state of the art symposium intestinal transplantation · ifald, intestinal failure associated liver...
TRANSCRIPT
Trapianto di intestino e insufficienza intestinale cronica benigna: un update
Loris Pironi
Centro Insufficienza Intestinale Cronica Benigna “M. Miglioli”
Dipartimento Malattie Digestive
Policlinico S. Orsola – Università di Bologna

PROFESSORE ASSOCIATO, SSD MED/09, presso il Dipartimento di Scienze Mediche e Chirurgiche dell'Universitа di Bologna,
&
RESPONSABILE DEL“CENTRO REGIONALE DI RIFERIMENTO PER INSUFFICIENZA INTESTINALE CRONICA BENIGNA”
⌘
Attività scientifica
INSUFFICIENZA INTESTINALE NUTRIZIONE CLINICA IN AMBITO OSPEDALIERO E DOMICILIARE TRAPIANTO INTESTINALE
Home Artificial Nutrition & Chronic Intestinal Failure Special Interest Group
1992, membro fondatore
2006 ad oggi, coordinatore


The CIF pathway
1st definition of IF, Fleming 1981
ESPEN HPN Guidelines, 2009
ESPEN definition and classification of IF, 2015
ESPEN CIF Guidelines, 2016
ESPEN AIF Pos P, 2016
IF inclusion in ICD-11, 2018
1st ITx, 1964
1st HPN, 1969
Tacrolimus for ITx, 1989
All-in-One PN bag, 1972
Portable HPN, ’90s
PACIFHAN (Int. Pts. All., 2015)
ESPEN indications for ITx, 2012
Medicare indications for ITx, 2001
Fish oil lipid E., 2000
CVC taurolidine lock, 2003
GLP-2, intestinal growth factor EMA, 2012
Specific QoL tool, 2010
Intestinal lengthening procedures Bianchi (1981), STEPS (2003), ...

The reduction of gut function below the minimum necessary for the absorption of macronutrients and/or water and electrolytes, such that intravenous supplementation (IVS) is required to maintain health and/or growth.
Warning: PN and IF are not synonymous
Definition
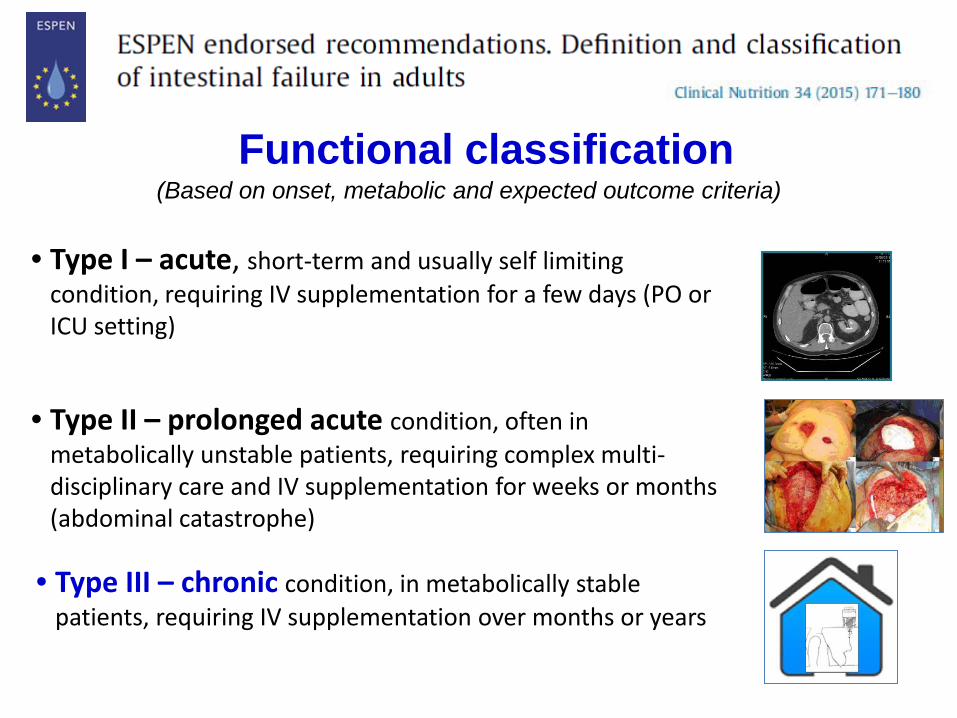
• Type III – chronic condition, in metabolically stable patients, requiring IV supplementation over months or years
Functional classification
• Type I – acute, short-term and usually self limiting condition, requiring IV supplementation for a few days (PO or ICU setting)
• Type II – prolonged acute condition, often in metabolically unstable patients, requiring complex multi-disciplinary care and IV supplementation for weeks or months (abdominal catastrophe)
(Based on onset, metabolic and expected outcome criteria)

Pironi L, BMC Nutrition 2017
12 casi/106 abitanti (adulti 9.5 – pediatrici 2.5)
Indagine SINPE
•Regioni: 18 (90%) • ASLs: 95 (65%) • Abitanti (Mln): 44 (73%)
• Territorio (Km2): 204 (68%)
Prevalenza della IICB in Italia nel 2012

Pironi L, Am J Gastroenterol 2006
Cross-sectional investigation on HPN for benign CIF in Europe
Pathophysiological Classification
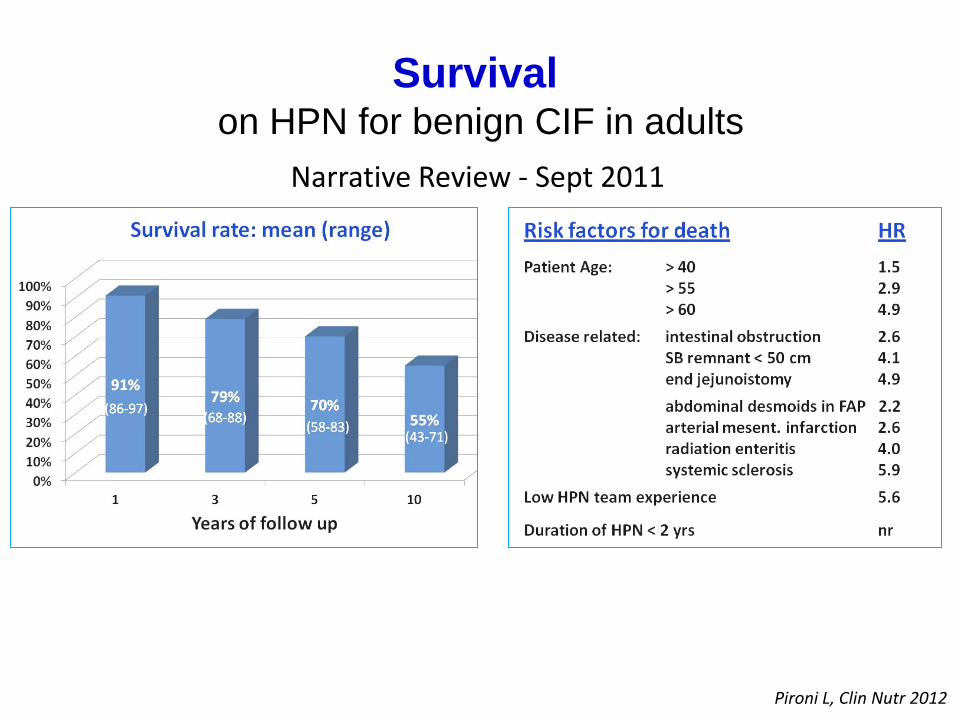
Pironi L, Clin Nutr 2012
Narrative Review - Sept 2011
Survival on HPN for benign CIF in adults

Causes of death on HPN for benign CIF in adults
IFALD, intestinal failure associated liver disease CVC, central venous catheter
Narrative Review - Sept 2011
Pironi L, Clin Nutr 2012

Mechanisms • Broad antimicrobial activity • Non toxic – rapidly metabolised • Reacts irreversibly with cell wall • Prevents bacterial adhesion bio-
surface • No resistance reported • Proved efficacy in hemodialysis
Number of CVC-infection free days
Taurolidine
Heparin
Bisseling TM, Clin Nutr 2010
Taurolidine Lock for the prevention of CVC-infection
Guidelines for CIF We suggest, for prevention of CVC-related infections: • ……… • CVC-locking with taurolidine may be used • ………

Proposed mechanisms
•Improved bile flow •Immunomodulatory (↓ inflamm.) •Decreased steatosis •↑ content of α-tochopherol •Replacement of soybean oil LE
Studies with liver histology in adults
Pironi L, eSPEN 2010; Jurewitsch B, JPEN 2011;Xu Z, Clin Nutr 2012
Fish oil lipid emulsion for IFALD prevention and treatment
Guidelines for CIF We suggest for treatment of intestinal failure-associated liver disease: • ……… • to revise the lipid component of the PN admixture, in order to decrease the
total amount and/or to decrease the ω6/ω3 PUFA ratio • ………

Joly F, Clin Nutr Suppl 2010; Pironi L, Clin Nutr 2012
Intestinal rehabilitation - weaning off HPN in benign CIF in adults
472 adults

Jeppesen PB, GUT 1999; Martin GR, World J Gastroenterol 2006; Wallis K, Curr Opin Clin Nutr Metab Care 2009
Glucagon-Like Peptide-2 analogue (teduglutide, FDA and EMA approved)
↑ mucosal growth in small and large bowel (↑ crypt cell proliferation + ↓ villous cell apoptosis)
↑ absorptive capacity
↑ mesenteric blood flow
↓ gastric emptying and acid secretion
↓ intestinal permeability
• anti-inflammatory action
Intestinal growth factors Intestinal rehabilitation in SBS

• Patients 88 (time from surgery: > 1 yr)
• Dosage 0.05 mg/Kg/day
• Treatment duration 24-36 (months)
• Discontinuation 23 (26%) Acute Events 16 Pt. decision 4 Investig. decision 2 Death 1 (CVC-sepsis)
Schwartz L, Clin Transl Gastroenterol. 2016
• Treatment Emergent AEs 85 (95%) Abdominal pain 34% CVC-sepsis 28% Decreased weight 25% Others 17%
• Possible long-term risk: GI cancer • Colonoscopy (50 pts) Polyps 9 (adenoma 5; hyperplastic 1, inflammatory 1, unclassified 2

• ITT clinical response (≥ 20% reduction of PN): 57 (65%)
Schwartz L, Clin Transl Gastroenterol. 2016
HPN weaned off
Guidelines for CIF We recommend …….. to objectively evaluate and balance the benefit and clinical meaningfulness of the interventions versus the inconveniences, adverse effects, potential risks, and cost-effectiveness.

Data from January 1985 to February 2013
Grant D. et al, AJT 2014
Contributing centers 82
Transplant activity • North America • Europe • Asia+Australia+South America
76% ~ 20% ~ 4%
Total transplants • Children (< 18 yr) • Adults
2887 (2699 pts) 1611 (55.8%) 1276 (44.2%)
Type of transplant • SBT • Liver-SB • MVT+Modified MVT
582 (36.2%) 734 (45.5%) 257+38 (18.3%)

Conditional 5-yr actuarial graft survival (defined as graft survival after 1-year)
Actuarial Graft Survival Over Time (All Recipients)
Grant D. et al, AJT 2014

Intestinal Transplants Performed Grant D. et al, AJT 2014
Possible causes of the decline of ITx rate
• Improved ability to prevent or resolve IFALD
• Improved medical therapy and non-transplant surgical rehabilitative procedures
• Narrow risk–benefit ratio for ITx, in an era of improving outcomes with long-term HPN
Grant D. et al, AJT 2014

Disease-related risk of death • Invasive intra-abdominal desmoids • Congenital mucosal diseases • Ultra short bowel
High morbidity IF / HPN refusal • Frequent hospitalization, poor pain
control, … • Pt. unwillingness to continue HPN
HPN-Failure
• Liver failure: impending or overt
• CVC-Thrombosis: occluding ≥ 2 central veins
• CVC-Sepsis: severe and ≥ 2 /yr
• Dehydration: frequent and severe
Indications for ITx – 2001 devised by U.S.A. Medicare-Medicaid & Am Soc of Transplantation
AGA,Gastroenterology 2003; Kaufman SS,Pediatr Transplant 2001
We recommend assessment for candidacy for intestinal transplantation, when one of the following indications exists:

Survival rate and Relative risk of death on HPN according to the indications for ITx
High morbidity 100%
Pironi L et al, ESPEN-HAN & CIF WG, Am J Gastroenterol, 2006 , Gastroenterology, 2008, GUT, 2011
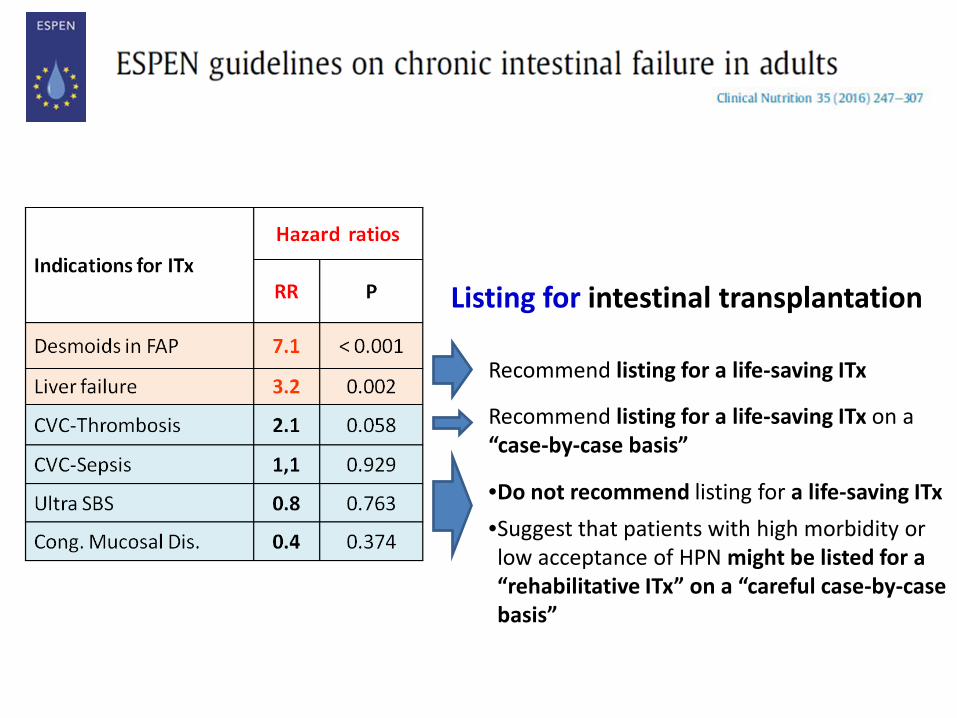
Listing for intestinal transplantation
Recommend listing for a life-saving ITx
Recommend listing for a life-saving ITx on a “case-by-case basis”
•Do not recommend listing for a life-saving ITx •Suggest that patients with high morbidity or low acceptance of HPN might be listed for a “rehabilitative ITx” on a “careful case-by-case basis”
Referral for potential “rehabilitative ITx” in case-by-case carefully selected and appropriately informed patients with irreversible intestinal failure
The clinical dilemma
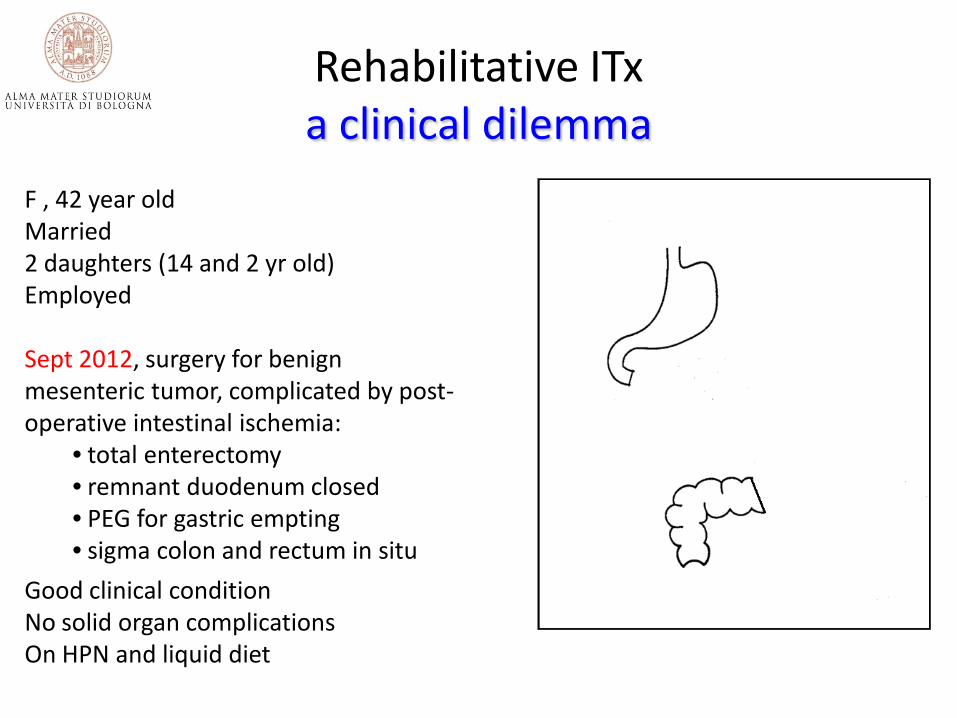
F , 42 year old Married 2 daughters (14 and 2 yr old) Employed Sept 2012, surgery for benign mesenteric tumor, complicated by post-operative intestinal ischemia:
• total enterectomy • remnant duodenum closed • PEG for gastric empting • sigma colon and rectum in situ
Good clinical condition No solid organ complications On HPN and liquid diet
Rehabilitative ITx a clinical dilemma

• Factors determining the choice •Survival •Safety •Efficacy •Timing for ITx
HPN or ITx a clinical dilemma

HPN or ITx Survival
ITx registry
ITx Pittsburgh
HPN unselected
HPN selected (no contraindications to ITx)
Pironi L, Clin Nutr 2012

HPN (A)
ITx (A+C)
Osteoporosis 41% 42%
Acute rejection 40%
De-novo cancer Rare 17%
Diabetes Rare 17%
Renal dialysis or Tx Rare 9%
PTLD 4%
↑ LFT/Liver disease 15-85% Rare
CVC-sepsis (per CVC-yr) 0.14-0.48
CVC-thrombosis (CVC-yr) 0.02-0.09
HPN (A)
ITx (A+C)
Total Liver failure CVC-sepsis CVC-thrombosis
14% (4) (8) (2)
Total Graft failure Complications of therapy
85% (37) (48)
HPN or ITx Safety
Treatment related death (% of total death)
Late morbidities (% of patients)
A, adults C, children
Abu-Elmagd K. Ann Surg 2012; Pironi L et al Clin Nutr 2012
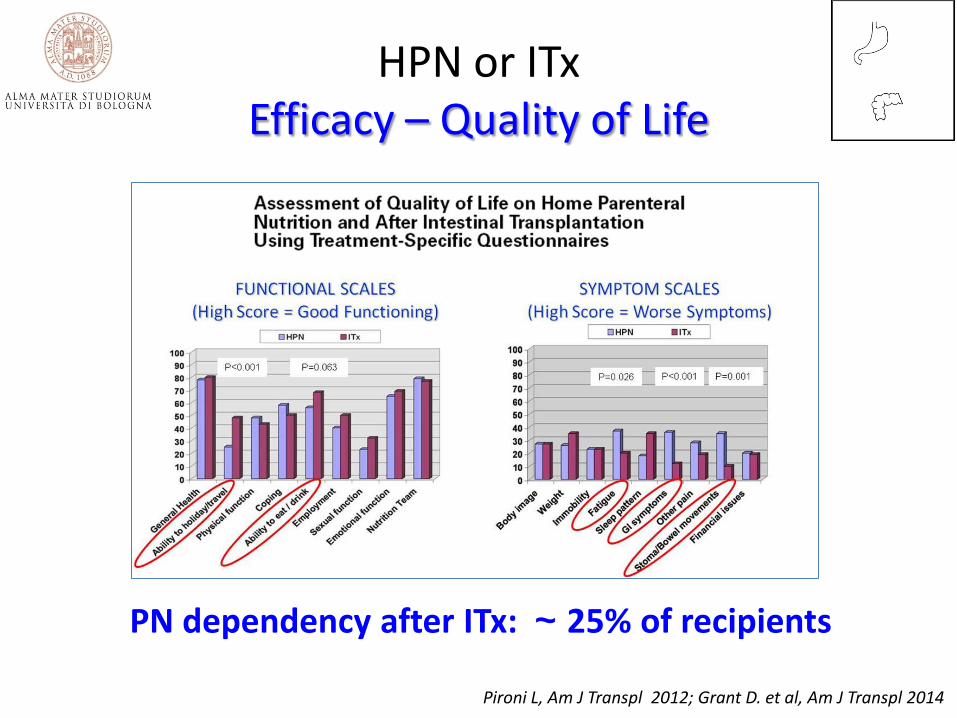
HPN or ITx Efficacy – Quality of Life
PN dependency after ITx: ~ 25% of recipients
Pironi L, Am J Transpl 2012; Grant D. et al, Am J Transpl 2014

Risk factors for death or graft failure Timing for ITx
2008 OPTN/SRTR Annual Report; Grant D. ITA Registry Report 2011at http://www.tts.org
0
10
20
30
40
50
60
Unadjusted 5-year survival of ITx recipients for patient age
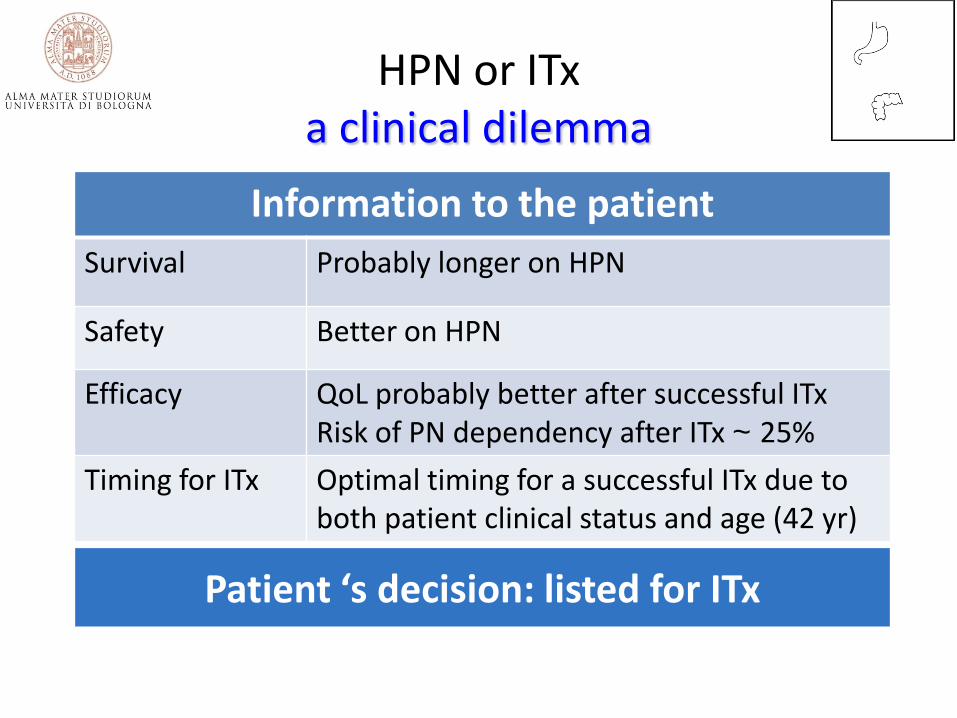
HPN or ITx a clinical dilemma
Information to the patient Survival Probably longer on HPN
Safety Better on HPN
Efficacy QoL probably better after successful ITx Risk of PN dependency after ITx ~ 25%
Timing for ITx Optimal timing for a successful ITx due to both patient clinical status and age (42 yr)
Patient ‘s decision: listed for ITx

but …4.5 years later • General well being on HPN • Working part time • Good family and social life
• Mild increase of LFT, normal bilirubin • One episode of CVC-infection • 100% survival on HPN
Patient’s decision: stay on HPN
HPN or ITx a clinical dilemma
