carcinoma thyroid
TRANSCRIPT

CARCINOMA THYROID
DR GAURAV TYAGIDR SHEHTAJ KHAN SURGERY UNIT I

“Thyroid” –Thomas Wharton

Theodor Bilroth
Emil Theodor Kocher
Nobel Prize 1909
EPIDEMIOLOGY AND STATISTICS
•Commonest malignant Endocrine tumour.
•Comprise 1% of all malignancies.•Sex Ratio is 3:1 (Female:Male)•Can occur at any age group
▫Peak incidence after age of 30.▫Aggressiveness increases with old age.

• Incidence of Carcinoma of thyroid has risen 189% during 1973-2003 in the world.
• In a survey conducted by The National Cancer Registry Programme in Bangalore & ICMR, Delhi, “a belt of thyroid cancer” in women of coastal districts of Kerala, Karnataka, and Goa.
India has some of the highest cancer rates in the world Ganapati Mudur
BMJ. 2005 January 29;

ETIOLOGY & RISK FACTORS:•Female gender•Radiation exposure•Family h/o•Iodine deficiency states•Thyroiditis (Hashimoto’s
diseaseLymphoma)•Genetics/Mutations: -RET-proto-oncogene -MEN2A/2B -Gardener’s synd, FAP


PRESENTATION•The most common presentation is a
painless neck mass/solitary thyroid nodule.•Symptoms consistent with malignancy.
Cervical lymphadenopathy. Rapid enlargement. Dysphagia Stridor. Hemoptysis. Hoarseness. Pain Bone pain, fractures.

CLINICAL EVALUATION
Physical Examination
•Size•Consistency - hard vs. soft•Mobility•Well circumscribed vs. ill defined borders•Multinodular vs. solitary nodule
▫multi nodular - 3% chance of malignancy▫solitary nodule - 5%-12%.

•Systematic palpation of the neck Metastatic adenopathy commonly found:
Central compartment (level VI) Lateral group (regions III and IV)
•Indirect or fiberoptic laryngoscopy. vocal cord mobility evaluate airway preoperative documentation of any unrelated
abnormalities

LABORATORY INVESTIGATIONS Thyroid function tests: T3, T4, TSH
Serum Calcitonin: basal/pentagastrin stimulated calcitonin levels (>300 pg/ml)
Thyroglobulin(Tg)At 6-months interval then annually when disease-free< 2ng/mL in total or near-total thyroidectomy> 2ng/mL = Recurrence/Persistent thyroid tissue
Carcinoembryonic antigen (CEA) the reference value is less than 3 ng/dL.

ULTRASONOGRAPHY
•7.5-16 MHz probe•B-mode USG can be used intraoperatively•Increasingly used to assist FNA•Limited ability to predict the diagnosis of
solid nodules accurately

Findings suggestive of malignancy:
• Microcalcifications• Hypervascularity• Infiltrative margins• Hypoechogenicity• Height>>width on transverse view

Nodules <1 cm with benign characterstics are not further evaluated except :
• Lymphadenopathy• h/o radiation exposure• Family h/o• Prior h/o Ca thyroid• PET positive lesions
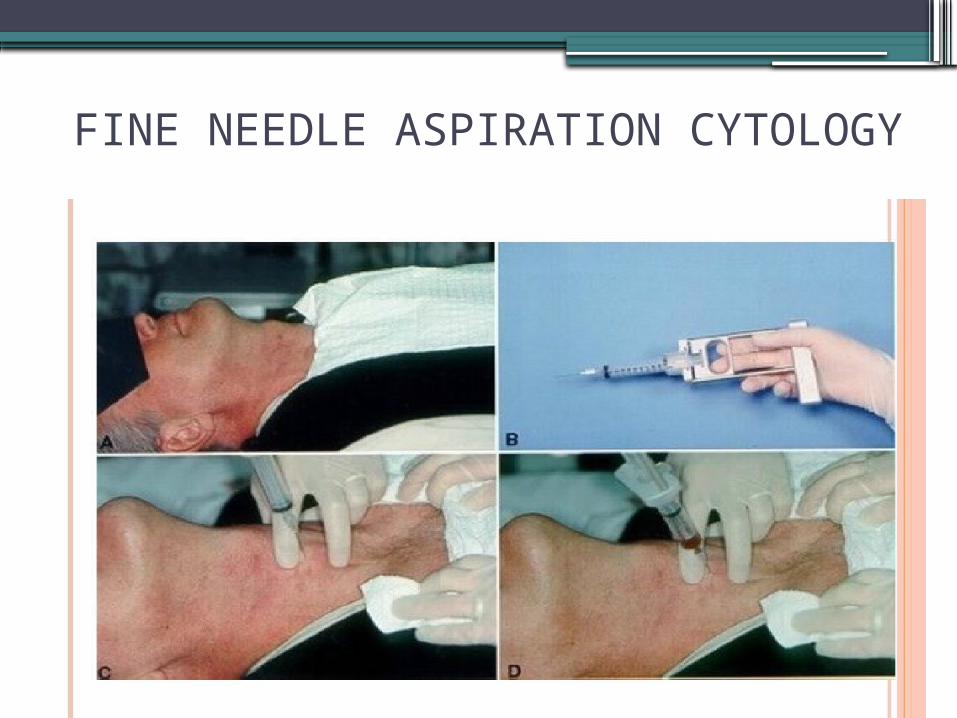
FINE NEEDLE ASPIRATION CYTOLOGY

•Popularized in the 1960s by Einhorn and Franzen in Stockholm, Sweden.
•Replaced intra-op frozen section •23 to 27G needle•Imaging guidance is recommended—
Especially--non palpable deep located -posteriorly located -cystic masses

TATA MEMORIAL HOSPITAL GUIDELINES FOR FNAC RESULTS

RADIOISOTOPE SCANNING Functionality of the lesion Staging of the carcinoma 15-20% cold
nodules MALIGNANCY 5-9% warm/hot
nodules
-Malignancy neither confirmed nor excluded

Technetium-99m pertechnate(Tc99m): -Trapped by follicular
cells but not organified. -Short t1/2 , low radiation
exposure. -Also taken up salivary
glands & highly vascular structures.

•RADIOIODINE Trapped & organified
I-123 I-131-Low dose radiation -High beta radiation-Short t1/2 (12-13h) -t1/2-8days-Lingual thyroid & -Optimal for imaging Substernal goitres carcinoma -Screening
modality of choice for metastasis

PET- 18F-fluorodeoyglucose• Provides 3D reconstruction images.• Detecting primary, metastatic & recurrent
cancer.• 1-2% thyroid incidentalomas, usually benign.• Limited availabilty & cost.
Gallium-67Used in evaluation of lymphoma.

CT SCAN/MRI
-Both equally sensitive & specific-No added advantage to the workup of
uncomplicated cases-Large doses of Iodine in iv contrast
interfere with use of radioiodine for imaging/therapy

Useful in-
•Assessment of local extension in advanced stages & suspicious lesions with palpable lymph nodes
•Pre-op evaluation of large masses with tracheal deviation especially substernal masses
•Post-op follow up especially for suspicion of recurrence

CLASSIFICATIONPRIMARY:• Follicular epithelium – Well differentiated Undifferentiated Papillary Anaplastic Follicular Hurthle cell • Parafollicular cells (C-cells) Medullary • Lymphoid cells Lymphoma SECONDARY/METASTATIC:-Kidney -Breast -Colon-Direct extension -Melanoma


TNM STAGING OF THYROID CANCER

PROGNOSTIC INDICATORS
•AGES: AMES:-Age -Age-Hisological Grade -Metastasis-Extrathyroidal invasion -Extent-Size -Size
•MACIS(post-operative): Distant Metastasis Age Completeness of original surgical resection Extrathyroidal Invasion Size of original lesion

PAPILLARY CARCINOMA THYROID•Most common thyroid malignancy, 70-80%•30-50 years peak incidence•F/M ratio is 2.5:1•Excellent prognosis(>95% after 10 years)•Risk factors--Radiation exposure Family h/o, Familial
syndromes (Werner Syndrome,
Carney complex, Familial polyposis)

CLINICAL FEATURES
•Mostly presents as a “solitary thyroid nodule”
•Sometimes detected incidentally---”incidentaloma” 0r “microcarcinoma”(<1 cm)
•Spreads through lymphatic, lateral palpable lymph node can be a presenting feature “lateral aberrant thyroid”
•Spread to lungs, bones & brain is very rare.
•Mostly solid on USG but sometimes may have a cystic component.

PATHOLOGIACAL CLASSIFICATION•Diagnosis definitively made on FNAC.•Findings -cellular grooving -intranuclear
inclusion bodies -“PSAMMOMA
BODIES” -ground glass
cytoplasmic inclusions “ORPHAN ANNIE EYES”


CLASSIFICATION:
•Papillary carcinoma well differentiated•Follicular variant---10%•Insular •Columnar <1%, elder age
group,•Tall cell variant poor prognosis

TREATMENT
•SURGERY•RADIO IODINE THERAPY•POST OP THYROXINE REPLACEMENT
THERAPY

SURGICAL RESECTION
-Hemithyroidectomy/Lobectomy with/without Isthmusectomy
-Near Total Thyroidectomy ? Lymph Node
-Total Thyroidectomy Dissection

TOTAL V/S NEAR TOTAL THYROIDECTOMY
Recent American Thyroid Association Guide lines recommends more aggressive (total thyroidectomy) for well differentiated thyroid carcinonoma.
Advantages—• Higher survival, lower recurrence• Reduces risk of pulmonary mets• Improved sensitivity for Tg levels• RAIodine can be used better• Reduces risk of development of Anaplastic ca

NEAR TOTAL THYROIDECTOMY:
Leaves a much smaller(<1g) immediately adjacent to the Ligament of Berry.
•Less chances of postop hypoparathyroidism.
•Low risk of RLN injury.•Less chances of SLN injury.•Technically easy to perform.

LYMPH NODE DISSECTION
American Thyroid Association Revised Guidelines
•Therapeutic level VI dissection: clinically involved central neck nodes
•Prophylactic level VI dissection advanced primary (T3 or T4).
•Near-total or total thyroidectomy appropriate for (T1 or T2), non-invasive node-negative PTC.


Randomized Prospective Multicenter Trial of Prophylactic Central Node Dissection for Papillary Thyroid Carcinoma
FOR AGAINST
• Lower recurrence and mortality rates
• Decreases postop Tg levels
• Improves accuracy of staging
• Performed as safely as total thyroidectomy, experienced hands
• Central nodal metastasis can’t be reliably identified preoperatively or at surgery
• Higher rates of hypoparathyroidism.
• Higher rates of recurrent nerve injury
• Absence of level I data that it would lead to lower recurrence and mortality rates
• Majority of thyroidectomies in India are performed by low-volume surgeons.

BERRY PICKING:
•Increased Local Recurrence.•Complications Associated with Berry
Picking and Formal Neck Dissection are same.
•MRND preserves Spinal Accessory Nerve, IJV, and Sternocleidomastoid Muscle
•MRND-- Excellent Cosmetic, Oncologic, and Functional Outcomes
•Save the Picking for the Berries

•UNDIAGNOSED/SUSPICIOUS NODULE—
Thyroid lobectomy is an appropriate initial resection and serves as diagnostic biopsy except:
->4cm tumor.-marked atypia on FNAC/ suspicious of Ca.-Family h/o.-H/o radiation exposure.-Men >50 years of age.
These patients should undergo TOTAL/NEAR TOTAL THYROIDECTOMY.

•MICROCARCINOMA-
A unilateral lobectomy with/without isthmusectomy except :
-Clinically positive lymph nodes-Multicentricity-H/o head & neck radiation
In these cases total/near total thyroidectomy with or without lymph node dissection followed by radio iodine ablation.

•COMPLETION THYROIDECTOMY- ->1cm lesion-multifocal tumor-positive lymph nodes-high risk groups
ADVANTAGES:
Complete clearanceFacilitates radioiodine therapyEnables surveillance with serum Tg levels.

RADIOIODINE THERAPY
•The Indications:
1.To destroy residual thyroid tissue post-op. 2.Treat metastases to the lymph nodes,
lungs or bones. 3.Treat recurrence after initial treatment
by surgery or previous radioactive iodine or both.

Recent American Thyroid Association Guidelines recommended radioiodine
ablation for:
• Pt. with stage III or IV disease. • All Pt. with stage II disease <45 years. • Selected Pt. with stage I disease those with:
- large tumor ( >1.5 cm )- multifocality- residual disease- nodal metastasis

Radio Iodine (I-131) is given a in single dose on OPD basis- 6 weeks after surgery
•Low dose ablation (30 mCi) -young, low risk patients
•High dose ablation (100-200mCi) -older, high risk patients -incomplete resection

THYROXINE THERAPY
•Long term thyroxine(T4) replacement. (2.5-3.5 mcg/kg of L-T4 every day)•TSH suppression.
•High risk pt. TSH level below 0.1 mU/L
•Low risk pt. TSH level 0.1- 0.5 mU/L

SURVEILLANCE

FOLLICULAR CARCINOMA
•Account for 10% of all thyroid cancers.•More common in I-deficient areas.•F/M ratio is 3:1•40-60 years.•Age at diagnosis- most important
prognostic factor.•10 year survival---95% in <40 years 80% in 40-60 years

PRESENTATION
•Solitary thyroid nodule, rapid increase in size of long-standing goiter.
•Blood borne metastasis, most commonly lytic lesions in bones>>lungs.
•Cervical LN metastasis is uncommon(5%).•Hyperfunctioning <2% (thyrotoxicosis).

DIAGNOSIS:
•FNAC has limited value.•Unifocal lesion.•Histopathology provides
definitive diagnosis—•Follicular cells occupying
abnormal positions including capsular, vascular & lymphatic invasion.
•Frozen section- limited value.

TREATMENTFNAC suggestive of follicular neoplasm:
•Size <2cm----Hemithyroidectomy with Isthmusectomy.
•Size >2cm----Total Thyroidectomy
Histopathology shows carcinoma in lobectomy specimen should all be managed by a Completion Thyroidectomy.

Post-operative management-
-Radio Iodine Ablation. -Thyroxine Replacement Therapy. -Long term follow-up with serum Tg
levels.

HURTHLE CELL CARCINOMA
•Subtype of Follicular Carcinoma.•Multifocal & usually bilateral.• 60-75 years.•Abundance of oxyphilic cells/ oncocytes. (HURTHLE CELLS)•FNAC results are better suggestive than
in FTC

•Worse prognosis--increased incidence of lymphatic spread.-higher rate of recurrence.-poor uptake of iodine.
•TOTAL THYROIDECTOMY WITH LN DISSECTION is the treatment of choice.

MEDULLARY CARCINOMA
•5% of all thyroid malignancies.•Parafollicular C-cells. •25% Inherited (Germline mutation RET
oncogene).•F/M ratio 1.5:1•50 and 60 yrs age group in sporadic
cases.•Neck mass + palpable cervical LN(15-
20%).


MTC secretes a range of compounds:Calcitonin, CEA, CGRP, PGA2 and F2α,
Serotonin.May develop flushing and diarrhoea,
Cushing’s syndrome (ectopic ACTH).
Diagnosis:Family history.↑Sr Calcitonin(Basal & Pentagastrin
stimulated), ↑CEAFNAC.

MANAGEMENT:
Screen patient for:RET mutation.Pheochromocytoma (24-hour urinary level
of VMA, catecholamine, metanephrine).Hyperparathyroidism (Serum calcium).

•Surgery provides the only cure:
SPORADIC MTC
Total Thyroidectomy + : Bilateral Central Node Dissection as routine
(No LN involvement) Bilateral Modified-Radical Neck Dissection
(palpable LN) Ipsilateral Prophylactic Nodal Dissection in
tumor size >1.5cm.External Beam Radiation for unresectable
residual or recurrent tumor.No effective Chemotherapy.

FAMILIAL MTC (RET mutation +ve)
•Prophylactic Thyroidectomy:▫Before age of 6 yrs for MEN2A▫Before age of 1 yr for MEN2B
Pheochromocytoma when associated should be operated first

POSTOPERATIVE MANAGEMENT
Disease surveillance:
Serial Calcitonin and CEA▫2 weeks postop▫3 monthly for one year▫Biannually If Calcitonin rises ▫Metastatic work-up▫Surgical excision▫If metastases - external beam radiation

ANAPLASTIC CARCINOMA
•Most aggressive: Mortality ~100%.•1% of all thyroid tumors.•Older patients with dysphagia,
hoarseness, rapidly enlarging painful neck mass.
•Superior vena cava syndrome may be present.
•h/o prior/coexistent well differentiated cancer.
•50% have h/o goitre.•p53 mutations in 15%.

Pathology-
•FNAC accurate in ~90% cases•Giant cells, sheets of squamous cells or
islands of more recognisible differentiated carcinoma like PTC can be seen.
•Three subtypes -small cell -giant cell -squamous cell

MANAGEMENT:
•Distant spread esp to lungs present at the time presentation in 90% cases.
•If Resectable (CT/MRI)– Total Thyroidectomy with LN Dissection EBRT or Chemotherapy.
•Unresectable Tumors- Counseling, end of life planning & palliative surgery.
•EBRT limited
•Chemotherapy(DOXORUBICIN) role

LYMPHOMA OF THE THYROID GLAND
•Relatively rare, <1% of all lymphoma.•Mostly Non Hodgkin Lymphoma.•F/M ratio 3:1 to 8:1. •Median age is 7th decade.•Locally invasive.•Hypothyroidism in cases of Autoimmune
thyroiditis or Hashimoto’s thyroiditis.

•MANAGEMENT:
FNAC is highly suggestive but definitive diagnosis requires tissue diagnosis.
Primary treatment should be EBRT combined with Chemotherapy regimen based on histo-pathological subtype of lymphoma.
MALT lymphoma – Surgical Excision

RECENT ADVANCES

THYROID SURGERY
MIVATS- Minimally Invasive Video Assisted Thyroid Surgery
Miccoli, et al

Trans Axillary Gasless Robotic Thyroidectomy
Kang et al

Natural orifice surgery on thyroid gland:
Totally Transoral Video-Assisted Thyroidectomy (TOVAT)
CHEMOTHERAPEUTIC AGENTS
Vandetanib Tyrosinie kinase inhibitors
Carbzantinib Advanced MTC
Carboplatin + Paclitaxel - Anaplastic Ca
Sunitnib & Selumetinib - Tumor non responsive to Radio Iodine
Retinoic Acid - Increases tissue (Redifferentiation
therapy) response to Radio Iodine
