spine injuries which cases should have early surgery? … problems can cause serious problems, even...
TRANSCRIPT

Spine injuries – Which cases should have early surgery? And which should NOT?
Tolga Aydoğ, MD, PhD
Acıbadem Fulya HospitalAcıbadem Sports
Acıbadem Mehmet Ali Aydınlar UniversityEczacıbaşı Sports Club

Spine problems can cause serious problems, even if they are relatively minor
• Low back pain affects
– Up to 80% of the general population,
– Nearly 30% of athletes
• All spine injuries
– 55% is cervical spine
– 45% is split thoracal, thoracolumbar, lumbosacral
• Totally 12,500 SCI new cases each year in US
– In athlets 9% of these
Li Y, Hresko MT. Clin Sports Med 2012
The content of the talk
• Evaluation on sideline
– Who can continue to game, who has to out?
– Should we take out? Take him to hospital andhow?
• Injuries requiring surgery
– Early
– In coming period
• Take home message

Evaluation on sideline
1st Step Airway (with C-spine)
2nd Step Breathing
3rd Step Circulation
4th Step Disability
5th Step Extraction from field of play
Gordon J, Nordstrom A. Ency of Football Med 2017

Evaluation on sideline
• Primary injuries; direct trauma affect the bone and/or soft tissue
• Secondary injuries; – Arterial disruption, arterial thrombosis Hypoxia
(ischemia free radicals due to reperfusion)
– Hypovolemiamicrocirculation breakdown, loss of autoregulation, etc• Deterioration of energy metabolism
Rackauskas Z et all. J Neurol Surg A 2016Gordon J, Nordstrom A. Ency of Football Med 2017

Evaluation on sideline
• Mechanism of injury;– Falling onto face;
• Central cord injury
– Falling flexion position with axial load;• Vertebral wedge fracture
– Falling from height onto the head• Burst fracture of the C1
• 10-15% of the cervical vertebrae injuries – Accompanied by spinal injuries in the other region
Anderson S, Schnebel B. Curr Pain Headache Rep 2016Gordon J, Nordstrom A. Ency of Football Med 2017

Evaluation on sideline –Cervical injury
• CCS (Canada Cervical Spine) rules– Absence of posterior midline C-spine tenderness
– GCS = 15
– An absence of focal neurological deficit (motor orsensory)
– Lateral neck rotation > 45°
– Axial load to head or fall from elevation < 90cm
– An absence of any distracting injury• Open fracture
• Visceral organ injury
Gordon J, Nordstrom A. Ency of Football Med 2017

Evaluation on sideline
• Possibility of cervical injury according to CCS
– Immobilization
• Hard Collar
– Transfer to hospital
Gordon J, Nordstrom A. Ency of Football Med 2017

Treatment algorithm for C- spine injury
Huang P et all. Sports Health 2016
Imaging in spinal injuries
• X-ray– Cervical AP, lat ve open mouth AP graphy (for odontoid)
• 93% sensitive for fracture
+ Flex/ext X-ray (attention)• 99% negative predictive value
• CT-scan– For cervicothoracic region absolutely
– Other region may be add
• MRI – Effective in revealing disc and ligamentous structure
Huang P et all. Sports Health 2016Chin LS et all. e-medicine 2017
Puvanesarajah V et all. Clin Spine Surg 2017
Indications for surgery
Early surgery
– Acute fractures with instability
– Compression on spinal cord and cauda equina
Surgery in the following period
– Do not response conservative treatment
– Progressive weakness
Eddy D et all. Clin J Sports Med 2005Rackauskas Z et all. J Neurol Surg A 2016

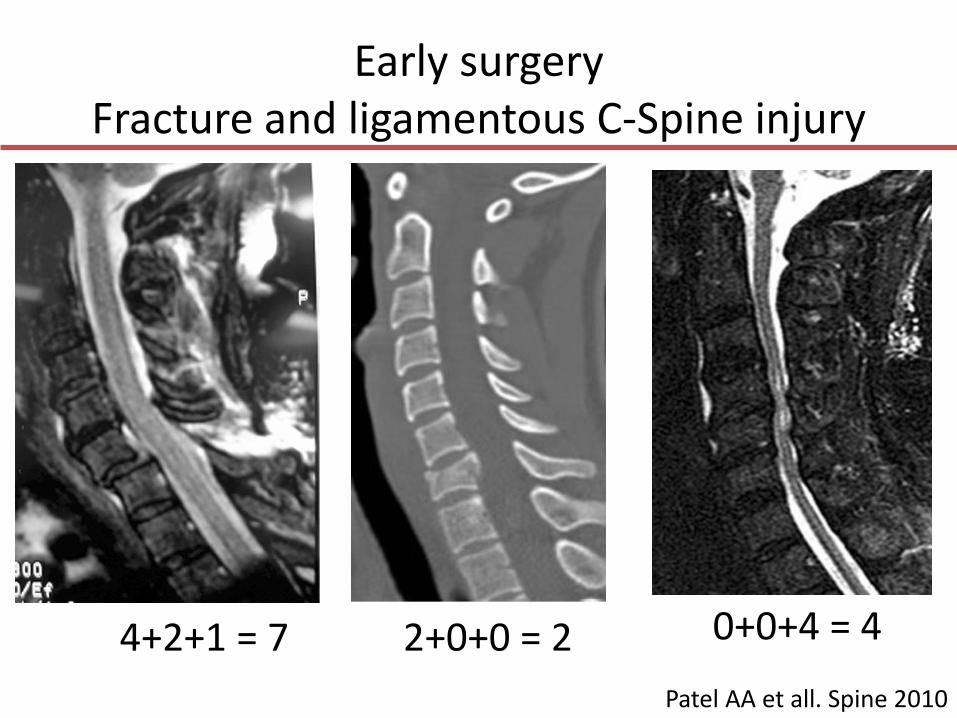
Early surgeryFracture and ligamentous C-Spine injury
SLIC (Subaxial Cervical Injury Classification)
Patel AA et all. Spine 2010
Early surgeryFracture and ligamentous C-Spine injury
SLIC (Subaxial Cervical Injruy Classification)– For morphology
• X-ray ve CT-scan is enough, MRI makes a serious contribution
– For discoligamantous complex• X-ray and CT are effective to demonstrate complete
rupture, MRI is effective in partially injured
– Neurological status• MRI effective
Finally 1-3 cons, 4 cons/surgery, >4 operation
Patel AA et all. Spine 2010
Early surgeryFracture and ligamentous C-Spine injury
Patel AA et all. Spine 2010
4+2+1 = 7 2+0+0 = 2 0+0+4 = 4

Early surgeryFracture and ligamentous TL-Spine injury
• AOSpine Classificatios System were based on:– Morphology of the fracture– Neurological status– Clinical modifiers
• The classical AO-Magerl system’s describe the observed mode of failure of the spinal column as a mechanicalconstruct.– Type A: Compression injuries with intact tension band.– Type B: Failure of the posterior or anterior tension band
through distraction. – Type C: Failure of all elements leading to dislocation,
translation, or displacement in any plane.
Schnake KJ AA et all. J Orthop Trauma 2017
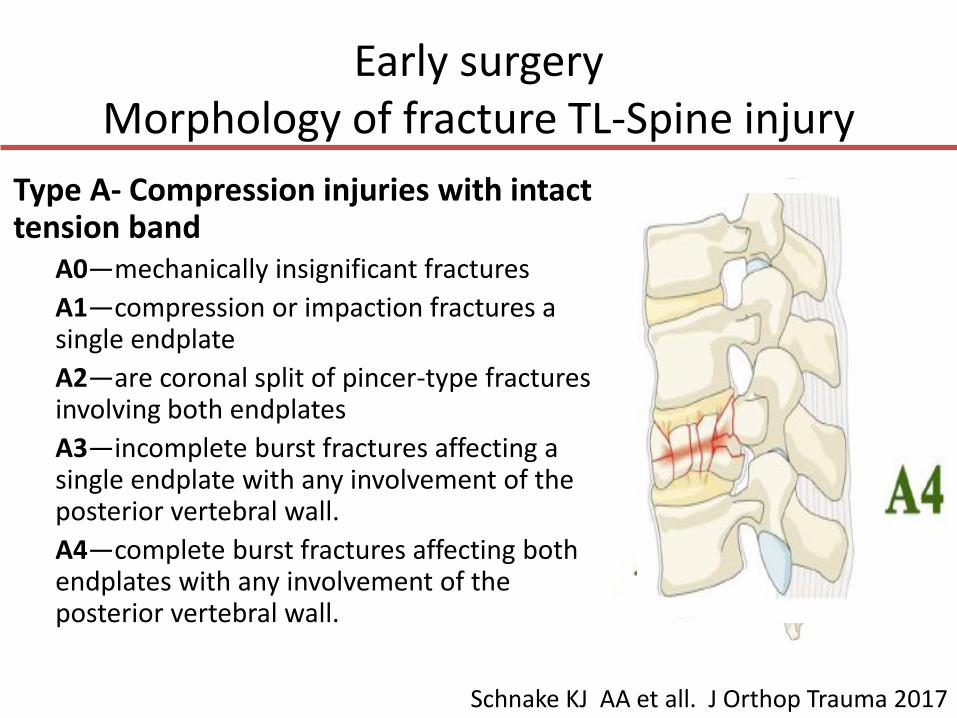
Early surgeryMorphology of fracture TL-Spine injury
Type A- Compression injuries with intact tension band
A0—mechanically insignificant fractures
A1—compression or impaction fractures a single endplate
A2—are coronal split of pincer-type fractures involving both endplates
A3—incomplete burst fractures affecting a single endplate with any involvement of the posterior vertebral wall.
A4—complete burst fractures affecting both endplates with any involvement of the posterior vertebral wall.
Schnake KJ AA et all. J Orthop Trauma 2017

Early surgeryMorphology of fracture TL-Spine injury
Type B: Failure of the posterior or anterior tension band through distraction
B1—monosegmental osseous failure of the posterior tension band extending into the vertebral body.
B2—disruption of the posterior tension band with or without osseousinvolvement.
B3—anterior tension band injury with disruption or separation of the anterior structures (bone/disc) with tethering
Schnake KJ AA et all. J Orthop Trauma 2017

Early surgeryMorphology of fracture TL-Spine injury
Type C Injuries: Displacement / Translational Injury
• No subdivision
• Highly unstable due to separation, displacement, or translation of 1 vertebral body (or elements) relative to another in any direction.
Schnake KJ AA et all. J Orthop Trauma 2017

Early surgeryMorphology of fracture TL-Spine injury
Reinhold M et all. Eur Spine 2013

Early surgeryMorphology of fracture TL-Spine injury
Reinhold M et all. Eur Spine 2013

Early surgeryMorphology of fracture TL-Spine injury
Reinhold M et all. Eur Spine 2013

Early surgeryConus medullaris or cauda equina syndrome
• Cauda equina syndrome (CES) - multiple 2nd motor neurons injury,
• Conus medullaris - 1st w/wo 2nd motor neuron injury– Neurological pathologies in lower extremity
• Tingling / numbness (saddle anesthesia)
• Weakness
– Urinary-bowel (red flag)• Incontinence
• Retention
– Leg pain
– Impotence
Dawadu ST et all. e-medicine 2017Hsu WK, Jenkins TJ. JAAOS 2017

Early surgeryConus medullaris or CESConus medullaris CES
Presentation Sudden and bilateral Gradual and bilateral
Reflexes Knee jerks preserved but ankle jerks affected
Both ankle and knee jerks affected
Radicular pain Less severe More severe
Low back pain More Less
Motor strength
Typically symmetric Asymmetric areflexic paraplegia
Sensorysymptoms
More localized to perianal area; symmetrical
More localized to saddle area; asymmetrical
Impotence Frequent Less frequent
Sphincterdysfunction
Urinary retention,atonic anal sphincter
Present late in course of disease

Early surgeryConus medullaris or CES
• Causes– Herniated nucleus pulposus (cause of 2-6% of cases of
cauda equina syndrome
– Lumbar spinal stenosis
– Inflammatory conditions (such as AS)
– Infections of the spinal canal
– Tumors/neoplasms
– Trauma to the lumbar spine,
Hsu WK, Jenkins TJ. JAAOS 2017

Early surgeryConus medullaris or CES
• Tx
– Specific treatment due to the primary cause
– The application of steroids is controversial, but doctors want to apply it
– If no relief of symptoms is achieved during 24h, immediate surgical decompression is necessary to minimize the chances of permanent neurologic injury
• Most surgeons suggest decompression as soon as possible(within 8h) the onset of symptoms if symptoms developsuddenly.
Hsu WK, Jenkins TJ. JAAOS 2017

Early surgeryConus medullaris or CES
• Morbidity rates are determined by the underlying etiology.
– Bilateral sciatica
– Complete perineal anesthesia
– The extent of perineal or saddle sensory deficit
– Females and patients with bowel dysfunction
have been reported to have a less favorable prognosis
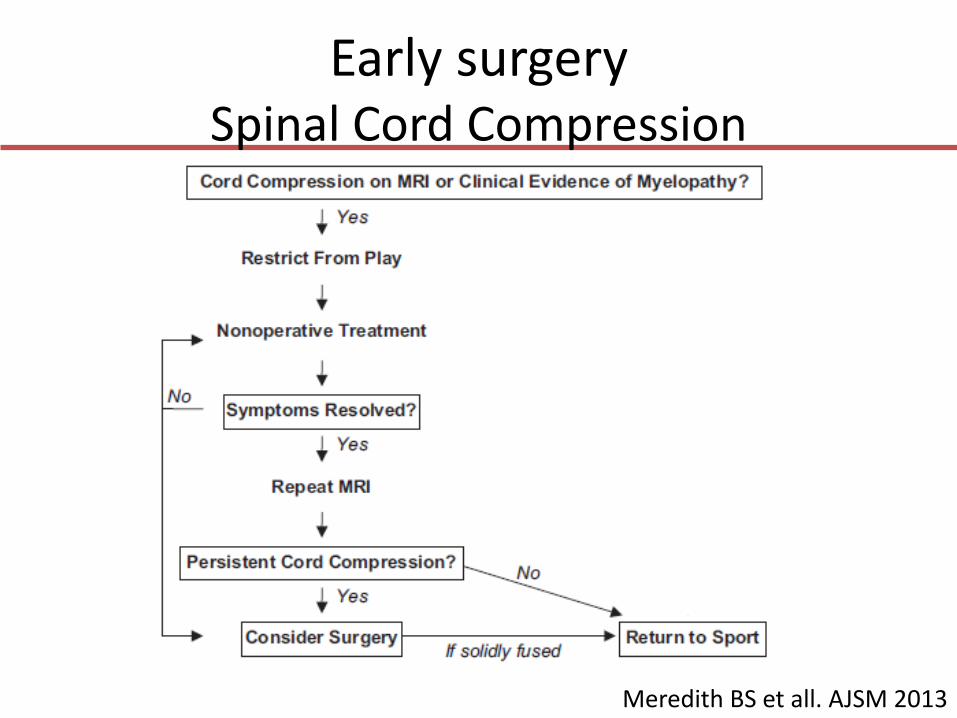
Early surgerySpinal Cord Compression
Meredith BS et all. AJSM 2013

Early surgerySpinal Cord Compression
Meredith BS et all. AJSM 2013

Early surgerySpinal Cord Compression and Cord Neuropraxia
• Spinal cord compression may disrupts motor, sensory and autonomic functions
• Compression due to– The bony structure
• Cervical spine– C3-7 less 13mm at lateral cervical on X-ray
• Thoracal spine– Stenosis is low, because the spinal cord / canal ratio ↓
– Soft tissue structure (to disc, facet or ligament)
• Spinal Cord Injury Without RadiologicalAbnormality (SCIWORA)
• Actually better prognosis with SCI+radiologic evidence
Eddy D et all. Clin J Sports Med 2005Huang P et all. Sports Health 2016

• Torg-Pavlov ratio;
– cervical canal /body of vertebra > 1
– < 0.8 stenosis (it is not always true)
Sensitivity 93% in American football
Positive Predictive Value 0.2%
Eddy D et all. Clin J Sports Med 2005Huang P et all. Sports Health 2016
Early surgery C-Spine stenosis and Cord Neuropraxia
siti

Cord Neuropraxia
• A Cervical cord neurapraxia is characterized by a transient neurologic deficit
– Fully recovers without any apparent structural damage
• If the player has cord neuropraxia
– Need to plain radiographs and MRI
• Stenosis, ligamentous injury, cord defects, or edema, RTP is contraindicated ??
Eddy D et all. Clin J Sports Med 2005Huang P et all. Sports Health 2016

Early surgeryCentral Cord Syndrome (CCS)
• Hyperextension injury
– Compression fracture
– Fracture dislocation
especially in a congenitally narrowed spinalcanal
• Axonal disruption in the lateral columnsat the level of the injury of the spinal cord
• Motor impairment results from thepattern of lamination of the corticospinaland spinothalamic tracts
Eddy D et all. Clin J Sports Med 2005Rackauskas Z et all. J Neurol Surg A 2016

Early surgeryCentral Cord Syndrome
Symptoms
– Greater impairment of motor function in the upper extremities than in the lower
– Bladder dysfunction
– A variable amount of sensory loss below thelevel of injury
– DTRs may initially be absent but will eventually return along with variable degrees of spasticity in affected muscles.
Eddy D et all. Clin J Sports Med 2005Rackauskas Z et all. J Neurol Surg A 2016

Early surgeryCentral Cord Syndrome
• Surgery is rarely indicated
– Because of the inherently favorable prognosis for patients with central cord syndrome
– Surgery;
• Compression of the spinal cord persists
• Gross spinal instability is present
• Neurologic deficits progress
• Guidelines (2016 by Wilson), early surgery be considered as a treatment option in adult patients with traumatic central cord syndrome.
Wilson JR et all. Neurosurgery 2016Rackauskas Z et all. J Neurol Surg A 2016

Surgery in the following periodHerniated Nuclues Pulposus (HNP)
• Although frequent in sports, there is notreatment guide. Surgery need if– Conservative tx not responding within 6w
– Progressive neurological deficits
– Pain interferes with social, work and home life
• The flagship study of the lumbar HNP in the athlete– Cons 82%
– Opere 81%
An additional 3.3 years to their careers
Hsu WK et all. Spine J. 2011Huang P et all. Sports Health 2016

Surgery in the following periodSurgery for huge HNP
• Patients with Lomber HNP
– In 46% of pateints, 75-100% resorption of HNPsSaal JA et all. Spine 1990
– In 48% of patients, 70% resorption of HNPs, and 15% of patients, 30% to 70% resorption of HNPs
Bozzao A et all Radiology 1992
Eddy D et all. Clin J Sports Med 2005

Surgery in the following periodSurgery for much pain in HNP
• Initial treatment of HNP is conservative, we haveto decrease the pain
• In 17 athlets, 37 were injected during 27 attacks– The injections were administered at an average of 4
days after the acute pain– RTP 89% after injection (24 of27)– Missed # training 2.8 (0-12), missed # match 0.6 (0-2)– 4 athletes needed 2nd injection for pain, 3 of them
went to surgery• The main underlying cause is sequestre disc and the
presence of weakness
Krych AJ et all. Med Sci Sports Exerc 2012

Surgery in the following periodSurgery for hyperintense site in spinal cord
• Is hyperintense site present on the cervicalcord an indication for surgery?
– Hyperintense in the cord can be completelyremedied by treatment
Temple ZJ et all. Neurosurg 2015Joaquim AF et all. Neurosurg Focus 2016

Possible surgery - early return? Lumbar HNP
Li Y, Hresko MT. Clin Sports Med 2012Kang DG ve ark. Clin Sports Med 2016

Surgery in the following periodSpondylolysis
• 3-6% in the general population, 80% asymptomatic
• 14% for young athletes
– The cause of 47% of young athletes with back pain
– It is high in some sports (diving, dancing, wrestling, shooting sports, rowing and gymnastics)
Li Y, Hresko MT. Clin Sports Med 2012Burgmeier RJ, Hsu WK. Asian J Sports Med. 2014
Huang P et all. Sports Health 2016

Surgery in the following periodSpondylolysis
• Tx;
– Conservative tx
• Rest and Boston / TLS Orthosis
• Use may be interrupted when the pain is reduced
– Surgery tx
• Do not respond to 6 months of conservative tx
• If go to lystesis
• Stubborn neurological deficit
Non-contact sports RTP at 6 months 62-66%
Li Y, Hresko MT. Clin Sports Med 2012Burgmeier RJ, Hsu WK. Asian J Sports Med. 2014
Huang P et all. Sports Health 2016

Surgery in the following periodStingers / Burners
• Brachial plexus and cervical root affected, – Sensory and / or motor-related burning,
tingling. Three mechanisms:
1. Nerve tension (as opposed to the head symptomatic side, shoulder and arm depressed on the symptomatic side)
2. Foraminal compression when the head is on the symptomatic side and in the extension
3. Direct trauma to the brachial plexus
Eddy D et all. Clin J Sports Med 2005Huang P et all. Sports Health 2016

Surgery in the following periodStingers / Burners
• Every year, half of college-level footballers suffer
– Repeat 20%
– Athlete should see a doctor who has had three problems at the same season
– More than half of those living in this condition have less than 1 day of RTP
• For conservative treatment-resistant conditions resulting from foraminal or HNP go to surgery
Eddy D et all. Clin J Sports Med 2005Huang P et all. Sports Health 2016

Take home message
• Maximum attention to athlete who are likely to suffer spinal injuries
– Midline C-spine tenderness, GCS <15, neurologic deficient, side rotation <45 °, falling type, distracting injury
• Emergent surgery
– Unstable fracture,
– Spinal cord compresion and CES
• No need emergent surgery
– HNP • Based on MRI or pain
• Early return to play
– Spondylolysis
– Central cord syndrome• Dependent to etiology

Thank you

Early surgeryFracture and ligamentous C-Spine injury
• 32y hockey player – Violent collision with another
player
• Neurolocial Exam is normal,
• X-ray and CT-scan showedisolated right C5-6 fascetfracture and instability
• PLL partially injured in MRI but no stenosis or cord injury
Molinari RW et all. Global Spine J 2016
• Tx: Cervical discectomy, fusion was applied, RTP after 6 months and continued for 3 years.

Early surgeryNeurlogical status TL-Spine injury
Neurological status :
N0—neurologically intact.
N1—transient neurological deficit, which is nolonger present by the time of clinical examination.
N2—symptoms or signs of radiculopathy.,
N3—incomplete spinal cord or cauda equina injury.
N4—complete spinal cord injury.
NX—neurology undetermined (due to intubation, sedation, intoxication, cerebral trauma etc).