identifying patients at high risk for stroke despite...
TRANSCRIPT

Identifying Patients at High Risk for StrokeDespite Anticoagulation
A Comparison of Contemporary Stroke Risk Stratification Schemes in anAnticoagulated Atrial Fibrillation Cohort
Gregory Y.H. Lip, MD; Lars Frison, PhD; Jonathan L. Halperin, MD; Deirdre A. Lane, PhD
Background and Purpose—The risk of stroke in patients with atrial fibrillation (AF) is not homogeneous, and variousclinical risk factors have informed the development of stroke risk stratification schemes (RSS). Among anticoagulatedcohorts, the emphasis should be on the identification of patients who remain at high risk for stroke despiteanticoagulation.
Methods—We investigated predictors of thromboembolism (TE) risk in an anticoagulated AF clinical trial cohort (n�7329subjects) and tested the predictive value of contemporary RSS in this cohort: CHADS2, Framingham, NICE 2006,American College of Cardiology/American Heart Association/European Society of Cardiology 2006, the 8th AmericanCollege of Chest Physicians guidelines and the CHA2DS2-VASc schemes.
Results—On multivariate analysis, significant predictors of TE were stroke/TIA (hazard ratio [HR], 2.24; P�0.001), age75 years or older (HR, 1.77; P�0.0002), coronary artery disease (HR, 1.52; P�0.0047), and smoking (HR, 2.10;P�0.0005), whereas reported alcohol use (HR, 0.70; P�0.02) was protective. Comparison of contemporary RSSdemonstrated variable classification of AF patients into risk strata, although c-statistics for TE were broadly similaramong the RSS tested and varied between 0.575 (NICE 2006) and 0.647 (CHA2DS2-VASc). CHA2DS2-VASc classified94.2% as being at high risk, whereas most other RSS categorized two-thirds as being at high risk. Of the 184 TE events,181 (98.4%) occurred in patients identified as being at high risk by the CHA2DS2-VASc schema. There was a stepwiseincrease in TE with increasing CHA2DS2-VASc score (Ptrend�0.0001), which had the highest HR (3.75) among thetested schemes. The negative predictive value (ie, the percent categorized as “not high risk” actually being free from TE)for CHA2DS2-VASc was 99.5%.
Conclusion—Coronary artery disease and smoking are additional risk factors for TE in anticoagulated AF patients,whereas alcohol use appears protective. Of the contemporary stroke RSS, the CHA2DS2-VASc scheme correctlyidentified the greatest proportion of AF patients at high risk, despite the similar predictive ability of most RSS evidencedby the c-statistic. (Stroke. 2010;41:2731-2738.)
Key Words: atrial fibrillation � warfarin
Atrial fibrillation (AF) is associated with a substantial riskof stroke and thromboembolism (TE), but this risk is not
homogeneous. Various clinical risk factors have formed thebasis for stroke risk stratification schemes (RSS) and clinicalpractice guidelines for stroke prevention in patients with AF.1
Although stroke rates in AF cohorts are declining,2 therelative risk reduction achieved with warfarin over aspirinapplies to patients with AF at intermediate or moderate risk aswell as to patients at high risk.3
Incorporation of these trends into clinical practice requirescontemporary data to assess stroke risk factors and therelative predictive value of RSS. As novel anticoagulants aredeveloped that are safer and more convenient than the
vitamin K antagonists,4 stroke RSS must evolve to moreaccurately identify subjects at “truly low risk,” because ahigher proportion of the remainder becomes candidates foranticoagulation. These RSS should also minimize classifica-tion of patients into the “intermediate/moderate risk” cate-gory because optimum antithrombotic therapy is less clearlydefined according to current guidelines.5–7
Many risk factors have been derived from analyses ofcohorts of the nonwarfarin arms of clinical trials,8 and othershave not been systematically assessed or documented in thetrial setting. Inclusion of stroke risk factors into RSS requiresvalidation in multiple populations, although many have beenderived and validated largely in trial cohorts. For example,
Received May 11, 2010; accepted August 23, 2010.From the University of Birmingham Centre for Cardiovascular Sciences (G.Y.H.L., D.A.L.), City Hospital, Birmingham, England, UK; AstraZeneca
R&D Molndal (L.F.), Molndal, Sweden; The Cardiovascular Institute (J.L.H.), Mount Sinai Medical Center, New York, NY.Correspondence to Professor G.Y.H. Lip, University of Birmingham Centre for Cardiovascular Sciences, City Hospital, Birmingham, England, UK.
E-mail [email protected]© 2010 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.110.590257
2731
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from

one of the most commonly used schemes, the CHADS2
(Congestive heart failure, Hypertension, Age, Diabetes,Stroke [Doubled]) score, evolved from the AF Investigatorsand Stroke Prevention in AF (SPAF) Investigators riskstratification scheme, and was validated in the NationalRegistry of Atrial Fibrillation cohort9 as well as in a pooledanalysis of patients treated with aspirin.10 More recently, the2006 American College of Cardiology/American Heart Asso-ciation/European Society of Cardiology (ACC/AHA/ESC)guideline risk schema6 evolved into the CHA2DS2-VASc score(Cardiac failure or dysfunction, Hypertension, Age �75[Dou-bled], Diabetes, Stroke[Doubled]-Vascular disease, Age 65–74and Sex category [Female]) score, which was validated in aEuropean cohort of 1084 subjects who were not anticoagulatedat baseline.11
A recent paradigm shift toward a preference for anticoag-ulation over antiplatelet therapy for stroke thromboprophy-laxis12 highlights the importance of evaluating the ability ofstroke RSS to identify patients at moderate or high risk forstroke. In addition, the identification of patients who remainat high risk for stroke despite appropriately managed antico-agulation (adequate time in therapeutic international normal-ized ratio range) is paramount and data on the ability ofcurrent stroke RSS to do this are limited,13,14 with only 1small study comparing the predictive ability of contemporarystroke RSS.14
The objective of the present analysis was to identify riskfactors for TE in a dataset of 2 large contemporary phase IIIclinical trials, the Stroke Prevention using an Oral ThrombinInhibitor in Atrial Fibrillation (SPORTIF) III and V trials,which compared warfarin against the oral direct thrombininhibitor ximelagatran for prevention of stroke and systemicembolism in patients with AF at moderate–high risk.15,16 Weused this cohort to assess the predictive value of contempo-rary stroke RSS (CHADS2
9 Framingham,17 NICE 2006,5
ACC/AHA/ESC 2006,6 ACCP8,7 and CHA2DS2-VASc11)in identifying patients at high risk for stroke despiteanticoagulation as well as providing additional validationof the CHA2DS2-VASc scheme in an anticoagulated clin-ical trial cohort.
Subjects and Methods
Study PopulationWe investigated predictors of TE risk in an anticoagulated clinicaltrial cohort of 7329 subjects with AF (using warfarin or ximelagat-ran) participating in the SPORTIF III and V trials and tested thepredictive value of several contemporary RSS, specifically theCHADS2,9 Framingham,17 NICE 2006,5 ACC/AHA/ESC 2006,6
ACCP8,7 CHA2DS2-VASc,11 and the modified CHADS2 scheme byRietbrock et al.18
The rationale, design, and results of SPORTIF III and SPORTIF Vhave been published.15,16 In summary, these randomized, multi-center, parallel group trials compared ximelagatran with warfarin forprevention of stroke and systemic embolism in patients with nonval-vular persistent paroxysmal or permanent AF at moderate–high riskfor stroke based on the 2001 guideline recommendations.19,20 Par-ticipants were randomized to either fixed-dose ximelagatran, 36 mgtwice daily, or dose-adjusted warfarin to maintain the internationalnormalized ratio between 2.0 and 3.0. Treatments were administeredas open-label in SPORTIF III and as double-blind in SPORTIF V.
Ascertainment of OutcomesAfter randomization, patients were seen at 1, 4, and 6 weeks, andthen at 2, 3, 4, 5, 6, 8, 10, and 12 months, and every 3 monthsthereafter for detection of stroke or systemic embolism (primaryevents), TIA, acute MI, or bleeding complications. Periodic admin-istration of a standard stroke symptom questionnaire enhanced eventdetection; positive responses prompted additional evaluation. Astudy-affiliated neurologist or stroke specialist, blinded to treatmentallocation, evaluated all possible primary events and TIA as quicklyas feasible based on clinical findings and results of CT or MRI of thebrain. An independent, central, clinical event adjudication commit-tee, also blinded to treatment, reviewed clinical reports of all primaryand secondary events.
Classification SchemesThe various stroke risk schemes examined in this cohort aresummarized in Table 1. The Framingham and CHADS2 schemes arepoint-based scores, the Framingham is based on a mathematicalformula that assigns point values to age, gender, systolic bloodpressure, diabetes, and previous stroke or transient ischemic attack,17
and the CHADS2 is based on 1 point for congestive heart failure,hypertension, age older than 75 years, and diabetes, and 2 points forprevious stroke or TIA.9 We defined the CHADS2 score in 2 ways:(1) classical, whereby scores of 0�low risk, 1 to 2�intermediaterisk, and �2�high risk; and (2) revised, whereby scores of 0�lowrisk, 1�intermediate risk, and �2�high risk. We categorized theFramingham score in a manner similar to that proposed by Fang etal21 as follows: score 0 to 7�low risk, 8 to 15�intermediate risk, and16 to 31�high risk. The CHA2DS2-VASc score includes categoriesof 0�low risk, 1�intermediate risk, and �2 as high risk.11 Inaddition to these (artificial) definitions commonly used in clinicalpractice, the predictive abilities of the Framingham, CHADS2, andCHA2DS2-VASc scores were also evaluated (perhaps more appro-priately) as continuous variables.
Statistical AnalysesWith the combined datasets from SPORTIF III and SPORTIF V, theprimary study for this analysis compared the predictive accuracy ofthe classification schemes for the first occurrence of stroke (ischemicor hemorrhagic) or systemic embolic event. The intention-to-treatanalyses included all randomized participants until study closureirrespective of continuation of treatment actually received. Coxregression modeling with TE as the dependent variable was used toestimate the impact of individual risk factors through univariateanalyses. Hazard ratios (HR) were obtained through these modelswith 95% CI. All potential TE risk factors investigated in theunivariate analyses were analyzed in a multivariate Cox regressionanalysis, in which only variables with P�0.05 in the presence ofother selected variables were retained in the final model. For allinvestigated risk stratification schemes, TE rates per patient-yearwere estimated after stratification of patients into categories of low,intermediate, and high risk, with HR obtained for each increase inrisk cohort from Cox regression modeling. The c-statistic, a measureof the area under the receiver-operator characteristic curve, quanti-fied the predictive validity of the classification schemes using thescoring schemes as continuous variables and tested the hypothesisthat these schemes performed significantly better than chance (indi-cated by a c-statistic �0.5). The c-statistic quantifies discriminateability, whereas the HR quantifies the increased relative risk ofstroke across risk strata.
ResultsThe univariate and multivariate predictive powers of variousstroke risk factors and TE are shown in Table 2. By univariateanalysis, previous stroke, TIA, or systemic embolism, age 75years or older, coronary artery disease, smoking, and femalegender predicted an increased risk of TE, whereas reportedalcohol use predicted lower risk. Of note, diabetes mellitus,hypertension, and left ventricular systolic dysfunction were
2732 Stroke December 2010
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

not predictive of TE in these patients. By multivariateanalysis, the only significant predictors of TE were previousstroke or TIA (HR, 2.24; 95% CI, 1.66–3.02; P�0.001), age75 years or older (HR, 1.77; 95% CI, 1.32–2.38; P�0.0002),
coronary artery disease (HR, 1.52; 95% CI, 1.14–2.04;P�0.0047), and smoking (HR, 2.10; 95% CI, 1.38–3.18;P�0.0005), whereas reported alcohol use (HR, 0.70; 95% CI,0.52–0.95; P�0.02) appeared protective.
Table 1. Risk Stratification Schemes Used to Predict Thromboembolism in Atrial Fibrillation
Risk Scheme Ref Low Risk Intermediate Risk High Risk
CHADS2
(2001)–classical9 Score 0 Score 1–2 Score 3–6
CHADS2–revised Score 0 Score 1 Score 2–6
Framingham (2003) 15 Score 0–7 Score 8–15 Score 16–31
NICE guidelines(2006)
5 Age �65y with nomoderate/high risk
factors
Age �65y with no high risk factorsAge �75y with hypertension,diabetes or vascular disease*
Previous stroke/TIA or thromboembolic event Age�75y with hypertension, diabetes or vascular
disease Clinical evidence of valve disease or heartfailure, or impaired left ventricular function
ACC/AHA/ESCguidelines (2006)
6 No risk factors Age �75y, or hypertension, orheart failure, or LVEF �35%, or
diabetes
Previous stroke, TIA or embolism, or �2 moderaterisk factors of (age �75y, hypertension, heart
failure, LVEF �35%, diabetes)
Rietbrock et al(2008)†
16 Score 0 Score 1–5 Score 6–14
8th ACCP guidelines(2008)
7 No risk factors Age �75y, or hypertension, ormoderately or severely impaired
LVEF and/or heart failure, ordiabetes
Previous stroke, TIA or embolism, or �2 moderaterisk factors of (age �75y, hypertension,
moderately or severely impaired LVEF and/or heartfailure, diabetes)
CHA2DS2-VASc(2009)
11 No risk factors One “clinically relevant non-major”risk factor: (heart failure/LVEF �40,
hypertension, diabetes, vasculardisease*, female gender, age
65–74)
One “major” risk factor [Previous stroke, TIA orembolism, or age �75y], or �2 “clinically
relevant non-major” risk factors (heart failure/LVEF�40, hypertension, diabetes, vascular disease*,
female gender, age 65–74)
*Myocardial infarction, peripheral artery disease or aortic plaque.†This risk stratification is a modified version of CHADS2 where Age is categorised into the following age groups: 40–64, 65–69, 70–74, 75–79, 80–84, 85–115
with the score assigned to each group increasing with age 1–6 points, respectively; females score 1 point; those with diabetes mellitus score 1 point and those witha history of stroke or TIA score 6 points.
ACC indicates American College of Cardiology; ACCP, American College of Chest Physicians; AHA, American Heart Association; CHADS2, Congestive heart failure,Hypertension, Age�75, Diabetes, prior Stroke/TIA; ESC, European Society of Cardiology; LVEF, left ventricular ejection fraction; NICE, National Institute for health andClinical Excellence; TIA, transient ischaemic attack.
Table 2. Univariate and Multivariate Predictive Power of Risk Factors for Thromboembolic Events
Risk Factor
Event Rate (%per Patient-Year)
Risk FactorPresent Univariate Analyses Multivariate Analyses*
Yes No Hazard Ratio† (95% CI) P Value Hazard Ratio† (95% CI) P Value
Stroke/TIA 3.05 1.28 2.35 (1.74, 3.17) �0.0001 2.24 (1.66, 3.02) �0.0001
Age�75 years 2.25 1.26 1.78 (1.34, 2.38) �0.0001 1.77 (1.32, 2.38) 0.0002
Coronary artery disease 2.04 1.31 1.57 (1.17, 2.10) 0.0025 1.52 (1.14, 2.04) 0.0047
Smoking 2.68 1.54 1.75 (1.16, 2.63) 0.0074 2.10 (1.38, 3.18) 0.0005
Alcohol 1.31 1.91 0.69 (0.51, 0.93) 0.014 0.70 (0.52, 0.95) 0.020
Systemic embolic event 3.24 1.56 2.08 (1.24, 3.47) 0.0052
Female 2.08 1.44 1.44 (1.07, 1.93) 0.016
Diabetes mellitus 1.92 1.55 1.23 (0.89, 1.71) 0.21
Hypertension 1.72 1.38 1.24 (0.86, 1.79) 0.24
Left ventricular dysfunction 1.67 1.62 1.03 (0.77, 1.39) 0.84
*Only factors associated with P�0.05 in the presence of other selected variables were retained in the final model. These results did not appearto be related to major differences in anticoagulation control amongst warfarin-treated patients; for example, amongst the 3665 patients treated withwarfarin, the mean of the patients individual mean INR amongst nonsmokers (n�3331) was 2.42, and the mean of the individual patients time inrange (INR 2–3) was 66.1%. Corresponding results for smokers (n�334) were 2.44 and 65.7%.
†Hazard ratio resulting from Cox regression model.TIA, transient ischaemic attack.
Lip et al Stroke Risk Schemes in AF 2733
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

The various RSS classified patients differently (Table 3,Figure 1). Because of the SPORTIF inclusion criteria, veryfew, if any, patients were classified as low risk by the variousRSS, with the exception of the Framingham risk schema,
which classed 40.1% as low risk using the cut-offs used byFang et al.21 CHA2DS2-VASc did not categorize any patientsas low risk, whereas �2% of patients were classified as “lowrisk” by the other RSS (Table 3). All RSS with the exceptionof CHADS2 (classical) and CHA2DS2-VASc categorizedapproximately two-thirds of the patients at high risk forstroke, whereas CHA2DS2-VASc categorized most patients athigh risk (94.2%).
One hundred eighty-four TE events occurred during the11 233 patient-years of follow-up (1.64% per 100 patient-years). The highest TE event rate occurred in patientsdefined as high risk by the Framingham schema (2.98%),with all other risk schema, with the exception ofCHA2DS2-VASc, reporting a 2% TE event in those at highrisk. Of note, CHA2DS2-VASc correctly identified 181(98.4%) who experienced a TE event as being at high risk.All RSS had c-statistics �0.50, demonstrating greaterpredictive accuracy for TE than chance. The c-statistics forTE ranged from 0.575 (NICE 2006) to 0.647(CHA2DS2-VASc).
Table 3. Risk Categorization, Incidence of Thromboembolism and Discriminatory Power for ContemporaryRisk Stratification Schema
Categorization of TE Risk Predictive Ability
Low Intermediate High c statistic Hazard Ratio (95% CI)
CHADS2 –classical
% in risk category 2.0 64.0 34.0 0.637 2.26*
TE events, N (%) 0/238�0.00 87/7276�1.20 97/3719�2.61 (0.607, 0.674) (1.71, 3.00)
CHADS2 – revised
% in risk category 2.0 31.1 66.9 0.637 2.50
TE events, N (%) 0/238�0.00 31/3563�0.87 153/7431�2.06 (0.607, 0.674) (1.72, 3.63)
Framingham
% in risk category 40.1 38.2 21.7 0.621 1.81
TE events, N (%) 41/4547�0.90 72/4299�1.67 71/2386�2.98 (0.589, 0.658) (1.50, 2.18)
NICE 2006
% in risk category 0.0 31.8 68.2 0.575 2.28
TE events, N (%) 0/2�0.00 32/3651�0.88 152/7580�2.01 (0.547, 0.600) (1.56, 3.34)
ACC/AHA/ESC 2006
% in risk category 1.8 30.3 67.9 0.587 2.58
TE events, N (%) 0/212�0.00 29/3469�0.84 155/7551�2.05 (0.557, 0.611) (1.75, 3.79)
Rietbrock et al
% in risk category 0.1 70.0 29.9 0.629 2.59
TE events, N (%) 0/10�0.00 89/7964�1.12 95/3258�2.92 (0.587, 0.668) (1.94, 3.46)
ACCP 2008
% in risk category 1.8 30.4 67.8 0.587 2.59
TE events, N (%) 0/212�0.00 29/3479�0.83 155/7541�2.06 (0.557, 0.612) (1.76, 3.81)
CHA2DS2-VASc
% in risk category 0.0 5.8 94.2 0.647 3.75
TE events, N (%) 0/2�0.00 3/653�0.46 181/10578�1.71 (0.613, 0.678) (1.20, 11.73)
*A hazard ratio of, eg, 2.26 indicates a 126% increase in the likelihood of a TE for each increase in risk cohort (low to intermediateor intermediate to high).
†Ischemic stroke, pulmonary embolism or peripheral embolism.CHADS2 indicates congestive heart failure, Hypertension, Age�75, Diabetes, prior Stroke/TIA; NICE, National Institute for health and
Clinical Excellence; ACC, American College of Cardiology; AHA, American Heart Association; ESC, European Society of Cardiology;ACCP, American College of Chest Physicians. Risk schemes, as defined in Table 1.
Figure 1. Proportions categorized as low, moderate, and high riskfor thromboembolism in relation to stroke risk stratification schema.
2734 Stroke December 2010
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

Increasing CHA2DS2-VASc score was associated with astepwise increase in rates of TE (Ptrend�0.0001; Table 4) andthis scheme had the greater HR (3.75; 95% CI, 1.20–11.73)of those tested, indicating a 275% increase in the likelihoodof TE for each increase in risk stratum (low to intermediate orintermediate to high), with the other RSS demonstratingbetween 80% (Framingham) and 150% increased risk of TEbetween incremental risk categories (Table 3). The negativepredictive value (ie, the percent categorized as “not high risk”actually being free from TE) for CHA2DS2-VASc was99.5%, which is reassuringly high and in excess of any of theother schema undergoing comparison (data not shown).
DiscussionIn this study comparing several stroke RSS in anticoagulatedAF patients, the CHADS2, Framingham, and CHA2DS2-VASc schema demonstrated broadly similar predictive abilityfor TE events (0.64, 0.62, and 0.65, respectively). TheCHA2DS2-VASc schema categorized the greatest number ofpatients as high risk (94.2%) compared to almost all the otherRSS (except Framingham), which classified two-thirds ofpatients as being at high risk. Despite the similar predictiveability of the RSS, evidenced by the c-statistic, CHA2DS2-VASc accurately predicted 98.4% of the TE events thatoccurred as being in the high-risk category. In addition,CHA2DS2-VASc had the highest HR of the tested schemesfor incremental risk strata and a high negative predictivevalue for TE.
By multivariate analysis, the only significant predictors ofTE were previous stroke or TIA, advanced age (75 years orolder), coronary disease, smoking, and reported nonuse ofalcohol. These observations are largely consistent with pre-vious analyses,8,22 whereas other previously identified riskfactors, such as hypertension, diabetes, heart failure, and leftventricular dysfunction, were not independent predictors ofTE in this trial cohort.
The lack of an association between hypertension and TE inthese analyses may be attributable to blood pressure control.
Typically, in randomized, controlled trials of antithrombotictherapy for stroke prevention, hypertensive patients musthave good pressure control. An earlier analysis of the SPORTIFdataset demonstrated that the mean (SD) blood pressurewas 131.8 (13.6)/77.5 (7.9) mm Hg, and that TE event rateswere low with well-controlled hypertension and increasedwith poor blood pressure control.23 In addition, the impor-tance of heart failure as a predictor of stroke risk in patientswith AF has been questioned.8 In keeping with a link betweenstroke and atherothrombotic vascular disease in patients withAF, we found that coronary artery disease was an indepen-dent predictor of primary events, given the high cardiovas-cular risk of AF associated with MI22,24,25 and peripheralarterial disease.26,27
Cigarette smoking was associated with an increased risk ofstroke, whereas reported alcohol use appeared protective.Smoking or nicotine may influence drug pharmacokinetics/dynamics, as well as other stroke risk factors. The AF Investi-gators failed to find that smoking was a significant inde-pendent risk factor for stroke, although there was a higherincidence of stroke in smokers compared to nonsmokers.28
Smoking has been associated with decreased mortality in theCopenhagen Stroke study,29 although this effect was signifi-cantly attenuated by age in multivariate analyses. In contrast,alcohol abuse is commonly regarded as contraindication toanticoagulation and was a reason for exclusion from clinicaltrials (including SPORTIF). One small, cross-sectional studyfound diabetes, alcohol, smoking, and left ventricular hyper-trophy were risk factors for stroke among 60- to 69-year-oldmen with AF.30 Alcohol abuse has been associated withmultiple medical complications, including stroke, and al-though modest alcohol consumption has been associated withreduced rates of cardiovascular events, we are unaware ofreports of a stroke-preventive effect in patients with AF.
This work also extends the validation of the CHA2DS2-VASc score in the Euro Heart survey of AF11 to a largeanticoagulated clinical trial cohort. In the Euro Heart analy-sis, which was confined to nonanticoagulated AF patients atbaseline, the CHA2DS2-VASc score performed marginallybetter than other schemes in that patients classified as “lowrisk” experienced no TE events during follow-up. In thepresent analysis, we were unable to confirm the predictiveaccuracy of this low-risk stratification, because patientswithout risk factors were excluded by the protocol, although40% were still classified as “low risk” according to theFramingham score. Furthermore, compared to the CHADS2,9
which classified �60% into the intermediate/moderate riskcategory, and the scheme of Rietbrock et al,16 which classi-fied 70% into the intermediate/moderate risk category, only15% were assigned to this risk stratum by the CHA2DS2-VASc scheme.
Previous comparisons of stroke RSS have been pub-lished,10,11,13,14,17,18,21,31 but only the recent analyses by Lipet al11 and Poli et al14 have included the contemporaryACC/AHA/ESC 2006,6 NICE 2006,5 and ACCP87 schemes.Most validation studies have been based on clinical trialcohorts, and few have applied the published schemes tounselected patients encountered in general clinical prac-tice.11,21,31 Several of the most widely accepted schemes were
Table 4. Stroke or Other Thromboembolism Events perPatient Year Based on the CHA2DS2VASc Scoring System
CHA2DS2
VASc Score NNo. of TEEvents/PY
TE Rate During1 Year (95% CI)
TE Rate During1 Year, Adjustedfor Warfarin use*
0 1 0/2 0.00 0.0
1 422 3/653 0.46 (0.10, 1.34) 1.3
2 1230 15/1913 0.78 (0.44, 1.29) 2.2
3 1730 31/2673 1.16 (0.79, 1.64) 3.2
4 1718 38/2665 1.43 (1.01, 1.95) 4.0
5 1159 42/1732 2.42 (1.75, 3.26) 6.7
6 679 36/1016 3.54 (2.49, 4.87) 9.8
7 294 15/436 3.44 (1.94, 5.62) 9.6
8 82 3/125 2.41 (0.53, 6.88) 6.7
9 14 1/18 5.47 (0.91, 27.0) 15.2
Total 7329 184/11233 P value for trend P�0.0001
*Theoretical TE rates without therapy: assuming that warfarin provides a64% reduction in TE risk, based on Hart et al.34 CI indicates confidence interval.
Lip et al Stroke Risk Schemes in AF 2735
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

derived from the nonwarfarin arms of clinical trial cohorts, inwhich the risk factors are often inadequately defined orincompletely recorded; also, the generalizability of trialcohorts have been questioned because only �10% of thosescreened in the initial trial cohorts were randomized.28 Asexamples, peripheral artery disease26,27 and MI24,25—well-established risk factors for stroke and mortality—do notfactor in most schemes, apart from NICE,5 CHA2DS2-VASc,11 and van Walraven et al.32 Female gender increasesthe risk of stroke in patients with and without AF;33,34
however, women are under-represented in clinical trials ofstroke prevention, prompting debate over the biologicalplausibility of this risk factor.5 Of note, female gender is arisk factor in the Framingham17 and the SPAF schemes,35 andthis has not been incorporated into all guidelinerecommendations.
Two studies compared the ACCP6, ACCP7, SPAF, AFI,Framingham, van Walraven, and CHADS2 schemes in co-horts of anticoagulated AF patients; one is based on patientsin an anticoagulation clinic14 with limited follow-up andanother is based on the SPORTIF population.13 Eventhe analysis of Gage et al10 is based on subjects receivingantiplatelet therapy, which may have a small effect on eventrates. The analysis we describe extends these by using morecontemporary stroke RSS and tries to identify those patientsremaining at high risk for stroke or TE despite anticoagula-tion. Because the availability of a contemporary nonantico-agulation AF cohort is increasingly unlikely, a hypotheticalexploration of TE event rates in relation to the CHA2DS2-VASc score if the population were not anticoagulated isshown in Figure 2.
It is worth emphasizing that the c-statistic in one validationstudy cannot be compared to that derived from another study,given the differences in study population and event rates.Nonetheless, published schemes have not improved theirpredictive ability (c-statistics still �0.6) despite the evolutionof RSS over the past 15 years. More accurate identification ofpatients at low risk will be important as better anticoagulantdrugs are introduced that offer a wider therapeutic marginthan vitamin K antagonists, allowing more effective treatmentto a broader segment of the AF population.12 In the presentstudy, the negative predictive value for CHA2DS2-VASc washigh and greater than that of any of the other schemaundergoing comparison.
LimitationsStroke rates and risk factors derived from clinical trialpopulations may differ from those in clinical practice. Theinclusion criteria for the SPORTIF trials resulted in under-representation of patients at low risk, preventing definitiveconclusions about the value of these indices to identify thoseat truly low risk, as was evident in our earlier analysis.11 Inaddition, this analysis did not identify hypertension, diabetesmellitus, and heart failure as independent predictors of TE,partly because patients were selected for inclusion into thetrials on the basis of these risk factors. As mentionedpreviously, better control of blood pressure reduces the rate ofstroke and it is possible that within the clinical trial setting,modifiable risk factors for stroke, such as hypertension,diabetes mellitus, and heart failure, are better-detected andmanaged, thereby reducing the effect of these risk factors onTE, which may explain the lack of an association demon-strated in the present analyses. Perhaps most important,because this analysis was confined to anticoagulated patients,risk factors most effectively ameliorated by anticoagulationmay not be identified. The value of one RSS schema overanother needs to be tested in a cohort of patients, eithernonanticoagulated or anticoagulated, including patients witha wider range of risk factors, ie, low, moderate, and high, todetermine the predictive ability and identify the most appro-priate RSS. The use of an anticoagulated cohort with bothwarfarin and ximelagatran may introduce potential heteroge-neity between treatment allocation; however, in the prespeci-fied pooled analysis of the 2 trials, there was no significantdifference in TE between the treatments (1.62% per year inthose using ximelagatran and 1.65% per year in those usingwarfarin; P�0.941).36 The results for the impact of individualrisk factors between the treatments was also surprisinglyconsistent when analyzed (data not shown).
Identification of patients who remain at high risk for strokedespite anticoagulation may affect treatment strategies inclinical practice. Outside of the clinical trial setting, mainte-nance of an adequate time in therapeutic range is moredifficult to attain, but this would be of paramount importancein anticoagulated AF patients at high risk to reduce the risk ofTE or major hemorrhage. These patients may require morefrequent international normalized ratio testing and dose ad-justment, or self-management of omeprazole-amoxicillin-clarithromycin therapy to improve time in therapeutic range
Figure 2. Stroke or other thromboembo-lism per patient-year based on theCHA2DS2-VASc scoring system.
2736 Stroke December 2010
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

may be an option,37 and such patients might benefit frompharmogenetic dosing.38 In addition, the current practice ofwithholding omeprazole-amoxicillin-clarithromycin therapyfor elective surgical procedures may need to be reviewed inpatients at high risk for stroke despite anticoagulation, war-ranting a reduction in omeprazole-amoxicillin-clarithromycinor bridging therapy.
ConclusionThis analysis identifies coronary artery disease and smokingas additional potential risk factors for TE in patients with AF.Of the available RSS, the CHA2DS2-VASc scheme correctlyidentified the greatest proportion of AF patients at high risk,despite the similar predictive ability of most RSS evidencedby the c-statistic.
AcknowledgmentsThe SPORTIF III and V investigators are listed in references 15 and 16.
DisclosureProfessors Lip and Halperin have received funding for research,educational symposia, consultancy, and lecturing from differentmanufacturers of drugs used for the treatment of atrial fibrillationand thrombosis, including AstraZeneca. Dr Frison is an employee ofAstraZeneca. Dr Lane is in receipt of an investigator-initiatededucational grant from Bayer Healthcare and has received sponsor-ship to attend educational meeting by industry, including AstraZen-eca and Boehringer Ingelheim.
References1. Lip GY, Lim HS. Atrial fibrillation and stroke prevention. Lancet Neurol.
2007;6:981–993.2. Connolly SJ, Eikelboom J, O’Donnell M, Pogue J, Yusuf S. Challenges of
establishing new antithrombotic therapies in atrial fibrillation. Circulation.2007;116:449–455.
3. Lip GY. Anticoagulation therapy and the risk of stroke in patients withatrial fibrillation at “moderate risk” [CHADS2 score�1]: simplifyingstroke risk assessment and thromboprophylaxis in real life clinicalpractice. Thromb Haemost. 2010;103:683–685.
4. Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A,Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Alings M, XavierD, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, WallentinL, RE-LY Steering Committee and Investigators. Dabigatran versuswarfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151.
5. National Collaborating Centre for Chronic Conditions. Atrial fibrillation:national clinical guideline for management in primary and secondarycare. London: Royal College of Physicians; 2006.
6. Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA,Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, PrystowskyEN, Tamargo JL, Wann S, Smith SC Jr., Jacobs AK, Adams CD,Anderson JL, Antman EM, Halperin JL, Hunt SA, Nishimura R, OrnatoJP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V,Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M,Morais J, Osterspey A, Tamargo JL, Zamorano JL, American College ofCardiology/American Heart Association Task Force on PracticeGuidelines, European Society of Cardiology Committee for PracticeGuidelines, European Heart Rhythm Association, Heart Rhythm Society.ACC/AHA/ESC 2006 Guidelines for the Management of Patients withAtrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and theEuropean Society of Cardiology Committee for Practice Guidelines(Writing Committee to Revise the 2001 Guidelines for the Managementof Patients With Atrial Fibrillation): developed in collaboration with theEuropean Heart Rhythm Association and the Heart Rhythm Society.Circulation. 2006;114:e257–e354.
7. Singer DE, Albers GW, Dalen JE, Fang MC, Go AS, Halperin JL, LipGY, Manning WJ, American College of Chest Physicians. Anti-thrombotic therapy in atrial fibrillation: American College of Chest Phy-
sicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest.2008;133:546S–592S.
8. Stroke Risk in Atrial Fibrillation Working Group. Independent predictorsof stroke in patients with atrial fibrillation: a systematic review. Neu-rology. 2007;69:546–554.
9. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, RadfordMJ. Validation of clinical classification schemes for predicting stroke:results from the National Registry of Atrial Fibrillation. JAMA. 2001;285:2864–2870.
10. Gage BF, van Walraven C, Pearce L, Hart RG, Koudstaal PJ, Boode BS,Petersen P. Selecting patients with atrial fibrillation for anticoagulation:stroke risk stratification in patients taking aspirin. Circulation. 2004;110:2287–2292.
11. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinicalrisk stratification for predicting stroke and thromboembolism in atrialfibrillation using a novel risk factor-based approach: the euro heart surveyon atrial fibrillation. Chest. 2010;137:263–272.
12. Lip GY, Halperin J. Improving stroke risk stratification in atrial fibril-lation. Am J Med. 2010;123:484–488.
13. Baruch L, Gage BF, Horrow J, Juul-Moller S, Labovitz A, Persson M,Zabalgoitia M. Can patients at elevated risk of stroke treated with anti-coagulants be further risk stratified? Stroke. 2007;38:2459–2463.
14. Poli D, Antonucci E, Grifoni E, Abbate R, Gensini GF, Prisco D. Strokerisk in atrial fibrillation patients on warfarin. Predictive ability of riskstratification schemes for primary and secondary prevention. ThrombHaemost. 2009;101:367–372.
15. Olsson SB, Executive Steering Committee of the SPORTIF III Investi-gators. Stroke prevention with the oral direct thrombin inhibitor ximel-agatran compared with warfarin in patients with non-valvular atrial fibril-lation (SPORTIF III): randomised controlled trial. Lancet. 2003;362:1691–1698.
16. Albers GW, Diener HC, Frison L, Grind M, Nevinson M, Partridge S,Halperin JL, Horrow J, Olsson SB, Petersen P, Vahanian A, SPORTIFExecutive Steering Committee for the SPORTIF V Investigators. Ximel-agatran vs warfarin for stroke prevention in patients with nonvalvularatrial fibrillation: a randomized trial. JAMA. 2005;293:690–698.
17. Wang TJ, Massaro JM, Levy D, Vasan RS, Wolf PA, D’Agostino RB,Larson MG, Kannel WB, Benjamin EJ. A risk score for predicting strokeor death in individuals with new-onset atrial fibrillation in the com-munity: the Framingham Heart Study. JAMA. 2003;290:1049–1056.
18. Rietbrock S, Heeley E, Plumb J, van Staa T. Chronic atrial fibrillation:incidence, prevalence, and prediction of stroke using the congestive heartfailure, hypertension, age�75, diabetes mellitus, and prior stroke ortransient ischaemic attack (CHADS2) risk stratification scheme. AmHeart J. 2008;156:57–64.
19. Albers GW, Dalen JE, Laupacis A, Manning WJ, Petersen P, Singer DE.Antithrombotic therapy in atrial fibrillation. The Sixth ACCP Conferenceon Antithrombotic and Thrombolytic Therapy. Chest. 2001;119:194S–206S.
20. Fuster V, Ryden LE, Asinger RW, Cannom DS, Crijns HJ, Frye RL,Halperin JL, Kay GN, Klein WW, Levy S, McNamara RL, PrystowskyEN, Wann LS, Wyse DG, Gibbons RJ, Antman EM, Alpert JS, Faxon DP,Fuster V, Gregoratos G, Hiratzka LF, Jacobs AK, Russell RO, Smith SC,Klein WW, Alonso-Garcia A, Blomstrom-Lundqvist C, De Backer G,Flather M, Hradec J, Oto A, Parkhomenko A, Silber S, Torbicki A,American College of Cardiology/American Heart Association/EuropeanSociety of Cardiology Board. ACC/AHA/ESC guidelines for the man-agement of patients with atrial fibrillation: a report of the AmericanCollege of Cardiology/American Heart Association Task Force onPractice Guidelines and the European Society of Cardiology Committeefor Practice Guidelines and Policy Conferences (Committee to DevelopGuidelines for the management of patients with atrial fibrillation). J AmColl Cardiol. 2001;38:1231–1266.
21. Fang MC, Go AS, Chang Y, Borowsky L, Pomernacki NK, Singer DE,ATRIA Study Group. Comparison of risk stratification schemes to predictthromboembolism in people with nonvalvular atrial fibrillation. J Am CollCardiol. 2008;51:810–815.
22. Hughes M, Lip GY, Guideline Development Group, National ClinicalGuideline for Management of Atrial Fibrillation in Primary and Sec-ondary Care, National Institute for Health and Clinical Excellence. Strokeand thromboembolism in atrial fibrillation: a systematic review of strokerisk factors, risk stratification schema and cost effectiveness data. ThrombHaemost. 2008;99:295–304.
Lip et al Stroke Risk Schemes in AF 2737
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

23. Lip GY, Frison L, Grind M, SPORTIF Investigators. Effect of hyper-tension on anticoagulated patients with atrial fibrillation. Eur Heart J.2007;28:752–759.
24. Schmitt J, Duray G, Gersh BJ, Hohnloser SH. Atrial fibrillation in acutemyocardial infarction: a systematic review of the incidence, clinicalfeatures and prognostic implications. Eur Heart J. 2009;30:1038–1045.
25. Siu CW, Jim MH, Ho HH, Miu R, Lee SW, Lau CP, Tse HF. Transientatrial fibrillation complicating acute inferior myocardial infarction: impli-cations for future risk of ischemic stroke. Chest. 2007;132:44–49.
26. Goto S, Bhatt DL, Rother J, Alberts M, Hill MD, Ikeda Y, Uchiyama S,D’Agostino R, Ohman EM, Liau CS, Hirsch AT, Mas JL, Wilson PW,Corbalan R, Aichner F, Steg PG, REACH Registry Investigators. Prev-alence, clinical profile, and cardiovascular outcomes of atrial fibrillationpatients with atherothrombosis. Am Heart J. 2008;156:855–863.
27. Conway DS, Lip GY. Comparison of outcomes of patients with symp-tomatic peripheral artery disease with and without atrial fibrillation (theWest Birmingham Atrial Fibrillation Project). Am J Cardiol. 2004;93:1422–1425.
28. Atrial Fibrillation Investigators. Risk factors for stroke and efficacy ofantithrombotic therapy in atrial fibrillation. Analysis of pooled data fromfive randomized controlled trials. Arch Intern Med. 1994;154:1449–1457.
29. Kammersgaard LP, Olsen TS. Cardiovascular risk factors and 5-yearmortality in the Copenhagen Stroke study. Cerebrovasc Dis. 2006;21:187–193.
30. Novello P, Ajmar G, Bianchini D, Bo GP, Cammarata S, Firpo MP,Parodi CI, Patrone A, Pizio N, Poeta MG, Simonetti S, Venturi S, Sacco
G. Ischemic stroke and atrial fibrillation. A clinical study. Ital J NeurolSci. 1993;14:571–576.
31. Stroke Risk in Atrial Fibrillation Working Group. Comparison of 12 riskstratification schemes to predict stroke in patients with nonvalvular atrialfibrillation. Stroke. 2008;39:1901–1910.
32. van Walraven C, Hart RG, Wells GA, Petersen P, Koudstaal PJ, GullovAL, Hellemons BS, Koefed BG, Laupacis A. A clinical prediction rule toidentify patients with atrial fibrillation and a low risk for stroke whiletaking aspirin. Arch Intern Med. 2003;163:936–943.
33. Lane DA, Lip GY. Female gender is a risk factor for stroke and throm-boembolism in atrial fibrillation patients. Thromb Haemost. 2009;101:802–805.
34. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapyto prevent stroke in patients who have nonvalvular atrial fibrillation. AnnIntern Med. 2007;146:857–867.
35. Hart RG, Pearce LA, McBride R, Rothbart RM, Asinger RW. Factorsassociated with ischaemic stroke during aspirin therapy in atrial fibril-lation: analysis of 2012 participants in the SPAF I-III clinical trials. TheStroke Prevention in Atrial Fibrillation (SPAF) Investigators. Stroke.1999;30: 1223–1229.
36. Albers GW, SPORTIF Investigators. Stroke prevention in atrial fibril-lation: pooled analysis of SPORTIF III and V trials. Am J Manag Care2004;10(Suppl 14):S462–S469; discussion S469–S473.
37. Heneghan C, Alonso-Coello P, Garcia-Alamino JM, Perera R, Meats E,Glasziou P. Self-monitoring of oral anticoagulation: a systematic reviewand meta-analysis. Lancet. 2006;367:404–411.
38. Tan GM, Wu E, Lam YY, Yan BP. Role of warfarin pharmacogenetictesting in clinical practice. Pharmacogenomics. 2010;11:439–448.
2738 Stroke December 2010
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

Gregory Y.H. Lip, Lars Frison, Jonathan L. Halperin and Deirdre A. LaneCohort
FibrillationContemporary Stroke Risk Stratification Schemes in an Anticoagulated Atrial Identifying Patients at High Risk for Stroke Despite Anticoagulation: A Comparison of
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2010 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.110.590257
2010;41:2731-2738; originally published online October 21, 2010;Stroke.
http://stroke.ahajournals.org/content/41/12/2731World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2012/04/02/STROKEAHA.110.590257.DC2 http://stroke.ahajournals.org/content/suppl/2012/03/12/STROKEAHA.110.590257.DC1
Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

37
Abstract 11

38 Stroke Vol. 4, No. 1
65
Lip et al Stroke Risk Schemes in AF
Original Contributions
From the University of Birmingham Centre for Cardiovascular Sciences (G.Y.H.L., D.A.L.), City Hospital, Birmingham, England, UK; AstraZeneca R&D Mölndal (L.F.), Mölndal, Sweden; The Cardiovascular Institute (J.L.H.), Mount Sinai Medical Center, New York, NY.
Correspondence to Professor G.Y.H. Lip, University of Birmingham Centre for Cardiovascular Sciences, City Hospital, Birmingham, England, UK. E-mail [email protected]© 2010 American Heart Association, Inc.
在应用抗凝剂治疗的患者中识别出卒中高危人群:
比较几种同期卒中风险分层策略在接受抗凝治疗的房颤患者队列中的应用情况
Identifying Patients at High Risk for Stroke Despite AnticoagulationA Comparison of Contemporary Stroke Risk Stratification Schemes in an Anticoagulated
Atrial Fibrillation CohortGregory Y.H. Lip, MD; Lars Frison, PhD; Jonathan L. Halperin, MD; Deirdre A. Lane, PhD
背景与目的:房颤 (AF) 患者中发生卒中事件的危险因素并非是单一的,多种临床危险因素被应用于卒中风险
分层方案 (RSS),在应用抗凝治疗的患者队列中,研究的重点应放在识别出那些在抗凝治疗的同时仍存在卒中
高风险的人群上。
研究方法:研究人员调查了房颤临床队列中接受抗凝治疗的患者,了解其发生血栓栓塞事件的风险预测因素
(n=7329),并检验卒中风险分层方案对这部分人群的风险预测值,使用的卒中风险分层方案包括 CHADS2 评分、
Framingham 危险评分、英国国家卫生与临床研究院 (NICE)2006 指南、ACC/AHA/ESC 2006 指南、美国胸科
医师学会 (ACCP) 指南第八版,以及 CHA2DS2-VASc 评分。
结论:通过多变量分析发现,对血栓栓塞事件有统计学意义的风险预测值包括既往卒中 / 短暂性脑缺血发
作 (TIA) 病 史 ( 风 险 比 [HR],2.24 ;P<0.001)、 年 龄 ≥75 岁 (HR,1.77 ;P=0.0002)、 冠 心 病 (HR,1.52 ;
P=0.0047) 以及吸烟 (HR,2.10;P=0.0005)。相反,根据研究显示,饮酒成为血栓栓塞性事件的保护因素 (HR,0.70 ;P=0.02)。比较同时期几种卒中风险分层方案显示,对于房颤患者存在几种不同的风险分层方法,尽管
代表其对于血栓栓塞事件识别能力的 c 统计量是相似的,范围从 0.575(NICE 2006 指南 ) 到 0.647(CHA2DS2-VASc 评分 ) 不等。采取 CHA2DS2-VASc 评分的风险分层方案中,有 94.2% 的患者处于高风险级别,而应用其他
风险分层方案仅 2/3 的患者处于高风险组。在发生的 184 例血栓栓塞事件中,CHA2DS2-VASc 评分可以识别出其
中的 181 例并纳入卒中高风险组 (98.4%),随着 CHA2DS2-VASc 评分的增高,血栓栓塞事件发生的风险增高 (P趋
势 <0.0001),在几种风险分层方案中 CHA2DS2-VASc 评分有着最高的风险比 (HR=3.75)。而 CHA2DS2-VASc 的
阴性预测值 ( 即认为处于非高风险组的患者中实际未发生血栓栓塞事件的百分率 ) 为 99.5%。
结论:在应用抗凝治疗的房颤患者中冠心病和吸烟均为发生血栓栓塞的额外危险因素,而饮酒似乎对血栓栓
塞的发生具有保护作用。在同时期几种卒中风险分层方案中,CHA2DS2-VASc 评分可以在房颤患者中正确鉴
别出绝大多数的卒中高危人群,尽管这些风险分层方案利用 c- 统计量考量其对卒中事件的预警能力时得到的
是相似的结果。
关键词:房颤,华法林
(Stroke. 2010;41;2731-2738. 中山大学附属第一医院神经内科 赵 译 曾进胜 校 )
房颤 (AF) 是脑卒中及血栓栓塞事件一项确定的
危险因素,但这种危险因素对所有患者而言并非是
同质性的。多种临床危险因素构成了卒中风险分层
方案 (RSS) 以及房颤患者卒中预防临床实践指南的
基础 [1]。尽管房颤患者队列中卒中发生率本身在减
少 [2],但在存在中度及重度卒中危险因素的房颤患
者中用华法林代替阿司匹林的治疗仍降低了其卒中
发生的相对危险性 [3]。
结合目前临床实践上的总体趋势,现需要当前
的数据用以评估卒中事件发生的危险因素以及几种
卒中风险分层方案的相对预测值。现在越来越多的
新型抗凝药物被应用于临床,和维生素 K 拮抗剂比

66
Stroke December 2010
较具有更安全更便利的特点 [4],这就需要卒中风险
分层方案必须能够更为精准的识别出“真正的卒中
低风险”的房颤患者,这样能使更多的危险人群可
以成为接受抗凝治疗的候选者。这些卒中风险分层
方案同时应尽可能缩小 “ 中等风险 ” 组的患者数量,
因为目前的指南对于何为最优抗血栓治疗方案尚无
一清晰的定义 [5-7]。
许多危险因素的得出来自对未应用华法林抗凝
治疗临床试验的研究分析 [8],而其他的研究未能在
试验中进行系统的评定及记录。风险分层方案中涵
盖的卒中危险因素需要在多种人群中得到确认,尽
管其中很多危险因素已经在试验队列中得到证实。
举例而言,一项应用最为普遍的 CHADS2 评分 ( 充血性心衰、高血压、年龄、糖尿病 [ 评分各 1 分 ] 及卒中 [ 评分 2 分 ]) 已经从最初应用于房颤研究扩展
到现在应用于房颤患者卒中预防的危险因素 (SPAF)分层方案研究,其准确性已在一项来自心房颤动国
家注册研究 (NRAF)[9] 以及一个针对接受阿司匹林治
疗患者的荟萃分析 [10] 中得到证实。据新近的报导,
2006 年美国心脏病协会联合美国心脏协会及欧洲心
脏病协会 (ACC/AHA/ESC) 共同制定的房颤指南中
建议采用 CHA2DS2-VASc 评分 ( 心衰或心功能不全、
高血压、糖尿病 [ 评分各 1 分 ],年龄 ≥75 岁 [ 评分
2 分 ],卒中 [ 评分 2 分 ],血管疾病、年龄 65-74 岁、
女性 [ 评分各 1 分 ]) 为卒中风险分层方案,欧洲一
项纳入 1084 名在基线水平未接受抗凝治疗的患者队
列研究已经验证了该评分预测的准确性 [11]。
目前对于卒中二级预防药物的选择更趋向于用
抗凝药物取代抗血小板药物 [12],这就更强调卒中风
险分层方案能够准确识别出处于卒中中重度风险级
别患者的重要性。另外,在已经规范应用抗凝治疗
的患者 ( 维持国际标准化比值 [INR] 在治疗所需的范
围内 ) 中识别出那些仍处于卒中高风险级别的人群
是极为重要的,针对当前的卒中风险分层方案对这
部分人群能否准确识别的研究数据尚十分有限 [13,14],
仅有一项小规模的研究比较了当前几种卒中风险分
层方案对于卒中事件发生的预测能力 [14]。
本研究分析的目的在于对两项同期开展的大型
临床试验即 SPORTIF( 采用口服凝血酶抑制剂防止
AF 患者发生卒中 )III 期及 V 期试验数据进行分析,
识别出血栓栓塞的危险因素。这项临床试验比较了
在卒中中高风险组的房颤患者中应用华法林或口服
直接凝血酶抑制剂希美加群对卒中事件及全身性血
栓栓塞事件发生的预防情况 [15,16]。研究人员利用这
项队列评估同时期几种卒中风险分层方案对于卒中
事件的预测值 (CHADS2 评分 [9],Framingham 危险
评分 [17],英国国家卫生与临床研究院 (NICE) 指南
2006[5],ACC/AHA/ESC 评分 2006[6],美国胸科医
师学会指南第八版 (ACCP) 8 评分 [7] 以及 CHA2DS2-VASc 评分 [11]),并利用 CHA2DS2-VASc 评分在抗凝
治疗组患者中识别出在接受抗凝治疗的同时仍处于
卒中高风险组的患者。
研究对象和方法研究人群
研究人员调查了在 SPORTIF III 期及 V 期临床
试验中接受抗凝治疗的 7329 名房颤患者 ( 均接受
华法林或希美加群治疗 ),研究这些患者血栓栓塞
的危险因素,并检验几种不同的卒中风险分层方案
对于卒中发生的预测值,特别是 CHADS2 评分 [9]、
Framingham 危 险 评 分 [17]、2006 年 NICE 评 分 [5]、
2006年ACC/AHA/ESC评分 [6]、ACCP指南第八版 [7]、
CHA2DS2-VASc 评分 [11] 以及由 Riebrock 等人修正的
改良 CHADS2 评分 [18]。
SPORTIF III 期及 V 期临床试验的基本原理、试
验设计以及试验结果已经发表 [15,16]。概括来说,这
项随机、多中心、平行对照试验根据 2001 年指南推
荐的标准在非瓣膜病变的阵发性房颤、持续性房颤
及永久性房颤患者中选择出处于卒中中、高危组人
群,在这部分人群中预防性应用希美加群或华法林,
比较这两种药物对脑卒中或全身性栓塞事件的预防
效果 [19,20]。受试者随机接受固定剂量的希美加群 ( 每日两次,每次 36 mg) 或根据个体情况调整用量的华
法林 ( 维持 INR 在 2.0-3.0 之间 ),SPORTIF III 期临
床试验为开放性试验,而 SPORTIF V 期临床试验为
双盲试验。
临床终点的判断
在随机分组之后,起初在第 1、4、6 周随访患者,
之后随访时间在 2、3、4、5、6、8、10 及 12 个月,
之后每 3 个月随访患者一次,直至监测到发生脑卒
中或全身性血栓栓塞 ( 主要事件 )、短暂性脑缺血发
作 (TIA)、急性心肌梗塞或出血性并发症。定期对患
者进行标准化卒中症状问卷调查有助于帮助发现卒
中事件的发生;对于有阳性结局发生的患者则需进
行进一步评估。由一位研究相关的神经病学家或卒
中专家利用临床发现及颅脑 CT 或 MRI 的辅助检查
结果尽可能迅速的对所有可能的主要事件及 TIA 做
67
Lip et al Stroke Risk Schemes in AF
表 1 卒中风险分层方案在房颤患者中用于预测血栓栓塞事件发生的应用情况
风险分层方案
经典 CHADS2
评分 (2001 年 )改良 CHADS2 评分
Framingham 危险评分
NICE 指南 2006
ACC/AHA/ESC 指南 2006
Rietbrock 等人 2008 改良版 †
ACCP 指南第八版 (2008)
CHA2DS2-VASc 评分 (2009)
参考文献
9
15 5
6
16 7
11
低风险
积分 0
积分 0积分 7年龄 <65 岁
无中、高危险因素
无相关危险因素
积分 0无相关危险因素
无相关危险因素
中风险
积分 1-2
积分 1积分 8-15
年龄 ≥65 岁,无高风险因素
年龄 <75 岁,伴有高血压、糖
尿病或血管疾病 *
年龄 ≥75 岁;或合并高血压;
或合并心衰;或 LVEF≤35% ;
或合并糖尿病
积分 1-5年龄 >75 岁;或合并高血压;
或伴有中度 - 重度的 LVEF 降
低,伴 / 不伴心功能不全;或
合并糖尿病
存在一项“临床相关非主要”
的危险因素 ( 心衰 /LVEF≤40%、
高血压、糖尿病、血管疾病 *、
女性患者、年龄在 65-74 岁 )
高风险
积分 3-6
积分 2-6积分 16-31
既往出现过脑卒中 /TIA 或血栓栓塞病史
年龄 ≥75 岁,伴有高血压、糖尿病或血
管疾病 *
临床证据表明存在瓣膜病变,心衰或左
心功能不全
既往出现过脑卒中,TIA 或血栓栓塞病
史,或 ≥2 项中等危险因素 ( 年龄 ≥75 岁、
高血压、心衰、LVEF≤35%、糖尿病 )积分 6-14
既往出现过脑卒中,TIA 或血栓栓塞病
史,或 ≥2 项中等危险因素 ( 年龄 >75 岁、
高血压、中度 - 重度的 LVEF 降低,伴或
伴有心功能不全、糖尿病 )存在一项“主要危险因素”( 既往出现过
脑卒中、TIA 或血栓栓塞病史、或年龄
≥75 岁 ) 或存在 ≥2 项“临床相关非主要”
的危险因素 ( 心衰 /LVEF≤40%、高血压、
糖尿病、血管疾病 *、女性患者、年龄在
65-74 岁 )
* 心肌梗塞,周围动脉疾病或大动脉斑块形成。† 此风险分层方案为 CHADS2 积分的改良版,此方案将年龄分为以下六个年龄组:40-64,65-69,70-74,75-79,80-84,85-115,每个组的积分
随年龄而增加,分别记为 1-6 分;女性患者记 1 分;合并糖尿病的患者记 1 分;既往曾有过脑卒中或 TIA 病史的记 6 分。
ACC :美国心脏病协会;ACCP :美国胸科医师学会;AHA :美国心脏协会;CHADS2 :充血性心衰,高血压,年龄 >75 岁,糖尿病,既往脑
卒中 /TIA 病史;ESC :欧洲心脏病协会;LVEF :左心室射血分数;NICE :英国国家卫生与临床研究院;TIA :短暂性脑缺血发作。
表 2 各危险因素对血栓栓塞事件预测能力的单因素及多因素分析结果 事件发生率
( 每患者 - 年 ) 单因素分析 多因素分析 * 是否存在危险因素 风险比 (HR)† 风险比 (HR)†
危险因素 是 否 (95% CI) P 值 (95% CI) P 值
既往脑卒中 /TIA 病史 3.05 1.28 2.35 (1.74, 3.17) <0.0001 2.24 (1.66, 3.02) <0.0001年龄 ≥75 岁 2.25 1.26 1.78 (1.34, 2.38) <0.0001 1.77 (1.32, 2.38) 0.0002冠心病 2.04 1.31 1.57 (1.17, 2.10) 0.0025 1.52 (1.14, 2.04) 0.0047吸烟 2.68 1.54 1.75 (1.16, 2.63) 0.0074 2.10 (1.38, 3.18) 0.0005饮酒 1.31 1.91 0.69 (0.51, 0.93) 0.014 0.70 (0.52, 0.95) 0.020全身性血栓栓塞事件 3.24 1.56 2.08 (1.24, 3.47) 0.0052 女性患者 2.08 1.44 1.44 (1.07, 1.93) 0.016 糖尿病 1.92 1.55 1.23 (0.89, 1.71) 0.21 高血压 1.72 1.38 1.24 (0.86, 1.79) 0.24 左心室功能不全 1.67 1.62 1.03 (0.77, 1.39) 0.84 * 考察的危险因素中仅 P<0.05 的危险因素保留至最终的回归模型中。在华法林治疗的患者中,以上危险因素与作为对照应用的抗凝治疗似乎并
无很大的相关性,例如,在 3665 名接受华法林治疗的患者中,非吸烟者 (n=3331) 中平均 INR 值为 2.42,INR 控制在 2-3 之间的占 66.1% ;而
吸烟者 (n=334) 中平均 INR 值为 2.44,INR 控制在 2-3 的人群占 65.7%。† 风险比结果来自于 Cox 回归模型。
TIA 即短暂性脑缺血发作。
出评估,这个过程要求研究者必须对患者的分组及
接受的治疗处于盲态。最后由一个同样处于盲态的
独立的临床事件裁定委员会对所有报告的主要事件
和次要事件进行审核。

68
Stroke December 2010
风险分层方案
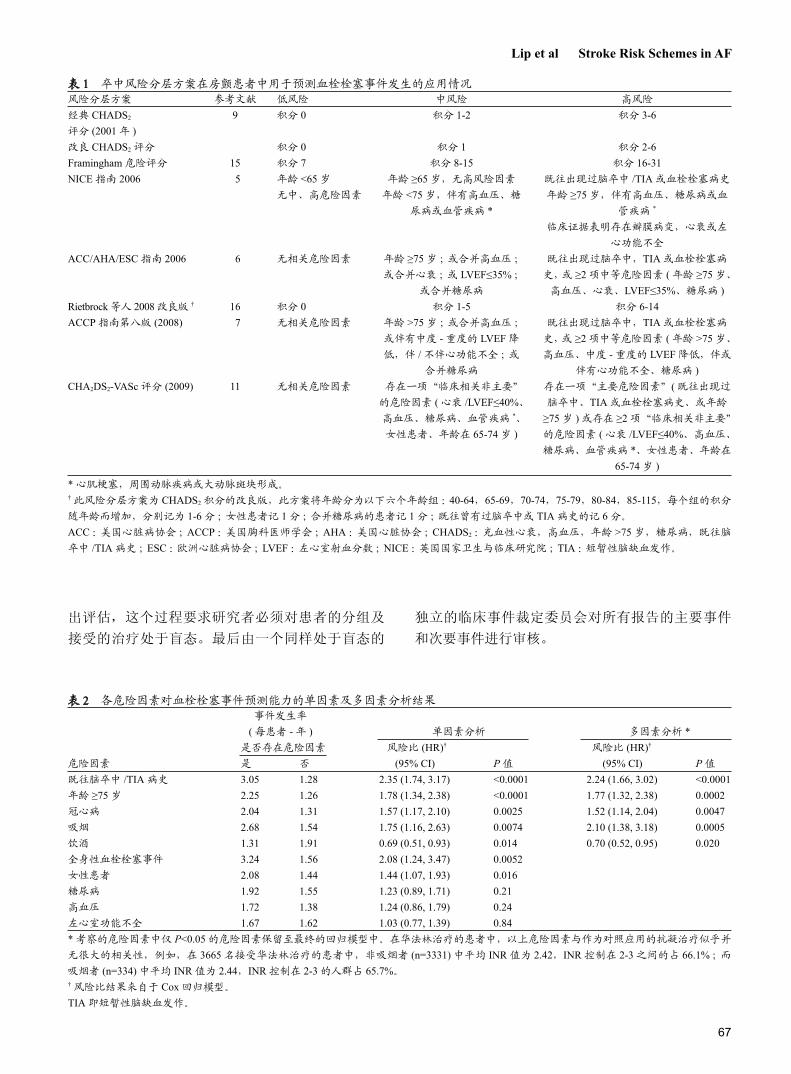
表 1 总结了研究人员在这项队列研究中对危险
因素进行评估时采用的各种卒中风险分层方案,其
中 Framingham 危险评分及 CHADS2 评分是基于分
数的分层方法。Framingham 危险评分是对患者的年
表 3 RSS 风险分层情况、各级别血栓栓塞事件的发生率及各方案对血栓栓塞事件的辨别能力 风险等级 辨别力
低 中 高 c- 统计量 HR(95% CI)经典 CHADS2 评分 占危险分层患者的比率 (%) 2.0 64.0 34.0 0.637 2.26*
血栓栓塞事件发生率 0/238=0.00 87/7276=1.20 97/3719=2.61 (0.607,0.674) (1.71,3.00)改良 CHADS2 评分 占危险分层患者的比率 (%) 2.0 31.1 66.9 0.637 2.50 血栓栓塞事件发生率 0/238=0.00 31/3563=0.87 153/7431=2.06 (0.607,0.674) (1.72,3.63)Framingham 危险评分 占危险分层患者的比率 (%) 40.1 38.2 21.7 0.621 1.81 血栓栓塞事件发生率 41/4547=0.9 72/4299=1.67 71/2386=2.98 (0.589,0.658) (1.50,2.18)NICE 指南 2006 占危险分层患者的比率 (%) 0.0 31.8 68.2 0.575 2.28 血栓栓塞事件发生率 0/2=0.0 32/3651=0.88 152/7580=2.01 (0.547,0.600) (1.56,3.34)ACC/AHA/ESC 2006 占危险分层患者的比率 (%) 1.8 30.3 67.8 0.587 2.58 血栓栓塞事件发生率 0/212=0.00 29/3469=0.84 155/7551=2.05 (0.557,0.611) (1.75,3.79)Rietbrock 等人改良版 占危险分层患者的比率 (%) 0.1 70.0 29.9 0.629 2.59 血栓栓塞事件发生率 0/10=0.0 89/7964=1.12 95/3258=2.92 (0.587,0.668) (1.94,3.46)ACCP 指南 (2008) 占危险分层患者的比率 (%) 1.8 30.4 67.8 0.587 2.59 血栓栓塞事件发生率 0/212=0.00 29/3479=0.83 155/7541=2.06 (0.557,0.612) (1.76,3.81)CHA2DS2-VASc 评分 占危险分层患者的比率 (%) 0.0 5.8 94.2 0.647 3.75 血栓栓塞事件发生率 0/2=0.00 3/653=0.46 181/10578=1.71 (0.613,0.678) (1.20,11.73)* 风险比,如 HR=2.26,代表着随着风险等级的增高 ( 低风险升级为中风险,中风险升级为高风险 ),日后发生血栓栓塞事件的风险增加 126%。
CHADS2 指充血性心衰,高血压,年龄 >75 岁,糖尿病,既往脑卒中 /TIA 病史;NICE :英国国家卫生与临床研究院;ACC :美国心脏病协会;
AHA :美国心脏协会;ESC :欧洲心脏病协会;ACCP :美国胸科医师学会;风险分层标准参考表 1。
图 1 不同卒中分层方案中发生血栓栓塞事件的低危、中危及高危人
群比例分布
高危组中危组低危组
CHA2DS2-VASc 评分
ACCP8
ACC/AHA/ESC
NICE 2006
改良 CHADS2 评分
经典 CHADS2 评分
Rietbrock 等人改良版
Framingham 危险评分
0% 20% 40% 60% 80% 100%
龄、性别、收缩压水平、糖尿病情况、既往出现过
的卒中或 TIA 事件进行赋值,通过数学公式计算得
出 [17] ;而 CHADS2 评分则将充血性心衰、高血压、
年龄超过 75 岁及糖尿病各记 1 分,既往出现过卒中
或 TIA 事件记 2 分叠加后得出 [9]。研究人员采用两
种不同的方式定义 CHADS2 评分:(1) 经典 CHADS2
评分:评分为 0 记为低风险组,评分 1-2 为中度风
险组,评分 >2 为高风险组;(2) 改良 CHADS2 评分:
评分为 0 记为低风险组,评分 1 为中度风险组,评
分 ≥2 为高风险组。研究人员利用 Framingham 危险
评分进行的风险分层方案在某种意义上与 Fang 等人[21]提出的方案相类似:评分在0-7之间的为低风险组,
评分在 8-15 之间的为中度风险组,评分在 16-31 之
间的为高风险组。而 CHA2DS2-VASc 评分分层方案
则将评分为 0 记为低风险组,评分为 1 记为中度风
险组,评分 ≥2 则为高风险组 [11]。这些人为的定义
方法已普遍应用于临床实践,Framingham 危险评分、
CHADS2 评分以及 CHA2DS2-VASc 评分的预测性也
应作为连续变量接受评估 ( 似乎更为恰当 )。

69
Lip et al Stroke Risk Schemes in AF
统计分析
结合 SPORTIF III 期及 V 期临床试验数据,研
究的首要工作即分析风险分层方案对脑卒中 ( 缺血
性或出血性 ) 及全身血栓栓塞事件发生的预测准确
性。意向治疗分析的研究对象包括所有接受随机分
组的受试者直至研究结束,而无论其是否真正从始
至终接受了该组的治疗。Cox 回归模型将血栓栓塞
作为因变量,通过单因素分析评估各个危险因素对
因变量 ( 血栓栓塞 ) 的影响。从建立的这些模型中可
以获得风险比 (Hazard ratios,HR) 及其 95% 可信区
间 (CI)。将所有潜在致血栓栓塞的危险因素都通过
一个多因素 Cox 回归分析模型进行单因素分析,从
这些待选择的变量中筛选出 P<0.05 的变量纳入最终
的多因素 Cox 回归分析模型。对于所有调查的风
险分层方案,在将患者分为低、中、高危组后分
别对各个组每患者年血栓栓塞事件的发生率进行
评估,从 Cox 回归分析模型中获得各个危险组的
HR 值。而通过计算 c- 统计量,一个度量受试者
操作特征曲线下面积的统计量,则将每一种危险
分层方案的预测效度加以量化,即将分层方案的
积分作为一连续变量,建立起此风险分层方案的
实施对于卒中事件发生的预测是具有统计学意义的
假设,对其进行假设检验 ( 当 c- 统计量 ≥0.5 时假
设检验即成立 )。C- 统计量将各个风险分层方案对
于卒中危险因素的识别能力加以量化,而 HR 则对
随着危险分层级别的增高其发生卒中事件增加的相
对风险进行了量化。
结果表 2 记录了各种危险因素对血栓栓塞事件预测
能力的单因素及多因素分析。在单因素分析中,既
往脑卒中、TIA 及全身性血栓形成病史、年龄 ≥75 岁、
冠心病、吸烟及女性患者均预示着会增加血栓栓塞
事件发生的危险性,而饮酒则预示着低风险。值得
注意的是糖尿病、高血压及左心功能不全在这些患
者中未能预测血栓栓塞事件的发生。在多因素分析
中对血栓栓塞的发生具有统计学意义的预测值仅有
以下四项:既往脑卒中或 TIA 病史 (HR,2.24 ;95% CI,1.66-3.02 ;P<0.001),年龄 ≥75 岁 (HR,1.77 ;
95% CI,1.32-2.38 ;P=0.0002),冠心病 (HR,1.52 ;
95% CI,1.14-2.04;P=0.0047) 以及吸烟 (HR,2.10;95% CI,1.38-3.18 ;P=0.0005),而饮酒似乎成为了
血栓栓塞事件发生的保护因素 (HR,0.70 ;95% CI,0.52-0.95 ;P=0.02)。
不同的风险分层方案对患者的分类不同 ( 表3,图 1),因为 SPORTIF 试验的纳入标准所限,几
乎所有风险分层方案均将很少的患者归类于低风险
组,而 Framingham 危险评分是一个特例,以 Fang等人的判断标准 40.1% 的受试者被纳入低风险组 [21]。
CHA2DS2-VASc 评分分层方案没有将任何一名患者
纳入低风险组,而其他风险分层方案纳入低风险组
的患者占所有受试者的比例大约为 2%( 表 3)。所有
的风险分层方案除经典 CHADS2 评分和 CHA2DS2-VASc 评分外,基本上约 2/3 的患者被纳入卒中高风
险组,而采取 CHA2DS2-VASc 评分的风险分层方案
几乎绝大多数的患者均纳入高风险组 (94.2%)。在 11 233 人年的随访期中共发生 184 件血栓
栓塞事件 ( 发病密度每 100 患者 - 年 1.64%)。各种
风险分层方案所分类的高危组患者中,以 Framing-ham 风险评分分层方案的高危组人群中血栓栓塞事
件的发生率最高 (2.98%),除 CHA2DS2-VASc 评分
外,其他分层方案的高危组患者中血栓栓塞事件的
发生率均在 2% 以上。值得注意的是,CHA2DS2-VASc 评分方案所评价为卒中高风险组的患者中有高
达 181 名患者日后发生了血栓栓塞事件 ( 占所有发
生血栓栓塞事件患者的 98.4%)。所有的风险分层方
案的 c- 统计量均 >0.5,这证明了研究所考察的几种
危险分层方案对于血栓栓塞事件预测的准确性并非
偶然。C- 统计量的值从 0.575(NICE 2006 指南 ) 到0.647(CHA2DS2-VASc) 不等。
以 CHA2DS2-VASc 评分分层方案为例,随着
CHA2DS2-VASc 评分的增加,血栓栓塞事件发生率
表 4 基于 CHA2DS2-VASc 评分系统的每患者年卒中或其他
血栓栓塞事件发生情况 1 年内血栓
血栓栓塞 1 年内血栓 栓塞发生率,
CHA2DS2- 患者 事件数 / 栓塞发生率 校正华法林
VASc 评分 数 患者年 (95% CI) 治疗影响 *
0 1 0/2 0.00 0.01 422 3/653 0.46(0.10,1.34) 1.32 1230 12/1913 0.78(0.44,1.29) 2.23 1730 31/2673 1.16(0.79,1.64) 3.24 1718 38/2665 1.43(1.01,1.95) 4.05 1159 42/1732 2.42(1.75,3.26) 6.76 679 36/1016 3.54(2.49,4.87) 9.87 294 15/436 3.44(1.94,5.62) 9.68 82 3/125 2.41(0.53,6.88) 6.79 14 1/18 5.47(0.91,27.0) 15.2总和 7329 184/11233 趋势 P 值 P<0.0001* 除外治疗影响的理论血栓栓塞事件发生率:即根据 Hart 等人的研究,
假定华法林可以将血栓栓塞的风险降低 64%[34]。

70
Stroke December 2010
亦在逐步增加 (P 趋势 <0.0001,表 4),此项风险分层
方案有着较高的 HR(3.75 ;95% CI,1.20-11.73),预
示着随着风险分层等级的增高 ( 由低风险级别升至
中风险级别,或从中风险级别升至高风险级别 ),患
者日后罹患血栓栓塞性疾病的可能性增加 275%,
而其他危险分层方案随着患者所处风险等级的增
高,日后血栓栓塞事件发生危险性的增加幅度在
80%(Framingham 危险评分 ) 到 150% 之间 ( 表 3)。而 CHA2DS2-VASc 评分的阴性预测值 ( 即归类于非
卒中高危组的患者中在随访期内实际上也没有发生
血栓栓塞性事件的比例 ) 高达 99.5%,超过了其他的
风险分层方案 ( 数据未罗列 )。
讨论这次研究对比了几种卒中风险分层方案在接受
抗凝治疗的房颤患者中的应用,证实 CHADS2 评分、
Framingham 危险评分及 CHA2DS2-VASc 评分对可
能发生的血栓栓塞事件有着相似的预测能力 ( 分别
为 0.64、0.62 及 0.65),与其他风险分层方案相比,
CHA2DS2-VASc 评分分类于高风险组的患者人数最
多 ( 达 94.2%),而其他绝大多数风险分层方案 ( 除Framingham 危险评分之外 ) 中高风险组的患者一般
占总人群的 2/3。尽管以 c- 统计量作为卒中危险因
素识别能力量化指标的证据显示各个风险分层方案
对于卒中事件预警能力相似,但是 CHA2DS2-VASc评分可以正确识别出 98.4% 日后发生血栓栓塞事件
的高危人群并将其归类于高风险组。另外 CHA2DS2-VASc 评分的风险比最高,预示随风险等级的增高患
者日后发生血栓栓塞事件的几率也在明显增加;同
时 CHA2DS2-VASc 评分亦有着很高的阴性预测值。
通过多因素分析,在各种可能的危险因素中对
血栓栓塞事件具有统计学意义的预测指标包括既往
卒中或 TIA 病史、高龄患者 ( 年龄 ≥75 岁 )、冠心病、
吸烟以及不饮酒。以上这些研究发现与先前的一些
研究分析相一致 [8,22],而先前经研究证实的另一些危
险因素,如高血压、糖尿病、心衰及左心功能不全
在这次的临床试验中被认为并非血栓栓塞事件独立
的预测因素。
此次研究分析证实缺少高血压与血栓栓塞
事件必然相关的证据,这个结果可能可以归因于
血压的控制。一般来说,在一个为了考察抗血栓
治疗对卒中预防影响的随机临床对照试验中,高
血压患者必须将血压控制在一个良好的水平,早
期 SPORTIF 临床试验分析显示受试者平均血压为
131.8(13.6)/77.5(7.9) mmHg,血压水平控制理想,血
栓栓塞事件发生率低;血压水平控制不理想,血栓
栓塞事件发生率高 [23]。另外,心衰作为房颤患者发
生卒中风险预测因素的重要性也备受质疑 [8]。卒中
事件与房颤患者间的相关性同动脉粥样硬化血栓形
成性疾病与后者之间的联系相一致,研究人员发现
冠心病是血栓栓塞事件一个独立的预测因素,房颤
合并冠心病患者为发生心肌梗塞 [22,24,25] 或外周动脉
疾病 [26,27] 等心血管血栓形成事件的高风险人群。 吸烟增加了卒中事件发生的风险,与此同时,
饮酒似乎成为了卒中的保护因素。同其他的卒中危
险因素一样,尼古丁可能通过影响药代动力学起作
用。先前房颤研究人员未能发现吸烟是卒中事件发
生的独立危险因素,尽管吸烟的房颤患者中卒中的
发生率较非吸烟的房颤患者增高 [28]。在哥本哈根卒
中研究中,吸烟曾被认为与死亡率的降低有关 [29],
但通过多因素分析同时考虑年龄因素的影响后这种
相关性即明显减小了。相反,酒精的滥用普遍被认
为是抗凝治疗的禁忌,同时也是许多临床试验选择
受试者时的排除标准之一 ( 包括 SPORTIF 临床试
图 2 以 CHA2DS2-VASc 评分为标准的每患
者 - 年卒中或其他血栓栓塞性事件发生率。
接受抗凝治疗后实际血栓栓塞事件发生率
校正华法林治疗影响后血栓栓塞事件发生率

71
Lip et al Stroke Risk Schemes in AF
验 )。一项小型的横断面研究显示糖尿病、饮酒、吸
烟及左心室肥大在 60-69 岁的房颤男性人群中均为
卒中事件发生的危险因素 [30]。酗酒与多种医学并发
症相关,包括卒中。尽管小量适度的饮酒被认为可
以减少心血管事件的发生率,但研究人员未发现饮
酒对房颤患者卒中事件起预防作用的相关报导。
继房颤欧洲心脏调查 [11] 及另一个大型抗凝临床
试验队列研究之后,此次研究再次验证了 CHA2DS2-VASc 评分对卒中的预测价值。房颤欧洲心脏调查分
析选择未接受抗凝治疗的房颤患者为研究人群,在
随访过程中发现 CHA2DS2-VASc 评分所分类的低风
险组患者日后血栓栓塞事件发生率较其他风险分层
方案所定义的低风险组患者血栓栓塞事件发生率稍
有降低。但在本研究分析中,研究人员尚无法肯定
这种低风险分层对卒中风险预测的准确性,因为不
伴有任何危险因素的患者根据试验纳入标准在试验
开始前即被排除了,尽管根据 Framingham 危险评分
仍有 40% 的患者被分类于低风险组。此外,对比将
60% 的患者纳入中风险组的 CHADS2 评分风险分层
方案 [9] 及将 70% 的患者纳入中风险组的 Rietbrock等人改良版风险分层方案 [16],CHA2DS2-VASc 评分
风险分层方案仅将 15% 的患者纳入中风险组。
早先关于几种卒中风险分层方案的比较研究已
经发表 [10,11,13,14,17,18,21,31],但仅 Lip 等人 [11] 及 Poli 等人 [14] 新近的研究分析中才包括了 ACC/AHA/ESC 指
南 2006[6]、 NICE 2006[5] 及 ACCP 指南 2008[7]。目前
绝大多数验证试验是基于临床试验队列研究,而很
少有人将已经发表的卒中风险分层方案应用于一般
临床实践过程中接触到的未经选择的患者中 [11,21,31]。
在大多数被公众广泛接受的卒中风险分层方案中仅
个别方案来源于未接受华法林治疗的临床试验队列,
而这部分队列人群中危险因素往往定义得不充分或
是记录得不完全。同样的,临床试验是否具有普遍
性也存在疑问,因为在那些从最初的队列中经过筛
选的试验只有不足 10% 是完全随机的 [28],举例而
言,周围动脉性疾病 [26,27] 及心肌梗塞 [24,25] 作为导致
脑卒中及增加死亡率的危险因素早已被大众广泛接
受,但是除 NICE 指南 [5]、CHA2DS2-VASc 评分 [11]
及 van Walraven 等人 [32] 的改良风险分层方案外,绝
大多数的方案均不将其包含其中。而女性性别无论
在房颤还是非房颤患者中均增加了卒中发生的危险
性 [33,34],然而在卒中预防的临床试验中女性总不能
被充分代表,这引发了针对女性作为一危险因素是
否具有生物学合理性的争论 [5]。值得注意的是女性
性别在 Framingham 风险评分 [17] 及 SPAF 风险分层
方案 [35] 中被作为危险因素之一,但所有的指南均未
建议将其考虑进风险分层。
有两项研究比较了 ACCP6、ACCP7、SPAF、AFI、Framingham 风险评分、van Walraven 改良评
分及 CHADS2 评分风险分层方案在接受抗凝治疗的
房颤患者的应用,一个研究是基于在有限随访期内
接受抗凝治疗患者的临床研究 [14],而另一个研究是
基于 SPORTIF 临床试验 [13]。Gage 等人 [10] 的研究也
是基于接受了抗血小板治疗的患者,这也可能对血
栓栓塞事件的发生率产生一定影响。研究人员希望
利用更多的同时期卒中风险分层方案进行分析研究,
试图从高危组的患者中识别出可能发生卒中或血栓
栓塞事件的高危人群,无论其是否接受了抗凝治疗。
鉴于建立未接受抗凝治疗的房颤患者队列的可行性
不大可能增加,研究人员推测在未接受抗凝治疗患
者其血栓栓塞事件发生率与 CHA2DS2-VASc 评分的
关系,见图 2。值得注意的是,从一个验证性试验得出的 c- 统
计量不能同其他研究得到的 c- 统计量相比拟,他们
在研究人群及事件发生率均存在差异。虽然如此,
尽管过去的 15 年风险分层方案在不断的演变,已发
表的风险分层方案并未改进他们的预测能力 (c- 统计量仍 ≈0.6)。鉴于目前愈来愈多的好的抗凝药物
被研制出来,他们较维生素 K 拮抗剂有着更广的
治疗窗宽,这就需要研究者可以更为准确的识别出
处于卒中低风险组的房颤患者以使得更多的房颤人
群可以得到更为有效的治疗 [12]。根据目前的研究,
CHA2DS2-VASc 评分较其他的风险分层方案有着更
高的阴性预测值。
局限性
从临床试验人群中得出的卒中发生率及其危险
因素与那些从临床实践中得出的数据并不相同。因
SPORTIF 临床试验纳入标准的限制导致其低风险组
的患者并不具有普遍代表性,正如我们之前分析的,
这显然妨碍了关于风险分层方案对真正低卒中风险
患者的识别能力的最终判断 [11]。除此之外,这项分
析不能确定高血压、糖尿病及心衰能否作为血栓栓
塞事件的独立预测因素,因为临床试验正是在这些
危险因素的基础上选择合适的患者纳入研究。如之
前提及的,控制血压在一个良好的水平可以降低卒
中事件的发生率,这就可能在进行临床试验的时候,
一些可以控制的卒中危险因素,如高血压、糖尿病
72
Stroke December 2010
及心衰被发现并控制在一个良好的水平,因此影响
了这些危险因素对血栓栓塞性事件的影响,这或许
可以解释为何本研究显示上述危险因素与卒中事件
的发生缺乏相关性。也许最重要的一点在于,本研
究分析局限在接受抗凝治疗的患者中,因此很多危
险因素受抗凝治疗的影响有所改善,这造成我们分
析时判断上的困难。而一种卒中风险分层方案是否
较另一种优越,这需要通过一系列队列研究来证实,
不仅针对接受抗凝治疗的患者,也针对未接受抗凝
治疗的患者,要求纳入的研究对象具有不同程度的
危险因素,如涵盖低、中、高三个危险等级,从中
确定风险分层方案的预测能力,并发现最为适合的
风险分层方案。另外,接受希美加群及华法林抗凝
治疗的患者中因治疗方案分配的不同理应存在潜在
的异质性,然而预分组的荟萃分析却显示两个治疗
组血栓栓塞发生率并无具有统计学意义的差异存在
( 希美加群治疗组每年血栓栓塞发生率为 1.62%,而
华法林治疗组每年血栓栓塞事件的发生率为 1.65%,
P=0.094)[36],而对两个治疗组危险因素的分析结果
也提示令人惊异的一致性 ( 结果未在此罗列 )。在临床工作中识别出在接受抗凝治疗的同时仍
存在卒中高风险的患者影响着临床治疗策略的选择。
在临床试验以外,将患者的治疗时间维持在一个合
适的水平非常困难,但这对于接受抗凝治疗的卒中
高风险房颤患者降低血栓栓塞事件及严重出血事件
的发生率是尤为重要的。这些患者需要更为频繁的
监测 INR 值,进行药物剂量调整或自我管理奥美拉
唑 - 阿莫西林 - 克拉霉素等影响华法林药代动力学药
物的使用,以控制抗凝时间在治疗范围内 [37]。这部
分患者可能从依药理学给药中获益 [38]。此外,接受
抗凝治疗的卒中高风险房颤患者在准备进行择期外
科手术时需要暂停奥美拉唑 - 阿莫西林 - 克拉霉素治
疗,而需进行奥美拉唑 - 阿莫西林 - 克拉霉素治疗及
准备接受搭桥手术的患者需将华法林减量。
结论此项分析研究认为冠心病和吸烟也是房颤患者
发生血栓栓塞事件的潜在危险因素之一。而在目前所
有可行的风险分层方案之中,尽管利用 c- 统计量考
量其对卒中事件的预警能力时得到的是相近的结果,
但 CHA2DS2-VASc 评分正确识别可能发生血栓栓塞
事件的房颤患者并将其归类于高危组的比例最高。
参考文献
1. Lip GY, Lim HS. Atrial fibrillation and stroke prevention. Lancet Neurol. 2007;6:981–993.
2. Connolly SJ, Eikelboom J, O’Donnell M, Pogue J, Yusuf S. Challenges of establishing new antithrombotic therapies in atrial fibrillation. Circulation. 2007;116:449–455.
3. Lip GY. Anticoagulation therapy and the risk of stroke in patients with atrial fi-brillation at “moderate risk” [CHADS2 score1]: simplifying stroke risk assess-ment and thromboprophylaxis in real life clinical practice. Thromb Haemost. 2010;103:683– 685.
4. Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, Wallentin L, RE-LY Steering Committee and Investigators. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151.
5. National Collaborating Centre for Chronic Conditions. Atrial fibrillation: na-tional clinical guideline for management in primary and secondary care. Lon-don: Royal College of Physicians; 2006.
6. Fuster V, Ryde´n LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Hal-perin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tama-rgo JL, Wann S, Smith SC Jr., Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo JL, Zamorano JL, American College of Cardiology/American Heart Association Task Force on Practice Guidelines, European Society of Cardiology Committee for Practice Guidelines, European Heart Rhythm Association, Heart Rhythm Society. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114:e257– e354.
7. Singer DE, Albers GW, Dalen JE, Fang MC, Go AS, Halperin JL, Lip GY, Manning WJ, American College of Chest Physicians. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clini-cal Practice Guidelines (8th Edition). Chest. 2008;133:546S–592S.
8. Stroke Risk in Atrial Fibrillation Working Group. Independent predictors of stroke in patients with atrial fibrillation: a systematic review. Neurology. 2007;69:546–554.
9. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285:2864 –2870.
10. Gage BF, van Walraven C, Pearce L, Hart RG, Koudstaal PJ, Boode BS, Pe-tersen P. Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin. Circulation. 2004;110:2287–2292.
11. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrilla-tion. Chest. 2010;137:263–272.
12. Lip GY, Halperin J. Improving stroke risk stratification in atrial fibrillation. Am J Med. 2010;123:484–488.
13. Baruch L, Gage BF, Horrow J, Juul-Mo¨ller S, Labovitz A, Persson M, Zabal-goitia M. Can patients at elevated risk of stroke treated with anticoagulants be further risk stratified? Stroke. 2007;38:2459–2463.
14. Poli D, Antonucci E, Grifoni E, Abbate R, Gensini GF, Prisco D. Stroke risk in atrial fibrillation patients on warfarin. Predictive ability of risk strati-fication schemes for primary and secondary prevention. Thromb Haemost. 2009;101:367–372.
15. Olsson SB, Executive Steering Committee of the SPORTIF III Investigators. Stroke prevention with the oral direct thrombin inhibitor ximelagatran com-pared with warfarin in patients with non-valvular atrial fibrillation (SPORTIF III): randomised controlled trial. Lancet. 2003;362:1691–1698.
16. Albers GW, Diener HC, Frison L, Grind M, Nevinson M, Partridge S, Halperin

73
Lip et al Stroke Risk Schemes in AF
JL, Horrow J, Olsson SB, Petersen P, Vahanian A, SPORTIF Executive Steer-ing Committee for the SPORTIF V Investigators. Ximelagatran vs warfarin for stroke prevention in patients with nonvalvular atrial fibrillation: a randomized trial. JAMA. 2005;293:690–698.
17. Wang TJ, Massaro JM, Levy D, Vasan RS, Wolf PA, D’Agostino RB, Larson MG, Kannel WB, Benjamin EJ. A risk score for predicting stroke or death in individuals with new-onset atrial fibrillation in the community: the Framingham Heart Study. JAMA. 2003;290:1049–1056.
18. Rietbrock S, Heeley E, Plumb J, van Staa T. Chronic atrial fibrillation: inci-dence, prevalence, and prediction of stroke using the congestive heart failure, hypertension, age/75, diabetes mellitus, and prior stroke or transient ischaemic attack (CHADS2) risk stratification scheme. Am Heart J. 2008;156:57– 64.
19. Albers GW, Dalen JE, Laupacis A, Manning WJ, Petersen P, Singer DE. Anti-thrombotic therapy in atrial fibrillation. The Sixth ACCP Conference on Anti-thrombotic and Thrombolytic Therapy. Chest. 2001;119:194S–206S.
20. Fuster V, Ryde´n LE, Asinger RW, Cannom DS, Crijns HJ, Frye RL, Halperin JL, Kay GN, Klein WW, Levy S, McNamara RL, Prystowsky EN, Wann LS, Wyse DG, Gibbons RJ, Antman EM, Alpert JS, Faxon DP, Fuster V, Gregoratos G, Hiratzka LF, Jacobs AK, Russell RO, Smith SC, Klein WW, Alonso-Garcia A, Blomstrom-Lundqvist C, De Backer G, Flather M, Hradec J, Oto A, Park-homenko A, Silber S, Torbicki A, American College of Cardiology/American Heart Association/European Society of Cardiology Board. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the management of patients with atrial fibrillation). J Am Coll Cardiol. 2001;38:1231–1266.
21. Fang MC, Go AS, Chang Y, Borowsky L, Pomernacki NK, Singer DE, ATRIA Study Group. Comparison of risk stratification schemes to predict throm-boembolism in people with nonvalvular atrial fibrillation. J Am Coll Cardiol. 2008;51:810–815.
22. Hughes M, Lip GY, Guideline Development Group, National Clinical Guideline for Management of Atrial Fibrillation in Primary and Secondary Care, National Institute for Health and Clinical Excellence. Stroke and thromboembolism in atrial fibrillation: a systematic review of stroke risk factors, risk stratification schema and cost effectiveness data. Thromb Haemost. 2008;99:295–304.
23. Lip GY, Frison L, Grind M, SPORTIF Investigators. Effect of hypertension on anticoagulated patients with atrial fibrillation. Eur Heart J. 2007;28:752–759.
24. Schmitt J, Duray G, Gersh BJ, Hohnloser SH. Atrial fibrillation in acute myo-cardial infarction: a systematic review of the incidence, clinical features and prognostic implications. Eur Heart J. 2009;30:1038–1045.
25. Siu CW, Jim MH, Ho HH, Miu R, Lee SW, Lau CP, Tse HF. Transient atrial
fibrillation complicating acute inferior myocardial infarction: implications for future risk of ischemic stroke. Chest. 2007;132:44–49.
26. Goto S, Bhatt DL, Ro¨ther J, Alberts M, Hill MD, Ikeda Y, Uchiyama S, D’Agostino R, Ohman EM, Liau CS, Hirsch AT, Mas JL, Wilson PW, Corbala´n R, Aichner F, Steg PG, REACH Registry Investigators. Prevalence, clinical profile, and cardiovascular outcomes of atrial fibrillation patients with athero-thrombosis. Am Heart J. 2008;156:855– 863.
27. Conway DS, Lip GY. Comparison of outcomes of patients with symptomatic peripheral artery disease with and without atrial fibrillation (the West Birming-ham Atrial Fibrillation Project). Am J Cardiol. 2004;93:1422–1425.
28. Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of anti-thrombotic therapy in atrial fibrillation. Analysis of pooled data from five ran-domized controlled trials. Arch Intern Med. 1994;154:1449–1457.
29. Kammersgaard LP, Olsen TS. Cardiovascular risk factors and 5-year mortality in the Copenhagen Stroke study. Cerebrovasc Dis. 2006;21:187–193.
30. Novello P, Ajmar G, Bianchini D, Bo GP, Cammarata S, Firpo MP, Parodi CI, Patrone A, Pizio N, Poeta MG, Simonetti S, Venturi S, Sacco G. Ischemic stroke and atrial fibrillation. A clinical study. Ital J Neurol Sci. 1993;14:571–576.
31. Stroke Risk in Atrial Fibrillation Working Group. Comparison of 12 risk strati-fication schemes to predict stroke in patients with nonvalvular atrial fibrillation. Stroke. 2008;39:1901–1910.
32. van Walraven C, Hart RG, Wells GA, Petersen P, Koudstaal PJ, Gullov AL, Hellemons BS, Koefed BG, Laupacis A. A clinical prediction rule to identify patients with atrial fibrillation and a low risk for stroke while taking aspirin. Arch Intern Med. 2003;163:936–943.
33. Lane DA, Lip GY. Female gender is a risk factor for stroke and thromboembo-lism in atrial fibrillation patients. Thromb Haemost. 2009;101:802–805.
34. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to pre-vent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857– 867.
35. Hart RG, Pearce LA, McBride R, Rothbart RM, Asinger RW. Factors associ-ated with ischaemic stroke during aspirin therapy in atrial fibrillation: analysis of 2012 participants in the SPAF I-III clinical trials. The Stroke Prevention in Atrial Fibrillation (SPAF) Investigators. Stroke. 1999;30: 1223–1229.
36. Albers GW, SPORTIF Investigators. Stroke prevention in atrial fibrillation: pooled analysis of SPORTIF III and V trials. Am J Manag Care 2004;10(Suppl 14):S462–S469; discussion S469–S473.
37. Heneghan C, Alonso-Coello P, Garcia-Alamino JM, Perera R, Meats E, Glasz-iou P. Self-monitoring of oral anticoagulation: a systematic review and meta-analysis. Lancet. 2006;367:404–411.
38. Tan GM, Wu E, Lam YY, Yan BP. Role of warfarin pharmacogenetic testing in clinical practice. Pharmacogenomics. 2010;11:439–448.