sod1 misfolding and aggregation in als -...
TRANSCRIPT
SOD1 misfolding and aggregation in ALS
In the light of conformation-specific antibodies
Manuela Lehmann
Pharmacology and Clinical Neuroscience Umeå 2019
Cover: Primary astrocyte derived from the thoracic spinal cord of a SOD1A4V ALS patient embodying “peace” With this cover, I would like to express my sincere gratitude to all patients who donate for research. Without your generous contribution, preclinical reseach would not have the opportunity to sudy any disease in a human context and this thesis would have not been possible. Thank you!
This work is protected by the Swedish Copyright Legislation (Act 1960:729) Dissertation for PhD ISBN: 978-91-7855-032-6 ISSN: 0346-6612 Series No: 2021 Cover illustration: Image taken by Anna-Lena Bolender Figure design: Ida Åberg Electronic version available at: http://umu.diva-portal.org/ Printed by: UmU Print Service, Umeå university Umeå, Sweden 2019

To the memory of my father
i
Table of Contents Abstract ii
Enkelsammanfattningpåsvenska iv
Abbreviations vi
Listofpublications vii
Author’scontribution viii
Introduction 1AmyotrophicLateralSclerosis 1Superoxidedismutase 5SOD1inALS 8Antibodies 16Immunotherapy 24
Aimsofthisthesis 27
MaterialsandMethods 28Humanmaterials 28Cellcultures 28SOD1transgenicmice 31AntibodiesagainstmisfoldedSOD1 31Immunocapture 32Immunohistochemistry 32PassiveImmunotherapy 33
Results 34PaperI 34PaperII 37PaperIII 41PaperIV 43
Discussion 48
Conclusions 53
Acknowledgement 54
References 58
ii
Abstract
Mutations in the superoxide dismutase 1 (SOD1) gene are linked to the progressive neurodegenerative disease amyotrophic lateral sclerosis (ALS). ALS-associated mutations affect the stability of the SOD1 protein and promote its unfolding. As a consequence, disordered SOD1 species can misfold and accumulate into insoluble aggregates. Cytoplasmic inclusions containing misfolded SOD1 are a hallmark of ALS pathology in patients as well as transgenic mouse models. However, it remains unclear, which SOD1 species are pathogenic and how they arise and contribute to the disease.
The aim of this thesis was to use antibodies as tools to study the role of disordered and aggregated SOD1 species in ALS. These antibodies recognize epitopes exposed in disordered SOD1 species and hence, discriminate between natively folded SOD1 and the disordered or misfolded protein.
SOD1 is expressed in all cell types, but aggregates of misfolded SOD1 are predominantly found in motor neurons and associated glial cells in the spinal cord of ALS patients. To understand why misfolded SOD1 targets the motor system, we used ELISA and immunocapture methods to quantify soluble SOD1 species in patient-derived cell models of ALS. The highest levels of soluble disordered SOD1 were detected in induced pluripotent stem cell (iPSC)-derived motor neuron and astrocytes cultures (MNACs) compared to fibroblasts, iPSCs and sensory neuron cultures. These results suggest that the selective vulnerability of motor areas to SOD1-ALS could derive from an enhanced burden of disordered SOD1.
To understand factors that might promote SOD1 unfolding, we focussed on the disulfide bond that is required for the stability of natively folded SOD1. Formation of the bond is oxygen-dependent and reduction of the bond promotes SOD1 unfolding. We studied the stability of SOD1 in patient-derived cells exposed to lowered oxygen tensions. This induced increases in disulfide-reduced, disordered mutant and wild-type SOD1. The response was time- and concentration-dependent and more pronounced in MNACs, where even increased aggregation of mutant SOD1 was observed. These results are consistent with the enhanced vulnerability of the motor system in ALS and suggest that conditions causing impaired oxygen perfusion could contribute to the initiation and progression of the disease.
Inclusions containing aggregated misfolded wild-type SOD1 have been found in sporadic ALS (sALS) patients without SOD1 mutations and those carrying mutations in genes other than SOD1. However, other groups have reported contrasting results and the contribution of misfolded wild-type SOD1 to ALS pathology is controversial. Guidelines for preservation, storage and analysis of tissues under standardized conditions would facilitate the comparison of results between different laboratories.

iii
We established an optimized immunohistochemistry protocol to detect misfolded wild-type SOD1 in paraffin-embedded spinal cord samples from sALS patients. We also developed a method to immunocapture disordered SOD1 from frozen post-mortem tissue. High, but variable, levels of disordered SOD1 were detected in spinal cords from sALS patients. Our data support a possible pathological role of misfolded wild-type SOD1 in sALS.
Recent evidence suggests that SOD1 aggregates can induce templated aggregation of disordered SOD1 and spread from cell-to-cell via a prion-like mechanism. To test if antibodies could block this process in vivo, we conducted an immunotherapy study in a model of prion-like spread, where SOD1 aggregate seeds are inoculated into the lumbar spinal cord of SOD1G85R transgenic mice and lead to accelerated disease onset and progression. Novel monoclonal antibodies (mAb) against disordered domains of SOD1 aggregates were developed and validated for their reactivity to disordered and aggregated SOD1 species in vitro and in vivo. Immunotherapy using a mAb against the C-terminal end of SOD1 attenuated the onset and progression of prion-like SOD1 spread. However, no effect was seen on onset, duration or progression of the underlying disease. This suggests that, under the conditions tested, immunotherapy against disordered domains of SOD1 does not affect intracellular aggregation and additional strategies might be needed to reduce intracellular accumulation of misfolded SOD1 aggregation.
In conclusion, we show that conformation-specific antibodies are powerful tools to investigate disordered and potentially pathogenic species of SOD1 in various biochemical, cellular and in vivo contexts. The development of the novel immunocapture strategy could facilitate future research on characterizing SOD1 aggregates from mouse tissues, patient-derived cells or post-mortem tissues with the goal of determining their role in ALS disease pathogenesis.
iv
Enkel sammanfattning på svenska
SOD1 felveckning och aggregering i ALS - i fokus för strukturspecifika antikroppar Mutationer i superoxiddismutas 1 (SOD1) genen kan orsaka den progressiva neurodegenerativa sjukdomen Amyotrofisk lateralskleros (ALS). ALS-associerade mutationer påverkar stabiliteten hos SOD1-proteinet och gör att det förlorar sin naturliga struktur. Det ostrukturerade muterade proteinet kan sedan fel-veckas och aggregera. Ansamlingar av aggregerat SOD1 protein i drabbade motoriska nervceller är ett välkänt fenomen, både hos patienter samt i transgena musmodeller för SOD1-ALS. Syftet med denna avhandling var att utveckla och karaktärisera nya antikroppar och metoder för att studera hur, och varför dessa sjukdomsassocierade SOD1 aggregat bildas, ansamlas och sprider sig vid ALS. Vårt slutgiltiga mål var att identifiera en antikropp som kunde användas för immunterapibehandling för att bromsa sjukdomen. SOD1 protein uttrycks i kroppens alla celltyper. Varför är det då specifikt ryggmärgens, och hjärnans motoriska nervceller och de omkringliggande stödjecellerna (astrocyter) som påverkas vid ALS, och bara där som aggregat av felveckat SOD1 bildas? För att förstå varför muterat SOD1 är specifikt farligt för motorsystemet odlade vi celler från ALS patienter i vårt laboratorium, och använde biokemiska metoder för att mäta mängden lösligt ostrukturerat SOD1 protein i olika celltyper. De högsta nivåerna av lösligt ostrukturerat SOD1 detekterades i celler som omprogrammerats till pluripotenta stamceller (iPSC), och sedan differentierats ut till motoriska nervceller och astrocyter. Vi jämförde med fibroblaster, iPSCs och iPSCs deriverade sensoriska nervceller. Våra resultat tyder på att den selektiva sårbarheten hos motorsystemet vid SOD1-ALS skulle kunna härledas till en ökad ansamling av ostrukturerat SOD1 protein i motoriska nervceller och astrocyter. Vilka mijöfaktorer skulle kunna bidra till att SOD1 tappar sin naturliga struktur och börjar bilda aggregat? Här fokuserade vi på en disulfidbrygga som stärker stabiliteten hos normal-veckat SOD1 protein. Disulfidbryggan är syreberoende och reduktion av denna leder till ökad sannolikhet att SOD1 proteinet tappar sin normala struktur, kan fel-veckas och bilda aggregat. Vi studerade hur låg syrehalt påverkade disulfidbryggan och mängden ostrukturerat SOD1 i celler från patienter. Låg syrenivå ledde till reducerad disulfidbindning, och ökad mängd ostrukturerat SOD1 protein. Både celler med ALS-länkade mutationer i SOD1, och med normalt vildtypsprotein, påverkades av lågt syre, och effekten var tid- och koncentrationsberoende. Motoriska nervceller och astrocyter påverkades mest, och i dessa celler ledde låg syrehalt även till aggregering av mutant SOD1. Dessa resultat bidrar till att förklara motorsystemets sårbarhet
v
vid ALS, och föreslår att tillstånd som orsakar nedsatt syresättning i nervsystemet kan bidra till sjukdomsutveckling. Flera studier har rapporterat att det även bildas aggregat av felveckat vildtyps-SOD1 i vävnad från patienter med sporadisk ALS (sALS), och patienter med mutation i andra ALS-länkade gener, utan SOD1-mutationer. Andra studier har dock rapporterat motsatt resultat, så både förekomst och betydelse av aggregerat vildtyps-SOD1 är kontroversiellt. Vi har sammanställt gemensamma riktlinjer för fixering, lagring och analysprotokoll som skulle kunna underlätta jämförelsen av resultat från olika laboratorier. Vi beskriver i detalj ett etablerat, optimerat immunohistokemiprotokoll för att färga aggregerat vildtyps-SOD1 i vävnadssnitt från från sALS-patienter. Vi har också utvecklat en antikroppsbaserad metod för att detektera sjukdomsassocierat SOD1 i homogeniserad frusen ryggmärgsvävnad. Höga, men varierande, nivåer av ostrukturerat och felveckat SOD1 detekterades i vävnad från sALS-patienter. Våra resultat stöder hypotesen att felveckat vildtyps-SOD1 kan bidra till sjukdomsutveckling hos ALS-patienter utan SOD1 mutation. Med mål att utveckla immunterapi mot SOD1-ALS producerade, och karaktäriserade vi monoklonala antikroppar som specifikt binder sjukdoms-associerat SOD1 protein. Tidigare studier tyder på att SOD1 aggregat kan få ostrukturerat SOD1 protein att börja aggregera och spridas från cell till cell via en prion-liknande mekanism. Vi använde en musmodell för ALS, som bygger på att en liten mängd aggregerat SOD1 injiceras i ryggmärgen hos transgena möss och leder till prion-liknande spridning av SOD1 aggregat, och progressiv ALS-liknande förlamning. Immunoterapibehandling med hjälp av en av våra monoklonala antikroppar som binder den C-terminala änden av SOD1 kunde binda SOD1 aggregat in vivo, dämpade SOD1-aggregatens aktivitet och förlängde mössens överlevnad. Immunterapi behandling kunde däremot inte hämma start, progression eller förlänga överlevnad hos transgena möss som uttrycker muterat humant SOD1 och utvecklar ALS-liknande förlamningssjukdom. Våra resultat tyder på att antikroppsbaserad behandling kan bromsa extracellulär spridning av SOD1 aggregat men har svårt att komma in i motoriska nervceller och förhindra intracellulär SOD1 aggregering. Sammanfattningsvis visar vi att strukturspecifika antikroppar är kraftfulla verktyg för att undersöka ostrukturerat och patogena arter av SOD1 protein i olika biokemiska, cellulära och in vivo studier. Utvecklingen av nya antikroppar och metoder kan underlätta ny forskning om de cellulära mekanismer som påverkar bildningen av patogena arter av SOD1 aggregat och nervcells död vid ALS.
vi
Abbreviations
AD Alzheimer’s disease ALS amyotrophic lateral sclerosis BBB blood brain barrier C9ORF72 chromosome 9 open reading frame 72 CCS copper chaperone for SOD ChAT choline acetyltransferase CNS central nervous system CSF cerebrospinal fluid CST corticospinal tract DNA deoxyribonucleic acid DMEM Dulbecco's Modified Eagle Medium EGF epidermal growth factor EDTA Ethylenediaminetetraacetic acid ER endoplasmatic reticulum ESC embryonic stem cells FBS fetal bovine serum FGF-2 fibroblast growth factor 2 FTD frontotemporal dementia FUS FUS RNA binding protein GFAP glial fibrillary acidic protein GlutaMax L-alanyl-L-glutamine HSP heat shock protein iPSC induced pluripotent stem cell iPSC-Astros iPSC-derived astrocytes LMN lower motor neurons MNAC iPSC mixed motor neuron/astrocyte cultures PAGE polyacrylamide gel electrophoresis PBS phosphate buffered saline PD Parkinson’s disease PDGF-AB Platelet-derived growth factor AB RA retonic acid RNA ribonucleic acid SNC sensory neurons SOD superoxide dismutase TDP-43 TAR DNA binding protein UMN upper motor neurons WT wild type
vii
List of publications
I. E. Forsgren, M. Lehmann, M. Weygandt Mathis, I. Keskin, P. Zetterström, J. Nijssen, E. R. Lowry, A. Garcia, J. Sandoe, E. Hedlund, H. Wichterle, Ch. E. Henderson, K. Eggan, E. Kiskinis, P. M. Andersen, S. L. Marklund and J. D. Gilthorpe “Enhanced protein misfolding in patient-derived models of amyotrophic lateral sclerosis” Manuscript
II. I. Keskin, E. Forsgren, M. Lehmann, P. M. Andersen, T. Brännström, D. J. Lange, M. Synofzik, U. Nordström, P. Zetterström, S. L. Marklund
and J. D. Gilthorpe “The molecular pathogenesis of superoxide dismutase 1-linked ALS is promoted by low oxygen tension” Manuscript submitted to Acta Neuropathologica
III. B. Paré, M. Lehmann, M. Beaudin, U. Nordström, S. Saikali, J.-P. Julien, J. D. Gilthorpe, S. L. Marklund, N. R. Cashman, P. M. Andersen, K. Forsberg, N. Dupré, P. Gould, T. Brännström and F. Gros-Louis “Misfolded SOD1 pathology in sporadic ALS” Sci Rep. (2018) 8 (1): 14223
IV. M. Lehmann, M. Marklund, A.-L. Bolender, E.E. Bidhendi, A. Olofsson, P. M. Andersen, T. Brännström, S. Marklund, J. D. Gilthorpe, U. Nordström “An aggregate-selective monoclonal antibody attenuates seeded but not spontaneously evolving SOD1 aggregation in ALS model mice” Manuscript
Paper III is reprinted in this thesis with the kind permission from the publishers.
viii
Author’s contribution
I. The author took part in the practical work by maintaining cells,
differentiating iPSCs and performing western blots. The author was responsible for the acquisition, analysis and representation of the immunocapture data. Prior to that, the author carried out immunocapture tests to identify and overcome obstacles. The author was involved in revisions of the manuscript.
II. The author was responsible for the practical work involving immunocapture experiments and primary astrocyte cultures. The author generated the cultures from post-mortem tissue as well as executed and analysed experiments with these cells. The author produced figures for the obtained data and contributed to revisions of the manuscript.
III. The author was involved in the planning and design of the study. The author was responsible for the execution, analysis and representation of the immunocapture experiments. The author was involved in writing and revisions of the manuscript.
IV. The author was significantly involved in the planning and design of the study. The author carried out the in vivo experiments and was greatly involved in the acquisition and analysis of the in vitro experiments including immunohistochemistry, dot blots, western blots and ELISAs. The author generated all the figures and was involved in writing the manuscript.

1
Introduction
Amyotrophic Lateral Sclerosis Amyotrophic lateral sclerosis (ALS) belongs to a group of rare, but severe neurodegenerative disorders commonly referred to as motor neuron diseases. The first reports of this fatal neurological syndrome appeared in the early 19th century. Affected patients showed symptoms of limb weakness and muscle atrophy with a focal onset that spread progressively to anatomically related areas 1,2. The French neurologist Jean-Martin Charcot introduced the name ALS in 1874 to describe his observations of the disease 3. He was the first to establish a relationship between clinical symptoms and the pathology of the disease. He noted the characteristic degeneration of motor neurons in the motor cortex, brainstem and spinal cord. Based on these findings, he concluded that the chronic progressive paralysis resulted from lesions within the lateral column of the spinal cord 4. The descriptive name “ALS” provides an accurate representation of these neuropathological hallmarks. The term “amyotrophic” is composed of the Greek words for muscle (myos) and nutrition (trophos). Hence, amyotrophic refers to the loss of muscle tissue due to a deficiency in supporting trophic signals caused by the depletion of connected motor neurons. The term “lateral sclerosis” describes the connective tissue of the spinal cord that replaces degenerated corticospinal axons 1. Despite numerous genetic and molecular discoveries that have facilitated a clearer understanding of the disease process, the original description of clinical and pathological findings remained nearly unaltered 4. Clinical Characteristics The clinical manifestation of ALS is very heterogeneous and goes far beyond standard parameters such as age and site of onset (reviewed in 5). Despite different clinical patterns, the progressive nature of the disease causes nearly all motor systems to become affected. Only a few motor areas are relatively spared, including the oculomotor pathways and motor neurons in the Onuf’s nuclei involved in controlling eye movements and sphincter control, respectively 5. In classical ALS, symptoms start with muscle weakness in one foot or hand and subsequently spread to the contralateral side. The symptoms contiguously progress and eventually affect all extremities 6,7. Patients may also experience cramps and involuntary muscle twitching as signs of lower motor neuron degeneration. Signs of upper motor neuron degeneration involve hyperreflexia, spasticity and the pathological extension of the big toe, also known as Babinski sign 8,9.

2
The majority of ALS patients eventually die from respiratory complications due to the paralysis of the motor system that controls breathing 10,11. In addition to spinal onset, a subset of ALS patients initially develops abnormal speech or swallowing abilities before the typical limb weakness appear. This form of ALS involves the degeneration of motor neurons in the bulbar nuclei of the brain stem and is therefore known as bulbar onset ALS. It generally presents at an older age and is associated with a more rapid disease progression compared to classical ALS 12-14. ALS shares clinical and pathological characteristics with various other adult-onset degenerative diseases. As the disease progresses a large proportion of ALS patients develop cognitive deficits of variable degrees, which cause impulsivity, impaired judgement, and a general deterioration in the ability to execute daily tasks 15. These clinical features closely resemble the neurodegenerative disease fronto-temporal dementia (FTD) that is characterized by the loss of cortical neurons in the frontal and temporal lobes of the brain. Similar structural abnormalities and fronto-temporal atrophy have also been identified in ALS patients, further supporting an overlap between these two diseases 16. Epidemiology The worldwide incidence of ALS is approximately 2 new cases per year in every 100 000 people 17 with an estimated total number of 5 living cases per 100 000 18,19. Several studies reported an increased incidence and prevalence with age, reaching a plateau between the ages of 65–70 years 19-24. Due to the rising life expectancy of the global population, the number of ALS cases is predicted to increase in the coming years 25.
ALS affects people most commonly in their midlife, with an average onset between the ages of 45-60 18. Patients with juvenile ALS develop symptoms in their late teenage or early adult years 26 and often involve an inherited family trait 27,28. Men have a slightly higher risk of developing ALS than women with a lifetime risk of 1:450 and 1:350, respectively 29. The average life expectancy after symptom onset is around 3 years, depending on the rate of disease progression. There are, however, reports of patients dying within months after onset and others having survived for more than a decade 13. Neuropathology Examination of post mortem tissues from ALS patients reveals several morphological changes. The key histological findings are the degeneration of upper motor neurons in the motor cortex and brainstem as well as the loss of lower motor neurons in the brainstem motor nuclei and anterior horns of the spinal cord. The remaining motor neurons display axonal abnormalities, such as a swollen soma and a disorganized cytoskeleton 30.
3
The degeneration of motor neurons is further accompanied by muscle atrophy, scarring of the spinal cord and neuroinflammatory processes. Activated astrocytes, microglia and oligodendroglia cells are commonly observed within the degenerating spinal cord 31,32.
Cytoplasmic protein inclusions are common pathological features of the normal ageing brain. However, certain inclusions found in motor areas are associated with ALS 33,34 and some of the most commonly occuring ones are described below. Bunina bodies Bunina bodies are small, dense, and granular inclusions found in the cytoplasm of degenerating motor neurons. They contain cystatin C and transferrin and can be visualized by hematoxilin and eosin staining (HES). While it is not clear from where they originate, or what their significance is, Bunina bodies are commonly found in both familial and sporadic ALS patients upon autopsy 35,36. Corpora amylacea Corpora amylacea are small, spherical translucent structures composed of polysaccharides and numerous proteins involved in aging and stress. They are derived from either glia or neuronal cells. Although corpora amylacea are typically found in the central nervous system (CNS) of normal aging individuals, they have also been observed in several neurodegenerative diseases including ALS. While showing morphological similarities, they differ in size, biochemical and chemical composition 37,38. Ubiquitinylated inclusions Ubiquitin-positive inclusions are common features in neurodegenerative diseases including ALS. They are identified using anti-ubiquitin antibodies and are composed of aggregated proteins. In ALS, they are typically found in degenerating motor neurons and occasionally in surrounding glia cells in the spinal cord and brain stem 39. The main protein in these inclusions has been identified as transactive response DNA-binding protein 43 (TDP-43) 40. Based on their morphology, ubiquitinylated inclusions can be classified into Lewy body-like hyaline inclusions and skein-like inclusions 33,41. Lewy body-like hyaline inclusions Lewy body-like hyaline inclusions mimic Lewy bodies found in Parkinson’s disease. They are composed of condensed filamentous aggregates, but unlike Lewy bodies, do not contain α-synuclein 42. These inclusions are typically found in the cytoplasm of motor neurons of familial ALS patients. In ALS patients carrying a mutation in superoxide dismutase-1 (SOD1) and sporadic ALS cases, these inclusions stain positively for SOD1 43,44.

4
Skein-like inclusions Skein-like inclusions are filamentous structures found in the cytoplasm of motor neurons. They stain positive for TDP-43, p62 and SOD1, but not cystatin C or α-synuclein 39-41,45. Skein-like inclusions are observed in both familial and sporadic ALS 46,47. Etiology ALS patients are classified as either sporadic ALS (sALS) or familial ALS (fALS) with the hereditary cases accounting for 1-13 %, depending on population. The vast majority of patients develop the disease without a known genetic cause 48. However, incomplete disease penetrance, misdiagnosis, and inadequate family history result in frequent misclassification of sALS patients. Hence, the numbers reported for fALS cases are likely to be underestimated 49.
Many epidemiological studies have been conducted to identify non-genetic risk factors for ALS. Suggested risk factors are environmental factors such as metal exposure, viruses and pesticides 50,51, occupational factors, medical conditions, and lifestyle such as intense physical activity 52-54. Despite the wealth of studies, it has been difficult to conclusively link any of these factors to ALS 50. The only confirmed risk factors are a family history, older age and male sex 55. Ageing is a common risk factor for many diseases and numerous complex changes occur during the ageing process. For instance, there is a gradual decline in immune response accompanied with a gradual increase in pro-inflammatory cytokine release 56.
ALS is commonly inherited in an autosomal dominant fashion in patients with a familial history. The disease can also be passed on via alterations on the X-chromosome or in an autosomal recessive manner 49. Mutations in 37 genes have been implicated in ALS pathogenesis and the most frequently linked genes include those encoding chromosome 9 open reading frame 72 (C9orf72), fused in sarcoma RNA-binding protein (FUS), TDP-43, and SOD1 18. Chromosome 9 open reading frame 72 A pathological, non-coding expansion of a GGGGCC hexanucleotide repeat (>25-30 repeats) in C9ORF72 can be found in 40% of fALS and 7% of sALS patients 57,58. Hence, the non-coding expansion is the most common genetic cause of ALS and ALS/FTD 59,60. Although functions of the C9orf72 protein remain largely unknown, it has been reported that the protein is involved in vesicle trafficking 61,62. Fused in sarcoma RNA-binding protein Mutations in FUS have been identified in 4% of fALS patients and less than 1% of sALS cases 63. FUS is ubiquitously expressed and involved in mRNA splicing and processing as well as in DNA repair and transcription 64-66. It is further an
5
essential element of granule stress complexes, which form under cellular stress conditions such as oxidative stress. These granules contain proteins and RNA that are not required for the stress response and thus, conveying a protective mechanism 67. Transactive response DNA-binding protein Mutations in TDP-43 are associated with 1-5% of fALS and less than 2 % of sALS patients 68. Native TDP-43 protein is primarily located in the nucleus where it binds to RNA and DNA and plays a critical role in regulating transcription and alternative splicing. Similar to FUS, TDP-43 is an important component of the cytoplasmic stress granule response 69. Superoxide dismutase-1 The discovery of mutations in the gene superoxide dismutase-1 (SOD1) started the era of molecular discoveries in ALS and due to its central importance for this thesis, SOD1 will be discussed in section “superoxide dismutase” in more details. Despite intensive research, the exact mechanisms responsible for the neuropathology of ALS remain unsolved. Several cellular pathways have been proposed based on the function of ALS-associated proteins: (1) impaired RNA stability, function and metabolism; (2) altered DNA repair; (3) disturbed proteostasis including accumulation of aggregates and impaired protein degradation pathways; and (4) mitochondrial dysfunction and oxidative stress. Other proposed disease mechanisms include neuroinflammation, endoplasmic reticulum stress, excitotoxicity as well as defective axonal and vesicle transport. Detailed descriptions of these pathways is beyond the scope of this thesis, but have been extensively reviewed elsewhere 70,71.
Superoxide dismutase SOD enzymes are the main cellular defence mechanism against superoxide anions, a by-product of aerobic energy production 72. Although superoxide anions are only moderately reactive by themselves, they can participate in several reactions that generate a variety of reactive oxygen and nitrogen species such as hydroxyl radicals and peroxynitrites 73,74. These highly reactive metabolites can readily damage proteins, nucleic acids and even membranes 75. SODs can prevent the formation of these metabolites by catalysing the conversion of superoxide anion to oxygen and hydrogen peroxide in a two-step reaction. These ancient and universal antioxidant enzymes can be found in many organisms that live in the presence of oxygen, including bacteria, fungi, plants and animals. In humans, three different SOD isoenzymes (SOD1, SOD2,

6
SOD3) have been identified, each encoded by different genes and localized at distinct subcellular locations 76. However, all isoforms incorporate metal ions within their active site and catalyse the same net reaction. The following reactions exemplify the chain of events for SOD1 as a catalyst:
1.) SOD1-Cu2+ + O2.- à SOD1-Cu+ + O2 (reduction of copper)
2.) SOD1-Cu+ + O2.- à SOD1-Cu2+ + H2O2 (oxidation of copper)
O2.- + O2.- à O2 + H2O2 (net reaction) SOD1 is primarily a cytosolic enzyme, but has also been found in the nucleus, peroxisomes, lysosomes, and the mitochondrial intermembrane space 77,78. It is a homodimer that uses copper ions in its active sites to exert its dismutase activity 79.
SOD2 is located in the mitochondrial matrix and thus, the primary defence against superoxide anions produced by the electron transport chain 80,81. The SOD2 protein is a 96-kDa homotetramer that uses manganese ions to catalyse the reaction. It can be distinguished from SOD1 and SOD3 by its relative resistance to cyanide 76. SOD2 knockout experiments in mice resulted in neonatal mortality, highlighting the importance of superoxide metabolism in mitochondria 82.
The SOD3 protein is an extracellular enzyme anchored to the extracellular matrix or cell surface via its heparin-binding domain 76. It can also be found circulating in plasma, ascites, and cerebrospinal fluid. SOD3 is a 135-kDa homotetramer and, as SOD1, uses copper as metal cofactor 83. SOD1 The human SOD1 gene is located on chromosome 21 and comprises 5 exons separated by four introns. The mature, native SOD1 protein is assembled from two identical subunits that form a 32-kDa homodimer 84. Each monomer consists of 153 amino acids and contains three important features; a stabilizing zinc ion, a copper ion required for enzymatic activity, and the intra-subunit disulphide bond 79.
7
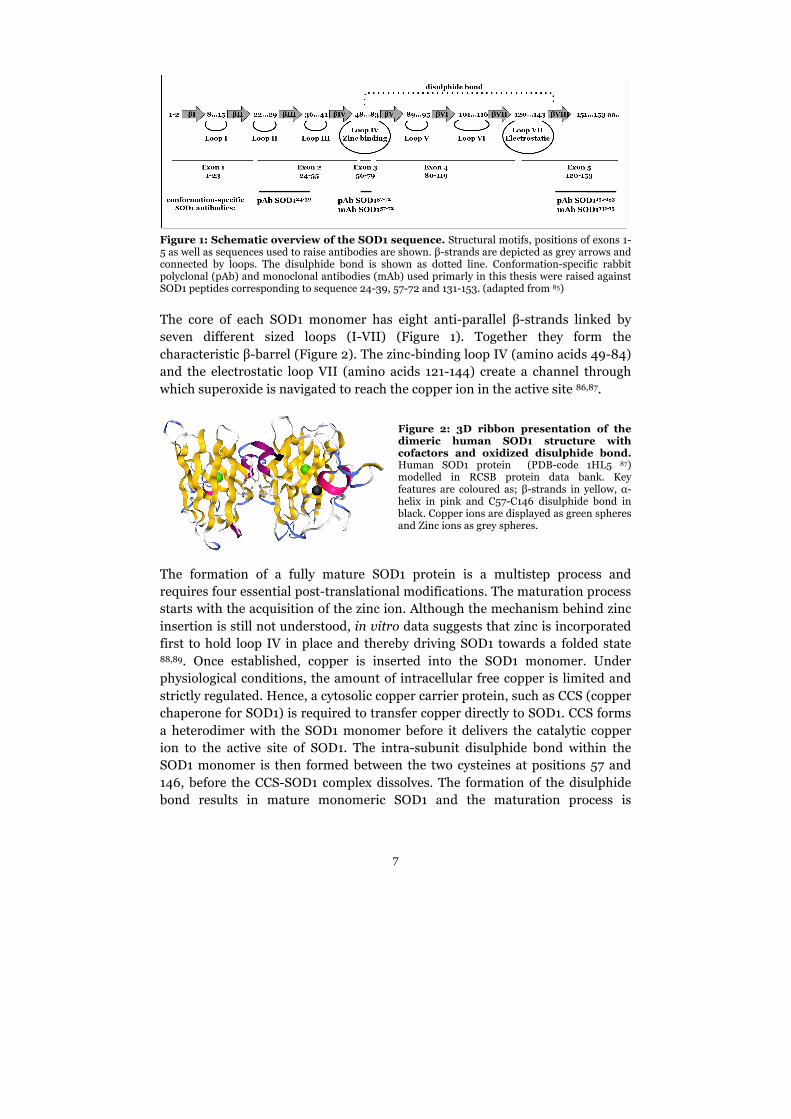
Figure 1: Schematic overview of the SOD1 sequence. Structural motifs, positions of exons 1-5 as well as sequences used to raise antibodies are shown. β-strands are depicted as grey arrows and connected by loops. The disulphide bond is shown as dotted line. Conformation-specific rabbit polyclonal (pAb) and monoclonal antibodies (mAb) used primarly in this thesis were raised against SOD1 peptides corresponding to sequence 24-39, 57-72 and 131-153. (adapted from 85) The core of each SOD1 monomer has eight anti-parallel β-strands linked by seven different sized loops (I-VII) (Figure 1). Together they form the characteristic β-barrel (Figure 2). The zinc-binding loop IV (amino acids 49-84) and the electrostatic loop VII (amino acids 121-144) create a channel through which superoxide is navigated to reach the copper ion in the active site 86,87.
Figure 2: 3D ribbon presentation of the dimeric human SOD1 structure with cofactors and oxidized disulphide bond. Human SOD1 protein (PDB-code 1HL5 87) modelled in RCSB protein data bank. Key features are coloured as; β-strands in yellow, α-helix in pink and C57-C146 disulphide bond in black. Copper ions are displayed as green spheres and Zinc ions as grey spheres.
The formation of a fully mature SOD1 protein is a multistep process and requires four essential post-translational modifications. The maturation process starts with the acquisition of the zinc ion. Although the mechanism behind zinc insertion is still not understood, in vitro data suggests that zinc is incorporated first to hold loop IV in place and thereby driving SOD1 towards a folded state 88,89. Once established, copper is inserted into the SOD1 monomer. Under physiological conditions, the amount of intracellular free copper is limited and strictly regulated. Hence, a cytosolic copper carrier protein, such as CCS (copper chaperone for SOD1) is required to transfer copper directly to SOD1. CCS forms a heterodimer with the SOD1 monomer before it delivers the catalytic copper ion to the active site of SOD1. The intra-subunit disulphide bond within the SOD1 monomer is then formed between the two cysteines at positions 57 and 146, before the CCS-SOD1 complex dissolves. The formation of the disulphide bond results in mature monomeric SOD1 and the maturation process is

8
complete after two metal-loaded and mature SOD1 monomers dimerize via non-covalent interactions and form the active SOD1 enzyme. This CCS-dependent activation of SOD1 requires oxygen for the formation of the disulphide bond, but the precise mechanism is still unknown 90,91. Human SOD1 can also be activated by a CCS-independent pathway, although not as efficiently as with CCS 92.
Native SOD1 is an extremely thermostabile protein with a melting point of 92°C 93. The protein can also withstand long-term storage at 5°C and maintain its enzymatic activity in the presence of strong denaturants 94. However, if the metals are not properly inserted in combination with other alterations in post-translational modifications, it can cause SOD1 to destabilise and subsequently monomerise and unfold 89,95-97.
SOD1 in ALS Mutant SOD1 Mutations in the SOD1 gene have been associated with the devastating disease for more than 25 years now 98. They were the first genetic link identified and to date, more than 185 ALS-associated SOD1 mutations have been described (http://alsod.iop.kcl.ac.uk/). The mutations are distributed over the entire primary protein sequence and have been identified in 2-6% of all ALS patients. Although the pathogenicity of some mutations is controversial 99, approximately 20-25% of all familial ALS patients carry a mutation in SOD1 100,101.
The majority of mutations are missense mutations, caused by the exchange of a single DNA base pair, resulting in the substitution of an amino acid in the translated protein. Nonsense mutations have also been identified and produce truncated proteins by introducing a premature stop codon. Frameshift mutations caused by DNA base pair deletions or insertions change the protein sequence and lead to the formation of truncated proteins 49,102. The most frequent SOD1 mutations are D90A and A4V, and are predominantly found in Europe and North America, respectively 102. The SOD1D90A protein has SOD1WT-like properties such as activity levels and stability, and is associated with a slow disease progession and long survival compared to the average ALS patient 103. In contrast, ALS patients with an A4V mutation have a rapid disease progression and a survival time of less than two years after onset 102. Mutations such as SOD1G127XinsTGGGfs*7 (SOD1G127X) and SOD1D125Tfs*24 generate truncated SOD1 variants and lack the cysteine at position 146. These SOD1 species are unable to fold into the native conformation and cannot form the stabilizing intra-subunit disulphide bond. Hence, they are completely unfolded and quickly degraded in vitro 104.
It was initially thought that SOD1 mutations cause the loss of enzymatic function leading to increased oxidative stress. This mechanism was already known to damage cells in aging cells and other neurodegenerative diseases by

9
impairing the DNA repair system and mitochondrial function 105. However, evidence from several in vitro and in vivo studies have shown that this is not the case for ALS. SOD1 mutations are most commonly inherited in a dominant fashion. Hence, patients carrying recessive SOD1 mutations retain around 50% enzyme activity from the wild-type SOD1 (SOD1WT) allele, sufficient to perform the necessary reactions 49,106. Although most mutations cause a reduced enzymatic activity, there are several ALS-associated SOD1 mutations that show normal enzymatic activities 107-111. Furthermore, deletion of SOD1 in mice causes motor neuron vulnerability and a reduced lifespan due to liver tumours, but does not result in an ALS-like phenotype per se 112,113. In contrast, transgenic mice overexpressing different human mutant or SOD1WT develop an ALS-like phenotype 114-116. Based on these results, it is now widely accepted that mutant SOD1 species gain a novel toxic function. Wild-type SOD1 The vast majority of ALS patients are classified as sporadic cases without a known genetic cause. The concept of a possible involvement of SOD1WT in ALS derived from studies in other neurodegenerative diseases. These demonstrated that wild-type versions of disease-related proteins are involved in sporadic cases in Alzheimer’s disease (AD) as well as in Parkinson’s disease (PD) 117.
In ALS, the hypothesis of a similar role for SOD1 is supported by several findings. Alterations in post-translational modifications, such as oxidation or demetallation can destabilize SOD1WT and induce its unfolding and aggregation in vitro 118-123. Exposure of motor neuron cultures to SOD1WT aggregates promotes cell death similar to aggregates formed from mutant SOD1 124. In transgenic mouse models, high expression levels of human SOD1WT cause an ALS-like phenotype including SOD1 aggregation and neuronal pathology in the CNS 115,125,126. Co-expression of high levels of human SOD1WT and mutant SOD1G85R exacerbate ALS-like disease in transgenic mice 127-129 indicating that SOD1WT can either enhance the toxic properties of mutant protein or is toxic by itself when expressed at high enough concentrations. Several groups have reported independently that misfolded SOD1WT accumulates in motor neurons and glia in post mortem samples from sporadic ALS patients 118,130-133. Altogether, these data indicate that alterations in SOD1WT protein folding could lead to the formation of toxic species similar to ALS-linked mutant SOD1. This supports a role for SOD1WT in the pathogenesis of ALS in patients without SOD1 mutations and point towards a possible common pathogenic mechanism.
However, this view has been challenged by several studies reporting that misfolded SOD1WT cannot be detected in spinal cord tissue post mortem, cerebrospinal fluids, or lymphocytes from sporadic ALS patients 134-138. Hence, the contribution of disordered SOD1WT in the pathogenesis of sALS is controversial and the debate continues.
10
Protein misfolding and aggregation As mentioned in ”Etiology”, several mechanisms of SOD1-mediated toxicity have been proposed. Among those are protein instability, misfolding and aggregation, disturbances in protein degradation, endoplasmic reticulum stress, mitochondrial dysfunction, excitotoxicity and impaired RNA processing. Each pathway has evidence from several in vitro and in vivo studies, but no mechanism by itself can fully explain all of the pathological changes seen in ALS. The following paragraphs will briefly review the processes of SOD1 unfolding and aggregation.
In addition to the natively folded state, proteins are able to adopt alternative conformations. The mechanism behind this process is called misfolding and is associated with a number of neurodegenerative diseases 139. Historically, the term misfolding has been used to refer to all non-native SOD1 species comprised of partially unfolded, disordered and misfolded SOD1 forms. Within this thesis, the term disordered is used to refer to any non-natively folded protein, while the term misfolded refers to disease associated protein species with a specific structure that promote aggregation.
SOD1 misfolding is initiated by destabilizing the protein either through changes in post-translational modifications or by weakening the dimer interface causing monomerisation 140,141. In addition, mutations in SOD1 can affect the stability by reducing the net negative charge and thereby increasing the propensity of conformational changes within the native protein structure 142. The zinc-binding loop is an important feature of the dimer interface and together with the electrostatic loop; they form the active site of the SOD1 protein. In the native protein, these highly dynamic regions are constrained by a network of stabilizing interactions upon metal binding. However, SOD1 mutations or loss of metal ions release the loops from their coordinated structural restraint and permit conformational freedom. Hence, these regions are most likely to be one of the first components to unfold and have been suggested as the primary locus for misfolding 140,143. The reduced stability of SOD1 in combination with stress conditions and impaired removal of disordered/misfolded protein can lead to aggregation.
The mechanism behind the formation of pathological SOD1 aggregates remains unknown. Aggregated proteins in other neurodegenerative diseases are generally amyloids 34. The classic amyloid is an extracellular deposit composed of tightly packed monomeric proteins with a rearranged structure into a series of β-strands. These strands are stabilized by hydrogen bonds and assembled into β-sheets, which are the building blocks of fibrils 144. Dyes such as Congo red and thioflavin-S and -T bind to the β-sheets and are regularly used to determine whether a protein aggregate has an amyloid structure 144.
11
Because these dyes do not stain CNS tissue preparations from patients with or without mutations, ALS is not considered to be a classical amyloid disease 136,145. Patients with SOD1 mutations also show no amyloid deposition at autopsy 136. However, thioflavin-S positive aggregates have been observed in several transgenic mouse models of ALS 146,147. These aggregates as well as aggregates from ALS patients have shown a fibrillar morphology when analysed by electron and atomic force microscopy, suggesting a potential to form amyloid depositions 148,149.
Compared to other proteins associated with neurodegenerative diseases, SOD1 is not an aggregation-prone protein in vitro. However, metal free (apo) SOD1 is capable of forming detergent-insoluble aggregates under destabilizing conditions such as low pH, high temperature or the presence of trifluoroethanol 146,150. Moreover, the spontaneous formation of SOD1WT or mutant SOD1 fibrils can be increased by constant shaking at 37 °C 151,152. Both SOD1WT and mutant SOD1 proteins have been found to aggregate without the need for denaturing conditions 153, although the initiation phase required a longer incubation time. However, loss of metals and a reduction in enzymatic activity preceded aggregation, implying that destabilization and unfolding were still necessary to initiate aggregation. Prion-like transmission Emerging evidence indicates that a prion-like propagation of misfolded and aggregated proteins is involved in the pathogenesis of neurodegenerative diseases including ALS 154,155. “Prions” are misfolded species of the normal cellular protein that interact with native forms of the same protein and induce their transformation into the aberrant form 156,157. This process is commonly known as nucleation and produces the “seeds” that act as templates to initiate the aggregation process. These seeds elongate rapidly to form larger aggregates and fibril structures 156. Fragmentation of fibrils accelerates the aggregation process by increasing the number of seeds. It also enables the propagation of fibrils in neighbouring cells if seeds are taken up by them 158.
In vitro studies have shown that exogenous hSOD1 aggregates are able to induce nucleation of soluble mutant SOD1 as well as SODWT in the cytosol, causing it to aggregate and creating a self-perpetuating cascade of SOD1 misfolding 159,160. These aggregates were constantly released from dying cells or through exosomes and taken up by neighbouring cells demonstrating a prion-like seeding character of SOD1 133,161. Aggregate transmission could be reduced by pre-incubation with anti-SOD1 antibodies 133,162.
Injections of spinal cord homogenates from paralyzed SOD1G93A or SOD1G37R mice into spinal cords or sciatic nerves of recipient mice induced the propagation of ALS-like disease in vivo 134,163.
12
Another hallmark of prion diseases is the existence of different aggregate species 164, which arise from the same protein, but adopt different conformations. These conformational variants are commonly referred to as strains and several studies have reported the existence of different strains for tau 165,166, Aβ 167 and α-synuclein 168,169. In ALS, SOD1 aggregation depends on the nature of the mutation and conditions under which nucleation is induced 148,170. Hence, this process is flexible and can generate different aggregate structures. While in vitro studies revealed several distinct pathways for SOD1 aggregation 171, two different strains (A and B) of SOD1 aggregates have been identified in spinal cords of mice expressing mutant SOD1. Both strain A and B differ from aggregates produced in vitro and exhibit distinct structural characteristics, molecular features, and growth kinetics 172. Furthermore, both strains induced different patterns of ALS-like disease progression when inoculated into the spinal cord of pre-symptomatic transgenic SOD1G85R mice, indicating that templated SOD1 aggregation can spread in a prion-like fashion 173. Additionally, a recent study demonstrated that SOD1G127X aggregates from an ALS patient induced pre-mature ALS-like disease in transgenic mice expressing mutant SOD1 174. These studies demonstrated the transmissibility and seeding capabilities of SOD1 in vivo, supporting a prion-like spread hypothesis for SOD1 aggregates. Models of SOD1 ALS ALS is a disease of the CNS with no possibility of routinely collecting biopsies to study disease pathogenesis or progression in patients. Hence, researchers are restricted to investigate affected CNS regions in post mortem tissues. Due to the severe loss of motor neurons at the end-stage of ALS, information that can be obtained on the complex mechanisms leading to motor neuron degeneration and cell death is very limited. To study these mechanisms, various model systems have been established that recapitulate different neuropathological and genetic aspects of the disease 175,176. The work of this thesis is based on several model systems that will be reviewed in the following paragraphs.
Cellular models Cell culture models are widely used to study the molecular basis of disordered and misfolded SOD1 toxicity in vitro. Due to their rodent or primate origin, most cell lines depend on overexpression of wild type or mutant human SOD1 protein 177-180 leading to an artificial model with non-physiologically levels of the target protein. Patient-derived cells, on the contrary, carry endogenous SOD1 mutations and express the protein at physiological levels. Hence, patient-derived cultures avoid an artificial overload of mutant SOD1 and may be used to model a disease that is more relevant to human ALS. Using cells from patients, it is also possible to investigate SOD1 toxicity in the context of the individual’s background.
13
A further advantage of this approach is the possibility to study sALS without known genetic cause or forms of fALS that lack suitable mouse models. Astrocyte cultures Patient-derived astrocytes can be isolated from surgical biopsy specimen or post mortem tissues and expanded in culture. In general, viable cells can be obtained from donors of diverse ages ranging from embryonic/foetal, post natal, and adult, with a post mortem delay of up to 36 hours 181,182. However, there are differences regarding yield, proliferative capacity and morphology between cells isolated from foetal compared to adult CNS samples. For instance, cultures from foetal tissues proliferate twice as many times than adult derived-cells, before showing signs of senescence 182.
Astrocytes are either retrieved directly from CNS tissue 183 or generated from isolated neural progenitor cells (NPCs) 182. NPCs consist of multipotent cells capable of differentiating into functional neurons and glia cells including astrocytes 184-187. In ALS, NPC-derived astrocytes generated from both fALS and sALS cases induced degeneration of mouse and human motor neurons upon co-culture 188,189. Nevertheless, human CNS tissue from ALS patients is only occasionally available and due to biological aging, only a limited number of studies can be performed using these models. Dermal fibroblast cultures Human fibroblasts can be obtained from patients via skin biopsies and propagated in culture at relatively low costs. Although they are not a primary target of ALS, fibroblasts share pathophysiological abnormalities with the affected neuronal tissue 190,191 and hence, are a valuable model system with which to study the disease. Fibroblast cultures have been used to assess biological changes in sALS patients with regard to stress response, energy metabolism, and RNA processing 190,192-194 as well as to study the pathogenicity of several ALS-associated mutations in familial cases 195,196 including SOD1 104,196,197. Induced pluripotent stem cell-derived cells Originally, experiments utilizing stem cells to model neurons relied upon differentiation of embryonic stem cells (ESCs) 198. Since ESCs are not patient-derived, disease modelling depends on the expression of a transfected target gene/protein. Hence, they encounter the same aforementioned drawbacks of overexpression models. The possibility to convert adult somatic cells into induced pluripotent stem cells (iPSCs) circumvents these issues and avoids ethical concerns raised by using human embryonic material to generate ESCs.
Human iPSCs can be generated from a variety of somatic cell types; including fibroblasts, keratinocytes 199, lymphocytes 200, and even post-mitotic neurons 201. Initial reprogramming methods used viral transduction to
14
simultaneously introduce four transcription factors into the genome 202. Since then, several strategies to convert somatic cells have been developed using either viral transduction or chemical transfection to express an optimized combination of reprogramming factors 203. One merit of human iPSCs lies in their capacity to differentiate into nearly any cell-type within the human body. A variety of protocols have been developed to generate several ALS-relevant cell types, such as spinal motor neurons, astrocytes 204, microglia 205, oligodendrocytes 206,207 and muscle cells 208. Sances and colleagues reviewed various motor neuron differentiation protocols that differ not only in the chemical composition of iPSC culture media, but also in the molecules used to initiate differentiation 209. Despite these differences, most protocols share three developmental phases; (I) inducing a neuronal identity by generating neural progenitors; (II) specification into motor neurons; and (III) their subsequent maturation 209-211. Depending on protocol and length of maturation phase, motor neurons can exhibit electrophysiological activity and generate action potentials similar to rodent motor neurons at an embryonic stage 209,212.
Analysis of iPSC-derived motor neurons from SOD1 fALS patients revealed important functional phenotypes including axonal degeneration, decreased cell survival, neurofilamentous disorganization and changes in excitability 213,214. In addition, motor neurons carrying SOD1 mutations recapitulated several pathological aspects of ALS, such as enhanced endoplasmic reticulum and oxidative stress 212,215. Hence, patient-derived motor neurons are a valuable model system with which to study the contribution of mutant SOD1 to the early stages of ALS. Rodent models Transgenic mice overexpressing different human mutant SOD1s are considered to be the gold standard of ALS model systems and a keystone of preclinical research. Murine models mirror human ALS more closely than many cellular models 216 and have been used to unravel pathogenic mechanisms and provide preclinical data on promising therapeutic targets. G93A hSOD1 The first transgenic mouse model was developed within a year after mutations in SOD1 were linked to ALS 116. This model expresses human SOD1 G93A (hSOD1G93A), under control of the endogenous human SOD1 promoter, to mimic the normal regulation of SOD1 expression. Originally, several lines of hSOD1G93A
transgenic mice were generated, but only mice with around 18 copies of the transgene and hence, a high expression of mutant SOD1 (G1 line) developed an ALS-like disease. The first signs of hind limb weakness appear at 90-100 days of age and mice become progressively paralyzed in one or more limbs. The average survival time of the G1 line is around 180 days. Analyses of spinal cord show loss

15
of motor neurons, glial activation and positive staining of aggregated SOD1 116,217,218. Since the original publication of the G1 line, several additional lines have been developed and characterized. Although low copy number hSOD1G93A mice are considered to more accurately mirror pathological findings in humans 219, the most commonly used mouse model in ALS research is the G1 sub-line G1H with 25 predicted copies of the transgene 220. G85R hSOD1 Several hSOD1G85R transgenic lines were generated using the human SOD1 promoter to regulate expression. Although the hSOD1G85R transgene is expressed broadly, the levels in the CNS are initially below the levels of endogenous murine SOD1. However, most hSOD1G85R lines developed an ALS-like disease and at end-stage, the hSOD1G85R levels have increased 2-fold. Early symptoms including reduced grip strength in one limb appear at around 245 days of age. The initial motor impairments progress rapidly and spread to other limbs leading to paralysis within two to three weeks. Spinal cords analyses reveal that hSOD1G85R mice developed degeneration of motor neurons and large axons, glial pathology as well as SOD1 aggregates in neurons and glia cells. Astrogliosis can be detected before the first motor symptoms appear. Moreover, these reactive astrocytes contain inclusions positive for SOD1 and as the diseases progresses, these SOD1 aggregates become more abundant 114. In addition to the hSOD1G93A and hSOD1G85R models, mice expressing other hSOD1 mutations have been generated including G37R 221, H46R 222, D90A 126, G127X 223, as well as models expressing wt hSOD1 224. All of these models develop pathological abnormalities that correlate with features identified in ALS patient tissues. These include the denervation of neuromuscular junctions, loss of spinal motor neurons, reactive gliosis, mitochondrial dysfunction, accumulation of misfolded SOD1 protein, and progressive paralysis leading to a reduced lifespan 114,116,219. However, development of ALS-like disease depends essentially upon the SOD1 mutation and the level of transgene expression, as well as on gender and the genetic background 225. Due to these factors, transgenic SOD1 mouse models differ in ages of disease onset and rates of disease progression. Additionally, the severity of the disease is determined by the expression levels of the transgene. For instance, hSOD1G93A transgenic mice carrying 4 or less copies of the transgene did not develop ALS-like symptoms 116,226. Hence, these confounding factors have to be taken into consideration when interpreting and comparing results between different transgenic SOD1 models.
16
Antibodies The earliest references to antibodies emerged in the late 19th century as the fields of bacteriology and immunology were evolving. In 1890, Behring and Kitasato successfully cured diphtheria by injecting antibody-containing serum from immune animals in to infected guinea pigs 227. This discovery was a milestone in the development of serum therapy and marked the beginning of the humoral theory of immunity 228. Since then, research revealed that antibodies are developed by the immune system as a means of defence against various threats including invading pathogenic microorganisms and altered self-cells. Two different branches of the immune system are known to generate the innate and the adaptive immune responses 185. The innate immune system is ready to fight at all times and consists of various components that both prevent the entry of pathogens and limit their ability to spread throughout the body. These components include physical barriers, such as the skin, as well as chemical and biological factors, such as tears, mucosa, antimicrobial molecules, and phagocytic cells. The innate immune system is activated by chemical properties of molecules present on common microbes including pathogens. Antigens are recognized by a limited number of constitutively expressed receptors and induce different responses including phagocytosis, proinflammatory signaling and apoptosis 185,229-232. However, the response is general and anything identified as foreign can be targeted for elimination 233. In contrast, the adaptive immune system uses specific molecular structures on the surface of antigens (epitopes) to strategically build an immune response. It acquires an immunological memory and thus, elicits a faster response the next time the same pathogen is recognized. The adaptive immune system can be further divided into cell-mediated and humoral immunity. Cell-mediated responses rely on the activation of cytotoxic cells by T-cells, while humoral responses depend on naïve B-cells and their differentiation into antibody-producing memory or effector B-cells. Antibodies, also commonly known as immunoglobulins (Ig), are either membrane-bound on memory B-cells or secreted into the blood stream by effector B-cells. The primary role of secreted antibodies is to circulate through the body and identify and mark specific foreign antigens for elimination 234,235.
Natural antibodies perform two main functions. First, they bind specifically to the target antigen, before inducing an immune response against the captured antigen. To better understand these functions, the following paragraphs will focus on antibody structures and inherent features in more details.
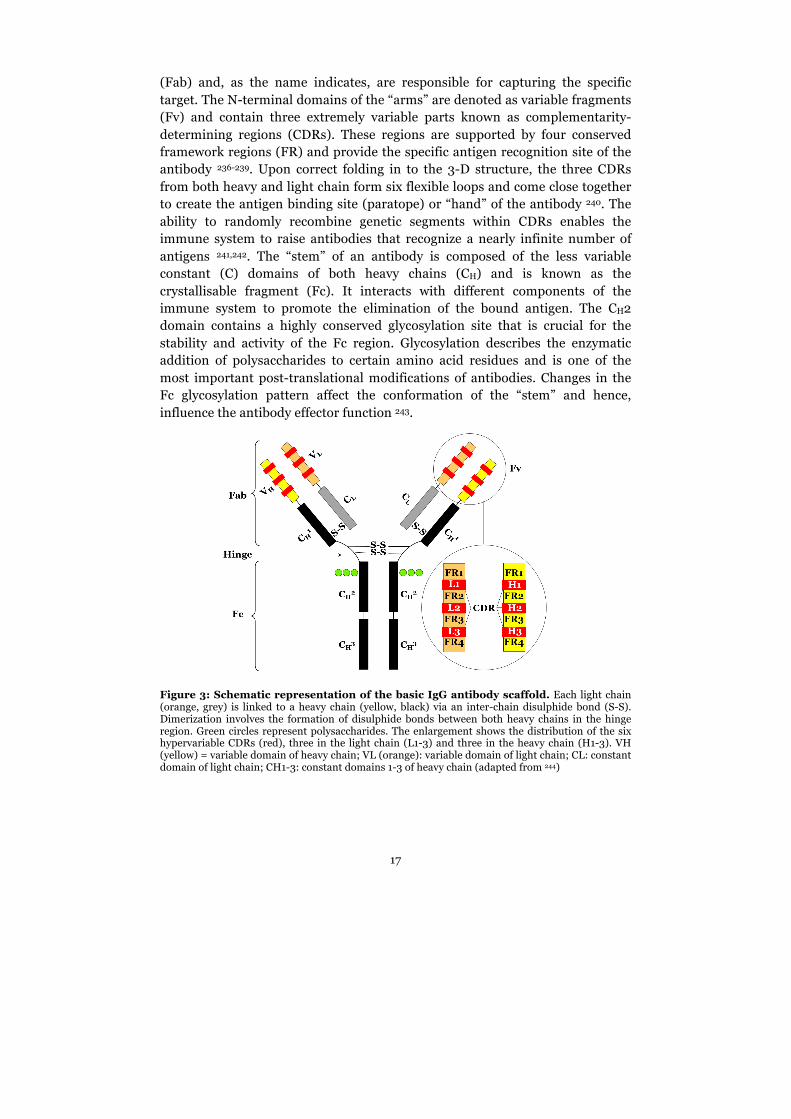
The basic scaffold of an Ig consists of two identical heavy chains and two identical light chains that are joined together by disulphide bonds. This arrangement forms the characteristic Y-shaped molecule with two “arms” and one “stem” (Figure 3). The “arms” represent the antigen-binding fragments
17
(Fab) and, as the name indicates, are responsible for capturing the specific target. The N-terminal domains of the “arms” are denoted as variable fragments (Fv) and contain three extremely variable parts known as complementarity-determining regions (CDRs). These regions are supported by four conserved framework regions (FR) and provide the specific antigen recognition site of the antibody 236-239. Upon correct folding in to the 3-D structure, the three CDRs from both heavy and light chain form six flexible loops and come close together to create the antigen binding site (paratope) or “hand” of the antibody 240. The ability to randomly recombine genetic segments within CDRs enables the immune system to raise antibodies that recognize a nearly infinite number of antigens 241,242. The “stem” of an antibody is composed of the less variable constant (C) domains of both heavy chains (CH) and is known as the crystallisable fragment (Fc). It interacts with different components of the immune system to promote the elimination of the bound antigen. The CH2 domain contains a highly conserved glycosylation site that is crucial for the stability and activity of the Fc region. Glycosylation describes the enzymatic addition of polysaccharides to certain amino acid residues and is one of the most important post-translational modifications of antibodies. Changes in the Fc glycosylation pattern affect the conformation of the “stem” and hence, influence the antibody effector function 243.
Figure 3: Schematic representation of the basic IgG antibody scaffold. Each light chain (orange, grey) is linked to a heavy chain (yellow, black) via an inter-chain disulphide bond (S-S). Dimerization involves the formation of disulphide bonds between both heavy chains in the hinge region. Green circles represent polysaccharides. The enlargement shows the distribution of the six hypervariable CDRs (red), three in the light chain (L1-3) and three in the heavy chain (H1-3). VH (yellow) = variable domain of heavy chain; VL (orange): variable domain of light chain; CL: constant domain of light chain; CH1-3: constant domains 1-3 of heavy chain (adapted from 244)
18
The effector responses triggered by antibodies can be summarized into two principal pathways; (1) activation of the complement system and (2) binding to Fc receptors present on the surface of macrophages and other immune cells 245. The nature of induced effector functions depends on the type of heavy chain the particular antibody contains. In mammals, there are five main variants of the Ig heavy chain (α, δ, ε, γ and µ) that differ in sequence and number of constant domains. Based on these different heavy chains, immunoglobulins are classified into five isotypes - IgA (α), IgD (δ), IgE (ε), IgG (γ) and IgM (µ). The isotypes differ further in the hinge region that joins the Fab and Fc domains and thus, provides stability and flexibility to the antibody 246,247.
Besides structural differences, isotypes vary also in serum half-life, localization in the body and timing of appearance during an immune response. Briefly, monomeric IgA is secreted into plasma and cerebrospinal fluid at low levels, while the majority of IgA exists as dimers or tetramers in mucosal secretions such as tears, saliva, breast milk and gastrointestinal fluids. Human IgA is divided in two subclasses, termed IgA1 and IgA2 and their distribution vary significantly between different mucosal secretions. Among other functions, IgA interferes with the uptake of soluble or particulate antigens by mucosal surfaces and inhibit bacterial adherence 248. The isotype IgD exhibits an extended hinge region that is responsible for the antibody’s vulnerability to proteolytic cleavage. It is mainly membrane bound and part of the B-cell receptor, but can also be secreted in the nasal mucosa and tonsils. However, the precise function of IgD is still unknown 249. Unlike IgD, IgE has two additional constant domains in place of a hinge region. In plasma, IgE is the least abundant antibody isotype and has the shortest half-life. It is involved in allergic reactions and provides protection against multicellular parasites 250. In a similar fashion to IgE, IgM possesses two additional constant domains instead of a hinge region. This isotype is classically represented as a pentamer or hexamer and hence, the largest of the immunoglobulins. Due to its size, IgM is mainly confined to the intravascular pool and initially dominates the humoral immune response. During the course of the immune reaction, IgM undergoes class switching into the IgG isotype, the most abundant antibody in human serum 251. IgG is also the major antibody isotype of the adaptive immune response and has the longest half-life. IgG exists as a monomer and can be further divided into subclasses that differ in the hinge region and the degree to which they activate the immune system. In humans, there are four subclasses (IgG1, IgG2, IgG3 and IgG4) and although the amino acid sequence is more than 90% identical, each subclass induces a unique set of effector functions. In mice and rats, the IgG class is categorized into five (IgG1, IgG2A, IgG2B, IgG2C and IgG3) and four subclasses (IgG1, IgG2A, IgG2B, IgG2C), respectively. It is noteworthy that the subclass nomenclature has been derived independently for each species. Hence, no general relationship can be established between subclasses from different species 252-254.
19
Tools to study proteins Antibodies exhibit an extraordinary diversity of binding specificity to an abundance of targets that represent all kinds of structures and features. Due to their unique binding characteristics, antibodies have a great potential to be utilized as biochemical tools in various applications that can be categorized into three main areas; diagnostics, research and therapeutics 240.
In diagnostic assays, antibodies have become crucial components in the detection of a wide range of conditions, such as infections, allergies, hormone imbalance or levels of biological markers in blood 255-258. Within life science research, antibodies are vital tools for analytical methods used to adress basic research questions. They are used to isolate, identify and characterize molecules and their interaction partners. This in turn enables researchers to draw conclusions about cellular organisations and pathways 259. The natural occurrence and physiological role of antibodies in organisms predetermined their use as suitable therapeutics. Since the 1990s, immunoglobulins have been the fastest growing class of biological therapeutics and are utilized to successfully treat infectious diseases, inflammatory disorders, respiratory diseases, cardiovascular diseases and cancer 260.
Sensitivity and specificity Whether an antibody is suitable as a tool for a certain application is determined by its sensitivity and specificity towards a particular target. Sensitivity is a measure of the antibody’s ability to elicit a detectable signal above a common background to a low concentration of target molecules. In other words, sensitivity refers to the detection limit of an antibody in an immunoassay 261. Specificity is a measure of the antibody’s ability to discriminate between its specific target protein and unrelated proteins competing for the same binding 235. Both sensitivity and specificity are defined by the antibody’s binding affinity to its particular antigen. Affinity describes the strength of all interactions between the paratope of the antibody and the epitope of the target antigen. The molecular interactions are reversible and depend on non-covalent forces such as hydrogen bonds, Van der Waals forces, hydrophobic interactions and electrostatic forces. These interactions are influenced by several parameters including temperature, pH, pressure, ionic strength and concentrations of molecules in solution 262,263. Affinity can be measured in several ways based on equilibrium or kinetic measurements. It is classically reported by a KD value that is determined by the association rate of a single paratope and epitope (Kon) and the dissociation rate of the complex (Koff) according to equation (1) 235,264.
𝐾! = !!""!!"
M (1)
20
Typical KD values for antibodies are in the low micromolar (10-6) to picomolar (10-10) range and in general, smaller KD values indicate higher affinity of the antibody 235. Considering that antibodies exhibit typically more than one antigen-binding site, affinity is further divided into intrinsic affinity and functional affinity. The term intrinsic affinity refers to the interaction of a single paratope with its corresponding epitope. Functional affinity, on the other hand, describes the accumulated binding strength of multiple intrinsic affinities and is commonly known as avidity 262. For instance, IgG has two antigen-binding sites and hence is bivalent, whereas IgM is deca- or hexavalent and therefore has a higher avidity. Polyclonal, monoclonal or synthetic? Researchers in life science and translational medicine are dependent on reliable antibodies, although they are often only interested in the target and not the antibody itself. The type of information obtained from a specific experiment is, however, directly influenced by the antibody. Hence, a thoughtful antibody design and the right scaffold are vital when selecting the right binder for a specific research question. All antibodies have benefits as well as drawbacks as research tools and have distinct characteristics that differentiate them from each other.
Due to their abundance, long half-life and efficacy, IgGs are the main isotype utilized as tools in research and therapeutics and hence, hereafter the term antibody refers to the IgG isotype. Polyclonal antibodies Polyclonal antibodies (pAb) are a heterogeneous mixture of antibodies generated from independent B-cell clones. As a consequence, pAbs recognize several epitopes on the same antigen with different specificities and affinities. Animals used to generate pAbs are generally chosen based on the evolutionary relationship between the source of the antigen and the animal species. The more distant the organisms, the more immunogenic the antigen will be. An alternative approach to enhance the immune response in the host is to inject an adjuvant together with the antigen. Adjuvants are substances used to generate a more robust immune response than the antigen alone 265. Another factor to consider when choosing the right animal is its size, since a bigger animal (e.g. goats) has a larger blood volume than a small one (e.g. mouse), and hence, more antisera can be obtained. Following blood collection and the separation of antibody-containing serum from red blood cells and coagulation factors, the antisera may be used directly in experiments. However, since the pAb specific to the antigen compromise around 1% of the total antibody population, purification of the pAbs are recommended 266.

21
The heterogeneous nature of pAbs is both a blessing and a curse. Advantages of pAb include applications such as immunohistochemical (IHC) staining of tissues, where epitopes are often inaccessible due to fixation-produced cross-linking. Additionally, pAbs are the preferred choice of detecting denatured proteins in western blotting, where some epitopes have been destroyed. They are also a suitable tool for detection of proteins at low concentrations due to the detection of multiple epitopes on the same target and a signal amplification effect. Another advantage of pAb is their tolerance to minor antigen changes caused by post-translational modifications 266. However, the heterogeneity and the limited availability of antisera are major drawbacks of pAbs. It is not possible to generate the exact same composition of antibodies in two animals, even if they are of the same species and are inbred. Hence, batch-to-batch consistency has to be ensured by testing each newly purified batch under the same experimental conditions and comparing the results to the original specification 266. Monoclonal antibodies The true potential of antibodies as research tools was not appreciated until the revolutionary work by Köhler and Milstein in 1975 resulted in the production of monoclonal antibodies (mAb) 267. They generated an immortal cell line, known as a hybridoma, by fusing antibody-producing B-cells with a mouse myeloma cell line. Cells were then cultured in a selective media in which only hybridoma clones could survive and proliferate. Each hybridoma clone expresses a single antibody with specificity for one particular epitope on the antigen. Once hybridoma cells are established, clones are screened with appropriate analytical methods to determine specificity and affinity as well as to identify good antibody-producers 268.
Hybridoma cells can be cultured long-term in vitro allowing the purification of large quantities of mAbs. Due to the single-epitope binding characteristics, mAb are less prone to cross-react with other proteins and have nearly no batch-to-batch variation. Thus, mAbs are suitable tools for therapeutic uses and applications requiring quantification 268. However, mAbs are sensitive to epitope changes and experimental conditions that could impact the epitope as well as the formation of binding interactions. Furthermore, hybridoma cells are prone to mutations and can lose mAb expression, and thus, require frequent retesting 268. Synthetic antibodies Advances in biotechnology and protein engineering allowed the development of alternative binding molecules to overcome the inherent limitations of antibodies. One of the key differences between naturally occurring and synthetic antibodies is the way they are generated.
22
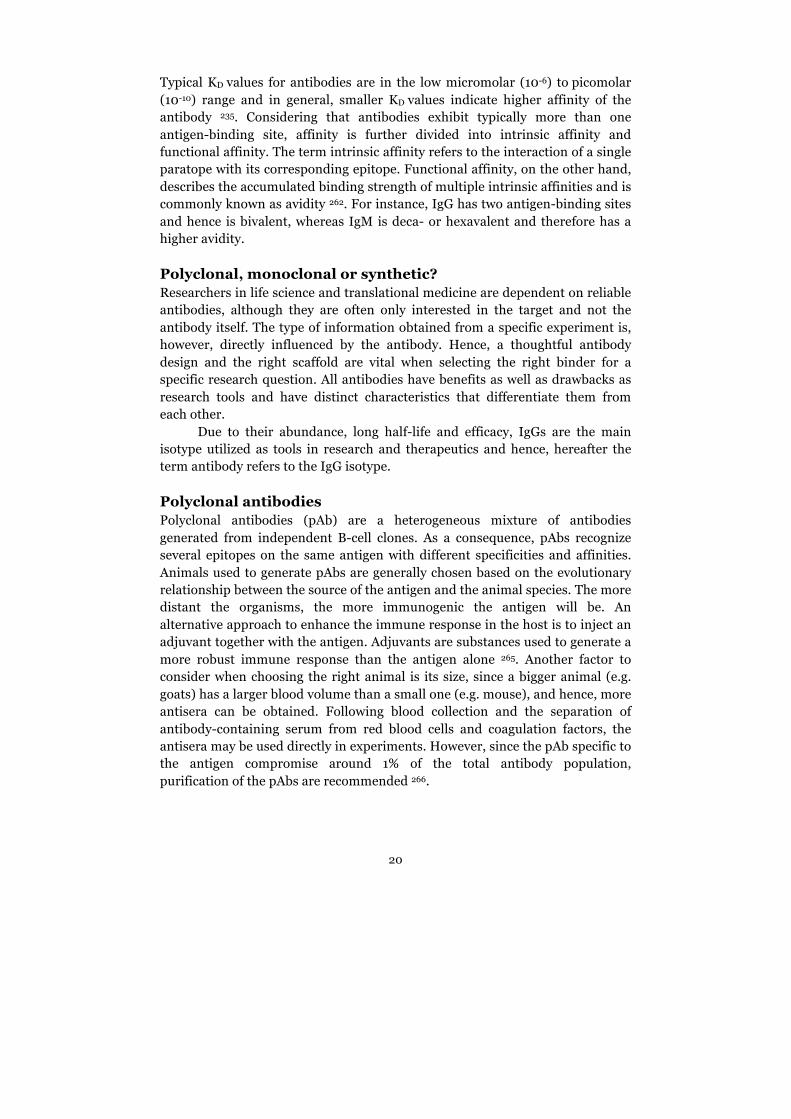
As mentioned above, polyclonal and monoclonal antibodies are generated in vivo by recombination and hypermutation during B-cell development and differentiation 241,242. In contrast, synthetic antibodies are engineered in vitro and thus, bypass the immune system and the need for animals for their production. The synthetic methodology also allows for the generation of affinity reagents against antigens that are toxic to animals 269. Synthetic antibodies include recombinant antibodies and their derivatives, as well as antibody-like molecules based on alternative scaffolds. Recombinant antibody derivatives The genetic manipulation of recombinant full-length antibodies enables the expression of a wide range of small antibody formats, such as single-chain Fv fragments (scFvs). These small monovalent antibodies consist only of the variable domains, VH and VL, which are joined by a flexible peptide linker (Figure 4). ScFvs retain the antigen-binding affinity of the parent IgG and can be developed by cloning the variable domain genes from hybridoma cells secreting a specific antibody 270. As an alternative, scFvs can be produced from antibody libraries that are built on the variable domain gene repertoires from non-immunized animals, immunized animals, or completely synthetic sources 271,272. Using a suitable display system, such as phage display or yeast display, these libraries can be screened to identify scFvs with desired characteristics. In addition, scFvs can be rebuilt into multivalent binders, such as diabodies to obtain desired avidities (Figure 4). They can further be fused to a wide range of molecules including radio-isotopes for imaging, enzymes for drug testing, and biosensors 273. Other small antibody derivatives are the variable domain proteins found in the immune system of camelids or sharks 274 (Figure 4). These nanobodies consist only of a single variable domain that is homologous to the full-length antibody VH domain. Nanobodies exhibit high specificities and affinities towards their target antigens and due to their molecular stability and small size, nanobodies are suitable tools for intracellular environments 275,276.
Figure 4: Overview of different synthetic antibodies. scFv, diabodies and nanobodies are small derivatives of full-length antibodies. The variable light chain (VL, orange) is linked to the variable heavy chain (VH, yellow) via a flexible linker. Affibody (PDB code: 2KZI 277) was modelled in RCSB protein data bank with the three α-helices in violet. Knottins (adapted from 278) contain six cysteines (yellow circles, I-VI) that are connected by three disulphide bonds (dotted blue line) forming the characteristic knot. β-strands are shown as blue arrows.

23
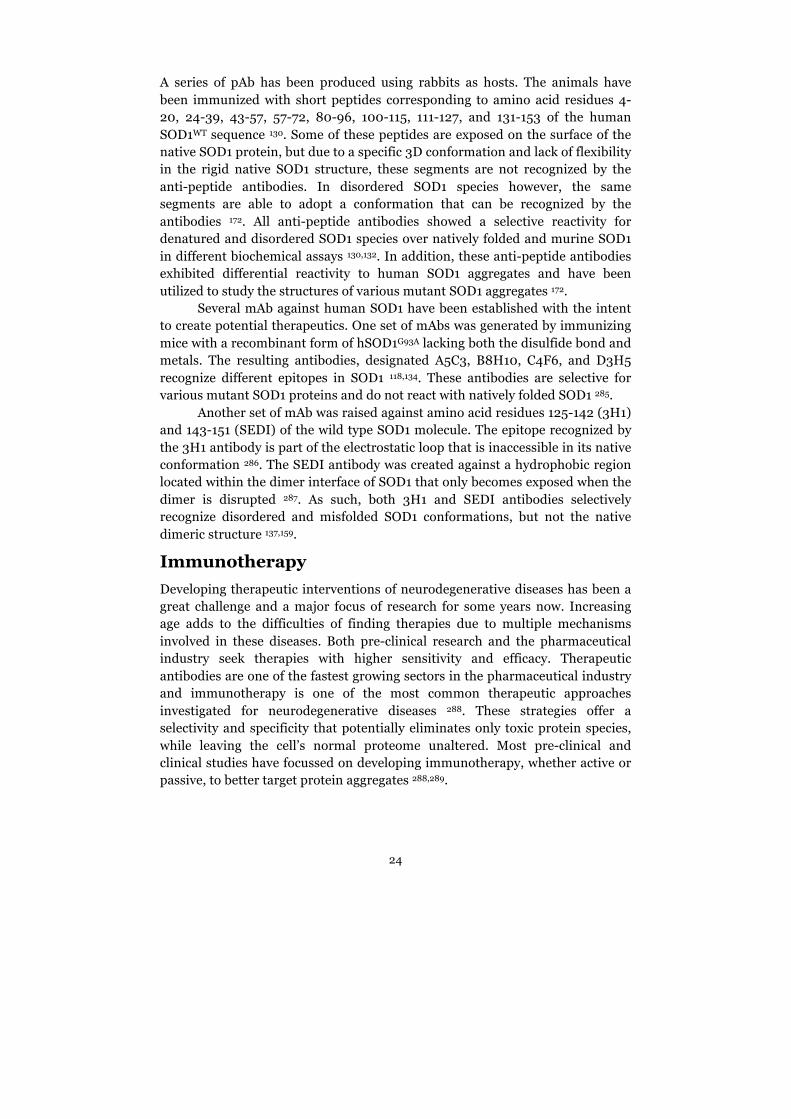
Alternative affinity scaffolds In addition to using antibody domains as a basis to create molecules for affinity applications, other scaffolds have also shown promising results 279. These antibody-like molecules are known as antibody mimetics and are mainly based on proteins or polypeptides. They have no structural relation to antibodies, but are able to bind specific antigens similar to antibodies. Many different types of antibody mimetics have been synthesized as reviewed by Yu and colleagues 279. The most important and widely used molecules are affibodies, knottins and aptamers. Affibody molecules originate from Staphylococcus aureus and compise a 58 amino acid-long polypeptide that folds into three α-helices (Figure 4). Their small and simple structure has led to applications in immunoassays, microarrays, enzyme regulation, in vivo imaging, and diagnostics 280. Knottins are a large family of structurally related peptides and are characterized by a rigid molecular knot. The knot is created by a particular arrangement of three disulfide bonds (Figure 4) and confers a high thermal, chemical and proteolytic stability 281. Knottins are used for non-invasive molecular imaging 278 and several naturally occurring knottins have been approved for treating chronic pain and gastrointestinal diseases 282. In contrast to affibodies and knottins, aptamers are composed of ribonucleic acid (RNA) or single-stranded deoxyribonucleic acid (DNA) oligonucleotides. Aptamers bind their corresponding target with high specificity and affinity and, like antibodies, can be used to activate or neutralize proteins upon binding 283. They have been used in immunoassays, microarrays, flow cytometry and imaging 284. Antibodies against SOD1 A wide range of antibodies against SOD1 has been generated over the years, many of them recognizing epitopes that are only accessible in disordered or misfolded SOD1 species. Hence, these antibodies discriminate between natively folded SOD1 and aberrant SOD1 species and are valuable tools to study potentially pathogenic SOD1 species (Figure 5).
Figure 5: Schematic overview of antibody binding to different SOD1 species. Epitopes are unavailable for antibody binding in the natively folded protein. They become accessible and adopt a conformation that is recognized by the antibodies in the unfolded/misfolded state of the SOD1 protein and in SOD1 aggregates.
24
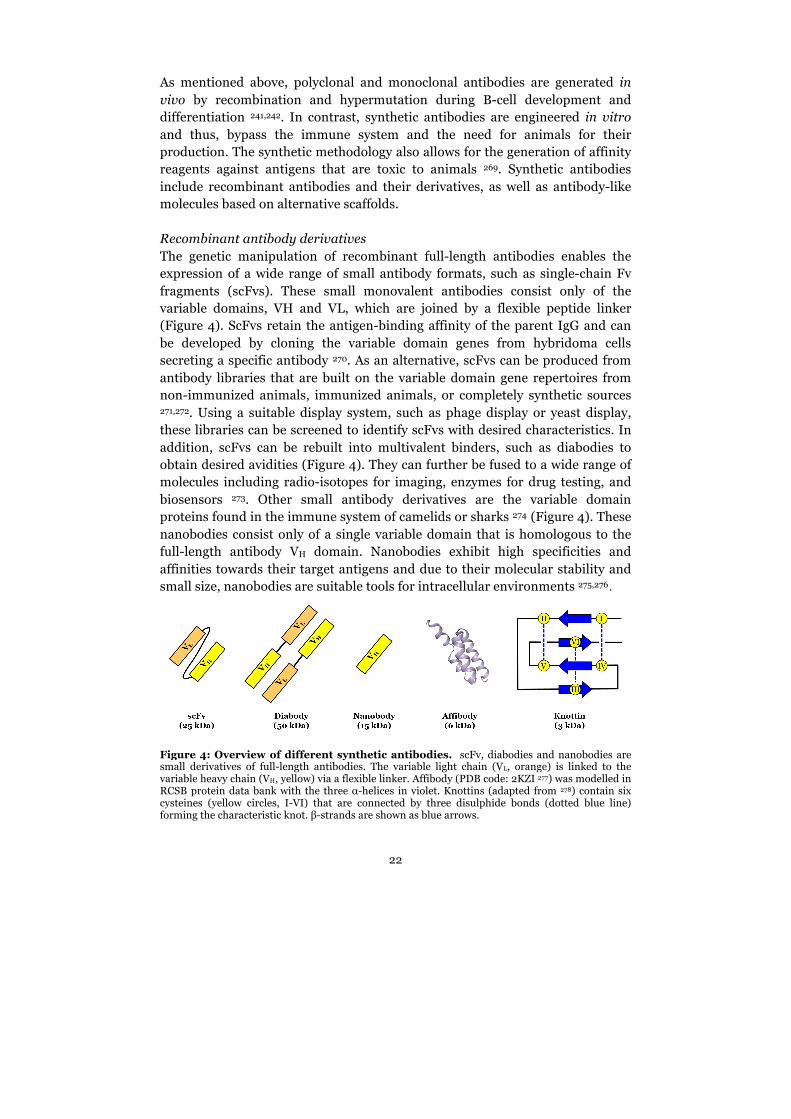
A series of pAb has been produced using rabbits as hosts. The animals have been immunized with short peptides corresponding to amino acid residues 4-20, 24-39, 43-57, 57-72, 80-96, 100-115, 111-127, and 131-153 of the human SOD1WT sequence 130. Some of these peptides are exposed on the surface of the native SOD1 protein, but due to a specific 3D conformation and lack of flexibility in the rigid native SOD1 structure, these segments are not recognized by the anti-peptide antibodies. In disordered SOD1 species however, the same segments are able to adopt a conformation that can be recognized by the antibodies 172. All anti-peptide antibodies showed a selective reactivity for denatured and disordered SOD1 species over natively folded and murine SOD1 in different biochemical assays 130,132. In addition, these anti-peptide antibodies exhibited differential reactivity to human SOD1 aggregates and have been utilized to study the structures of various mutant SOD1 aggregates 172.
Several mAb against human SOD1 have been established with the intent to create potential therapeutics. One set of mAbs was generated by immunizing mice with a recombinant form of hSOD1G93A lacking both the disulfide bond and metals. The resulting antibodies, designated A5C3, B8H10, C4F6, and D3H5 recognize different epitopes in SOD1 118,134. These antibodies are selective for various mutant SOD1 proteins and do not react with natively folded SOD1 285.
Another set of mAb was raised against amino acid residues 125-142 (3H1) and 143-151 (SEDI) of the wild type SOD1 molecule. The epitope recognized by the 3H1 antibody is part of the electrostatic loop that is inaccessible in its native conformation 286. The SEDI antibody was created against a hydrophobic region located within the dimer interface of SOD1 that only becomes exposed when the dimer is disrupted 287. As such, both 3H1 and SEDI antibodies selectively recognize disordered and misfolded SOD1 conformations, but not the native dimeric structure 137,159.
Immunotherapy Developing therapeutic interventions of neurodegenerative diseases has been a great challenge and a major focus of research for some years now. Increasing age adds to the difficulties of finding therapies due to multiple mechanisms involved in these diseases. Both pre-clinical research and the pharmaceutical industry seek therapies with higher sensitivity and efficacy. Therapeutic antibodies are one of the fastest growing sectors in the pharmaceutical industry and immunotherapy is one of the most common therapeutic approaches investigated for neurodegenerative diseases 288. These strategies offer a selectivity and specificity that potentially eliminates only toxic protein species, while leaving the cell’s normal proteome unaltered. Most pre-clinical and clinical studies have focussed on developing immunotherapy, whether active or passive, to better target protein aggregates 288,289.
25
Active immunotherapy involves the stimulation of the body’s own immune system to produce antibodies against an administered antigen. This approach is more natural, long lasting and requires only a few treatment sessions. However, active immunization can induce autoimmune reactions causing neuro-inflammation 290 and offers limited choice of epitopes and specificity 291,292.
Passive immunotherapy refers to the administration of externally synthesized antibodies to the body. The protection offered by foreign antibodies is instant, yet temporary and thus, requires continuous injections. Passive immunotherapy can be better controlled than active strategies, since antibodies can be engineered with a desired level of specificity to target only distinct strains of the disease-associated protein 288,293. Important biological barriers that determine effective therapeutic treatment are the passage through the blood brain barrier (BBB), blood spinal cord barrier and blood cerebrospinal fluid barrier. These barriers help maintain the CNS homeostasis by limiting the access of circulating molecules from the periphery 294. Among those barriers, the BBB is the most stringent one letting only 0.1-0.2% of circulating antibodies pass into the brain 295,296. Preferred methods of administering antibodies are intravenous or intraperitoneal (i.p.) injections, due to their relatively simple execution. To be able to pass the BBB in sufficient amounts, high doses of antibodies are required, because most of them are drained and eliminated via the peripheral blood stream 297. To overcome the poor penetration into the BBB, intra-cerebroventricular or intrathecal techniques administer antibodies directly into the CNS. However, these methods have raised concerns with respect to surgical methods and infection risks due to implanted catheters 298.
Both active and passive immunotherapeutic approaches are explored in several neurodegenerative diseases including AD, PD and tauopathies 288. Immunotherapies targeting Aβ, α-synuclein and tau have been shown to prevent protein aggregation and stimulate aggregate clearance in vivo. Consequently, this led to a reduction in the deposition of aggregated species and neurodegeneration 299. Furthermore, active immunization reduced the production of pro-inflammatory cytokines by stimulating a physiological microglial response 300-302. Despite the ongoing attempts and successes of immunotherapy in pre-clinical studies, translating these findings to the clinic has been of limited success. Notable examples are antibodies targeting Aβ including bapineuzumab and solanezumab. Following successful Phase 1 and 2 trials, both antibodies were abandoned after they did not show any clinical efficacy in a Phase 3 trial 303-305. A promising antibody is aducanumab, which is currently evaluated in a Phase 3 efficacy study (NCT02477800). Aducanumab recognizes aggregated Aβ and has been shown to decrease Aβ plaques in several brain regions in patients with mild AD 306.

26
Therapeutic interventions using either active immunization or antibody-based strategies have also been tested in mice models of SOD1-mediated ALS. Regarding active immunization, recombinant apo-SOD1G93A, apo-SOD1WT or a peptide corresponding to the amino acids 145-151 in the SOD1 sequence, were used as immunogens 307-309. All of these studies reported a therapeutic effect with a prolonged survival. However, the effect was dependent on the recipient transgenic mouse model. Survival was prolonged up to 40 days in the SOD1G37R transgenic mice, while the survival was extended by only a few days in the SOD1G93A mice expressing high levels of the transgene 307,309. In addition, one study reported adverse effects in the SOD1G93A low copy number mice, following active immunization using an antigenic peptide that targets the dimer interface of SOD1 310. In passive immunotherapeutic approaches, several mAbs have been administered by intracerebroventricular infusions into the SOD1G93A mice. These resulted in modest therapeutic effects with prolonged survival times 285,311. As an alternative route of administration, mAbs have also been delivered through i.p. injections. A substantially prolonged survival was only observed in the low copy number and slow progressing hSOD1G37R transgenic mouse model 311. Taken together, these data highlight the need for a better understanding of ALS disease mechanisms in order to develop effective therapeutic interventions in ALS.
27
Aims of this thesis
The general aim of this thesis was to use antibodies as tools to study disordered and aggregated SOD1 species in different ALS model systems and investigate their potential as therapeutic agents. The specific aims were to:
• Analyze misfolded SOD1 in patient-derived cell models with physiological levels of SOD1 expression
• Investigate the effects of low oxygen tension on soluble and aggregated misfolded SOD1 levels in patient-derived models
• Optimize methods to study misfolded SOD1 in post mortem tissues from SOD1-ALS patients and sporadic ALS cases
• Validate novel conformation-specific antibodies for their reactivity to disordered and aggregated SOD1 species in vitro and in vivo
• Investigate whether passive immunization can neutralize the spread of
SOD1 aggregates and slow disease progression in a mouse model of prion-like transfer of SOD1 pathology

28
Materials and Methods
In the following section, I will summarize the key materials and novel methods applied in this thesis. The reader is referred to the materials and methods of Paper I–IV for standard techniques and detailed descriptions of experimental set ups.
Human materials Studies involving human subjects were performed in accordance with the ethical principles for medical research defined in the Declaration of Helsinki (WMA, 1964) and approved by the appropriate national ethical review boards in Sweden (EPN at Umeå University, DNR 2014-17-31M and DNR 2014-137-31M) and Canada (ERB at CHU de Québec. Protocol number: 2012-1316).
Patient and control samples were obtained following a written informed consent for study participation from each donor. Cell lines included in Paper I and II were provided through a collaboration between Project ALS at Umeå University, Prof. Christopher E. Henderson’s lab at Colombia University and Prof. Kevin Eggan’s lab at Harvard University following material transfer agreements established between the affiliated institutions.
Cell cultures All cell lines were maintained at 37°C in a humidified incubator with 5% (v/v) CO2 supply. Cells were cultured with media components supplied by Thermo Fisher Scientific, unless otherwise stated. A summary of all cell types included in this thesis is illustrated in Figure 6. Human fibroblasts Fibroblast cell lines were established from skin biopsies taken from the upper arm of ALS patients and healthy controls with a 3 mm punch. Patient-derived fibroblasts were positively genotyped for ALS-linked mutations in SOD1, FUS, TBK1, TARDBP, ANG and C9ORF72 and were heterozygous for their respective mutation. The homozygous SOD1D90A patient was the only exception. The control fibroblast lines were generated from unaffected family members of ALS patients and were negative for any identified mutation in ALS associated genes. Paper I includes further a sporadic ALS patient line and an isogenic control line where the SOD1A4V mutation was genetically modified to wild type 214.
In Paper I, fibroblast cells were cultured in Dulbecco's Modified Eagle Medium (DMEM) supplemented with fetal bovine serum (FBS), L-glutamine and Penicillin-Streptomycin. In Paper II, fibroblast cells were cultured in
29
Roswell Park Memorial Institute (RPMI) 1640 medium supplemented with FBS, L-glutamine and penicillin (Meda).
Induced pluripotent stem cells IPSCs were generated from fibroblasts using different reprogramming strategies based on either retroviral transduction of the Yamanaka factors (Paper I) 214,312-
314, nucleofection of episomal vectors (Paper II) 315 or mRNA reprogramming (Paper II; material: Stemgent; Service: Takara Bio Europe AB). All iPSCs were maintained as a monolayer in the DEF-CS Culture System (Takara Bio Europe AB) until analysis or initiation of differentiation. iPSC-derived motor neurons IPSCs were differentiated to motor neurons using either 2D or 3D protocols. Both differentiation strategies are optimized to generate motor neurons with a limb-innervating phenotype 211,316. In addition, these motor neuron cultures contain proliferating astrocytes and are subsequently referred to as iPSC-derived motor neuron and astrocyte cultures (MNACs).
The protocols vary in cell culture dimension, media composition, duration of patterning phases and neuronal maturation 209. The 3D differentiation protocol stimulates the formation of embryonic bodies (EBs) in suspension cultures. Cells were neuralized by dual-SMAD inhibition using SB431542 (Sigma Aldrich) and LDN193189 (Stemgent) 210 and treated with retonic acid (RA) to stimulate the spinal cord identity. Purmorphamine (Stemgent) was used to convert spinal precursors to motor neuron progenitors. Neurotrophic factors including BDNF, CTNF, GDNF and IGF1 were added to promote neurogenesis, maturation and survival. After 31 days of differentiation, EBs were dissociated and resulting MNACs were further matured for up to 12 days before analysis.
2D differentiation was initiated on adherent iPSCs by dual-SMAD inhibition using SB431542 (Sigma Aldrich) and LDN193189 (Stemgent). Neural progenitors were exposed to RA and the hedgehog agonist SAG (Sigma Aldrich) to direct neural progenitors towards a spinal identity and induce motor neuron patterning. Neurogenesis was induced by exposure to the Notch inhibitor DAPT (Selleck Chemicals) and the fibroblast growth factor (FGF) signalling inhibitor SU5402 (Sigma Aldrich). After 14 days of differentiation, MNACs were dissociated to single cells and matured for 10 days before analysis. iPSC-derived astrocytes Astrocytes were isolated from 3D-differentiated MNACs by exchanging media to DMEM supplemented with FBS, B-27 Supplement minus antioxidants, L-glutamine, NEAA and heparin 317. MNACs were passaged and maintained in this media until cultures were only positive for proliferating astrocytes.
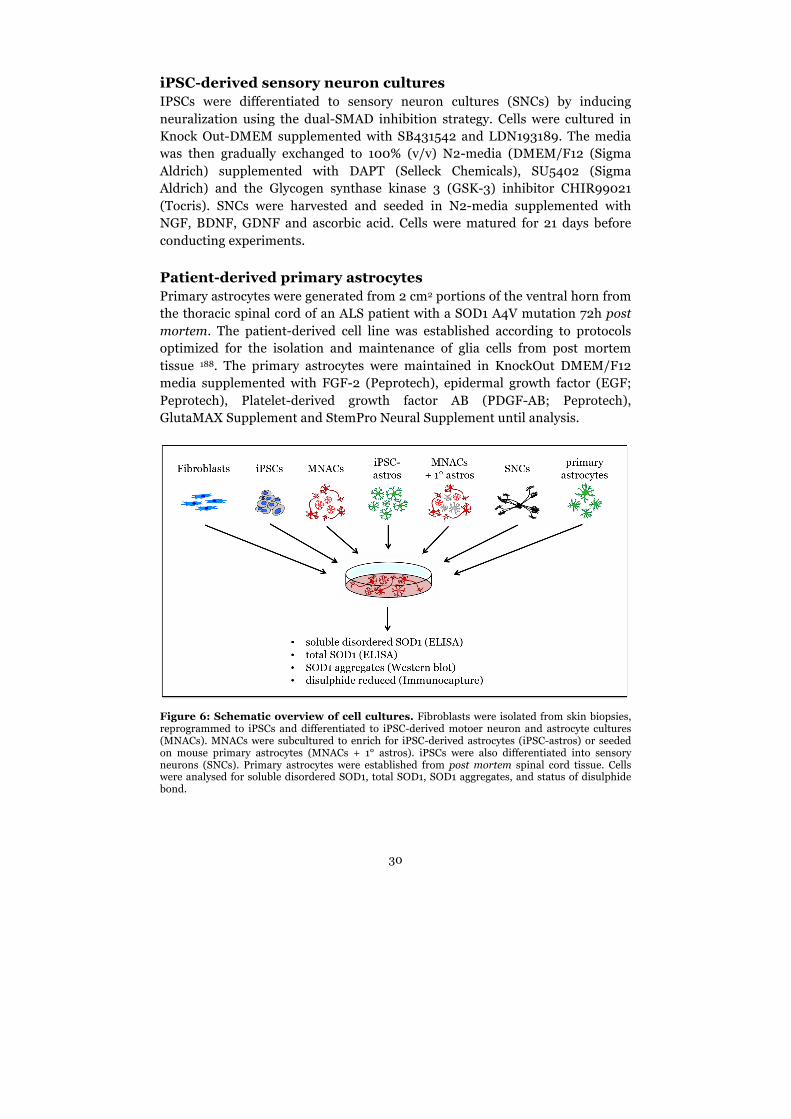
30
iPSC-derived sensory neuron cultures IPSCs were differentiated to sensory neuron cultures (SNCs) by inducing neuralization using the dual-SMAD inhibition strategy. Cells were cultured in Knock Out-DMEM supplemented with SB431542 and LDN193189. The media was then gradually exchanged to 100% (v/v) N2-media (DMEM/F12 (Sigma Aldrich) supplemented with DAPT (Selleck Chemicals), SU5402 (Sigma Aldrich) and the Glycogen synthase kinase 3 (GSK-3) inhibitor CHIR99021 (Tocris). SNCs were harvested and seeded in N2-media supplemented with NGF, BDNF, GDNF and ascorbic acid. Cells were matured for 21 days before conducting experiments. Patient-derived primary astrocytes Primary astrocytes were generated from 2 cm2 portions of the ventral horn from the thoracic spinal cord of an ALS patient with a SOD1 A4V mutation 72h post mortem. The patient-derived cell line was established according to protocols optimized for the isolation and maintenance of glia cells from post mortem tissue 188. The primary astrocytes were maintained in KnockOut DMEM/F12 media supplemented with FGF-2 (Peprotech), epidermal growth factor (EGF; Peprotech), Platelet-derived growth factor AB (PDGF-AB; Peprotech), GlutaMAX Supplement and StemPro Neural Supplement until analysis.
Figure 6: Schematic overview of cell cultures. Fibroblasts were isolated from skin biopsies, reprogrammed to iPSCs and differentiated to iPSC-derived motoer neuron and astrocyte cultures (MNACs). MNACs were subcultured to enrich for iPSC-derived astrocytes (iPSC-astros) or seeded on mouse primary astrocytes (MNACs + 1° astros). iPSCs were also differentiated into sensory neurons (SNCs). Primary astrocytes were established from post mortem spinal cord tissue. Cells were analysed for soluble disordered SOD1, total SOD1, SOD1 aggregates, and status of disulphide bond.
31
SOD1 transgenic mice Studies including transgenic mice overexpressing different mutant hSOD1 variants were approved by the Regional Ethics Committee for Animal Research at Umeå University (DNR A9-15 and A10-15). Mice were maintained at a 12 h light/dark cycle with food and water ad libitum and sacrificed at preselected ages or when end-stage was reached. End-stage was defined when mice were no longer able to reach food due to severe paralysis of the limbs and/or lost more than 25% body weight.
As described earlier, the genetic background is of great importance with regards to phenotype and onset 225. Mice used in this thesis were inbred for more than 30 generations with the C57BL/6JBomTac strain (B6) (Taconic Europe). The hemizygous hSOD1G93A model used in our laboratory is a sub-strain of the aforementioned G1 line. These mice incorporated about 25 copies of the transgene and due to the higher expression, develop a more aggressive disease than the founder model. In our laboratory, the first signs of motor impairment appear at around 90 days of age and the average lifespan of this mouse model is 135 days. The hemizygous hSOD1G85R strain (line 148) utilized in this thesis expresses approximately 57 % less hSOD1 mRNA than the hSOD1G93A strain 318, while hSOD1G85R protein levels are comparable to the endogenous mouse SOD1 levels (1-fold) 114. In our laboratory, the average life span of hSOD1G85R mice is 406 days, in contrast to the 200 days of the templated prion-like spread mouse model based on the hSOD1G85R strain 173. Non-transgenic littermates from the hSOD1G85R breeding or pure B6 mice were included as controls.
Antibodies against misfolded SOD1 Rabbit pAbs were generated against different hSOD1 variants, including native SOD1 purified from human erythrocytes (Marklund 1997), full-length apo-SOD1 and various peptides covering 90 % of the human wild-type SOD1 sequence 130,132,319. Antibodies against native SOD1 and full-length apo-SOD1 have been purified using Protein A or G chromatography. The anti-peptide antibodies were purified against the corresponding peptides coupled to Sulfolink gel (Pierce) 130. Antibodies directed against amino acids 24-39, 57-72 and 131-154 of hSOD1WT (SOD124-39, SOD157-72, SOD1131-154) showed the highest sensitivity in most applications and are used in this thesis.
Mouse mAbs were generated against peptides corresponding to amino acids 57-72 and 131-153 of the human SOD1WT sequence using hybridoma technology. For each SOD1 epitope, two antibodies were chosen for further in vitro analyses and belonged either to the IgG1 (mAb 5.7; mAb 85.11) or IgG2b (mAb 134.2; mAb 545.2) subclass.

32
All mAbs utilized in this study were produced from hybridoma cells maintained in HyClone SFM4MAb-Utility media (GE Healthcare) in CL1000 bioreactors (Argos). Antibodies were purified using HiTrap MabSelect SuRe columns (GE Healthcare). Buffers and consumables were endotoxin free and each purified antibody batch was tested for endotoxin levels using a kinetic chromogenic endpoint assay (Limulus amebocyte lysate; PharmaControl). Batches with detectable endotoxin levels of 1,0 EU/ml or higher were not used for in vivo injections. Antibodies were diluted in endotoxin-free Dulbecco Phosphate Buffered Saline (DPBS, Invitrogen) and stored in appropriate endotoxin free vials at -80°C until use. The monoclonal anti-hSOD1 antibody C4F6 320 was a kind gift from Dr. François Gros-Louis, Canada.
Immunocapture Misfolded hSOD1 species were immunocaptured with SOD1 antibodies cross-linked to Dynabeads M-270 Epoxy (Invitrogen). Potentially, all antibodies specific for misfolded SOD1 could be used, but pAb SOD124-39 and SOD157-72 (Agrisera) as well as the mAb C4F6 antibody (Medimabs) showed the highest sensitivity to soluble misfolded SOD1 in this particular assay.
Samples were prepared in phosphate-buffered saline (PBS, pH 7.0) with an ionic strength (150 mM NaCl) that mimics physiological conditions. The buffer was supplemented with the protease inhibitor cocktail Complete without Ethylenediaminetetraacetic acid (EDTA) (Roche) and the non-ionic detergent Nonidet P-40 (NP-40, Roche). Additionally, iodoacetamide (IAM, Sigma Aldrich) was used to prevent the formation of artificial disulfide bonds via irreversible alkylation of the free SH group of cysteine.
Antibody-coated beads were incubated with cell extracts (20.000 xg fraction) or spinal cord extracts (1.000 xg fraction) and after sufficient washing cycles, misfolded SOD1 was eluted and analysed by western blots. Unbound fractions of cell lysates have been additionally analysed by ELISA to determine the efficiency of the immunocapture method.
Immunohistochemistry Patient tissues samples from several brain and spinal cord regions as well as mouse spinal cord tissue were immersion-fixed and embedded in paraffin. Paraffin blocks were sectioned at a thickness of 10 µm (human tissue) or 4-6 µm (mouse tissue), deparaffinized, and subjected to antigen retrieval and primary antibodies. Sections were stained with the automated BenchMark Ultra (Ventana Tucson) and optimal antigen retrieval conditions and working concentration were determined for each antibody. The primary antibodies were detected with the ultraView Universal DAB detection kit (human tissue) or iView Universal DAB detection kit (Ventana Tucson) (mouse tissue).
33
All sections were counterstained with haematoxylin, dehydrated and mounted with Pertex (Histolab).
Passive Immunotherapy The prion-like ALS model was used to investigate the efficacy of mAbs in vivo. The model is based on the inoculation of isolated hSOD1G85R aggregate seeds into the lumbar spinal cord of pre-symptomatic SOD1G85R transgenic mouse 173. This induces a prion-like templated spread of SOD1 aggregation causing premature onset and aggressive progression of fatal motor neuron disease. The mAbs directed against epitopes SOD157-72 (mAb 134.2) and SOD1131-153 (mAb 85.11) as well as control antibodies, a mouse polyclonal IgG-mix and mAb IgG1 (anti-c-myc; clone 9E10) were i.p. injected into hSOD1G85R mice. Parameters such as antibody concentration, starting point and frequency of administration as well as inoculation of hSOD1G85R aggregates varied according to the experimental set up. For example, antibodies injections started three weeks before hSOD1G85R aggregates were inoculated to achieve a baseline antibody titre. Antibodies were continuously injected once per week until mice reached end-stage as defined above. In another experimental set up, antibodies were pre-incubated with hSOD1G85R aggregates before inoculation into the spinal cord.
Circulating antibody titres were assessed from all mice by collecting submandibular bleedings at predefined stages from all mice. The spinal cord and brain were dissected, divided into left/right, and analysed either by IHC or immunoblotting using western blotting and dot blotting. For more details on the individual experiments see Paper IV.

34
Results
Paper I Enhanced protein misfolding in patient-derived models of amyotrophic lateral sclerosis Aggregates containing misfolded SOD1 are characteristically found within motor neurons and astrocytes in SOD1 ALS patients as well as in transgenic mice overexpressing mutant hSOD1 or hSOD1WT 118,318. SOD1 aggregates are also found in non-SOD1 and sporadic ALS patients 130,132. Analysis of ALS models revealed that these large SOD1 aggregates appear relatively late in the disease process, at a time when symptoms, such as limb tremor and paresis, become already apparent 122,223. However, morphological and physiological abnormalities can be detected before macroscopic SOD1 aggregates appear 219,321-325. Electrical properties of motor neurons in hSOD1G93A mice exhibit alterations shortly after birth 326,327 and aberrant activation of glial cells can be found before symptom onset 328. These suggest that other toxic SOD1 species than the large, insoluble SOD1 aggregate arise earlier in the disease 45,329,330.
Due to the limited availability of patient material, it is unclear how closely these findings translate to the human disease. Most studies of mutant SOD1 toxicity have been conducted with transgenic models requiring overexpression of mutant hSOD1. High levels of SOD1 expression promote abnormal protein interactions 331 and this could mislead our understanding of ALS pathogenesis. Therefor, patient-derived in vitro models of ALS, where SOD1 is expressed at physiological levels would be useful to help dissect the molecular pathogenesis of SOD1 ALS.
The aim of this study was to quantify the levels of disordered SOD1 species in patient-derived cells and to see whether their levels were specifically enhanced in disease-susceptible cell types, such as motor neurons and astrocytes. We analysed cell lines from patients with mutations in SOD1, other ALS-linked genes as well as sporadic ALS. In addition, we examined cell lines from two non-disease controls and mouse ESC-derived motor neuron cultures overexpressing SOD1WT or hSOD1G93A (Paper I, Supplemental Table 1). To study disordered SOD1 in cell types more relevant to ALS, we differentiated patient-derived iPSCs to a mixed population of mature motor neurons and astrocytes based on previous reports 312,313,316. To obtain pure astrocyte cultures, we expanded MNACs in media containing serum as previously described 317. The levels of soluble disordered SOD1 were quantified from cell extracts via an enzyme-linked immunosorbent assay (ELISA). This ELISA utilizes the conformation-specific pAb hSOD124-39, which specifically detects disordered and misfolded hSOD1 and does not react with native forms of human or mouse SOD1 319.
35
The same antibody was used in immunocapture experiments to study the disulphide status of disordered SOD1. Detergent-insoluble SOD1 aggregates were evaluated by western blotting using the pAb hSOD157-72.
We first quantified the baseline levels of disordered SOD1 in different cell types from two non-disease control lines expressing SOD1WT only. Non-neuronal fibroblasts and iPSCs showed low, but comparable levels of disordered SOD1 in both control lines. In contrast, MNACs showed significantly higher levels of disordered SOD1 indicating an increased destabilisation of SOD1WT even in the absence of a SOD1 mutation (Figure 1B in Paper I). These results suggest further that disordered SOD1 is higher in cell types affected by ALS.
Analysis of disordered SOD1 was then expanded to a number of different ALS patient-derived MNACs as well as to mouse MNACs overexpressing SOD1. Sporadic ALS and non-SOD1 familial ALS patient lines exhibited levels of disordered SOD1WT similar to those detected in non-disease control MNACs and mouse MNACs overexpressing SOD1WT (Figure 2B in Paper I). In contrast, patient-derived MNACs carrying SOD1 mutations showed significantly increased levels of disordered SOD1 over non-disease controls. The levels were even further enhanced in mouse MNACs overexpressing SOD1G93A.
Ideally, patients and non-disease controls should be matched as closely as possible. Hence, siblings or partner to a patient are often used. This approach is thought to minimize confounding variables, such as different genetic backgrounds and unknown effects of environmental factors. However, iPSC clones from different individuals can be highly variable and efficiency of neuronal differentiation may vary between different clones derived from the same patient 332,333. Hence, the most suitable controls for genetic diseases are the patient’s own cells in which the disease causing mutation has been corrected to wild type. Gene-editing technology enables the generation of such “isogenic” controls by genetic correction of mutations in the human genome 334. We utilized iPSCs from an SOD1A4V patient and its isogenic control in order to determine whether disordered SOD1 levels were dependent on the SOD1 mutation or were due to other unknown factors 214,215. ELISA analysis showed elevated levels of disordered SOD1 in MNACs carrying the SOD1A4V mutation compared to its isogenic control (Figure 2D in Paper I). This suggests that variations in disordered SOD1 levels arise due to the mutation. The SOD1A4V and its isogenic control iPSCs were further differentiated to sensory neuron cultures (SNCs) in order to establish whether enhanced levels of disordered SOD1 were a specific feature of motor neurons. We detected significantly lower levels of disordered SOD1 in SNCs in both lines, reinforcing the earlier observation that increased amounts of disordered SOD1 are a distinct characteristic of MNACs.
MNACs consist of a heterogeneous mixture of neurons, motor neurons and proliferating astrocytes. Although the degeneration of motor neurons is a pathological hallmark of ALS 10,49, astrocytes are also actively involved in the disease 188,335-337.
36
To assess levels of disordered mutant SOD1 in astrocytes separate from motor neurons, we established pure iPSC-derived astrocyte cultures (iPSC-astros) from MNACs expressing mutant SOD1. We also enriched motor neurons from MNACs by seeding newly differentiated MNACs on a confluent layer of mouse primary astrocytes and thereby supressing the growth of human astrocytes in the culture (Figure 3A in Paper I). Analysis of these cultures revealed significantly increased levels of disordered SOD1 in iPSC-astros compared to their corresponding MNACs. In contrast, motor neurons grown on primary mouse cells exhibited lower levels of disordered SOD1 compared to mixed MNACs. This suggests that iPSC-astros were mainly responsible for the high levels of disordered SOD1 in MNACs.
Soluble disordered SOD1 monomers are the building blocks for SOD1 aggregates in vitro and in vivo 146,151,338. Furthermore, these monomeric SOD1 species lack the intrasubunit disulphide bond, which is important for protein stability 91,96,185. To ascertain the nature of soluble disordered SOD1 in our ALS patient-derived cells, we utilized size exclusion chromatography (SEC) and immunocapture methods. SEC analysis revealed that the majority of disordered mutant SOD1 in patient-derived MNACs had an apparent molecular mass of 55 kDa representing highly disordered, monomeric SOD1 species (Figure 4A in Paper I). This coincides with results obtained in several transgenic mouse models overexpressing mutant SOD1 339, confirming for the first time that soluble disordered SOD1 exists in the same form in patient-derived cells is it does in mouse models. Immunocapture experiments supported this by showing that all disordered SOD1 in MNACs was disulphide reduced (Figure 4B in Paper II). Hence, soluble disordered SOD1 species in patient-derived MNACs exists as disulphide-reduced monomers. We then quantified detergent-insoluble SOD1 aggregates in extracts from MNACs to study the relationship between soluble and aggregated SOD1 species. While very low levels of aggregation were detected in non-disease control and isogenic control lines, MNACs expressing SOD1A4V showed higher levels of SOD1 aggregates (Figure 4C in Paper I). In contrast, MNACs expressing SOD1G85S had comparable levels of aggregation to control lines. However, this particular ALS patient-line showed very high levels of soluble disordered SOD1 indicating that levels of soluble disordered SOD1 do not necessarily correlate with the level of aggregated SOD1 in MNACs.
In summary, this study validated the utility of patient-derived model systems to study SOD1-driven ALS pathology. Our approach of using patient-derived iPSC cells combined with antibody-based analyses enabled us to demonstrate that human SOD1 is more disordered in MNACs and astrocyte cultures than other cell types. Disordered SOD1 species existed as disulphide-reduced monomers. This will help in our mechanistic understanding of SOD1 aggregation when translating between results gained in mouse and human SOD1 ALS models. Our findings also suggest that iPSC-derived models are suitable tools to study the selective vulnerability of the motor system to the

37
ubiquitously expressed SOD1 protein. They could further help to bridge the gap between successful animal studies and clinical trials by using them to validate results in the context of human cells bearing patient-specific mutations.
Paper II The molecular pathogenesis of superoxide dismutase 1-linked ALS is promoted by low oxygen tension
The central nervous system requires a constant supply of oxygen to meet its high energetic demands. Reduced vascular perfusion due to ageing or pathological conditions such as stroke, can lead to either temporary or chronic local deprivation of oxygen and induce cell death 54,340,341. Beside its vital role in energy production during cellular respiration, oxygen is also crucial for the formation of disulphide bonds, which are post-translational modifications required for the correct folding and maturation of most newly synthesized proteins, including SOD1. The intrasubunit disulphide bond in SOD1 is formed through oxidation of the thiol groups in C57 and C146 and the reaction is primarily catalysed by CCS 90,91,342. The formation of the bond stabilizes monomeric SOD1 and facilitates its dimerization, maturation, and activation. Absence of the disulphide bond promotes conformational changes in SOD1 leading to disordered and misfolded SOD1 species in vitro 104,119,146,338,343. Disulphide-reduced SOD1 monomers are further substrates for aggregation and the principal substrate for aggregates in vitro and in vivo 122,146,344. Native SOD1 is an extremely stable protein predominantly found in the cytosol 345, which is an energetically reducing environment and thus, does not favour oxidized disulphide bonds 346. Hence, preservation of the bond could be a weakness of the otherwise stable SOD1 protein 95. Furthermore, the availability of oxygen could affect the formation of the disulphide bond in SOD1 and thereby affect the protein stability.
The aim of this study was to investigate the role of lowered oxygen tensions on the redox status of the SOD1 disulphide bond using conformation-specific SOD1 antibodies. We analysed levels of soluble disordered and aggregated misfolded SOD1 in patient-derived fibroblasts, MNACs and primary astrocytes. Cells were cultured under different oxygen concentrations ranging from the standard atmospheric concentrations (19% oxygen) down to hypoxic conditions (1% oxygen). Disordered SOD1 was then analysed using the same ELISA, immunocapture and western blotting methods as in Paper I.
We first explored the effect of different oxygen tensions on SOD1 stability in selected patient-derived fibroblast lines. Fibroblasts carrying full-length mutant SOD1 showed a dose-dependent increase of soluble disordered SOD1 with the strongest response at 1% oxygen for 24 hours (Figure 2A in Paper II). There was no increase observed in the fibroblast line carrying a SOD1G127X
38
mutation. This mutation introduces a premature stop codon and results in a truncated protein that lacks C146 and consequently, cannot form the disulphide bond. This suggests that enhanced disordered SOD1 in response to hypoxic conditions is dependent on the presence of the C57-C146 disulphide bond. Elevated levels of disordered SOD1 could already be detected after 4 hours exposure to 1% oxygen and reached a plateau after 8 hours. (Figure 2B in Paper II). Upon returning fibroblast cultures back to 19% oxygen, the levels of disordered SOD1 returned to baseline levels after approximately 1 hour. Hence, the enhanced levels of disordered SOD1 in response to low oxygen were not only dose- and time-dependent, but also reversible. Analysis of a wide range of SOD1 mutant fibroblast lines cultured under 1% oxygen revealed increased levels of soluble disordered SOD1 in all that carried full-length SOD1 mutant protein. This was also seen in non-SOD1 familial ALS and control lines, which only express SOD1WT (Figure 3a in Paper II). Fibroblast lines carrying C-terminal truncated SOD1 mutations, (SOD1G127X, SOD1D125Tfs*24), did not show enhanced levels of disordered protein when cultured under hypoxic conditions. Similar to SOD1G127X, SOD1D125Tfs*24 lacks C146 and cannot form the disulphide bond. Hence, this result confirmed the earlier observation that the response requires the C57-C146 disulphide bond.
Since the motor system is the primary target of ALS, we next wanted to investigate the SOD1 response to low oxygen tension in patient-derived cells more relevant for the disease. Hence, primary astrocyte cultures were established from the thoracic spinal cord of an ALS patient carrying the SOD1A4V mutation 72 hours post mortem. The cells stained positive for the astrocyte marker S1oo calcium-binding protein B (Figure S2 in Paper II). Upon exposure to low oxygen conditions (1% for 24 hours), the soluble disordered SOD1 level increased similar to the levels seen in fibroblasts from another SOD1A4V patient (Figure 2D in Paper II). Hence, we could confirm that low oxygen treatment affects SOD1 stability by using primary cells derived from the CNS of an ALS patient. We then analysed iPSC-derived MNACs cultured under different oxygen concentrations. Similar to fibroblasts, we observed a dose-dependent increase in soluble disordered SOD1 when cultured under lowered oxygen concentrations. However, exposure of MNACs to 1% oxygen for 24 hours caused axonal fragmentation, which was not observed at 2% oxygen for the same period. Furthermore, cells cultured with 2% oxygen showed no signs of cellular toxicity as assessed by cellular ATP levels and cell viability. Hence, 2% oxygen for 24 hours was chosen as the optimal conditions for studying the effect of low oxygen tension on disordered SOD1 levels in MNACs. The levels of soluble disordered SOD1 at 19 % oxygen were higher in MNACs compared to the corresponding fibroblast lines (Figure 4 in Paper II). The effect was also observed in control lines expressing only SOD1WT and in MNAC lines carrying truncated SOD1 mutants that lack the C57-C146 disulphide bond.
39
Based on our findings in Paper I, these observations are likely to reflect the result of increased levels of disordered SOD1WT in MNACs compared to fibroblasts.
Previous studies in SOD1 transgenic mice have shown that soluble disordered SOD1 lack the stabilizing disulphide bond 318,339. To determine the proportion of disulphide-reduced to -oxidized SOD1 in our patient-derived cell models, we analysed MNACs extracts by non-reducing western blots and immunocapture. In both approaches, the alkylating agent IAM was added to preserve the status of the disulphide bond at the time of harvest. In addition, reducing agents such as dithiothreitol (DTT) or β-mercaptoethanol where omitted from all buffers in order to maintain the bond. Due to the different mobilities in non-reducing PAGE, disulphide-reduced and -oxidized SOD1 species can be distinguished by western blotting. Exposure of MNACs to 2% oxygen for 24 hours resulted in an increased proportion of disulphide-reduced SOD1 in both MNACs expressing mutant SOD1 and non-disease control lines carrying only SOD1WT SOD1. This was supported by immunocapture experiments using pAb SOD124-39, which specifically binds to disordered hSOD1 species, regardless of the disulphide status. The proportion of disulphide-reduced, disordered SOD1 increased considerably in MNAC lines expressing mutant SOD1 compared to non-disease control lines. These results provide further evidence that all disordered SOD1 species are disulphide-reduced. However, the majority of disulphide reduced SOD1 maintains a native, ordered structure, even in MNACs expressing mutant SOD1.
Elevated levels of disordered SOD1 in response to low oxygen could be a result of impaired formation of disulphide bonds in newly synthesized SOD1 proteins or due to reduction of disulphide bonds in the mature protein. The formation of the disulphide bond is catalysed by CCS in association with copper loading during the SOD1 maturation process. Reduction of the bond is performed by glutaredoxin and its co-factor glutathione, which exists in two states 347. The reduced form of glutathione (GSH) participates directly in the neutralization of reactive oxygen species and thereby, protects cells from oxidative stress. The oxidized form of glutathione (GSSG) is generated from two reactive GSH molecules either by reduction by peroxidases, or by disintegrating disulphide bonds 348. Hence, the ratio of GSH to GSSG can be used as an analytical method to assess disturbances in redox metabolism.
We analysed levels of CCS, glutaredoxin-1, GSH, and GSSG in extracts from fibroblasts and MNACs to determine whether they corresponded with increased levels of disordered SOD1 following low oxygen exposure. There were no detectable changes in CCS or glutaredoxin-1 levels as determined by western blotting. Although the concentrations of GSH and GSSG were higher in MNACs than fibroblasts, the ratios of GSH/GSSG were not affected by low oxygen tension in either fibroblast or MNACs (Figure 6 in Paper II). These results
40
indicate that low oxygen tensions do not induce disordered SOD1 by altered levels of CCS, glutaredoxin-1 or by disturbances of the GSH/GSSG redox couple.
To further investigate whether increased levels of disordered SOD1 were a result of impaired disulphide bond formation, or due to reduced stability of existing protein, we inhibited protein synthesis during oxygen treatment experiments in fibroblasts. We observed a slight increase in disordered SOD1 levels in control lines expressing SOD1WT at both oxygen concentrations. The effect was more pronounced in the SOD1G93A fibroblast line with a significant reduction in disordered SOD1 at both oxygen concentrations. This suggests that a proportion of disordered SOD1 comes from impaired formation of the disulphide bond due to a reduced availability of oxygen. However, the results also suggest that oxygen is required for maintaining the bond in mature SOD1, since the response was enhanced at 1% oxygen in the present of the protein synthesis inhibitor. (Figure 7 in Paper II).
It has previously been shown that disulphide-reduced and misfolded SOD1 lead to aggregation in vitro 146,338,343 as well as in vivo 122,344. To study the effect of low oxygen treatment on aggregate formation in our patient-derived cell models, we quantified detergent-insoluble aggregates in extracts from fibroblasts and MNACs. The level of aggregation was low in fibroblasts and did not increase in response to reduced oxygen concentrations. Similar results were observed in MNACs carrying SOD1WT or the SOD1L117V mutation, which exhibits wild type like stability. Furthermore, there was no increase in aggregation in MNACs carrying SOD1 mutations that impede the formation of the disulphide bond. In contrast, MNACs expressing full-length mutant SOD1 showed significant increases in aggregation upon low oxygen exposure. These results indicate a close correlation between increased levels of disordered SOD1 and enhanced aggregation in MNACs expressing full-length mutant SOD1s.
In conclusion, this study provides evidence for the importance of oxygen tensions on SOD1 stability. Using conformation-specific anti-peptide SOD1 antibodies, we showed that low oxygen concentrations lead to increased disulphide reduction and disordered SOD1 in various patient-derived cell types. Furthermore, enhanced disordered SOD1 promoted aggregation in MNACs but not in fibroblasts. This suggests that CNS areas with low oxygen supply could be the original initiation sites of SOD1 aggregation. Hence, conditions causing compromised vascular perfusion could contribute to the initiation as well as to the progression of ALS.
41
Paper III Misfolded SOD1 pathology in sporadic amyotrophic lateral sclerosis Aggregates of misfolded mutant SOD1 are considered a pathological hallmark of familial ALS carrying SOD1 mutations. However, previous work from our group as well as others have shown that misfolded SOD1WT aggregates are also present in motor neurons and glia cells in post mortem tissue from sporadic ALS patients and familial cases expressing other ALS-linked mutations 130-133,311,349. Studies in mouse models overexpressing SOD1WT support these findings, where misfolded SOD1WT aggregates accumulate in the CNS in association with neuronal pathology in aged mice 115,125,126,223,285,344,350,351. These results indicate that SOD1WT is able to adopt aberrant conformations and is involved in ALS pathogenesis 118. Several other studies have reported that misfolded SOD1 WT is not present in sporadic ALS patients 136,137,320,352 and concluded that the protein is not involved in the disease. This discrepancy could be due to differences in the methodology used to detect misfolded proteins. IHC is commonly performed to visualize the distribution and extent of misfolded SOD1 aggregates in post mortem tissue sections. However, the different steps required for an IHC protocol in fixed tissue imposes various limitations such as sensitivity and detection limits of the antibodies used. Immunocapture using antibodies is used to isolate misfolded SOD1 from tissues and validate their presence. Studies that investigated aggregates of misfolded SOD1WT in spinal cord tissue have relied upon a number of different polyclonal or monoclonal conformation-specific antibodies. These antibodies recognize epitopes in the misfolded protein that are not recognized in the native SOD1. Therefore they are able to detect disordered SOD1 species but not the natively folded protein.
The aim of this study was to optimize the IHC and immunocapture protocol for several conformation-specific antibodies. We then used these methods to investigate the presence and distribution of misfolded SOD1WT in several brain and spinal cord tissues from a number of sporadic ALS patients using conformation-specific antibodies. CNS tissue sections from 13 sporadic ALS patients without SOD1 mutation were analysed and compared to a SOD1A4V
patient and 4 control patients (2 neurological, 2 non-neurological). Five different antibodies were utilized in our IHC study including the pAb raised against hSOD14-20, hSOD124-39, hSOD157-72, hSOD1131-153, and mAb C4F6. The pAb hSOD124-39 and mAb C4F6 antibody were used to evaluate disordered SOD1 species by immunocapture.
Initially, we optimized the IHC conditions for each of the five antibodies with respect to antigen retrieval time and working dilution in spinal cord sections from the SOD1A4V patient and 2 non-neurological controls. We standardized the protocols for each antibody using an automated IHC machine. All five antibodies detected aggregated misfolded SOD1 in the cytoplasm of
42
motor neurons. Aggregates were also observed in axons, dendrites and neutrophils (Figure 1 in Paper III). In contrast, no staining was seen in the control specimen, confirming that the antibodies reacted specifically with SOD1 in a patient with ALS. Using the optimized IHC conditions, tissue sections from the sporadic ALS patients were analysed. This revealed the presence of SOD1-positive staining in all evaluated tissue sections from all sporadic ALS patients. We identified several different SOD1-positive staining patterns, which were independent of the antibody used (Figure 3 in Paper III). The most frequently observed pattern was diffuse cytoplasmic staining in motor neurons. We also found small, granular aggregates dispersed throughout the cytoplasm of motor neurons. Furthermore, we detected inclusions in dendrites and axons and ring-like structures surrounding corpora amylacea-like structures within the anterior horn of the spinal cord. These different staining patterns were not always detected together in the same section with each antibody. Hence, it was decided that more than two sections per region had to display at least two staining patterns in order for a sporadic ALS patient to be declared positive for misfolded SOD1WT aggregates. Based on these criteria, we found that misfolded SOD1 was present in all 13 sporadic ALS cases (Table S1 in Paper III). In contrast, no SOD1 staining was detected in spinal cord and brain tissues from the neurodegenerative control patients. The same was true for the non-neurological controls. This indicated that, using an optimized IHC protocol misfolded SOD1WT was specifically and consistently detected in sporadic ALS patients.
To validate the presence of misfolded SOD1 in sporadic ALS patients and support the results gained via IHC, we also performed immunocapture experiments from homogenates of unfixed and frozen lumbar spinal cord. Initial comparison of all five antibodies revealed that mAb C4F6 and pAb SOD124-39 were the most sensitive for this application. The amount of immunocaptured misfolded SOD1 was normalized to total amount of SOD1 present in the input sample as determined by western blot. Variable levels of misfolded SOD1WT were detected amongst the six sporadic ALS cases analysed (Figure 6 in Paper III). The amounts of misfolded SOD1 were lower than those found in the SODA4V patient. However, all sporadic ALS cases exhibited higher levels of misfolded SOD1WT than the non-neurological control case. These results supported the IHC observations that misfolded SOD1WT is present in all sporadic ALS cases.
In summary, we optimized and validated the sensitivity of IHC and immunocapture methods to detect misfolded SOD1WT in sporadic ALS patients. Due to low levels of misfolded SOD1WT, detection in sporadic ALS post mortem tissue is associated with several methodological challenges. Our IHC approach identified misfolded SOD1 staining in all sporadic ALS cases, but not in any of the control samples. These results were supported by the immunocapture experiments, suggesting that misfolded SOD1WT species may be characteristic

43
for all forms of ALS. Our standardized approaches could help to clarify whether or not misfolded SOD1 is detected in other non-SOD1 ALS cases by re-analysing tissue samples from ALS patients previously reported to be negative for misfolded SOD1WT. Although the detection of misfolded SOD1 at the end stage of the disease does not prove a causative role of SOD1, it provides circumstantial evidence that SOD1WT may still participate in the pathogenesis of ALS.
Paper IV An aggregate-selective monoclonal antibody attenuates seeded but not spontaneously evolving SOD1 aggregation in ALS model mice Emerging evidence supports the hypothesis that proteins involved in neurodegenerative diseases acquire their pathogenicity by a prion-like mechanism 353. These include amyloid-β and tau in AD, α-synuclein in PD and huntingtin in Huntington disease 354. ALS-associated proteins, including SOD1, have been shown to display self-propagating prion-like properties in vitro 151,160 and in vivo 134. Results from our groups have demonstrated that inoculation of two conformational distinct human SOD1 strains induces templated aggregation and spread the ALS-like disease in vivo 173. Cell-to-cell transmission of SOD1 aggregates is thought to involve their release into the extracellular space and uptake into neighbouring cell. This transfer can be neutralized by conformation-specific SOD1 antibodies in vitro 133,162. These data indicate that antibodies, which bind to SOD1 aggregates and block their transmission, could inhibit disease progression driven by prion-like mechanisms.
The aim of this study was to evaluate the efficacy of novel mAb to interfere with the SOD1 aggregation pathology in a prion-like ALS mouse model. Monoclonal antibodies against disordered segments of SOD1 aggregates were characterized for their ability to bind to disordered, misfolded and aggregated SOD1 species in vitro. The transgenic mouse model expressing the human SOD1G85R variant was used in this study. Additionally, we utilized the previously established mouse model of SOD1 prion-like spread. It is based on the SOD1G85R model, in which seeds of partially purified hSOD1G85R aggregate were inoculated into the lumbar spinal cord of pre-symptomatic mice. This leads to both accelerated disease onset and progression 173. These mice were injected with two mAb and the disease course followed until the mice reached disease end-stage. Up to five serial blood samples as well as CSF samples at end-stage were analysed for antibody titre using an ELISA with denatured human apo-SOD1. Aggregates were analysed in CNS tissue using dot blot, western blot and IHC.
We first validated a set of newly developed mouse mAb with several biochemical methods. These antibodies have been generated against two peptides covering
44
the amino acid sequence 57-72 (hSOD157-72) and 131-153 (hSOD1131-153) of the monomeric human SOD1. While hSOD157-72 is located within the zinc-binding loop IV, the epitope hSOD1131-153 is located at the C-terminus (Figure 1 in Paper IV). Based on previous studies from our group, both epitopes lose their native contacts but are not recruited to the fibril core of SOD1 aggregates. Hence, these epitopes retain a disordered structure and remain available for antibody binding in aggregates 172. Furthermore, it has been shown that pAb produced against those epitopes react with all identified SOD1 aggregate strains, but not natively folded SOD1 172.
Following initial screening to determine good binders, two antibodies per epitope (mAb 5.7 and 134.2 against hSOD157-72; mAb 85.11 and 545.2 against hSOD1131-153) were chosen for further validation (Table S1 in Paper IV). All four mAbs were found to recognize specifically disordered SOD1 and showed no binding to the rigid structure of the native SOD1 protein in immunocapture. We further characterized their binding kinetics by surface plasmon resonance (SPR). While mAb 134.2 displayed the strongest binding to disordered SOD1, mAb 5.7 showed only moderate binding. The C-terminal-reactive mAb 85.11 exhibited the weakest overall binding due to a rapid dissociation of the antibody-antigen complex. No SPR data was obtained for mAb 545.2, indicating low affinity to denatured SOD1.
An antibody typically binds a target epitope of 5-7 amino acids long 355. However, the peptides SOD157-72 and SOD1131-153 used for generating the antibodies comprise 16 and 23 amino acids, respectively. To further define the target epitopes of all four mAbs, we used shorter peptides in an ELISA . This revealed that both mAb 5.7 and 134.2 bound strongest to peptide hSOD166-76. Although the overall binding of mAb 545.2 was lower than 85.11 in this assay, both mAb bound efficiently to hSOD1142-153 (Figure S1 in Paper IV).
The amino acid sequence between mouse and human SOD1 differ at position 66 and 70 in the SOD157-72 peptide (Figure 1 in Paper IV). In contrast, there is no sequence difference at SOD1142-153 between both species. Using western blot analysis, we found that both mAb 5.7 and 134.2 bound specifically to human SOD1 but not to mouse, confirming the previous results that SOD166-76
is part of their target sequence. On the other hand, both mAb 85.11 and 545.2 detected both mouse and human SOD1 in western blot analysis. Since all proteins in the homogenate have been denatured before analysis, the detected binding to mouse SOD1 does not imply that these antibodies react with natively folded mouse SOD1. We next examined the binding specificity to disordered and aggregated misfolded SOD1 species in mouse spinal cord tissues using IHC. All four antibodies bound strongly to disordered hSOD1G85R species in 200 days old pre-symptomatic transgenic mice. Less binding was observed in terminal transgenic mice, suggesting that disordered SOD1 species are recruited in to aggregates. To test this hypothesis further, we treated spinal cord sections first with proteinase to remove all monomeric and oligomeric hSOD1G85R species,

45
before antibody staining. No staining was found in 200-day pre-symptomatic transgenic mice, indicating that at this stage no large aggregates had been formed. In contrast, all four mAb showed strong reactivity to spinal cord sections from terminal mice. These results were confirmed by dot blot analyses, in which large hSOD1G85R or hSOD1G93A aggregates were captured on a membrane with 0.2-µm pore size and disordered SOD1 monomers and smaller aggregates are removed from the sample (Figure 2 in Paper IV). Taken together, the in vitro data confirmed that all four mAbs specifically recognize disordered and misfolded human SOD1 species under conditions relevant for in vivo studies. Based on these findings (summarized in Table 1 in Paper IV), mAb 134.2 and 85.11 were chosen for further in vivo studies.
We choose weekly i.p. injections as route of administering the antibodies into the system. Although this method requires high doses of antibodies, we aimed at long-term mAb treatment that could not be achieved without complications when using other injections routes such as intravenous or intracerebroventricular. Before initiating long-term mAb injections, we first determined basic pharmacokinetic behaviour including elimination rate and distribution of both antibodies. Following a single mAb injection (50 mg/kg), continuous blood samples were collected every 7 days for 28 days and analysed by ELISA. While mAb 134.2 had a fast elimination rate and a half-life of 7 days, mAb 85.11 exhibited a slower elimination rate and a half-life of 10 days (Figure 4 in Paper IV). The half-life of both antibodies was longer than the average half-lives of serum IgG in adult mice in regards to their subtype. While mAb 134.2 belongs to the IgG2b subclass with a reported half-live of 4-6 days, mAb 85.11 is an IgG1 subtype with a half-live of 6-8 days 356. Hence, weekly injections of both antibodies are sufficient to ensure a continuous mAb supply.
Next, we investigated whether long-term administration of mAb had a potential therapeutic effect on the spontaneously developing hSOD1G85R aggregates. Previous results from our group indicated that the initial nucleation of SOD1 aggregation starts around 100 days before mice of the hSOD1G85R model reached the terminal disease stage at around 406 days 173. Hence, the aggregation process starts at around 306 days. To achieve a baseline antibody titre before the first SOD1 aggregate emerge, we initiated weekly injections in 250 days old hSODG85R mice using mAb 85.11, an isotype control IgG1 and PBS as vehicle control. Survival analysis showed no significant differences in disease onset or survival between the mAb 85.11 treated group compared to either control groups. However, there was a trend for a shorter lifespan observed in both mAb treated groups compared to non-injected mice. This could be related to stress caused by weekly injections and screening for symptoms. These results suggest that antibodies do not affect the intracellular aggregation process.
They further indicate that injections up to 50 mg/kg of mAb 85.11 were safe for a long period of time.
46
We then wanted to examine the efficacy in the prion-like ALS model involving an extracellular route of prion-like transmission of SOD1 pathology. To test whether mAbs could block seeded aggregation, we pre-incubated seeds with mAb 85.11, at a stoichiometric molar ratio of 1:1 or 1:10, or with PBS as vehicle control, before inoculating the mixture into the lumbar spinal cord (Figure 3 in Paper IV). Pre-incubation with mAb 85.11 prolonged survival by more than 30%. These results indicate that mAb 85.11 reduced the prion-like properties of the inoculated seeds and hence, delayed the development of aggregation pathology in these mice. This was supported by an additional group of mice inoculated with the same hSOD1G85R seeds at a 1:3 dilution but without mAb pre-incubation. The survival time in these mice was increased by 39%.
To test a potential therapeutic effect of peripherally administered mAbs in the SOD1 model of prion-like spread, we initiated i.p. injections 28 days before hSOD1G85R seed inoculations (Figure 4 in Paper IV). This was done to ensure a steady baseline of circulating antibodies at the time of seed inoculation. Weekly i.p. injections of a low dose of either mAb 134.2 or 85.11 (10 mg/kg bodyweight) had no significant effect on survival. Mice treated with high doses of mAb 134.2 (50 mg/kg bodyweight) had a reduced life span by around 10%. However, a high dose of mAb 85.11 (50 mg/kg bodyweight) significantly prolonged survival by around 47%. During the treatment phase, we collected up to five blood samples at pre-defined time-points, with the last one collected at the day of sacrifice. At this time point, we also collected CSF samples and spinal cord tissues for biochemical and IHC analysis. ELISA was used to determine mAb titres in serum and CSF. We found that both mAb had crossed the BBB with similar levels varying between 0.1-0.6% of serum mAb concentrations (Figure 5 in Paper IV). Spinal cord analysis from these mice revealed similar levels of aggregated hSOD1G85R, mouse SOD1 and hSOD1G85R between mAb treated and control groups. Aggregate analysis via dot blot showed that aggregates from mAb 85.11 treated mice immunoreacted with an anti-mouse IgG antibody. This indicated that mAb 85.11 was bound to the aggregates in vivo. The reactivity to the anti-mouse IgG was stronger in mice treated with 50 mg/kg of mAb 85.11. Aggregates from mAb 134.2 treated mice displayed only weak reactivity, similar to the control group. These results suggests that mAb 134.2 was able to pass the BBB, but did bound to aggregates in vivo and hence, had no therapeutic effect in this experimental set up.
Analyses of spinal cord sections by IHC were then performed to visualize the localization of mAb associated with SOD1 aggregates. We did detect IgG antibodies co-localized with hSOD1G85R aggregates (Figure 5 in Paper IV). However, there was no IgG staining within ChAT+ motor neurons or activated microglia or astrocytes. These results further support the notion that mAb based therapy does not efficiently target SOD1 aggregates derived from overexpression or massive
47
intracellular accumulation of toxic SOD1 species, but successfully target SOD1 aggregate seeds in the extracellular space. In conclusion, the novel mAbs presented in this study are valuable tools to study misfolded SOD1 and prion-like transmission of aggregated SOD1 in vivo. We showed that peripherally injected mAb 85.11 entered the CNS, bound to aggregates of hSOD1G85R and reduced seeding activity of hSOD1G85R aggregates inoculated into the CNS. However, passive immunotherapy using the conditions tested was not sufficient to affect the spontaneously developing disease. Additional strategies might be needed to inhibit the intracellular accumulation of misfolded SOD1 as an effective disease modifying approach.
48
Discussion
SOD1 misfolding and accumulation in the CNS are pathological hallmarks of SOD1-associated ALS and the aggregation process is likely to be an important event in the pathophysiology of the disease. The detailed molecular mechanisms underlying SOD1 unfolding, accumulation and aggregation have not been resolved. Further, it is unknown which SOD1 species are the most toxic and how they might contribute to the disease. In order to address these questions, suitable tools and methods to study the unfolding and aggregation process in vitro and in vivo are necessary. Antibodies are invaluable tools for analytical methods and have been used throughout this thesis to isolate, quantify, characterize and visualize different SOD1 species in vitro and in vivo. In addition to a set of well-characterized rabbit pAb, novel mouse mAb have been established and validated in several assays side-by-side with their polyclonal counterpart to ensure specificity and sensitivity for the specific application.
In Paper I, II and III, pAb were mainly used in ELISA, immunocapture or IHC methods.
The sandwich ELISA format (termed misELISA in the papers) was used to detect soluble disordered SOD1 species using affinity purified pAb hSOD124-39
as capture antibody. This antibdoy specifically recognizes disordered human SOD1 and does not recognise native human SOD1 319. Hence, the capture antibody only catches the antigen of interest and all other proteins in the sample are washed away. An anti-SOD1 pAb raised against full-length human apo-SOD1 was used for detection. This antibody is suited for the detection of a wide range of misfolded species, because human apo-SOD1 can adopt many different conformations 357. However, it should be noted that the ELISA might not recognize all forms of disordered mutant SOD1 to the same extent, which is due to several factors. For instance, SOD1 mutations can interfer with the conformation of immature SOD1, which in turn could affect the antibody binding 358. While SOD1 mutants with SOD1WT-like characteristics disintegrate at temperatures above 40°C, other SOD1 mutants show a significant degree of unfolding already at 23°C 359. In order to diminish the potential effects of different SOD1 mutations in the assay, the optimal incubation temperature for the ELISA was selected to be 23°C 339. This is because some, but not all, folded mutant SOD1 species unfold continuously at 37°C. The optimized ELISA is sensitive and can be used to detect very low levels of disordered SOD1 in extracts from patient-derived cells.
This has been a great challenge, because cell models derived from patients express SOD1 at physiological levels, where amounts of disordered SOD1 are expected to be very low.

49
Using this ELISA, we have characterized soluble disordered SOD1 in patient-derived cultures and observed enhanced levels of disordered SOD1 without alterations in total SOD1 expression. We have determined that disordered SOD1 is increased in MNACs compared to other cell types. MNACs are an in vitro model for the ventral spinal cord from the forelimb region and thereby should represent cell-types that are most sensitive to ALS. Most significantly, enhanced levels of disordered SOD1 were detected in MNACs carrying SOD1 mutations, but were also increased in MNACs carrying SOD1WT. Additionally, exposure of patient-derived cells to low oxygen tension led to an increase of disordered mutant SOD1 and SOD1WT. MNAC cultures were more sensitive to oxygen changes than other cell types. Taken together, the antibody-based ELISA is a suitable approach to detect small changes in soluble disordered SOD1 levels in patient-derived models due to conformation-specific antibodies. By combining ELISA analysis with iPSC-based models, we have validated human models of ALS and used these to understand more about the role of disordered SOD1 in the disease process. This approach could be used to evaluate therapeutic strategies that could reduce levels of disordered SOD1. It could also be applied as tools to screen and validate therapeutic drugs in a patient-specific context.
One limitation of the ELISA method is that the capture antibody SOD124-
39 can react with any disordered SOD1 species that presents the epitope for binding. To study disordered disulphide-reduced or -oxidized SOD1 species in more detail, we developed an immunocapture method. It is often referred to as immunoprecipitation and a useful technique for the detection, isolation, and quantification of an antigen in solution. The basis of this method is the formation of an antibody-antigen complex where the antigen is in as near in vivo state as possible. Immunocapture enabled the isolation and concentration of disordered SOD1 from cell lysates. The isolated fractions were analysed by western blotting using a detection antibody generated in a different species. In Paper I and II, the same pAb used in the ELISA experiments was utilized to capture disordered SOD1 and the mAb 134.2 was used for detection in western blotting. Both antibodies recognise different epitopes on disordered SOD1 and by this approach we could ensure maximal capture efficiency with the pAb and detection specificity with the mAb. Using this method, we determined that disordered SOD1 in patient-derived cells exists mainly as soluble disulphide-reduced species. The levels increased substantially when cells were cultured under low oxygen tensions. In Paper III, we captured misfolded SOD1WT from post mortem spinal cord tissues from sALS patients. However, this newly developed method is not only limited to the isolation of disordered SOD1, but could be used to purify SOD1 aggregates from iPSC cells, mouse tissues or post mortem human tissues with the goal of determining the role of SOD1 aggregation in ALS pathogenesis.
50
In addition to verifying the presence of disorderes/misfolded SODWT in tissue samples from sALS patients, the main results in Paper III depended on IHC staining using a panel of antibodies. IHC is a basic method to study the pathophysiology of ALS. However, a standard protocol for the detection of unfolded or aggregated SOD1 does not exist. There are many critical steps involved in such a protocol including tissue preservation and storage, antigen retrieval, quality of primary antibody, incubation time, washing and counterstaining. Each one of these come with its own challenges and may affect the outcome 360. Hence, IHC protocols have to be adapted for each antigen and antibody. Using optimized conditions for multiple antibodies, we detected varying levels of misfolded SOD1WT in CNS samples from sporadic ALS patients. This result supports the hypothesis that SOD1WT may be involved in the pathogenesis of non-SOD1 ALS. However, the results only reflect the disease at end stage and it is unclear whether misfolding of SOD1WT is just a downstream event or if the protein is actively involved disease pathogenesis.
Accumulating evidence indicates that SOD1 aggregates have prion-like properties and spread through the CNS via templated aggregation 163,173,174. This hypothesis depends upon a transcellular transmission of SOD1 aggregates. Approaches for prion-specific interventions aim at the clearance of aggregates from the extracellular space in conjunction with inhibition of cellular uptake. We used a recently established model of seedind and prion-like spread of SOD1 aggregates 173 to investigate potential therapeutic effects of our novel mAbs. This was encouraged by promising immunotherapeutic results in other neurodegenerative diseases such as PD and AD 306,361. In ALS, an antibody against misfolded SOD1 has been shown to extend the life span of the rapidly progressing SOD1G93A mouse model by eliminating misfolded SOD1 via Fc receptor-mediated clearance 311. Our immunotherapeutic study showed that weekly i.p. injections of mAb 85.11 recognizing the C-terminus of SOD1 prolonged survival of transgenic hSOD1G85R mice inoculated with SOD1 seeds. Similarly, pre-treatment of SOD1 seeds with mAb 85.11 prior to their inoculation reduced prion-like activity of the seeds in the recipient mice and extended their survival. However, all seed-inoculated mice treated with mAb 85.11 reached the terminal stage earlier than non-seeded control mice. In addition, long-term treatment with mAb 85.11 had no effect on survival in transgenic hSOD1G85R mice. This suggests that mAb 85.11 can bind to and block the uptake/seeding capacity of SOD1 aggregates when injected extracellularly. However, mAb 85.11 was not able to interfere with the SOD1 aggregation process intracellularly or the intercellular transmission of SOD1 aggregates.
It has been suggested that SOD1 aggregates may be transmitted by the release of SOD1 aggregates into the extracellular space by dying cells, but also via vesicles released in to the extracellular space (exosomes), or intercellular connections such as tunneling nanotubes 349. Hence, SOD1 aggregates could be shielded by these mechanisms and not available for binding by extracellular
51
antibody. This suggests that combinatorial approaches targeting the intracellular aggregation process and/or the extracellular transfer are needed to block disease progression in ALS.
In addition to mAb 85.11, we also studied the efficacy of mAb 134.2 in an immunotherapeutic approach. However, no effect on survival could be observed when seed inoculated transgenic mice were treated with mAb 134.2. Blood analysis showed that both mAbs diffused efficiently from the interstitial space at the side of injection into the cardiovascular system. Furthermore, approximately ~0.1 - 0.6 % of the antibody concentration in plasma was found circulating in the CNS. These concentrations are consistent with previous reports of antibody efflux from the periphery to the CNS 296. Hence, the lack of effect of mAb 134.2 in the prion-like model was not likely to be due to low bioavailability of the antibody in the CNS. Analysis of CNS tissue from terminal mice showed no association of mAb 134.2 with SOD1G85R aggregates, suggesting low binding to aggregates. The binding affinity of mAb 134.2 towards aggregates could be affected by the in vivo environment. Validation experiments in vitro, where mAb 134.2 bound efficiently to aggregates, were controlled for factors such as ionic strength and pH to mimic physiological conditions as far as possible 362. However, methods used for validation including ELISA, SPR and IHC involved artificial conditions, such as high concentration of purified antigens, rigid surfaces, to which antigens or antibodies were bound to, or to chemical treatment to retrieve antigens. Hence, these methods do not reflect in vivo conditions. Another reason for the negative effect of mAb 134.2 treatment might be due to the nature of the antibody. mAb 134.2 could preferentially bind to soluble disordered SOD1 species in vivo and hence, may be to diluted to adequately bind to aggregates. Furthermore, the target of mAb 134.2, the zinc-binding loop IV in SOD1, is a very flexible structure that acquires conformational freedom upon loss of its native contacts. Hence, loop IV could potentially adopt additional confirmations in vivo that are not recognized by mAb 134.2. Dot blot analysis of in vivo produced SOD1 aggregates show that the epitope is available for binding 172. However, these aggregates have been purified and only large species are captured on the dot blot filters. Smaller SOD1 aggregate species that could potentially be toxic and spread the disease are removed in this assay. Hence, the preferred binding species of mAb 134.2 could be lost in this assay.
Another important criteria to consider when designing immuno-therapeutic approaches are antibody subclasses in order to trigger the desired response by the antibody-antigen complex. Antibodies of various IgG subclasses and their respective receptors comprise complex networks that induce different downstream responses. The mAbs used in Paper IV belonged to the IgG1 (mAb 85.11) and IgG2b (mAb 134.2) subclasses. Since mouse IgG1 binds preferentially to the inhibitory IgG receptor, than to any of the activating receptors, its mode of action should induce less pro-inflammatory signalling compared to the IgG2b
52
subtype. Using IHC quantification, we could not see any differences in immune response in either mAb 85.11 or 134.2 treated mice. However, these analyses have been carried out on tissues from terminal diseased mice, when limb paralysis was so severe that mice could not reach wet food. To assess immune responses during treatment, it would be necessary to analyse mice at pre-defined time points before and after disease onset.
The most frequently approved human IgG subclass for therapeutic use by the FDA is IgG1 260. The mouse homologue to this subclass is IgG2a and was successfully used in preclinical studies targeting aggreated proteins associated with PD, AD and ALS 306,311,361. However, the C57BL/6 mouse, which is the genetic background of the SOD1G85R mouse model, does not express the IgG2a subclass. Instead it produces an alternative subclass called IgG2c 363. Mice lacking the IgG2a gene could be intolerant to injected IgG2a antibodies. Possible consequences may be increased plasma clearance and/or induced immune response, which will interfere with the conclusion of the study. Hence, consideration of the genetic background of the model system is vital to ensure reliable and meaningful data from immunotherapy studies.
Despite considerations of the appropriate therapeutic antibody and its desired response in vivo, the target antigen is not of minor importance. The main targets for the mAbs used in immunotherapy study were disordered SOD1 regions in aggregated SOD1 species. However, both mAb 85.11 and 134.2 also bind to disordered SOD1 monomers. Depending on the SOD1 mutation and environmental conditions, such as pH and temperature, SOD1 and aggregates formed from it can adopt different conformations, giving rise to different aggregate strains 172,173. Different SOD1 aggregate strains formed in vivo induced different disease phenotypes with regard to progression rate, level of aggregates and histopathological findings 173. This strain-dependant toxicity could explain the diverse progression and severity of familial ALS patients expressing different SOD1 mutations. This means that a successful treatment for one mutation might be insufficient for another.
In summary, we have established antibodies as powerful tools to characterize disordered, misfolded and aggregated SOD1 species. These antibodies have been validated in biochemical assays in vitro, but also in cells, human tissues and in mouse models in vivo. Using antibodies to analyse soluble disordered SOD1 in patient-derived cell models can be used to study early stages of ALS disease. These techniques could also be used to better understand the SOD1 aggregation process. The mAbs developed and used in this thesis are valuable tools with which to study disordered SOD1 and the prion-like transmission of SOD1 aggregates in vivo.
53
Conclusions
Conformation-specific antibodies are valuable tools to detect and study disordered and potentially pathogenic species of SOD1. Using them in various biochemical and in vivo assays, we were able to show that:
• iPSC-derived MNACs expressing physiological levels of SOD1 are a useful in vitro model to study disordered SOD1 species
• Disordered SOD1 species are more abundant in patient-derived MNACs and astrocytes than in sensory neurons, iPSCs and fibroblasts
• Disordered SOD1 in MNACs from a SOD1 ALS patient exists in the same disulphide-reduced form as in SOD1 transgenic models
• Low oxygen tension leads to increased levels of disordered SOD1 in
patient-derived fibroblasts, astrocytes and MNACs
• The SOD1 response to hypoxic conditions is reversible, time- and concentration-dependent
• Reduced oxygen concentrations result in increased disulphide-reduced, disordered SOD1 and aggregation in MNACs
• Misfolded SOD1WT is detected in brain and spinal cord tissue from ALS patients without SOD1 mutations
• Levels of misfolded SOD1WT isolated from spinal cord samples varied
between sporadic ALS patients, but are higher compared to the non-disease control sample
• Novel mAbs against disordered segments of SOD1 detect disordered
and aggregated SOD1 species with differential affinity in vitro
• Long-term treatment with mAbs did not interfere with spontaneously developing aggregation in vivo
• The C-terminal mAb 85.11 reduces the seeding properties of mutant SOD1 seeds in an ALS mouse model

54
Acknowledgement
With this thesis, my time as a PhD student comes finally to an end. Nearly 10 years ago, I arrived in Umeå looking for adventures and new horizons. I will be leaving with a bag full of memories that last for a lifetime. Along this journey I worked with many colleagues that deserve sincere thanks. First and foremost, I would like to thank Jonathan Gilthorpe: I wrote only one mail to apply for a master project and you immediately gave me a chance to work in the group. Your enthusiasm, passion for science and infinitive source of new ideas is truly inspiring. Thanks for teaching me independence from the first day of my PhD and giving me a lot of space to try out many different things, prove myself and bang my head against a few walls until they crumbled. Although it did not seemed at times, I’ve enjoyed working in your lab and learned so incredibly much.
I would also like to express my gratitude to my co-supervisors. Thanks to Peter Andersen, for sharing your clinical knowledge and the interesting life stories behind all these cell-lines. They are reminders for what the work and research is all about. Stefan Marklund, your vast knowledge about SOD1 is fascinating and your demonstration of the folding and unfolding process of SOD1 will follow me forever. Thanks to Thomas Brännström for sharing your never-ending knowledge about neuropathology during autopsies. Ulrika Nordström, my beloved 5th (co-) supervisor. To write everything down for what I am grateful for, would fill another 50 pages (and believe me that would be way easier and quicker than writing this thesis J). Our work at the animal house with all the jokes and laughter were by far the most enjoyable, even when the project did not turned out the way we hoped. Thank you for always spreading a good mood and keeping my spirits up at all time. Knowing you would not allow for things to go south, kept me calm to the very end. Thank you for the scientific discussions, critical input, encouragement and all the pep talks! Your end-less energy, love and dedication for science will accompany me to wherever I go! This ultimately leads me to Matthew Marklund – a man whose style changes quicker than the seasons in North Sweden. Thanks for all the little and big help I received “off the records” as well as the “quick” scientific and non-scientific discussions. Without you I would still be buried in staining’s and ImageJ analysis. - But don’t worry, I will send you an email with all the details for your records J Elin Forsgren, I am so glad to had such an amazing PhD sister – you taught me everything about iPSCs, differentiation and cell culture. You made everything look so easy! I admire you for your way of simplifying the most complex things. You kept your head up high and smiled even in the darkest hours (including the nights and early mornings). I truly miss you and your confused Swenglish at work! I hope we keep in touch and I will hear about little Henny’s wellbeing and progress in the future.
Thanks to Uma Muthukrishnan for showing me around the lab when I first arrived and teaching me western blotting from scratch. You taught me also so many things about your culture and I still need to smile when thinking of you cruising through the streets on a motorcycle.
Ann and Ash Haeger, thanks for the cup of tea when things were not going as planned and your never-ending willingness to help out! Thanks also for all the fun
55
we had outside the lab with BBQs at the lake or game nights. I will never forget the impact of a game on our otherwise so calm Bala ;) I hope to visit you sometime and say hello to my favourite British girl Freyja and her (not so little anymore) brother Thorsten. Anna-Karin Jonasson, Anna-Lena Bolender and Thorina Boenke - my favourite students! It was a real pleasure to teach you girls. Your enthusiasm, passion for science and life was contagious. Having you around was great fun. I miss you girls and wish you all the best for your future. Anna-Lena – Thanks for all the trips, fikas, and baking fun we had outside the lab! Good luck in Harvard! Thorina – I will keep my promise and make it to Vienna quite soon!
I would also like to thank all the other project students in Jonathan’s lab over the years: Hanna, Thomas, Johan, Emil, Tomasz, David, Andreas, Antonia, Marcus, Hauke, Kazuma, Max, Axel, Bala, Harsha, Sina, Chloe, Karim, Yersin (I think that were all J)- thanks for your great company in the lab, and during fika times! Isil Keskin – Queen of fibroblasts and western blots. Thanks for always spreading a light-hearted mood with your big smile and your cheerful talks. It’s a real energy booster in dark times J Thanks also for all the fun we had on conferences! I will never forget when you tried to teach me how to use an eyeliner and the look of hopelessness in your eyes when you gave up! Special thanks also to Eva Jonsson, Helena Alstermark and Ann-Charloth Nilsson for all your help with cell cultures and around the lab and organizing social group events. Together with Agneta Öberg and Eva Bern, it was fun working with you and thanks for always making time for answering questions. Bastien Paré, my Canadian collaborator and co-author. It was a real pleasure to meet you and good luck with your thesis – the end is finally near for both of us! J Per Zetterström, thanks for all the “modern talking” we had about immunocapture and SOD1. Thanks also to all present and past members of the ALS group in Umeå that are too many to be named here – and there is a too high risk I will be forgetting somebody... Thanks for making ALS meetings and social events fun! Many thanks also to Agneta Valleskog, Birgitta Nordin, Per-Arne Lundström, Lina Sollén and Clara Olsson for all the administrative help over the years. Thanks also to all the helpful people at UCMM and Medical Biosciences/Pathology. Thanks Lennart Östermann, for all the laughters, pep talks and endless stories we shared. The word “Schwedenschnuckel” will never mean the same again J. Alexej Schmidt, my antibody guru. Vielen Dank für deine Ratschläge und Hilfe wenn ich mal wieder nicht weiter wusste. Danke auch für das Heimatgefühl, was du mit deinem unverwechselbaren Schwabengemüt verbreitet hast. Thanks also to all the other people at the 6M building that I have gotten to know and received encouragement and support from: Sandhya, Cyrinne, Denise, Erik B., Erik D., Pramod, Karthik, Fredrik, Mattias, Björn, Xingru, Greg & Linda, Simona & Carl, Lee-Ann, Mona and many more…
56
Pursuing a PhD can be quite demanding and ease of mind is therefor essential. I can consider myself fortunate to got to know many great people that helped me to stay calm and collected in various ways. Many thanks to Rui & Jenny, Viqar & Saima, Gautam and Asim for all the great times we had here in Umeå. Alexandros Sykaras, my dear friend. Thanks for all the late night councils and fascinating discussions during your time in Umeå. I would love to come back to Greece for another visit. John, Julia and Kiro, my dogsitters and best friends of Marley. Thank you so much for those 30 min fun play dates every day for the last couple of months and the inspiring topics we discussed during that time. Jeanette, Helder and Joseph, thanks for all the delicious dinners, fun evenings, political discussions, dog sitting and so many other good memories. I am looking forward for your next big adventure to arrive. You always can count on us as baby sitters J My girls from Umeå – Zahra and Helena – I am not only happy that I got to share my time as a PhD with you, but also that you became my closest friends here. Thank you so much for your support, love and sharing your passion for science, books and life. Together with Hélène, Masoumeh, Vicky and William thanks for all the great evenings, amazing trips, countless other events and, of course, the game nights (wizzard is accumulating dust J). Meine Mädels aus Rostock – Maria (& Steve), Carola (& Kai) und Katrin (& Sascha) – ihr seid und bleibt so kostbar wie die Sterne! Tausend Dank für all die tollen kulturellen Reisen und eure Unterstützung. Am allermeisten aber Danke für eure Freundschaft und das immer, wenn wir uns wiedersehen, es sich so anfühlt als wäre kaum Zeit vergangen und wir würden nach wie vor alle in der kleinen Stadt am Meer wohnen. Ich freu mich schon sehr euch alle wiederzusehen und auch den kleinsten in unserer Gruppe endlich persönlich zu treffen – Emil. Anja, Freundin aus Kindertagen und bevor wir wussten was Promotion bedeutet. Wir könnten nicht weiter voneinander entfernt liegen in unserem wissenschaftlichen Interesse und doch können wir bei unseren alljährlichen Wiedersehen einfach da wieder anknüpfen, wo wir aufgehört haben. Deine Bodenständigkeit und pragmatische Sichtweise aufs Leben gibt mir jedes Mal neue Energie und erinnert mich daran mich nicht an den kleinen Dingen festzuhalten. Danke dafür! Special thanks also to my Moroccan family. Thanks for opening your hearts for me and making me feel welcome in your home. Thanks also for all the trips and great summers we spend together and all the amazing food. Laila, Zineb and Amina – I enjoyed watching you grow into the women you became. I am so proud of you! Rabia and Mohammed – I’m looking forward to welcome you soon here in Umeå! Sylvia, my baby sister. Vielen Dank, dass du mich immer wieder auf den Boden der Tatsachen zurückholst. Danke, dass du mich verstehst wie keine Andere und genau weißt, wann ein motivierender oder zynischer Kommentar angebracht ist. Vielen Dank auch dafür, dass du und Bernd mich in euer Heim aufnehmt wann immer ich in die Heimat komme und ich in eurem Garten neue Energie schöpfen kann.

57
Danke, dass ihr und Nadine, mich immer wieder daran erinnert, dass das Leben auch ohne Promotion lebenswert ist. Ganz besonderen Dank auch, dass ihr viele familiäre Pflichten übernommen habt, seitdem ich nach Schweden gezogen bin. Ich hoffe, dass wir das in naher Zukunft ein bisschen besser verteilt bekommen. Nadine – vielen Dank, dass ich immer auf dich zählen kann, wenn es mal wieder heiß hergeht. Danke für deine Ermutigungen und Selbstlosigkeit. Mama, vielen, lieben Dank für deine bedingungslose Unterstützung und dein Vertrauen in all meinen Entscheidungen. Danke auch für all die Aufopferungen, die du auf dich genommen hast, um mir die Chance zu ermöglichen meinen Träumen zu folgen. Vielen Dank, dass du und Papa uns ständig vorgelebt habt, was harte Arbeit wirklich bedeutet und das man nichts geschenkt bekommt im Leben. Last, but with no means least Nabil Souihi – love of my life and pillar of my strength. Without your love, support and encouragement I would have been lost and this thesis would surely have taken longer than it already did. I never thought that my Sweden adventure will turn my life upside down in this way. Thank you for being my best friend, sharing this passion for life and adventure, and helping me to laugh and love, even in the toughest of times. I am looking forward to where life is sending us next, but most of all I am very excited for the perhaps biggest adventure in our lives! J Kanbrek bezaf!

58
References
1. Rowland, L.P. How amyotrophic lateral sclerosis got its name: The clinical-pathologic genius of jean-martin charcot. Archives of Neurology 58, 512-515 (2001).
2. Drouin, E. et al. Cruveilhier versus Charcot. The Lancet Neurology 15, 362 (2016). 3. Charcot, J.M. De la sclérose latérale amyotrophique. Prog Med 2, 325-327, 341-342, 453-
455 (1874). 4. Goetz, C.G. Amyotrophic lateral sclerosis: early contributions of Jean-Martin Charcot.
Muscle Nerve 23, 336-43 (2000). 5. Al-Chalabi, A. et al. Amyotrophic lateral sclerosis: moving towards a new classification
system. The Lancet Neurology 15, 1182-1194 (2016). 6. Ravits, J. et al. Implications of ALS focality: rostral-caudal distribution of lower motor
neuron loss postmortem. Neurology 68, 1576-82 (2007). 7. Ravits, J.M. et al. ALS motor phenotype heterogeneity, focality, and spread:
deconstructing motor neuron degeneration. Neurology 73, 805-11 (2009). 8. Swinnen, B. et al. The phenotypic variability of amyotrophic lateral sclerosis. Nat Rev
Neurol 10, 661-70 (2014). 9. Wijesekera, L.C. et al. Amyotrophic lateral sclerosis. Orphanet J Rare Dis 4, 3 (2009). 10. Cleveland, D.W. et al. From Charcot to Lou Gehrig: deciphering selective motor neuron
death in ALS. Nat Rev Neurosci 2, 806-19 (2001). 11. Lyall, R.A. et al. Respiratory muscle strength and ventilatory failure in amyotrophic lateral
sclerosis. Brain 124, 2000-13 (2001). 12. Chio, A. et al. Phenotypic heterogeneity of amyotrophic lateral sclerosis: a population
based study. J Neurol Neurosurg Psychiatry 82, 740-6 (2011). 13. Chio, A. et al. Prognostic factors in ALS: A critical review. Amyotroph Lateral Scler 10,
310-23 (2009). 14. Turner, M.R. et al. The diagnostic pathway and prognosis in bulbar-onset amyotrophic
lateral sclerosis. J Neurol Sci 294, 81-5 (2010). 15. Merrilees, J. et al. Cognitive and behavioral challenges in caring for patients with
frontotemporal dementia and amyotrophic lateral sclerosis. Amyotrophic lateral sclerosis : official publication of the World Federation of Neurology Research Group on Motor Neuron Diseases 11, 298-302 (2010).
16. Ferrari, R. et al. FTD and ALS: a tale of two diseases. Current Alzheimer research 8, 273-294 (2011).
17. Marin, B. et al. Variation in worldwide incidence of amyotrophic lateral sclerosis: a meta-analysis. Int J Epidemiol (2016).
18. Al-Chalabi, A. et al. Gene discovery in amyotrophic lateral sclerosis: implications for clinical management. Nat Rev Neurol 13, 96-104 (2017).
19. Chio, A. et al. Global epidemiology of amyotrophic lateral sclerosis: a systematic review of the published literature. Neuroepidemiology 41, 118-30 (2013).
20. Bettini, M. et al. Incidence and prevalence of amyotrophic lateral sclerosis in an HMO of Buenos Aires, Argentina. Amyotroph Lateral Scler Frontotemporal Degener 14, 598-603 (2013).
21. Logroscino, G. et al. Incidence of amyotrophic lateral sclerosis in southern Italy: a population based study. J Neurol Neurosurg Psychiatry 76, 1094-8 (2005).
22. Logroscino, G. et al. Global, regional, and national burden of motor neuron diseases 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet Neurology 17, 1083-1097 (2018).
23. Logroscino, G. et al. Incidence of amyotrophic lateral sclerosis in Europe. J Neurol Neurosurg Psychiatry 81, 385-90 (2010).
24. Traynor, B.J. et al. Incidence and prevalence of ALS in Ireland, 1995-1997: a population-based study. Neurology 52, 504-9 (1999).
25. Arthur, K.C. et al. Projected increase in amyotrophic lateral sclerosis from 2015 to 2040. Nat Commun 7, 12408 (2016).
26. Gouveia, L.O. et al. Young‐onset sporadic amyotrophic lateral sclerosis: A distinct nosological entity? Amyotrophic Lateral Sclerosis 8, 323-327 (2007).
27. Bäumer, D. et al. Juvenile ALS with basophilic inclusions is a FUS proteinopathy with FUS mutations. Neurology 75, 611-618 (2010).
28. Chen, Y.-Z. et al. DNA/RNA helicase gene mutations in a form of juvenile amyotrophic lateral sclerosis (ALS4). American journal of human genetics 74, 1128-1135 (2004).
59
29. Alonso, A. et al. Incidence and lifetime risk of motor neuron disease in the United Kingdom: a population-based study. Eur J Neurol 16, 745-51 (2009).
30. Millecamps, S. et al. Axonal transport deficits and neurodegenerative diseases. Nat Rev Neurosci 14, 161-76 (2013).
31. Kang, S.H. et al. Degeneration and impaired regeneration of gray matter oligodendrocytes in amyotrophic lateral sclerosis. Nature neuroscience 16, 571-579 (2013).
32. Philips, T. et al. Glial cells in amyotrophic lateral sclerosis. Experimental neurology 262 Pt B, 111-120 (2014).
33. Blokhuis, A.M. et al. Protein aggregation in amyotrophic lateral sclerosis. Acta Neuropathol 125, 777-94 (2013).
34. Ross, C.A. et al. Protein aggregation and neurodegenerative disease. Nat Med 10 Suppl, S10-7 (2004).
35. Mizuno, Y. et al. Transferrin localizes in Bunina bodies in amyotrophic lateral sclerosis. Acta Neuropathol 112, 597-603 (2006).
36. Okamoto, K. et al. Bunina bodies in amyotrophic lateral sclerosis. Neuropathology 28, 109-15 (2008).
37. Rohn, T.T. Corpora Amylacea in Neurodegenerative Diseases: Cause or Effect? International journal of neurology and neurotherapy 2, 031 (2015).
38. Singhrao, S.K. et al. Corpora amylacea could be an indicator of neurodegeneration. Neuropathology and Applied Neurobiology 19, 269-276 (1993).
39. Arai, T. et al. Neuronal and glial inclusions in frontotemporal dementia with or without motor neuron disease are immunopositive for p62. Neuroscience Letters 342, 41-44 (2003).
40. Arai, T. et al. TDP-43 is a component of ubiquitin-positive tau-negative inclusions in frontotemporal lobar degeneration and amyotrophic lateral sclerosis. Biochem Biophys Res Commun 351, 602-11 (2006).
41. Neumann, M. et al. Ubiquitinated TDP-43 in frontotemporal lobar degeneration and amyotrophic lateral sclerosis. Science 314, 130-3 (2006).
42. He, C.Z. et al. Expression of peripherin in ubiquinated inclusions of amyotrophic lateral sclerosis. Journal of the Neurological Sciences 217, 47-54 (2004).
43. Okamoto, Y. et al. Colocalization of 14-3-3 proteins with SOD1 in Lewy body-like hyaline inclusions in familial amyotrophic lateral sclerosis cases and the animal model. PLoS One 6, e20427 (2011).
44. Shibata, N. et al. Cu/Zn superoxide dismutase-like immunoreactivity in Lewy body-like inclusions of sporadic amyotrophic lateral sclerosis. Neurosci Lett 179, 149-52 (1994).
45. Kato, S. et al. New consensus research on neuropathological aspects of familial amyotrophic lateral sclerosis with superoxide dismutase 1 (SOD1) gene mutations: inclusions containing SOD1 in neurons and astrocytes. Amyotroph Lateral Scler Other Motor Neuron Disord 1, 163-84 (2000).
46. Hirano, A. Neuropathology of ALS: an overview. Neurology 47, S63-6 (1996). 47. Kawashima, T. et al. Skein-like inclusions in the neostriatum from a case of amyotrophic
lateral sclerosis with dementia. Acta Neuropathol 96, 541-5 (1998). 48. Haverkamp, L.J. et al. Natural history of amyotrophic lateral sclerosis in a database
population. Validation of a scoring system and a model for survival prediction. Brain 118 ( Pt 3), 707-19 (1995).
49. Andersen, P.M. et al. Clinical genetics of amyotrophic lateral sclerosis: what do we really know? Nat Rev Neurol 7, 603-15 (2011).
50. Ingre, C. et al. Risk factors for amyotrophic lateral sclerosis. Clin Epidemiol 7, 181-93 (2015).
51. Sutedja, N.A. et al. Exposure to chemicals and metals and risk of amyotrophic lateral sclerosis: a systematic review. Amyotroph Lateral Scler 10(2009).
52. Chancellor, A.M. et al. Risk factors for motor neuron disease: a case-control study based on patients from the Scottish Motor Neuron Disease Register. J Neurol Neurosurg Psychiatry 56, 1200-6 (1993).
53. Sutedja, N.A. et al. What we truly know about occupation as a risk factor for ALS: a critical and systematic review. Amyotroph Lateral Scler 10, 295-301 (2009).
54. Turner, M.R. et al. Cerebrovascular injury as a risk factor for amyotrophic lateral sclerosis. Journal of neurology, neurosurgery, and psychiatry 87, 244-6 (2016).
55. Armon, C. An Evidence-Based Medicine Approach to the Evaluation of the Role of Exogenous Risk Factors in Sporadic Amyotrophic Lateral Sclerosis. Neuroepidemiology 22, 217-228 (2003).
60
56. Vasto, S. et al. Immunity & Ageing: a new journal looking at ageing from an immunological point of view. Immunity & ageing : I & A 1, 1-1 (2004).
57. DeJesus-Hernandez, M. et al. Expanded GGGGCC hexanucleotide repeat in noncoding region of C9ORF72 causes chromosome 9p-linked FTD and ALS. Neuron 72, 245-56 (2011).
58. Renton, A.E. et al. A hexanucleotide repeat expansion in C9ORF72 is the cause of chromosome 9p21-linked ALS-FTD. Neuron 72, 257-68 (2011).
59. Majounie, E. et al. Frequency of the C9orf72 hexanucleotide repeat expansion in patients with amyotrophic lateral sclerosis and frontotemporal dementia: a cross-sectional study. The Lancet Neurology 11, 323-330 (2012).
60. Nordin, A. et al. Extensive size variability of the GGGGCC expansion in C9orf72 in both neuronal and non-neuronal tissues in 18 patients with ALS or FTD. Hum Mol Genet 24, 3133-42 (2015).
61. Aoki, Y. et al. C9orf72 and RAB7L1 regulate vesicle trafficking in amyotrophic lateral sclerosis and frontotemporal dementia. Brain 140, 887-897 (2017).
62. Farg, M.A. et al. C9ORF72, implicated in amytrophic lateral sclerosis and frontotemporal dementia, regulates endosomal trafficking. Hum Mol Genet 23, 3579-95 (2014).
63. Rademakers, R. et al. Fus gene mutations in familial and sporadic amyotrophic lateral sclerosis. Muscle Nerve 42, 170-6 (2010).
64. Udagawa, T. et al. FUS regulates AMPA receptor function and FTLD/ALS-associated behaviour via GluA1 mRNA stabilization. Nature communications 6, 7098-7098 (2015).
65. Yasuda, K. et al. The RNA-binding protein Fus directs translation of localized mRNAs in APC-RNP granules. The Journal of cell biology 203, 737-746 (2013).
66. Yu, Y. et al. FUS functions in coupling transcription to splicing by mediating an interaction between RNAP II and U1 snRNP. Proceedings of the National Academy of Sciences of the United States of America 112, 8608-8613 (2015).
67. Anderson, P. et al. Stress granules: the Tao of RNA triage. Trends Biochem Sci 33, 141-50 (2008).
68. Kirby, J. et al. Broad clinical phenotypes associated with TAR-DNA binding protein (TARDBP) mutations in amyotrophic lateral sclerosis. Neurogenetics 11, 217-25 (2010).
69. Liu-Yesucevitz, L. et al. Tar DNA binding protein-43 (TDP-43) associates with stress granules: analysis of cultured cells and pathological brain tissue. PLoS One 5, e13250 (2010).
70. Taylor, J.P. et al. Decoding ALS: from genes to mechanism. Nature 539, 197-206 (2016). 71. Polymenidou, M. et al. Misregulated RNA processing in amyotrophic lateral sclerosis.
Brain research 1462, 3-15 (2012). 72. Murphy, M.P. How mitochondria produce reactive oxygen species. Biochem J 417, 1-13
(2009). 73. Beckman, J.S. et al. Nitric oxide, superoxide, and peroxynitrite: the good, the bad, and
ugly. American Journal of Physiology-Cell Physiology 271, C1424-C1437 (1996). 74. Stamler, J.S. et al. Biochemistry of nitric oxide and its redox-activated forms. Science
258, 1898 (1992). 75. Guzik, T.J. et al. Vascular NADPH oxidases as drug targets for novel antioxidant
strategies. Drug Discov Today 11, 524-33 (2006). 76. Fukai, T. et al. Superoxide dismutases: role in redox signaling, vascular function, and
diseases. Antioxid Redox Signal 15, 1583-606 (2011). 77. Crapo, J.D. et al. Copper,zinc superoxide dismutase is primarily a cytosolic protein in
human cells. Proceedings of the National Academy of Sciences 89, 10405 (1992). 78. Okado-Matsumoto, A. et al. Subcellular distribution of superoxide dismutases (SOD) in
rat liver: Cu,Zn-SOD in mitochondria. J Biol Chem 276, 38388-93 (2001). 79. Perry, J.J. et al. The structural biochemistry of the superoxide dismutases. Biochim
Biophys Acta 1804, 245-62 (2010). 80. Weisiger, R.A. et al. Superoxide dismutase. Organelle specificity. J Biol Chem 248, 3582-
92 (1973). 81. Wispe, J.R. et al. Synthesis and processing of the precursor for human mangano-
superoxide dismutase. Biochim Biophys Acta 994, 30-6 (1989). 82. Li, Y. et al. Dilated cardiomyopathy and neonatal lethality in mutant mice lacking
manganese superoxide dismutase. Nat Genet 11, 376-81 (1995). 83. Marklund, S.L. Extracellular superoxide dismutase in human tissues and human cell lines.
J Clin Invest 74, 1398-403 (1984).
61
84. Barra, D. et al. The complete amino acid sequence of human Cu/Zn superoxide dismutase. FEBS Lett 120, 53-6 (1980).
85. Forsgren, E. Umeå University (2017). 86. Getzoff, E.D. et al. Faster superoxide dismutase mutants designed by enhancing
electrostatic guidance. Nature 358, 347-51 (1992). 87. Strange, R.W. et al. The structure of holo and metal-deficient wild-type human Cu, Zn
superoxide dismutase and its relevance to familial amyotrophic lateral sclerosis. J Mol Biol 328, 877-91 (2003).
88. Kayatekin, C. et al. Zinc binding modulates the entire folding free energy surface of human Cu,Zn superoxide dismutase. Journal of molecular biology 384, 540-555 (2008).
89. Nordlund, A. et al. Functional features cause misfolding of the ALS-provoking enzyme SOD1. Proc Natl Acad Sci U S A 106, 9667-72 (2009).
90. Brown, N.M. et al. Oxygen and the copper chaperone CCS regulate posttranslational activation of Cu,Zn superoxide dismutase. Proc Natl Acad Sci U S A 101, 5518-23 (2004).
91. Furukawa, Y. et al. Oxygen-induced maturation of SOD1: a key role for disulfide formation by the copper chaperone CCS. Embo j 23, 2872-81 (2004).
92. Leitch, J.M. et al. Activation of Cu,Zn-superoxide dismutase in the absence of oxygen and the copper chaperone CCS. J Biol Chem 284, 21863-71 (2009).
93. Stathopulos, P.B. et al. Calorimetric analysis of thermodynamic stability and aggregation for apo and holo amyotrophic lateral sclerosis-associated Gly-93 mutants of superoxide dismutase. J Biol Chem 281, 6184-93 (2006).
94. Parge, H.E. et al. Atomic structures of wild-type and thermostable mutant recombinant human Cu,Zn superoxide dismutase. Proc Natl Acad Sci U S A 89, 6109-13 (1992).
95. Lindberg, M.J. et al. Folding of human superoxide dismutase: disulfide reduction prevents dimerization and produces marginally stable monomers. Proc Natl Acad Sci U S A 101, 15893-8 (2004).
96. Arnesano, F. et al. The unusually stable quaternary structure of human Cu,Zn-superoxide dismutase 1 is controlled by both metal occupancy and disulfide status. J Biol Chem 279, 47998-8003 (2004).
97. Hornberg, A. et al. The coupling between disulphide status, metallation and dimer interface strength in Cu/Zn superoxide dismutase. J Mol Biol 365, 333-42 (2007).
98. Rosen, D.R. et al. Mutations in Cu/Zn superoxide dismutase gene are associated with familial amyotrophic lateral sclerosis. Nature 362(1993).
99. Felbecker, A. et al. Four familial ALS pedigrees discordant for two SOD1 mutations: are all SOD1 mutations pathogenic? J Neurol Neurosurg Psychiatry 81, 572-7 (2010).
100. Pasinelli, P. et al. Molecular biology of amyotrophic lateral sclerosis: insights from genetics. Nature Reviews Neuroscience 7, 710 (2006).
101. Andersen, P.M. et al. Sixteen novel mutations in the Cu/Zn superoxide dismutase gene in amyotrophic lateral sclerosis: a decade of discoveries, defects and disputes. Amyotroph Lateral Scler Other Motor Neuron Disord 4, 62-73 (2003).
102. Andersen, P.M. Amyotrophic lateral sclerosis associated with mutations in the CuZn superoxide dismutase gene. Curr Neurol Neurosci Rep 6, 37-46 (2006).
103. Andersen, P.M. et al. Autosomal recessive adult-onset amyotrophic lateral sclerosis associated with homozygosity for Asp90Ala CuZn-superoxide dismutase mutation. A clinical and genealogical study of 36 patients. Brain 119 ( Pt 4), 1153-72 (1996).
104. Keskin, I. et al. Effects of Cellular Pathway Disturbances on Misfolded Superoxide Dismutase-1 in Fibroblasts Derived from ALS Patients. PLoS One 11, e0150133 (2016).
105. Bowling, A.C. et al. Superoxide dismutase activity, oxidative damage, and mitochondrial energy metabolism in familial and sporadic amyotrophic lateral sclerosis. J Neurochem 61(1993).
106. Al-Chalabi, A. et al. Modelling the effects of penetrance and family size on rates of sporadic and familial disease. Hum Hered 71, 281-8 (2011).
107. Andersen, P.M. et al. Amyotrophic lateral sclerosis associated with homozygosity for an Asp90Ala mutation in CuZn-superoxide dismutase. Nat Genet 10, 61-6 (1995).
108. Borchelt, D.R. et al. Superoxide dismutase 1 with mutations linked to familial amyotrophic lateral sclerosis possesses significant activity. Proc Natl Acad Sci U S A 91, 8292-6 (1994).
109. Deng, H.X. et al. Amyotrophic lateral sclerosis and structural defects in Cu,Zn superoxide dismutase. Science 261, 1047-51 (1993).
110. Saccon, R.A. et al. Is SOD1 loss of function involved in amyotrophic lateral sclerosis? Brain 136, 2342-58 (2013).

62
111. Synofzik, M. et al. Mutant superoxide dismutase-1 indistinguishable from wild-type causes ALS. Hum Mol Genet 21, 3568-74 (2012).
112. Reaume, A.G. et al. Motor neurons in Cu/Zn superoxide dismutase-deficient mice develop normally but exhibit enhanced cell death after axonal injury. Nat Genet 13, 43-7 (1996).
113. Elchuri, S. et al. CuZnSOD deficiency leads to persistent and widespread oxidative damage and hepatocarcinogenesis later in life. Oncogene 24, 367 (2004).
114. Bruijn, L.I. et al. ALS-Linked SOD1 Mutant G85R Mediates Damage to Astrocytes and Promotes Rapidly Progressive Disease with SOD1-Containing Inclusions. Neuron 18, 327-338 (1997).
115. Graffmo, K.S. et al. Expression of wild-type human superoxide dismutase-1 in mice causes amyotrophic lateral sclerosis. Hum Mol Genet 22, 51-60 (2013).
116. Gurney, M. et al. Motor neuron degeneration in mice that express a human Cu,Zn superoxide dismutase mutation. Science 264, 1772-1775 (1994).
117. Taylor, J.P. et al. Toxic proteins in neurodegenerative disease. Science 296, 1991-5 (2002).
118. Bosco, D.A. et al. Wild-type and mutant SOD1 share an aberrant conformation and a common pathogenic pathway in ALS. Nat Neurosci 13, 1396-403 (2010).
119. Chattopadhyay, M. et al. The Disulfide Bond, but Not Zinc or Dimerization, Controls Initiation and Seeded Growth in Amyotrophic Lateral Sclerosis-linked Cu,Zn Superoxide Dismutase (SOD1) Fibrillation. The Journal of biological chemistry 290, 30624-36 (2015).
120. Ezzi, S.A. et al. Wild-type superoxide dismutase acquires binding and toxic properties of ALS-linked mutant forms through oxidation. J Neurochem 102, 170-8 (2007).
121. Gruzman, A. et al. Common molecular signature in SOD1 for both sporadic and familial amyotrophic lateral sclerosis. Proc Natl Acad Sci U S A 104, 12524-9 (2007).
122. Karch, C.M. et al. Role of mutant SOD1 disulfide oxidation and aggregation in the pathogenesis of familial ALS. Proc Natl Acad Sci U S A 106, 7774-9 (2009).
123. Oztug Durer, Z.A. et al. Loss of metal ions, disulfide reduction and mutations related to familial ALS promote formation of amyloid-like aggregates from superoxide dismutase. PLoS One 4, e5004 (2009).
124. Kabashi, E. et al. Oxidized/misfolded superoxide dismutase-1: the cause of all amyotrophic lateral sclerosis? Ann Neurol 62, 553-9 (2007).
125. Jaarsma, D. et al. Human Cu/Zn superoxide dismutase (SOD1) overexpression in mice causes mitochondrial vacuolization, axonal degeneration, and premature motoneuron death and accelerates motoneuron disease in mice expressing a familial amyotrophic lateral sclerosis mutant SOD1. Neurobiol Dis 7, 623-43 (2000).
126. Jonsson, P.A. et al. Motor neuron disease in mice expressing the wild type-like D90A mutant superoxide dismutase-1. J Neuropathol Exp Neurol 65, 1126-36 (2006).
127. Deng, H.X. et al. Conversion to the amyotrophic lateral sclerosis phenotype is associated with intermolecular linked insoluble aggregates of SOD1 in mitochondria. Proc Natl Acad Sci U S A 103, 7142-7 (2006).
128. Prudencio, M. et al. An examination of wild-type SOD1 in modulating the toxicity and aggregation of ALS-associated mutant SOD1. Hum Mol Genet 19, 4774-89 (2010).
129. Wang, L. et al. Wild-type SOD1 overexpression accelerates disease onset of a G85R SOD1 mouse. Hum Mol Genet 18, 1642-51 (2009).
130. Forsberg, K. et al. Novel antibodies reveal inclusions containing non-native SOD1 in sporadic ALS patients. PLoS One 5, e11552 (2010).
131. Pokrishevsky, E. et al. Aberrant localization of FUS and TDP43 is associated with misfolding of SOD1 in amyotrophic lateral sclerosis. PLoS One 7, e35050 (2012).
132. Forsberg, K. et al. Glial nuclear aggregates of superoxide dismutase-1 are regularly present in patients with amyotrophic lateral sclerosis. Acta Neuropathol 121, 623-34 (2011).
133. Grad, L.I. et al. Intercellular propagated misfolding of wild-type Cu/Zn superoxide dismutase occurs via exosome-dependent and -independent mechanisms. Proc Natl Acad Sci U S A 111, 3620-5 (2014).
134. Ayers, J.I. et al. Experimental transmissibility of mutant SOD1 motor neuron disease. Acta Neuropathol 128, 791-803 (2014).
135. Brotherton, T.E. et al. Localization of a toxic form of superoxide dismutase 1 protein to pathologically affected tissues in familial ALS. Proceedings of the National Academy of Sciences of the United States of America 109, 5505-5510 (2012).
136. Kerman, A. et al. Amyotrophic lateral sclerosis is a non-amyloid disease in which extensive misfolding of SOD1 is unique to the familial form, 335-44 (2010).
63
137. Liu, H.N. et al. Lack of evidence of monomer/misfolded superoxide dismutase-1 in sporadic amyotrophic lateral sclerosis. Ann Neurol 66, 75-80 (2009).
138. Pickles, S. et al. Mitochondrial damage revealed by immunoselection for ALS-linked misfolded SOD1. Human molecular genetics 22, 3947-3959 (2013).
139. Dobson, C.M. Protein misfolding, evolution and disease. Trends in Biochemical Sciences 24, 329-332 (1999).
140. Broom, H.R. et al. Destabilization of the dimer interface is a common consequence of diverse ALS-associated mutations in metal free SOD1. Protein Sci 24, 2081-9 (2015).
141. Lindberg, M.J. et al. Systematically perturbed folding patterns of amyotrophic lateral sclerosis (ALS)-associated SOD1 mutants. Proc Natl Acad Sci U S A 102, 9754-9 (2005).
142. Furukawa, Y. et al. Amyotrophic lateral sclerosis mutations have the greatest destabilizing effect on the apo- and reduced form of SOD1, leading to unfolding and oxidative aggregation. J Biol Chem 280, 17266-74 (2005).
143. Ding, F. et al. Dynamical roles of metal ions and the disulfide bond in Cu, Zn superoxide dismutase folding and aggregation. Proceedings of the National Academy of Sciences 105, 19696 (2008).
144. Sipe, J.D. et al. Review: History of the Amyloid Fibril. Journal of Structural Biology 130, 88-98 (2000).
145. Kwong, L.K. et al. TDP-43 Proteinopathies: Neurodegenerative Protein Misfolding Diseases without Amyloidosis. Neurosignals 16, 41-51 (2008).
146. Furukawa, Y. et al. Complete loss of post-translational modifications triggers fibrillar aggregation of SOD1 in the familial form of amyotrophic lateral sclerosis. The Journal of biological chemistry 283, 24167-76 (2008).
147. Wang, J. et al. Fibrillar Inclusions and Motor Neuron Degeneration in Transgenic Mice Expressing Superoxide Dismutase 1 with a Disrupted Copper-Binding Site. Neurobiology of Disease 10, 128-138 (2002).
148. Chan, P.K. et al. Structural similarity of wild-type and ALS-mutant superoxide dismutase-1 fibrils using limited proteolysis and atomic force microscopy. Proceedings of the National Academy of Sciences 110, 10934 (2013).
149. Jaarsma, D. et al. Neuron-specific expression of mutant superoxide dismutase is sufficient to induce amyotrophic lateral sclerosis in transgenic mice. J Neurosci 28, 2075-88 (2008).
150. Stathopulos, P.B. et al. Cu/Zn superoxide dismutase mutants associated with amyotrophic lateral sclerosis show enhanced formation of aggregates <em>in vitro</em>. Proceedings of the National Academy of Sciences 100, 7021 (2003).
151. Chattopadhyay, M. et al. Initiation and elongation in fibrillation of ALS-linked superoxide dismutase. Proc Natl Acad Sci U S A 105, 18663-8 (2008).
152. Chia, R. et al. Superoxide Dismutase 1 and tgSOD1G93A Mouse Spinal Cord Seed Fibrils, Suggesting a Propagative Cell Death Mechanism in Amyotrophic Lateral Sclerosis. PLOS ONE 5, e10627 (2010).
153. Hwang, Y.-M. et al. Nonamyloid aggregates arising from mature copper/zinc superoxide dismutases resemble those observed in amyotrophic lateral sclerosis. The Journal of biological chemistry 285, 41701-41711 (2010).
154. Guest, W.C. et al. Generalization of the Prion Hypothesis to Other Neurodegenerative Diseases: An Imperfect Fit, 1433-59 (2011).
155. Ugalde, C.L. et al. Pathogenic mechanisms of prion protein, amyloid-β and α-synuclein misfolding: the prion concept and neurotoxicity of protein oligomers. Journal of Neurochemistry 139, 162-180 (2016).
156. Collins, S.R. et al. Mechanism of prion propagation: amyloid growth occurs by monomer addition. PLoS Biol 2, e321 (2004).
157. Kabir, M.E. et al. Implications of prion adaptation and evolution paradigm for human neurodegenerative diseases. Prion 8, 111-116 (2014).
158. Frost, B. et al. Prion-like mechanisms in neurodegenerative diseases. Nat Rev Neurosci 11, 155-9 (2010).
159. Grad, L.I. et al. Intermolecular transmission of superoxide dismutase 1 misfolding in living cells. Proc Natl Acad Sci U S A 108, 16398-403 (2011).
160. Munch, C. et al. Prion-like propagation of mutant superoxide dismutase-1 misfolding in neuronal cells. Proc Natl Acad Sci U S A 108, 3548-53 (2011).
161. Silverman, J.M. et al. Disease Mechanisms in ALS: Misfolded SOD1 Transferred Through Exosome-Dependent and Exosome-Independent Pathways. Cell Mol Neurobiol 36, 377-81 (2016).

64
162. Pokrishevsky, E. et al. Spinal cord homogenates from SOD1 familial amyotrophic lateral sclerosis induce SOD1 aggregation in living cells. PloS one 12, e0184384-e0184384 (2017).
163. Ayers, J.I. et al. Prion-like propagation of mutant SOD1 misfolding and motor neuron disease spread along neuroanatomical pathways. Acta Neuropathol 131, 103-14 (2016).
164. Bett, C. et al. Biochemical properties of highly neuroinvasive prion strains. PLoS pathogens 8, e1002522-e1002522 (2012).
165. Kaufman, S.K. et al. Tau Prion Strains Dictate Patterns of Cell Pathology, Progression Rate, and Regional Vulnerability In Vivo. Neuron 92, 796-812 (2016).
166. Sanders, D.W. et al. Distinct tau prion strains propagate in cells and mice and define different tauopathies. Neuron 82, 1271-1288 (2014).
167. Qiang, W. et al. Structural variation in amyloid-β fibrils from Alzheimer's disease clinical subtypes. Nature 541, 217-221 (2017).
168. Bousset, L. et al. Structural and functional characterization of two alpha-synuclein strains. Nature communications 4, 2575-2575 (2013).
169. Guo, J.L. et al. Distinct α-synuclein strains differentially promote tau inclusions in neurons. Cell 154, 103-117 (2013).
170. Furukawa, Y. et al. Mutation-dependent polymorphism of Cu,Zn-superoxide dismutase aggregates in the familial form of amyotrophic lateral sclerosis. The Journal of biological chemistry 285, 22221-22231 (2010).
171. Toichi, K. et al. Disulfide scrambling describes the oligomer formation of superoxide dismutase (SOD1) proteins in the familial form of amyotrophic lateral sclerosis. J Biol Chem 288, 4970-80 (2013).
172. Bergh, J. et al. Structural and kinetic analysis of protein-aggregate strains in vivo using binary epitope mapping. Proc Natl Acad Sci U S A 112, 4489-94 (2015).
173. Bidhendi, E.E. et al. Two superoxide dismutase prion strains transmit amyotrophic lateral sclerosis-like disease. J Clin Invest 126, 2249-53 (2016).
174. Bidhendi, E.E. et al. Mutant superoxide dismutase aggregates from human spinal cord transmit amyotrophic lateral sclerosis. Acta Neuropathologica (2018).
175. Van Damme, P. et al. Modelling amyotrophic lateral sclerosis: progress and possibilities. Disease Models &amp; Mechanisms 10, 537 (2017).
176. Dawson, T.M. et al. Animal models of neurodegenerative diseases. Nature Neuroscience 21, 1370-1379 (2018).
177. Kabuta, T. et al. Degradation of amyotrophic lateral sclerosis-linked mutant Cu,Zn-superoxide dismutase proteins by macroautophagy and the proteasome. J Biol Chem 281, 30524-33 (2006).
178. Kawamata, H. et al. Different regulation of wild-type and mutant Cu,Zn superoxide dismutase localization in mammalian mitochondria. Human molecular genetics 17, 3303-3317 (2008).
179. Prudencio, M. et al. Variation in aggregation propensities among ALS-associated variants of SOD1: correlation to human disease. Human molecular genetics 18, 3217-3226 (2009).
180. Zhang, F. et al. Interaction between Familial Amyotrophic Lateral Sclerosis (ALS)-linked SOD1 Mutants and the Dynein Complex. Journal of Biological Chemistry 282, 16691-16699 (2007).
181. Palmer, T.D. et al. Cell culture. Progenitor cells from human brain after death. Nature 411, 42-3 (2001).
182. Schwartz, P.H. et al. Isolation and characterization of neural progenitor cells from post-mortem human cortex. Journal of Neuroscience Research 74, 838-851 (2003).
183. De Groot, C.J.A. et al. Establishment of human adult astrocyte cultures derived from postmortem multiple sclerosis and control brain and spinal cord regions: immunophenotypical and functional characterization. Journal of Neuroscience Research 49, 342-354 (1998).
184. Song, H.-j. et al. Neural stem cells from adult hippocampus develop essential properties of functional CNS neurons. Nature Neuroscience 5, 438 (2002).
185. Akira, S. et al. Pathogen Recognition and Innate Immunity. Cell 124, 783-801 (2006). 186. McKay, R. Stem Cells in the Central Nervous System. Science 276, 66 (1997). 187. Temple, S. et al. Stem cells in the adult mammalian central nervous system. Current
Opinion in Neurobiology 9, 135-141 (1999). 188. Haidet-Phillips, A.M. et al. Astrocytes from familial and sporadic ALS patients are toxic to
motor neurons. Nat Biotechnol 29, 824-8 (2011).
65
189. Re, Diane B. et al. Necroptosis Drives Motor Neuron Death in Models of Both Sporadic and Familial ALS. Neuron 81, 1001-1008 (2014).
190. Raman, R. et al. Gene expression signatures in motor neurone disease fibroblasts reveal dysregulation of metabolism, hypoxia-response and RNA processing functions. Neuropathol Appl Neurobiol 41, 201-26 (2015).
191. Onesto, E. et al. Gene-specific mitochondria dysfunctions in human TARDBP and C9ORF72 fibroblasts. Acta neuropathologica communications 4, 47-47 (2016).
192. Allen, S.P. et al. Altered age-related changes in bioenergetic properties and mitochondrial morphology in fibroblasts from sporadic amyotrophic lateral sclerosis patients. Neurobiology of Aging 36, 2893-2903 (2015).
193. Kirk, K. et al. Bioenergetic markers in skin fibroblasts of sporadic amyotrophic lateral sclerosis and progressive lateral sclerosis patients. Annals of neurology 76, 620-624 (2014).
194. Konrad, C. et al. Fibroblast bioenergetics to classify amyotrophic lateral sclerosis patients. Molecular neurodegeneration 12, 76-76 (2017).
195. Orrù, S. et al. Reduced stress granule formation and cell death in fibroblasts with the A382T mutation of TARDBP gene: evidence for loss of TDP-43 nuclear function. Human Molecular Genetics 25, 4473-4483 (2016).
196. Sabatelli, M. et al. Primary fibroblasts cultures reveal TDP-43 abnormalities in amyotrophic lateral sclerosis patients with and without SOD1 mutations. Neurobiol Aging 36, 2005 e5-2005 e13 (2015).
197. Allen, S.P. et al. Superoxide dismutase 1 mutation in a cellular model of amyotrophic lateral sclerosis shifts energy generation from oxidative phosphorylation to glycolysis. Neurobiol Aging 35, 1499-509 (2014).
198. Thomson, J.A. et al. Embryonic Stem Cell Lines Derived from Human Blastocysts. Science 282, 1145 (1998).
199. Warren, L. et al. Highly efficient reprogramming to pluripotency and directed differentiation of human cells with synthetic modified mRNA. Cell Stem Cell 7, 618-30 (2010).
200. Loh, Y.-H. et al. Generation of induced pluripotent stem cells from human blood. Blood 113, 5476 (2009).
201. Kim, J. et al. Reprogramming of Postnatal Neurons into Induced Pluripotent Stem Cells by Defined Factors. STEM CELLS 29, 992-1000 (2011).
202. Yu, J. et al. Induced pluripotent stem cell lines derived from human somatic cells. Science 318, 1917-20 (2007).
203. Malik, N. et al. A review of the methods for human iPSC derivation. Methods Mol Biol 997, 23-33 (2013).
204. Serio, A. et al. Astrocyte pathology and the absence of non-cell autonomy in an induced pluripotent stem cell model of TDP-43 proteinopathy. Proc Natl Acad Sci U S A 110, 4697-702 (2013).
205. Almeida, S. et al. Induced Pluripotent Stem Cell Models of Progranulin-Deficient Frontotemporal Dementia Uncover Specific Reversible Neuronal Defects. Cell Reports 2, 789-798 (2012).
206. Ferraiuolo, L. et al. Oligodendrocytes contribute to motor neuron death in ALS via SOD1-dependent mechanism. Proc Natl Acad Sci U S A 113, E6496-E6505 (2016).
207. Livesey, M.R. et al. Maturation and electrophysiological properties of human pluripotent stem cell-derived oligodendrocytes. Stem cells (Dayton, Ohio) 34, 1040-1053 (2016).
208. Lenzi, J. et al. Differentiation of control and ALS mutant human iPSCs into functional skeletal muscle cells, a tool for the study of neuromuscolar diseases. Stem Cell Research 17, 140-147 (2016).
209. Sances, S. et al. Modeling ALS with motor neurons derived from human induced pluripotent stem cells. Nat Neurosci 16, 542-53 (2016).
210. Chambers, S.M. et al. Highly efficient neural conversion of human ES and iPS cells by dual inhibition of SMAD signaling. Nat Biotechnol 27, 275-80 (2009).
211. Wichterle, H. et al. Directed Differentiation of Embryonic Stem Cells into Motor Neurons. Cell 110, 385-397 (2002).
212. Bhinge, A. et al. Genetic Correction of SOD1 Mutant iPSCs Reveals ERK and JNK Activated AP1 as a Driver of Neurodegeneration in Amyotrophic Lateral Sclerosis. Stem Cell Reports 8, 856-869 (2017).
213. Chen, H. et al. Modeling ALS with iPSCs reveals that mutant SOD1 misregulates neurofilament balance in motor neurons. Cell Stem Cell 14, 796-809 (2014).
66
214. Kiskinis, E. et al. Pathways disrupted in human ALS motor neurons identified through genetic correction of mutant SOD1. Cell Stem Cell 14, 781-95 (2014).
215. Wainger, B.J. et al. Intrinsic membrane hyperexcitability of amyotrophic lateral sclerosis patient-derived motor neurons. Cell Rep 7, 1-11 (2014).
216. Kato, S. Amyotrophic lateral sclerosis models and human neuropathology: similarities and differences. Acta Neuropathol 115, 97-114 (2008).
217. Johnston, J.A. et al. Formation of high molecular weight complexes of mutant Cu, Zn-superoxide dismutase in a mouse model for familial amyotrophic lateral sclerosis. Proceedings of the National Academy of Sciences of the United States of America 97, 12571-12576 (2000).
218. Hall, E.D. et al. Relationship of microglial and astrocytic activation to disease onset and progression in a transgenic model of familial ALS. Glia 23, 249-56 (1998).
219. Canto, M.C.D. et al. A low expressor line of transgenic mice carrying a mutant human Cu,Zn superoxide dismutase (SOD1) gene develops pathological changes that most closely resemble those in human amyotrophic lateral sclerosis. Acta Neuropathol 93, 537-50 (1997).
220. Chiu, A.Y. et al. Age-Dependent Penetrance of Disease in a Transgenic Mouse Model of Familial Amyotrophic Lateral Sclerosis. Molecular and Cellular Neuroscience 6, 349-362 (1995).
221. Wong, P.C. et al. An adverse property of a familial ALS-linked SOD1 mutation causes motor neuron disease characterized by vacuolar degeneration of mitochondria. Neuron 14(1995).
222. Sasaki, S. et al. Motor Neuron Disease in Transgenic Mice With an H46R Mutant SOD1 Gene. Journal of Neuropathology & Experimental Neurology 66, 517-524 (2007).
223. Jonsson, P.A. et al. Minute quantities of misfolded mutant superoxide dismutase-1 cause amyotrophic lateral sclerosis. Brain 127, 73-88 (2004).
224. Epstein, C.J. et al. Transgenic mice with increased Cu/Zn-superoxide dismutase activity: animal model of dosage effects in Down syndrome. Proc Natl Acad Sci U S A 84, 8044-8 (1987).
225. Heiman-Patterson, T.D. et al. Effect of genetic background on phenotype variability in transgenic mouse models of amyotrophic lateral sclerosis: A window of opportunity in the search for genetic modifiers. Amyotrophic Lateral Sclerosis 12, 79-86 (2011).
226. Alexander, G.M. et al. Effect of transgene copy number on survival in the G93A SOD1 transgenic mouse model of ALS. Molecular Brain Research 130, 7-15 (2004).
227. Behring, E. et al. Über das Zustandekommen der Diphtherie-Immunität und der Tetanus-Immunität bei Thieren. Dtsch Med Wochenschrift 49, 1113–1114 (1890).
228. Kaufmann, S.H.E. Remembering Emil von Behring: from Tetanus Treatment to Antibody Cooperation with Phagocytes. mBio 8(2017).
229. Beutler, B. Innate immunity: an overview. Molecular Immunology 40, 845-859 (2004). 230. Hoffmann, J.A. The immune response of Drosophila. Nature 426, 33 (2003). 231. Janeway, C.A. et al. Innate Immune Recognition. Annual Review of Immunology 20, 197-
216 (2002). 232. Knowles, M.R. et al. Mucus clearance as a primary innate defense mechanism for
mammalian airways. The Journal of Clinical Investigation 109, 571-577 (2002). 233. Medzhitov, R. et al. Decoding the Patterns of Self and Nonself by the Innate Immune
System. Science 296, 298 (2002). 234. Hoffman, W. et al. B Cells, Antibodies, and More. Clinical Journal of the American
Society of Nephrology : CJASN 11, 137-154 (2016). 235. Paul, W.E. Fundamental Immunology. LIPPINCOTT WILLIAMS & WILKINS, a
WOLTERS KLUWER business 7th Edition(2013). 236. Inbar, D. et al. Localization of Antibody-Combining Sites within the Variable Portions of
Heavy and Light Chains. Proceedings of the National Academy of Sciences of the United States of America 69, 2659-2662 (1972).
237. Kabat, E.A. et al. Unusual distributions of amino acids in complementarity-determining (hypervariable) segments of heavy and light chains of immunoglobulins and their possible roles in specificity of antibody-combining sites. J. Biol. Chem. 252, 6609-16 (1977).
238. Kirkham, P.M. et al. Antibody structure and the evolution of immunoglobulin V gene segments. Seminars in Immunology 6, 347-360 (1994).
239. Padlan, E.A. et al. Identification of specificity-determining residues in antibodies. The FASEB Journal 9, 133-139 (1995).

67
240. MacCallum, R.M. et al. Antibody-antigen Interactions: Contact Analysis and Binding Site Topography. Journal of Molecular Biology 262, 732-745 (1996).
241. Tonegawa, S. Somatic generation of antibody diversity. Nature 302, 575-581 (1983). 242. Li, Z. et al. The generation of antibody diversity through somatic hypermutation and class
switch recombination. Genes & Dev. 18, 1-11 (2004). 243. Jennewein, M.F. et al. The Immunoregulatory Roles of Antibody Glycosylation. Trends in
Immunology 38, 358-372 (2017). 244. Sela-Culang, I. et al. The Structural Basis of Antibody-Antigen Recognition. Frontiers in
Immunology 4(2013). 245. Ravetch, J.V. et al. Fc Receptors. Annual Review of Immunology 9, 457-492 (1991). 246. Huber, R. et al. Antibody–antigen flexibility. Nature 326, 334 (1987). 247. Oi, V.T. et al. Correlation between segmental flexibility and effector function of
antibodies. Nature 307, 136 (1984). 248. Woof, J.M. et al. Mucosal immunoglobulins. Immunological Reviews 206, 64-82 (2005). 249. Chen, K. et al. The Function and Regulation of Immunoglobulin D. Current opinion in
immunology 23, 345-352 (2011). 250. Oettgen, H.C. Fifty years later: Emerging functions of IgE antibodies in host defense,
immune regulation, and allergic diseases. The Journal of allergy and clinical immunology 137, 1631-1645 (2016).
251. Boes, M. Role of natural and immune IgM antibodies in immune responses. Molecular Immunology 37, 1141-1149 (2000).
252. Bazin, H. et al. Three classes and four (sub)classes of rat immunoglobulins: IgM, IgA, Ige and IgG1, IgG2a, IgG2b, IgG2c. European Journal of Immunology 4, 44-48 (1974).
253. Collins, A.M. IgG subclass co-expression brings harmony to the quartet model of murine IgG function. Immunology and Cell Biology 94, 949-954 (2016).
254. Vidarsson, G. et al. IgG Subclasses and Allotypes: From Structure to Effector Functions. Frontiers in Immunology 5, 520 (2014).
255. Braunstein, G.D. et al. Serum human chorionic gonadotropin levels throughout normal pregnancy. American Journal of Obstetrics and Gynecology 126, 678-681 (1976).
256. Jaffe, A.S. et al. Biomarkers in Acute Cardiac Disease: The Present and the Future. Journal of the American College of Cardiology 48, 1-11 (2006).
257. Ross, J.S. et al. The HER-2/neu Gene and Protein in Breast Cancer 2003: Biomarker and Target of Therapy. The Oncologist 8, 307-325 (2003).
258. Wang, J. et al. Correlation of serum allergy (IgE) tests performed by different assay systems. Journal of Allergy and Clinical Immunology 121, 1219-1224 (2008).
259. Goldman, R.D. Antibodies: indispensable tools for biomedical research. Trends in Biochemical Sciences 25, 593-595 (2000).
260. Kaplon, H. et al. Antibodies to watch in 2018. mAbs 10, 183-203 (2018). 261. Ekins, R. et al. Point On the meaning of “sensitivity”. Clinical Chemistry 43, 1824-1831
(1997). 262. Greenspan, N.S. Affinity, complementarity, cooperativity, and specificity in antibody
recognition. Curr Top Microbiol Immunol 260, 65-85 (2001). 263. Greenspan, N.S. et al. Complementarity, specificity and the nature of epitopes and
paratopes in multivalent intereactions. Immunology Today 16, 226-230 (1995). 264. Rispens, T. et al. Label-free assessment of high-affinity antibody–antigen binding
constants. Comparison of bioassay, SPR, and PEIA-ellipsometry. Journal of Immunological Methods 365, 50-57 (2011).
265. Pasquale, A.D. et al. Vaccine Adjuvants: from 1920 to 2015 and Beyond. Vaccines 3, 320-343 (2015).
266. Uhlen, M. et al. Antibody-based Proteomics for Human Tissue Profiling. Molecular &amp; Cellular Proteomics 4, 384 (2005).
267. Köhler, G. et al. Continuous cultures of fused cells secreting antibody of predefined specificity. Nature 256, 495 (1975).
268. Liu, J.K.H. The history of monoclonal antibody development – Progress, remaining challenges and future innovations. Annals of Medicine and Surgery 3, 113-116 (2014).
269. Bradbury, A.R.M. et al. Beyond natural antibodies: the power of in vitro display technologies. Nature biotechnology 29, 245-254 (2011).
270. Fields, C. et al. Creation of recombinant antigen-binding molecules derived from hybridomas secreting specific antibodies. Nature Protocols 8, 1125 (2013).
271. Hust, M. et al. A human scFv antibody generation pipeline for proteome research. Journal of Biotechnology 152, 159-170 (2011).

68
272. Steinhauer, C. et al. Single framework recombinant antibody fragments designed for protein chip applications. Biotechniques Suppl, 38-45 (2002).
273. Hudson, P.J. et al. High avidity scFv multimers; diabodies and triabodies. Journal of Immunological Methods 231, 177-189 (1999).
274. Hamers-Casterman, C. et al. Naturally occurring antibodies devoid of light chains. Nature 363, 446-448 (1993).
275. Chakravarty, R. et al. Nanobody: the "magic bullet" for molecular imaging? Theranostics 4, 386-398 (2014).
276. Van Audenhove, I. et al. Nanobodies as Versatile Tools to Understand, Diagnose, Visualize and Treat Cancer. EBioMedicine 8, 40-48 (2016).
277. Eigenbrot, C. et al. Structural basis for high-affinity HER2 receptor binding by an engineered protein. Proceedings of the National Academy of Sciences 107, 15039 (2010).
278. Kintzing, J.R. et al. Engineered knottin peptides as diagnostics, therapeutics, and drug delivery vehicles. Current Opinion in Chemical Biology 34, 143-150 (2016).
279. Yu, X. et al. Beyond Antibodies as Binding Partners: The Role of Antibody Mimetics in Bioanalysis. Annual Review of Analytical Chemistry 10, 293-320 (2017).
280. Löfblom, J. et al. Affibody molecules: Engineered proteins for therapeutic, diagnostic and biotechnological applications. FEBS Letters 584, 2670-2680 (2010).
281. Kolmar, H. Biological diversity and therapeutic potential of natural and engineered cystine knot miniproteins. Current Opinion in Pharmacology 9, 608-614 (2009).
282. Schmidtko, A. et al. Ziconotide for treatment of severe chronic pain. The Lancet 375, 1569-1577 (2010).
283. Lakhin, A.V. et al. Aptamers: problems, solutions and prospects. Acta naturae 5, 34-43 (2013).
284. Song, K.-M. et al. Aptamers and their biological applications. Sensors (Basel, Switzerland) 12, 612-631 (2012).
285. Gros-Louis, F. et al. Intracerebroventricular infusion of monoclonal antibody or its derived Fab fragment against misfolded forms of SOD1 mutant delays mortality in a mouse model of ALS. Journal of Neurochemistry 113, 1188-1199 (2010).
286. Vande Velde, C. et al. Selective association of misfolded ALS-linked mutant SOD1 with the cytoplasmic face of mitochondria. Proc Natl Acad Sci U S A 105, 4022-7 (2008).
287. Rakhit, R. et al. An immunological epitope selective for pathological monomer-misfolded SOD1 in ALS. Nature Medicine 13, 754 (2007).
288. Valera, E. et al. Immunotherapeutic Approaches Targeting Amyloid-β, α-Synuclein, and Tau for the Treatment of Neurodegenerative Disorders. Neurotherapeutics : the journal of the American Society for Experimental NeuroTherapeutics 13, 179-189 (2016).
289. Folch, J. et al. Current Research Therapeutic Strategies for Alzheimer’s Disease Treatment. Neural Plasticity 2016, 15 (2016).
290. Gilman, S. et al. Clinical effects of Aβ immunization (AN1792) in patients with AD in an interrupted trial. Neurology 64, 1553 (2005).
291. Bard, F. et al. Epitope and isotype specificities of antibodies to beta -amyloid peptide for protection against Alzheimer's disease-like neuropathology. Proc Natl Acad Sci U S A 100, 2023-2028 (2003).
292. Winblad, B. et al. Active immunotherapy options for Alzheimer’s disease. Alzheimer's Research & Therapy 6, 7 (2014).
293. Lemere, C.A. Immunotherapy for Alzheimer's disease: hoops and hurdles. Molecular neurodegeneration 8, 36-36 (2013).
294. Neuwelt, E.A. et al. Engaging neuroscience to advance translational research in brain barrier biology. Nature reviews. Neuroscience 12, 169-182 (2011).
295. Freskgård, P.-O. et al. Antibody therapies in CNS diseases. Neuropharmacology 120, 38-55 (2017).
296. Yu, Y.J. et al. Developing therapeutic antibodies for neurodegenerative disease. Neurotherapeutics : the journal of the American Society for Experimental NeuroTherapeutics 10, 459-472 (2013).
297. Ryman, J.T. et al. Pharmacokinetics of Monoclonal Antibodies. CPT: pharmacometrics & systems pharmacology 6, 576-588 (2017).
298. Calias, P. et al. Intrathecal delivery of protein therapeutics to the brain: A critical reassessment. Pharmacology & Therapeutics 144, 114-122 (2014).
299. Valera, E. et al. Immunotherapy for neurodegenerative diseases: focus on α-synucleinopathies. Pharmacology & therapeutics 138, 311-322 (2013).

69
300. Hutter-Saunders, J.A.L. et al. Pathways towards an effective immunotherapy for Parkinson's disease. Expert review of neurotherapeutics 11, 1703-1715 (2011).
301. Mandler, M. et al. Active immunization against alpha-synuclein ameliorates the degenerative pathology and prevents demyelination in a model of multiple system atrophy. Molecular neurodegeneration 10, 10-10 (2015).
302. Schott, J.M. et al. Inflammation in Alzheimer’s disease: insights from immunotherapy. Brain 136, 2654-2656 (2013).
303. Doody, R.S. et al. Phase 3 Trials of Solanezumab for Mild-to-Moderate Alzheimer's Disease. New England Journal of Medicine 370, 311-321 (2014).
304. Salloway, S. et al. Two phase 3 trials of bapineuzumab in mild-to-moderate Alzheimer's disease. The New England journal of medicine 370, 322-333 (2014).
305. Vandenberghe, R. et al. Bapineuzumab for mild to moderate Alzheimer’s disease in two global, randomized, phase 3 trials. Alzheimer's Research & Therapy 8, 18 (2016).
306. Sevigny, J. et al. The antibody aducanumab reduces Aβ plaques in Alzheimer’s disease. Nature 537, 50 (2016).
307. Liu, H.-N. et al. Targeting of Monomer/Misfolded SOD1 as a Therapeutic Strategy for Amyotrophic Lateral Sclerosis. The Journal of Neuroscience 32, 8791 (2012).
308. Takeuchi, S. et al. Induction of Protective Immunity by Vaccination With Wild-Type Apo Superoxide Dismutase 1 in Mutant SOD1 Transgenic Mice. Journal of Neuropathology & Experimental Neurology 69, 1044-1056 (2010).
309. Urushitani, M. et al. Therapeutic effects of immunization with mutant superoxide dismutase in mice models of amyotrophic lateral sclerosis. Proceedings of the National Academy of Sciences 104, 2495 (2007).
310. Sábado, J. et al. Adverse effects of a SOD1-peptide immunotherapy on SOD1G93A mouse slow model of amyotrophic lateral sclerosis. Neuroscience 310, 38-50 (2015).
311. Maier, M. et al. A human-derived antibody targets misfolded SOD1 and ameliorates motor symptoms in mouse models of amyotrophic lateral sclerosis. Science Translational Medicine 10, eaah3924 (2018).
312. Boulting, G.L. et al. A functionally characterized test set of human induced pluripotent stem cells. Nat Biotechnol 29, 279-86 (2011).
313. Dimos, J.T. et al. Induced pluripotent stem cells generated from patients with ALS can be differentiated into motor neurons. Science 321, 1218-21 (2008).
314. Li, Y. et al. A comprehensive library of familial human amyotrophic lateral sclerosis induced pluripotent stem cells. PLoS One 10, e0118266 (2015).
315. Okita, K. et al. A more efficient method to generate integration-free human iPS cells. Nat Methods 8, 409-12 (2011).
316. Amoroso, M.W. et al. Accelerated high-yield generation of limb-innervating motor neurons from human stem cells. J Neurosci 33, 574-86 (2013).
317. Roybon, L. et al. Human stem cell-derived spinal cord astrocytes with defined mature or reactive phenotypes. Cell Rep 4, 1035-1048 (2013).
318. Jonsson, P.A. et al. Disulphide-reduced superoxide dismutase-1 in CNS of transgenic amyotrophic lateral sclerosis models. Brain 129, 451-64 (2006).
319. Zetterstrom, P. et al. Misfolded superoxide dismutase-1 in CSF from amyotrophic lateral sclerosis patients. J Neurochem 117, 91-9 (2011).
320. Ayers, J.I. et al. Conformational specificity of the C4F6 SOD1 antibody; low frequency of reactivity in sporadic ALS cases. Acta Neuropathol Commun 2:55(2014).
321. Amendola, J. et al. Morphological differences between wild-type and transgenic superoxide dismutase 1 lumbar motoneurons in postnatal mice. Journal of Comparative Neurology 511, 329-341 (2008).
322. Saxena, S. et al. A role for motoneuron subtype-selective ER stress in disease manifestations of FALS mice. Nat Neurosci 12, 627-36 (2009).
323. Azzouz, M. et al. Progressive motor neuron impairment in an animal model of familial amyotrophic lateral sclerosis. Muscle & Nerve 20, 45-51 (1997).
324. Mourelatos, Z. et al. The Golgi apparatus of spinal cord motor neurons in transgenic mice expressing mutant Cu,Zn superoxide dismutase becomes fragmented in early, preclinical stages of the disease. Proceedings of the National Academy of Sciences of the United States of America 93, 5472-5477 (1996).
325. Williamson, T.L. et al. Slowing of axonal transport is a very early event in the toxicity of ALS–linked SOD1 mutants to motor neurons. Nature Neuroscience 2, 50 (1999).
70
326. Quinlan, K.A. et al. Altered postnatal maturation of electrical properties in spinal motoneurons in a mouse model of amyotrophic lateral sclerosis. The Journal of physiology 589, 2245-2260 (2011).
327. van Zundert, B. et al. Neonatal neuronal circuitry shows hyperexcitable disturbance in a mouse model of the adult-onset neurodegenerative disease amyotrophic lateral sclerosis. The Journal of neuroscience : the official journal of the Society for Neuroscience 28, 10864-10874 (2008).
328. Gerber, Y.N. et al. Early Functional Deficit and Microglial Disturbances in a Mouse Model of Amyotrophic Lateral Sclerosis. PLOS ONE 7, e36000 (2012).
329. Brotherton, T.E. et al. Cellular toxicity of mutant SOD1 protein is linked to an easily soluble, non-aggregated form in vitro. Neurobiology of disease 49, 49-56 (2013).
330. Weisberg, S.J. et al. Compartmentalization of superoxide dismutase 1 (SOD1G93A) aggregates determines their toxicity. Proc Natl Acad Sci U S A 109, 15811-6 (2012).
331. Bergemalm, D. et al. Overloading of stable and exclusion of unstable human superoxide dismutase-1 variants in mitochondria of murine amyotrophic lateral sclerosis models. J Neurosci 26, 4147-54 (2006).
332. Bock, C. et al. Reference Maps of human ES and iPS cell variation enable high-throughput characterization of pluripotent cell lines. Cell 144, 439-52 (2011).
333. Hu, B.-Y. et al. Neural differentiation of human induced pluripotent stem cells follows developmental principles but with variable potency. Proceedings of the National Academy of Sciences 107, 4335 (2010).
334. Kim, H.S. et al. Genomic editing tools to model human diseases with isogenic pluripotent stem cells. Stem cells and development 23, 2673-2686 (2014).
335. Di Giorgio, F.P. et al. Non-cell autonomous effect of glia on motor neurons in an embryonic stem cell-based ALS model. Nat Neurosci 10, 608-14 (2007).
336. Wang, L. et al. Astrocyte loss of mutant SOD1 delays ALS disease onset and progression in G85R transgenic mice. Hum Mol Genet 20, 286-93 (2011).
337. Yamanaka, K. et al. Astrocytes as determinants of disease progression in inherited amyotrophic lateral sclerosis. Nat Neurosci 11, 251-3 (2008).
338. Lang, L. et al. Fibrillation precursor of superoxide dismutase 1 revealed by gradual tuning of the protein-folding equilibrium. Proceedings of the National Academy of Sciences of the United States of America 109, 17868-73 (2012).
339. Zetterstrom, P. et al. Composition of soluble misfolded superoxide dismutase-1 in murine models of amyotrophic lateral sclerosis. Neuromolecular Med 15, 147-58 (2013).
340. Iadecola, C. The Neurovascular Unit Coming of Age: A Journey through Neurovascular Coupling in Health and Disease. Neuron 96, 17-42 (2017).
341. Rosenbohm, A. et al. Can lesions to the motor cortex induce amyotrophic lateral sclerosis? Journal of neurology 261, 283-90 (2014).
342. Culotta, V.C. et al. The copper chaperone for superoxide dismutase. J Biol Chem 272, 23469-72 (1997).
343. Chattopadhyay, M. et al. Initiation and elongation in fibrillation of ALS-linked superoxide dismutase. Proceedings of the National Academy of Sciences of the United States of America 105, 18663-8 (2008).
344. Bergemalm, D. et al. Superoxide dismutase-1 and other proteins in inclusions from transgenic amyotrophic lateral sclerosis model mice. J Neurochem 114, 408-18 (2010).
345. Miller, A.F. Superoxide dismutases: ancient enzymes and new insights. FEBS Lett 586, 585-95 (2012).
346. Jones, D.P. et al. Cysteine/cystine couple is a newly recognized node in the circuitry for biologic redox signaling and control. The FASEB Journal 18, 1246-1248 (2004).
347. Carroll, M.C. et al. The effects of glutaredoxin and copper activation pathways on the disulfide and stability of Cu,Zn superoxide dismutase. J Biol Chem 281, 28648-56 (2006).
348. Begas, P. et al. Glutaredoxin catalysis requires two distinct glutathione interaction sites. Nature communications 8, 14835-14835 (2017).
349. Grad, L.I. et al. Exosome-dependent and independent mechanisms are involved in prion-like transmission of propagated Cu/Zn superoxide dismutase misfolding. Prion 8, 331-335 (2014).
350. Rakhit, R. et al. An immunological epitope selective for pathological monomer-misfolded SOD1 in ALS. Nat Med 13, 754-9 (2007).
351. Tokuda, E. et al. Immunochemical characterization on pathological oligomers of mutant Cu/Zn-superoxide dismutase in amyotrophic lateral sclerosis. Molecular Neurodegeneration 12, 2 (2017).

71
352. Da Cruz, S. et al. Misfolded SOD1 is not a primary component of sporadic ALS. Acta neuropathologica 134, 97-111 (2017).
353. Jucker, M. et al. Self-propagation of pathogenic protein aggregates in neurodegenerative diseases. Nature 501, 45-51 (2013).
354. Brundin, P. et al. Prion-like transmission of protein aggregates in neurodegenerative diseases. Nat Rev Mol Cell Biol 11, 301-7 (2010).
355. Kringelum, J.V. et al. Structural analysis of B-cell epitopes in antibody:protein complexes. Molecular immunology 53, 24-34 (2013).
356. Vieira, P. et al. The half-lives of serum immunoglobulins in adult mice. European Journal of Immunology 18, 313-316 (1988).
357. Lindberg, M.J. et al. Common denominator of Cu/Zn superoxide dismutase mutants associated with amyotrophic lateral sclerosis: decreased stability of the apo state. Proc Natl Acad Sci U S A 99, 16607-12 (2002).
358. Rodriguez, J.A. et al. Destabilization of apoprotein is insufficient to explain Cu,Zn-superoxide dismutase-linked ALS pathogenesis. Proceedings of the National Academy of Sciences of the United States of America 102, 10516 (2005).
359. Sekhar, A. et al. Probing the free energy landscapes of ALS disease mutants of SOD1 by NMR spectroscopy. Proceedings of the National Academy of Sciences 113, E6939 (2016).
360. Kim, S.-W. et al. Immunohistochemistry for Pathologists: Protocols, Pitfalls, and Tips. Journal of pathology and translational medicine 50, 411-418 (2016).
361. Weihofen, A. et al. Development of an aggregate-selective, human-derived α-synuclein antibody BIIB054 that ameliorates disease phenotypes in Parkinson's disease models. Neurobiology of Disease 124, 276-288 (2019).
362. Reverberi, R. et al. Factors affecting the antigen-antibody reaction. Blood transfusion = Trasfusione del sangue 5, 227-240 (2007).
363. Zhang, Z. et al. Possible allelic structure of IgG2a and IgG2c in mice. Molecular Immunology 50, 169-171 (2012).

