steve - rph on the go to read, speak, and write in english. ... rph on the go is an equal...
TRANSCRIPT

RPhon the go RPh On The Go USA, Inc. 5510 Howard St. Telephone: 847.588.7170 1.800.553.7359 Careers in Pharmacy Skokie, IL 60077 Facsimile: 847.588.7060 www.rphonthego.com Hello! Thank you for your interest in RPh on the Go. We are excited to share the opportunity for a rewarding career with you. We have a few requirements and forms for you to complete and return to us in the enclosed envelope:
Application Packet — includes a general job description, required HIPAA training, application for employment, skills checklist, a variety of authorization forms. Please complete the application, skills checklist and sign the authorization forms and return them to us in the enclosed envelope or via email or fax.
W-4 — Please complete the bottom portion and return it with your application. Direct Deposit Application — If you would like your paychecks deposited
electronically, please complete the application for direct deposit. License and Resume — Please include a copy of any active licenses and a copy of
your resume. I-9 Form — Please review the instructions for the Employment Eligibility Verification (I-9)
form carefully. We must receive your Employment Eligibility Verification (I-9) soon after the first day you work for us. If you are not in the Skokie, Illinois area, please take this form and the required supporting documents to a notary public on your first day of work with us. The notary will review the documents, complete the Section 2 and Certification sections. Please FAX a copy to us immediately and send the original, with the notary seal, to us in the second envelope. If you are in the Skokie, Illinois area, please call us to arrange a time to come to our headquarters to complete this process.
Also, some of our clients may require additional materials from you, such as a recent TB test, MMR, proof of varicella immunization, proprietary training on their systems and processes, a physical exam or other requirements. We will contact you as these items are needed and in many cases, we will help make arrangements for completing the requirements. Thank you for your interest in working with RPh on the Go. When your application has been processed and approved, we will send information about benefits, an employee handbook and a nametag. In the meantime, please feel welcome to sign-in at www.rphonthego.com and update your availability calendar and register your email address to receive our newsletters. Thank you for joining our diverse and dynamic healthcare team. Please call me at 800-553-7359 with any questions. My best, Steve Steve Sidell Director, Quality Assurance & Compliance enc.

Job Title: Traveling Pharmacist Reports To: Career Advisor Updated Date: July 2008
Position Summary: This is a per diem position for a registered pharmacist to provide professional services to a variety of clients on behalf of RPh on the Go. Duties and Responsibilities: • Maintains active state license. • Provides required health records, as determined by assignment. • Submits to requested drug screening(s). • Provides professional pharmacist cognitive services, which can include:
− Filling prescriptions − Counseling patients − Checking for drug interactions − Other duties as defined on an assignment basis
• Completes pre-assignment training requirements. • Each assignment that you accept will be performed by you to its completion. • Provide service to those assignments that you feel comfortable with and capable of
performing at a maximum professional level. • Comply with all applicable State laws and pharmacy regulations in the states where you are
working. • Submit a weekly timecard for each client, following the guidelines in the employee handbook. • Communicate with your Career Advisor and other RPh on the Go staff.
− Maintain accurate contact information with RPh on the Go. − Immediately inform your Career Advisor or someone else on the RPh on the Go staff of
any adverse event, injury, or a concern about your working condition or assignment. Please refer to the Employee Handbook for emergency contact information.
• For each assignment: − Punctuality: Allow enough time to arrive and orient yourself to the facility before the
scheduled start-time. − Timecard: Submit a weekly timecard for each client, following the guidelines in the
employee handbook. − Cooperation: Work in conjunction with the client staff at each assignment to provide the
highest quality healthcare. − Dress code: Present yourself in a professional manner, in accordance with client
requirements. − Customer service: Provide the highest level of customer service possible.
Required Qualifications: • Active, valid pharmacist license in a U.S. state or territory • Must be eligible to work in the United States Language Skills: Ability to read, speak, and write in English. Ability to read and interpret documents such as safety rules, pharmaceutical documents and procedure manuals. Ability to write routine reports and correspondence. Ability to effectively present information and respond to questions from patients, coworkers and other healthcare professionals.
Physical Demands: Physical demands vary on a per-assignment basis. Reasonable accommodations may be made to enable individuals with disabilities to perform the essential functions.

Employment Application RPh on the Go is an equal opportunity employer and does not discriminate on the basis of race, religion, color, national origin, age, sex, gender, disability or any other characteristic protected by law. PERSONAL INFORMATION (please print) First Name:___________________________ MI: ________ Last:__________________________ Suffix: _____
How should your first name appear on your nametag? _______________________________________________
Address: __________________________________________________________________________________
City: ________________________________________ State: _______ Zip Code: ________________________
Social Security #: _________________________Driver’s License #: _____________________ State: ________
List any other names (including maiden names) or social security numbers you have used: __________________
__________________________________________________________________________________________
Home Phone: _________________________________ Work Phone: __________________________________
Cell Phone:___________________________________ Email:________________________________________
Emergency contact: _________________________________________________________________________
Relationship: ______________________________ Telephone: _______________________________________ EDUCATIONAL AND PROFESSIONAL INFORMATION Please include your resume, with your complete education and residency experience.
Pharmacy School Attended:____________________________________________________________________
Degree(s): BS Pharmacy PharmD Other: ________________________________________________ Please list all active and inactive pharmacist license(s). Please send a photocopy of all active licenses.
Disciplinary Action reprimand, probation, suspension, voluntary surrender, revocation State License Number Expiration
Date Past Disciplinary Action
Current Disciplinary Action
No Yes* No Yes*
No Yes* No Yes*
No Yes* No Yes*
No Yes* No Yes*
No Yes* No Yes*
No Yes* No Yes*
If you have other active or inactive licenses, please attach an additional sheet with details.
* Year of Disciplinary Action: ____________________ Explanation of past or current license disciplinary actions
(attach a separate page if necessary): _________________________________________________________________
__________________________________________________________________________________________ Have you ever been convicted of a felony? No Yes If yes, please explain (attach a separate page if necessary):
__________________________________________________________________________________________
__________________________________________________________________________________________ Do you have liability/malpractice insurance? No Yes If yes:
Provider:__________________________ Policy Number: __________________ Expiration Date ____________
PHYSICAL RECORD Do you need any special accommodations to perform the essential functions of your job? Yes No
If yes, please describe accommodations needed: ___________________________________________________
__________________________________________________________________________________________ WORK EXPERIENCE Please list your three most recent pharmacy-related positions. Please attach a copy of your current resume. CURRENT EMPLOYER: ______________________________________________________________________ Please list any requests for contacting your current employer: _________________________________________ __________________________________________________________________________________________ Type of Business: Retail Long-term Care Hospital Out-Patient Hospital In-Patient Home Infusion Managed Care Other Address: __________________________________________________________________________________ City: __________________________________ State: _______ Phone Number: _________________________ Position: ____________________________________________ Salary: ________________________________ Dates Employed: from ________ to ___________ Reason for Leaving: ___________________________________ 1) Supervisor or peer who can serve as a reference: _______________________________________________ Title: __________________________ Work Phone: ___________________Cell phone: ________________ Email: __________________________________Dates worked together:____________________________ 2) Supervisor or peer who can serve as a reference: _______________________________________________ Title: __________________________ Work Phone: ___________________Cell phone: ________________ Email: __________________________________Dates worked together:____________________________ EMPLOYER: _______________________________________________________________________________ Type of Business: Retail Long-term Care Hospital Out-Patient Hospital In-Patient Home Infusion Managed Care Other Address: __________________________________________________________________________________ City: __________________________________ State: _______ Phone Number: _________________________ Position: ____________________________________________ Salary: ________________________________ Dates Employed: from ________ to ___________ Reason for Leaving: ___________________________________ 1) Supervisor or peer who can serve as a reference: _______________________________________________ Title: __________________________ Work Phone: ___________________Cell phone: ________________ Email: __________________________________Dates worked together:____________________________ 2) Supervisor or peer who can serve as a reference: _______________________________________________ Title: __________________________ Work Phone: ___________________Cell phone: ________________ Email: __________________________________Dates worked together:____________________________ EMPLOYER: _______________________________________________________________________________ Type of Business: Retail Long-term Care Hospital Out-Patient Hospital In-Patient Home Infusion Managed Care Other Address: __________________________________________________________________________________ City: __________________________________ State: _______ Phone Number: _________________________ Position: ____________________________________________ Salary: ________________________________ Dates Employed: from ________ to ___________ Reason for Leaving: ___________________________________ 1) Supervisor or peer who can serve as a reference: _______________________________________________ Title: __________________________ Work Phone: ___________________Cell phone: ________________ Email: __________________________________Dates worked together:____________________________ 2) Supervisor or peer who can serve as a reference: _______________________________________________ Title: __________________________ Work Phone: ___________________Cell phone: ________________ Email: __________________________________Dates worked together:____________________________

SKILLS CHECKLIST
Instructions: Please complete the following skills checklist by placing an "X" in the column which most accurately indicates your level of experience with each listed item. The correlation between the numerical scale and level of experience is as follows: 1 - No Experience (Would require substantial training and instruction to perform independently) 2 - Minimal Experience (Would require supervision before performing independently) 3 - Moderate Experience (Would require a brief review before performing independently) 4 - Significant Experience (Can perform independently) PRACTICE SETTINGS 1 2 3 4 SKILLS 1 2 3 4 Community/Retail Adverse Event Reporting Hospital Inpatient Anesthesia Drug Management Hospital Outpatient Anticoagulation Monitoring Hospital Clinical Services Chemotherapy Preparation Home Infusion/Home Care Computerized Order Entry Long Term Care Compounding Managed Care Disease State Management Nuclear Drug Utilization Review Other (list): Epidural/PCA Pump Mgmt. Hepatic Dose Adjustment AUTOMATION Immunizations Abbott Investigational Products Baxter Kinetic Dosing Connexus Lab Value Interpretation Meditech Nuclear Product Preparation McKesson Home Ordering/Inventory Control PDX Parenteral Product Preparation Pyxis Rx Patient Education QS-1 Personnel Management Other (list): Renal Dose Adjustment Other (list): SPECIALTIES Cardiology Chemotherapy SCRIPT VOLUME (with technician support) Critical Care 50-100/day Diabetes 101-200/day Dialysis 201+/day Emergency Medicine Endocrinology PATIENT POPULATIONS HIV/AIDS Neonates Home Care Pediatrics Hospice Adolescents Infectious Disease Adults Kinetics Geriatrics Nuclear Nutrition POSITIONS HELD Oncology Staff RPh Pain Management Pharmacist in Charge Pharmacoeconomics Director/Chief of Pharmacy Pharmacy Management Clinical Pharmacist Psychiatrics Other (list): Other (list):

Terms and Agreements By signing below, I agree to the following list of terms and agreements: • I certify that the facts contained in this application are true and complete to the best of my
knowledge and understand that, if hired, falsified statements on this application can be grounds for dismissal.
• HIPAA: I have reviewed the training material regarding the implementation and legal consequences of HIPAA, Title II. I understand that I am responsible for reviewing each client’s procedures on protecting the patient’s private health information.
• PURPOSE: RPh on the Go was formed to provide licensed Registered Pharmacists in good standing with a source of temporary employment. By signing this Agreement, you represent that you are such a pharmacist and you agree to furnish pharmacy services performed by you to our Clients as an employee of our company. We will offer these assignments to you so that we mutually can fulfill our contractual obligations to these Clients.
• COMPLIANCE: Each assignment that you accept will be performed by you to its completion. You only need to service those assignments that you feel comfortable with and capable of performing at a maximum professional level. In providing these services, you agree to comply with all applicable State laws and pharmacy regulations in the states where you are working.
• WAGE AND TIMECARDS: We will pay you a base rate, negotiated at the time of agreement for each assignment. Additional compensation you might receive is reimbursement for distances traveled from your home, room and board (if overnight accommodations are necessary and approved), required “on call” time, appropriate pre-approved overtime work, and special rates for certain specific jobs. These “extras” will be agreed upon by us before any services are rendered by you. We will be fully responsible for these compensations once confirmed. When you provide pharmacy services to our Clients, you will provide us with signed time cards for the work once completed. You shall make no schedules or schedule changes without written confirmation by RPh on the Go.
• INSURANCE: If you drive a car to work, your responsibilities include maintaining current and adequate auto insurance. We recommend that you maintain professional liability insurance. Include proof of liability coverage with this application.
• DISCIPLINARY ACTIONS: If any disciplinary action has occurred that affects your ability to perform as a pharmacist in good standing, or you have been convicted of a felony, we must be immediately informed by telephone and in writing. These changes may affect any future assignments we can offer you.
• NON-COMPETE: During the term of an assignment and for twelve months following termination of an assignment, you agree that you will provide pharmacy services to our Clients only through our service. You agree that you will not provide pharmacy services to such Clients directly or indirectly (as an employee, independent contractor, etc) for that twelve-month period. Our contract with the Client prohibits the Client from hiring you without paying a permanent placement fee to our company. Therefore, if prior to the expiration of these twelve months a Client wants to hire you (as an employee or independent contractor, etc), you agree to immediately notify us. In our sole judgment, we may waive the twelve-month non-compete clauses provided we enter into a satisfactory compensation agreement with the Client or you.
• TERMS: This Agreement shall continue until (a) in our judgment, it is violated; or (b) thirty days written notice is given by either party to terminate this Agreement. In either event, you agree that the twelve month non-compete clause set forth above shall survive the termination of this Agreement. This Agreement describes the entire obligation of each party to the other and can only be changed in writing by both parties.
Pharmacist/Employee Signature: ______________________________________________________________
Print Name: ______________________________________________________Date: _____________________
RPh on the Go USA, Inc. Signature: _____________________________________________________________
Print Name: ______________________________________________________Date: _____________________

RPh on the Go Mandatory Training: HEALTH INSURANCE PORTABILITY & ACCOUNTABILITY ACT OF 1996 Please read the following information about the Health Insurance Portability and Accountability Act of 1996. By signing the following page, you acknowledge that you are responsible for upholding the HIPAA guidelines and reviewing each client’s procedures on protecting the patient’s private health information.
What is the purpose of HIPAA? • To provide health insurance portability from one employer to another • To improve healthcare efficiency by standardizing the exchange of medical information • To protect the patient’s privacy against the misuse or improper disclosure of health records
Who is affected by HIPAA? All employee pharmacists, relief pharmacists, owner pharmacists, consultant pharmacists, health care system pharmacists, interns, health care providers, health plan administrators, pharmacy technicians & support staff, who may have access to a patient’s health information.
What is the definition of Personal Health Information (PHI)? Any “individually identifiable” health information transmitted through conversation, computer, or paper. This includes conversations with a patient, physician, nurse, clinic, health insurance representative, or pharmacy technician. Identifiable information includes a patient’s name, address, social security number, e-mail address, photograph, date of birth, gender, fax or phone number, driver’s license, or relative’s name. HIPAA does allow the use or disclosure of PHI to provide treatment, to collect payment, and to conduct health care operations. Treatment is defined as dispensing, DUR counseling, disease management, & refill reminders. Collecting payment is defined as verifying insurance coverage, reconciliation of claims, and third party billing. Operations are defined as malpractice insurance and hardware/software/database management. In addition, you may disclose PHI when required by law enforcement investigations, court orders, subpoenas, government benefit programs, State Boards of Pharmacy, the FDA for adverse events or product defects/recalls, or the Department of Health or CDC for disease or injury reporting.
How does HIPAA affect pharmacy operations? When you counsel a patient (either in person or on the phone) regarding their medication, you should keep your voice low and attempt to do so in a discreet area, so others cannot eavesdrop. PHI should not be within open view of other patients, guests, customers, pharmaceutical sales reps, or delivery personnel. At the start of any assignment, it is imperative that you review each client’s operations policies regarding documents and prescription vials containing PHI. Most pharmacies staple the prescription receipt on the outside of the bag for identification purposes. To protect the patient’s privacy, the pharmacy may use a smaller type font, so this information is not so visible. At the register checkout, the pharmacy may place the receipt inside the bag or fold the receipt inside out and staple it to the outside of the bag. To discard paper documents containing PHI, either tear or shred the document. Either return the old vial to the customer or destroy the label before tossing any vial.
What is the Notice of Privacy Practices (NOPP)? Effective with any prescriptions filled after 4-13-03, HIPAA requires that you post a copy of the Notice of Privacy Practices in the pharmacy and provide a copy to each patient. This notice describes the patient’s privacy rights and explains how the pharmacy intends to use and disclose PHI. You must attempt to obtain the patient’s written acknowledgement that he/she has received the pharmacy’s privacy policy. If the patient refuses to sign, you are required to document your efforts to obtain a signature and the reason why the patient did not comply. A parent or guardian may sign for a child’s prescription. If requested by the patient, you are required to provide a written accounting of disclosures of PHI and the pharmacy’s prescription records for up to 6 years prior to the date of request (but not prior to HIPAA’s effective date of 4-13-03). Patients may request additional restrictions on the use or disclosure of their PHI and the type of communications they prefer. Please familiarize yourself with and follow the client’s procedures.
Complaint Procedures If a patient feels the pharmacy has breached their privacy by inappropriately sharing their PHI, communicate that the pharmacy makes every attempt to respect their right to privacy. If the patient decides to pursue this further, provide the contact information as described in Notice of Privacy Practices. In addition, a formal complaint may be filed with the Secretary of Health & Human Services (listed on the NOPP).
How does HIPAA affect state laws? HIPAA is a federal law that supercedes less stringent state laws, but not more stringent state laws. What are the legal consequences of non-compliance with HIPAA?
• Civil penalties up to $25,000 per rule violation. • Criminal penalties up to $50,000 and one year in prison for knowingly and improperly obtaining or disclosing private
health information. • Up to $250,000 fine and 10 years in prison for the sale, use, or transfer of private health information for personal gain
or malicious harm. • Sanctions apply to individual employees, not just the pharmacies.
Please keep this for your records.

Form W-4 (2010)Purpose. Complete Form W-4 so that youremployer can withhold the correct federal incometax from your pay. Consider completing a newForm W-4 each year and when your personal orfinancial situation changes.
Head of household. Generally, you may claimhead of household filing status on your taxreturn only if you are unmarried and pay morethan 50% of the costs of keeping up a homefor yourself and your dependent(s) or otherqualifying individuals. See Pub. 501,Exemptions, Standard Deduction, and FilingInformation, for information.
Exemption from withholding. If you areexempt, complete only lines 1, 2, 3, 4, and 7and sign the form to validate it. Your exemptionfor 2010 expires February 16, 2011. SeePub. 505, Tax Withholding and Estimated Tax.
Check your withholding. After your Form W-4takes effect, use Pub. 919 to see how theamount you are having withheld compares toyour projected total tax for 2010. See Pub.919, especially if your earnings exceed$130,000 (Single) or $180,000 (Married).
Basic instructions. If you are not exempt,complete the Personal Allowances Worksheetbelow. The worksheets on page 2 further adjustyour withholding allowances based on itemizeddeductions, certain credits, adjustments toincome, or two-earners/multiple jobs situations.
Two earners or multiple jobs. If you have aworking spouse or more than one job, figurethe total number of allowances you are entitledto claim on all jobs using worksheets from onlyone Form W-4. Your withholding usually willbe most accurate when all allowances areclaimed on the Form W-4 for the highestpaying job and zero allowances are claimed onthe others. See Pub. 919 for details.
Personal Allowances Worksheet (Keep for your records.)
Enter “1” for yourself if no one else can claim you as a dependentA A
● You are single and have only one job; orEnter “1” if:B ● You are married, have only one job, and your spouse does not work; or B
● Your wages from a second job or your spouse’s wages (or the total of both) are $1,500 or less.� �
Enter “1” for your spouse. But, you may choose to enter “-0-” if you are married and have either a working spouse ormore than one job. (Entering “-0-” may help you avoid having too little tax withheld.)
CC
Enter number of dependents (other than your spouse or yourself) you will claim on your tax returnD D
E E
F F
Add lines A through G and enter total here. (Note. This may be different from the number of exemptions you claim on your tax return.) �H H● If you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions
and Adjustments Worksheet on page 2.For accuracy,complete allworksheetsthat apply.
● If you have more than one job or are married and you and your spouse both work and the combined earnings from all jobs exceed$18,000 ($32,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 to avoid having too little tax withheld.
● If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below.�
Cut here and give Form W-4 to your employer. Keep the top part for your records.
OMB No. 1545-0074Employee’s Withholding Allowance CertificateW-4Form
Department of the TreasuryInternal Revenue Service
� Whether you are entitled to claim a certain number of allowances or exemption from withholding issubject to review by the IRS. Your employer may be required to send a copy of this form to the IRS.
Type or print your first name and middle initial.1 Last name 2 Your social security number
Home address (number and street or rural route) MarriedSingle3 Married, but withhold at higher Single rate.
City or town, state, and ZIP code
Note. If married, but legally separated, or spouse is a nonresident alien, check the “Single” box.
55 Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2)$66 Additional amount, if any, you want withheld from each paycheck
7 I claim exemption from withholding for 2010, and I certify that I meet both of the following conditions for exemption.● Last year I had a right to a refund of all federal income tax withheld because I had no tax liability and● This year I expect a refund of all federal income tax withheld because I expect to have no tax liability.
7If you meet both conditions, write “Exempt” here �
8
Under penalties of perjury, I declare that I have examined this certificate and to the best of my knowledge and belief, it is true, correct, and complete.
Employee’s signature(Form is not valid unless you sign it.) � Date �
9 Employer identification number (EIN)Employer’s name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.) Office code (optional) 10
Enter “1” if you have at least $1,800 of child or dependent care expenses for which you plan to claim a credit
4 If your last name differs from that shown on your social security card,check here. You must call 1-800-772-1213 for a replacement card. �
Cat. No. 10220Q
Enter “1” if you will file as head of household on your tax return (see conditions under Head of household above)
Note. You cannot claim exemption fromwithholding if (a) your income exceeds $950and includes more than $300 of unearnedincome (for example, interest and dividends)and (b) another person can claim you as adependent on his or her tax return.
Nonwage income. If you have a large amountof nonwage income, such as interest ordividends, consider making estimated tax
G Child Tax Credit (including additional child tax credit). See Pub. 972, Child Tax Credit, for more information.
G● If your total income will be between $61,000 and $84,000 ($90,000 and $119,000 if married), enter “1” for each eligible
child plus “1” additional if you have six or more eligible children.
● If your total income will be less than $61,000 ($90,000 if married), enter “2” for each eligible child; then less “1” if you have three or more eligible children.
(Note. Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.)
Tax credits. You can take projected taxcredits into account in figuring your allowablenumber of withholding allowances. Credits forchild or dependent care expenses and thechild tax credit may be claimed using thePersonal Allowances Worksheet below. SeePub. 919, How Do I Adjust My TaxWithholding, for information on convertingyour other credits into withholding allowances.
Nonresident alien. If you are a nonresidentalien, see Notice 1392, Supplemental FormW-4 Instructions for Nonresident Aliens, beforecompleting this form.
For Privacy Act and Paperwork Reduction Act Notice, see page 2. Form W-4 (2010)
Complete all worksheets that apply. However, youmay claim fewer (or zero) allowances. For regularwages, withholding must be based on allowancesyou claimed and may not be a flat amount orpercentage of wages.
payments using Form 1040-ES, Estimated Taxfor Individuals. Otherwise, you may oweadditional tax. If you have pension or annuityincome, see Pub. 919 to find out if you shouldadjust your withholding on Form W-4 or W-4P.
2010
Page 2Form W-4 (2010)
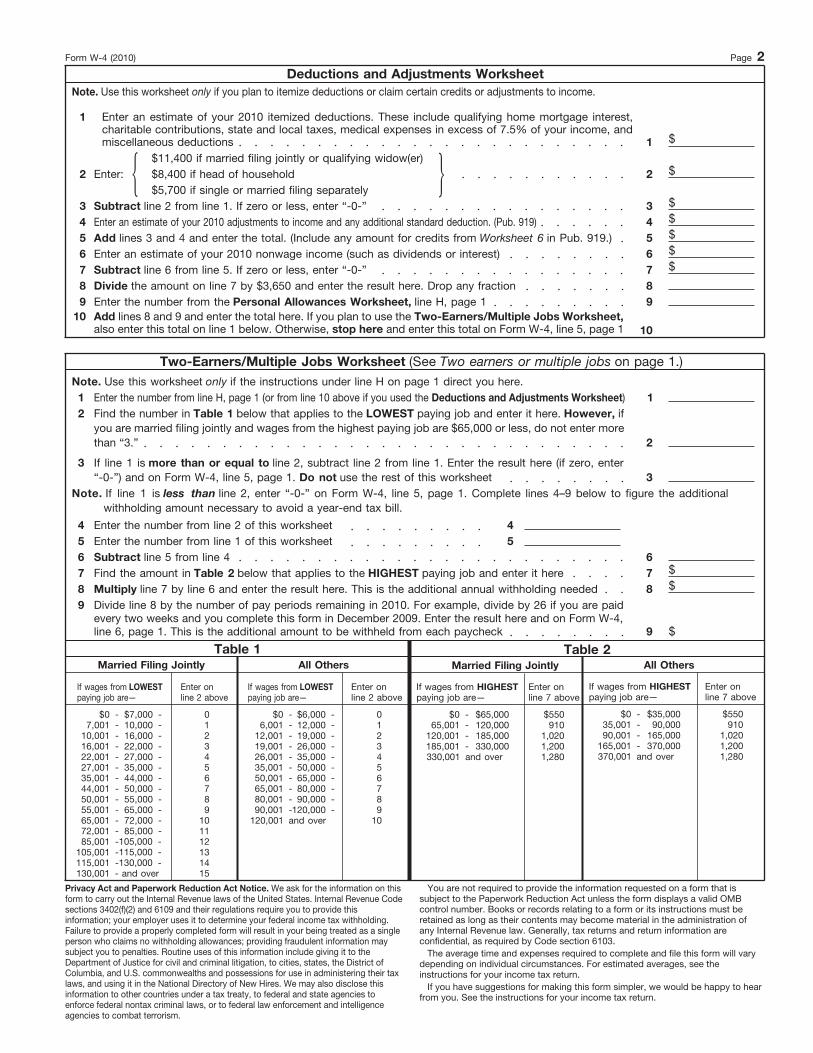
Deductions and Adjustments WorksheetNote. Use this worksheet only if you plan to itemize deductions or claim certain credits or adjustments to income.
Enter an estimate of your 2010 itemized deductions. These include qualifying home mortgage interest,charitable contributions, state and local taxes, medical expenses in excess of 7.5% of your income, andmiscellaneous deductions
1
$1$11,400 if married filing jointly or qualifying widow(er)
$$8,400 if head of household 2Enter:2$5,700 if single or married filing separately ��
$3 Subtract line 2 from line 1. If zero or less, enter “-0-” 3$Enter an estimate of your 2010 adjustments to income and any additional standard deduction. (Pub. 919)4$5Add lines 3 and 4 and enter the total. (Include any amount for credits from Worksheet 6 in Pub. 919.)5$6Enter an estimate of your 2010 nonwage income (such as dividends or interest)6$7Subtract line 6 from line 5. If zero or less, enter “-0-”7
Divide the amount on line 7 by $3,650 and enter the result here. Drop any fraction8 8Enter the number from the Personal Allowances Worksheet, line H, page 19 9Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet,also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1
1010
Two-Earners/Multiple Jobs Worksheet (See Two earners or multiple jobs on page 1.)
Note. Use this worksheet only if the instructions under line H on page 1 direct you here.1Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet)1
2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, ifyou are married filing jointly and wages from the highest paying job are $65,000 or less, do not enter morethan “3.” 2
3 If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter“-0-”) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet 3
Note. If line 1 is less than line 2, enter “-0-” on Form W-4, line 5, page 1. Complete lines 4–9 below to figure the additionalwithholding amount necessary to avoid a year-end tax bill.
Enter the number from line 2 of this worksheet4 4Enter the number from line 1 of this worksheet5 5Subtract line 5 from line 46 6
$Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here7 7$Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed8 8
Divide line 8 by the number of pay periods remaining in 2010. For example, divide by 26 if you are paidevery two weeks and you complete this form in December 2009. Enter the result here and on Form W-4,line 6, page 1. This is the additional amount to be withheld from each paycheck
9
$9
Privacy Act and Paperwork Reduction Act Notice. We ask for the information on thisform to carry out the Internal Revenue laws of the United States. Internal Revenue Codesections 3402(f)(2) and 6109 and their regulations require you to provide thisinformation; your employer uses it to determine your federal income tax withholding.Failure to provide a properly completed form will result in your being treated as a singleperson who claims no withholding allowances; providing fraudulent information maysubject you to penalties. Routine uses of this information include giving it to theDepartment of Justice for civil and criminal litigation, to cities, states, the District ofColumbia, and U.S. commonwealths and possessions for use in administering their taxlaws, and using it in the National Directory of New Hires. We may also disclose thisinformation to other countries under a tax treaty, to federal and state agencies toenforce federal nontax criminal laws, or to federal law enforcement and intelligenceagencies to combat terrorism.
The average time and expenses required to complete and file this form will varydepending on individual circumstances. For estimated averages, see theinstructions for your income tax return.
4
Table 1All OthersMarried Filing Jointly
If wages from LOWESTpaying job are—
Table 2All OthersMarried Filing Jointly
If wages from HIGHESTpaying job are—
Enter online 7 above
If wages from HIGHESTpaying job are—
Enter online 7 above
Enter online 2 above
If wages from LOWESTpaying job are—
You are not required to provide the information requested on a form that issubject to the Paperwork Reduction Act unless the form displays a valid OMBcontrol number. Books or records relating to a form or its instructions must beretained as long as their contents may become material in the administration ofany Internal Revenue law. Generally, tax returns and return information areconfidential, as required by Code section 6103.
Enter online 2 above
0123456789
10
If you have suggestions for making this form simpler, we would be happy to hearfrom you. See the instructions for your income tax return.
$0 -7,001 -
10,001 -16,001 -22,001 -27,001 -35,001 -44,001 -50,001 -55,001 -65,001 -72,001 -85,001 -
105,001 -115,001 -
$7,000 -10,000 -16,000 -22,000 -27,000 -35,000 -44,000 -50,000 -55,000 -65,000 -72,000 -85,000 -
130,001 - and over
0123456789
101112131415
$0 -6,001 -
12,001 -19,001 -26,001 -35,001 -50,001 -65,001 -80,001 -90,001 -
$6,000 -12,000 -19,000 -26,000 -35,000 -50,000 -65,000 -80,000 -90,000 -
120,000 -120,001 and over
$0 -65,001 -
120,001 -185,001 -
$550910
1,0201,2001,280330,001 and over
$65,000120,000185,000330,000
$0 -35,001 -90,001 -
165,001 -
$550910
1,0201,2001,280370,001 and over
$35,00090,000
165,000370,000
105,000 -115,000 -130,000 -


All MPS Companies/ Background Search Data Form Rev. 05/2009
BACKGROUND SEARCH DATA FORM The purpose of this form is to gather the information necessary to conduct your post-offer background search. All employment is contingent upon favorable background search results. All information will be kept confidential.
1. CANDIDATE INFORMATION Candidate Name: _____________________________________________________________________________ First Middle Last Current Street Address: _____________________________________________________________________________
City, State, Zip code: _____________________________________________________________________________
Social Security #: __________________________________ Driver’s License #: __________________________________ State Issued: _____________________ 2. THE FOLLOWING IS FOR IDENTIFICATION PURPOSES ONLY TO PERFORM THE BACKGROUND CHECK Race: (Circle one) Caucasian Black / African American Indian Hispanic Asian / Pacific Islander American Indian Gender: (Circle one) Male Female Date of Birth:____________________________ Additional Names Used in past 5 years: _____________________________________________________________________________________
3. LIST ALL CITIES, COUNTIES, STATES AND COUNTRIES WHERE YOU HAVE RESIDED DURING THE PAST 5 YEARS OR NUMBER OF YEARS AS DETERMINED BY CLIENT:
CITY/PROVINCE COUNTY STATE COUNTRY* APPROXIMATE DATES
• If you have lived outside the United States you will be contacted for additional information 4. Educational Data
School Print Name Of School City, State and Zip Years Attended (i.e. 2002-2004)
Did You Graduate?
Degree Type (i.e. BS,MBA)
College or University
Yes No
Other College/Graduate
Yes No
5. I certify that the above information is correct:
Signature: _____________________________________________
Print Name: _____________________________________________
Date: _____________________________________________
BRANCH INFORMATION – FOR INTERNAL USE ONLY Business Unit Name: ____________ Branch Number: ___________________ Title Applied for: ________________________________ Branch/Dept. Contact: _____________________________ Start Date: ____________________ Starting Salary: _____________________
All MPS Companies/FCRA Acknowledgement & Consent Rev. 5/09
ACKNOWLEDGEMENT AND CONSENT FOR RELEASE OF CONSUMER REPORTS
In connection with your application for employment to MPS Group, Inc. its affiliates and subsidiaries, (including contract for services), understand that consumer reports or investigative consumer reports which may contain public record information may be requested or made on you including consumer credit, criminal records, driving record, education, prior employer verification, workers compensation claims and others. These reports will include experience information along with reasons for termination of past employment. Further, understand that information from various Federal, State, local and other agencies which contain your past activities will be requested. A consumer report containing injury and illness records and medical information may be obtained only after a tentative offer of employment has been made. You have the right to make a request of First Advantage Corporation, 100 Carillon Parkway, St. Petersburg, FL 33716, (727) 214-3411, upon proper identification and the payment of any authorized fees, for the information in its files on you at the time of your request. You hereby authorize and request, without any reservation, any present or former employer, school, police department, financial institution, division of motor vehicles, consumer reporting agencies, or other persons or agencies having knowledge about you to furnish First Advantage Corporation with any and all background information in their possession regarding you, in order that your employment qualifications may be evaluated. By signing below, you hereby authorize without reservation, any party or agency contacted by this employer to furnish the above-mentioned information. You further authorize ongoing procurement of the above-mentioned reports at any time during your employment (or contract). You also agree that a fax or photocopy of this authorization with your signature be accepted with the same authority as the original. Finally, you understand that the reporting of negative or adverse information will not necessarily disqualify you from employment, assignment, placement or advancement. THIS ACKNOWLEDGES THAT I UNDERSTAND AND CONSENT TO THE REPORTING OF CONSUMER REPORT AND CONSUMER INVESTIGATIVE REPORT INFORMATION ON ME NOW AND IN THE FUTURE. __________________________________ __________________________________ ________________________ Signed Full Name Printed Full Name Date For all Consultants, Hourly Associates and Direct Hire Candidates I also consent to the sharing and transferring of information reported or learned regarding me among MPS Group, Inc. and its clients, affiliates and subsidiaries, now and at the time that I seek or maintain employment, assignment, or placement with or through any of them. __________________________________ ___________________________________ Signed Full Name Witness to Signature __________________________________ Printed Full Name __________________________________ ___________________________________ Date Date For California, Minnesota or Oklahoma applicants only, if you would like to receive a copy of the consumer report, if one is obtained, please check this box
NOTICE TO CALIFORNIA APPLICANTS Under section 1786.22 of the California Civil Code, you may view the file maintained on you by the consumer reporting agency named above during normal business hours. You may also obtain a copy of this file upon submitting proper identification and paying the costs of duplication services, by appearing at the Consumer Reporting Agency identified above in person or by mail. You may also receive a summary of the file by telephone. The agency is required to have personnel available to explain your file to you and the agency must explain to you any coded information appearing in your file. If you appear in person, a person of your choice may accompany you, provided that this person furnishes proper identification.

All MPS Companies/FCRA Notification & Disclosure Rev. 12/2008
NOTIFICATION AND DISCLOSURE The employees, associates and clients of MPS Group, Inc., and its affiliates and subsidiaries, are our most valued assets. In order to protect their interests and ensure the selection and advancement of qualified and capable people, we may obtain background information on you that includes consumer reports and/or investigative consumer reports for employment purposes now or at any time that you seek or maintain employment or placement with or through MPS Group, Inc., and its affiliates or subsidiaries. This may include personal references, employment and education verifications, personal credit histories and reports, criminal and civil records, and any other information bearing on your character and trustworthiness. The reporting or disclosure of negative or adverse information will not necessarily disqualify you from employment, assignment or advancement. THIS ACKNOWLEDGES THAT I RECEIVED AND READ THIS NOTICE AND DISCLOSURE.
______________________________ Employee Signature ______________________________ Print Name ______________________________ Date
Health Care Professional Instructions for Completing Form I-9 04/09
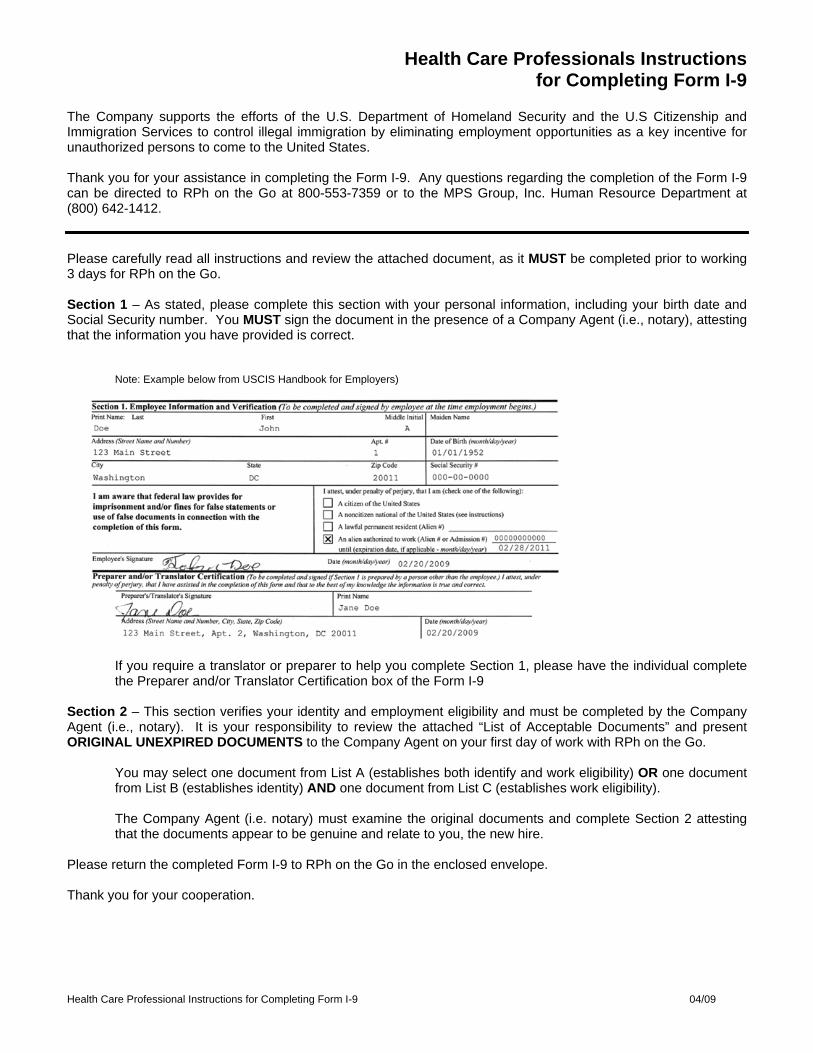
Health Care Professionals Instructions for Completing Form I-9
The Company supports the efforts of the U.S. Department of Homeland Security and the U.S Citizenship and Immigration Services to control illegal immigration by eliminating employment opportunities as a key incentive for unauthorized persons to come to the United States. Thank you for your assistance in completing the Form I-9. Any questions regarding the completion of the Form I-9 can be directed to RPh on the Go at 800-553-7359 or to the MPS Group, Inc. Human Resource Department at (800) 642-1412. Please carefully read all instructions and review the attached document, as it MUST be completed prior to working 3 days for RPh on the Go. Section 1 – As stated, please complete this section with your personal information, including your birth date and Social Security number. You MUST sign the document in the presence of a Company Agent (i.e., notary), attesting that the information you have provided is correct.
Note: Example below from USCIS Handbook for Employers)
If you require a translator or preparer to help you complete Section 1, please have the individual complete the Preparer and/or Translator Certification box of the Form I-9
Section 2 – This section verifies your identity and employment eligibility and must be completed by the Company Agent (i.e., notary). It is your responsibility to review the attached “List of Acceptable Documents” and present ORIGINAL UNEXPIRED DOCUMENTS to the Company Agent on your first day of work with RPh on the Go.
You may select one document from List A (establishes both identify and work eligibility) OR one document from List B (establishes identity) AND one document from List C (establishes work eligibility). The Company Agent (i.e. notary) must examine the original documents and complete Section 2 attesting that the documents appear to be genuine and relate to you, the new hire.
Please return the completed Form I-9 to RPh on the Go in the enclosed envelope. Thank you for your cooperation.






This EmployerParticipates in E-Verify
This employer will provide the Social Security Administration
(SSA) and, if necessary, the Department of Homeland Security
(DHS), with information from each new
employee’s Form I-9 to confirm work
authorization.
IMPORTANT: If the Government cannot
confirm that you are authorized to work,
this employer is required to provide you
written instructions and an opportunity
to contact SSA and/or DHS before taking
adverse action against you, including
terminating your employment.
Employers may not use E-Verify to pre-screen job applicants or
to re-verify current employees and may not limit or influence the
choice of documents presented for use on the Form I-9.
In order to determine whether Form I-9 documentation is valid,
this employer uses E-Verify’s photo screening tool to match
the photograph appearing on some
permanent resident and employment
authorization cards with the official U.S.
Citizenship and Immigration Services’
(USCIS) photograph.
If you believe that your employer has
violated its responsibilities under this
program or has discriminated against
you during the verification process
based upon your national origin or
citizenship status, please call the Office of Special Counsel at
1-800-255-7688 (TDD: 1-800-237-2515).
N O T I C E:
Federal law requires all employers
to verify the identity and employment eligibility
of all persons hired to work in the United States.
For more information on E-Verify, please contact DHS at:
1-888-464-4218

Para mayor información sobre E-Verify, favor ponerse en contacto con la oficina del DHS llamando al:
1-888-464-4218
Este empleador le proporcionará a la Administración del Seguro Social (SSA), y si es necesario, al Departamento de Seguridad Nacional (DHS), información obtenida del Formulario I-9 correspondiente a cada empleado recién contratado con el propósito de confirmar la autorización de trabajo.
IMPORTANTE: En dado caso que el gobierno no pueda confirmar si está usted autorizado para trabajar, este empleador está obligado a proporcionarle las instrucciones por escrito y darle la oportunidad a que se ponga en contacto con la oficina del SSA y, o el DHS antes de tomar una determinación adversa en contra suya, inclusive despedirlo.
Los empleadores no pueden utilizar E-Verify con el propósito de realizar una preselección de aspirantes a empleo o para hacer nuevas verificaciones de los empleados actuales, y no deben
restringir o influenciar la selección de los documentos que sean presentados para ser utilizados en el Formulario I-9.
A fin de poder determinar si la documentación del Formulario I-9 es valida o no, este empleador utiliza la herramienta de selección fotográfica de E-Verify para comparar la fotografía que aparece en algunas de las tarjetas de residente y autorizaciones de empleo, con las fotografías oficiales del Servicio de Inmigración y Ciudadanía de los Estados Unidos (USCIS).
Si usted cree que su empleador ha violado sus responsabilidades bajo este programa,
o ha discriminado en contra suya durante el proceso de verificación debido a su lugar de origen o condición de ciudadanía, favor ponerse en contacto con la Oficina de Asesoría Especial llamando al 1-800-255-7688 (TDD: 1-800-237-2515).
A V I S O:
La Ley Federal le exige a todos los empleadores
que verifiquen la identidad y elegibilidad de empleo
de toda persona contratada para trabajar en
los Estados Unidos.
Participa en E-VerifyEste Empleador
IF YOU HAVE THE RIGHT TO WORK, Don’t let anyone take it away.
If you have a legal right to work in the United States, there are laws to protect you against discrimination in the workplace.
You should know that –
No employer can deny you a job or fire you because of your national origin. Unless mandated by law or government contract, employers cannot require you to be a U.S. Citizen or permanent resident or refuse any legally acceptable documents.
If any of these things have happened to you, you may have a valid charge of discrimination that can be filed with the OSC. Contact the OSC for assistance in your own language.
Call 1-800-255-7688. TDD for the hearing impaired is 1-800-237-2515.
In the Washington, D.C., area, please call 202-616-5594, TDD 202-616-5525
Or write to: U.S. Department of Justice Office of Special Counsel - NYA 950 Pennsylvania Ave., N.W. Washington, DC 20530
U.S. Department of Justice Civil Rights Division
Office of Special Counsel for Immigration-Related Unfair Employment Practices

SI USTED TIENE DERECHO A TRABAJAR,no deje que nadie se lo quite.
Si tiene derecho a trabajarlegalmente en los EstadosUnidos, existen leyes paraprotegerlo contra la discrim-inación en el trabajo.
Debe saber que –
Ningún patrón puede negarletrabajo, ni puede despedirlo, debidoa su país de origen o su condiciónde inmigrante.
En la mayoría de los casos, lospatrones no pueden exigir que ustedsea ciudadano de los Estados Unidoso residente permanente o negarse aaceptar documentos válidos por ley.
Si se ha encontrado encualquiera de estas situa-ciones, usted podría tener unaqueja válida de discriminación.Comuníquese con OSC paraobtener ayuda en español.
Llame al 1-800-255-7688.La línea telefónica parapersonas con problemasde audición, es1-800-237-2515. EnWashington, D.C., llame al202-616-5594, o al202-616-5525 (personascon problemas de audición), oescríba a la Oficina delConsejero Especial, División deDerechos Civiles, P.O. Box 27728,Washington, DC 20038-7728.
Departamento de JusticiaDe los Estados Unidos,División de Derechos Civiles
Oficina del Consejero Especial

Mandatory Contact Notice
1) I understand and agree that, upon conclusion of each assignment, I must immediately contact my RPh on the
Go recruiter. I understand that such notification is for the purpose of determining eligibility and availability of additional work assignments as well as other administrative purposes. If the recruiter who initially placed me is not available, I can speak with another recruiter, leave a detailed voicemail message in my recruiter’s mailbox, or email the detailed message to my recruiter or to the email address below. I accept that:
a) My failure to contact RPh on the Go as indicated above within two business days* of completion of assignment may be considered a voluntary resignation and/or termination which may lead to the denial and/or interruption of unemployment benefits.
b) It is my responsibility to inquire about any available assignment with RPh on the Go upon conclusion of my assignment. If I fail to inquire about another assignment prior to filing for unemployment benefits, it may lead to an interruption and/or denial of unemployment benefits.
c) If a suitable assignment is available with RPh on the Go upon conclusion of my assignment and I refuse an offer of suitable work, it may lead to an interruption and/or denial of unemployment benefits.
2) I also understand and agree that I am required to contact my RPh on the Go recruiter at the telephone number
or email address listed below:
a) When my address, email or phone number changes; b) If I experience any type of harassment or unlawful discrimination; c) If I am not being provided a meal or rest break to which I am entitled; d) If I have a complaint or dispute about my wages earned; e) If I am exposed to blood and/or bodily fluid or injured while on assignment.
If you have any questions, please contact your RPh on the Go recruiter. RPh on the Go Contact Information:
General Email Address: [email protected]
Main Telephone: ? I certify that I have read, fully understand, and accept all terms of the foregoing agreement: Employee Name: ______________________________________________________________________________ Employee Signature: ___________________________________________________________________________ Date: _______________________________________________________________________________________ *Exceptions to the two business day notification period are listed below:
Iowa – Associates must contact RPh on the Go within three working days of completion of the temporary assignment. Michigan – Associates must contact RPh on the Go within seven working days of completion of the temporary assignment.