steps for qapi success - amazon s3 · 1 steps for qapi success jan allison, rn, chsp sr. director...
TRANSCRIPT

1
Steps for QAPI Success
Jan Allison, RN, CHSP
Sr. Director of Regulatory
Amsurg
DisclosureFacultyJan Allison, RN, CHSP
No conflict• It is the policy of the Ambulatory Surgery Center Association (ASCA) to ensure that all individuals who have the ability to
control or influence the content of an educational activity disclose all financial relationships with any entity whose products or services are pertinent to the content of the educational activity. The financial disclosure will include the name of the entity, and the nature of the relationship the individual has with the entity during the time the relationship is in effect and for 12 months afterward.
Requirements for successful completion of the educational activity • Attendee must be present for the duration of the educational program• Completed evaluation form
Expiration of enduring materials• Contact hours will be awarded until June 30, 2016 for the educational program
– ASCA is an approved provider for nursing contact hours by the California Board of Registered Nursing, Provider #6949
– ASCA is an approved provider for Administrator Education Units (AEUs) by BASC Provider #3272
Commercial Support: NoneSponsorship: None

2
Learning Objectives
• Discuss regulatory requirements
• Describe the elements of a QAPI Plan
• Identify quality indicators that support QAPI
Begin With a QAPI (Quality Assurance, Performance Improvement) Plan
Include:
Goals
• What the plan will strive to meet, i.e., improving patient outcomes.
Scope
• How QAPI is integrated into the care and services of the facility, i.e., ongoing, comprehensive, scope of participation in QAPI activities.

3
QAPI Plan
Include:
Governance/Leadership
• Responsibilities of Governing Body.
– Set expectations around safety and quality.
– Ensure staff accountability while creating an atmosphere where staff is comfortable identifying and reporting quality problems as well as opportunities for improvement.
QAPI Plan
• Responsibilities of Governing Body.
– Assure adequate resources exist to conduct QAPI efforts.
• Designating one person accountable for QAPI.
• Developing leadership and facility-wide training on QAPI.
• Ensuring staff time, equipment, and technical training as needed.
• Ensure that policies and procedures are developed to sustain QAPI despite turnover.

4
QAPI Plan
Include:
Data/Monitoring
• What indicators are monitored, how they are collected, and the frequency with which they’ll be measured.
PI projects/teams
• How projects are prioritized and selected, overall plan for conducting.
QAPI Plan
Include:
Analysis
• Process for analyzing data.
Communication
• Who is the audience for QAPI communication, how is it done.
Evaluation
• Frequency for review/revision of plan.

5
QAPI Plan: Annual Evaluation
CMS Self Assessment Tool
https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/QAPI/Downloads/QAPISelfAssessment.pdf
Annual Review
Next: Identify quality indicators to track
Quality indicators associated with improved health outcomes
Types of Indicators:
• Outcomes – results of care.
• Process of Care-how often standard of care was met.
• Patient Perception-patient’s experience.

6
Indicators
Incident Reports
• Patient Falls
• Medication errors
• Burns
• Wrong site
• Hospital Transfers
• Infections
Indicators
• Patient Satisfaction • Adverse Events

7
Indicators: Best Practice Processes
• Influenza vaccination coverage
• DVT risk assessment
• Sterilization and high level disinfection processes
• Maintaining normothermia
• Time-out performance
• Hand hygiene
• Safe medication practices
Indicators
• Audits – Medical records
• Program Evaluations – Infection control
– Environment
– Medication administration
• Grievances/Complaints
• Physician Comments
• Teammate Engagement Surveys

8
Indicators
• Strategic Plan
• Accreditation and Regulatory Surveys
• Peer Review
Using Peer Review in QAPI
Random Peer Review
• Medical Record Review: – Appropriateness of care
– ASA classification
– H&P within 30 days of procedure
– Informed consent
– Timeliness of record completion
Specialty Based Peer Review
• GI: – Post-polypectomy bleeding
– Perforation rate
– Moderate sedation adverse events

9
Department Specific Indicators
Preoperative
• Missed hand-off communication.
• Failure of a patient to stop taking medication.
• Adherence to pre-procedure fluid and food restrictions.
• Incomplete patient history information.
Intraoperative
• Procedure delays.
• Turnover times.
• Instrument or equipment problems.
• Improper aseptic technique.
• Performance of unplanned procedures.
• Procedures exceeding their scheduled time by more than one hour.
Department Specific Indicators
Postoperative
• Missed hand-off communication.
• Instances when significant changes in patient vital signs required intervention.
• Prolonged recovery time from anesthesia effects or complications.
• Discrepancies between narcotic amounts documented in the patient’s record versus the narcotic log.

10
Next: Track, Measure and Analyze the Data
Have a process for analyzing data including how findings will be reviewed against benchmarks and/or targets established by the facility.
Benchmark
• Comparing to your own previous performance:
– Example – Hand Hygiene

11
Benchmark
• Comparing to other similar organizations:– ASCs in geographical region (identify top performers).
• ASC Quality Collaboration Quality Report.
• Professional Societies – networking among members, current publications.
• State specific reporting.
• Collaborative Study – designed by 3rd party (e.g., ASCA).
• Vendors.
Next: Meeting of the Quality Committee
• Members
– Multi-disciplinary, includes physician, meets regularly.
– Written descriptions and competencies of each role.

12
Documents for the Quality Committee
• QAPI Plan with minimum reporting requirements.
• Quality Committee agenda/minutes.
• Reports compiled from audits, inspections, maintenance activities, etc.
Activities of the Quality Committee
• Each member provides a summarized report of:– Aggregated data collection
- (use graphs).
– Analysis of data (internal and external benchmarking).
• Example report for environmental safety:– Occurrence of preventative
maintenance, inspections, repairs and testing.
– Drills or occurrence of codes – description and critique.
– Education and training.
– Results from rounds/audits.
– Annual review of the environmental plans.

13
Conduct a QAPI project
• Use the data to identify an opportunity for improvement.
• Establish Goal: Where do you want to be?
• Prioritize the project and time frame to complete.
• Determine the root cause of the problem.
Sample Project Priority Tool

14
Useful QI Tools for Identifying Root Causes
• Cause and Effect Diagram (fishbone)
• Flow Chart
Conduct a QAPI Project
• QAPI Committee designates a PI Team.
• Implement improvement/prevention strategies.
• Schedule needed training.
• Collect data to ensure improvement occurred.

15
Conduct a QAPI Project• Did the action work?• Is the desired outcome
achieved? • Is the process working as
predicted or is further refinement needed?
• Change process if needed to achieve desired outcomes.
• Repeat steps as needed to maximize improvement.
• Finalize and implement full scale.
• Develop new Policy & Procedure for redesigned process.
• Educate.• Report/communicate
results to teammates and leadership (MEC/GB).
Conduct a QAPI Project
• Did you make an improvement/fix the problem?• Yes?! Done…but continue to monitor compliance
to ensure improvement is sustained.• No? Then repeat the process until you’re done. • Understand that some improvements require a
culture change which can take a significant amount of time and patience.
• Volume of PI projects annually should be reflected by the scope of identified issues in the facility.

16
Summarize Project in a Report
Writing a QAPI Report
• Explain why the project was undertaken.
• State the identified problem/issue.
• Describe the analysis of data to support it’s a problem/issue, including benchmarking results.
• Describe how this problem/issue impacts patient safety.
• Name the corrective actions that are put into place.
17
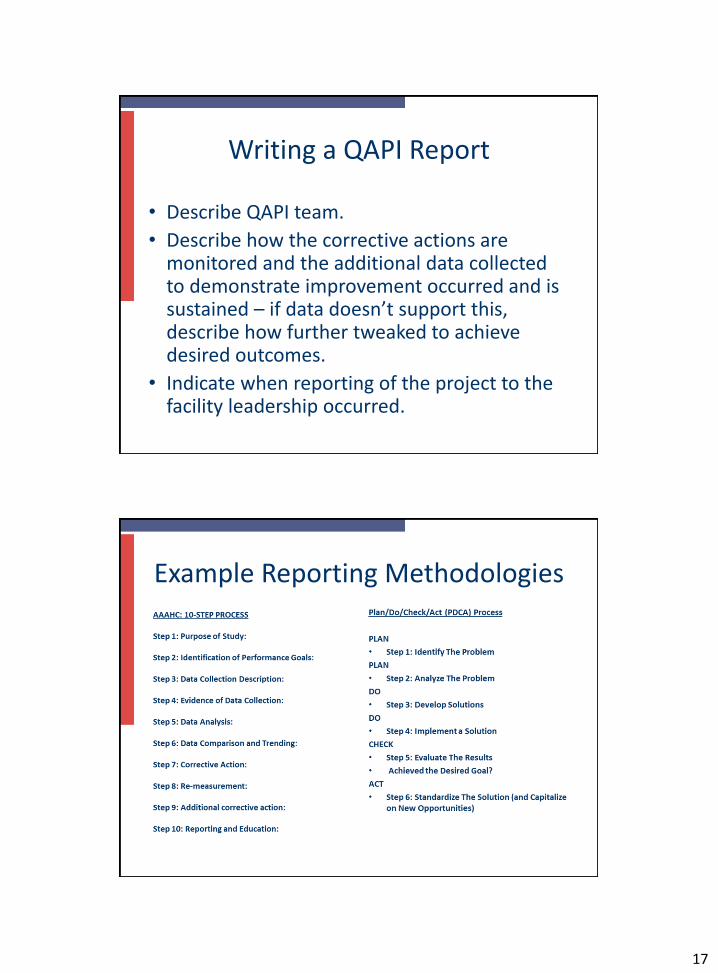
Writing a QAPI Report
• Describe QAPI team.
• Describe how the corrective actions are monitored and the additional data collected to demonstrate improvement occurred and is sustained – if data doesn’t support this, describe how further tweaked to achieve desired outcomes.
• Indicate when reporting of the project to the facility leadership occurred.
Example Reporting Methodologies
18
Questions?
References
Center for Medicare and Medicaid Services (CMS) Condition for Coverage Interpretive Guidelines: §416.43: Quality Assessment & Performance Improvement
The Joint Commission (TJC) standards for Ambulatory Surgery Centers: Performance Improvement Chapter
Accreditation Association for Ambulatory Healthcare, Inc. (AAAHC) Accreditation Handbook: Chapter 5, Quality Management and Improvement