spine mri bir 2 copy
TRANSCRIPT

Spine MRI- Quality
Quantity QED!Dr W J Rennie
University Hospitals of Leicester
Leicester Royal Infirmary
Layout
• MRI sequences/Planes
• Protocol Logic- Briefly Image Quality!
• Disc Herniation
• Common & Uncommon Pathologies
• Reporting-How I do it!
• Why Spinal MRI is different!

Investigations in Clinical
Medicine - to reduce the degree
of Uncertainty!
What is Truth?
-Pontius Pilate
John c18:v38

MRI Protocols- How I do it!
• 30 minutes per body part
• 10 minutes for patient
transfer/positioning
• 20 minutes - Sequences
• Longest Sequence X 2
• Remaining time -Any number
of sequences!

Beware the Localiser
• Spinal MRI planned from
pedicle to pedicle!
• Localisers are quick GRE
sequences prone to
susceptibility and signal void!
• What you see is not always
what is True!

MRI Sequences
• Short TE
• T2W
• Fluid Sensitive sequences
• Sagittal plane
• Transverse plane

MRI Sequences
• Short TE
• Saturation bands
• Slice thickness and
Interspace
• Most Important Plane and
sequence in Spine

MRI Sequences
• T2 W
• Look good but are less
important in the Spine
• Spinal Surgeon Sequence
• Sagittal Imaging - Important
Plane
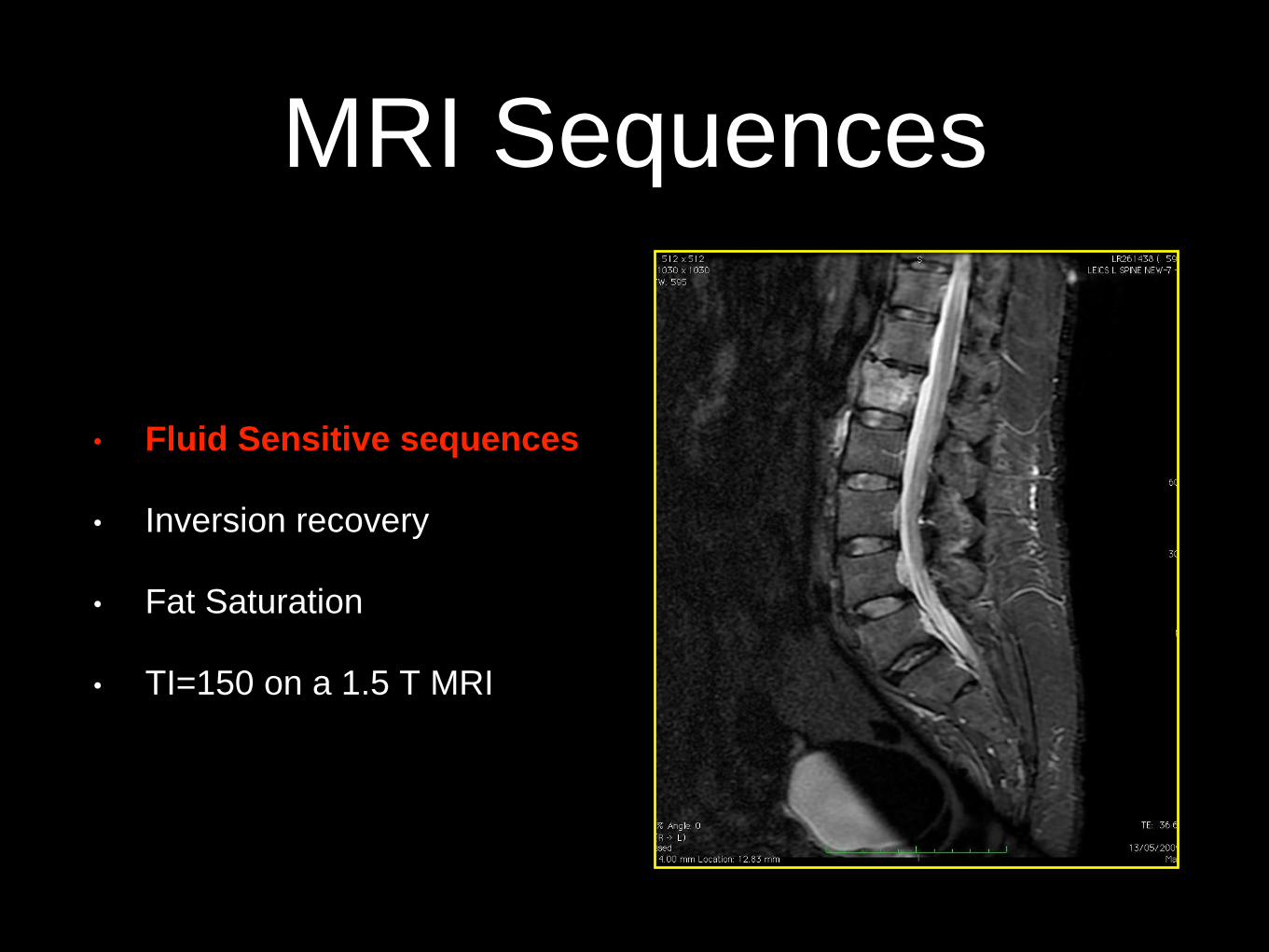
MRI Sequences
• Fluid Sensitive sequences
• Inversion recovery
• Fat Saturation
• TI=150 on a 1.5 T MRI

MRI Sequences
• Transverse Plane
• Ax T1
• Ax T2
• Angled to the disc/pathology
Level

Uncertainty & Quality
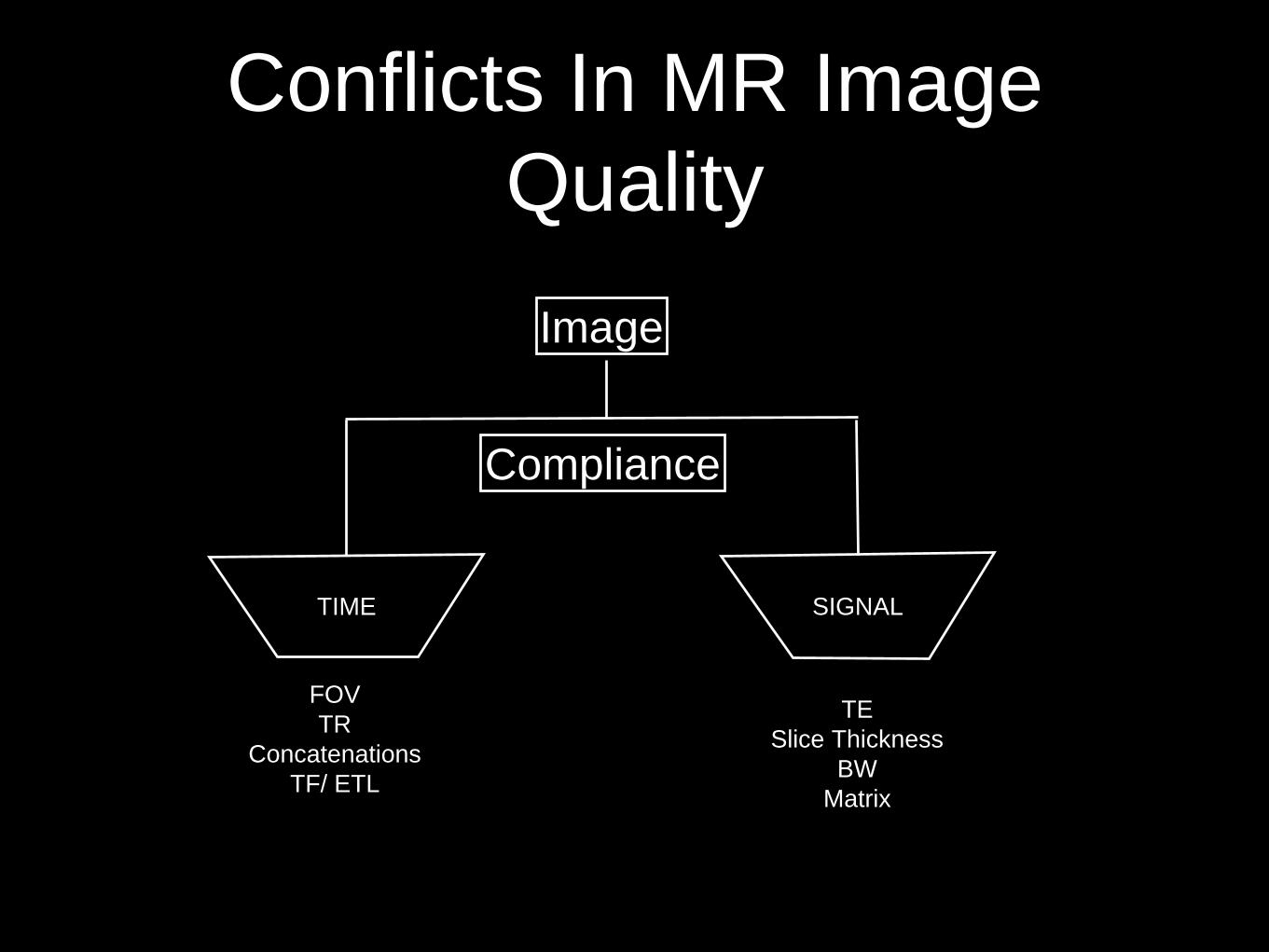
Conflicts In MR Image
Quality
TIME SIGNAL
Compliance
Image
FOV
TR
Concatenations
TF/ ETL
TE
Slice Thickness
BW
Matrix

MRI Protocol Planning
• Time/Resolution/Compliance
• Lumbar Spine Std=30mins
• 20 mins for sequences
• STIR = 4 mins x 2 =8mins
• 12mins plan any number of
sequences you can fit!
• FOV & Slice Thickness
• TE and TR = Weighting

Pathology

Common Pathologies
• Disc
degeneration/dehydration
• Disc Bulge
• Disc Herniation
• Spinal Stenosis
https://www.spine.org/Documents/ResearchClinical
Care/Nomenclature.pdf

Disc Herniation Report
• Location
• Containment
• Morphology
• Volume
• Continuity
• Migration
• Composition
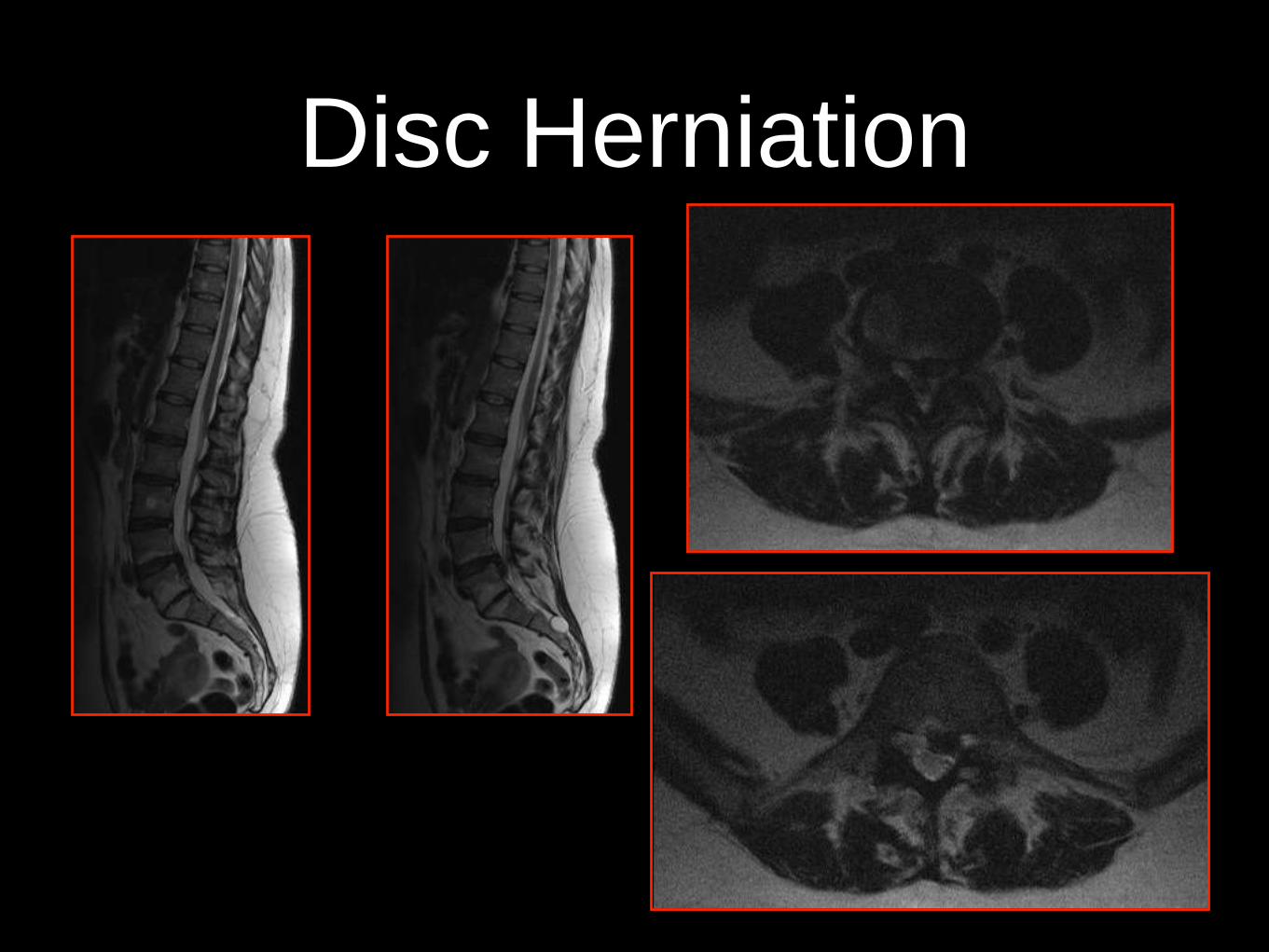
Disc Herniation

Disc Herniation
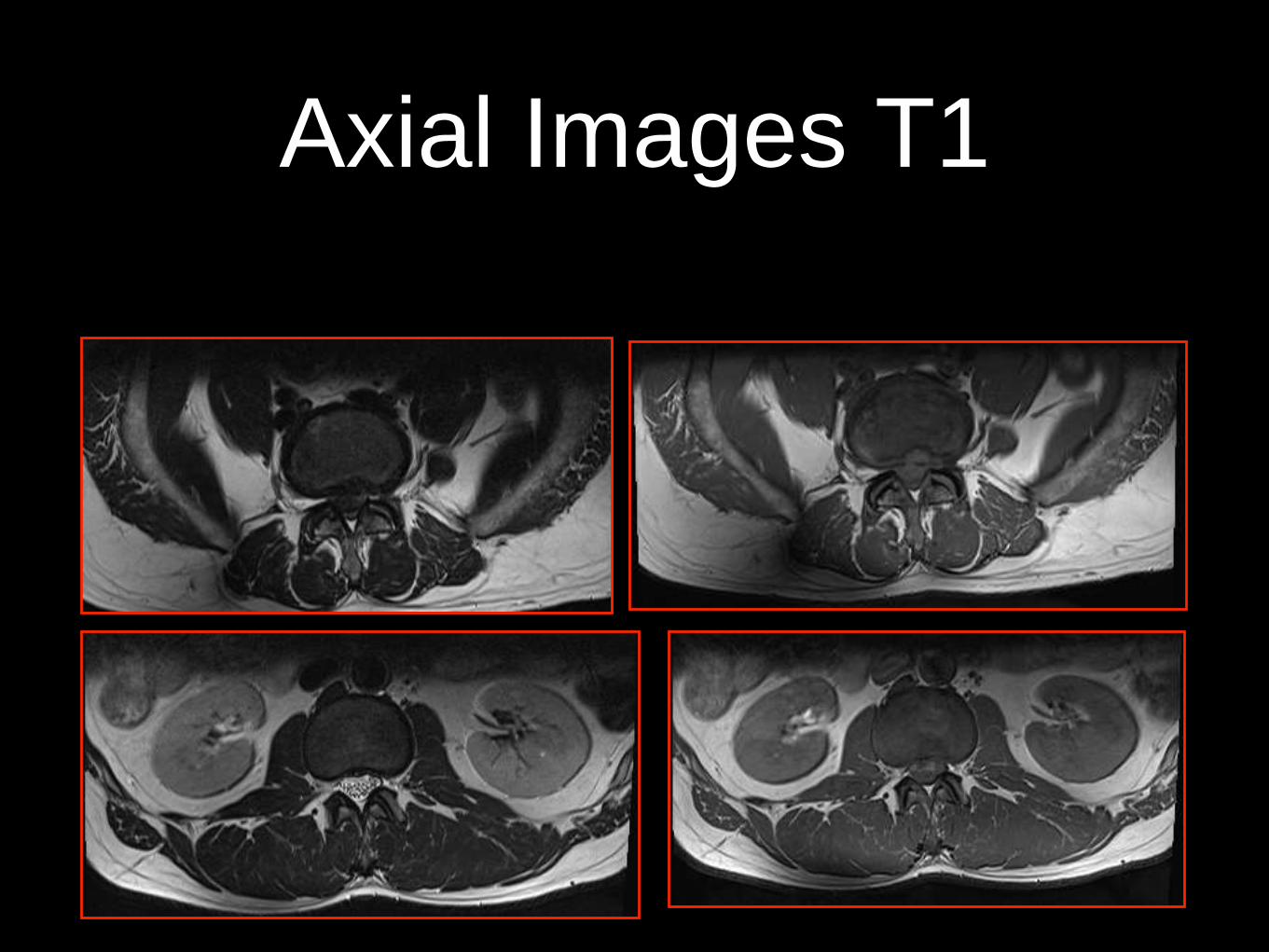
Axial Images T1

Pathology
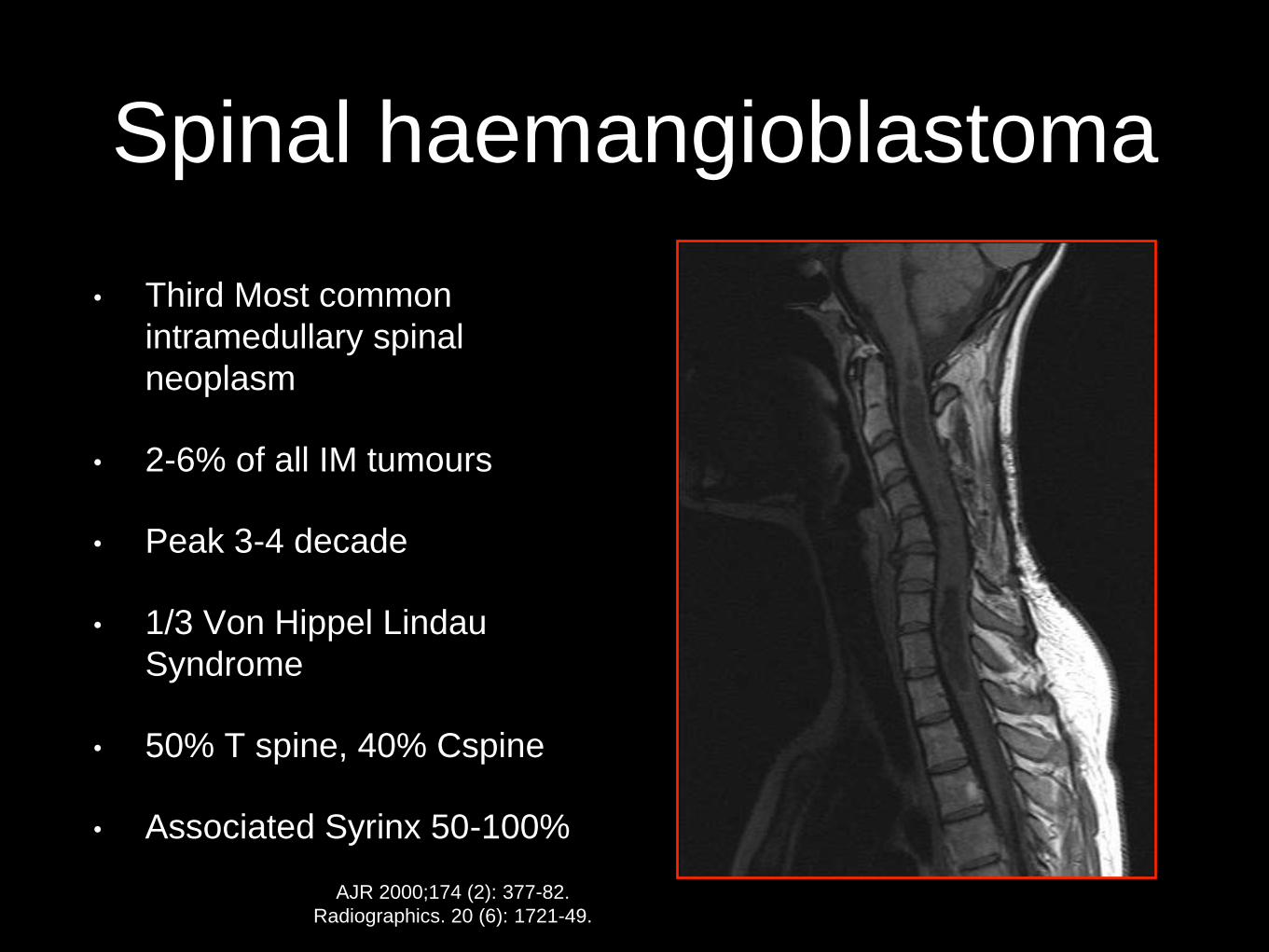
Spinal haemangioblastoma
• Third Most common
intramedullary spinal
neoplasm
• 2-6% of all IM tumours
• Peak 3-4 decade
• 1/3 Von Hippel Lindau
Syndrome
• 50% T spine, 40% Cspine
• Associated Syrinx 50-100%
AJR 2000;174 (2): 377-82.
Radiographics. 20 (6): 1721-49.
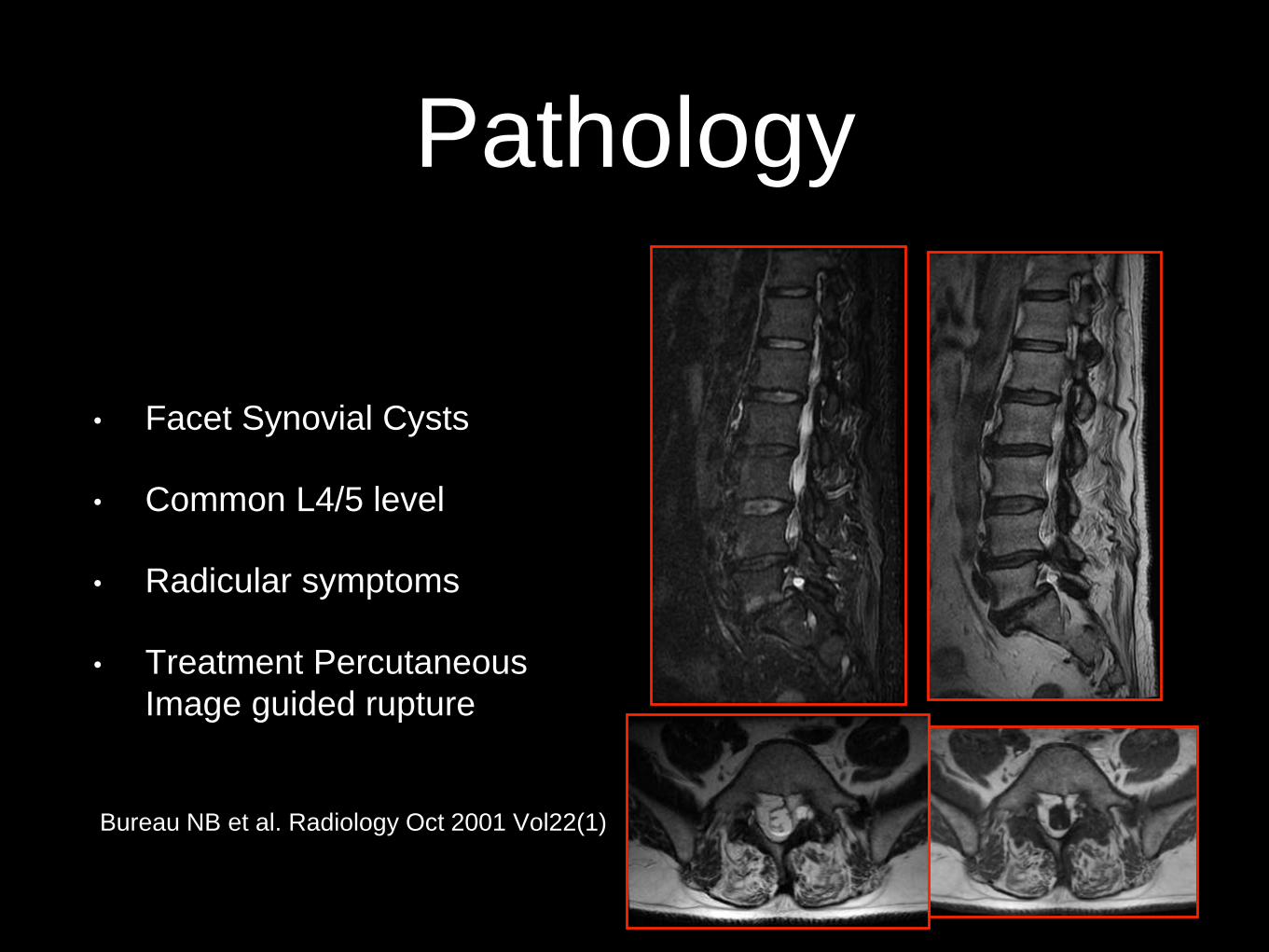
Pathology
• Facet Synovial Cysts
• Common L4/5 level
• Radicular symptoms
• Treatment Percutaneous
Image guided rupture
Bureau NB et al. Radiology Oct 2001 Vol22(1)

Pathology

Dural AVF

Spinal Dural AVF
• 70% of all vascular
malformations
• 5-6 decades
• M>F
• 60% Spontaneous
• Insidious Onset of progressive
weakness
AJNR Am J Neuroradiol. 2005;26 (8): 1949-54.
J Neurosurg Spine. 2011;15 (5): 541-9.

Pathology

Adhesive Arachnoiditis
• Empty Theca Sign
• Nodular/ Clumping
• Post surgical
• Post infective
• Associated with a syrinx
• Maybe asymptomatic
J Craniovertebr Junction Spine. 2010 Jul-Dec; 1(2): 100–106.

Pathology

Myeloma

Pathology
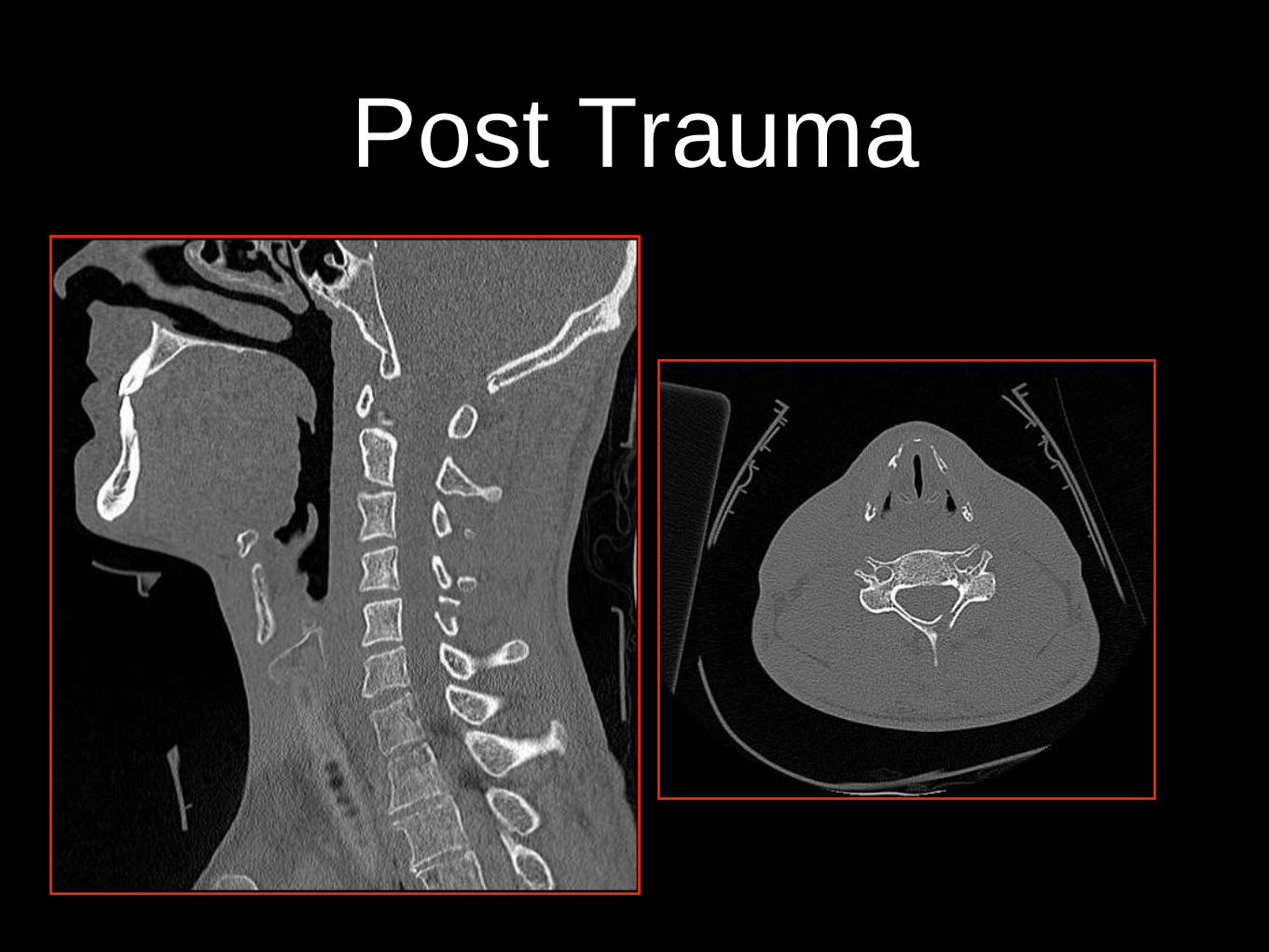
Post Trauma

Vertebral Artery Dissection
• Rare but not uncommon in <40
• Post traumatic
• Fractures extend into the
foramen transversarium
• Can have a latent period 3-4
days
• lateral medullary dysfunction
Wallenberg’s Syndrome
• Assess intracranial Extension
Radiographics. 20 (6): 1687-96.

Pathology

Demyelination
• Primary
• Infective
• Toxic
• Metabolic
• Ischaemic

Pathology

Intradural Haemorrhage
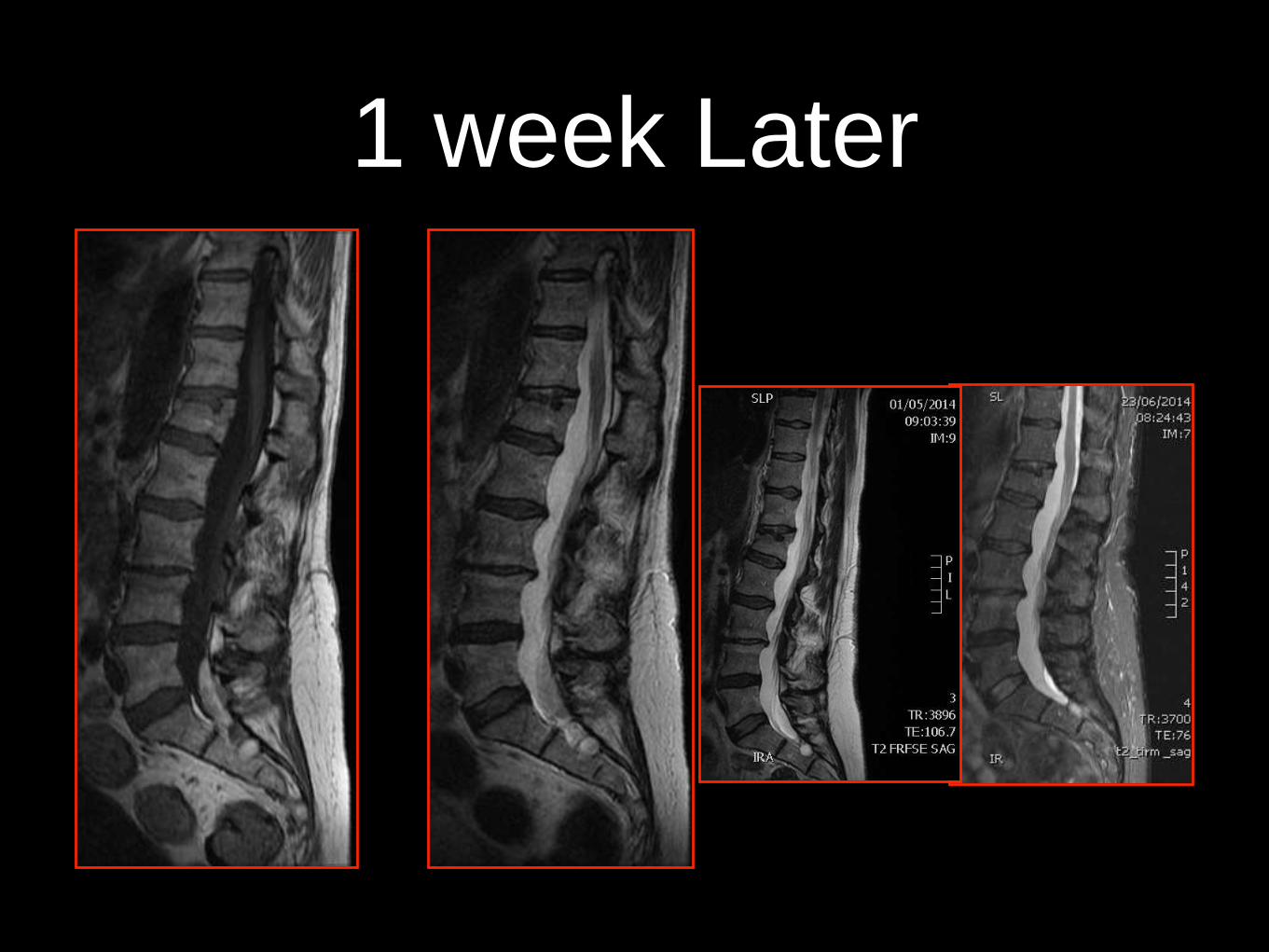
1 week Later

Intradural haemorrhage

Pathology

AAA
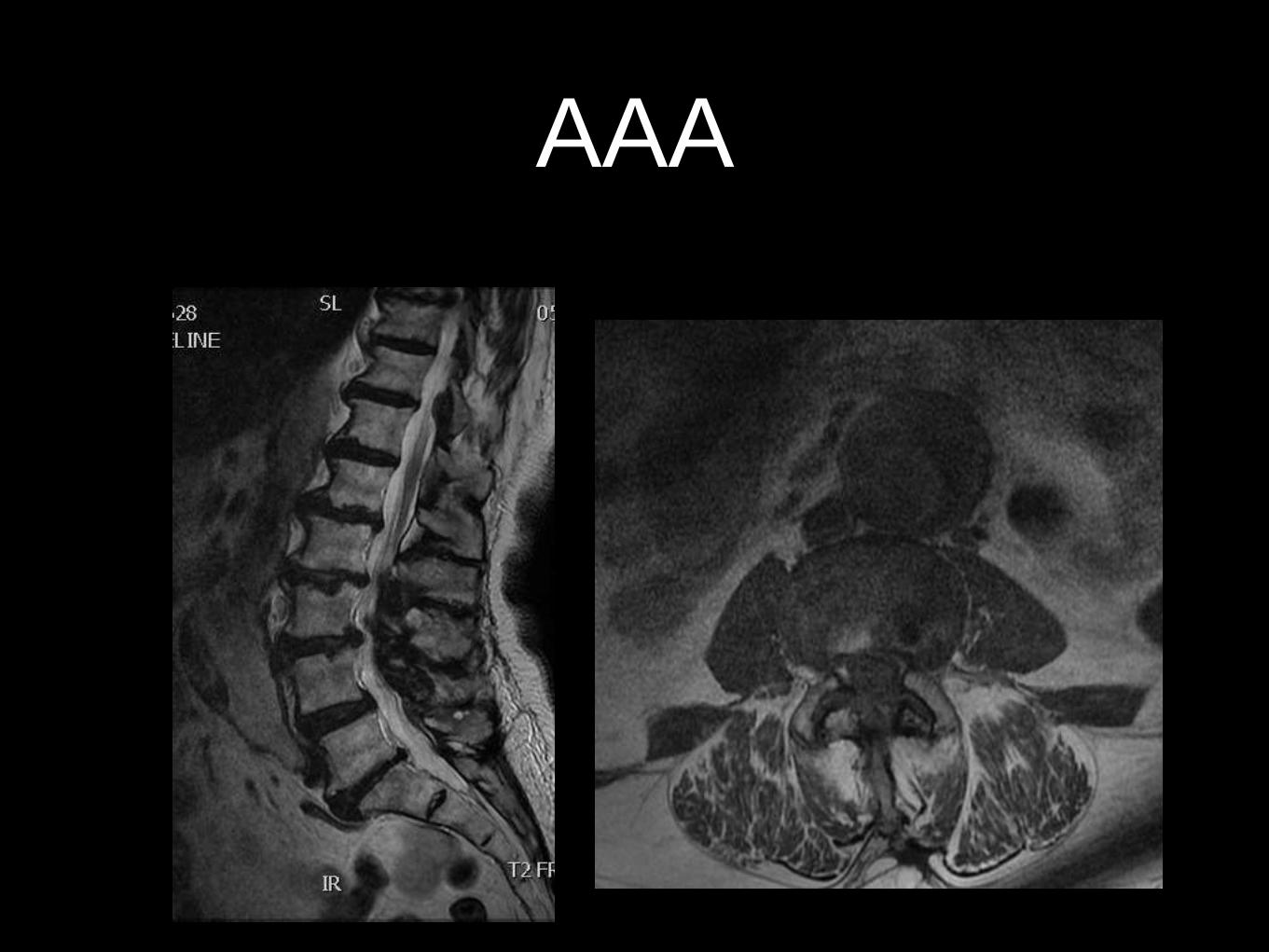
AAA
SpA

SpA MRI Protocol
• Costovertebral
• Costo transverse
• Lateral vertebral
• Lateral TP
Rennie WJ, Dhillon SS, Conner- Spady
B,MaksymowychWP, Lambert RGW. Arthritis
Rheum. 2009 Sep 15;61(9):1187-93.

SpA Spine
• Wide coverage laterally-
Check localiser
• Cervico Thoracic
• Thoraco Lumbar
• SIJ
• T1 &STIR
• 40 min-Book knee or brain
next= 2 parts in 1 hour!

Spine- SpA

SpA- SIJ
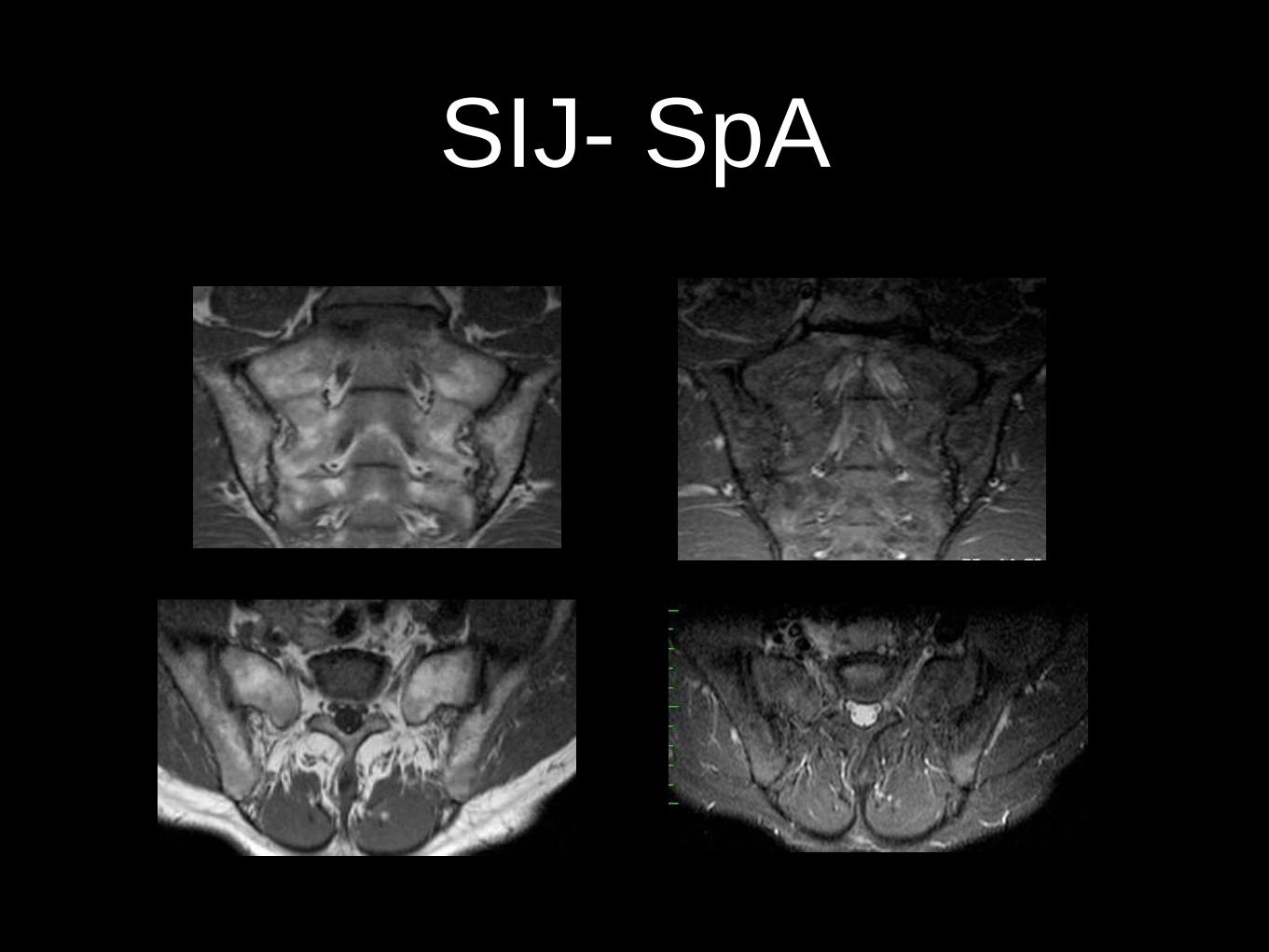
SIJ- SpA

www.carearthritis.com/mriportal/
login/
MRI Course Self-paced Learner

Reporting

Reporting
• Always related to the clinical Information
Provided
• Many ‘findings’ are clinically irrelevant
• Correlate Clinical History
• Spinal MRI Confounding Bias!
• Complications Of Spine Surgery

How I do It
• There are five Lumbar type vertebrae
• The conus is normal in signal intensity and
terminates at T12/L1
• No cauda or radicular compressive lesion is
demonstrated
• The lumbar Lordosis is preserved
• No spinal or paraspinal mass demonstrated

Why Spinal Imaging is prone
to Confounding Bias!
• Best plane in Cross-
sectional Imaging!
• Best Sequence for
Pathology
• Clinical Information
not always relevant
• Standard Protocols
• Sagittal
• T1W images
• Clinical Information always
relevant
• Tailored protocols
Summary
• MRI sequences/Planes
• How to obtain high quality images
• Disc Herniation
• Common & Uncommon Pathologies/ SpA
• Reporting How I do it!
• Why Spinal MRImaging is Prone to confounding Bias!
