specific treatment for the si joint - cook children's€¦ · tests to determine type of...
TRANSCRIPT

Specific treatment for the SI jointJenny Arey, PT, DPT, OCS, CMPT
SPORTS Physical TherapistCook Children’s Rehabilitation Services

ObjectivesO Describe the connection between the low back,
pelvis, and lower extremity that can have impairments that promote sacroiliac joint dysfunction
O Demonstrate postural assessments and cluster tests to determine type of sacroiliac dysfunction
O Perform an initial treatment technique for the most common sacroiliac dysfunction and differentiate when to refer to a physical therapist.

AssessmentO Mechanism of InjuryO Pain LocationO PostureO Special tests
O Primary Stress testsO Secondary Stress
tests
O Kinetic TestsO Positional TestsO Sacral positioningO Palpation

Posture
O Visual Observation/palpationO Plum Line
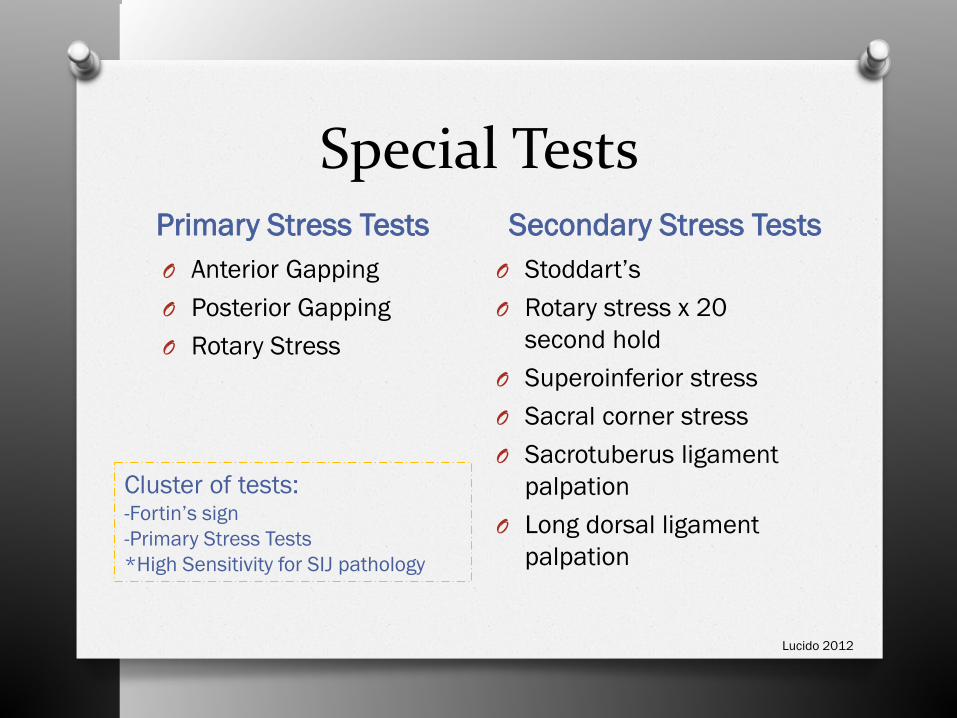
Special TestsPrimary Stress Tests Secondary Stress TestsO Anterior GappingO Posterior GappingO Rotary Stress
O Stoddart’sO Rotary stress x 20
second holdO Superoinferior stressO Sacral corner stressO Sacrotuberus ligament
palpationO Long dorsal ligament
palpation
Cluster of tests:-Fortin’s sign-Primary Stress Tests*High Sensitivity for SIJ pathology
Lucido 2012
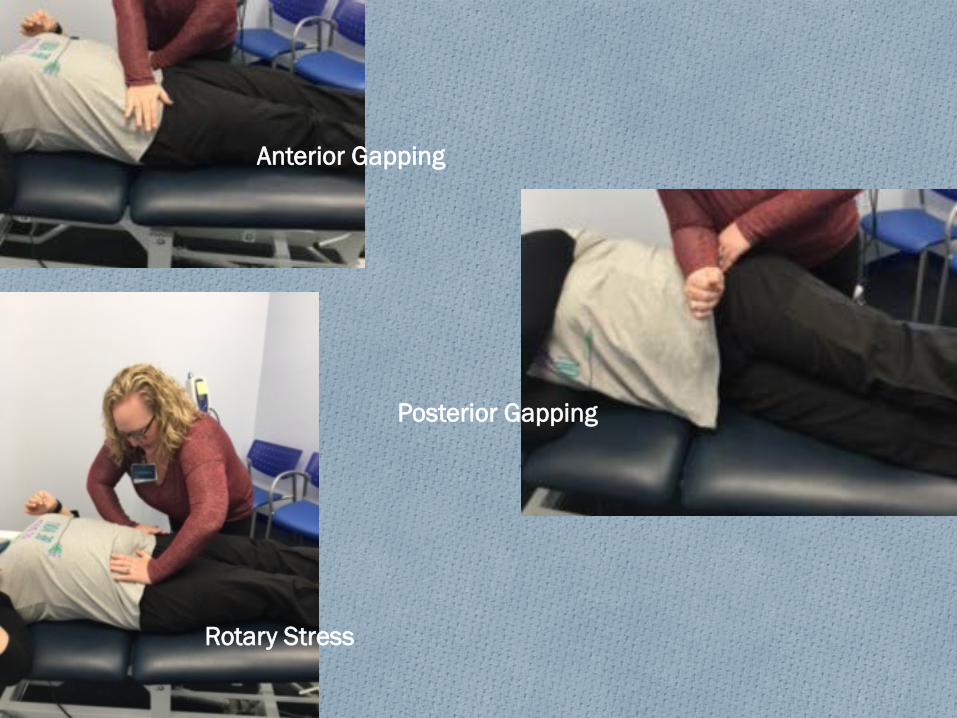
Anterior Gapping
Posterior Gapping
Rotary Stress

Stoddart’s
Superoinferior Stress
Sacral Corners
Long Dorsal Ligament Stress
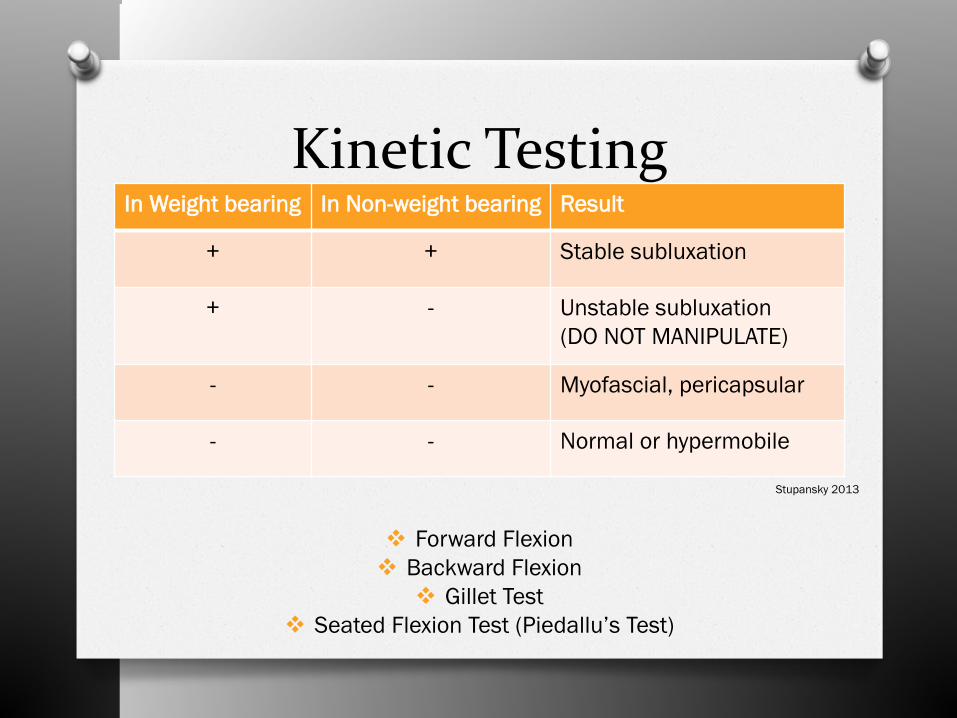
Kinetic TestingIn Weight bearing In Non-weight bearing Result
+ + Stable subluxation
+ - Unstable subluxation(DO NOT MANIPULATE)
- - Myofascial, pericapsular
- - Normal or hypermobile
Forward Flexion Backward Flexion Gillet Test
Seated Flexion Test (Piedallu’s Test)
Stupansky 2013

Positional TestsO Assessment of Landmarks
O StandingO Sitting flexedO SupineO Prone propped on elbows
O Supine to sitO FABERO Active SLRO Sacral torsion

Standing Extension
FABER
Forward Flexion
Gillet’s Test
Flexibility Assessment
Can’t forget the…Pubic Symphysis
O Supported by ligamentous structureO Impacted by instability
O Pain is Local, disabling, and aggravated by unilateral weight bearing
Clinical Test: Shearing one pubic cranially and other caudally
Stupansky 2013

Treatment Techniques

TreatmentO Refer to PhysicianO StrengtheningO Muscle Energy TechniquesO Joint Mobilization / ManipulationO Joint Stabilization

StrengtheningO Engage the coreO Dynamic lumbar stabilization progressionO Hip strengtheningO FlexibilityO Functional skillsO Balance control
*Focus on neutral pelvis/reduce drop*Coordination of core/pelvis strengthening*Incorporate pelvic floor

Engage the Core-Add Bridge-Dynamic Lumbar stabilization progression-Add abduction resistance at knees-Progress to planks

Hip strengthening

Piriformis stretchHamstring stretchHip flexor/ iliopsoas stretch
Dynamic warm upFoam Roller
Flexibility

Functional Skills Balance

Muscle Energy Technique(MET)
O Hip abduction/adduction (belt/ball)O Hip flexion/extension (push/pull)O Sacral rotation correction
O IliopsoasO Piriformis
O Prone hamstring isometric contraction for posterior innominate rotation
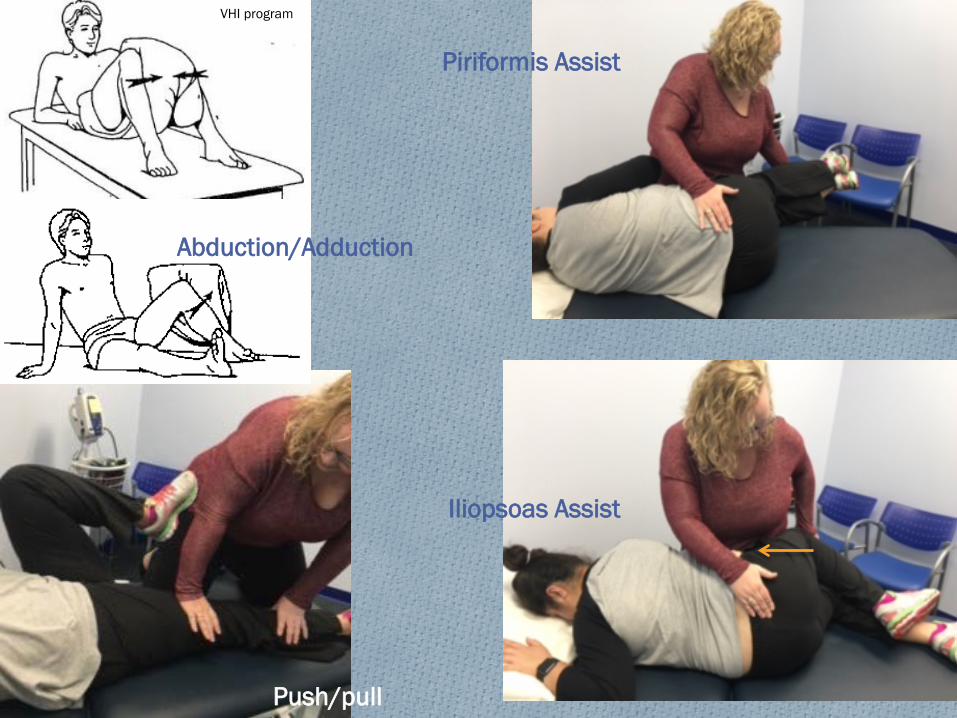
Abduction/Adduction
Push/pull
Piriformis Assist
Iliopsoas Assist
VHI program
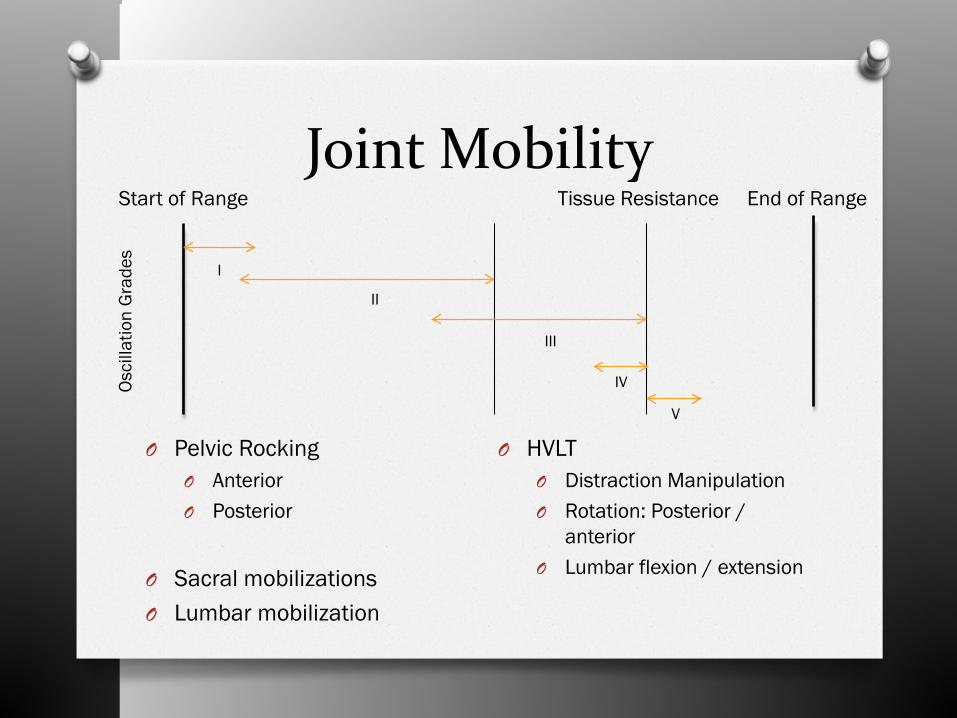
Joint Mobility
O Pelvic RockingO AnteriorO Posterior
O Sacral mobilizationsO Lumbar mobilization
O HVLTO Distraction ManipulationO Rotation: Posterior /
anteriorO Lumbar flexion / extension
Osci
llatio
n G
rade
s
I
II
III
IV
V
Tissue ResistanceStart of Range End of Range

MobilizationAnterior Rotation Posterior Rotation
Lucido 2012Stupansky 2013

Distraction Manipulation
Lucido 2012Stupansky 2013

Joint StabilizationO Force vs Form Closure
O Force: Stability from muscles supporting pelvisO Very vulnerable to shear forces
O Form: Stability from self locking of pelvisO Stabilization through exercise
O Stabilization through external support (belt)
Van Wingerden et al (2004)Arumugam et al (2012)
Other Treatment Techniques
O Shoe InsertsO Postural Re-educationO Functional Re-training

Case StudyO 16 year old Female with reports of low back pain
and hip pain ~ 10 months
O History of (R) L5 Spondylolysis with TLSO wear –at time of eval wearing 8 hours per day
O Radiographic evidence of spondy being stable, but not healing
O Competitive soccer player
PainO 3/10, achy, constantO Central low backO Worst: 7/10O Best: 0/10O Aggravating: sitting on hard chair, stair
ascend/descend, prolonged walkingO Relieving: rest, laying down, soft chairs

ImpairmentsO Tenderness to palpation (L) PSIS and ILA of sacrum, spasm
(L) lumbar paraspinalsO Posture:
O PSIS High on (L)O Rounded shouldersO Sacral sitting/posterior rotation
O ROMO Lumbar: flexion limited 10%, Extension : not testedO Hip and knee: WNLS bilaterally
O Flexibility:O Popliteal angle -10 degrees bilaterally
O Leg Length: (L) 85cm, (R) 84cmO Strength: Reduced hip abduction/extension, pain (L) low
back/hip with flexion/abduction resistance

Special TestsO Nutated sacrumO Primary Stress tests (+)O Secondary Stress Tests (+)O Supine to sit: (L) equal to short translationO Standing flexion: (L) positiveO Gillet’s test: (L) Positive, posterior rotation
O Shuttering in SIJ noted during movementO Repetitive flexion: no peripheralizationO Slump test: NegativeO Joint play:
O Hypomobility T8-12, L1-2

AssessmentO (L) sacroiliac joint anterior innominate
rotationO Reduced muscular stability in bilateral SIJO (L) hip abduction/extension weaknessO Core weakness

TreatmentO MET
O Hip abduction/adductionO Hip flexor on RightO Hip flexion/extension
O Mobilization/ManipulationO Posterior innominate mobilizations Grade III-IVO Thoracic posterior anterior mobs Grade III-IVO T12-L1 grade V with above and below flexion
lockingO StrengtheningO Stabilization Belt

ResultsO Discharged TLSO without back, hip, or LE
painO 1 occurrence of mild hypomobility in 6
weeks with ability to self correct and strengthen
O Progressed out of SIJ stabilization belt for all activities: Jog x 10-15 mins, soccer scrimmages

Questions?

ReferencesO Adhia D, Tumilty S, Mani R, Milosavljevic S, Bussey M. Can hip abduction and external rotation discriminate
sacroiliac joint pain? Manual Therapy 2016; 21. O Arumugam A, Milosavljevic S, Woodley S, Sole G. Effects of external pelvic compression on form closure,
force closure, and neuromotor control of the lumbopelvic spine – a systemic review. Musculoskeletal science and practice 2012; 17(4): 275-284.
O Asgaonkar B, Angal N. Effects of muscle energy technique (MET) versus MET with shoe insoles in pain and functional leg length discrepancy in patients with sacroiliac joint dysfunction. Indian Journal of Physiotherapy and Occupational Theapy 2017; 11(1): 90-5.
O Bernini, PM. Spine. Netter's Orthopaedics. By Walter B. Greene and Frank H. Netter. 1st ed. Philadelphia: Saunders, 2006. 252-81. Print
O Bhushan V, Sahay P, Alam S, Equebal A. Efficacy of maitland mobilization and lumbar segmental exercises as compared to lumbar segmental stabilization exercises in subjects with mechanical low back pain: A randomized controlled trial. Indian Journal of Physiotherapy and Occupational Thearpy 2016; 10(4): 113-8.
O Bogduk N. Pain provocation tests for the assessment of sacroiliac joint dysfunction. J Spinal Disord1999;12(4):357-8.
O Brolinson PG, Kozar AJ, Cibor G. Sacroiliac joint dysfunction in athletes. Current Sports Medicine Reports 2003: 47-56.
O Ditton M. Manual Therapy of the Spine: An Integrated Approach: McGraw-Hill; 2002.O Hoppenfeld, S, Hutton, R. Physical examination of the hip and pelvis. Physical Examination of the Spine
and Extremities. New York: Prentice Hall, 1976. 144+. O Lucido, M. Level II Lower Quadrant. NAIOMT 610 Certification Course. Texas Woman's University, Dallas.
2012. Lecture. O Magee, D. Orthopedic physical assessment. Canada: Saunders Elsevier; 5th Edition: 2008.O Panjabi MM, White AA. Biomechanics in the musculoskeletal system. New York: Churchill Livingstone;
2001.O Richardson C, Snijders C, Hides J, Damen L, Pas MS, Storm J. The relation between the transverse
abdominis muscles, sacroiliac joint mechanics, and low back pain. Spine 2002; 27(4):399-405.O Schwarzer AC, April CN, Bogduk N. The sacroiliac joint in chronic low back pain. Spine 1995;20(1):31-7.O Slipman CW, Patel RK, Zhang L, Vresilovic E, Lenrow D, Shin C, et al. Side of symptomatic annular tear and
site of low back pain: is there a connection? Spine 2001;28(6): 165-9.O Stoev I, Powers AK, Puglisi JA, Munro R, Leonard JR. Sacroiliac joint pain in the pediatric population. J
Neurosurg Pediatrics 2012; 9: 602-7.O Stupansky, Kathy. Level III Lower Quadrant. NAIOMT 710 Certification Course. Texas Woman's University,
Dallas. 2013. Lecture. O van Wingerden, J.P., Vleeming, A., Buyruk, H.M. et al. Eur Spine J (2004) 13: 199. O Zhao U, Qi L, Yang J, Zhu X, Yang C, Li M. Factors affecting pelvic rotation in idiopathic scoliosis: Analysis of
85 cases in a single center. Medicine 2016; 95: 46