squamous cell carcinoma of the thyroid: a report of two cases
TRANSCRIPT

Journal of Surgical Oncology 9:567-578 (1977)
Squamous Cell Carcinoma of the Thyroid: A Report of Two Cases
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ................................................................................... EDWARD B. KAMPSEN,M.D., NIRMALA JAGER, M.D. , and MARTIN H. MAX, M.I).
Two patients with squainous cell carcinoma, wliich accounts for 1.1% of all primary thyroid car- cinomas, are described. Squamous nietaplasia is tlie most likely etiology, but an occasional carcinoma may be derived from remnants of embryonic origin. Although squanious metaplasia has been docu- mcnted in several conditions involving tlie thyroid, no evidence exists that this predisposes to squanious cell carcinoma. Metastases and direct extension of squanious cell carcinoma in the thyroid gland are much more frequent than primary involvement and are always part of a generalized carcinomatosis. A primary lesion must always be sought; however, diagnosis niay not be possible until an initially occult tumor becomes evident or even until autopsy. B c ~ ~ u s e this lesion typically runs a fulminant course, radical surgical resection at the earliest opportunity offers the best hope for cure. The lesions ;ire usually radioresistant. and chemotherapy has riot been shown to alter thc course of this disease.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Key words: squamous carcinoma, thyroid carcinoma
INTRODUCTION
Squanious cell carcinoma of the thyroid gland is an extremely rare primary neo- plasm, comprising only 1.1% of all primary thyroid cancers (Goldman, 1964). So fat-, about 50 cases of this rare disease have been documented in the world literature (Huang and Assor. 1971). Some of these are isolated case reports but many represent individual cases included in postmortem series of thyroid carcinomas. Once a matter of much de- bate, the histogenesis of this neoplasm is now considered t o be squamous nietaplasia. Differentiating between primary and secondary squamous cell carcinomas is important, and a thorough search for an occult primary neoplasm is always indicated. Because of the aggressive nature of this tumor, radical surgical resection offers the best hope of cure. Radiation therapy has been uniformly unsuccessful, and little is known about the results of chemotherapy because o f the rarity of the lesion. Because there is a uniform lack of experience in dealing with squamous cell carcinoma o f the thyroid, the present report details the authors’ experience with 2 patients with this disease and reviews the literature.
From tlie Dcpartment of Surgery, University of Louisville School of Medicine, Health Sciences Center, Louisville, Kentucky
Address reprint requests to Hiram C. Polk, Jr., Univcrsity of Louisville School of Medicine, Health Sciences Center, Louisville, KY 40201.
567 @ 1977 Alan R . Liss, Inc., 150 Fifth Avenue, New York, NY 10011
568 Kampsen, Jager, and Max
CASE REPORTS
A 73-year-old woman was admitted t o hospital complaining of a chronically drain- ing sinus in the neck, subsequent to a partial thyroidectomy performed some 8 months earlier. At that time she had gone t o her physician with a history o f rapid increase in a goiter that she had had from childhood and also with symptoms of dyspnea and pain in the neck. She underwent removal of a tumor from the right lobe of the thyroid gland. This was reported t o be a thyroglossal ductal cyst. Postoperatively, she developed a wound infection and underwent excision of a draining sinus tract in the wound. The wound continued t o drain, and the patient was referred t o the university teaching hos- pital. Physical examination disclosed a draining infected sinus in the surgical wound, a mass in the thyroid region o n the right side, and a palpable anterior cervical lymph node. Routine laboratory tests were all within normal limils. Thyroid function tests were nor- mal. I'31 uptake was nonnal, but scintiscan of the thyroid showed n o activity in the right lobe except in its upper pole. Chest x-ray examination showed a calcified granuloma in the right lung. Tomograms of the trachea demonstrated subglottic constriction by a right paratracheal mass indenting the trachea and displacing it lo the left. Bronchoscopy con- firmed the subglottic stenosis of the trachea. Exploration of the neck disclosed an infil- trating squamous cell carcinoma. A tracheostomy tube was inserted for ventilatory assis-
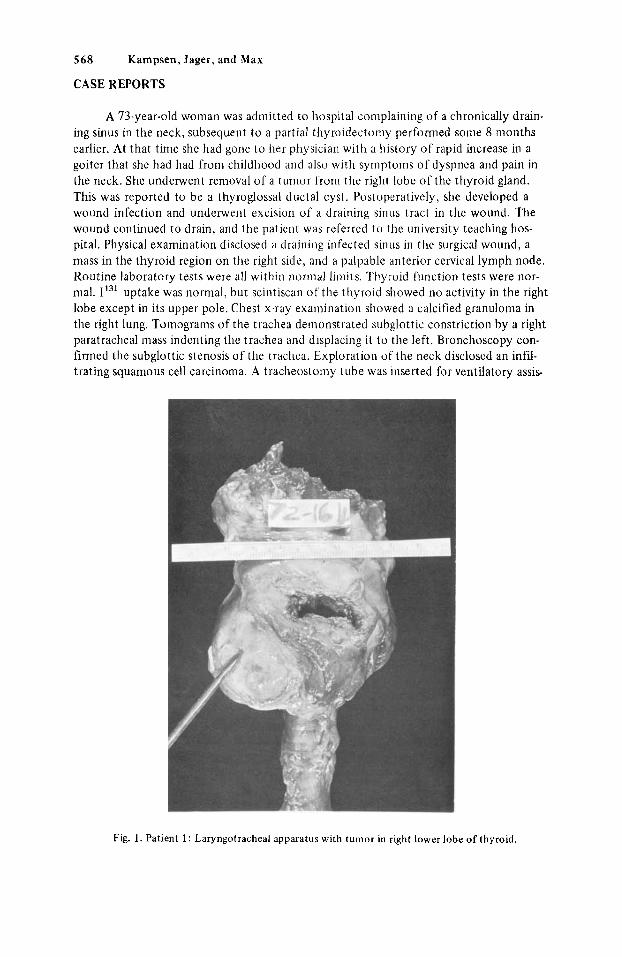
Fig. 1. Patient 1 : Laryngotracheal apparatus with tumor in right lower lobe of thyroid.
Squamous Cell Ca of Thyroid 569
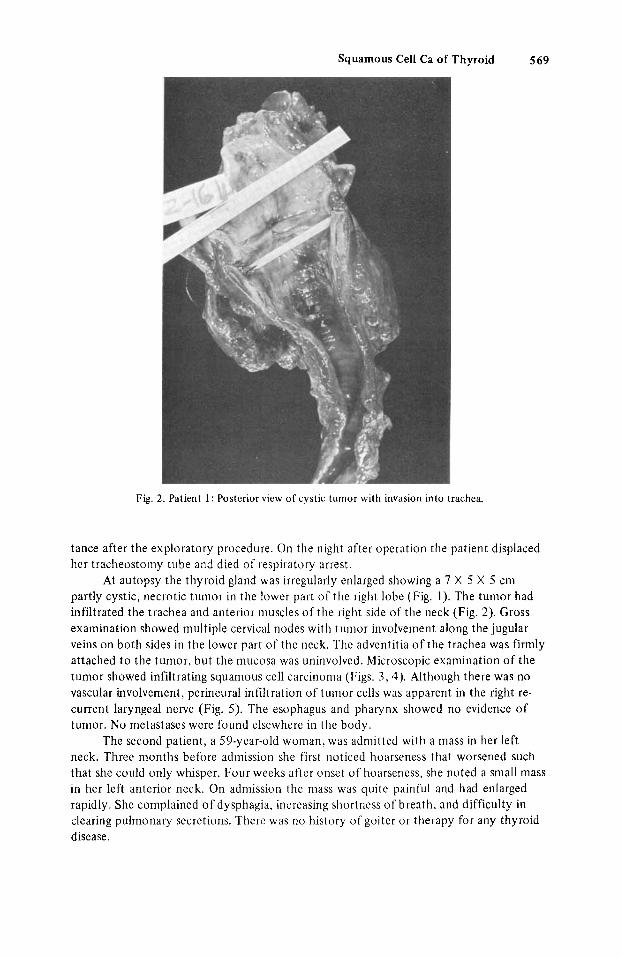
Fig. 2. Patient I : Posterior view of cystic tumor with invasion into trachea.
tance after the exploratory procedure. On the night after operation the patient displaced her tracheostoniy tube and died of respiratory arrest.
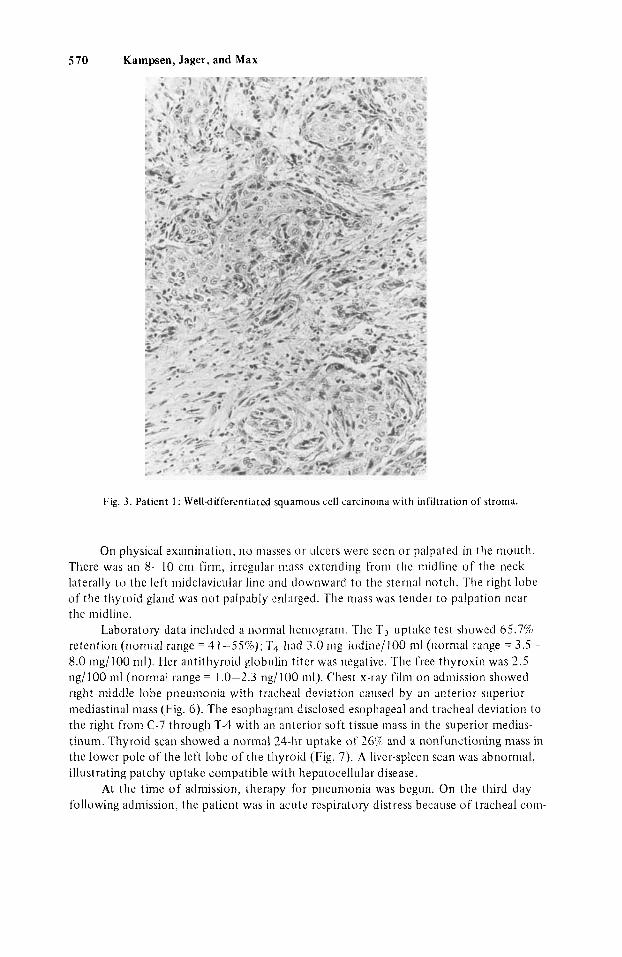
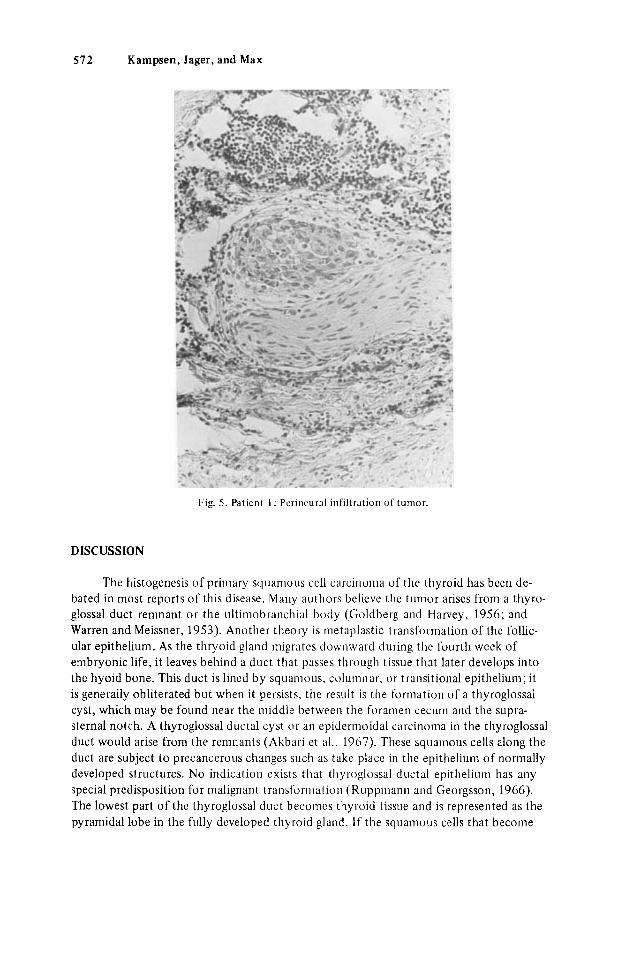
At autopsy the thyroid gland was irregularly enlarged showing a 7 X 5 X 5 cm partly cystic, necrotic tiinior in the lower part of the right lobe (Fig. 1). The tumor had infiltrated the trachea and anterior muscles of the right side of the neck (,Fig. 2 ) . Gross examination showed multiple cervical nodes with tumor involvement along the jugular veins on both sides in the lower part of the neck. The adventitia o f the trachea was firmly attached t o the tumor, but the niucosa was uninvolved. Microscopic examination of the tumor showed infiltrating squamous cell carcinoma (Figs. 3.4). Although there was no vascular involvement, perineum1 infiltration of tumor cells was apparent in the right re- current laryngeal nerve (Fig. 5). The esophagus and pharynx showed no evidence of tumor. No metastases were found elsewhere in the body.
The second patient, a 59-year-old woman, was admitted with a niass in her left neck. Three months before admission she first noticed hoarseness that worsened such that she could only whisper. Four weeks after onset of hoarseness, she noted a small mass in her left anterior neck. On admission the niass was quite painful and had enlarged rapidly. She complained o f dysphagia, increasing shortness of breath, and difficulty in clearing pulmonary secretions. There was no history of goiter or therapy for any thyroid disease.
5 70 Kampsen, Jager, and Max
Fig. 3 . Patient I : Well-differentiated squamous cell carcinoma with infiltration of stroma.
On physical examination, no masses or ulcers were seen or palpated i n tlie rnouttl. There was an 8-10 cm firm, irregular mass extending from tlie midline of the neck laterally t o the left midclavicular line and downward t o the sternal notch. The right lobe of the thyroid gland was not palpably tlnl;it-ged. The mass was tender to palpation near the midline.
retention (normal range = 4 1-.55%,); T4 had 3.0 mg iodine/100 nil (normal range = 3.5 - 8.0 mg/100 ml). Her antithyroid globulin titer was negative. The free thyroxin was 2.5 ng/100 ml (normal range = 1.0-2.3 ng/100 nil). Chest x-ray film on admission showed right middle lobe pneumonia with tracheal deviation caused by an anterior superior mediastinal mass (Fig. 6). The esophagram disclosed esophageal and tracheal deviation to the right from C-7 through T-4 with an anterior soft tissue mass in the superior medias- tinum. Thyroid scan showed a normal 24-hr uptake of 26% and a nonfunctioning mass in the lower pole of the left lobe of the thyroid (Fig. 7). A liver-spleen scan was abnormal, illustrating patchy uptake compatible with hepatocellular disease.
At the time o f admission, therapy for pneunionia was begun. On tlie third day following admission, the patient was in acute respiratory dist I-ess because of tracheal com-
Luboratory data included a nomial liemograni. The T 3 uptake test showed 65.7%

Squamous Cell Ca of Thyroid 571
Fig. 4. Patient 1: Nests of squainous cells invading thyroid parenchyma.
pression and infection, and she required nasotracheal intubation. When the patient’s con- dition stabilized, surgical exploration of the neck was carried out. and a cystic mass in the thyroid gland, adherent to the trachea and esophagus and extending downward to below the sternal notch, was found. Laterally, the cystic mass compressed the left coninion carotid artery; pulsation of the subclavian artery could be felt in the inferior wall below the clavicle. Partial removal of the left neck mass, a tracheostomy, and direct laryngos- copy were performed. The mass was an infiltrating keratinizing squamous cell carcinoma, involving the thyroid gland (Fig. 8), infiltrating the adjacent skeletal muscle (Fig. c)), and invading the lymphatics (Fig. 10).
Postoperatively, an extensive search for ;I primary focus was begun. Gallium scan disclosed increased uptake in the base of the left side of the neck and an area of less in- tensity in the right posterior superior niediastinum. Liver biopsy showed fatty meta- morphosis only. Bronchoscopy was normal, and repeat evaluation of the nasopharynx was within normal limits. On the 17th postoperative day, radiation therapy to the neck and mediastinuni was begun, the patient receiving 3,750 rads over 20 days. She died 7 months after diagnosis of diffuse metastases without evidence of another primary lesion.
572 Kampsen, Jager, and Max
Fig. 5 . Patient 1 : Pcrincural infiltration of tumor.
DISCUSSION
The histogenesis of primary squanious cell carcinoma of the thyroid has been de- bated in most reports of this disease. Many authors believe the tumor arises from a thyro- glossal duct remnant or the ultiniobranchial body (Goldberg and Harvey, 1956; and Warren and Meissner, 1953). Another theory is metaplastic transformation of the follic- ular epithelium. As the thryoid gland migrates downward during the fourth week of embryonic life, it leaves behind a duct that passes through tissue that later develops into the hyoid bone. This duct is lined by squamous. columnar, or transitional epithelium; it is generally obliterated but when it persists, the result is the formation of a thyroglossal cyst, which may be found near the middle between the foramen cecum and the supra- sternal notch. A thyroglossal ductal cyst or an epidennoidal carcinoma in the thyroglossal duct would arise from the remnants (Akbari et al., 1967). These squanious cells along the duct are subject t o precancerous changes such as take place in the epithelium of normally developed structures. No indication exists that thyroglossal ductal epithelium has any special predisposition for malignant transt'orniation (Ruppmann and Georgsson, 1966). The lowest part of the thyroglossal duct becomes thyroid tissue and is represented as the pyramidal lobe in the fully developed thyroid gland. If the squamous cells that become

Squamous Cell Ca of Thyroid 573
Fig. 6 . Patient 2 : Anterior superior mediastinal mass with tracheal deviation to the left.
malignant in the gland are from this source. then one could expect squamous cell car- cinoma t o occur more frequently in the pyramidal lobe. However, because almost all instances of primary squamous cell carcinoma have been situated in the lateral lobes (Goldberg and Harvey, 1956), considerable doubt arises that the thyroglossal ductal remnant is the source of the squamous cell carcinoma o f the thyroid gland.
in the thyroid. This structure is formed as an out-pouching of the caudal aspect of the fourth branchid complex. In the human embryo, Kingsbury was consistently able t o detect ultimobranchial cells up t o the 31 inm stage (Goldberg and Harvey, 1956). After this stage the ultimobranchial body is indistinguishable from the thyroid gland itself (Goldberg and Harvey, 1956). Embryologic studies have documented its incorporation into the thyroid gland of sheep and guinea pigs (Harcourt-Webster, 1966; Jaffe, 1937). By feeding rats a diet deficient in vitamin A, cysts lined with squarnous epithelium have been produced in the exact area normally occupied b y the ultimobranchial body (Dube and Joyce, 1971). Although this hypothesis is intriguing, no one has been able to docu- ment the presence of the ultiniobranchial body in the human embryo after the 35 mrn stage. Thus, whether this body contributes squamous cells that give rise t o squarnous cell carcinomas in adults is not known (Goldberg and Harvey, 1956).
The ultimobranchial body is also mentioned as a possible source for squamous cells

574 Kampsen, Jager, and Max
Fig. 7 . Patient 2: Thyroid scan showing cold nodule, left lower pole.
Squamous metaplasia is the most widely accepted etiologic theory for squamous cell carcinoma of the thyroid. Benign squamous cells occur in the thyroid glands under several conditions. Altered environment or a stimulus for altered function are the usual reasons given for the resultant squamous nietaplasia (Dube and Joyce, 197 1 ; Goldberg and Harvey, 1956), which may take place when old cells are injured or degenerate as a result of changing environment and new cells are generated in the new environment (Dube and Joyce, 1971; Jaffe, 1937). This would be consistent with the findings of squamous cells in strunia lyniphomatosa (Hashimoto’s struma) in areas of scar formation in patients with involuting thyroids and particularly in patients suffering from chronic nonspecific thyroiditis (Goldberg and Harvey, 1956; Jaffe, 1937; Klinck and Menk, 195 1). The histologic characteristics of these cells with their well-defined intercellular bridges leave no doubt that they are squamous cells (Klinck and Menk, 1951 ; Saxen, 1951).
changes, but this has not been proved (Dube and Joyce; 197 1). Papillary adenocarcinoma mixed with areas of benign squamous cells and squamous cell carcinoma has also been documented (Dube and Joyce, 1971; Harcourt-Webster, 1965; McKenzie e t al., 1958). Klinck and Menk (1951) demonstrated a gradual transition in thyroid cysts from follic- ular epithelium to squamous epithelium. This is very important, for if areas that show all stages in the metaplastic process were not found, the theory would lack a solid basis. But
An immunologic basis or a biochemical abnormality might also account for the
Squamous Cell Ca of Thyroid 5 7 5
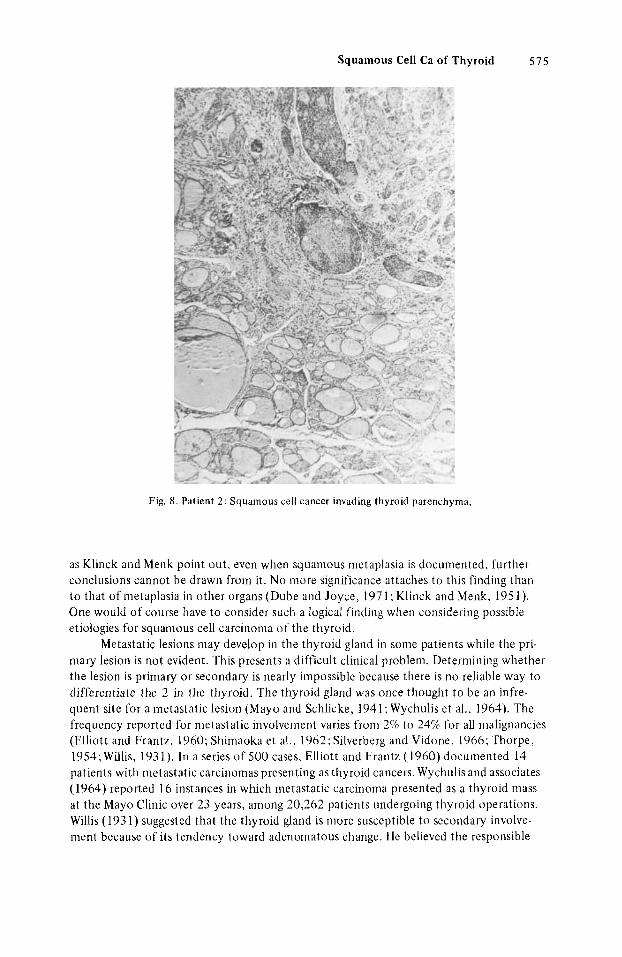
Fig. 8. Patient 2 : Squamous cell cancer invading thyroid parenchyma.
as Klinck and Menk point out. even when squamous nietaplasia is documented, further conclusions cannot be drawn from it. No more significance attaches to this finding than to that of metaplasia in other organs (Dube and Joyce, 1971; Klinck and Menk, 195 1 ) . One would of course have to consider such a logical finding when considering pvssibIe etiologies for squamous cell carcinoma of the thyroid.
Metastatic lesions niay develop in the thyroid gland in some patients while the pri- mary lesion is not evident. This presents a difficult clinical problem. Determining whether the lesion is primary or secondary is nearly impossible because there is n o reliable way to differentiate the 2 in the thyroid. The thyroid gland was once thought t o be an infre- quent site for a metastatic lesion (Mayo and Schlicke, 1941; Wychulis et al.. 1964). The frequency reported for metastatic involvement varies from 2% to 24%) for all malignancies (Elliott and Frantz. 1960; Shimaoka et al., 1962; Silverberg and Vidone, 1966; Thorpe, 1954; Willis, 193 1). In a series of 500 cases, Elliott and Frantz (1960) documented 14 patients with metastatic carcinomas presenting as thyroid cancers. Wychulis and associates (1964) reported 16 instances in which metastatic carcinoma presented as a thyroid mass at the Mayo Clinic over 23 years, among 20,262 patients undergoing thyroid operations. Willis (1931) suggested that the thyroid gland is niore susceptible t o secondary involve- ment because of its tendency toward adenornatous change. He believed the responsible

516 Kampsen, Jager, and Max
Fig. 9. Patient 2 : Invasion of skeletal muscle by yuamous cancer.
mechanisms t o be vascular stasis, which would yield a more favorable state for the fin- plantation of blood-borne emboli of tumor cells, and chemical changes in an adeno- matous gland, which would lower the iodine and oxygen content of the gland, making it a more favorable site for metastasis. Willis considered the latter mechanism to be more significant than stasis. Mayo and Schlicke (1941) also noted the propensity for metastatic lesions t o be found in the adenomatous glands. However, in a later study, Wychulis and colleagues (1964) noted that there was no such increase in the involvement of the thyroid glands with adenomatous changes. Reports by Mortenson and co-workers (1956) and also by Silverberg and Vidone (1966) noted that the thyroid gland was neither more suscep- tible nor more resistant t o metastases than any other organ with comparable blood and lymphatic flow. A review o f the study by Mortensen and associates is helpful if one is t o make the diagnosis of a primary neoplasm in the thyroid. In their autopsy studies, in n o patient was the thyroid gland the only organ involved by metastatic processes. Several reports have confirmed their findings that metastatic lesions in the thyroid are part of a generalized carcinomatosis (Harcourt-Webster, 1965 ; Mayo and Sclilicke, 194 1 ; Morten- sen et al., 1956; Silverberg and Vidone, 1966; and Thorpe, 1954). Only 1 % of the meta- static thyroid nodules were of enough clinical concern t o merit thyroidectomy in the report by Shiniaoka and associates (1962).

Squamous Cell Ca of Thyroid 577
Fig. 10. Patient 2 : Lymphatic plugging with tumor.
Often the identity of the primary carcinoma is obvious from the cell type of the metastatic lesion. The cell type and grade of cancer are usually identical in both the primary and metastatic lesions. Without the history of a previously identified carcinoma, a poorly differentiated tumor may be difficult to distinguish from a primary neoplasm. Primary squamous cell carcinoma is rare and the identification of a squamous neoplasm in the thyroid should initiate an immediate investigation to determine its source. Car- cinoma of the lung is a frequent primary squanious cell cancer that can metastasize to the thyroid. Direct involvement from the larynx, esophagus, trachea, or regional lymph nodes is also very conmion (Elliott and FI antL, 1960). Head and neck tumors, excluding those of the larynx, seldom nietastasiLe to the thyroid. This is not to say that the thyroid is not invaded by neoplasms originating in the head and neck. Willis (193 1) found inva- sion of the thyroid in 9 of 35 patients with epidermoidal carcinoma of the head and neck. Even after a thorough search, diagnosis is equivocal because many primary lesions may not become apparent until several months after the metastatic lesion is first documented.
Most patients present in the fifth or sixth decade of life (Warren and Meissner, 1953). Often there will be a long history of goiter in patients with primary carcinoma as opposed to those patients with metastases, as is exhibited by our first patient (Warren and Meissner, 1953). Both patients described herein experienced a rapid increase in the size of their tumors associated with dyspnea and pain. At the time of operation, local soft tissue

578 Kampsen. Jager, and Max
invasion is often noted; this was found in both of our patients. Hoarseness and dysphagia are also common complaints. The course of the disease is rapid, death usually occurring within 1 year. Radiation therapy has been unifomily unsuccessful despite a well-differ- entiated cell type in most tumors (Goldman, 1964; and Huang and Assor, 1971). Chemo- therapeutic effects cannot be evaluated because of a lack of experience in dealing with this cancer. Radical surgical resection is currently the treatment of choice. Diagnosis must be made early, however, or the lesion may prove inoperable.
REFERENCES
1. AkLxiri, Y ., Richter. R.M., Papadakis. L.1:. ( 1967): Thyroid carcinoma arising in thyroglossal duct
2. Dube, V.1, .., Joyce, G.T. ( 1 97 1): 1:xtrctne squainous metaplasia in Hashimoto’s thyroiditis. Canccr
3 . Elliott, R.I1. , Jr . , ITrantz, V.K. (1960): Metastatic carcinoma masquerading as primary thyroid
4. Goldberg, H .M. , Harvey, P. (1956): Squamous-cell cysts of tlie thyroid with special reference to
5. Goldman, R.L. (1964): Primary squamous cell carcinoma o f the thyroid gland: Report of a case
6. Ilarcourt-Webster. J.N. (1965): Secondary neoplasm of the thyroid presenting as a goitre. J. Clin.
7. t~arcourt-\\’cbster, J.N. ( 1 966) . Squanious cpitliclium in the human thyroid gland. J. Clin. Path.
8. Huang, T.Y., Assor, D. (1971): Primary squainous cell carcinoma of the thyroid gland: A report
9. Jaffe, K.11. (1937): Epithelial metaplasia of t l ie thyroid gland with special reference to the histo-
remnants: Report o f a case and review of the literature. Arch. Surg. 94:235.
2 7 4 3 4 .
cancer: A report of authors’ 14 cases. Ann. Surg. 151:551.
the aetiology of squamous epitlielium i n the human thyroid. 131. J . Surg. 33:565.
and review of the literature. A m . Surg. 30:247.
Path. 18:282.
19:384.
of four cases. Am. J. Clin. Path. 55:93.
genesis of squamous cell carcinoma of the thyroid gland. Arch. Path. 23 :821. 10. Kliiick, G.H.. Menk, K.F. (1951): Squamous cells in the human thyroid. Milit. Surg. 109:406. I I . Mayo, C.W., Schlicke, C.P. (1941): 1:sogenous tumors of tlie thyroid gland. Am. J. Path. 17:283. 12. McKenzie, A.11.. Moore, J.R., b‘idlcr, H.K. (1958): Cancer of the thyroid: Undifferentiated and
13. hlortenscn, J.D., Woolner, L.H., Ucnnctt, W.A. (1956): Secondary malignant tuinors of the
14. Ruppniann, E., Georgsson. G. (1966): Squanious carcitioiiia of tlie tliyroglossal duct . German
15. Saxen, 1;. (195 I ) : Squarnous iiictaplasia in the thyroid gland and histogenesis of epiderinoid car-
16. Sliimaoka, K., Sokal. J.E., PiLkt-en. J . W . (1962) : Metastatic neoplasnis in the thyroid gland:
17. Silverberg, S.G., Vidone, 1I.A. (1966): Metastatic tumors in the thyroid. Pacif. Med. Surg. 4:175. 18. Thorpe, J.D. (1954): Metastatic cancer in the thyroid gland; report of four cases. West. J. Surg.
6 2 5 7 4 . 19. Warren, S., Mcissner, W.A. (1953): Tumors of the thyroid gland. “Atlas of Tumor Pathology.”
Washington, D.C., Armed Forces Institute of Pathology, See. IV, Fasc. 14. 20. Wiliis. R.A. (1931): Metastatic tumors i n the thyroid gland. Am. J. Path. 7:187. 21. Wychulis, A.R. , Beahrs, O.H.. Woolner, L.B. (1964): Metastasis of carcinonia to the thyroid
miscellaneous carcinomas. Can. J . Surg. 2:73.
thyroid gland. Cancer 9:306.
Mcd. Monthly 11 :442.
cinoma of thc thyroid. Acta Path. Micrubiol. Scand. 28:S5.
Palhological and clinical findings. C‘anccr 15 :5S 7.
gland. Ann. Surg. 160: 169.