defect, ataxia, and movement disorder. Strokes that fulfilled the above clinical criteria were classified as ischemic un-less the stroke was clearly hemorrhagic judged by a cranial computed tomography, MRI, and blood in spinal fluid. Hemorrhagic strokes were not included in this study’s end point.
Statistical AnalysisData were analyzed using the Statistical Analytical Software version 9.2 (SAS, Cary, NC). Continuous data are expressed as mean±SD and categorical variables as proportions. Differences in discrete and con-tinuous variables were evaluated by χ2, Fisher exact, Wilcoxon, and the Student t tests as appropriate. To isolate the predictive values of echocardiographic and clinical covariates for ischemic stroke, patients receiving OAC (n=54, of which 85% [n=46] were diagnosed with AF) were excluded (Figure I in the online-only Data Supplement). Baseline variables differing (P<0.10) between patients experiencing versus re-maining free from incident ischemic stroke (CHA
2DS
2-VASc, body
mass index, diastolic blood pressure, AF, diuretics, β-blockade, and aortic valve area index) were entered into univariate Cox regression models. Randomized treatment and LV ejection fraction were forced covariates in univariate Cox models because of clinical trial design of SEAS and importance of LV systolic function for clinical evaluation of need for AVR. Variables relating to incident stroke in the univariate Cox analyses were examined in multivariable Cox models using forward selection to eliminate nonsignificant variables. Three separate Cox pro-portional hazard models were used to identify the independent predic-tors of stroke with respect to AVR. The first model censored patients at the time of AVR provided that no stroke had occurred before the procedure. The second model assessed all strokes by including AVR as a time-dependent covariate.17 To account for perioperative strokes that may have resulted from intraoperative dislodgment of intra-aortic atheromas or of left atrial appendage thrombi, time-dependent analyses were performed with and without strokes <24 hours after AVR (n=4). A third exploratory model assessed strokes >24 hours after AVR. To evaluate if the results after AVR were sensitive to competing risks, the latter model was supplemented by an additional analysis examining the first of ischemic stroke or death after AVR. Results are given as cause-specific hazard ratios (HR) with 95% confidence intervals (CI). Time-varying modified Kaplan–Meier curves taking into account the multistate effect, that is, avoiding that the same subject appears in 2 separate survival curves at the same time point, were used to depict rates of ischemic stroke before and after AVR.18 The cumulative hazard estimate of incident stroke after AVR was calculated from the time of the first postoperative stroke (10 months after enrollment, the first pa-tient underwent AVR after 28 days after inclusion in the SEAS trial). Outcome analyses could not be related to the presence or absence of postoperative AF because ECGs were recorded annually and no reli-able estimation of perioperative AF was, therefore, available. Linear and proportional hazard assumptions were investigated by cumula-tive Martingale residuals (10 000 random resamplings were compared with the models functional form). All covariates aside from left atrial volumes fulfilled assumptions for Cox modeling. As such, left atrial volumes were entered into the Cox model on the log2-scale (log2-scale was chosen because an increase of 1 on the log2-scale corresponds to a doubling in left atrial volumes on the original scale and because
by guest on May 22, 2018
http://stroke.ahajournals.org/D
ownloaded from

Greve et al Stroke in Aortic Stenosis 1941
log-transformation fulfilled the linear assumption). To account for the correlated prognostic information contained in left atrial volumes and AF, survival analyses using left atrial volumes were stratified by AF status. Differences in 30-day and 1-year mortality after in-study stroke were evaluated by Fisher exact test. The performance of the indepen-dent predictors of stroke in the Cox models stratified by AVR was eval-uated by changes in the c-index (using the macro SURVCSTD; http://www.mayo.edu/research/departments-divisions/department-health-sciences-research/division-biomedical-statistics-informatics/software/locally-written-sas-macros) as described by Cook.19 For all hypothesis testing, a 2-tailed P<0.05 was required for statistical significance.
ResultsBaseline ECG data and thus AF status were available in 1563 patients (83%). Age, sex, and AS severity were not statistically different in those with and without ECG data (all P>0.288). Excluding those prescribed OAC, 1509 patients remained in this study (Figure I in the online-only Data Supplement). The study population consisted of 923 men (61%) and 586 women (39%) followed for a mean of 4.3 years, totaling 6529 patient-years of follow-up. Demographic and clinical characteristics
Table 1. Baseline Characteristics and Subsequent Ischemic Stroke During 4.3 Years of Follow-Up
CharacteristicAll Patients (n=1509)
No Stroke (n=1467)
Stroke (n=42) P Value
Age, y 67.3±9.7 67.2±9.7 71.0±9.5 0.012
Current or ex-smokers, n (%) 833 (55.2) 811 (55.3) 22 (52.4) 0.709
Body mass index, kg/m2 27.0±4.3 26.9±4.3 28.6±5.0 0.015
Systolic blood pressure, mm Hg 145.2±20.3 145.1±20.3 149.0±17.2 0.217
Diastolic blood pressure, mm Hg 82.1±10.5 82.0±10.5 85.6±10.6 0.031
LDL cholesterol, mmol/L 3.56±0.88 3.56±0.89 3.69±0.86 0.357
HDL cholesterol, mmol/L 1.51±0.43 1.51±0.43 1.47±0.32 0.385
Estimated GFR, mL/min per 1.73 m2 68.3±12.1 67.9±12.9 68.3±12.1 0.822
Thyroid-stimulating hormone, mU/L 1.87±1.21 1.87±1.21 1.82±1.05 0.785
Baseline atrial fibrillation, n (%) 96 (6.4) 90 (6.1) 6 (14.3) 0.046
Left bundle branch block, n (%) 42 (2.8) 41 (2.8) 1 (2.4) 1.000
Heart rate, min−1 64.9±11.0 64.9±11.0 66.9±12.8 0.241
CHA2DS
2-VASc (score) 1.8±1.2 1.8±1.2 2.1±1.3 0.066
Baseline hypertension, n (%) 784 (52.0) 759 (51.7) 25 (59.5) 0.319
Age 65–74 y, n (%) 566 (37.5) 548 (50.4) 18 (75.0) 0.017
Age ≥75 y, n (%) 398 (26.4) 380 (41.4) 18 (75.0) 0.001
Female sex, n (%) 586 (38.8) 572 (39.0) 14 (33.3) 0.458
Echocardiographic parameters
Peak aortic jet velocity, m/s 3.08±0.55 3.08±0.55 3.19±0.52 0.214
Aortic valve area index, cm2/m2 0.61±0.19 0.61±0.19 0.55±0.14 0.007
Mean gradient, mm Hg 22.7±8.7 22.7±8.8 23.5±8.0 0.594
Bicuspid aortic valve, n (%) 67 (5.5) 67 (5.6) 0 (0.0) 0.255
Aortic regurgitation grade ≥2, n (%) 228 (16.6) 222 (16.6) 5 (15.4) 0.835
Mitral regurgitation grade ≥2, n (%) 147 (10.6) 145 (10.7) 2 (5.3) 0.422
LA systolic volume index, mL/m2 35.8±16.4 35.7±16.5 39.4±12.3 0.049
LA diastolic volume index, mL/m2 18.9±11.9 18.8±11.9 21.8±10.4 0.035
LV mass index, g/m2 99.9±30.5 99.7±30.5 107.3±28.7 0.125
LV ejection fraction, % 65.9±8.2 65.8±8.2 67.9±7.9 0.121
Stroke volume index, mL/m(height)2.04 25.8±6.3 25.8±6.2 24.6±6.7 0.221
Cardiac index, L/min per m2 2.65±0.75 2.65±0.75 2.61±0.69 0.706
Medicine
Simvastatin/ezetimibe, n (%) 755 (50.3) 738 (50.3) 17 (40.5) 0.209
Aspirin,* n (%) 289 (19.2) 285 (19.4) 4 (9.5) 0.108
Diuretics, n (%) 689 (45.7) 662 (45.1) 27 (64.3) 0.014
β-Blockade, n (%) 749 (49.6) 719 (49.0) 30 (71.4) 0.004
Renin–angiotensin system blocker, n (%) 619 (41.0) 599 (40.8) 20 (47.6) 0.378
CHA2DS
2-VASc indicates congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke/transient ischemic attack,
vascular disease, age 65–74 years and female sex; GFR, glomerular filtration rate; HDL, high-density lipoprotein; LA, left atrial; LDL, low-density lipoprotein; and LV, left ventricular.
*Defined as continuous prescription during the course of the study.
by guest on May 22, 2018
http://stroke.ahajournals.org/D
ownloaded from
1942 Stroke July 2014
at baseline are given in Table 1; mean CHA2DS
2-VASc score
was 1.8 and prevalence of baseline AF 6%.
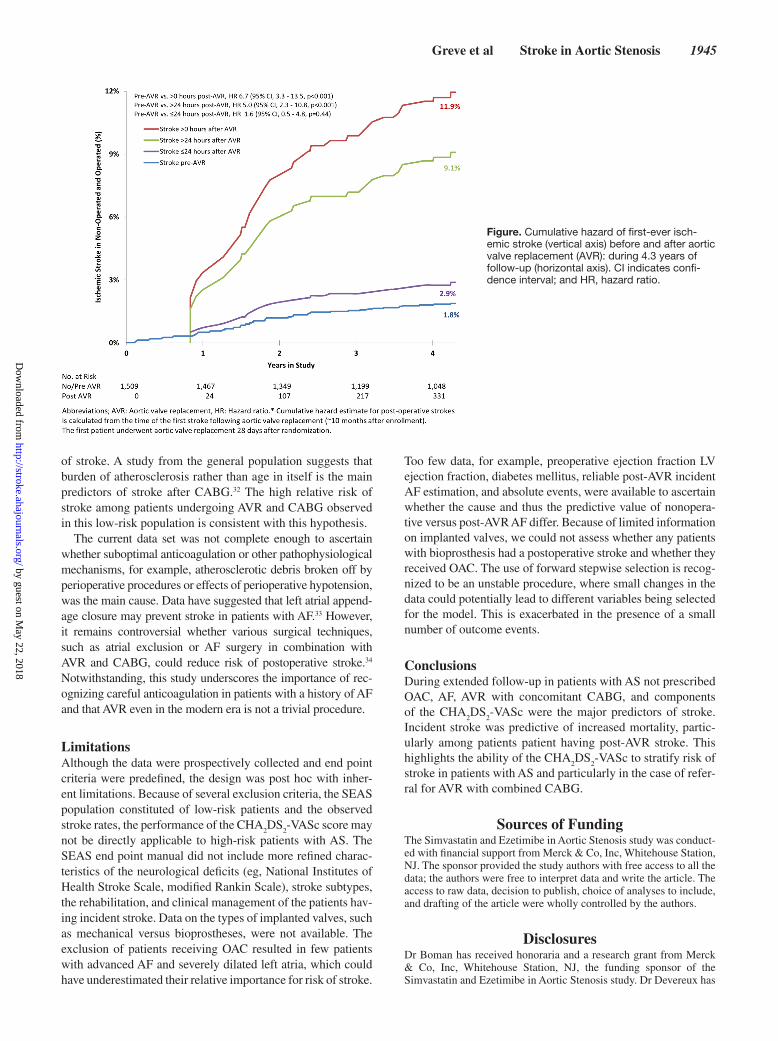
Entire Follow-Up and Pre-AVR StrokesA total of 47 (3%) strokes occurred, 42 (3%) patients had isch-emic strokes, of which 10% had a fatal outcome, incident AF was detected in 84 (6%) patients without baseline AF, a total of 139 (9%) died, and 429 (28%) underwent AVR, of which 30% (n=129) had AVR combined with CABG (Figure I in the online-only Data Supplement). Of the 42 ischemic strokes, 62% (n=26) occurred before AVR, which translated to 5.6 versus 21.8 strokes per 1000 patient-years pre- and post-AVR (P<0.001), respectively.
All-cause mortality also tended to be higher after AVR than in nonoperated patients, although this difference did not reach statistical significance (HR, 1.5; 95% CI, 1.0–2.3; P=0.072). Of the 110 deaths in nonoperated patients, only 7% (n=8) occurred in individuals with previous stroke. In contrast, of the 29 deaths that occurred after AVR, 24% (n=7) had previous stroke of which 86% (n=6) were post-AVR strokes. Although there were few events, this translated to a tendency to increased 30-day and 1-year mortality rates in patients experiencing post-AVR stroke (30-day mortal-ity: 22% and 1-year mortality: 36%) compared with that
observed after stroke in nonoperated patients (30-day mor-tality: 5% and 1-year mortality: 22%, both P≥0.150 in com-parison of all-cause mortality after stroke in operated and nonoperated). Combining data from operated and nonoper-ated patients, in-study stroke was associated with 8.1-fold (95% CI, 4.7–14.0; P<0.001) greater risk of death in the study period. When excluding patients with perioperative strokes (<24 hours after AVR, n=4), predictors of ischemic stroke stratified by AVR are given in Tables 2 to 4. There was no detectable effect of randomized treatment on the observed stroke rates before (HR, 0.7; 95% CI, 0.4–1.3) or after AVR (HR, 0.6; 95% CI, 0.2–1.7; both P≥0.326; Tables 3–4). Importantly, increased body mass index (HR, 1.1; 95% CI, 1.0–1.2) and age ≥75 years (HR, 4.5; 95% CI, 1.6–12.6; both P≤0.004) were the only multivariable predictor of isch-emic stroke before AVR. Adding strokes that occurred ≥24 hours after AVR CHA
2DS
2-VASc score (HR, 1.4; 95% CI,
1.1–1.8), greater diastolic blood pressure (HR, 1.4 per 10 mm Hg; 95% CI, 1.1–1.8), preoperative AF (HR, 2.7; 95% CI, 1.1–6.5), and AVR in itself (HR, 5.4; 95% CI, 2.5–11.8; all P≤0.026) remained as independent predictors of isch-emic stroke. The latter seemed to be driven by a markedly elevated relative risk of stroke in patients undergoing AVR combined with CABG (HR, 3.2; 95% CI, 1.4–7.2; P=0.006;
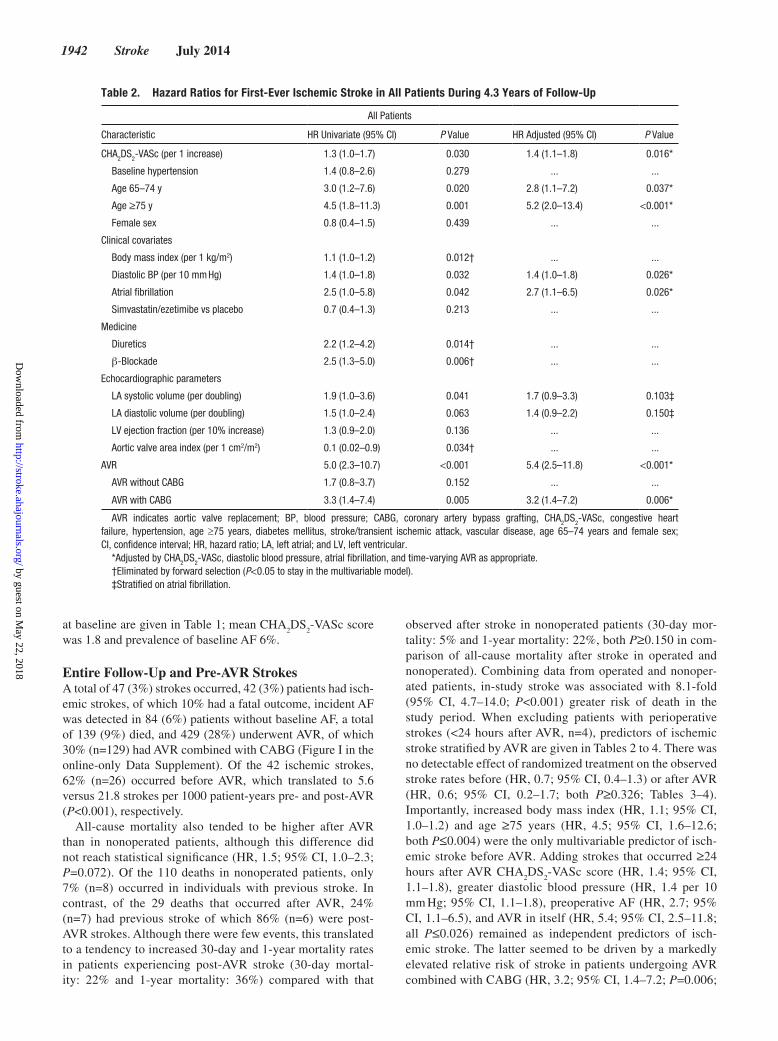
Table 2. Hazard Ratios for First-Ever Ischemic Stroke in All Patients During 4.3 Years of Follow-Up
All Patients
Characteristic HR Univariate (95% CI) P Value HR Adjusted (95% CI) P Value
CHA2DS
2-VASc (per 1 increase) 1.3 (1.0–1.7) 0.030 1.4 (1.1–1.8) 0.016*
Baseline hypertension 1.4 (0.8–2.6) 0.279 ... ...
Age 65–74 y 3.0 (1.2–7.6) 0.020 2.8 (1.1–7.2) 0.037*
Age ≥75 y 4.5 (1.8–11.3) 0.001 5.2 (2.0–13.4) <0.001*
Female sex 0.8 (0.4–1.5) 0.439 ... ...
Clinical covariates
Body mass index (per 1 kg/m2) 1.1 (1.0–1.2) 0.012† ... ...
Diastolic BP (per 10 mm Hg) 1.4 (1.0–1.8) 0.032 1.4 (1.0–1.8) 0.026*
Atrial fibrillation 2.5 (1.0–5.8) 0.042 2.7 (1.1–6.5) 0.026*
Simvastatin/ezetimibe vs placebo 0.7 (0.4–1.3) 0.213 ... ...
Medicine
Diuretics 2.2 (1.2–4.2) 0.014† ... ...
β-Blockade 2.5 (1.3–5.0) 0.006† ... ...
Echocardiographic parameters
LA systolic volume (per doubling) 1.9 (1.0–3.6) 0.041 1.7 (0.9–3.3) 0.103‡
LA diastolic volume (per doubling) 1.5 (1.0–2.4) 0.063 1.4 (0.9–2.2) 0.150‡
LV ejection fraction (per 10% increase) 1.3 (0.9–2.0) 0.136 ... ...
Aortic valve area index (per 1 cm2/m2) 0.1 (0.02–0.9) 0.034† ... ...
AVR 5.0 (2.3–10.7) <0.001 5.4 (2.5–11.8) <0.001*
AVR without CABG 1.7 (0.8–3.7) 0.152 ... ...
AVR with CABG 3.3 (1.4–7.4) 0.005 3.2 (1.4–7.2) 0.006*
AVR indicates aortic valve replacement; BP, blood pressure; CABG, coronary artery bypass grafting, CHA2DS
2-VASc, congestive heart
failure, hypertension, age ≥75 years, diabetes mellitus, stroke/transient ischemic attack, vascular disease, age 65–74 years and female sex; CI, confidence interval; HR, hazard ratio; LA, left atrial; and LV, left ventricular.
*Adjusted by CHA2DS
2-VASc, diastolic blood pressure, atrial fibrillation, and time-varying AVR as appropriate.
†Eliminated by forward selection (P<0.05 to stay in the multivariable model).‡Stratified on atrial fibrillation.
by guest on May 22, 2018
http://stroke.ahajournals.org/D
ownloaded from
Greve et al Stroke in Aortic Stenosis 1943
Table 2). In a separate analysis adding perioperative strokes (<24 hours after AVR [n=4]), the HR for stroke after AVR was even further substantiated (HR, 6.7; 95% CI, 3.3–13.6; P<0.001). Including perioperative strokes increased rela-tive risks of stroke 4.4-fold (95% CI, 2.1–9.2; P<0.001) in patients undergoing AVR with simultaneous CABG and increased the trend in patients undergoing isolated AVR (HR, 1.9; 95% CI, 0.9–4.0; P=0.089). c-Index analyses dem-onstrated intermediate prediction of incident stroke (c-index 0.71) and pointed toward AVR as a major risk factor for isch-emic stroke in this population (Table 5).
Strokes Post-AVRIncidence of stroke post-AVR was mainly driven by strokes occurring >24 hours after the procedure (Figure), although 75% (n=12) of post-AVR strokes occurred within a week of surgery (median time to post-AVR stroke was 3 days with interquartile ranges 0.5–49.5 days). Restricting the survival analyses to post-AVR follow-up in-study stroke was associ-ated with an 11.3-fold (95% CI, 4.5–28.6; P<0.001) greater risk of in-study death in patients experiencing post-AVR (n=16) stroke compared with post-AVR patients remaining free from stroke (n=407).
In an exploratory analysis of strokes occurring ≥24 hours after AVR, only preserved LV ejection fraction (HR 1.1 per 1% higher LV ejection fraction; 95% CI, 1.0–1.2; P=0.031) and older age displayed significant association with a postopera-tive stroke (Table 4). However, taking into account differences
in postoperative survival, the relationship between LV systolic function and post-AVR stroke risk was abolished (P=0.606). Thus, the longer time at risk in patients with preserved LV systolic function (HR 1.1 for increased post-AVR all-cause mortality per 1% lower ejection fraction; 95% CI, 1.0–1.1; P=0.019) partly explained the greater risk of experiencing a post-AVR stroke. Conversely, accounting for differences in postoperative survival seemed to enhance the univariate relationship of randomized treatment with postoperative end points (Table 4).
DiscussionThis study is, to the best of our knowledge, the first to examine independent predictors of ischemic stroke in initially asymp-tomatic mild-to-moderate AS. Several new findings add to current knowledge. First, in patients with AS with low risk of thromboembolism not prescribed OAC, components of the CHA
2DS
2-VASc scoring system were applicable for antici-
pating the risk of ischemic stroke irrespective of AF status. Second, AVR combined with CABG was independently asso-ciated with marked risks of peri- and postoperative ischemic stroke, which translated to reduced long-term survival. Third, the predictive information of left atrial volume of incident stroke was contained in AF status. Finally, randomized treat-ment with 40 mg of simvastatin and 10 mg of ezetimibe versus placebo did not lower the risk of stroke before or after AVR.
The observed higher incidence of all-cause mortality after stroke in post-AVR patients argues that aside from disabling
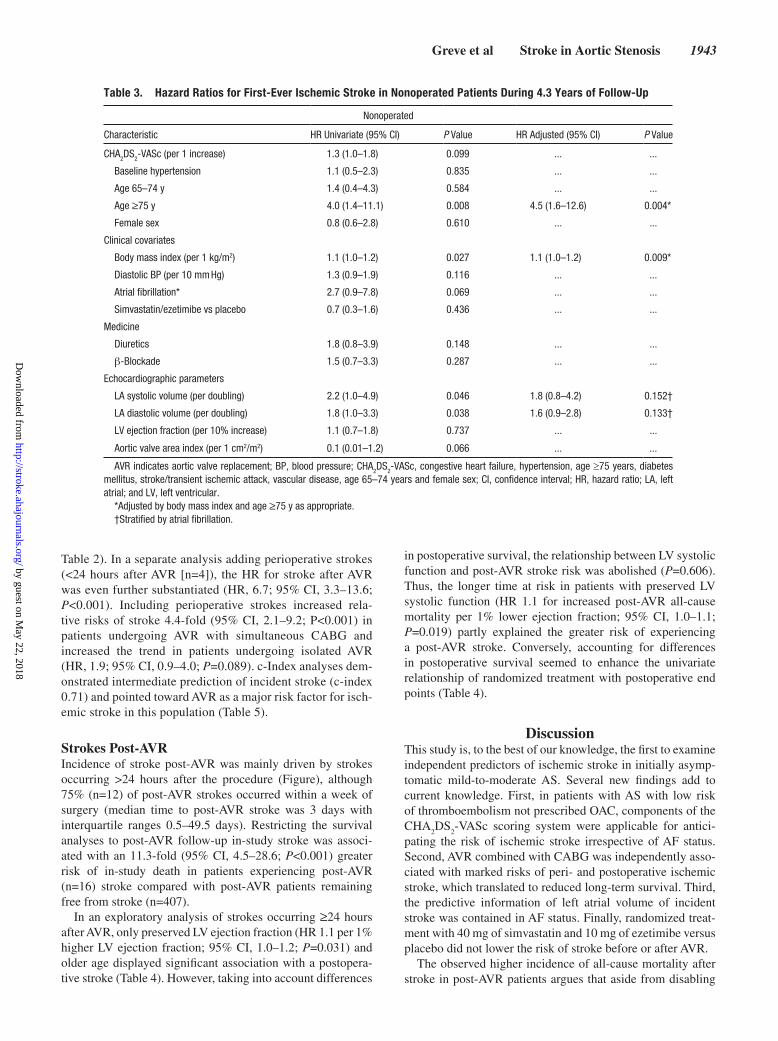
Table 3. Hazard Ratios for First-Ever Ischemic Stroke in Nonoperated Patients During 4.3 Years of Follow-Up
Nonoperated
Characteristic HR Univariate (95% CI) P Value HR Adjusted (95% CI) P Value
CHA2DS
2-VASc (per 1 increase) 1.3 (1.0–1.8) 0.099 ... ...
Baseline hypertension 1.1 (0.5–2.3) 0.835 ... ...
Age 65–74 y 1.4 (0.4–4.3) 0.584 ... ...
Age ≥75 y 4.0 (1.4–11.1) 0.008 4.5 (1.6–12.6) 0.004*
Female sex 0.8 (0.6–2.8) 0.610 ... ...
Clinical covariates
Body mass index (per 1 kg/m2) 1.1 (1.0–1.2) 0.027 1.1 (1.0–1.2) 0.009*
Diastolic BP (per 10 mm Hg) 1.3 (0.9–1.9) 0.116 ... ...
Atrial fibrillation* 2.7 (0.9–7.8) 0.069 ... ...
Simvastatin/ezetimibe vs placebo 0.7 (0.3–1.6) 0.436 ... ...
Medicine
Diuretics 1.8 (0.8–3.9) 0.148 ... ...
β-Blockade 1.5 (0.7–3.3) 0.287 ... ...
Echocardiographic parameters
LA systolic volume (per doubling) 2.2 (1.0–4.9) 0.046 1.8 (0.8–4.2) 0.152†
LA diastolic volume (per doubling) 1.8 (1.0–3.3) 0.038 1.6 (0.9–2.8) 0.133†
LV ejection fraction (per 10% increase) 1.1 (0.7–1.8) 0.737 ... ...
Aortic valve area index (per 1 cm2/m2) 0.1 (0.01–1.2) 0.066 ... ...
AVR indicates aortic valve replacement; BP, blood pressure; CHA2DS
2-VASc, congestive heart failure, hypertension, age ≥75 years, diabetes
mellitus, stroke/transient ischemic attack, vascular disease, age 65–74 years and female sex; CI, confidence interval; HR, hazard ratio; LA, left atrial; and LV, left ventricular.
*Adjusted by body mass index and age ≥75 y as appropriate.†Stratified by atrial fibrillation.
by guest on May 22, 2018
http://stroke.ahajournals.org/D
ownloaded from
1944 Stroke July 2014
the patient postoperative stroke is also indicative of impaired long-term survival (36% died within the first year of follow-up). Recent data have suggested comparable or higher risk of stroke after transcatheter AVR compared with conventional AVR.20–23 This is concerning in the context of observational studies demonstrating an incidence of cerebrovascular lesions, as detected by MRI, of >70% after transcatheter AVR.24 Prevention of ischemic stroke is, therefore, of key importance
for continued safe expansion of transcatheter AVR and con-ventional AVR. In long-term follow-up of 1014 patients, referred for AVR with a stentless valve, predictors of cerebro-vascular events were individual risk factors and not the type of valve prosthesis in itself.25 This corresponds well with compa-rable occurrence of thromboembolism in randomized compar-isons of bioprosthetic versus mechanical valves and suggests that comorbidities rather than intraoperative technique are the main predictors of stroke on the population level.26,27
The fact that CHA2DS
2-VASc scores worked in this asymp-
tomatic AS population with a low detected prevalence of AF concurs with data from the Randomized Evaluation of Long Term Anticoagulant Therapy (RE-LY) registry, sug-gesting that CHA
2DS
2-VASc scores relate to stroke also in
valvular AF28 and recent studies demonstrating the ability of CHA
2DS
2-VASc to predict outcome also in patients with-
out AF.29 Careful patient selection for AVR and transcatheter AVR and appropriate anticoagulation, that is, for AF status, CHA
2DS
2-VASc score, and presence of additional coronary
artery disease, therefore seem to be the modifiable risk factors for stroke prevention in AS, which may translate to improved post-AVR survival.30 This hypothesis is further supported by reduced risk of stroke in (1) low-risk patients with AS with sinus rhythm,31 (2) sufficiently anticoagulated post-AVR patients,21 and (3) no detectable effect of intensive lipid-low-ering in this study.
The fact that AVR combined with CABG was indepen-dently associated with a marked increase in the risk of stroke argues that procedure-related factors are separately predictive
Table 5. Contributions to Incident Stroke Prediction in the SEAS Study: During 4.3 Years of Follow-Up
Variable Variable χ2 P Value HR c-Index
Stroke in all patients (42 events)
Effect of adding variables to model with DBP only
DBP only (per 10 mm Hg) 4.6 0.032 1.4 0.60
+AF 5.5 0.019 2.8 0.62
+CHA2DS
2-VASc 4.4 0.035 1.3 0.64
+Time-varying AVR 17.9 <0.001 5.4 0.71
+ indicates the addition of each variable separately to the model beginning with diastolic blood pressure only. χ2 is the likelihood ratio statistic for each single covariate when added to the model. Hazard ratios are when each covariate is included in the model and display event rate ratios for diastolic blood pressure (per 10 mm Hg increments), atrial fibrillation (yes/no), CHA
2DS
2-
VASc score (per 1 U), and time-varying aortic valve replacement (yes/no). AF indicates atrial fibrillation; AVR, aortic valve replacement; CHA
2DS
2-VASc,
congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke/transient ischemic attack, vascular disease, age 65–74 years and female sex; DBP, diastolic blood pressure; HR, hazard ratio; and SEAS, Simvastatin and Ezetimibe in Aortic Stenosis.
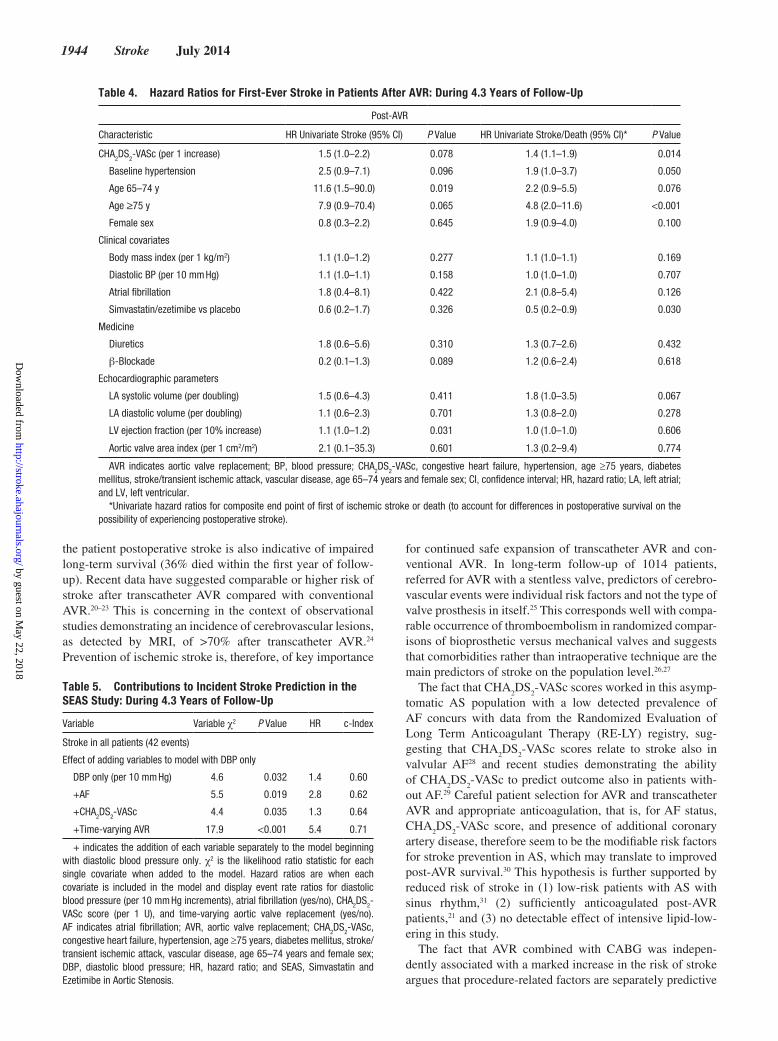
Table 4. Hazard Ratios for First-Ever Stroke in Patients After AVR: During 4.3 Years of Follow-Up
Post-AVR
Characteristic HR Univariate Stroke (95% CI) P Value HR Univariate Stroke/Death (95% CI)* P Value
CHA2DS
2-VASc (per 1 increase) 1.5 (1.0–2.2) 0.078 1.4 (1.1–1.9) 0.014
Baseline hypertension 2.5 (0.9–7.1) 0.096 1.9 (1.0–3.7) 0.050
Age 65–74 y 11.6 (1.5–90.0) 0.019 2.2 (0.9–5.5) 0.076
Age ≥75 y 7.9 (0.9–70.4) 0.065 4.8 (2.0–11.6) <0.001
Female sex 0.8 (0.3–2.2) 0.645 1.9 (0.9–4.0) 0.100
Clinical covariates
Body mass index (per 1 kg/m2) 1.1 (1.0–1.2) 0.277 1.1 (1.0–1.1) 0.169
Diastolic BP (per 10 mm Hg) 1.1 (1.0–1.1) 0.158 1.0 (1.0–1.0) 0.707
Atrial fibrillation 1.8 (0.4–8.1) 0.422 2.1 (0.8–5.4) 0.126
Simvastatin/ezetimibe vs placebo 0.6 (0.2–1.7) 0.326 0.5 (0.2–0.9) 0.030
Medicine
Diuretics 1.8 (0.6–5.6) 0.310 1.3 (0.7–2.6) 0.432
β-Blockade 0.2 (0.1–1.3) 0.089 1.2 (0.6–2.4) 0.618
Echocardiographic parameters
LA systolic volume (per doubling) 1.5 (0.6–4.3) 0.411 1.8 (1.0–3.5) 0.067
LA diastolic volume (per doubling) 1.1 (0.6–2.3) 0.701 1.3 (0.8–2.0) 0.278
LV ejection fraction (per 10% increase) 1.1 (1.0–1.2) 0.031 1.0 (1.0–1.0) 0.606
Aortic valve area index (per 1 cm2/m2) 2.1 (0.1–35.3) 0.601 1.3 (0.2–9.4) 0.774
AVR indicates aortic valve replacement; BP, blood pressure; CHA2DS
2-VASc, congestive heart failure, hypertension, age ≥75 years, diabetes
mellitus, stroke/transient ischemic attack, vascular disease, age 65–74 years and female sex; CI, confidence interval; HR, hazard ratio; LA, left atrial; and LV, left ventricular.
*Univariate hazard ratios for composite end point of first of ischemic stroke or death (to account for differences in postoperative survival on the possibility of experiencing postoperative stroke).
by guest on May 22, 2018
http://stroke.ahajournals.org/D
ownloaded from
Greve et al Stroke in Aortic Stenosis 1945
of stroke. A study from the general population suggests that burden of atherosclerosis rather than age in itself is the main predictors of stroke after CABG.32 The high relative risk of stroke among patients undergoing AVR and CABG observed in this low-risk population is consistent with this hypothesis.
The current data set was not complete enough to ascertain whether suboptimal anticoagulation or other pathophysiological mechanisms, for example, atherosclerotic debris broken off by perioperative procedures or effects of perioperative hypotension, was the main cause. Data have suggested that left atrial append-age closure may prevent stroke in patients with AF.33 However, it remains controversial whether various surgical techniques, such as atrial exclusion or AF surgery in combination with AVR and CABG, could reduce risk of postoperative stroke.34 Notwithstanding, this study underscores the importance of rec-ognizing careful anticoagulation in patients with a history of AF and that AVR even in the modern era is not a trivial procedure.
LimitationsAlthough the data were prospectively collected and end point criteria were predefined, the design was post hoc with inher-ent limitations. Because of several exclusion criteria, the SEAS population constituted of low-risk patients and the observed stroke rates, the performance of the CHA
2DS
2-VASc score may
not be directly applicable to high-risk patients with AS. The SEAS end point manual did not include more refined charac-teristics of the neurological deficits (eg, National Institutes of Health Stroke Scale, modified Rankin Scale), stroke subtypes, the rehabilitation, and clinical management of the patients hav-ing incident stroke. Data on the types of implanted valves, such as mechanical versus bioprostheses, were not available. The exclusion of patients receiving OAC resulted in few patients with advanced AF and severely dilated left atria, which could have underestimated their relative importance for risk of stroke.
Too few data, for example, preoperative ejection fraction LV ejection fraction, diabetes mellitus, reliable post-AVR incident AF estimation, and absolute events, were available to ascertain whether the cause and thus the predictive value of nonopera-tive versus post-AVR AF differ. Because of limited information on implanted valves, we could not assess whether any patients with bioprosthesis had a postoperative stroke and whether they received OAC. The use of forward stepwise selection is recog-nized to be an unstable procedure, where small changes in the data could potentially lead to different variables being selected for the model. This is exacerbated in the presence of a small number of outcome events.
ConclusionsDuring extended follow-up in patients with AS not prescribed OAC, AF, AVR with concomitant CABG, and components of the CHA
2DS
2-VASc were the major predictors of stroke.
Incident stroke was predictive of increased mortality, partic-ularly among patients patient having post-AVR stroke. This highlights the ability of the CHA
2DS
2-VASc to stratify risk of
stroke in patients with AS and particularly in the case of refer-ral for AVR with combined CABG.
Sources of FundingThe Simvastatin and Ezetimibe in Aortic Stenosis study was conduct-ed with financial support from Merck & Co, Inc, Whitehouse Station, NJ. The sponsor provided the study authors with free access to all the data; the authors were free to interpret data and write the article. The access to raw data, decision to publish, choice of analyses to include, and drafting of the article were wholly controlled by the authors.
DisclosuresDr Boman has received honoraria and a research grant from Merck & Co, Inc, Whitehouse Station, NJ, the funding sponsor of the Simvastatin and Ezetimibe in Aortic Stenosis study. Dr Devereux has
Figure. Cumulative hazard of first-ever isch-emic stroke (vertical axis) before and after aortic valve replacement (AVR): during 4.3 years of follow-up (horizontal axis). CI indicates confi-dence interval; and HR, hazard ratio.
by guest on May 22, 2018
http://stroke.ahajournals.org/D
ownloaded from

1946 Stroke July 2014
served as a consultant to Merck & Co, Inc. Dr Egstrup has received honoraria from Merck & Co, Inc. Dr Wachtell has received a research grant from Merck & Co, Inc. The other authors report no conflicts.
References 1. Bonow RO, Carabello BA, Chatterjee K, de Leon ACJ, Faxon DP,
Freed MD, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart dis-ease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2008;118: e523–e661.
2. Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012;33:2451–2496.
3. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart sur-vey on atrial fibrillation. Chest. 2010;137:263–272.
4. Otto CM, Lind BK, Kitzman DW, Gersh BJ, Siscovick DS. Association of aortic-valve sclerosis with cardiovascular mortality and morbidity in the elderly. N Engl J Med. 1999;341:142–147.
5. Petty GW, Khandheria BK, Whisnant JP, Sicks JD, O’Fallon WM, Wiebers DO. Predictors of cerebrovascular events and death among patients with valvular heart disease: a population-based study. Stroke. 2000;31:2628–2635.
6. Boon A, Lodder J, Cheriex E, Kessels F. Risk of stroke in a cohort of 815 patients with calcification of the aortic valve with or without stenosis. Stroke. 1996;27:847–851.
7. Rossebø AB, Pedersen TR, Allen C, Boman K, Chambers J, Egstrup K, et al. Design and baseline characteristics of the simvastatin and ezeti-mibe in aortic stenosis (SEAS) study. Am J Cardiol. 2007;99:970–973.
8. Rossebø AB, Pedersen TR, Boman K, Brudi P, Chambers JB, Egstrup K, et al; SEAS Investigators. Intensive lipid lowering with simvastatin and ezetimibe in aortic stenosis. N Engl J Med. 2008;359:1343–1356.
9. Greve AM, Gerdts E, Boman K, Gohlke-Baerwolf C, Rossebø AB, Hammer-Hansen S, et al. Differences in cardiovascular risk profile between electrocardiographic hypertrophy versus strain in asymp-tomatic patients with aortic stenosis (from SEAS data). Am J Cardiol. 2011;108:541–547.
10. Prineas RJ, Crowe RS, Blackburn H. The Minnesota Code Manual of Electrocardiographic Findings. Bristol, UK: John Wright; 1982.
11. Cramariuc D, Cioffi G, Rieck AE, Devereux RB, Staal EM, Ray S, et al. Low-flow aortic stenosis in asymptomatic patients: valvular-arterial impedance and systolic function from the SEAS Substudy. J Am Coll Cardiol Cardiovasc Imaging. 2009;2:390–399.
12. Carabello BA. What is new in the 2006 ACC/AHA guidelines on valvu-lar heart disease? Curr Cardiol Rep. 2008;10:85–90.
13. Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al; EAE/ASE. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. Eur J Echocardiogr. 2009;10:1–25.
14. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, et al. Echocardiographic assessment of left ventricular hypertrophy: com-parison to necropsy findings. Am J Cardiol. 1986;57:450–458.
15. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440–1463.
16. Cheitlin MD, Armstrong WF, Aurigemma GP, Beller GA, Bierman FZ, Davis JL, et al; ACC; AHA; ASE. ACC/AHA/ASE 2003 Guideline
Update for the Clinical Application of Echocardiography: summary article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocardiography). J Am Soc Echocardiogr. 2003;16:1091–1110.
17. Andersen PK, Gill R.D. Cox’s regression model for counting processes: a Large Sample Study. Ann Stat. 1982;10:1100–1120.
18. Andersen PK, Pohar Perme M. Inference for outcome probabilities in multi-state models. Lifetime Data Anal. 2008;14:405–431.
19. Cook NR. Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation. 2007;115:928–935.
20. Daneault B, Kirtane AJ, Kodali SK, Williams MR, Genereux P, Reiss GR, et al. Stroke associated with surgical and transcatheter treat-ment of aortic stenosis: a comprehensive review. J Am Coll Cardiol. 2011;58:2143–2150.
21. Higgins J, Ye J, Humphries KH, Cheung A, Wood DA, Webb JG, et al. Early clinical outcomes after transapical aortic valve implantation: a propensity-matched comparison with conventional aortic valve replace-ment. J Thorac Cardiovasc Surg. 2011;142:e47–e52.
22. Eggebrecht H, Schmermund A, Voigtländer T, Kahlert P, Erbel R, Mehta RH. Risk of stroke after transcatheter aortic valve implantation (TAVI): a meta-analysis of 10,037 published patients. EuroIntervention. 2012;8:129–138.
23. Barbash IM, Waksman R. Overview of the 2011 Food and Drug Administration Circulatory System Devices Panel of the Medical Devices Advisory Committee Meeting on the Edwards SAPIEN™ trans-catheter heart valve. Circulation. 2012;125:550–555.
24. Ghanem A, Müller A, Nähle CP, Kocurek J, Werner N, Hammerstingl C, et al. Risk and fate of cerebral embolism after transfemoral aortic valve implantation: a prospective pilot study with diffusion-weighted magnetic resonance imaging. J Am Coll Cardiol. 2010;55:1427–1432.
25. Gulbins H, Florath I, Ennker J. Cerebrovascular events after stentless aortic valve replacement during a 9-year follow-up period. Ann Thorac Surg. 2008;86:769–773.
26. Hammermeister K, Sethi GK, Henderson WG, Grover FL, Oprian C, Rahimtoola SH. Outcomes 15 years after valve replacement with a mechanical versus a bioprosthetic valve: final report of the Veterans Affairs randomized trial. J Am Coll Cardiol. 2000;36:1152–1158.
27. Stassano P, Di Tommaso L, Monaco M, Iorio F, Pepino P, Spampinato N, et al. Aortic valve replacement: a prospective randomized evaluation of mechanical versus biological valves in patients ages 55 to 70 years. J Am Coll Cardiol. 2009;54:1862–1868.
28. Healey J. Global variations in the 1-year rates of death and stroke in 15,432 patients presenting to the emergeny department with atrial fibril-lation in 47 countries: The RE-LY AF Registry. European Society of Cardiology 2012 Congress; August 29, 2012; Munich, Germany. 2012.
29. Ntaios G, Lip GY, Makaritsis K, Papavasileiou V, Vemmou A, Koroboki E, et al. CHADS2
, CHA2S
2DS
2-VASc, and long-term stroke outcome in
patients without atrial fibrillation. Neurology. 2013;80:1009–1017. 30. Turpie AG, Gent M, Laupacis A, Latour Y, Gunstensen J, Basile F, et al.
A comparison of aspirin with placebo in patients treated with warfarin after heart-valve replacement. N Engl J Med. 1993;329:524–529.
31. ElBardissi AW, DiBardino DJ, Chen FY, Yamashita MH, Cohn LH. Is early antithrombotic therapy necessary in patients with bioprosthetic aortic valves in normal sinus rhythm? J Thorac Cardiovasc Surg. 2010;139:1137–1145.
32. Mérie C, Køber L, Olsen PS, Andersson C, Jensen JS, Torp-Pedersen C. Risk of stroke after coronary artery bypass grafting: effect of age and comorbidities. Stroke. 2012;43:38–43.
33. Ostermayer SH, Reisman M, Kramer PH, Matthews RV, Gray WA, Block PC, et al. Percutaneous left atrial appendage transcatheter occlu-sion (PLAATO system) to prevent stroke in high-risk patients with non-rheumatic atrial fibrillation: results from the international multi-center feasibility trials. J Am Coll Cardiol. 2005;46:9–14.
34. Healey JS, Crystal E, Lamy A, Teoh K, Semelhago L, Hohnloser SH, et al. Left Atrial Appendage Occlusion Study (LAAOS): results of a ran-domized controlled pilot study of left atrial appendage occlusion dur-ing coronary bypass surgery in patients at risk for stroke. Am Heart J. 2005;150:288–293.
by guest on May 22, 2018
http://stroke.ahajournals.org/D
ownloaded from
Kristian WachtellBoman, Anne B. Rossebø, Christa Gohlke-Baerwolf, Richard B. Devereux, Lars Køber and Anders M. Greve, Morten Dalsgaard, Casper N. Bang, Kenneth Egstrup, Simon Ray, Kurt
StudyStroke in Patients With Aortic Stenosis: The Simvastatin and Ezetimibe in Aortic Stenosis
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2014 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.114.005296
2014;45:1939-1946; originally published online June 5, 2014;Stroke.
http://stroke.ahajournals.org/content/45/7/1939World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2014/06/05/STROKEAHA.114.005296.DC1Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 22, 2018
http://stroke.ahajournals.org/D
ownloaded from
SUPPLEMENTAL MATERIAL
Supplemental Figure I Study Flow-Chart: During 4.3 Years of Follow-Up.