smoke free buddhist monks and buddhism: buddhist monk and community survey questionnaire of five...
TRANSCRIPT

S u r v e y S u m m a r y
Smoking and Buddhism: Buddhist Monk and Community survey
questionnaire of five provinces in Cambodia.
Analysis and presentation of results from 2001 to 2004
Smoke Free Cambodian Communities Project
ADRA Cambodia
March 21, 2005
SFCC 2004 Survey Summary. March 21, 2005 2
Summary of Findings Buddhist monks
• The total functional sample size is 1936. • The total weighted smoking prevalence of Buddhist monks is 23.4%.
• The total weighted prevalence dropped 12.9% from 2001 to 2004. • Similar to 2001, Siem Reap had the highest prevalence at 37.5%, while
Phnom Penh had the lowest at 14.6%.
• The province with the greatest prevalence drop was Kampot province; it dropped from 34.5% in 2001 to 15.4% in 2004.
Community
• The total functional sample size is 2622 in five Cambodian provinces. • Only men were surveyed; they were asked what their wife’s smoking status is. • The weighted prevalence for men in all five provinces in 2004 is 43.3%. • The weighted prevalence for women in all five provinces is 4.0%. • For men, the un-weighted prevalence is the highest in Pousat at 56.0%, while
it is the lowest in Phnom Penh at 25.9%. • For women, the un-weighted prevalence is the highest in Siem Reap province
at 7.3% and the lowest in Phnom Penh at 2.48%.
SFCC 2004 Survey Summary. March 21, 2005 3
Table of Contents Summary of Findings........................................................................................... 2
1. Introduction ........................................................................................4 1.1 Background / justification ............................................................................. 5 1.2 Goal of survey: ............................................................................................... 6 1.3 Dates of the survey: ....................................................................................... 7
2. Methods..............................................................................................7 2.1 Survey Questionnaire .................................................................................... 7 2.2 Sample size..................................................................................................... 7 2.3 Power .............................................................................................................. 9 2.4 Design (Intervention/Control)...................................................................... 10
3. Results – Buddhist Monk Survey ...................................................12 3.1 Smoking Prevalence .................................................................................... 12 3.2 Practices of smoking ................................................................................... 17 3.3 Practices of current smokers...................................................................... 20 3.4 Attitudes toward an intervention ................................................................ 22 3.5 Attitudes about smoking ............................................................................. 23 3.6 Knowledge of Smoking and health............................................................. 26 3.7 Regression.................................................................................................... 28 3.8 Results of additional pagoda survey.......................................................... 30
4. Results - Community Survey ..........................................................30 4.1 Smoking prevalence .................................................................................... 30 4.2 Practices of smoking ................................................................................... 37 4.3 Attitudes about smoking ............................................................................. 43 4.4 Knowledge of Smoking................................................................................ 45
5. Conclusion........................................................................................47 6. Acknowledgments............................................................................48 Appendix 1 – Additional data ..............................................................49
Smoke Free Pagodas in Cambodia................................................................... 51 ADRA PROGRAMS 2001 – 2004........................................................................ 52 ADRA Media 2001 - 2004.................................................................................... 54
Appendix 3 – Results of Pagoda Survey Questionnaire...................63 Appendix 4 – Survey Questionnaires.................................................64 Appendix 5 - References .....................................................................71
SFCC 2004 Survey Summary. March 21, 2005 4
1. Introduction Diseases related to Tobacco represent one of the leading causes of fatal disease in the world1. Recent public health attention has focused on AIDS/HIV, which currently kills about 1 million people a year. Diseases related to tobacco addiction are now taking four times as many lives per year as HIV/AIDS2. Worldwide, this represents approximately 4 million people (1 in 10 adults) who die prematurely per year as a result of smoking. If this trend continues, 10 million (one person in six) per year will die by 20303. This epidemic started as chronic disease in rich countries; it is now rapidly shifting to the developing world and by 2020, seven of every 10 people killed by smoking will be from a low or middle-income nation4.
Worldwide, about one in three adults (1.3 billion people) smoke. By 2025, the
number is expected to rise to more than 1.6 billion. In the high-income countries, smoking has been in overall decline for decades, although it continues to rise in some groups. In low and middle-income countries, cigarette consumption has been increasing, and already accounts for 80% of all smokers5. In the near future, Tobacco will have the same role in damaging health and causing premature death as it has in industrialized countries6.
There are few policies to control tobacco in Cambodia and no limitations on
the movement and sales of tobacco products. The ministry of health has been attempting to ban tobacco advertising since 1993 with no success7.
Tobacco in Cambodia has many purposes and it has penetrated deep in the
contemporary culture. Cigarettes are given as gifts to Buddhist monks as daily offerings and at traditional ceremonies. Brides and grooms give their wedding guests cigarettes after meals at their reception. Cigarettes may also be used to bribe authority, and may sometimes be used in substitution for money. Cigarette smoke is believed to keep mosquitoes and other insects away. Chewing tobacco is also common among elderly men who chew it raw, and elderly women who mix it with their betel nut8.
As a Buddhist nation, Cambodia has a strong tradition for respect of Buddhist
monks. Buddhist monks have a great deal of influence in Cambodian society and are often looked to as role models, particularly in areas of behavior and belief. Tobacco use is not mentioned specifically in the ancient Buddhist script, but the Buddhist philosophy clearly discourages the use of harmful substances and addiction of any kind.
Data from the baseline 2001 survey9 show that over 35% of Buddhist Monks
smoke. Cambodian Monks have not known until recently about the harms of tobacco use. In the last two years monks around the country have begun to show interest for going "smoke free" and acting as role models.
This survey is the second in a series to measure the prevalence of cigarette
smoking in the Buddhist monk community. It also and assesses the monks' attitudes and practices regarding tobacco. In addition, this survey also addresses the community's prevalence and their beliefs and attitudes about monk's smoking. This midterm survey is part of a larger midterm evaluation for the ADRA Cambodia

SFCC 2004 Survey Summary. March 21, 2005 5
“Smoke Free Cambodian Communities” (SFCC) project. It uses data from the earlier “Smoke Free Buddhist Monk” (SFBM) project and assess differences from 2001 to 2004.
Picture 1. Survey conducted in rural village
1.1 Background / justification In the early part of 2000, ADRA Cambodia, the Ministry of Health counterparts, and funding organizations realized that they needed to have a valid survey to measure the tobacco epidemic in Buddhist monk populations. The SFBM project initiated this effort with a baseline survey in the summer of 2001. The baseline survey measured prevalence, practices, beliefs, and knowledge of cigarette smoking among the monk populations and lay population in five distinct provinces. The current 2004 survey takes the information gathered from the baseline and synthesizes it into a summary report of the status of smoking over the last 4 years.
SFCC 2004 Survey Summary. March 21, 2005 6
1.2 Goal of survey: To quantitatively assess prevalence, practices, beliefs, and knowledge of Buddhist monks and community members about tobacco use and compare them to the baseline 2001 survey. The survey measures the following objectives:
• The prevalence of smoking in Buddhist monks • The beliefs and practices of Buddhist monks concerning tobacco. • The community's beliefs about monks and smoking • The prevalence of smoking in communities • The community's relationship to pagodas for role models and advice with
health
This report summarizes data from the 2001 and 2004 survey questionnaires conducted by ADRA Cambodia’s “Tobacco or Health” team. The principle function of this report is to summarize all important data contained on the Buddhist Monk, and community survey questionnaires. The results section will go through all variables measured and some of the most obvious cross-tab analysis. Use of advanced statistics is restricted to simple measures of significance with t-tests and one regression analysis. Much more advanced statistical analysis is possible beyond what this survey summarizes. These advanced statistics may be pursued in other reports related to this summary. The reader is encouraged to contact the authors of this report if any additional statistical analysis is desired or suggested. Picture 2. A monk smoking at a Cambodian Pagoda
SFCC 2004 Survey Summary. March 21, 2005 7
1.3 Dates of the survey: The survey was conducted from June 15, 2004 to August 1, 2004. It began with four days of training and field tests. 2. Methods 2.1 Survey Questionnaire The purpose of using a survey questionnaire for this evaluation is to generate a set of data to analyze in reference to the 2001 survey. The 2004 dataset is be used to assess changes over time and a new prevalence of tobacco use in rural areas. The sampling frame, survey questionnaire, and sample size are comparable to the 2001 study. All community and pagoda selection methods are the same and are listed in appendix 2. The survey questionnaires are in Appendix 4.
In the community portion of the survey, the household unit is again the primary population sampled. The survey is conducted with men only. If possible the surveyor interviewed the married man of the house who is the household head. If he is not home, the surveyor interviewed any single male available older than 18. If he is not available, another male household authority member was selected. The male respondent will answer the entire survey questionnaire with one question about his wife’s smoking status. The 2004 survey differs from the 2001 in that it asks the man to report his wife’s smoking status. In 2001, both women and men were interviewed.
In the Buddhist monk portion of the survey, the pagoda will be again the primary population unit sampled. The Buddhist monk survey uses the exact methods as used in 2001. Please see appendix one for a description of these methods.
Additional questions are added to the 2004 survey to address the IEC efforts over the past three years. Respondents are asked about their familiarity with the posters, radio spots, and TV spots. Smokers who quit are asked if the IEC efforts had any effect on their decision. 2.2 Sample size When the sample size was calculated, it was decided that the study should attempt to be 80% certain (power) of being able to detect a change of as little as a 10% reduction in prevalence and 95% certain that the observed change could not have occurred by chance. The study decided on a sample size based on calculations from the following 2-sided formula from Kalton10 (Figure 1.a). In addition, the program EPI-INFO 3.2 statcalc11 was used for verification. After the calculations were made, the project used available funds to expand the sample size as much as possible. Table 1 shows the actual sample size by province for the community survey and the monk survey.

SFCC 2004 Survey Summary. March 21, 2005 8
Table 1. Actual Sample size for the 2004 SFCC survey questionnaire. ADRA Cambodia. Province Actual 2004 Actual 2001 Monks Men
Surveys Women
Surveys* Monks Men Women
Phnom Penh 348 441 404 295 138 174 Pousat 399 600 574 283 90 216 Kampot 403 601 579 290 130 192 Svay Rieng 383 602 572 283 174 124 Siem Reap 403 528 492 282 174 132 Total 1936 2622 2,621 1433 706 838 Un-weighted Smoking Prevalence
23% 43.32% 3.96% 35.7% 56.7% 7.2%
*Total amount of completed surveys by men indicating their wife’s smoking status.
For women, the prevalence of smoking in the ADRA 2001 SFBM survey was 7.2%. Because this is such a small prevalence number to detect any change in, the 2004 survey did not actively sample women respondents. Instead, the 2004 ADRA Cambodia survey incorporated the women’s smoking status question into the survey questionnaire for men. Men were asked about their wife’s smoking status. By doing this, both women and men’s smoking status were assessed from each household questionnaire.
Buddhist monks are again sampled in an identical way they were for the 2001 survey (appendix 2). A minimum of twenty pagodas were selected for each province. To accurately assess a change in prevalence as small as 10% the survey needs a population of 307 in the control population province and 307 in the intervention populations. Because many monks are chosen in the same pagoda, a design effect of 2 is chosen to account for clustering at the pagoda level.
[ ]2
12
2
11222/1
)()1()1()1(2
ppppppZppz
deftn−
−+−+−= − βα
Where, n = minimum sample size required per group or round deft= design effect anticipated (considers clustering if sampling 2 members per household)
2/1 α−z = the probability with which it is desired to be able to conclude that an observed change of magnitude (p2-p1) in either direction would not have occurred by chance (i.e. significance).
ZB = the probability with which it is desired to be certain of being able to detect a change of magnitude (p2-p1) if one had occurred (power).
p = (p1+p2)/2 = p1= expected population proportion at time 1 p2= expected population proportion at some future date such that the quantity (p2-p1) is the size of
the increase or decrease (of the subgroup difference) that it is desired and the survey effort able to detect (assumes equal variance across time or between subgroups).
Figure 1a. Two sided sample size formula used before the SFCC 2004 survey questionnaire was conducted.
SFCC 2004 Survey Summary. March 21, 2005 9
2.3 Power The calculated power of this study tells us the probability of detecting a difference between the 2001 and 2004 prevalence calculations. In other words, it tells us how well the study is at correctly identifying a difference between the two prevalence rates if they are actually different.
Because this study is stratified by province, monk status, and gender, we will calculate power of all of these stratifications between the 2001 and 2004 years. Table 2 shows a summary of the power calculations for these stratifications. To calculate the power, the formula in Figure 1.b was used.
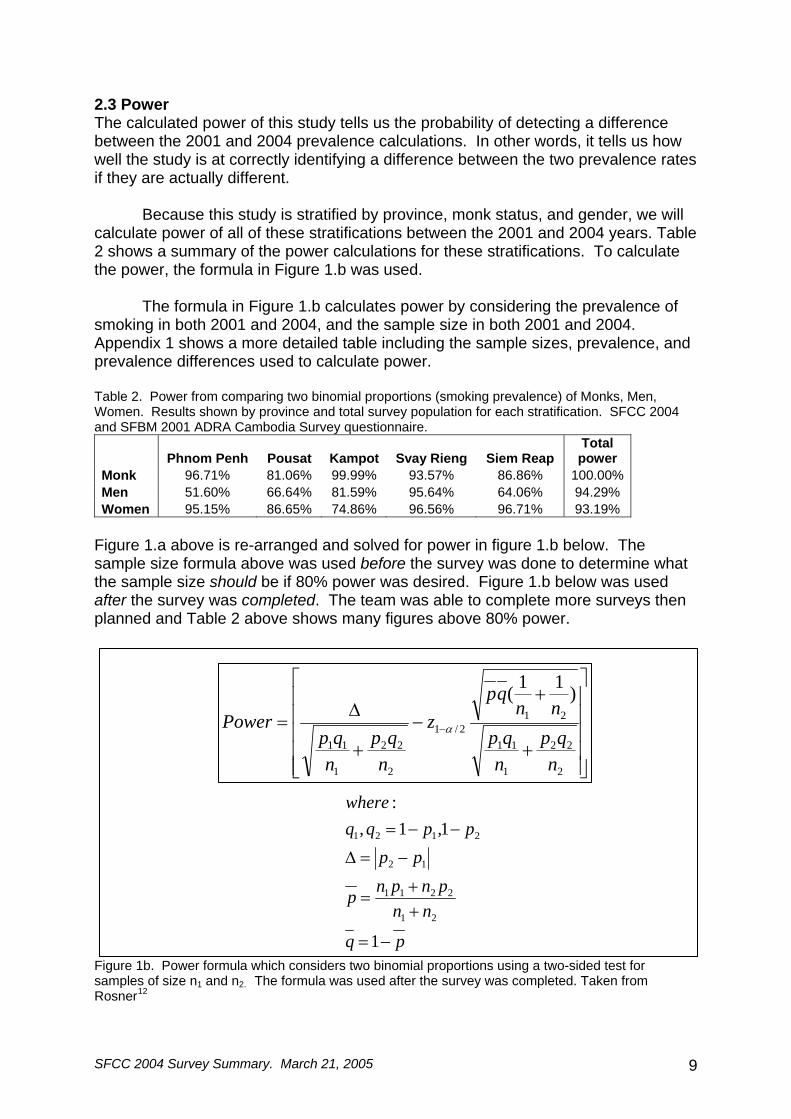
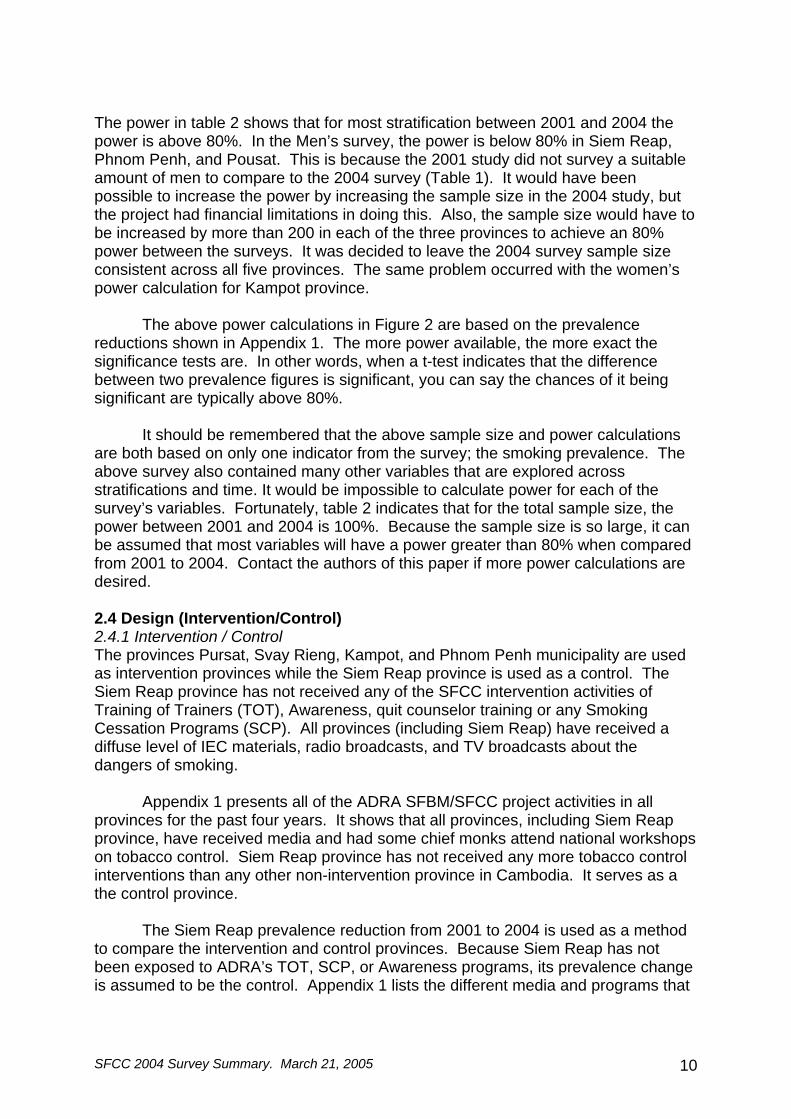
The formula in Figure 1.b calculates power by considering the prevalence of smoking in both 2001 and 2004, and the sample size in both 2001 and 2004. Appendix 1 shows a more detailed table including the sample sizes, prevalence, and prevalence differences used to calculate power. Table 2. Power from comparing two binomial proportions (smoking prevalence) of Monks, Men, Women. Results shown by province and total survey population for each stratification. SFCC 2004 and SFBM 2001 ADRA Cambodia Survey questionnaire.
Phnom Penh Pousat Kampot Svay Rieng Siem Reap Total power
Monk 96.71% 81.06% 99.99% 93.57% 86.86% 100.00% Men 51.60% 66.64% 81.59% 95.64% 64.06% 94.29% Women 95.15% 86.65% 74.86% 96.56% 96.71% 93.19%
Figure 1.a above is re-arranged and solved for power in figure 1.b below. The sample size formula above was used before the survey was done to determine what the sample size should be if 80% power was desired. Figure 1.b below was used after the survey was completed. The team was able to complete more surveys then planned and Table 2 above shows many figures above 80% power. Figure 1b. Power formula which considers two binomial proportions using a two-sided test for samples of size n1 and n2. The formula was used after the survey was completed. Taken from Rosner12
⎥⎥⎥⎥⎥
⎦
⎤
⎢⎢⎢⎢⎢
⎣
⎡
+
+−
+
Δ= −
2
22
1
11
212/1
2
22
1
11
)11(
nqp
nqp
nnqp
z
nqp
nqp
Power α
pq
nnpnpnp
ppppqq
where
−=
++
=
−=Δ
−−=
1
1,1,:
21
2211
12
2121
SFCC 2004 Survey Summary. March 21, 2005 10
The power in table 2 shows that for most stratification between 2001 and 2004 the power is above 80%. In the Men’s survey, the power is below 80% in Siem Reap, Phnom Penh, and Pousat. This is because the 2001 study did not survey a suitable amount of men to compare to the 2004 survey (Table 1). It would have been possible to increase the power by increasing the sample size in the 2004 study, but the project had financial limitations in doing this. Also, the sample size would have to be increased by more than 200 in each of the three provinces to achieve an 80% power between the surveys. It was decided to leave the 2004 survey sample size consistent across all five provinces. The same problem occurred with the women’s power calculation for Kampot province.
The above power calculations in Figure 2 are based on the prevalence reductions shown in Appendix 1. The more power available, the more exact the significance tests are. In other words, when a t-test indicates that the difference between two prevalence figures is significant, you can say the chances of it being significant are typically above 80%.
It should be remembered that the above sample size and power calculations are both based on only one indicator from the survey; the smoking prevalence. The above survey also contained many other variables that are explored across stratifications and time. It would be impossible to calculate power for each of the survey’s variables. Fortunately, table 2 indicates that for the total sample size, the power between 2001 and 2004 is 100%. Because the sample size is so large, it can be assumed that most variables will have a power greater than 80% when compared from 2001 to 2004. Contact the authors of this paper if more power calculations are desired. 2.4 Design (Intervention/Control) 2.4.1 Intervention / Control The provinces Pursat, Svay Rieng, Kampot, and Phnom Penh municipality are used as intervention provinces while the Siem Reap province is used as a control. The Siem Reap province has not received any of the SFCC intervention activities of Training of Trainers (TOT), Awareness, quit counselor training or any Smoking Cessation Programs (SCP). All provinces (including Siem Reap) have received a diffuse level of IEC materials, radio broadcasts, and TV broadcasts about the dangers of smoking.
Appendix 1 presents all of the ADRA SFBM/SFCC project activities in all provinces for the past four years. It shows that all provinces, including Siem Reap province, have received media and had some chief monks attend national workshops on tobacco control. Siem Reap province has not received any more tobacco control interventions than any other non-intervention province in Cambodia. It serves as a the control province.
The Siem Reap prevalence reduction from 2001 to 2004 is used as a method to compare the intervention and control provinces. Because Siem Reap has not been exposed to ADRA’s TOT, SCP, or Awareness programs, its prevalence change is assumed to be the control. Appendix 1 lists the different media and programs that

SFCC 2004 Survey Summary. March 21, 2005 11
have occurred in all provinces. Table D in Appendix 1 shows that although Siem Reap has not received any direct ADRA programs, it has received many types of diffuse media.
The Siem Reap prevalence change from 2001 to 2004 may not be directly
comparable to other provinces. Data from this survey and the 2004 NIS tobacco survey show that Siem Reap province normally has a higher prevalence than the other provinces. This could be due to Siem Reap being the most popular tourist destination in Cambodia or a variety of other reasons. Whatever the reason for the higher prevalence, the Siem Reap prevalence appears to behave differently than the other provinces. Aside from the above considerations, the Siem Reap province was designated as the control province for this project in early 2001; this research will use it as such. 2.4.2 Survey Representation
This survey stratifies the survey data by province and age. Age stratification by five year age groups will be possible at the multi-province-level. This age stratification will represent the prevalence only among the five selected provinces.
The survey does not represent the entire country; the 2004 NIS prevalence
study should be used for national prevalence figures. When referring to data from this survey, the term “five-province” should be used. When this study/ intervention was initially designed in 2001, the team of government, NGO, and International partners selected the five provinces as representative sections of the country. Conveniently, it has been found that the prevalence figures in the NIS survey and this study are very close. For the Buddhist monk survey, no other national effort exists to monitor prevalence among the 55,000 monks in the country. Because no other study exists, the population of monks is relatively small, and because the provinces are chosen to represent the country’s population dynamics, the data from this study’s “five-province” Buddhist monk survey can be used to approximate national data. 2.4.3 Weighting Only the five-province prevalence figures were weighted by province population. No other weighting occurred in any of the variables. In all tables, only un-weighted prevalence figures were used. 2.4.4 Urban / Rural The Urban / Rural designation used in the 2001 and 2004 surveys use the 1998 Cambodian census to select samples for the community survey. It specifies each village as urban or rural. Typically, every province surveyed has at least two or three villages in the provincial center which are designated as urban, while all others are rural. For the municipality of Phnom Penh, there are also villages that are designated as rural because of their distance from the city center. The unpublished results of the recently updated 2004 Cambodian Census now list all villages in Phnom Penh municipality as urban. This project only uses the 1998 definition.
Buddhist pagodas were selected using data from the Ministry of Cults and Religion which did not contain an urban/rural delineation. The villages that the
SFCC 2004 Survey Summary. March 21, 2005 12
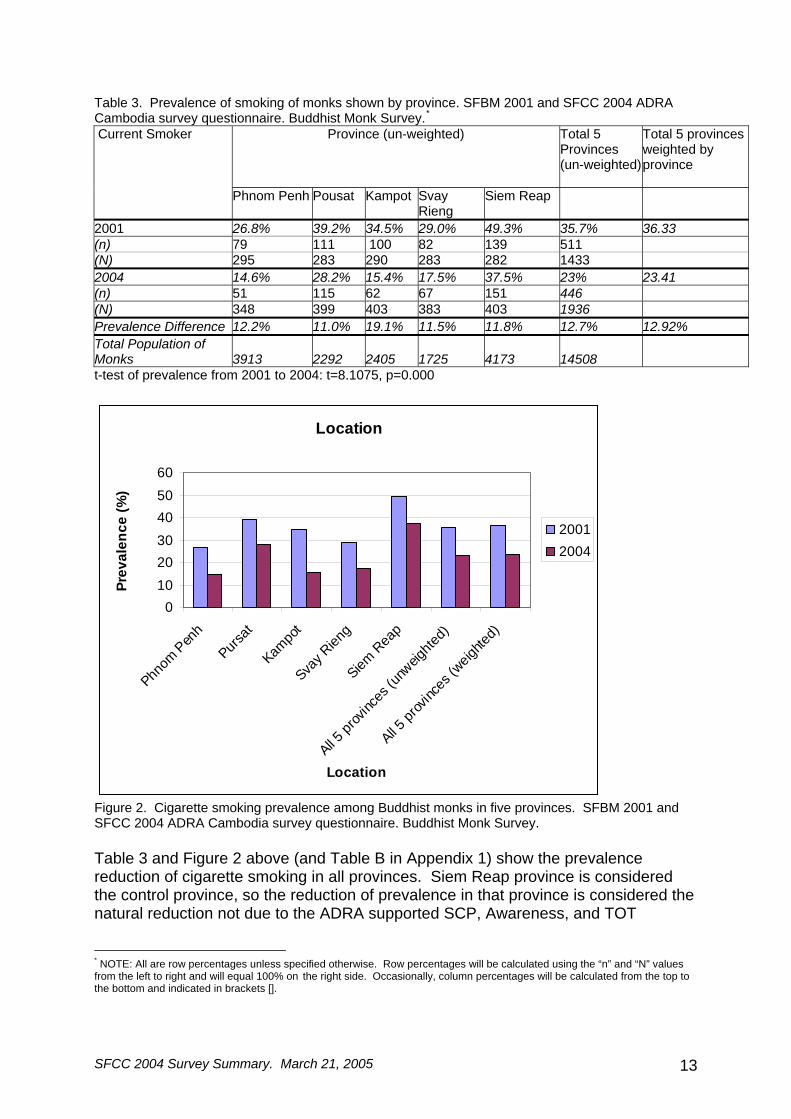
pagodas are in were used in reference to the Cambodian Census data to determine if the pagoda is urban or rural. 3. Results – Buddhist Monk Survey 3.1 Smoking Prevalence Table 3 shows that out of all the 1960 surveys completed, 1936 had a response for smoking status of the monk. The un-weighted decrease in smoking prevalence among all monks was significant; the drop from the 2001 survey to the 2004 survey was 12.7%. The province with the largest reduction in smoking prevalence among monks was Kampot province (19.1%), while the smallest drop (11.0%) was Pousat province. The weighted prevalence of 2001 and 2004 was not different than the un-weighted prevalence. The un-weighted prevalence is used for analysis throughout the remainder of this document.
SFCC 2004 Survey Summary. March 21, 2005 13
Table 3. Prevalence of smoking of monks shown by province. SFBM 2001 and SFCC 2004 ADRA Cambodia survey questionnaire. Buddhist Monk Survey.*
Province (un-weighted) Total 5 Provinces (un-weighted)
Total 5 provinces weighted by province
Current Smoker
Phnom Penh Pousat Kampot Svay Rieng
Siem Reap
2001 26.8% 39.2% 34.5% 29.0% 49.3% 35.7% 36.33 (n) 79 111 100 82 139 511 (N) 295 283 290 283 282 1433 2004 14.6% 28.2% 15.4% 17.5% 37.5% 23% 23.41 (n) 51 115 62 67 151 446 (N) 348 399 403 383 403 1936 Prevalence Difference 12.2% 11.0% 19.1% 11.5% 11.8% 12.7% 12.92% Total Population of Monks 3913 2292 2405 1725 4173 14508 t-test of prevalence from 2001 to 2004: t=8.1075, p=0.000
Location
0102030405060
Phnom
Pen
h
Pursat
Kampo
t
Svay R
ieng
Siem R
eap
All 5 pr
ovinc
es (u
nweig
hted)
All 5 pr
ovinc
es (w
eighte
d)
Location
Prev
alen
ce (%
)
20012004
Figure 2. Cigarette smoking prevalence among Buddhist monks in five provinces. SFBM 2001 and SFCC 2004 ADRA Cambodia survey questionnaire. Buddhist Monk Survey. Table 3 and Figure 2 above (and Table B in Appendix 1) show the prevalence reduction of cigarette smoking in all provinces. Siem Reap province is considered the control province, so the reduction of prevalence in that province is considered the natural reduction not due to the ADRA supported SCP, Awareness, and TOT
* NOTE: All are row percentages unless specified otherwise. Row percentages will be calculated using the “n” and “N” values from the left to right and will equal 100% on the right side. Occasionally, column percentages will be calculated from the top to the bottom and indicated in brackets [].

SFCC 2004 Survey Summary. March 21, 2005 14
programs. The reduction is of smoking prevalence from 2001 to 2004 among Buddhist monks in Siem Reap province is 11.8%. That reduction is surpassed by all other intervention provinces except Svay Rieng and Pousat where the reduction in prevalence is only 11.5% and 11.0%, respectively. Kampot province has the highest prevalence reduction at 19.1%. Table D in Appendix 1 show that Kampot province has had many of the ADRA programs of SCP, TOT, and Awareness from the beginning of the Smoke Free Buddhist Monk program in 2001. Table 3a. Prevalence of current smokers shown by how often they smoke. SFBM 2001 Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. How often? Percentage of current smokers Percentage of entire survey (n) % of smokers (N) % of entire survey (N) Every day 406 80.6 504 28.33 1433 Few/week 82 16.3 504 5.72 1433 Few/month 16 3.2 504 1.12 1433 504 100 Table 3b. Prevalence of current smokers shown by how often they smoke. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. How often? Percentage of current smokers Percentage of entire survey (n) % of smokers (N) % of entire survey (N) Every day 370 89.16 415 19.11 1936 Few/week 36 8.67 415 1.86 1936 Few/month 9 2.17 415 0.46 1936 Total 415 100 Table 3 shows that the percentage of daily smokers increases from 2001 to 2004 when the percentage is calculated among smokers. The percentage drops from 2001 to 2004 when it is calculated among the entire survey population. This could be an indication that although the prevalence of smoking is dropping, more smokers are now considered heavy smokers. Table 4. Prevalence of smoking of monks shown by rural / urban classification. SFBM 2001 Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Urban/Rural Percentage of current smokers (n) % of smokers (N) Urban 120 29.9 402 Rural 391 37.92 1031 Both Rural and Urban 511 35.7 1433 Table 4b. Prevalence of smoking monks shown by rural/urban classification. SFCC 2004 Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Urban/Rural Percentage of current smokers (n) % of smokers (N) Urban 83 18.57 447 Rural 361 24.31 1485 Both Rural and Urban 444 22.98 1932 A t-test was conducted on the smoking prevalence differences between urban and rural. The results showed no significant difference for both 2001 and 2004 (2001: t=-2.87, p=0.99; 2004: t=-2.53, p=0.99). The prevalence of rural and urban smokers does not appear to vary among the monk population.
SFCC 2004 Survey Summary. March 21, 2005 15
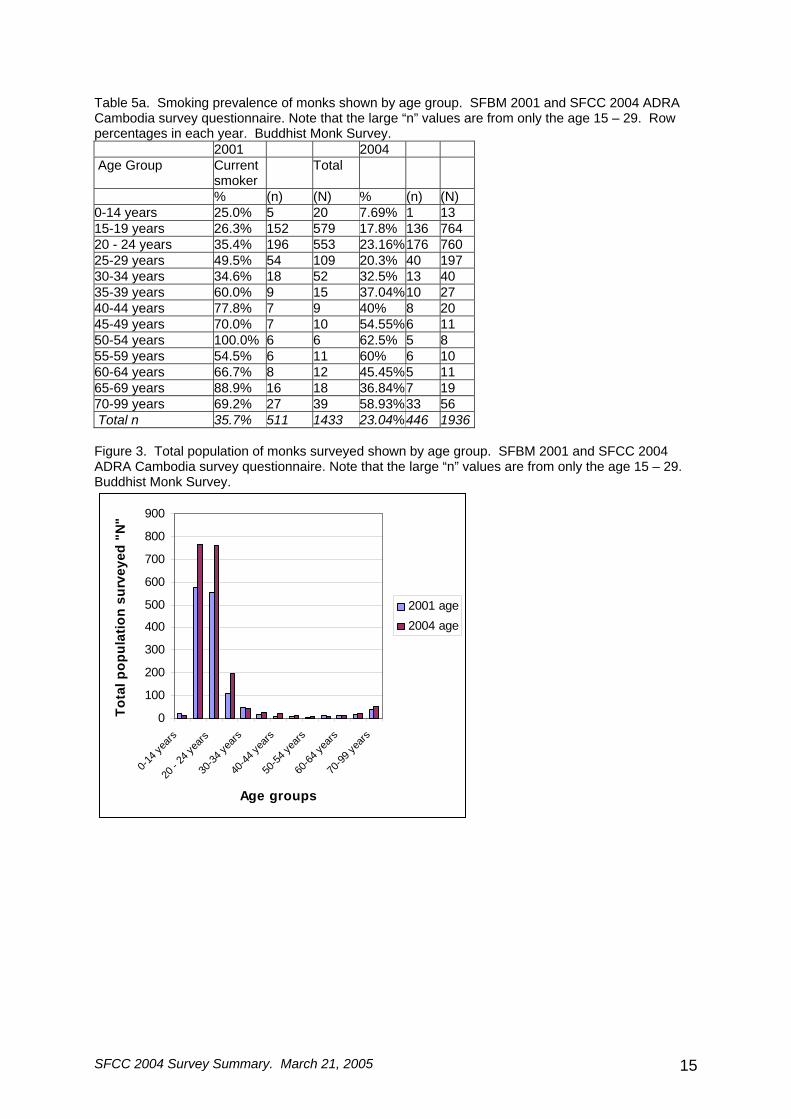
Table 5a. Smoking prevalence of monks shown by age group. SFBM 2001 and SFCC 2004 ADRA Cambodia survey questionnaire. Note that the large “n” values are from only the age 15 – 29. Row percentages in each year. Buddhist Monk Survey. 2001 2004 Age Group Current
smoker Total
% (n) (N) % (n) (N) 0-14 years 25.0% 5 20 7.69% 1 13 15-19 years 26.3% 152 579 17.8% 136 764 20 - 24 years 35.4% 196 553 23.16%176 760 25-29 years 49.5% 54 109 20.3% 40 197 30-34 years 34.6% 18 52 32.5% 13 40 35-39 years 60.0% 9 15 37.04%10 27 40-44 years 77.8% 7 9 40% 8 20 45-49 years 70.0% 7 10 54.55%6 11 50-54 years 100.0% 6 6 62.5% 5 8 55-59 years 54.5% 6 11 60% 6 10 60-64 years 66.7% 8 12 45.45%5 11 65-69 years 88.9% 16 18 36.84%7 19 70-99 years 69.2% 27 39 58.93%33 56 Total n 35.7% 511 1433 23.04%446 1936 Figure 3. Total population of monks surveyed shown by age group. SFBM 2001 and SFCC 2004 ADRA Cambodia survey questionnaire. Note that the large “n” values are from only the age 15 – 29. Buddhist Monk Survey.
0
100
200
300
400
500
600
700
800
900
0-14 y
ears
20 - 2
4 yea
rs
30-34
years
40-44
years
50-54
years
60-64
years
70-99
years
Age groups
Tota
l pop
ulat
ion
surv
eyed
"N
"
2001 age2004 age
SFCC 2004 Survey Summary. March 21, 2005 16
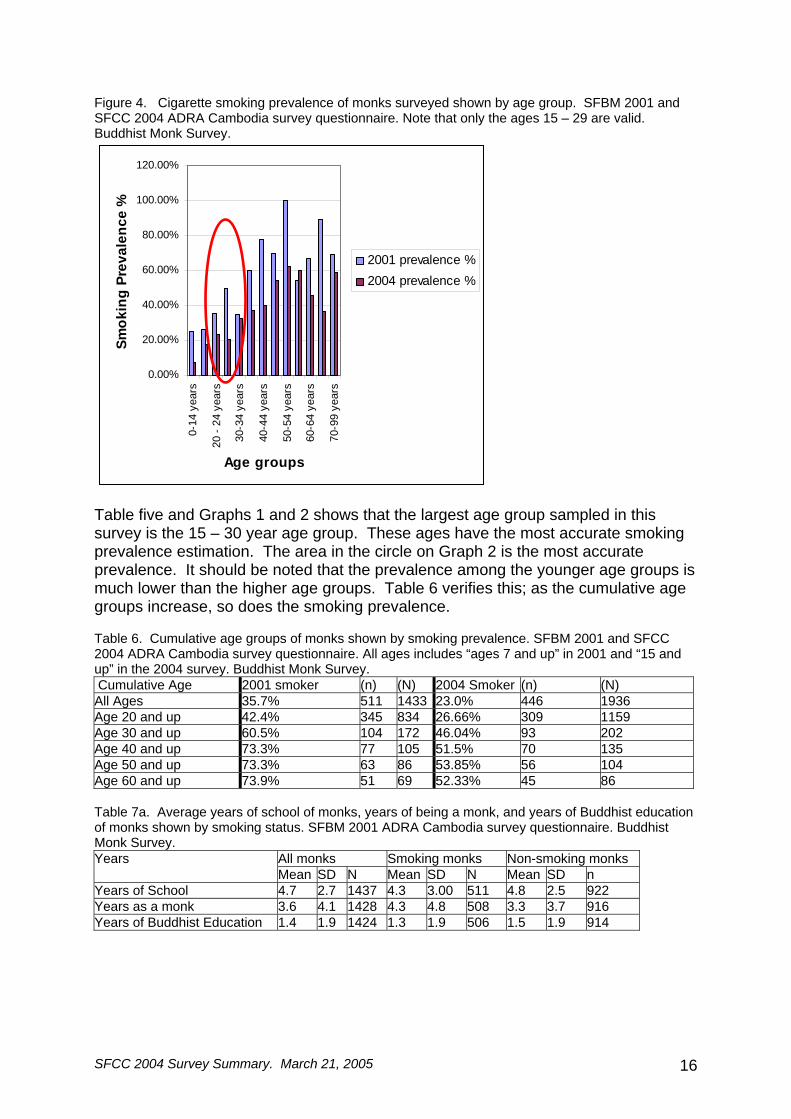
Figure 4. Cigarette smoking prevalence of monks surveyed shown by age group. SFBM 2001 and SFCC 2004 ADRA Cambodia survey questionnaire. Note that only the ages 15 – 29 are valid. Buddhist Monk Survey.
0.00%
20.00%
40.00%
60.00%
80.00%
100.00%
120.00%
0-14
yea
rs
20 -
24 y
ears
30-3
4 ye
ars
40-4
4 ye
ars
50-5
4 ye
ars
60-6
4 ye
ars
70-9
9 ye
ars
Age groups
Smok
ing
Prev
alen
ce %
2001 prevalence %2004 prevalence %
Table five and Graphs 1 and 2 shows that the largest age group sampled in this survey is the 15 – 30 year age group. These ages have the most accurate smoking prevalence estimation. The area in the circle on Graph 2 is the most accurate prevalence. It should be noted that the prevalence among the younger age groups is much lower than the higher age groups. Table 6 verifies this; as the cumulative age groups increase, so does the smoking prevalence. Table 6. Cumulative age groups of monks shown by smoking prevalence. SFBM 2001 and SFCC 2004 ADRA Cambodia survey questionnaire. All ages includes “ages 7 and up” in 2001 and “15 and up” in the 2004 survey. Buddhist Monk Survey. Cumulative Age 2001 smoker (n) (N) 2004 Smoker (n) (N) All Ages 35.7% 511 1433 23.0% 446 1936 Age 20 and up 42.4% 345 834 26.66% 309 1159 Age 30 and up 60.5% 104 172 46.04% 93 202 Age 40 and up 73.3% 77 105 51.5% 70 135 Age 50 and up 73.3% 63 86 53.85% 56 104 Age 60 and up 73.9% 51 69 52.33% 45 86 Table 7a. Average years of school of monks, years of being a monk, and years of Buddhist education of monks shown by smoking status. SFBM 2001 ADRA Cambodia survey questionnaire. Buddhist Monk Survey.
All monks Smoking monks Non-smoking monks Years Mean SD N Mean SD N Mean SD n Years of School 4.7 2.7 1437 4.3 3.00 511 4.8 2.5 922 Years as a monk 3.6 4.1 1428 4.3 4.8 508 3.3 3.7 916 Years of Buddhist Education 1.4 1.9 1424 1.3 1.9 506 1.5 1.9 914
SFCC 2004 Survey Summary. March 21, 2005 17
Table 7b. Average years of school of monks, years of being a monk, and years of Buddhist education of monks shown by smoking status. SFCC 2004 ADRA Cambodia survey questionnaire. Buddhist Monk Survey.
All monks Smoking monks Non-smoking monks Years Mean SD N Mean SD N Mean SD n Years of School 5.12 2.78 1935 4.36 2.98 446 5.35 2.67 1489 Years as a monk 3.95 4.67 1935 4.08 4.63 445 3.91 4.687 1490 Years of Buddhist Education 1.53 2.07 1933 1.150 1.76 445 1.65 2.15 1488 Table 8. Average number of years of education of monks by province. SFBM 2001 and SFCC 2004 ADRA Cambodia survey questionnaire. Buddhist Monk Survey. 2001 2004 Province Mean N SD Mean N SD Phnom Penh 5.73 297 3.03 6.48 353 2.94 Pousat 4.25 283 2.60 4.62 402 2.50 Kampot 4.80 290 2.10 5.60 402 2.46 Svay Rieng 5.20 283 2.52 5.52 384 2.34 Siem Reap 3.33 284 2.54 3.59 406 2.78 5 province average
4.67 1437 2.70 5.12 1947 2.78
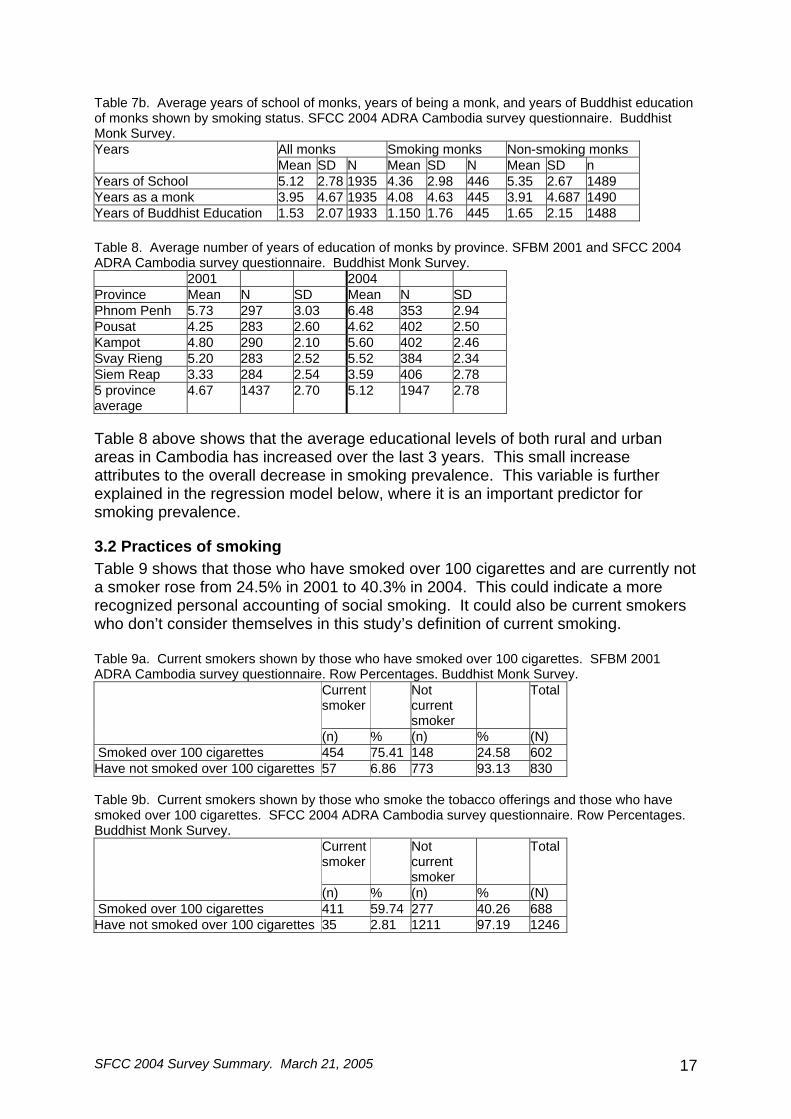
Table 8 above shows that the average educational levels of both rural and urban areas in Cambodia has increased over the last 3 years. This small increase attributes to the overall decrease in smoking prevalence. This variable is further explained in the regression model below, where it is an important predictor for smoking prevalence.
3.2 Practices of smoking Table 9 shows that those who have smoked over 100 cigarettes and are currently not a smoker rose from 24.5% in 2001 to 40.3% in 2004. This could indicate a more recognized personal accounting of social smoking. It could also be current smokers who don’t consider themselves in this study’s definition of current smoking. Table 9a. Current smokers shown by those who have smoked over 100 cigarettes. SFBM 2001 ADRA Cambodia survey questionnaire. Row Percentages. Buddhist Monk Survey.
Current smoker
Not current smoker
Total
(n) % (n) % (N) Smoked over 100 cigarettes 454 75.41 148 24.58 602 Have not smoked over 100 cigarettes 57 6.86 773 93.13 830 Table 9b. Current smokers shown by those who smoke the tobacco offerings and those who have smoked over 100 cigarettes. SFCC 2004 ADRA Cambodia survey questionnaire. Row Percentages. Buddhist Monk Survey.
Current smoker
Not current smoker
Total
(n) % (n) % (N) Smoked over 100 cigarettes 411 59.74 277 40.26 688 Have not smoked over 100 cigarettes 35 2.81 1211 97.19 1246
SFCC 2004 Survey Summary. March 21, 2005 18
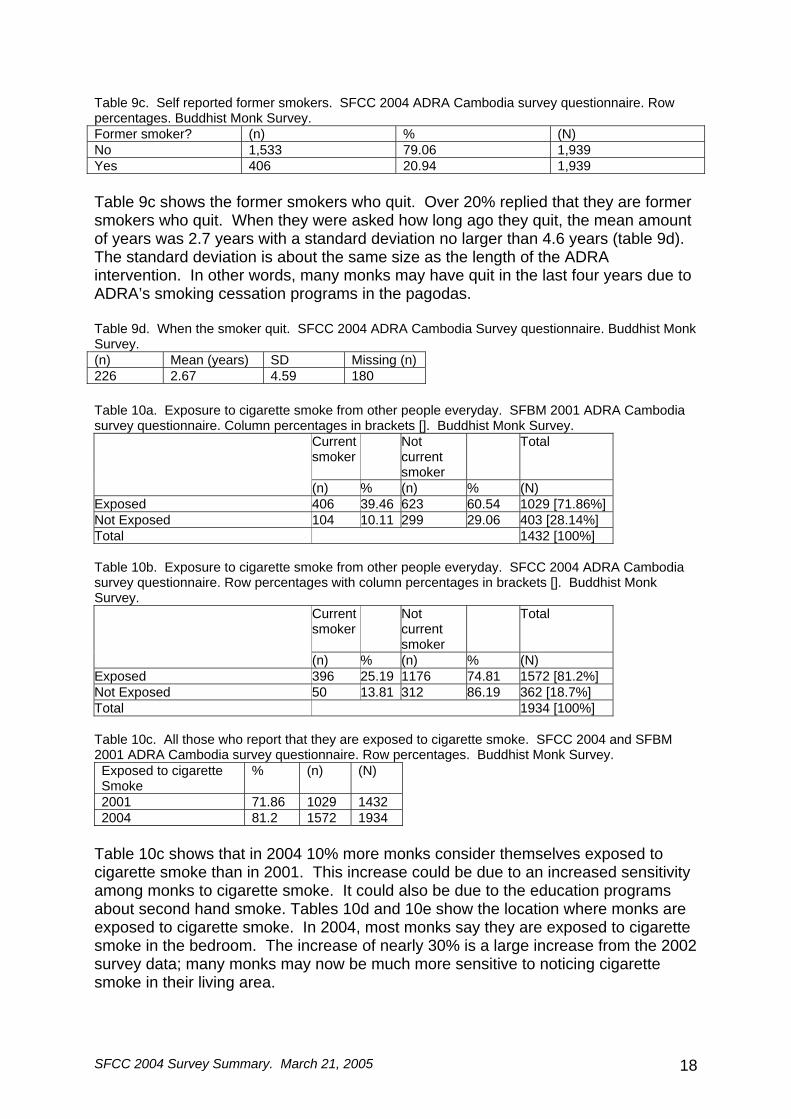
Table 9c. Self reported former smokers. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Former smoker? (n) % (N) No 1,533 79.06 1,939 Yes 406 20.94 1,939 Table 9c shows the former smokers who quit. Over 20% replied that they are former smokers who quit. When they were asked how long ago they quit, the mean amount of years was 2.7 years with a standard deviation no larger than 4.6 years (table 9d). The standard deviation is about the same size as the length of the ADRA intervention. In other words, many monks may have quit in the last four years due to ADRA’s smoking cessation programs in the pagodas. Table 9d. When the smoker quit. SFCC 2004 ADRA Cambodia Survey questionnaire. Buddhist Monk Survey. (n) Mean (years) SD Missing (n) 226 2.67 4.59 180 Table 10a. Exposure to cigarette smoke from other people everyday. SFBM 2001 ADRA Cambodia survey questionnaire. Column percentages in brackets []. Buddhist Monk Survey.
Current smoker
Not current smoker
Total
(n) % (n) % (N) Exposed 406 39.46 623 60.54 1029 [71.86%] Not Exposed 104 10.11 299 29.06 403 [28.14%] Total 1432 [100%] Table 10b. Exposure to cigarette smoke from other people everyday. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages with column percentages in brackets []. Buddhist Monk Survey.
Current smoker
Not current smoker
Total
(n) % (n) % (N) Exposed 396 25.19 1176 74.81 1572 [81.2%] Not Exposed 50 13.81 312 86.19 362 [18.7%] Total 1934 [100%] Table 10c. All those who report that they are exposed to cigarette smoke. SFCC 2004 and SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Exposed to cigarette Smoke
% (n) (N)
2001 71.86 1029 1432 2004 81.2 1572 1934
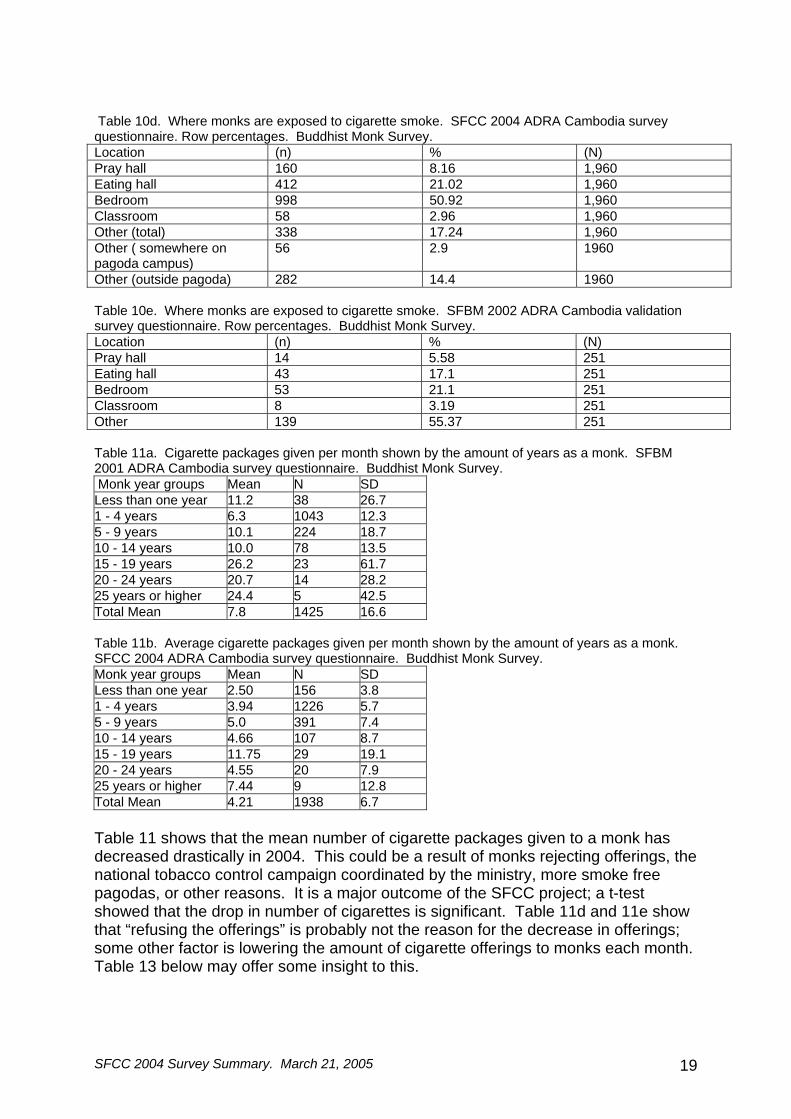
Table 10c shows that in 2004 10% more monks consider themselves exposed to cigarette smoke than in 2001. This increase could be due to an increased sensitivity among monks to cigarette smoke. It could also be due to the education programs about second hand smoke. Tables 10d and 10e show the location where monks are exposed to cigarette smoke. In 2004, most monks say they are exposed to cigarette smoke in the bedroom. The increase of nearly 30% is a large increase from the 2002 survey data; many monks may now be much more sensitive to noticing cigarette smoke in their living area.
SFCC 2004 Survey Summary. March 21, 2005 19
Table 10d. Where monks are exposed to cigarette smoke. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Location (n) % (N) Pray hall 160 8.16 1,960 Eating hall 412 21.02 1,960 Bedroom 998 50.92 1,960 Classroom 58 2.96 1,960 Other (total) 338 17.24 1,960 Other ( somewhere on pagoda campus)
56 2.9 1960
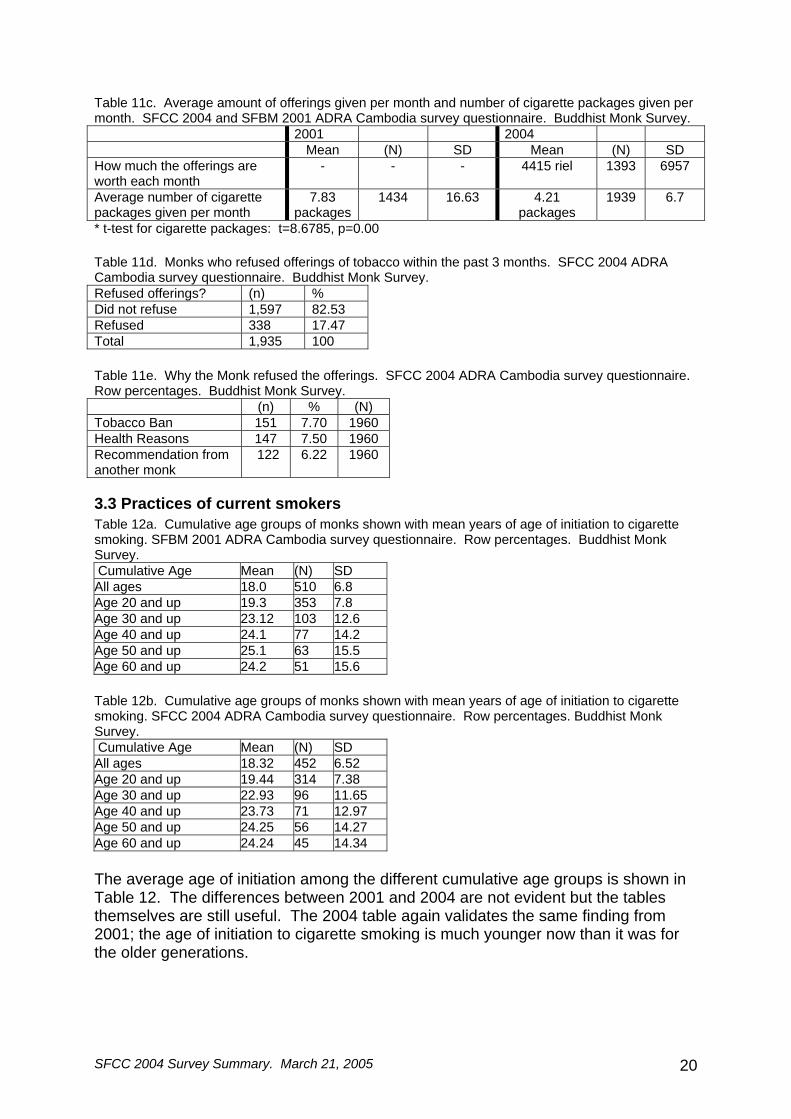
Other (outside pagoda) 282 14.4 1960 Table 10e. Where monks are exposed to cigarette smoke. SFBM 2002 ADRA Cambodia validation survey questionnaire. Row percentages. Buddhist Monk Survey. Location (n) % (N) Pray hall 14 5.58 251 Eating hall 43 17.1 251 Bedroom 53 21.1 251 Classroom 8 3.19 251 Other 139 55.37 251 Table 11a. Cigarette packages given per month shown by the amount of years as a monk. SFBM 2001 ADRA Cambodia survey questionnaire. Buddhist Monk Survey. Monk year groups Mean N SD Less than one year 11.2 38 26.7 1 - 4 years 6.3 1043 12.3 5 - 9 years 10.1 224 18.7 10 - 14 years 10.0 78 13.5 15 - 19 years 26.2 23 61.7 20 - 24 years 20.7 14 28.2 25 years or higher 24.4 5 42.5 Total Mean 7.8 1425 16.6 Table 11b. Average cigarette packages given per month shown by the amount of years as a monk. SFCC 2004 ADRA Cambodia survey questionnaire. Buddhist Monk Survey. Monk year groups Mean N SD Less than one year 2.50 156 3.8 1 - 4 years 3.94 1226 5.7 5 - 9 years 5.0 391 7.4 10 - 14 years 4.66 107 8.7 15 - 19 years 11.75 29 19.1 20 - 24 years 4.55 20 7.9 25 years or higher 7.44 9 12.8 Total Mean 4.21 1938 6.7 Table 11 shows that the mean number of cigarette packages given to a monk has decreased drastically in 2004. This could be a result of monks rejecting offerings, the national tobacco control campaign coordinated by the ministry, more smoke free pagodas, or other reasons. It is a major outcome of the SFCC project; a t-test showed that the drop in number of cigarettes is significant. Table 11d and 11e show that “refusing the offerings” is probably not the reason for the decrease in offerings; some other factor is lowering the amount of cigarette offerings to monks each month. Table 13 below may offer some insight to this.
SFCC 2004 Survey Summary. March 21, 2005 20
Table 11c. Average amount of offerings given per month and number of cigarette packages given per month. SFCC 2004 and SFBM 2001 ADRA Cambodia survey questionnaire. Buddhist Monk Survey. 2001 2004 Mean (N) SD Mean (N) SD How much the offerings are worth each month
- - - 4415 riel 1393 6957
Average number of cigarette packages given per month
7.83 packages
1434 16.63 4.21 packages
1939 6.7
* t-test for cigarette packages: t=8.6785, p=0.00 Table 11d. Monks who refused offerings of tobacco within the past 3 months. SFCC 2004 ADRA Cambodia survey questionnaire. Buddhist Monk Survey. Refused offerings? (n) % Did not refuse 1,597 82.53 Refused 338 17.47 Total 1,935 100 Table 11e. Why the Monk refused the offerings. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. (n) % (N) Tobacco Ban 151 7.70 1960 Health Reasons 147 7.50 1960 Recommendation from another monk
122 6.22 1960
3.3 Practices of current smokers Table 12a. Cumulative age groups of monks shown with mean years of age of initiation to cigarette smoking. SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Cumulative Age Mean (N) SD All ages 18.0 510 6.8 Age 20 and up 19.3 353 7.8 Age 30 and up 23.12 103 12.6 Age 40 and up 24.1 77 14.2 Age 50 and up 25.1 63 15.5 Age 60 and up 24.2 51 15.6 Table 12b. Cumulative age groups of monks shown with mean years of age of initiation to cigarette smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Cumulative Age Mean (N) SD All ages 18.32 452 6.52 Age 20 and up 19.44 314 7.38 Age 30 and up 22.93 96 11.65 Age 40 and up 23.73 71 12.97 Age 50 and up 24.25 56 14.27 Age 60 and up 24.24 45 14.34 The average age of initiation among the different cumulative age groups is shown in Table 12. The differences between 2001 and 2004 are not evident but the tables themselves are still useful. The 2004 table again validates the same finding from 2001; the age of initiation to cigarette smoking is much younger now than it was for the older generations.
SFCC 2004 Survey Summary. March 21, 2005 21
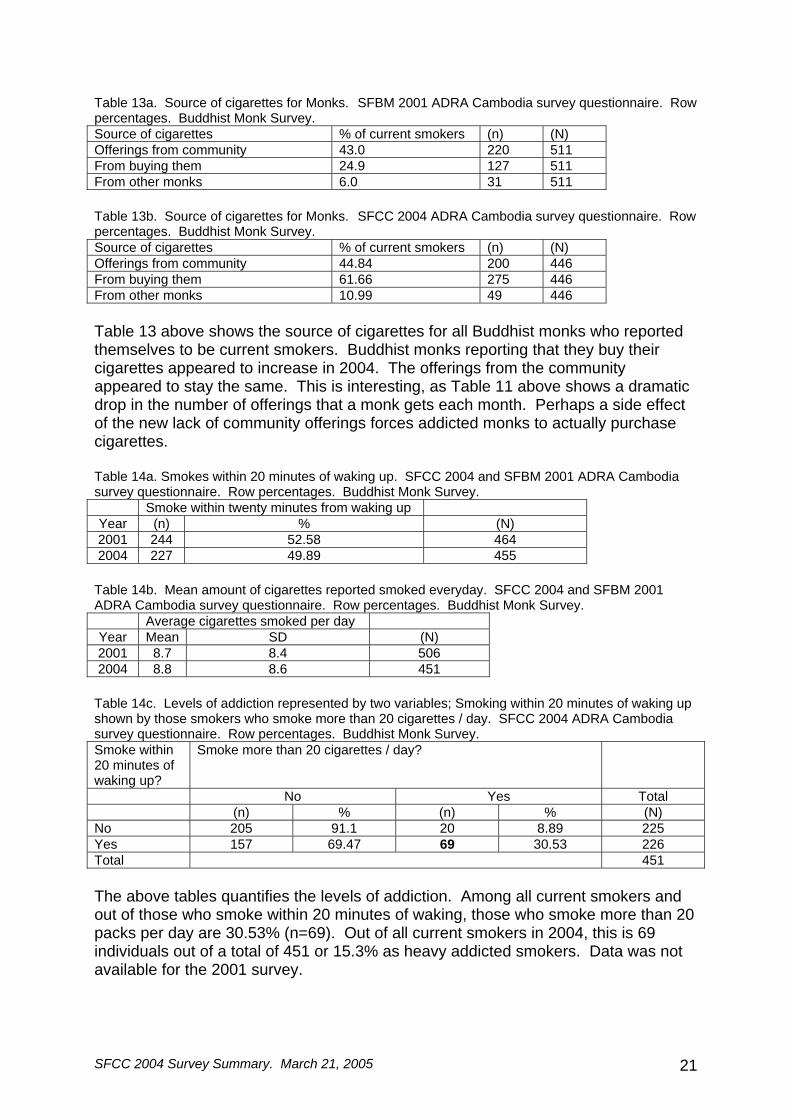
Table 13a. Source of cigarettes for Monks. SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Source of cigarettes % of current smokers (n) (N) Offerings from community 43.0 220 511 From buying them 24.9 127 511 From other monks 6.0 31 511 Table 13b. Source of cigarettes for Monks. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Source of cigarettes % of current smokers (n) (N) Offerings from community 44.84 200 446 From buying them 61.66 275 446 From other monks 10.99 49 446 Table 13 above shows the source of cigarettes for all Buddhist monks who reported themselves to be current smokers. Buddhist monks reporting that they buy their cigarettes appeared to increase in 2004. The offerings from the community appeared to stay the same. This is interesting, as Table 11 above shows a dramatic drop in the number of offerings that a monk gets each month. Perhaps a side effect of the new lack of community offerings forces addicted monks to actually purchase cigarettes. Table 14a. Smokes within 20 minutes of waking up. SFCC 2004 and SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Smoke within twenty minutes from waking up Year (n) % (N) 2001 244 52.58 464 2004 227 49.89 455 Table 14b. Mean amount of cigarettes reported smoked everyday. SFCC 2004 and SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Average cigarettes smoked per day Year Mean SD (N) 2001 8.7 8.4 506 2004 8.8 8.6 451 Table 14c. Levels of addiction represented by two variables; Smoking within 20 minutes of waking up shown by those smokers who smoke more than 20 cigarettes / day. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Smoke within 20 minutes of waking up?
Smoke more than 20 cigarettes / day?
No Yes Total (n) % (n) % (N) No 205 91.1 20 8.89 225 Yes 157 69.47 69 30.53 226 Total 451 The above tables quantifies the levels of addiction. Among all current smokers and out of those who smoke within 20 minutes of waking, those who smoke more than 20 packs per day are 30.53% (n=69). Out of all current smokers in 2004, this is 69 individuals out of a total of 451 or 15.3% as heavy addicted smokers. Data was not available for the 2001 survey.

SFCC 2004 Survey Summary. March 21, 2005 22
3.4 Attitudes toward an intervention Some attitudes changed drastically from 2001 to 2004. Table 15 shows that over 15% more monks in 2004 stated that they are willing to teach about smoking. This could be a result of the many programs or media about smoking. Table 15a. Willing to teach about the effects of smoking shown by current smoker. SFBM 2001 ADRA Cambodia survey questionnaire. Column percentages shown in brackets []. Buddhist Monk Survey. Current smoker Not current smoker Total Will teach 270 600 870 [62.0%] Will not 169 231 400 [28.5] Not sure 47 87 134 [9.5%] Total 486 918 1404 [100%] Table 15b. Willing to teach about the effects of smoking shown by current smoker. SFCC 2004 ADRA Cambodia survey questionnaire. Column percentages shown in brackets []. Buddhist Monk Survey. Current smoker Not current smoker Total Will teach 266 1192 1458 [77.6%]Will not 79 147 226 [12.0%] Not sure 75 120 195 [10.4%] Total 420 1459 1879 [100%] Table 15c. Interest in quitting smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Want to stop smoking
2001 2004
(n) % (N) (n) % (N) Want to stop 481 94.7 508 428 94.3 454 Don’t want to stop 15 3.0 508 7 1.5 454 Don’t know 12 2.3 508 19 4.2 454 T-test of desire to quit smoking between 2001 and 2004: t=-0.91, p=0.81 The desire to quit smoking appeared to stay the same between 2001 and 2004. A t-test was conducted which showed that there is no significant difference between means of 2001 and 2004. Table 15d and 15e were new questions added to the survey questionnaire in 2004. Most smoking monks state a health reason for wanting to stop smoking. Out of those monks who are former smokers, most cite using counseling or an “other” method for quitting. Only 4.4% cite using the SCP program to quit. Table 15d. Why the smoker quit. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Buddhist Monk Survey. Why quit (n) % (N) Health reasons 345 84.98 406 Money 79 19.46 406 Policy 36 8.87 406 Other 51 12.56 406
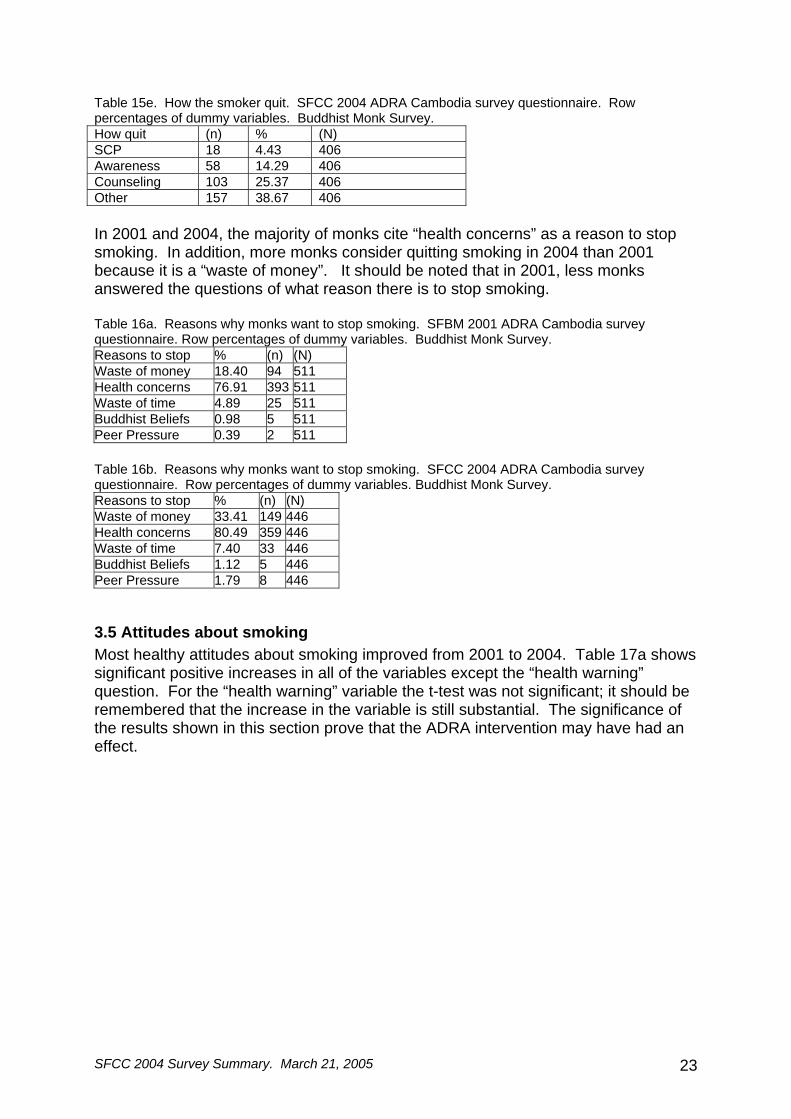
SFCC 2004 Survey Summary. March 21, 2005 23
Table 15e. How the smoker quit. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Buddhist Monk Survey. How quit (n) % (N) SCP 18 4.43 406 Awareness 58 14.29 406 Counseling 103 25.37 406 Other 157 38.67 406 In 2001 and 2004, the majority of monks cite “health concerns” as a reason to stop smoking. In addition, more monks consider quitting smoking in 2004 than 2001 because it is a “waste of money”. It should be noted that in 2001, less monks answered the questions of what reason there is to stop smoking. Table 16a. Reasons why monks want to stop smoking. SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Buddhist Monk Survey. Reasons to stop % (n) (N) Waste of money 18.40 94 511 Health concerns 76.91 393 511 Waste of time 4.89 25 511 Buddhist Beliefs 0.98 5 511 Peer Pressure 0.39 2 511 Table 16b. Reasons why monks want to stop smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Buddhist Monk Survey. Reasons to stop % (n) (N) Waste of money 33.41 149 446 Health concerns 80.49 359 446 Waste of time 7.40 33 446 Buddhist Beliefs 1.12 5 446 Peer Pressure 1.79 8 446
3.5 Attitudes about smoking Most healthy attitudes about smoking improved from 2001 to 2004. Table 17a shows significant positive increases in all of the variables except the “health warning” question. For the “health warning” variable the t-test was not significant; it should be remembered that the increase in the variable is still substantial. The significance of the results shown in this section prove that the ADRA intervention may have had an effect.

SFCC 2004 Survey Summary. March 21, 2005 24
Table 17a. Five attitude questions about smoking. SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages in each year. Buddhist Monk Survey. 2001 2004 t-test Questions about smoking % yes (n) (N) % yes (n) (N) (t) (p) Should monks smoke 14.9 214 1436 4.3 83 1937 10.94 0.00 Do you like being around a smoker?
16.6 238 1437 8.2 159 1947 7.58 0.00
Should there be a warning on tobacco products?
86.4 1242 1434 93.5 1819 1945 -6.8 1.00
Should advertising be allowed in Cambodia?
17.4 249 1434 10.5 204 1946 5.83 0.00
If a program was offered in your Pagoda to help monks stop smoking, would you attend? (current smokers)
98.0 500 510 99.3 452 455 3.51 0.00
Table 17b. Six attitude questions about smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. % yes (n) (N) Should the government increase tax on cigarette tobacco?
79.7 1548 1943
Table 18a. What Buddhist teachings say about smoking. SFCC 2004 and SFBM 2001 ADRA Cambodia survey questionnaire. Buddhist Monk Survey. Year 2001 2004 % (n) (N) % (n) (N) Nothing 50 718 1437 26.60 516 1937 Smoking is OK 5.40 77 1437 5.40 105 1937 Smoking is not OK 39.70 571 1437 62.20 1204 1937 Other 4.90 71 1437 5.80 112 1937 Total (N) 100 1437 100 1937
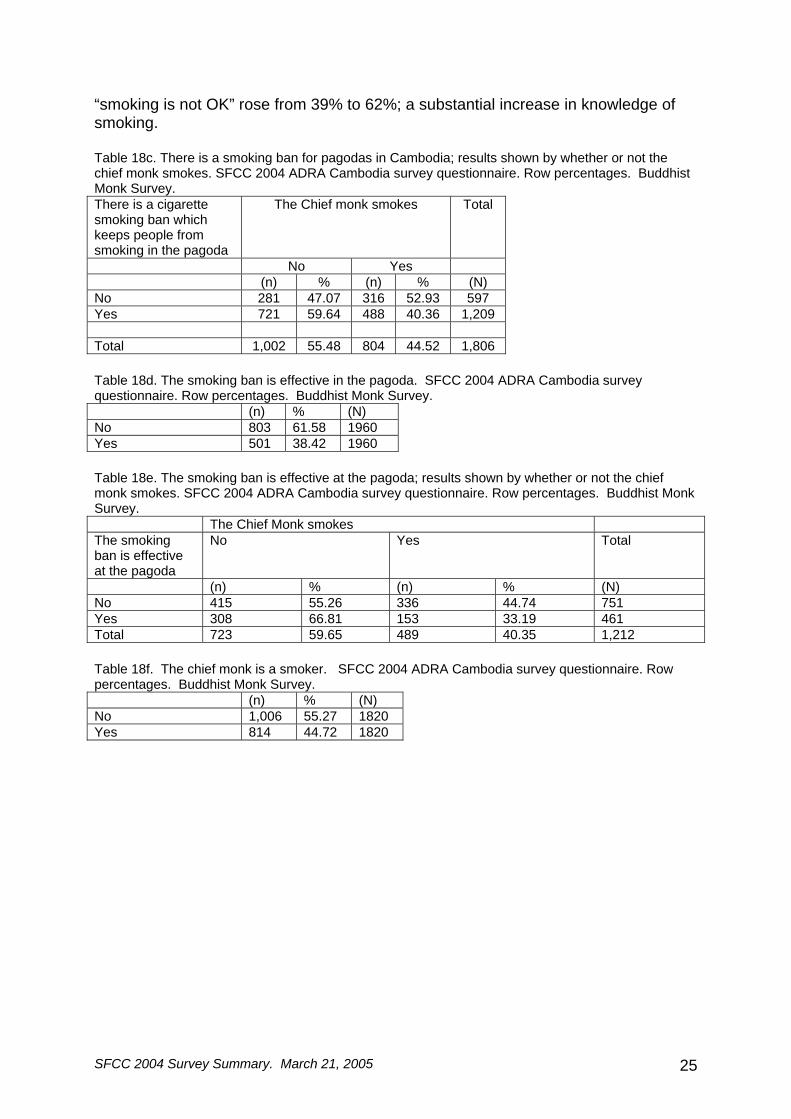
Table 18b. There is a smoking ban for pagodas in Cambodia. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. (n) % (N) No 644 33.09 1960 Yes 1,302 66.91 1960 Table 18b shows that only about 2/3rds of Cambodian Monks realize that that there is a smoking ban for pagodas in Cambodia. Table 18c show that although many of the monks realize there is a smoking ban in the pagodas, their chief monk still smokes (n=488 or 40.3% of all those who realize that there is a smoking ban). Over 38% (n=501) of the Buddhist monks interviewed stated that the smoking ban is effective at their pagoda. Table 18e presents some more interesting results; it shows that for Buddhist monks who state that the smoking ban is effective at the pagoda, 33.1% of the chief monks still smoke (n=153). The results presented in the above paragraph are from both the survey questionnaire with individual monks, and another survey questionnaire with the chief monk. Both questionnaires were administered at the same time. Table 18a shows a substantial increase from 2001 to 2004 in Buddhist monks who believe that Buddhist teachings say “smoking is not OK”. The monks who stated that
SFCC 2004 Survey Summary. March 21, 2005 25
“smoking is not OK” rose from 39% to 62%; a substantial increase in knowledge of smoking. Table 18c. There is a smoking ban for pagodas in Cambodia; results shown by whether or not the chief monk smokes. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. There is a cigarette smoking ban which keeps people from smoking in the pagoda
The Chief monk smokes Total
No Yes (n) % (n) % (N) No 281 47.07 316 52.93 597 Yes 721 59.64 488 40.36 1,209 Total 1,002 55.48 804 44.52 1,806 Table 18d. The smoking ban is effective in the pagoda. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. (n) % (N) No 803 61.58 1960 Yes 501 38.42 1960 Table 18e. The smoking ban is effective at the pagoda; results shown by whether or not the chief monk smokes. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. The Chief Monk smokes The smoking ban is effective at the pagoda
No Yes Total
(n) % (n) % (N) No 415 55.26 336 44.74 751 Yes 308 66.81 153 33.19 461 Total 723 59.65 489 40.35 1,212 Table 18f. The chief monk is a smoker. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. (n) % (N) No 1,006 55.27 1820 Yes 814 44.72 1820
SFCC 2004 Survey Summary. March 21, 2005 26
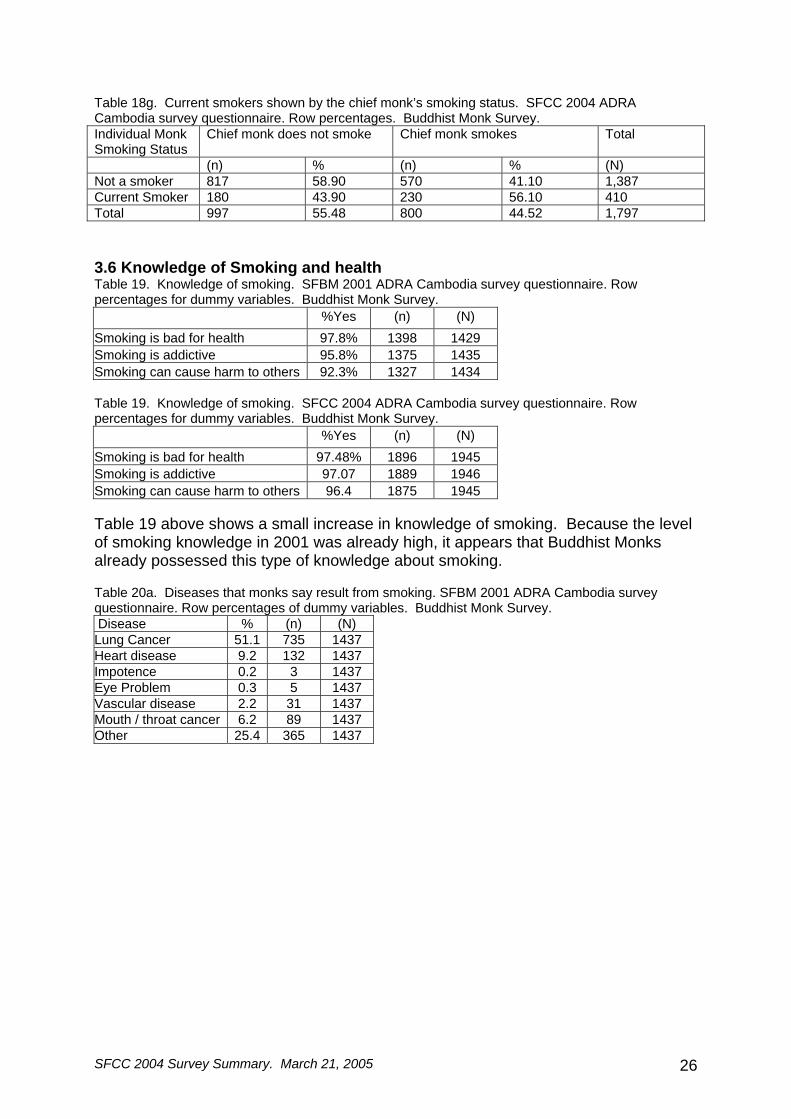
Table 18g. Current smokers shown by the chief monk’s smoking status. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Buddhist Monk Survey. Individual Monk Smoking Status
Chief monk does not smoke Chief monk smokes Total
(n) % (n) % (N) Not a smoker 817 58.90 570 41.10 1,387 Current Smoker 180 43.90 230 56.10 410 Total 997 55.48 800 44.52 1,797 3.6 Knowledge of Smoking and health Table 19. Knowledge of smoking. SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages for dummy variables. Buddhist Monk Survey. %Yes (n) (N) Smoking is bad for health 97.8% 1398 1429 Smoking is addictive 95.8% 1375 1435 Smoking can cause harm to others 92.3% 1327 1434 Table 19. Knowledge of smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages for dummy variables. Buddhist Monk Survey. %Yes (n) (N) Smoking is bad for health 97.48% 1896 1945 Smoking is addictive 97.07 1889 1946 Smoking can cause harm to others 96.4 1875 1945 Table 19 above shows a small increase in knowledge of smoking. Because the level of smoking knowledge in 2001 was already high, it appears that Buddhist Monks already possessed this type of knowledge about smoking. Table 20a. Diseases that monks say result from smoking. SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Buddhist Monk Survey. Disease % (n) (N) Lung Cancer 51.1 735 1437 Heart disease 9.2 132 1437 Impotence 0.2 3 1437 Eye Problem 0.3 5 1437 Vascular disease 2.2 31 1437 Mouth / throat cancer 6.2 89 1437 Other 25.4 365 1437
SFCC 2004 Survey Summary. March 21, 2005 27
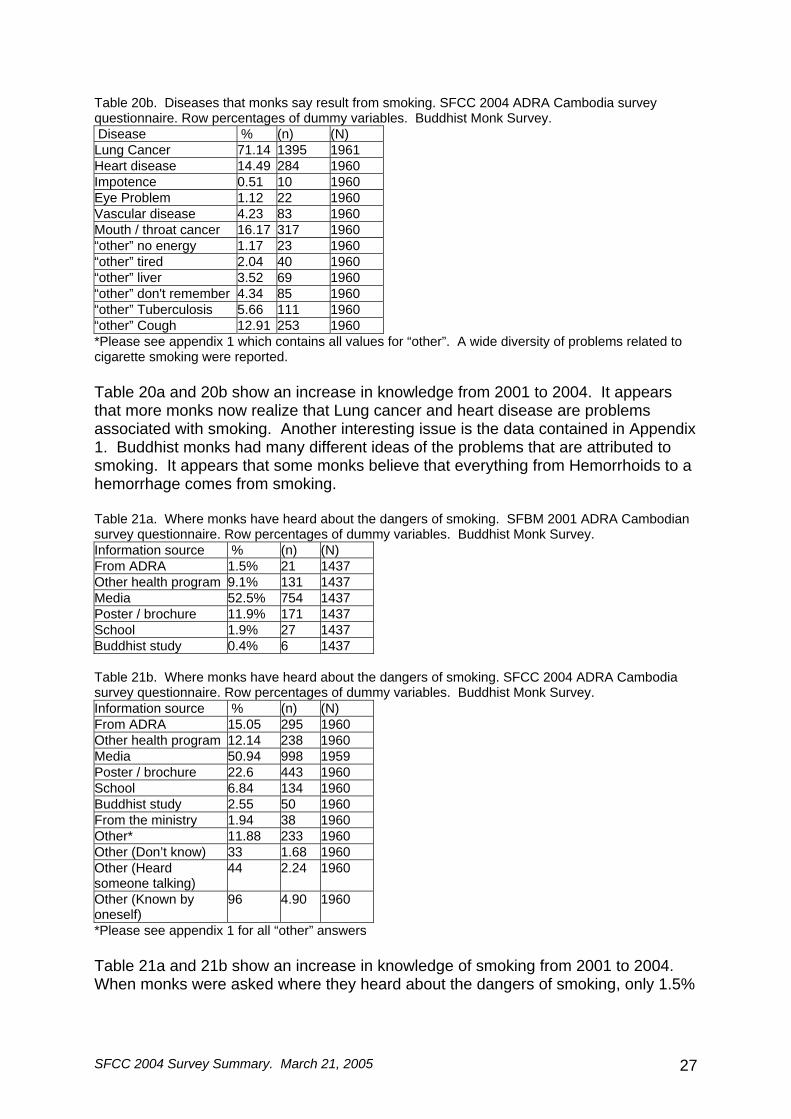
Table 20b. Diseases that monks say result from smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Buddhist Monk Survey. Disease % (n) (N) Lung Cancer 71.14 1395 1961 Heart disease 14.49 284 1960 Impotence 0.51 10 1960 Eye Problem 1.12 22 1960 Vascular disease 4.23 83 1960 Mouth / throat cancer 16.17 317 1960 “other” no energy 1.17 23 1960 “other” tired 2.04 40 1960 “other” liver 3.52 69 1960 “other” don't remember 4.34 85 1960 “other” Tuberculosis 5.66 111 1960 “other” Cough 12.91 253 1960 *Please see appendix 1 which contains all values for “other”. A wide diversity of problems related to cigarette smoking were reported. Table 20a and 20b show an increase in knowledge from 2001 to 2004. It appears that more monks now realize that Lung cancer and heart disease are problems associated with smoking. Another interesting issue is the data contained in Appendix 1. Buddhist monks had many different ideas of the problems that are attributed to smoking. It appears that some monks believe that everything from Hemorrhoids to a hemorrhage comes from smoking. Table 21a. Where monks have heard about the dangers of smoking. SFBM 2001 ADRA Cambodian survey questionnaire. Row percentages of dummy variables. Buddhist Monk Survey. Information source % (n) (N) From ADRA 1.5% 21 1437 Other health program 9.1% 131 1437 Media 52.5% 754 1437 Poster / brochure 11.9% 171 1437 School 1.9% 27 1437 Buddhist study 0.4% 6 1437 Table 21b. Where monks have heard about the dangers of smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Buddhist Monk Survey. Information source % (n) (N) From ADRA 15.05 295 1960 Other health program 12.14 238 1960 Media 50.94 998 1959 Poster / brochure 22.6 443 1960 School 6.84 134 1960 Buddhist study 2.55 50 1960 From the ministry 1.94 38 1960 Other* 11.88 233 1960 Other (Don’t know) 33 1.68 1960 Other (Heard someone talking)
44 2.24 1960
Other (Known by oneself)
96 4.90 1960
*Please see appendix 1 for all “other” answers Table 21a and 21b show an increase in knowledge of smoking from 2001 to 2004. When monks were asked where they heard about the dangers of smoking, only 1.5%

SFCC 2004 Survey Summary. March 21, 2005 28
replied “ADRA” in 2001. In 2004 this number rose to 15.05%. Knowledge gained from “posters” and “schools” also increased. Table 21c. Source of information about the dangers of smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Buddhist Monk Survey. Media source % (n) (N) Radio 46.48 911 1960 Daily News 1.89 37 1960 Radio talk show 3.21 63 1960 Print media 1.79 35 1960 Monk Preaching 2.60 51 1960 Cigarette Packaging
6.58 129 1960
TV spot 27.04 530 1960 Other * 0.3 6 1960 *This variable included “by learning”, “people talking”, and “from the elders”. Table 21d. Source of information about dangers of smoking; results shown by province. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages shown independently for each province. Dummy variables across columns. Buddhist Monk Survey.
PROVINCE Radio
Total Daily News Total Radio talk show Total Print Media Total
(n) % (N) (n) % (N) (n) % (N) (n) % (N)
Phnom Penh
199 55.12 361 25 6.93 361 15 4.16 361 16 4.43 361
Seim Reap 199 48.89 407 3 0.74 407 8 1.97 407 7 1.72 407 Svay Rieng 175 45.34 386 4 1.04 386 12 3.11 386 4 1.04 386 Pousat 169 42.04 402 4 1 402 15 3.73 402 3 0.75 402
Kampot 169 41.83 404 1 0.25 404 13 3.22 404 5 1.24 404 Total 911 46.48 1,960 37 1.89 1960 63 3.21 1960 35 1.79 1960
PROVINCE Monk Preaching Total Cigarette Packaging Total TV spot Total (n) % (N) (n) % (N) (n) % (N) Phnom Penh
22 6.09 361 40 11.08 361 175 48.48 361
Seim Reap 10 2.46 407 28 6.88 407 109 26.78 407 Svay Rieng 14 3.63 386 24 6.22 386 85 22.02 386 Pousat 3 0.75 402 22 5.47 402 77 19.15 402 Kampot 2 0.5 404 15 3.71 404 84 20.79 404 Total 51 2.6 1,960 129 6.58 1960 530 27.04 1960
Table 21d shows the provincial reach of media broadcasting. Out of all provinces, Phnom Penh municipality has the greatest media broadcasting, second to Siem Reap. Kampot province had the least amount of broadcasting related to the dangers of smoking.
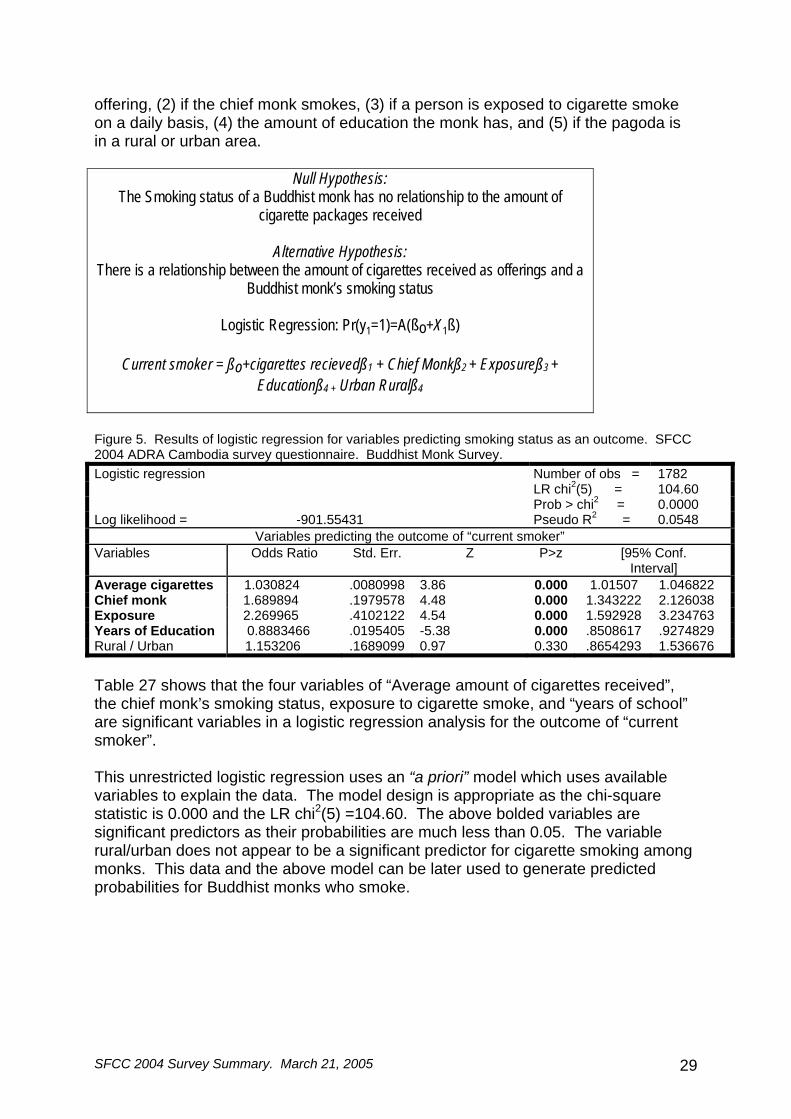
3.7 Regression It is possible to use the data from the 2004 survey to predict why a monk would smoke. Using logistic regression, we can make smoking the outcome and determine the effect that various predictors have on it. We can later use those predictors for predicted probabilities. The predictors from this survey which will directly effect the outcome of smoking are: (1) the amount of cigarettes received each month as an
SFCC 2004 Survey Summary. March 21, 2005 29
offering, (2) if the chief monk smokes, (3) if a person is exposed to cigarette smoke on a daily basis, (4) the amount of education the monk has, and (5) if the pagoda is in a rural or urban area.
Null Hypothesis: The Smoking status of a Buddhist monk has no relationship to the amount of
cigarette packages received
Alternative Hypothesis: There is a relationship between the amount of cigarettes received as offerings and a
Buddhist monk’s smoking status
Logistic Regression: Pr(y1=1)=A(ßo+X1ß)
Current smoker = ßo+cigarettes recievedß1 + Chief Monkß2 + Exposureß3 + Educationß4 + Urban Ruralß4
Figure 5. Results of logistic regression for variables predicting smoking status as an outcome. SFCC 2004 ADRA Cambodia survey questionnaire. Buddhist Monk Survey. Logistic regression Number of obs = 1782 LR chi2(5) = 104.60 Prob > chi2 = 0.0000 Log likelihood = -901.55431 Pseudo R2 = 0.0548
Variables predicting the outcome of “current smoker” Variables Odds Ratio Std. Err. Z P>z [95% Conf.
Interval] Average cigarettes 1.030824 .0080998 3.86 0.000 1.01507 1.046822 Chief monk 1.689894 .1979578 4.48 0.000 1.343222 2.126038 Exposure 2.269965 .4102122 4.54 0.000 1.592928 3.234763 Years of Education 0.8883466 .0195405 -5.38 0.000 .8508617 .9274829 Rural / Urban 1.153206 .1689099 0.97 0.330 .8654293 1.536676 Table 27 shows that the four variables of “Average amount of cigarettes received”, the chief monk’s smoking status, exposure to cigarette smoke, and “years of school” are significant variables in a logistic regression analysis for the outcome of “current smoker”. This unrestricted logistic regression uses an “a priori” model which uses available variables to explain the data. The model design is appropriate as the chi-square statistic is 0.000 and the LR chi2(5) =104.60. The above bolded variables are significant predictors as their probabilities are much less than 0.05. The variable rural/urban does not appear to be a significant predictor for cigarette smoking among monks. This data and the above model can be later used to generate predicted probabilities for Buddhist monks who smoke.
SFCC 2004 Survey Summary. March 21, 2005 30
3.8 Results of additional pagoda survey In addition to the Buddhist monk survey, another survey questionnaire was conducted simultaneously with each chief monk at each pagoda visited. The results of this analysis are in Appendix 3. 4. Results - Community Survey
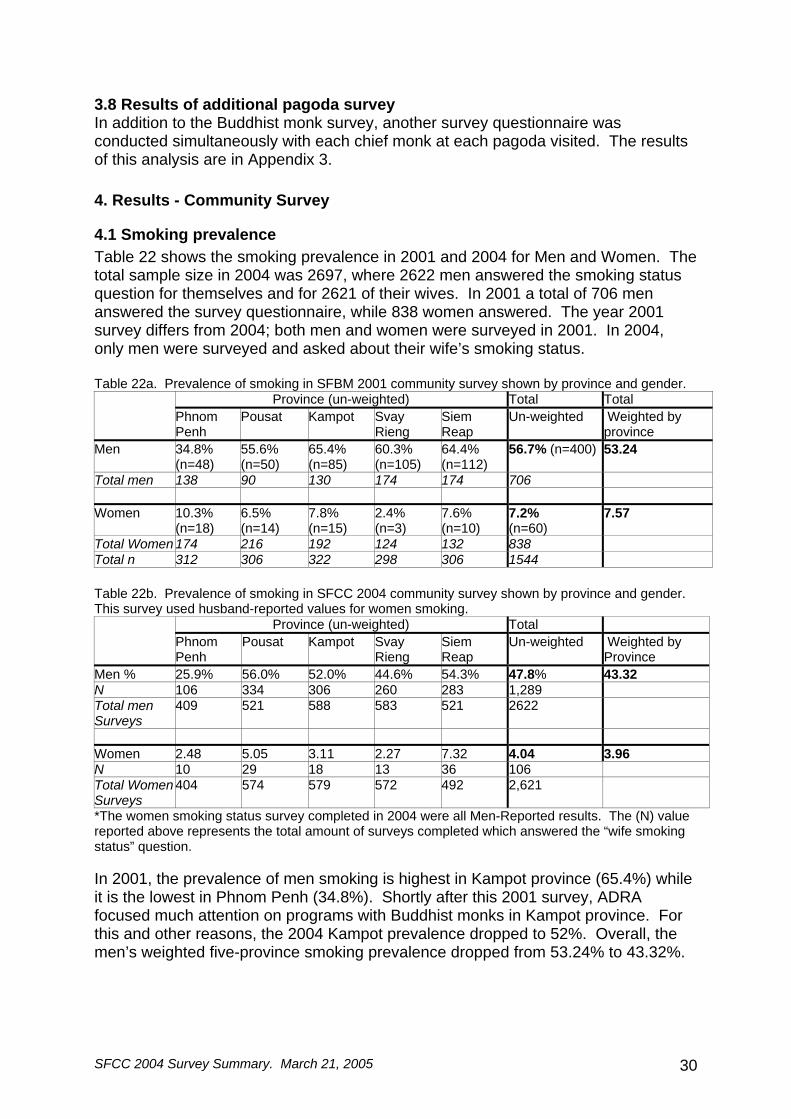
4.1 Smoking prevalence Table 22 shows the smoking prevalence in 2001 and 2004 for Men and Women. The total sample size in 2004 was 2697, where 2622 men answered the smoking status question for themselves and for 2621 of their wives. In 2001 a total of 706 men answered the survey questionnaire, while 838 women answered. The year 2001 survey differs from 2004; both men and women were surveyed in 2001. In 2004, only men were surveyed and asked about their wife’s smoking status. Table 22a. Prevalence of smoking in SFBM 2001 community survey shown by province and gender.
Province (un-weighted) Total Total Phnom
Penh Pousat Kampot Svay
Rieng Siem Reap
Un-weighted Weighted by province
Men 34.8% (n=48)
55.6% (n=50)
65.4% (n=85)
60.3% (n=105)
64.4% (n=112)
56.7% (n=400) 53.24
Total men 138 90 130 174 174 706 Women 10.3%
(n=18) 6.5% (n=14)
7.8% (n=15)
2.4% (n=3)
7.6% (n=10)
7.2% (n=60)
7.57
Total Women 174 216 192 124 132 838 Total n 312 306 322 298 306 1544 Table 22b. Prevalence of smoking in SFCC 2004 community survey shown by province and gender. This survey used husband-reported values for women smoking.
Province (un-weighted) Total Phnom
Penh Pousat Kampot Svay
Rieng Siem Reap
Un-weighted Weighted by Province
Men % 25.9% 56.0% 52.0% 44.6% 54.3% 47.8% 43.32 N 106 334 306 260 283 1,289 Total men Surveys
409 521 588 583 521 2622
Women 2.48 5.05 3.11 2.27 7.32 4.04 3.96 N 10 29 18 13 36 106 Total Women Surveys
404 574 579 572 492 2,621
*The women smoking status survey completed in 2004 were all Men-Reported results. The (N) value reported above represents the total amount of surveys completed which answered the “wife smoking status” question. In 2001, the prevalence of men smoking is highest in Kampot province (65.4%) while it is the lowest in Phnom Penh (34.8%). Shortly after this 2001 survey, ADRA focused much attention on programs with Buddhist monks in Kampot province. For this and other reasons, the 2004 Kampot prevalence dropped to 52%. Overall, the men’s weighted five-province smoking prevalence dropped from 53.24% to 43.32%.

SFCC 2004 Survey Summary. March 21, 2005 31
There is not a substantial difference between the two weighted prevalence figures for women. The weighted prevalence does differ by 4-5% in the men’s group.
SFCC 2004 Survey Summary. March 21, 2005 32
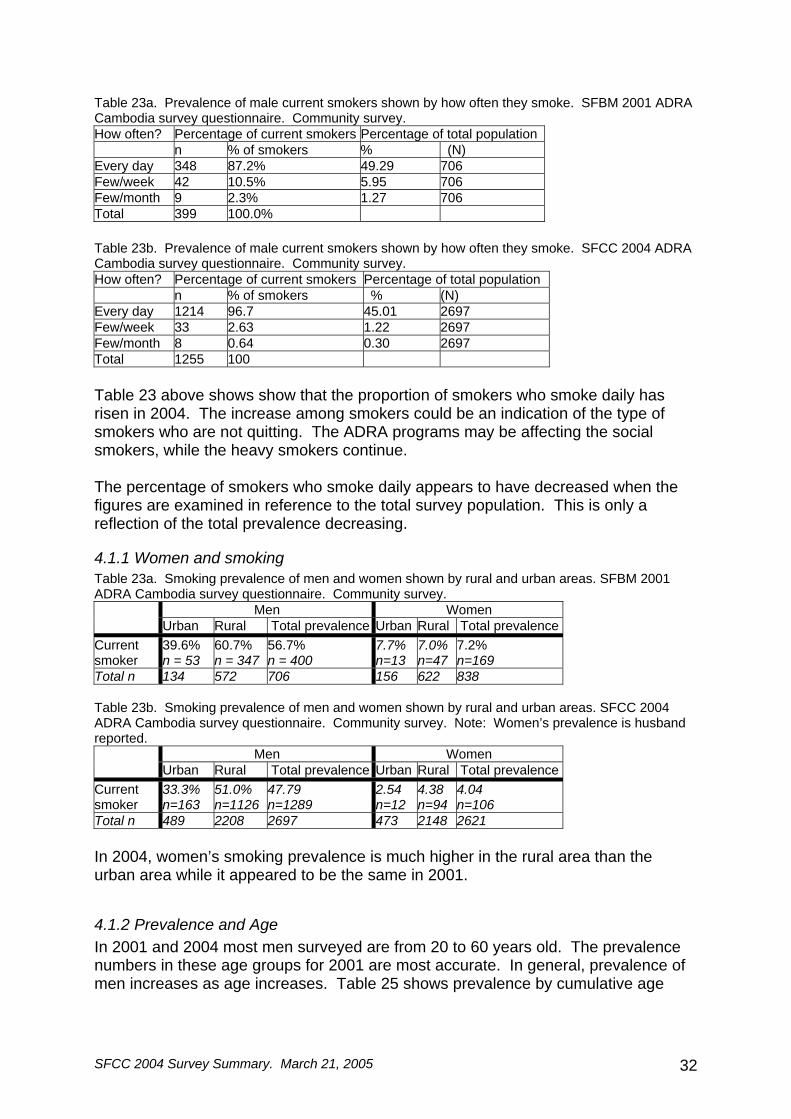
Table 23a. Prevalence of male current smokers shown by how often they smoke. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. How often? Percentage of current smokers Percentage of total population n % of smokers % (N) Every day 348 87.2% 49.29 706 Few/week 42 10.5% 5.95 706 Few/month 9 2.3% 1.27 706 Total 399 100.0% Table 23b. Prevalence of male current smokers shown by how often they smoke. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. How often? Percentage of current smokers Percentage of total population n % of smokers % (N) Every day 1214 96.7 45.01 2697 Few/week 33 2.63 1.22 2697 Few/month 8 0.64 0.30 2697 Total 1255 100 Table 23 above shows show that the proportion of smokers who smoke daily has risen in 2004. The increase among smokers could be an indication of the type of smokers who are not quitting. The ADRA programs may be affecting the social smokers, while the heavy smokers continue. The percentage of smokers who smoke daily appears to have decreased when the figures are examined in reference to the total survey population. This is only a reflection of the total prevalence decreasing.
4.1.1 Women and smoking Table 23a. Smoking prevalence of men and women shown by rural and urban areas. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey.
Men Women Urban Rural Total prevalence Urban Rural Total prevalence
Current smoker
39.6% n = 53
60.7% n = 347
56.7% n = 400
7.7% n=13
7.0% n=47
7.2% n=169
Total n 134 572 706 156 622 838 Table 23b. Smoking prevalence of men and women shown by rural and urban areas. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Note: Women’s prevalence is husband reported.
Men Women Urban Rural Total prevalence Urban Rural Total prevalence
Current smoker
33.3% n=163
51.0% n=1126
47.79 n=1289
2.54 n=12
4.38 n=94
4.04 n=106
Total n 489 2208 2697 473 2148 2621 In 2004, women’s smoking prevalence is much higher in the rural area than the urban area while it appeared to be the same in 2001.
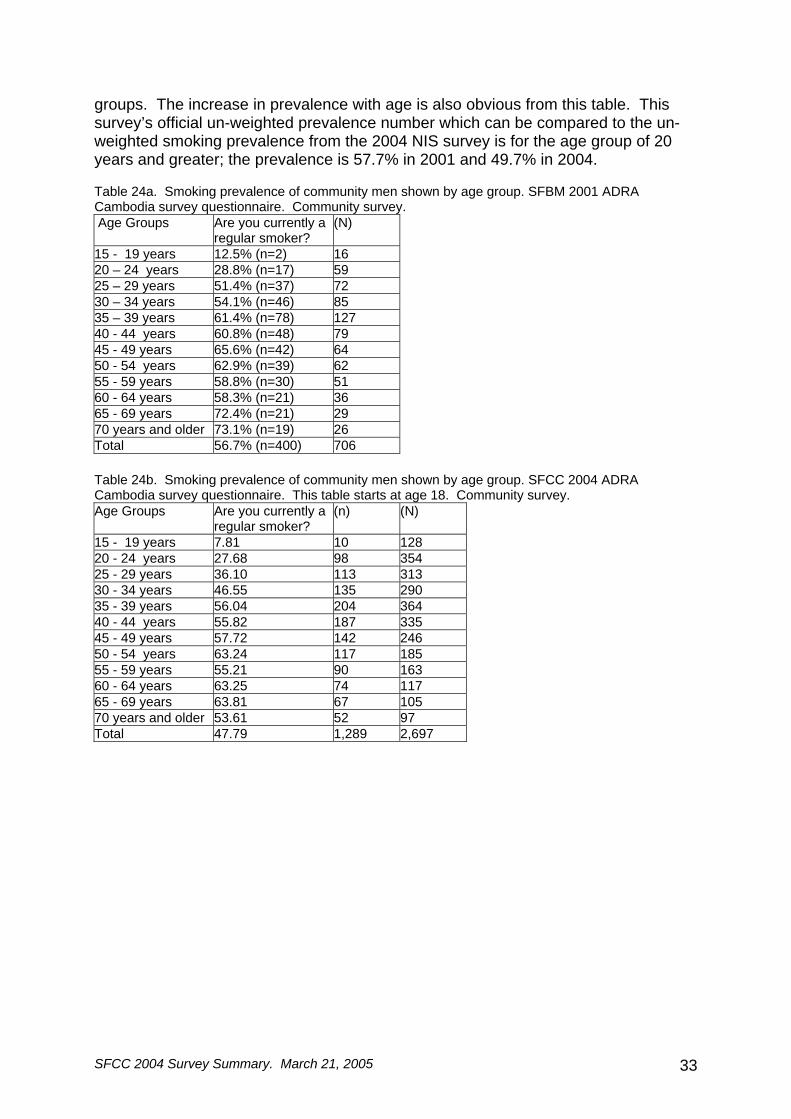
4.1.2 Prevalence and Age In 2001 and 2004 most men surveyed are from 20 to 60 years old. The prevalence numbers in these age groups for 2001 are most accurate. In general, prevalence of men increases as age increases. Table 25 shows prevalence by cumulative age
SFCC 2004 Survey Summary. March 21, 2005 33
groups. The increase in prevalence with age is also obvious from this table. This survey’s official un-weighted prevalence number which can be compared to the un-weighted smoking prevalence from the 2004 NIS survey is for the age group of 20 years and greater; the prevalence is 57.7% in 2001 and 49.7% in 2004. Table 24a. Smoking prevalence of community men shown by age group. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. Age Groups Are you currently a
regular smoker? (N)
15 - 19 years 12.5% (n=2) 16 20 – 24 years 28.8% (n=17) 59 25 – 29 years 51.4% (n=37) 72 30 – 34 years 54.1% (n=46) 85 35 – 39 years 61.4% (n=78) 127 40 - 44 years 60.8% (n=48) 79 45 - 49 years 65.6% (n=42) 64 50 - 54 years 62.9% (n=39) 62 55 - 59 years 58.8% (n=30) 51 60 - 64 years 58.3% (n=21) 36 65 - 69 years 72.4% (n=21) 29 70 years and older 73.1% (n=19) 26 Total 56.7% (n=400) 706 Table 24b. Smoking prevalence of community men shown by age group. SFCC 2004 ADRA Cambodia survey questionnaire. This table starts at age 18. Community survey. Age Groups Are you currently a
regular smoker? (n) (N)
15 - 19 years 7.81 10 128 20 - 24 years 27.68 98 354 25 - 29 years 36.10 113 313 30 - 34 years 46.55 135 290 35 - 39 years 56.04 204 364 40 - 44 years 55.82 187 335 45 - 49 years 57.72 142 246 50 - 54 years 63.24 117 185 55 - 59 years 55.21 90 163 60 - 64 years 63.25 74 117 65 - 69 years 63.81 67 105 70 years and older 53.61 52 97 Total 47.79 1,289 2,697
SFCC 2004 Survey Summary. March 21, 2005 34
01020304050607080
15 -
19 ye
ars
20 - 2
4 years
25 - 2
9 years
30 - 3
4 years
35 - 3
9 years
40 - 4
4 years
45 - 4
9 years
50 - 5
4 years
55 - 5
9 years
60 - 6
4 years
65 - 6
9 years
70 ye
ars an
d olde
r
Age Groups
Smok
ing
Prev
alen
ce
20012004
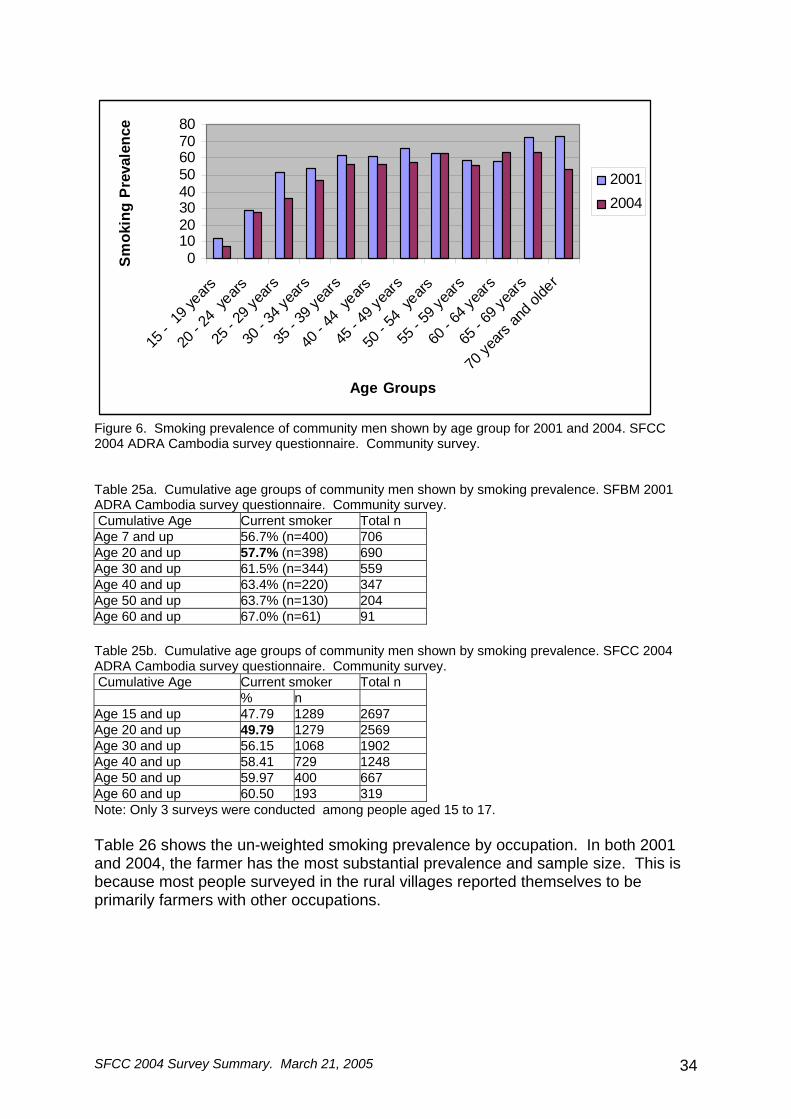
Figure 6. Smoking prevalence of community men shown by age group for 2001 and 2004. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Table 25a. Cumulative age groups of community men shown by smoking prevalence. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. Cumulative Age Current smoker Total n Age 7 and up 56.7% (n=400) 706 Age 20 and up 57.7% (n=398) 690 Age 30 and up 61.5% (n=344) 559 Age 40 and up 63.4% (n=220) 347 Age 50 and up 63.7% (n=130) 204 Age 60 and up 67.0% (n=61) 91 Table 25b. Cumulative age groups of community men shown by smoking prevalence. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Cumulative Age Current smoker Total n % n Age 15 and up 47.79 1289 2697 Age 20 and up 49.79 1279 2569 Age 30 and up 56.15 1068 1902 Age 40 and up 58.41 729 1248 Age 50 and up 59.97 400 667 Age 60 and up 60.50 193 319 Note: Only 3 surveys were conducted among people aged 15 to 17. Table 26 shows the un-weighted smoking prevalence by occupation. In both 2001 and 2004, the farmer has the most substantial prevalence and sample size. This is because most people surveyed in the rural villages reported themselves to be primarily farmers with other occupations.

SFCC 2004 Survey Summary. March 21, 2005 35
Table 26a. Prevalence of smoking shown by occupation. SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Community survey. Occupation Prevalence Total Cyclo, taxi, motodup 56.5% (n=13) 23 F/T student 16.7% (n=3) 18 Seller, small business 30.8% (n=20) 65 Skill pro office 30% (n=9) 30 Blue collar work 69.2% (n=18) 26 Military, security, police 43.2% (n=16) 37 Unemployed, home 60% (n=18) 30 Farmer 64.4% (n=293) 455 Teacher 31.3% (n=5) 16 Fisherman 60% (n=3) 5 Other Table 26b. Prevalence of men and women smoking shown by occupation. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Community survey. Men Women Occupation Prevalence Total Prevalence Total % n n % n n Cyclo, taxi, motodup 38.37 86 33 0 0 1 F/T student 6.06 165 10 0 0 2 Seller, small business 35.52 183 65 2.1 6 286 Skill pro office 35.27 224 79 0 0 64 Blue collar work 45.83 24 11 7.41 2 27 Military, security, police 37.93 87 33 0 0 2 Unemployed, home 37.80 82 31 2.67 2 75 Farmer 57.29 1,674 959 5.72 90 1573 Teacher 20.29 69 14 0 0 25` Fisherman 61.54 26 16 0 0 5 Other 51.43 70 36 3.62 5 138 Total 47.84 1,287 2,690 4.78 105 2198 The mean years of education increased in all provinces from the 2001 survey to the 2004 survey. This was similar to the monk study and probably is also another important predictor for smoking status. Tables 27c and 27d show the prevalence decreasing as the education increases. Table 27a. Average number of years of education of all community members shown by province. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. Province Mean N SD Phnom Penh 6.59 312 4.07Pousat 3.48 306 3.54Kampot 4.51 322 3.64Svay Rieng 4.48 296 3.10Siem Reap 2.89 306 3.17Total 4.40 1542 3.74
SFCC 2004 Survey Summary. March 21, 2005 36
Table 27b. Average number of years of education of all community members shown by province. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Province Mean N SD Phnom Penh 8.77 410 4.09 Pousat 5.82 596 3.66 Kampot 6.06 587 3.5 Svay Rieng 6.53 582 3.3 Siem Reap 4.04 521 3.72 Total 6.13 2696 3.9 Table 27c. Smoking prevalence of men; data shown by educational levels reached. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. Years of School (n) % (N) no school 51 60.71 84 year 1-3 79 64.23 123 year 4 47 87.04 54 year 5 38 59.38 64 year 6 17 56.67 30 year 7-10 96 46.60 206 year 11-25 22 30.99 71 Total 350 55.38 632 Table 27d. Smoking prevalence of men; data shown by educational levels reached. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Years of School (n) % (N) no school 185 68.27 271 year 1-3 299 63.08 474 year 4 144 57.83 249 year 5 135 49.63 272 year 6 101 52.60 192 year 7-10 343 39.84 861 year 11-25 79 21.18 373 Total 1,286 47.77 2,692 Table 28a. Prevalence of smoking status in community men shown by their history of being a monk. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. Have been a monk Have not been a monk Total N % N % Current smoker 74 69.8% 324 54.5 106 non smoker 324 30.2% 270 45.5 594 Total 398 100% 594 100.0% 700 Table 28b. Prevalence of smoking status in community men shown by their history of being a monk. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Have been a monk Have not been a
monk Total
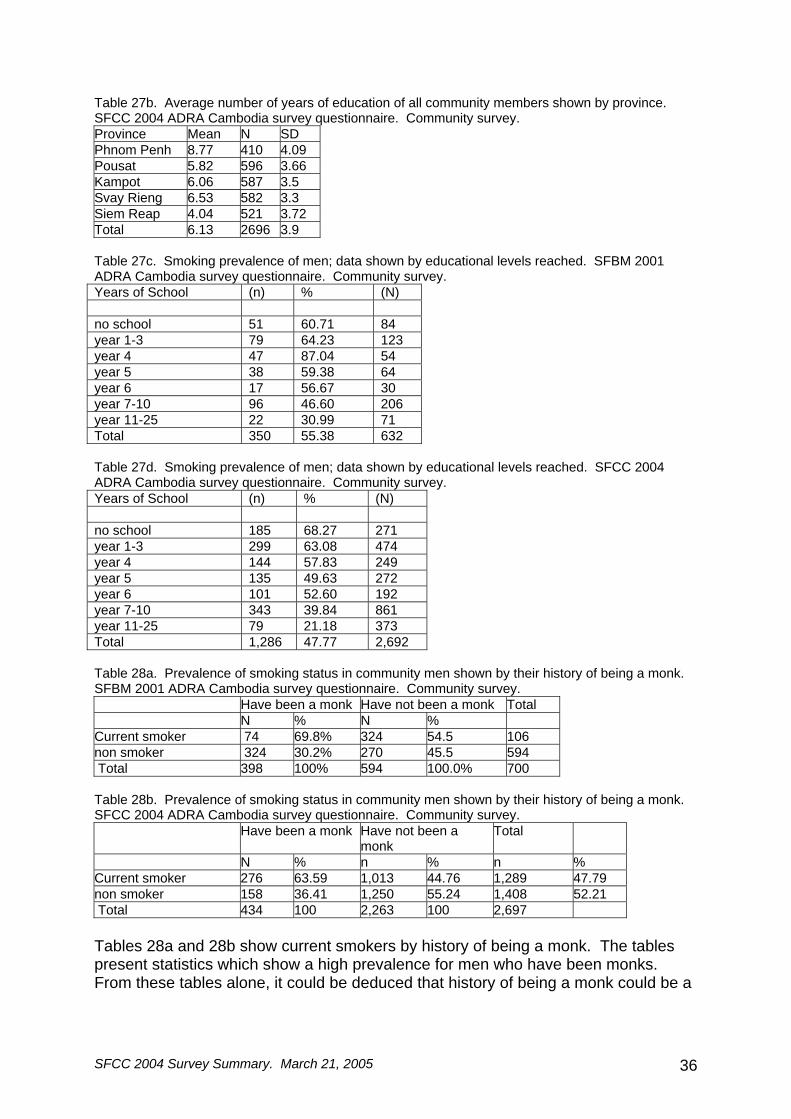
N % n % n % Current smoker 276 63.59 1,013 44.76 1,289 47.79 non smoker 158 36.41 1,250 55.24 1,408 52.21 Total 434 100 2,263 100 2,697 Tables 28a and 28b show current smokers by history of being a monk. The tables present statistics which show a high prevalence for men who have been monks. From these tables alone, it could be deduced that history of being a monk could be a
SFCC 2004 Survey Summary. March 21, 2005 37
partial predictor for a man’s smoking status. This would be a valid assumption if all other variables which effected smoking status were considered. This variable needs to be included in a regression analysis with all of the other potential predictors for smoking such as education, the family’s socio-economic-status, and the rural/urban variable.
4.2 Practices of smoking Table 29a. Male current smokers shown by if they had smoked 100 cigarettes. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey.
Have smoked over 100 cigarettes Have Not Have Total
Current Smoker
(n) % (n) % (N) % Not a smoker 203 91.44 78 19.02 281 44.46 Current Smoker 19 8.56 332 80.98 351 55.54 Total 222 100.00 410 100.00 632 100.00 Table 29b. Male current smokers shown by if they had smoked 100 cigarettes. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey.
Have Smoked over 100 cigarettes Have Not Have Total
Current Smoker
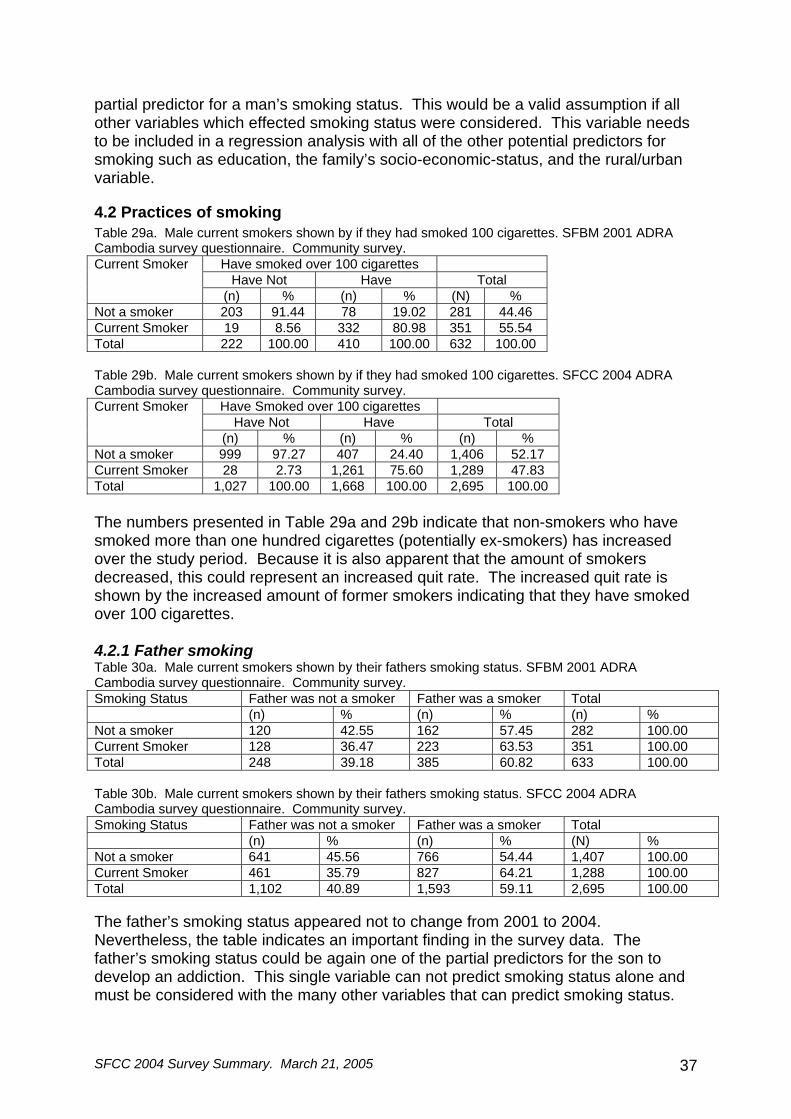
(n) % (n) % (n) % Not a smoker 999 97.27 407 24.40 1,406 52.17 Current Smoker 28 2.73 1,261 75.60 1,289 47.83 Total 1,027 100.00 1,668 100.00 2,695 100.00 The numbers presented in Table 29a and 29b indicate that non-smokers who have smoked more than one hundred cigarettes (potentially ex-smokers) has increased over the study period. Because it is also apparent that the amount of smokers decreased, this could represent an increased quit rate. The increased quit rate is shown by the increased amount of former smokers indicating that they have smoked over 100 cigarettes. 4.2.1 Father smoking Table 30a. Male current smokers shown by their fathers smoking status. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. Smoking Status Father was not a smoker Father was a smoker Total (n) % (n) % (n) % Not a smoker 120 42.55 162 57.45 282 100.00 Current Smoker 128 36.47 223 63.53 351 100.00 Total 248 39.18 385 60.82 633 100.00 Table 30b. Male current smokers shown by their fathers smoking status. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Smoking Status Father was not a smoker Father was a smoker Total (n) % (n) % (N) % Not a smoker 641 45.56 766 54.44 1,407 100.00 Current Smoker 461 35.79 827 64.21 1,288 100.00 Total 1,102 40.89 1,593 59.11 2,695 100.00 The father’s smoking status appeared not to change from 2001 to 2004. Nevertheless, the table indicates an important finding in the survey data. The father’s smoking status could be again one of the partial predictors for the son to develop an addiction. This single variable can not predict smoking status alone and must be considered with the many other variables that can predict smoking status.
SFCC 2004 Survey Summary. March 21, 2005 38
This variable needs to be included in a regression analysis with all of the other potential predictors for smoking such as history of being a monk, education, the family’s socio-economic-status, and the rural/urban variable. Table 35c. Smoke within 20 minutes of waking up. SFBM 2001 and SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Year Smoke within 20 minutes of waking up Total Current Smokers % (n) (N) 2001 62.2% 237 381 2004 58.72% 751 1279 Table 35d. Smoke more than 20 cigarettes per day; results shown by survey year. SFBM 2001 and SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Date Smoke 1-19 cigarettes/day Smoke more than
20 cigarettes/day Total
(n) % (n) % (N) 2001 survey 316 78.22 88 21.78 404 2004 survey 877 67.98 413 32.02 1,290 Total 1,193 70.43 501 29.57 1,694 (t-test results: Significant difference among the two years; t=-3.94, p=0.00) Table 35d shows an increase in those smokers who smoke more than 20 cigarettes / day. Out of all smokers, the percentage of those who say they smoke more than 20 cigarettes / day increases. This increase occurs simultaneously with a decrease in the prevalence of smoking among men. Table 23a and Table 23b also show this trend in smokers who report that they smoke daily. Similar to Table 23, Table 35d can be interpreted to explain that the perceived increase in heavy smokers is an illusion; most of 2001’s population of “light” smokers have quit. A higher percentage of heavy smokers remain addicted because of their relative addiction level. Table 35e. Smoke more than 20 cigarettes per day; results shown by those who smoke within 20 minutes of waking up in 2004 survey only. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Community survey. Smoke within 20 minutes of waking up?
Smoke 1-19 cigarettes / day -
Smoke more than 20 cigarettes/day
Total
(n) % (n) % (N) Do not smoke within 20 minutes of waking up
455 86.34 72 13.66 527
Smoke within 20 minutes of waking up
413 55.14 336 44.86 749
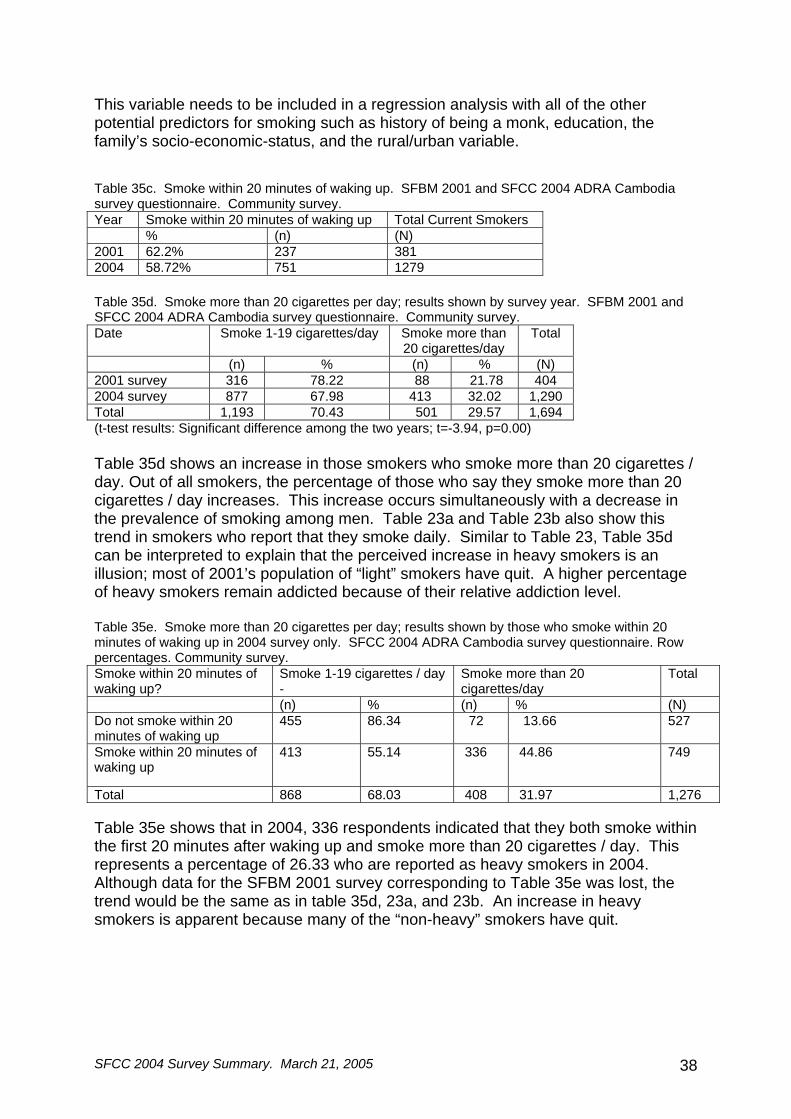
Total 868 68.03 408 31.97 1,276 Table 35e shows that in 2004, 336 respondents indicated that they both smoke within the first 20 minutes after waking up and smoke more than 20 cigarettes / day. This represents a percentage of 26.33 who are reported as heavy smokers in 2004. Although data for the SFBM 2001 survey corresponding to Table 35e was lost, the trend would be the same as in table 35d, 23a, and 23b. An increase in heavy smokers is apparent because many of the “non-heavy” smokers have quit.

SFCC 2004 Survey Summary. March 21, 2005 39
4.2.2 Second Hand Smoke Table 30c. Second hand smoke exposure reported by all survey respondents. SFCC 2004 and SFBM 2001 ADRA Cambodia survey questionnaire. Community survey.
2001 survey 2004 survey (n) % (N) (n) % (N)
Second Hand Smoke
805 59.02 1364 1683 62.48 2695 The survey asked community members if they are exposed to the cigarette smoke of others everyday. Although the results between 2001 and 2004 appear to be very similar, the statistic itself is important. About 60% of all community members are exposed to daily cigarette smoke. This is a high percentage that only seems to be slightly increasing. 4.2.3 Offerings Table 30d. Survey respondents reporting that they offer cigarettes to monks at the pagoda. SFCC 2004 and SFBM 2001 ADRA Cambodia survey questionnaire. Row Percentages. Community survey. Offer cigarettes to Monks (n) % (N) 2001 927 67.91 1,365 2004 1,327 49.20 2,697 Table 30e. How often the offerings of cigarettes are made to monks at the pagoda. SFCC 2004 and SFBM 2001 ADRA Cambodia survey questionnaire. Column Percentages. Community survey. How often do you offer cigarettes to monks
2001 survey 2004 survey
(n) % (N) (n) % (N) Weekly 51 5.49 929 30 2.25 1,332 Monthly 41 4.41 929 35 2.63 1,332 Special Ceremonies 837 90.10 929 1,267 95.12 1,332 Total 929 100 1,332 100 Table 30d and 30e show that there has been a decrease in the offering of tobacco to monks and also a decrease in the frequency that they offer; if people offer tobacco to monks, they are more likely to offer at a special ceremony and less likely to offer weekly or monthly. 4.2.4 Chewing Tobacco and betel nut Table 31a. Mean age of Men and Women's use of tobacco or betel leaf. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. Community survey. Mean Age Men Women Mean (n) SD Mean (n) SD Chew tobacco 47.1 19 13.0 45.6 46 11.90Betel 47.2 11 14.2 51.4 106 12.92Chew tobacco and betel 52.2 12 12.3 56.0 114 13.62No 41.1 659 14.0 37.9 569 12.67Total 41.6 701 14.1 42.5 835 14.60
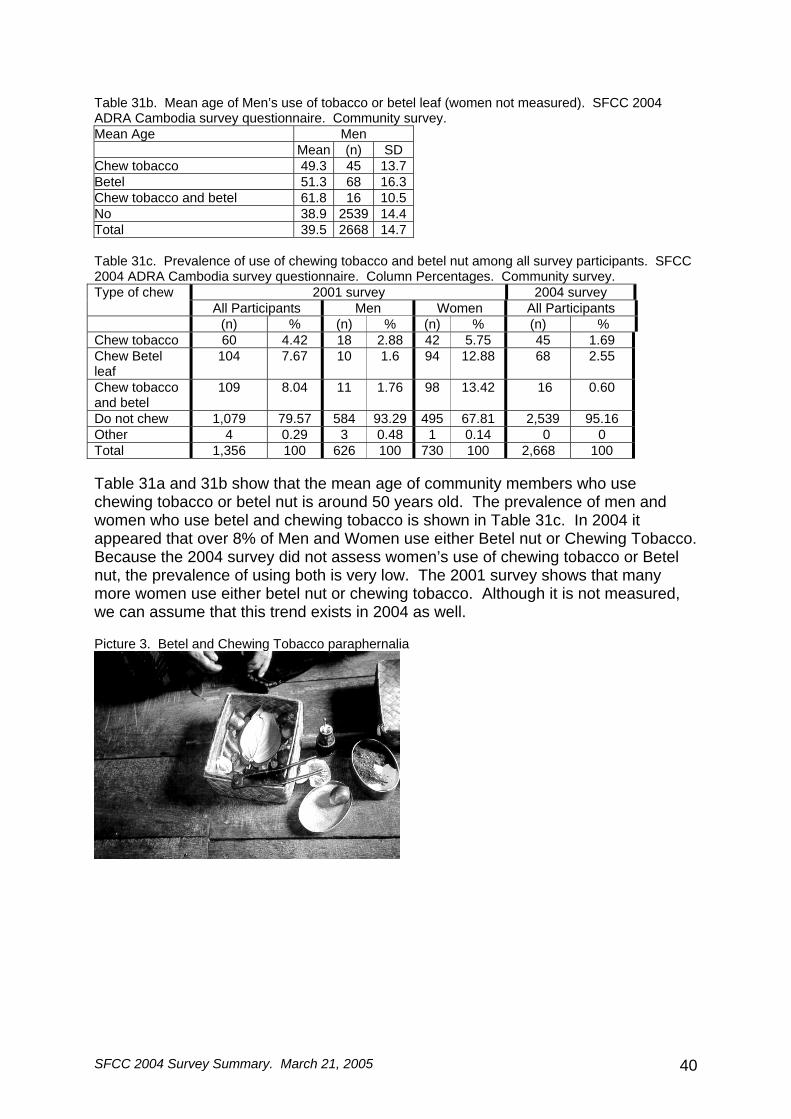
SFCC 2004 Survey Summary. March 21, 2005 40
Table 31b. Mean age of Men’s use of tobacco or betel leaf (women not measured). SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Mean Age Men Mean (n) SD Chew tobacco 49.3 45 13.7Betel 51.3 68 16.3Chew tobacco and betel 61.8 16 10.5No 38.9 2539 14.4Total 39.5 2668 14.7 Table 31c. Prevalence of use of chewing tobacco and betel nut among all survey participants. SFCC 2004 ADRA Cambodia survey questionnaire. Column Percentages. Community survey.
2001 survey 2004 survey Type of chew All Participants Men Women All Participants
(n) % (n) % (n) % (n) % Chew tobacco 60 4.42 18 2.88 42 5.75 45 1.69 Chew Betel leaf
104 7.67 10 1.6 94 12.88 68 2.55
Chew tobacco and betel
109 8.04 11 1.76 98 13.42 16 0.60
Do not chew 1,079 79.57 584 93.29 495 67.81 2,539 95.16 Other 4 0.29 3 0.48 1 0.14 0 0 Total 1,356 100 626 100 730 100 2,668 100 Table 31a and 31b show that the mean age of community members who use chewing tobacco or betel nut is around 50 years old. The prevalence of men and women who use betel and chewing tobacco is shown in Table 31c. In 2004 it appeared that over 8% of Men and Women use either Betel nut or Chewing Tobacco. Because the 2004 survey did not assess women’s use of chewing tobacco or Betel nut, the prevalence of using both is very low. The 2001 survey shows that many more women use either betel nut or chewing tobacco. Although it is not measured, we can assume that this trend exists in 2004 as well. Picture 3. Betel and Chewing Tobacco paraphernalia
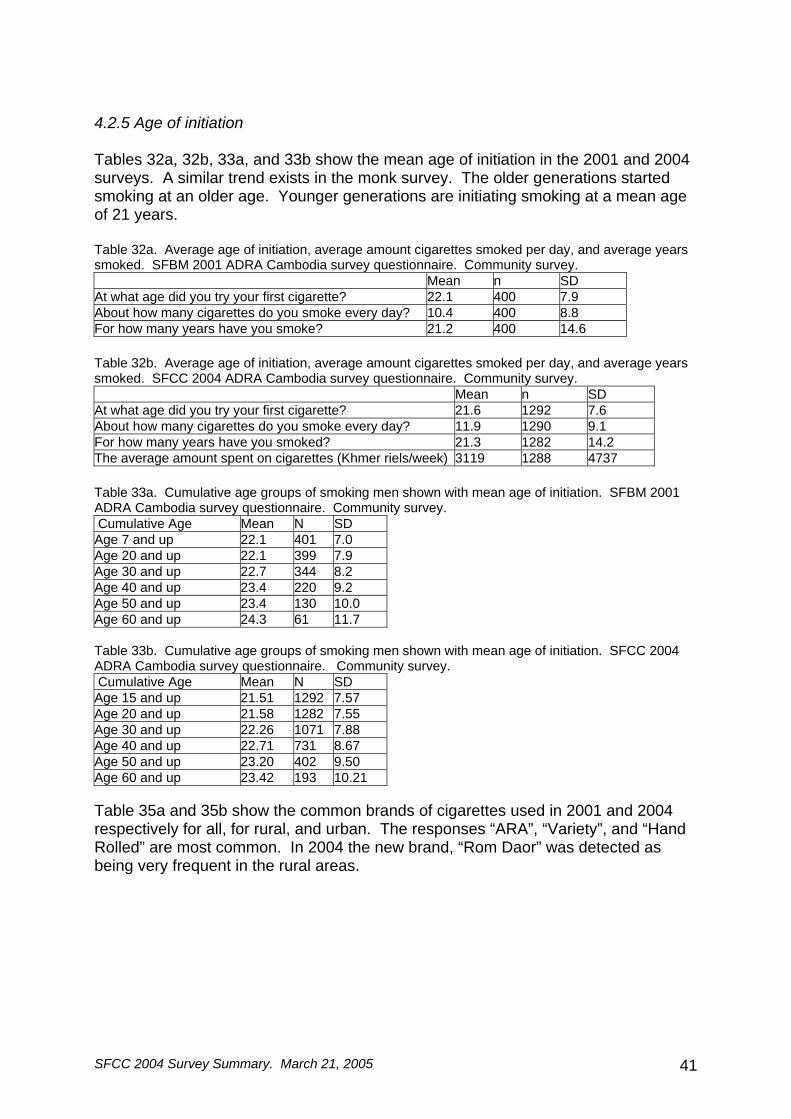
SFCC 2004 Survey Summary. March 21, 2005 41
4.2.5 Age of initiation Tables 32a, 32b, 33a, and 33b show the mean age of initiation in the 2001 and 2004 surveys. A similar trend exists in the monk survey. The older generations started smoking at an older age. Younger generations are initiating smoking at a mean age of 21 years. Table 32a. Average age of initiation, average amount cigarettes smoked per day, and average years smoked. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. Mean n SD At what age did you try your first cigarette? 22.1 400 7.9 About how many cigarettes do you smoke every day? 10.4 400 8.8 For how many years have you smoke? 21.2 400 14.6 Table 32b. Average age of initiation, average amount cigarettes smoked per day, and average years smoked. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Mean n SD At what age did you try your first cigarette? 21.6 1292 7.6 About how many cigarettes do you smoke every day? 11.9 1290 9.1 For how many years have you smoked? 21.3 1282 14.2 The average amount spent on cigarettes (Khmer riels/week) 3119 1288 4737 Table 33a. Cumulative age groups of smoking men shown with mean age of initiation. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. Cumulative Age Mean N SD Age 7 and up 22.1 401 7.0 Age 20 and up 22.1 399 7.9 Age 30 and up 22.7 344 8.2 Age 40 and up 23.4 220 9.2 Age 50 and up 23.4 130 10.0 Age 60 and up 24.3 61 11.7 Table 33b. Cumulative age groups of smoking men shown with mean age of initiation. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Cumulative Age Mean N SD Age 15 and up 21.51 1292 7.57 Age 20 and up 21.58 1282 7.55 Age 30 and up 22.26 1071 7.88 Age 40 and up 22.71 731 8.67 Age 50 and up 23.20 402 9.50 Age 60 and up 23.42 193 10.21 Table 35a and 35b show the common brands of cigarettes used in 2001 and 2004 respectively for all, for rural, and urban. The responses “ARA”, “Variety”, and “Hand Rolled” are most common. In 2004 the new brand, “Rom Daor” was detected as being very frequent in the rural areas.
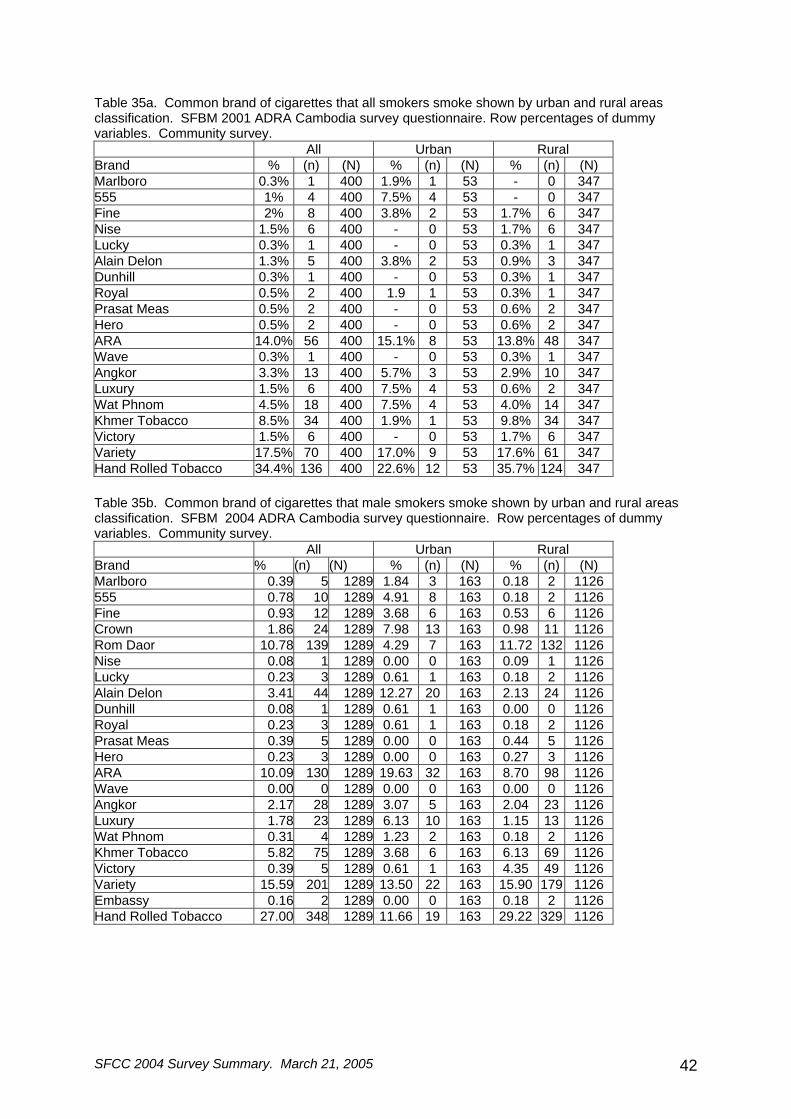
SFCC 2004 Survey Summary. March 21, 2005 42
Table 35a. Common brand of cigarettes that all smokers smoke shown by urban and rural areas classification. SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Community survey. All Urban Rural Brand % (n) (N) % (n) (N) % (n) (N) Marlboro 0.3% 1 400 1.9% 1 53 - 0 347 555 1% 4 400 7.5% 4 53 - 0 347 Fine 2% 8 400 3.8% 2 53 1.7% 6 347 Nise 1.5% 6 400 - 0 53 1.7% 6 347 Lucky 0.3% 1 400 - 0 53 0.3% 1 347 Alain Delon 1.3% 5 400 3.8% 2 53 0.9% 3 347 Dunhill 0.3% 1 400 - 0 53 0.3% 1 347 Royal 0.5% 2 400 1.9 1 53 0.3% 1 347 Prasat Meas 0.5% 2 400 - 0 53 0.6% 2 347 Hero 0.5% 2 400 - 0 53 0.6% 2 347 ARA 14.0% 56 400 15.1% 8 53 13.8% 48 347 Wave 0.3% 1 400 - 0 53 0.3% 1 347 Angkor 3.3% 13 400 5.7% 3 53 2.9% 10 347 Luxury 1.5% 6 400 7.5% 4 53 0.6% 2 347 Wat Phnom 4.5% 18 400 7.5% 4 53 4.0% 14 347 Khmer Tobacco 8.5% 34 400 1.9% 1 53 9.8% 34 347 Victory 1.5% 6 400 - 0 53 1.7% 6 347 Variety 17.5% 70 400 17.0% 9 53 17.6% 61 347 Hand Rolled Tobacco 34.4% 136 400 22.6% 12 53 35.7% 124 347 Table 35b. Common brand of cigarettes that male smokers smoke shown by urban and rural areas classification. SFBM 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Community survey. All Urban Rural Brand % (n) (N) % (n) (N) % (n) (N) Marlboro 0.39 5 1289 1.84 3 163 0.18 2 1126 555 0.78 10 1289 4.91 8 163 0.18 2 1126 Fine 0.93 12 1289 3.68 6 163 0.53 6 1126 Crown 1.86 24 1289 7.98 13 163 0.98 11 1126 Rom Daor 10.78 139 1289 4.29 7 163 11.72 132 1126 Nise 0.08 1 1289 0.00 0 163 0.09 1 1126 Lucky 0.23 3 1289 0.61 1 163 0.18 2 1126 Alain Delon 3.41 44 1289 12.27 20 163 2.13 24 1126 Dunhill 0.08 1 1289 0.61 1 163 0.00 0 1126 Royal 0.23 3 1289 0.61 1 163 0.18 2 1126 Prasat Meas 0.39 5 1289 0.00 0 163 0.44 5 1126 Hero 0.23 3 1289 0.00 0 163 0.27 3 1126 ARA 10.09 130 1289 19.63 32 163 8.70 98 1126 Wave 0.00 0 1289 0.00 0 163 0.00 0 1126 Angkor 2.17 28 1289 3.07 5 163 2.04 23 1126 Luxury 1.78 23 1289 6.13 10 163 1.15 13 1126 Wat Phnom 0.31 4 1289 1.23 2 163 0.18 2 1126 Khmer Tobacco 5.82 75 1289 3.68 6 163 6.13 69 1126 Victory 0.39 5 1289 0.61 1 163 4.35 49 1126 Variety 15.59 201 1289 13.50 22 163 15.90 179 1126 Embassy 0.16 2 1289 0.00 0 163 0.18 2 1126 Hand Rolled Tobacco 27.00 348 1289 11.66 19 163 29.22 329 1126
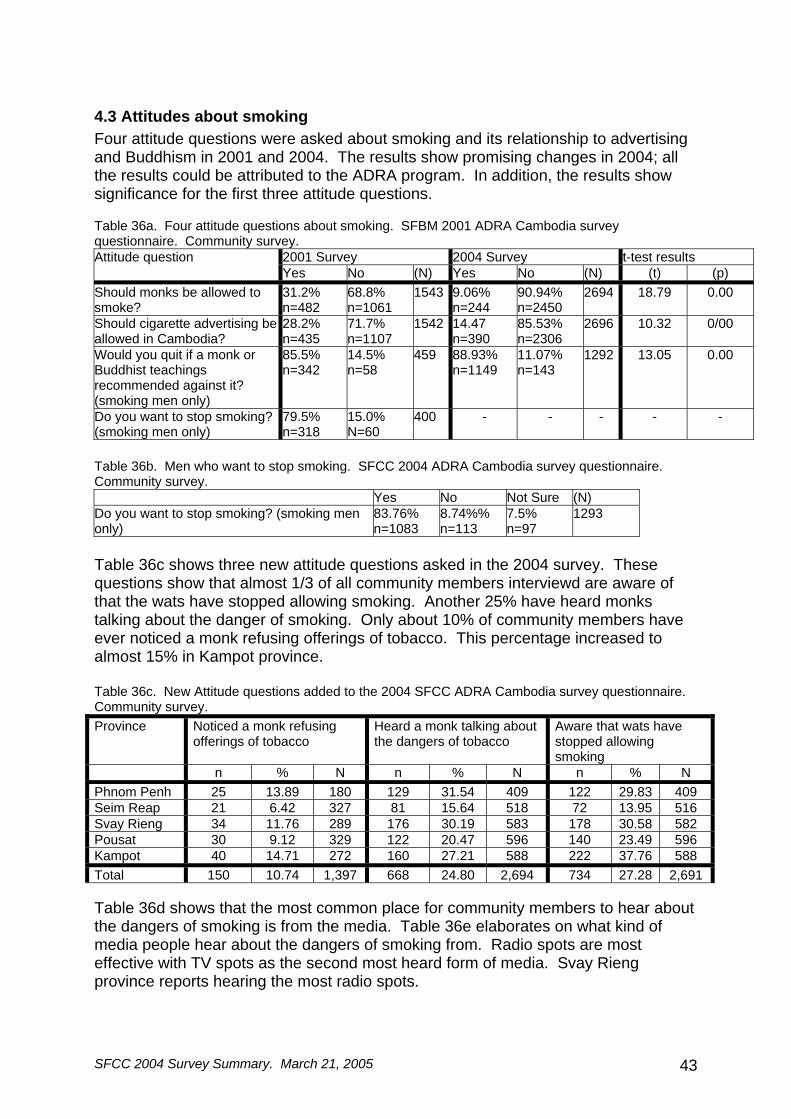
SFCC 2004 Survey Summary. March 21, 2005 43
4.3 Attitudes about smoking Four attitude questions were asked about smoking and its relationship to advertising and Buddhism in 2001 and 2004. The results show promising changes in 2004; all the results could be attributed to the ADRA program. In addition, the results show significance for the first three attitude questions. Table 36a. Four attitude questions about smoking. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey.
2001 Survey 2004 Survey t-test results Attitude question Yes No (N) Yes No (N) (t) (p)
Should monks be allowed to smoke?
31.2% n=482
68.8% n=1061
1543 9.06% n=244
90.94% n=2450
2694 18.79 0.00
Should cigarette advertising be allowed in Cambodia?
28.2% n=435
71.7% n=1107
1542 14.47 n=390
85.53% n=2306
2696 10.32 0/00
Would you quit if a monk or Buddhist teachings recommended against it? (smoking men only)
85.5% n=342
14.5% n=58
459 88.93% n=1149
11.07% n=143
1292 13.05 0.00
Do you want to stop smoking? (smoking men only)
79.5% n=318
15.0% N=60
400 - - - - -
Table 36b. Men who want to stop smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Yes No Not Sure (N) Do you want to stop smoking? (smoking men only)
83.76% n=1083
8.74%% n=113
7.5% n=97
1293
Table 36c shows three new attitude questions asked in the 2004 survey. These questions show that almost 1/3 of all community members interviewd are aware of that the wats have stopped allowing smoking. Another 25% have heard monks talking about the danger of smoking. Only about 10% of community members have ever noticed a monk refusing offerings of tobacco. This percentage increased to almost 15% in Kampot province. Table 36c. New Attitude questions added to the 2004 SFCC ADRA Cambodia survey questionnaire. Community survey. Province Noticed a monk refusing
offerings of tobacco Heard a monk talking about the dangers of tobacco
Aware that wats have stopped allowing smoking
n % N n % N n % N Phnom Penh 25 13.89 180 129 31.54 409 122 29.83 409 Seim Reap 21 6.42 327 81 15.64 518 72 13.95 516 Svay Rieng 34 11.76 289 176 30.19 583 178 30.58 582 Pousat 30 9.12 329 122 20.47 596 140 23.49 596 Kampot 40 14.71 272 160 27.21 588 222 37.76 588 Total 150 10.74 1,397 668 24.80 2,694 734 27.28 2,691 Table 36d shows that the most common place for community members to hear about the dangers of smoking is from the media. Table 36e elaborates on what kind of media people hear about the dangers of smoking from. Radio spots are most effective with TV spots as the second most heard form of media. Svay Rieng province reports hearing the most radio spots.
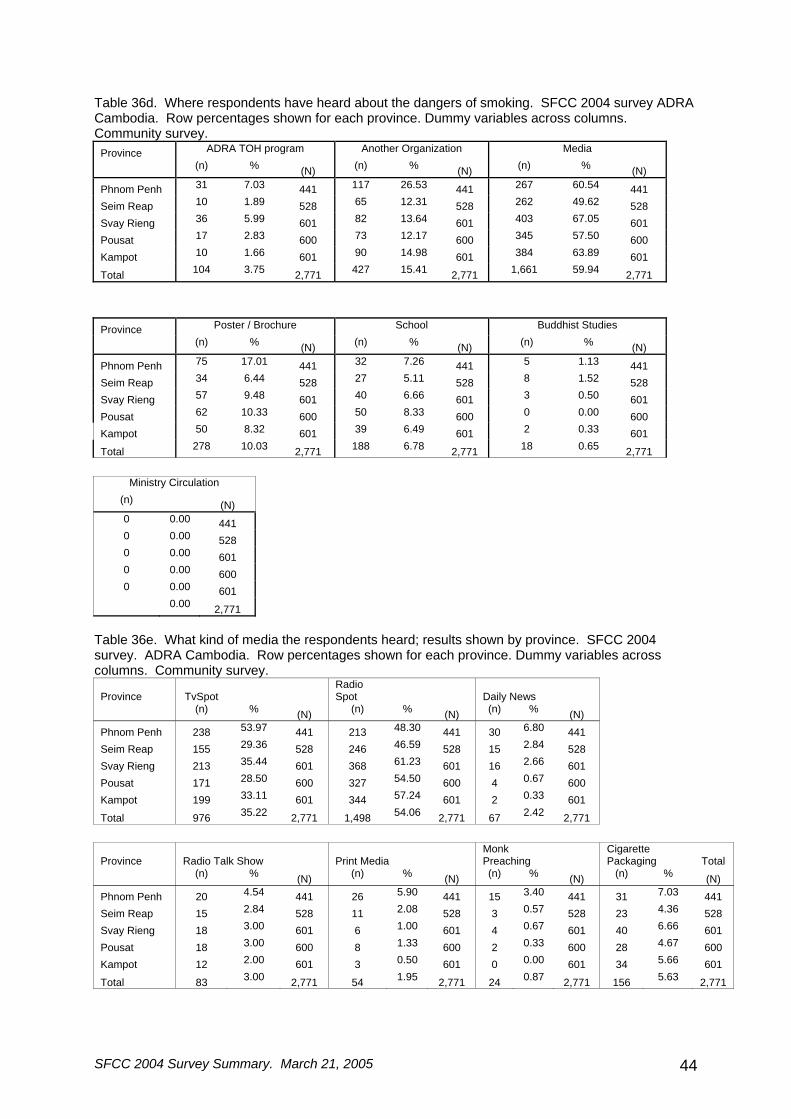
SFCC 2004 Survey Summary. March 21, 2005 44
Table 36d. Where respondents have heard about the dangers of smoking. SFCC 2004 survey ADRA Cambodia. Row percentages shown for each province. Dummy variables across columns. Community survey.
Province ADRA TOH program Another Organization Media
(n) % (N) (n) % (N) (n) % (N)
Phnom Penh 31 7.03 441 117 26.53 441 267 60.54 441 Seim Reap 10 1.89 528 65 12.31 528 262 49.62 528 Svay Rieng 36 5.99 601 82 13.64 601 403 67.05 601 Pousat 17 2.83 600 73 12.17 600 345 57.50 600 Kampot 10 1.66 601 90 14.98 601 384 63.89 601
Total 104 3.75 2,771 427 15.41 2,771 1,661 59.94 2,771
Province Poster / Brochure School Buddhist Studies
(n) % (N) (n) % (N) (n) % (N)
Phnom Penh 75 17.01 441 32 7.26 441 5 1.13 441 Seim Reap 34 6.44 528 27 5.11 528 8 1.52 528 Svay Rieng 57 9.48 601 40 6.66 601 3 0.50 601 Pousat 62 10.33 600 50 8.33 600 0 0.00 600 Kampot 50 8.32 601 39 6.49 601 2 0.33 601
Total 278 10.03 2,771 188 6.78 2,771 18 0.65 2,771
Ministry Circulation
(n) (N) 0 0.00 441 0 0.00 528 0 0.00 601 0 0.00 600 0 0.00 601 0.00 2,771
Table 36e. What kind of media the respondents heard; results shown by province. SFCC 2004 survey. ADRA Cambodia. Row percentages shown for each province. Dummy variables across columns. Community survey.
Province TvSpot Radio Spot Daily News
(n) % (N) (n) % (N) (n) % (N) Phnom Penh 238 53.97 441 213 48.30 441 30 6.80 441 Seim Reap 155 29.36 528 246 46.59 528 15 2.84 528 Svay Rieng 213 35.44 601 368 61.23 601 16 2.66 601 Pousat 171 28.50 600 327 54.50 600 4 0.67 600 Kampot 199 33.11 601 344 57.24 601 2 0.33 601
Total 976 35.22 2,771 1,498 54.06 2,771 67 2.42 2,771
Province Radio Talk Show Print Media Monk Preaching
Cigarette Packaging Total
(n) % (N) (n) % (N) (n) % (N) (n) % (N) Phnom Penh 20 4.54 441 26 5.90 441 15 3.40 441 31 7.03 441 Seim Reap 15 2.84 528 11 2.08 528 3 0.57 528 23 4.36 528 Svay Rieng 18 3.00 601 6 1.00 601 4 0.67 601 40 6.66 601 Pousat 18 3.00 600 8 1.33 600 2 0.33 600 28 4.67 600 Kampot 12 2.00 601 3 0.50 601 0 0.00 601 34 5.66 601
Total 83 3.00 2,771 54 1.95 2,771 24 0.87 2,771 156 5.63 2,771
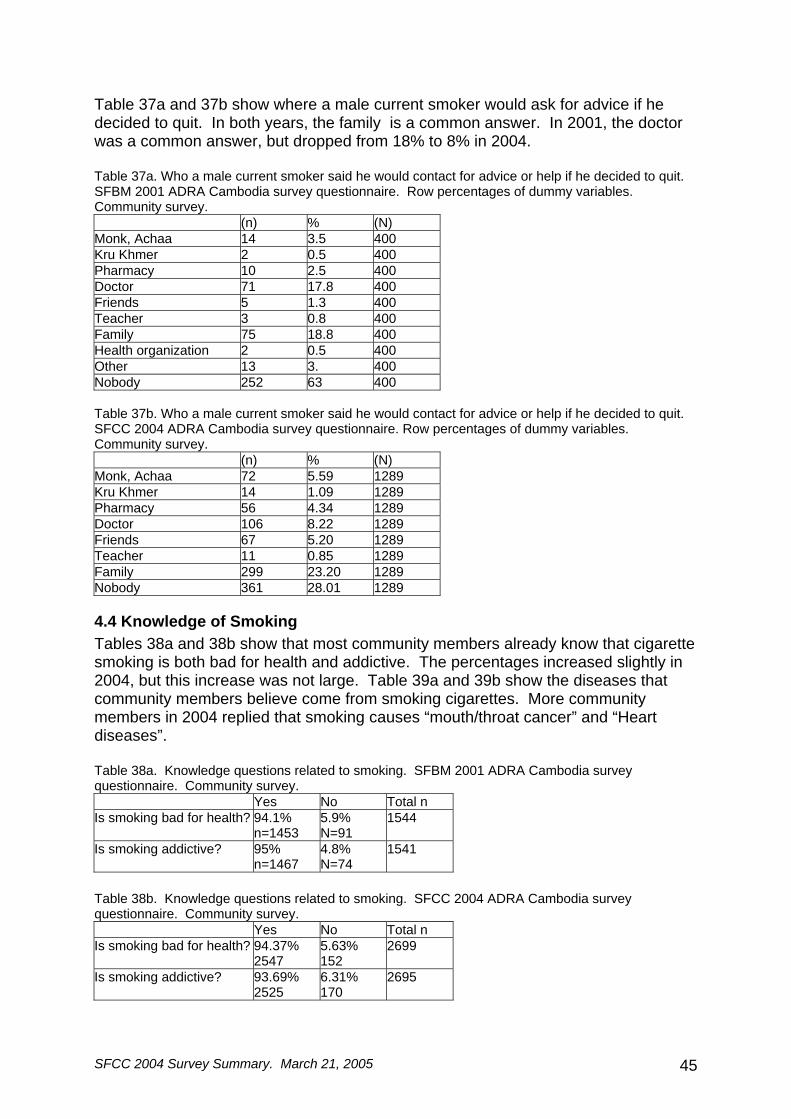
SFCC 2004 Survey Summary. March 21, 2005 45
Table 37a and 37b show where a male current smoker would ask for advice if he decided to quit. In both years, the family is a common answer. In 2001, the doctor was a common answer, but dropped from 18% to 8% in 2004. Table 37a. Who a male current smoker said he would contact for advice or help if he decided to quit. SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Community survey. (n) % (N) Monk, Achaa 14 3.5 400 Kru Khmer 2 0.5 400 Pharmacy 10 2.5 400 Doctor 71 17.8 400 Friends 5 1.3 400 Teacher 3 0.8 400 Family 75 18.8 400 Health organization 2 0.5 400 Other 13 3. 400 Nobody 252 63 400 Table 37b. Who a male current smoker said he would contact for advice or help if he decided to quit. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Community survey. (n) % (N) Monk, Achaa 72 5.59 1289 Kru Khmer 14 1.09 1289 Pharmacy 56 4.34 1289 Doctor 106 8.22 1289 Friends 67 5.20 1289 Teacher 11 0.85 1289 Family 299 23.20 1289 Nobody 361 28.01 1289
4.4 Knowledge of Smoking Tables 38a and 38b show that most community members already know that cigarette smoking is both bad for health and addictive. The percentages increased slightly in 2004, but this increase was not large. Table 39a and 39b show the diseases that community members believe come from smoking cigarettes. More community members in 2004 replied that smoking causes “mouth/throat cancer” and “Heart diseases”. Table 38a. Knowledge questions related to smoking. SFBM 2001 ADRA Cambodia survey questionnaire. Community survey. Yes No Total n Is smoking bad for health? 94.1%
n=1453 5.9% N=91
1544
Is smoking addictive? 95% n=1467
4.8% N=74
1541
Table 38b. Knowledge questions related to smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Community survey. Yes No Total n Is smoking bad for health? 94.37%
2547 5.63% 152
2699
Is smoking addictive? 93.69% 2525
6.31% 170
2695
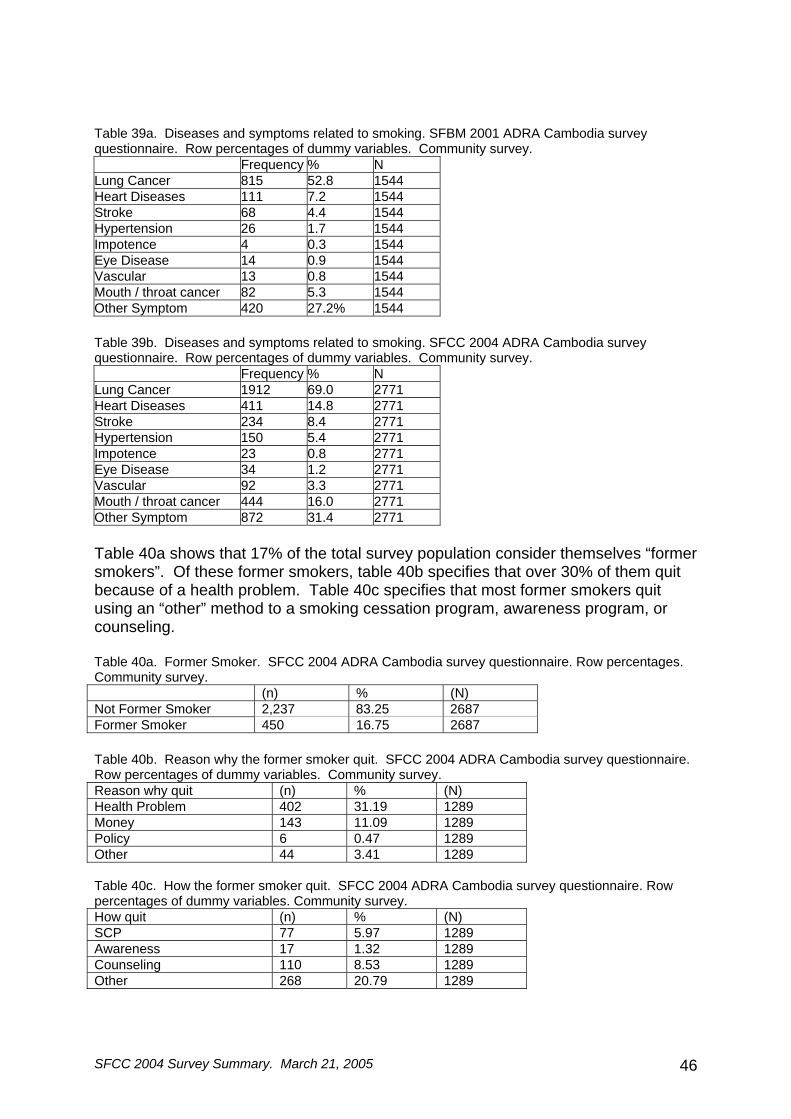
SFCC 2004 Survey Summary. March 21, 2005 46
Table 39a. Diseases and symptoms related to smoking. SFBM 2001 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Community survey. Frequency % N Lung Cancer 815 52.8 1544 Heart Diseases 111 7.2 1544 Stroke 68 4.4 1544 Hypertension 26 1.7 1544 Impotence 4 0.3 1544 Eye Disease 14 0.9 1544 Vascular 13 0.8 1544 Mouth / throat cancer 82 5.3 1544 Other Symptom 420 27.2% 1544 Table 39b. Diseases and symptoms related to smoking. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Community survey. Frequency % N Lung Cancer 1912 69.0 2771 Heart Diseases 411 14.8 2771 Stroke 234 8.4 2771 Hypertension 150 5.4 2771 Impotence 23 0.8 2771 Eye Disease 34 1.2 2771 Vascular 92 3.3 2771 Mouth / throat cancer 444 16.0 2771 Other Symptom 872 31.4 2771 Table 40a shows that 17% of the total survey population consider themselves “former smokers”. Of these former smokers, table 40b specifies that over 30% of them quit because of a health problem. Table 40c specifies that most former smokers quit using an “other” method to a smoking cessation program, awareness program, or counseling. Table 40a. Former Smoker. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages. Community survey. (n) % (N) Not Former Smoker 2,237 83.25 2687 Former Smoker 450 16.75 2687 Table 40b. Reason why the former smoker quit. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Community survey. Reason why quit (n) % (N) Health Problem 402 31.19 1289 Money 143 11.09 1289 Policy 6 0.47 1289 Other 44 3.41 1289 Table 40c. How the former smoker quit. SFCC 2004 ADRA Cambodia survey questionnaire. Row percentages of dummy variables. Community survey. How quit (n) % (N) SCP 77 5.97 1289 Awareness 17 1.32 1289 Counseling 110 8.53 1289 Other 268 20.79 1289

SFCC 2004 Survey Summary. March 21, 2005 47
5. Conclusion Most of the data in the results section of this report are self explanatory. Nonetheless, some comparisons between the two survey years and between the two survey populations need further explanation.
The prevalence of Buddhist monks who smoke is much lower than the prevalence of male community members who smoke in both 2001 and 2004. It is expected that these two prevalence rates should be the same; Buddhist Monks are also male community members. None of the many available justifications for this difference were discussed or explored in this report. The obvious explanation for this difference is that Buddhist Monks have to live a much regimented life. When they are ordained as a monk, they agree to live by a group of precepts; one of which specifies that they must live without addiction. This question needs to be further explored through qualitative and other research methods.
Another difference between the Monk survey and the community survey is that
no detectable difference in prevalence exists between rural and urban monks. Urban monks are reported to smoke just as much as rural monks do. This is much different from the community survey where many more rural men smoke in the rural areas than the urban areas. An explanation of this is that monks from the urban area may travel to the rural areas and vice-versa. This phenomena also needs further explanation.
In 2001, attitudes towards Buddhist monks being allowed to smoke were much lower in the monk population than the community population. Some 31.2% of community members in 2001 said that monks should be allowed to smoke, while only 14.3% of monks said this (Table 36a and 17a). In 2004 the difference between monks and community members dropped; some 9.0% of community men said that monks should be allowed to smoke, while 4.3% monks said this. Attitudes for other variables in Table 36a and 17a are similar; Buddhist monks show more interest in quitting smoking and helping others quit.
These results are promising; Buddhist monks are still more amenable to an
intervention than community members. An observation made during the 2001 survey held true for the 2004 survey. Buddhist monks were much more cooperative towards any kind of formal meeting than the community members. When the survey teams would travel to the pagoda, they were usually received well. When they traveled to communities, village chiefs were less predictable. Any organized meeting that the SFBM project can do with Buddhist monks will be received well.
The differences in the knowledge section of this report were interesting. It
appears that community members now have many more “ideas” about diseases related to smoking and “sources of information about the dangers” of smoking. Figure A in appendix 1 shows many different results for diseases related to smoking. Most community members now realize that smoking is bad for health and has some kind of undesirable health effect. The type information that villagers are exposed to about smoking is also increasing. This means that more villagers are getting more information about smoking. This may be due to increased marketing of tobacco to

SFCC 2004 Survey Summary. March 21, 2005 48
villagers or more readily available tobacco control information for villagers. More research on media needs to be conducted to further quantify these results.
Overall, this survey is successful in presenting an accurate prevalence figure for monks and showing very significant changes in prevalence, knowledge, attitudes, and practices between 2001 and 2004. The data presented in this report was usually analyzed to only the level of frequencies, percentages, and possibly t-tests. Much more analysis is possible and encouraged; please contact the authors of this report for any additional desired analysis. 6. Acknowledgments Task Personnel Analyze survey: Ryan Sinclair, Yel Daravuth, Ung Sophal Data entry and cleaning: Ung Sophal Training of Surveyors: Ryan Sinclair, Yel Daravuth, Mom Kong Survey organization and data collection:
Yel Daravuth, Ryan Sinclair, Mom Kong
Survey supervisors: Chum Kamrong, Som Yen, Ros Ravann, ,
Yel Daravuth, Mom Kong Survey design and field-test: Greg Hallen, Yel Daravuth, Ryan Sinclair
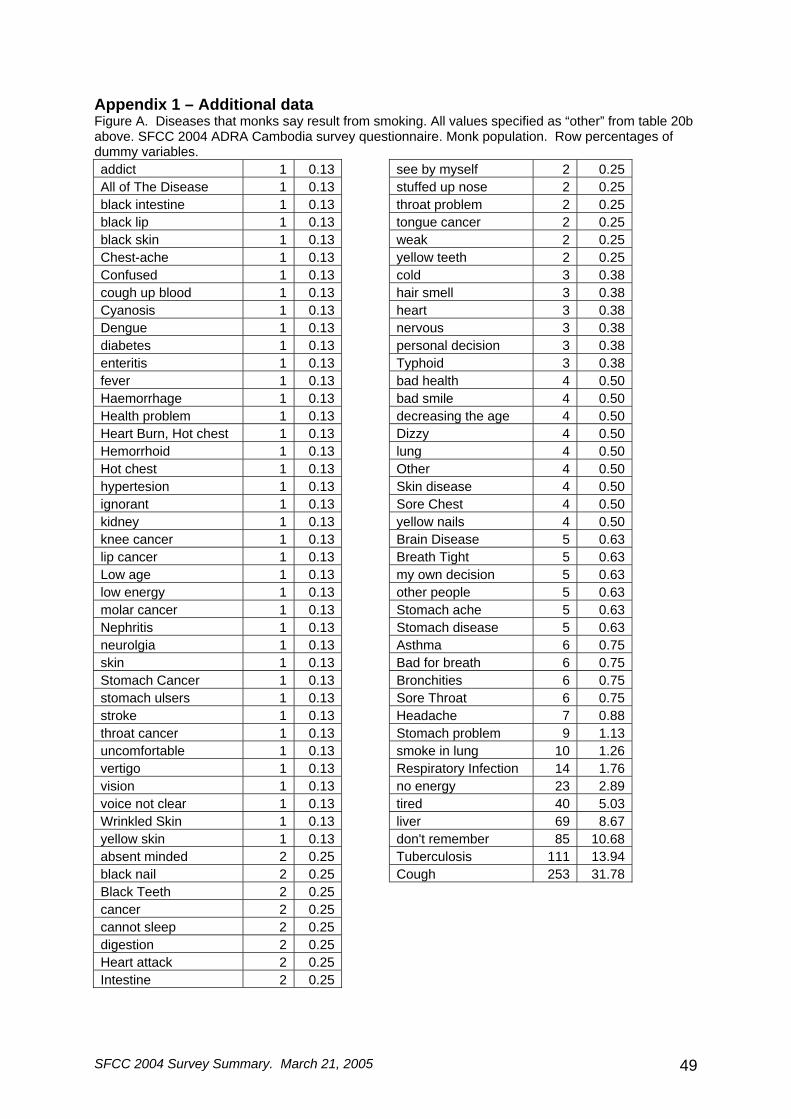
SFCC 2004 Survey Summary. March 21, 2005 49
Appendix 1 – Additional data Figure A. Diseases that monks say result from smoking. All values specified as “other” from table 20b above. SFCC 2004 ADRA Cambodia survey questionnaire. Monk population. Row percentages of dummy variables. addict 1 0.13 see by myself 2 0.25 All of The Disease 1 0.13 stuffed up nose 2 0.25 black intestine 1 0.13 throat problem 2 0.25 black lip 1 0.13 tongue cancer 2 0.25 black skin 1 0.13 weak 2 0.25 Chest-ache 1 0.13 yellow teeth 2 0.25 Confused 1 0.13 cold 3 0.38 cough up blood 1 0.13 hair smell 3 0.38 Cyanosis 1 0.13 heart 3 0.38 Dengue 1 0.13 nervous 3 0.38 diabetes 1 0.13 personal decision 3 0.38 enteritis 1 0.13 Typhoid 3 0.38 fever 1 0.13 bad health 4 0.50 Haemorrhage 1 0.13 bad smile 4 0.50 Health problem 1 0.13 decreasing the age 4 0.50 Heart Burn, Hot chest 1 0.13 Dizzy 4 0.50 Hemorrhoid 1 0.13 lung 4 0.50 Hot chest 1 0.13 Other 4 0.50 hypertesion 1 0.13 Skin disease 4 0.50 ignorant 1 0.13 Sore Chest 4 0.50 kidney 1 0.13 yellow nails 4 0.50 knee cancer 1 0.13 Brain Disease 5 0.63 lip cancer 1 0.13 Breath Tight 5 0.63 Low age 1 0.13 my own decision 5 0.63 low energy 1 0.13 other people 5 0.63 molar cancer 1 0.13 Stomach ache 5 0.63 Nephritis 1 0.13 Stomach disease 5 0.63 neurolgia 1 0.13 Asthma 6 0.75 skin 1 0.13 Bad for breath 6 0.75 Stomach Cancer 1 0.13 Bronchities 6 0.75 stomach ulsers 1 0.13 Sore Throat 6 0.75 stroke 1 0.13 Headache 7 0.88 throat cancer 1 0.13 Stomach problem 9 1.13 uncomfortable 1 0.13 smoke in lung 10 1.26 vertigo 1 0.13 Respiratory Infection 14 1.76 vision 1 0.13 no energy 23 2.89 voice not clear 1 0.13 tired 40 5.03 Wrinkled Skin 1 0.13 liver 69 8.67 yellow skin 1 0.13 don't remember 85 10.68 absent minded 2 0.25 Tuberculosis 111 13.94 black nail 2 0.25 Cough 253 31.78 Black Teeth 2 0.25 cancer 2 0.25cannot sleep 2 0.25digestion 2 0.25Heart attack 2 0.25Intestine 2 0.25
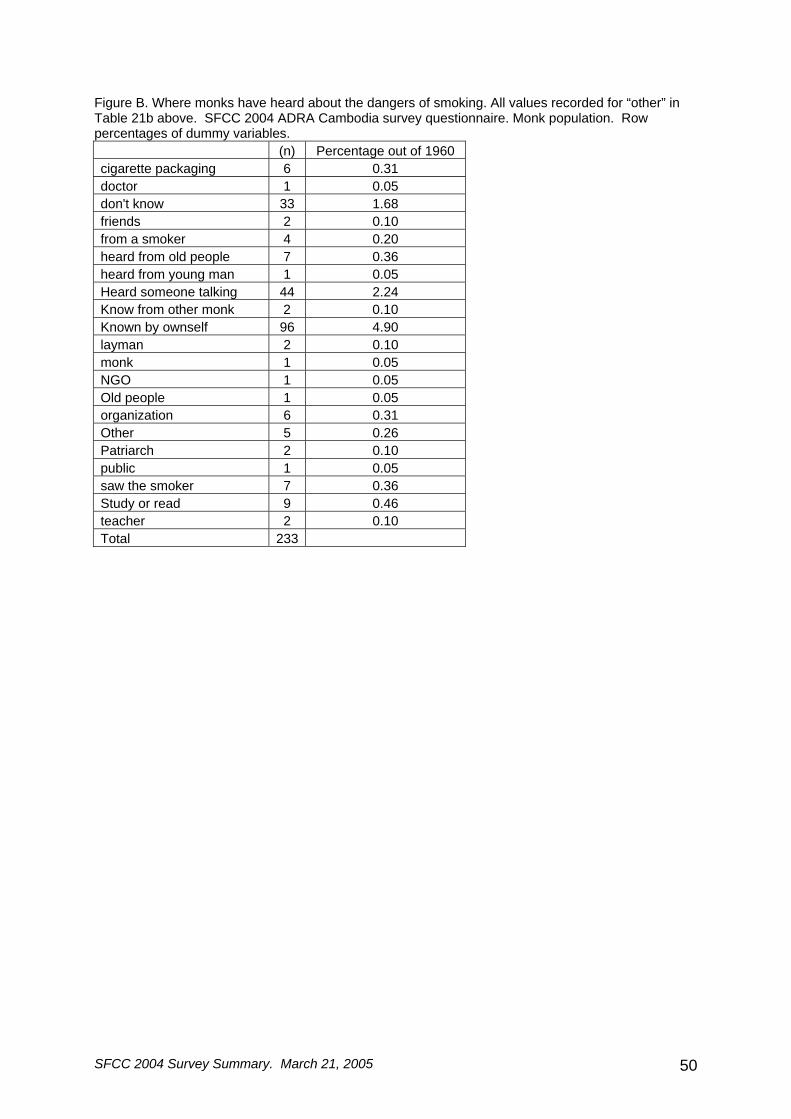
SFCC 2004 Survey Summary. March 21, 2005 50
Figure B. Where monks have heard about the dangers of smoking. All values recorded for “other” in Table 21b above. SFCC 2004 ADRA Cambodia survey questionnaire. Monk population. Row percentages of dummy variables. (n) Percentage out of 1960 cigarette packaging 6 0.31 doctor 1 0.05 don't know 33 1.68 friends 2 0.10 from a smoker 4 0.20 heard from old people 7 0.36 heard from young man 1 0.05 Heard someone talking 44 2.24 Know from other monk 2 0.10 Known by ownself 96 4.90 layman 2 0.10 monk 1 0.05 NGO 1 0.05 Old people 1 0.05 organization 6 0.31 Other 5 0.26 Patriarch 2 0.10 public 1 0.05 saw the smoker 7 0.36 Study or read 9 0.46 teacher 2 0.10 Total 233
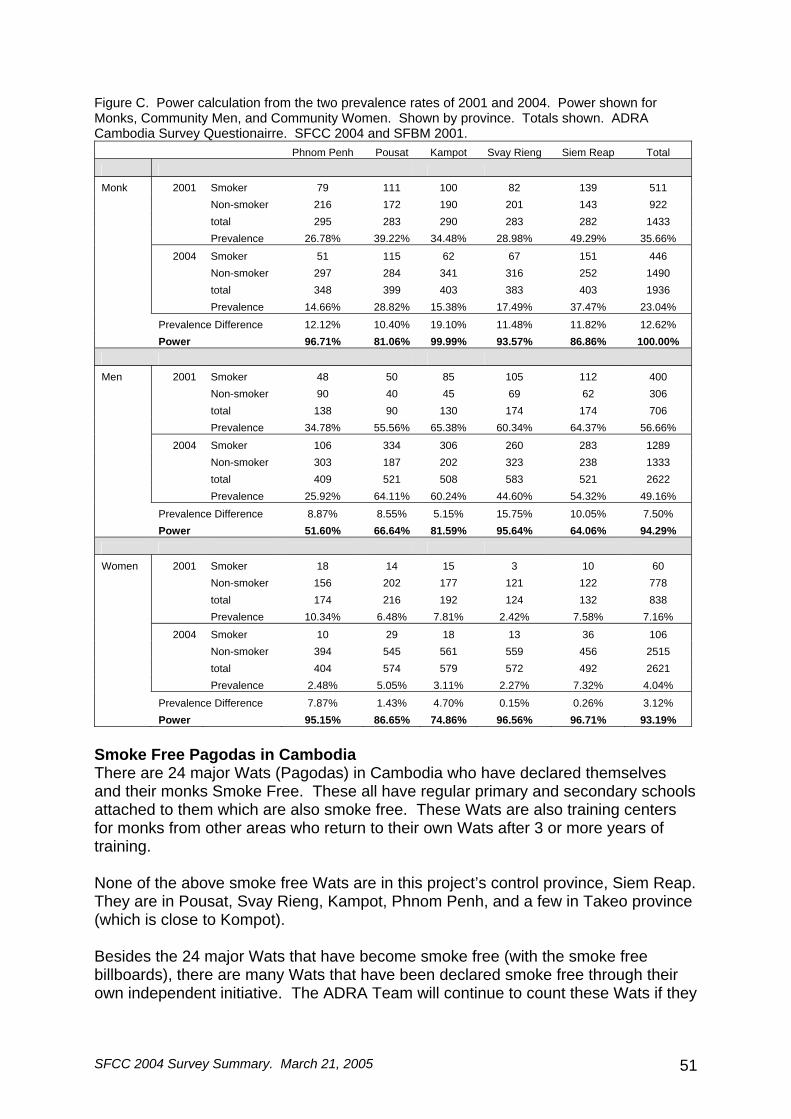
SFCC 2004 Survey Summary. March 21, 2005 51
Figure C. Power calculation from the two prevalence rates of 2001 and 2004. Power shown for Monks, Community Men, and Community Women. Shown by province. Totals shown. ADRA Cambodia Survey Questionairre. SFCC 2004 and SFBM 2001.
Phnom Penh Pousat Kampot Svay Rieng Siem Reap Total Monk 2001 Smoker 79 111 100 82 139 511 Non-smoker 216 172 190 201 143 922 total 295 283 290 283 282 1433 Prevalence 26.78% 39.22% 34.48% 28.98% 49.29% 35.66%
2004 Smoker 51 115 62 67 151 446 Non-smoker 297 284 341 316 252 1490 total 348 399 403 383 403 1936 Prevalence 14.66% 28.82% 15.38% 17.49% 37.47% 23.04% Prevalence Difference 12.12% 10.40% 19.10% 11.48% 11.82% 12.62% Power 96.71% 81.06% 99.99% 93.57% 86.86% 100.00% Men 2001 Smoker 48 50 85 105 112 400 Non-smoker 90 40 45 69 62 306 total 138 90 130 174 174 706 Prevalence 34.78% 55.56% 65.38% 60.34% 64.37% 56.66%
2004 Smoker 106 334 306 260 283 1289 Non-smoker 303 187 202 323 238 1333 total 409 521 508 583 521 2622 Prevalence 25.92% 64.11% 60.24% 44.60% 54.32% 49.16% Prevalence Difference 8.87% 8.55% 5.15% 15.75% 10.05% 7.50% Power 51.60% 66.64% 81.59% 95.64% 64.06% 94.29% Women 2001 Smoker 18 14 15 3 10 60 Non-smoker 156 202 177 121 122 778 total 174 216 192 124 132 838 Prevalence 10.34% 6.48% 7.81% 2.42% 7.58% 7.16%
2004 Smoker 10 29 18 13 36 106 Non-smoker 394 545 561 559 456 2515 total 404 574 579 572 492 2621 Prevalence 2.48% 5.05% 3.11% 2.27% 7.32% 4.04%
Prevalence Difference 7.87% 1.43% 4.70% 0.15% 0.26% 3.12% Power 95.15% 86.65% 74.86% 96.56% 96.71% 93.19%
Smoke Free Pagodas in Cambodia There are 24 major Wats (Pagodas) in Cambodia who have declared themselves and their monks Smoke Free. These all have regular primary and secondary schools attached to them which are also smoke free. These Wats are also training centers for monks from other areas who return to their own Wats after 3 or more years of training. None of the above smoke free Wats are in this project’s control province, Siem Reap. They are in Pousat, Svay Rieng, Kampot, Phnom Penh, and a few in Takeo province (which is close to Kompot). Besides the 24 major Wats that have become smoke free (with the smoke free billboards), there are many Wats that have been declared smoke free through their own independent initiative. The ADRA Team will continue to count these Wats if they

SFCC 2004 Survey Summary. March 21, 2005 52
have a written smoke-free policy enforced, which is agreed to by the Wat committee including the chief monk. The policy specifies that the grounds of the Wat are a no-smoking zone for monks and the public, that the monks will refuse offerings of tobacco and that monks will be active in encouraging and supporting smoke free lives among the community. ADRA PROGRAMS 2001 – 2004 Figure D presents a summary of all ADRA Cambodia anti-tobacco programs conducted from 2001 – 2004. The table presents all information by province in an attempt to show that Siem Reap province was used as the control province for the study. The programs that ADRA conducted are explained below. Figure D. Summary of TOT, SCP, and Awareness programs conducted in Cambodia by ADRA. SFCC 2004 and SFBM 2001 survey questionnaire. ADRA Cambodia.
2001 2002 TOT SCP Awareness Quit Counseling TOT SCP Awareness Quit Counsel
Phnom Penh 8 7 1 9 13 1
Pousat 2
Kampot 1 3 2 30 2 2
Svay Rieng
Siem Reap
Takeo† 10 1 2 8 2 2 Kompong
Speu* 1 1 1
Kandal* 1 Kompong
Cham* 4
TOTAL 1 19 12 2 3 55 17 2
2003 2004 TOT SCP Awareness Quit Counseling TOT SCP Awareness Quit Counsel
Phnom Penh 70 4 1 2 11 1
Pousat 2 25 4 1 8 2
Kampot 22 4 4
Svay Rieng 1 2 8 2 1
Siem Reap Kompong
Cham* 2
Kompong Speu*
4 2
Preah Vihear* 2
Takeo* 2 2
Battambang* 1 1
TOTAL 2 127 13 3 2 26 15 3
† Only Kompot, Svay Rieng, Phnom Penh, Siem Reap, and Pousat provinces are included in the SFCC/SFBM survey questionnaire study.
SFCC 2004 Survey Summary. March 21, 2005 53
TOT The ADRA Training of Trainers (TOT) program uses the “seven steps of freedom” program adapted from the Seventh Day Aventist Church’s “QUIT” program used in Austrailia. This program booklet was translated and adapted to Khmer culture, then reviewed by members of key ministries. A ten day intensive workshop was held where the booklet was criticized and adopted to the Cambodian situation. The intensive workshop decided that a 10 day program is suitable for a training of trainers (TOT) program.
In the TOT program, participants learn the method on how to get people to quit with the book, how to prepare a lesson plan, and how to evaluate the activity of the course. In the first three days, participants learn how to be a facilitator, how to communicate, how to get people to go to the program, and how to evaluate the program. During the next three days, participants learn the techniques of the “seven steps of freedom”. During the last 2 days the participants practice in the class by preparing a lesson plan and presenting a smoking cessation session. After the TOT program finishes, each participant will need to conduct one SCP program for a certificate. SCP The Smoking Cessation program is conducted by individuals who have been trained in the TOT program. The instructor typically goes to their wat and asks for all smokers want to quit, to attend a SCP program. They typically get 15-20 participants for each class.
The SCP class lasts 5 days to cover the nicotine withdrawal syndrome which lasts 3 days. Withdrawal symptoms are very intense and the SCP trainer can help the students through their withdrawal symptoms. If the SCP trainer can stay with them, the chance for relapse is low. The SCP instructor will monitor after 1 month, 3 months, 6 months, 9 months, and 1 year. Only after one month they will declare that participants of the program have quit. It is all based on self-reported quit rates. AWARENESS The awareness programs are meant to educate a large group people about the danger of smoking. The programs last three hours and present the following topics: the harmful chemicals in cigarettes, danger of cigarettes, Second Hand Smoke, economic cost to family and country, and an over view of the global tobacco problem. The programs advocate participants to quit smoking and invite participants to attend a stop smoking class. QUIT COUNCELING The quit counselor training sessions are a three day event. The sessions invite 25 participants to attend the 3-day training. The training sessions prepare individuals how they can help a smoker quit. They are trained in how to give advice to quit smoking without the use of willpower. They are taught in three steps:
1. Ask smoker if they want to quit 2. Assist all smokers to quit and encourage them to set a quit date
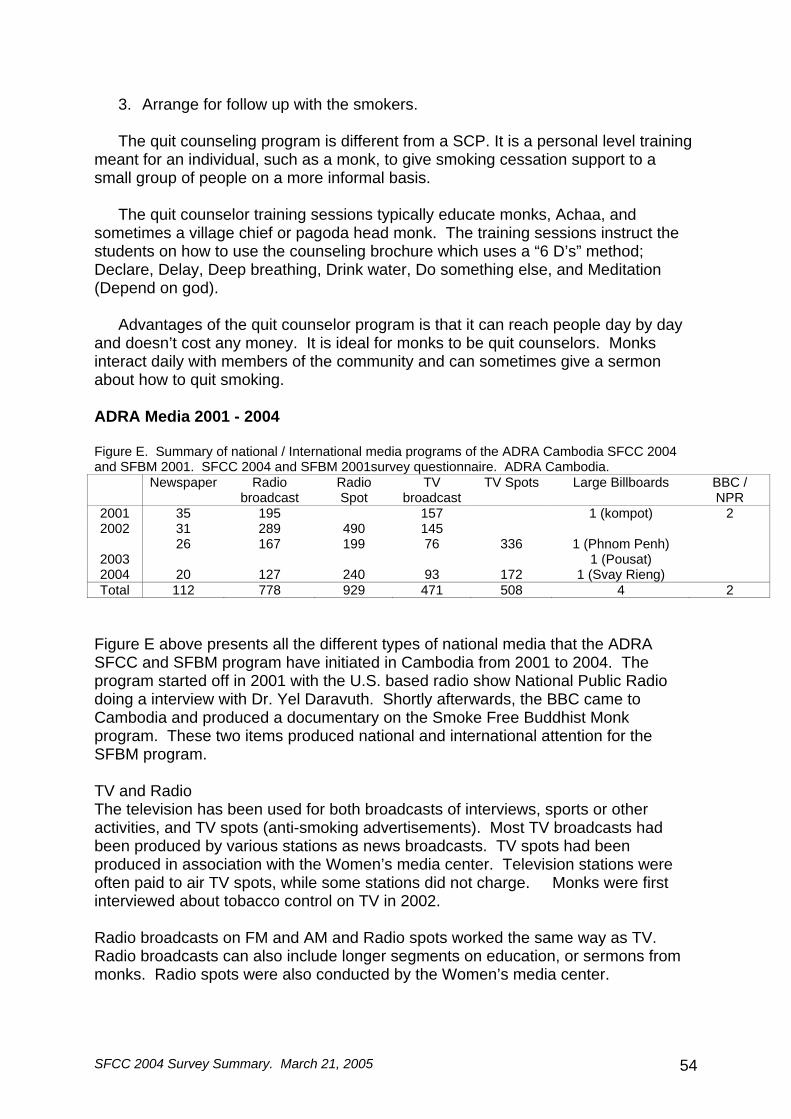
SFCC 2004 Survey Summary. March 21, 2005 54
3. Arrange for follow up with the smokers.
The quit counseling program is different from a SCP. It is a personal level training meant for an individual, such as a monk, to give smoking cessation support to a small group of people on a more informal basis.
The quit counselor training sessions typically educate monks, Achaa, and sometimes a village chief or pagoda head monk. The training sessions instruct the students on how to use the counseling brochure which uses a “6 D’s” method; Declare, Delay, Deep breathing, Drink water, Do something else, and Meditation (Depend on god).
Advantages of the quit counselor program is that it can reach people day by day and doesn’t cost any money. It is ideal for monks to be quit counselors. Monks interact daily with members of the community and can sometimes give a sermon about how to quit smoking. ADRA Media 2001 - 2004 Figure E. Summary of national / International media programs of the ADRA Cambodia SFCC 2004 and SFBM 2001. SFCC 2004 and SFBM 2001survey questionnaire. ADRA Cambodia. Newspaper Radio
broadcast Radio Spot
TV broadcast
TV Spots Large Billboards BBC / NPR
2001 35 195 157 1 (kompot) 2 2002 31 289 490 145
2003 26 167 199 76 336 1 (Phnom Penh)
1 (Pousat)
2004 20 127 240 93 172 1 (Svay Rieng) Total 112 778 929 471 508 4 2
Figure E above presents all the different types of national media that the ADRA SFCC and SFBM program have initiated in Cambodia from 2001 to 2004. The program started off in 2001 with the U.S. based radio show National Public Radio doing a interview with Dr. Yel Daravuth. Shortly afterwards, the BBC came to Cambodia and produced a documentary on the Smoke Free Buddhist Monk program. These two items produced national and international attention for the SFBM program. TV and Radio The television has been used for both broadcasts of interviews, sports or other activities, and TV spots (anti-smoking advertisements). Most TV broadcasts had been produced by various stations as news broadcasts. TV spots had been produced in association with the Women’s media center. Television stations were often paid to air TV spots, while some stations did not charge. Monks were first interviewed about tobacco control on TV in 2002. Radio broadcasts on FM and AM and Radio spots worked the same way as TV. Radio broadcasts can also include longer segments on education, or sermons from monks. Radio spots were also conducted by the Women’s media center.

SFCC 2004 Survey Summary. March 21, 2005 55
IEC printing Figure F below shows all of the IEC materials that have been produced by the ADRA SFCC and SFBM projects. The project is integrated with other TOH projects which also print stickers, shirts, pamphlets, brochures, and other items. All project IEC material is integrated together and shared. The numbers shown in the table below represent the amount of posters that ADRA staff has posted themselves in the actual provincial pagodas. All other posters, brochures, and books were distributed through the Ministries. Figure F. IEC materials produced by the SFCC 2001 or SFBM 2004 programs. The numbers in the table indicate the amount of posters that were posted by the ADRA staff themselves in Pagodas or other provincial locations. SFCC 2004 and SFBM 2001survey questionnaire. ADRA Cambodia. Year 2001 2002 2003 2004 Media Posters Posters Posters Quit
Counselor Book
Quit Counselor Brochure
Posters
Pousat 84 84 Pp 89 Kompot 160 174 174 Takeo 7 Svay Rieng 150 2500 6000 4500 2000 10000 5500

SFCC 2004 Survey Summary. March 21, 2005 56
Appendix 2 – Methods Excerpt Previous ADRA Report: Methods for Quantitative study for Smoke Free Buddhist Monk (SFBM) project, 2001. 2. Methods 2.1 The survey instrument Two survey forms were used for the community and the monk populations (Appendix 4). The two survey forms had similar questions, but collect some different information about Buddhism and smoking. In general, the two surveys assessed knowledge of smoking, practice of smoking, and beliefs about smoking. Questions for the survey were developed from WHO standard tobacco questions13, from the ADRA team, and from other consultants who have worked with ADRA since the inception of the ADRA tobacco program in 1995‡. The community survey is the end product of eight years of tobacco surveys completed in Cambodia and other areas. Many questions for the Buddhist Monk survey were modified from Marshall Smith's 1995 Buddhist monk14 survey. 2.2 Location of survey The survey was conducted in four provinces and one municipality: Phnom Penh, Pursat, Kampot, Svay Rieng, and Siem Reap. The decision to include these provinces was made during a research planning workshop which included from the Ministry of Health staff, ADRA, many other Cambodian NGOs, internal expatriate consultants, and external research consultants. The decision was made because of generalizability and distribution of the population in these provinces and the fact that ADRA already has projects in some of these provinces. These provinces (see figure 1) together represent a good cross section of Cambodian demographics because they include major urban areas, major rural areas, Vietnam and Thailand border areas, fishing communities, and rice farmers. Figure 1 also shows the distribution of villages and in Cambodia. This figure shows that the provinces selected for the survey (outlined in Black) are a good representative sample of the major population areas of Cambodia. During the survey, the supervisor noticed that Khmer and Vietnamese ethnicities were being sampled.
‡ Marshell Smith, Kaleinani Lau, Greg Hallen, Collin Ratford, WHO book.
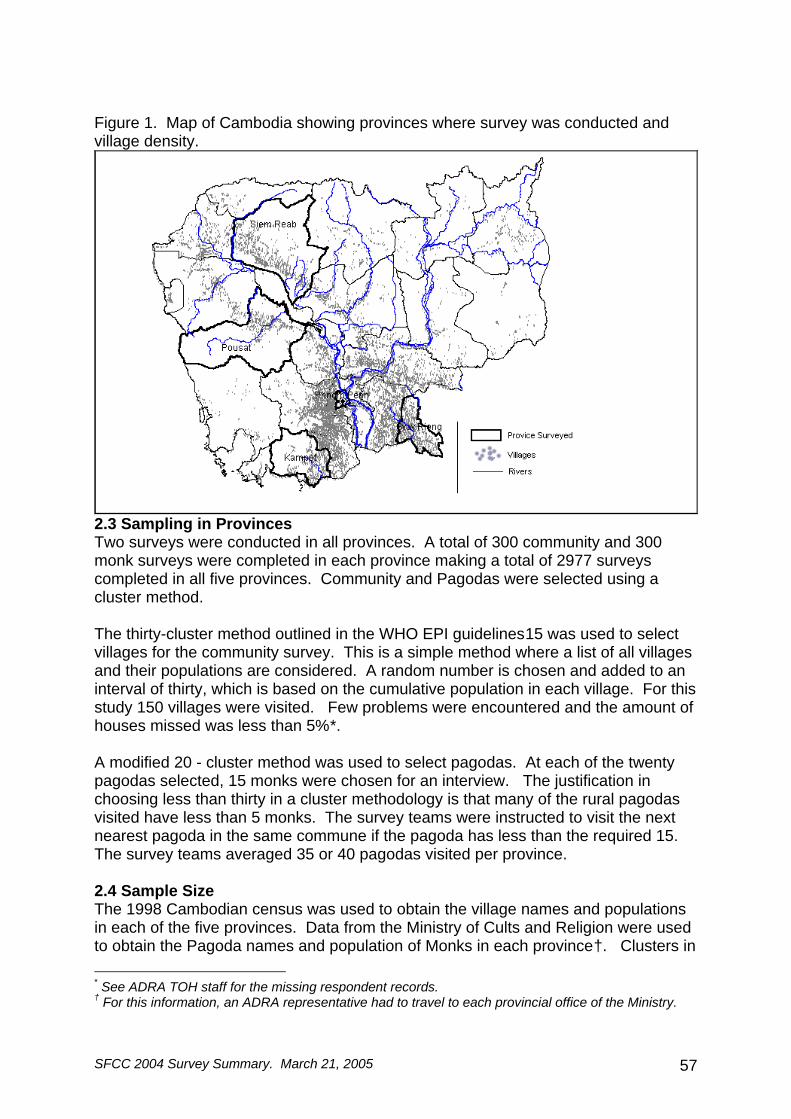
SFCC 2004 Survey Summary. March 21, 2005 57
Figure 1. Map of Cambodia showing provinces where survey was conducted and village density.
2.3 Sampling in Provinces Two surveys were conducted in all provinces. A total of 300 community and 300 monk surveys were completed in each province making a total of 2977 surveys completed in all five provinces. Community and Pagodas were selected using a cluster method. The thirty-cluster method outlined in the WHO EPI guidelines15 was used to select villages for the community survey. This is a simple method where a list of all villages and their populations are considered. A random number is chosen and added to an interval of thirty, which is based on the cumulative population in each village. For this study 150 villages were visited. Few problems were encountered and the amount of houses missed was less than 5%*. A modified 20 - cluster method was used to select pagodas. At each of the twenty pagodas selected, 15 monks were chosen for an interview. The justification in choosing less than thirty in a cluster methodology is that many of the rural pagodas visited have less than 5 monks. The survey teams were instructed to visit the next nearest pagoda in the same commune if the pagoda has less than the required 15. The survey teams averaged 35 or 40 pagodas visited per province. 2.4 Sample Size The 1998 Cambodian census was used to obtain the village names and populations in each of the five provinces. Data from the Ministry of Cults and Religion were used to obtain the Pagoda names and population of Monks in each province†. Clusters in * See ADRA TOH staff for the missing respondent records. † For this information, an ADRA representative had to travel to each provincial office of the Ministry.

SFCC 2004 Survey Summary. March 21, 2005 58
in each province were generated from this data. One village was considered a cluster, while one pagoda was sometimes considered only part of a cluster because it would have less than 15 monks*. The sample size for this study was calculated using the following formula: n=z²pq/d² For Village Men, p = Estimated prevalence of men's cigarette smoking = 60 n = 184 For village women, p = Estimated prevalence of women's cigarette smoking = 8.5%. n = 119.51 For Monks p = Estimated prevalence of monk's cigarette smoking = 40%. n=184 This makes the total recommended sample size for the community survey 303 (184 men + 119 women) while the monk survey should be at 184 (for 40% prevalence). To expand to the 5 provinces, this survey conducted 300 community and 300 monk surveys in each province†. For the five provinces together, 3000 surveys are more than enough for the Buddhist monks. 2.5 Survey Staff Surveyors were recruited from a pool of surveyors that have been used in previous tobacco surveys. Each group of five surveyors had a survey team supervisor. Both surveyors and supervisors were instructed in how to conduct a survey. They were trained for three days in May of 2001. The training began by discussing each question and making sure that each surveyor understands each question. The surveyors were reminded to properly introduce themselves, read every question, not to read the answers or interpret the questions, and other practical cluster survey training that is covered in appendix 6. The surveyors practiced with each other, and then they field-tested their survey skills and pre-tested the survey in a nearby community and Pagoda. After the pre-test, the survey instrument was modified. Some questions were deleted and some were changed. The survey supervisors were put in charge of each group of 5 surveyors. The supervisor's task was to lead the group to the village, ask permission from the village or pagoda chief, to select which houses or monks to interview (based on the methods described below), and to review the survey sheets for errors after the surveyors complete them. The supervisors were ADRA staff and worked very hard to complete the tasks assigned to them. Appendix 5 discusses some of the hardships and special circumstances that the survey supervisors had to deal with. * See the "sampling in Pagoda" section 2.3. † This sample size was generated for the prevalence question of "Are you a current smoker?" (appendix 3). All other behavior and practice questions assume the above sample size.

SFCC 2004 Survey Summary. March 21, 2005 59
A project manager and the expatriate advisor traveled to the provinces with the surveyors to ensure adherence to the strict random cluster sampling method. They would go with a different team every day to ensure the random method was being followed very closely. Picture2a. Expatriate supervisor with surveyors and motorbikes crossing a river.
SFCC 2004 Survey Summary. March 21, 2005 60
2.6 Sampling in Villages The survey team supervisors were instructed to use a random method to choose survey participants in both the pagoda and the community. In the community, the survey supervisors used a "spin the pen" method. Every second house was be selected in the direction that the pen points. The survey supervisors adhered to the following rules: The survey supervisor would meet the village chief, show the permission letter, and then go to the center of the village according to the village chief's definition of the center. If the village had a major cross roads, then the supervisor would spin the pen there and take side of the road that the pen points to. If the road that they initially took bends around, they would stay on the road. If the village had no road and the houses were scattered in rice paddies, then the survey team would walk in the general direction of the pen and survey every second house. If after walking through the fields, the survey supervisors would come upon a new road that goes in the direction of the pen, they would follow that road until the end of houses or their survey. When the survey team would come upon the end of the village, they would return to the center and spin the pen again. Picture 2b. Expatriate supervisor in the village with survey team.

SFCC 2004 Survey Summary. March 21, 2005 61
2.7 Sampling in Pagodas. When the survey teams would travel to a Pagoda, they would have to sample in two ways for the varying sizes of pagodas. Because the survey teams would sometimes need 15 monks in a pagoda, and sometimes less than 15, they would use varying methods below. The surveyor first obtains permission from the appropriate pagoda head monk or Achaa by presenting the letter from the provincial governor and the provincial director of cults of religion. This headman can then provide the total number of monks in the pagoda. In a small Pagoda: If the survey team needs 15 monks in a small pagoda with less than 15, then they survey all monks and go to the next nearest pagoda in the same commune. If the survey team needs a less than 15 monks in a pagoda (because they are surveying the second part of a cluster in one survey) then they must choose those monks in a random fashion. Example: If the surveyors need 7 monks and there are 20 in the pagoda, the supervisor is to select the seven randomly from the 20 available monks. The supervisor is to call all of the monks to the Pagoda central hall and have them sit in their formation. The supervisor is to then choose a random number from a bill note or a dice and count that number around the 20 monks until the seven monks are selected. The remaining monks are told to return to their quarters and the seven random monks are surveyed. In a large Pagoda: If the survey team is to select 15 monks from a pagoda with greater than 30 monks*, then they are to use a different method from above because it is difficult to call all of the monks to the central hall. The supervisor is to use the "spin the pen" technique and select a monk house to survey. The supervisor is then to choose every other bed in the house and survey until they complete 15 surveys. If they finish the house, they are to move to the next house. This method accounts for all missing monks because each monk has a bed and if it is vacant, it is easy to ask where the monk is. 2.8 Data management Data for all questionnaires were double entered and validated using Epi-Info 6.04c to minimize data entry errors and inconsistencies. SPSS 9.0 was used to generate frequencies and conduct more advanced statistics. A codebook was created for all variables (appendix 2). 2.9 Government collaboration ADRA Cambodia hired members of the Cambodian ministry of Cults and Religion and the ministry of health to help with the research process and future interventions. While traveling to the provinces, these government counterparts were key in helping ADRA prepare and receive permission letters from all government officials who * Sometimes pagodas with less than 30 monks were sampled in this way because it was difficult to call all monks to the central meeting place.
SFCC 2004 Survey Summary. March 21, 2005 62
should be contacted. Letters of permission for this survey were obtained from all provincial level Ministries of Cults and Religion, Ministries of Health, and from the Provincial governors (appendix 7). Two members of the National Center for Health Promotion also worked with the research team. These government counterparts were some of the best survey supervisors. They were trained in all the same research methodologies as all the ADRA staff and it is hoped that they can bring their new skills into their government health jobs. 2.10 Ethical consideration and permission for research All possible permissions and ethical measures were taken during this research. At all levels, the permissions were granted from the appropriate authorities. A general letter of permission (appendix 7) was obtained from the office of the governor at each province and this letter was shown to every village chief and pagoda head monk. A general letter from each provincial ministry of health, and a general permission letter from the Ministry of Cults and religion in Phnom Penh and in each province were also collected. When a survey team would enter a village or Pagoda, the survey supervisor would show the village chief, or Pagoda chief these letters, and kindly ask for his/her permission to conduct the survey. The chief was usually very happy to support the survey and often accompanied the survey team leader and assisted the survey supervisors in their random method to locate the participants.

SFCC 2004 Survey Summary. March 21, 2005 63
Appendix 3 – Results of Pagoda Survey Questionnaire. 2004 CAMBODIA BUDDHIST PAGODA SURVEY QUESTIONAIRRE FACT SHEET
Place surveyed: Wat / Pagoda (Buddhist Temple) in 5 provinces Total sample size: 167 Locations surveyed: Random selection of pagodas in Phnom Penh, Pousat, Svay Rieng, Kampot, and Siem Reap
province. Sampling Methodology:
This survey was conducted in association with the SFCC Buddhist Monk survey. For every pagoda sampled in the SFCC survey, this survey interviewed one chief monk. If a chief monk was not available, this survey interviewed the next highest ranking monk.
Purpose of Survey: To evaluate each Pagoda’s Socio-Economic-Status (SES)***, compliance with the ban on smoking in Buddhist Pagodas, and to evaluate the Chief monk’s smoking status. This survey’s variables are also coded in the larger 2004 Buddhist Monk survey.
Percentage of pagodas with people/monks smoking (observation): 42.68% Percentage of pagodas with promotional items or tobacco advertising: 6.06% Percentage of pagodas with "no smoking", warning signs, or other anti-tobacco signs: 65.24% Percentage of pagodas with tobacco selling on the campus: 16.87% Practices of Smoking % (n) (N) The chief monk smokes 43.71 73 167 Total number of Achaa reported to be in surveyed pagodas 561 Total number of Achaa reported to be in surveyed pagodas who smoke 349 Percentage of Achaa in the pagoda who smoke 62.21% Visible Compliance in Restricted Areas % (n) (N)
Percentage of pagodas with "no smoking", warning signs, or other anti-tobacco signs (observation) 65.24 107 164
Have received the circulation from the Ministry of Cults and Religion on the ban of smoking in pagodas 64.07 107 167
The tobacco control ban has been completely implemented at the surveyed pagoda 13.77 23 167
Only part of the tobacco control ban has been implemented at the pagoda 67.66 113 167
The tobacco control ban has not been implemented at the pagoda 18.56 31 167
Have a plan to implement the tobacco control ban at the surveyed pagoda 87.91 80 91
At the Observed Site (observations) % (n) (N) Percentage of pagodas with people/monks smoking (observation): 42.68 70 164 Percentage of pagodas with tobacco selling on the campus: 16.87 28 166 Percentage of pagodas with promotional items or tobacco advertising: 6.06 10 165 Percentage of Chief Monk who smokes shown by Province % (n) (N) Phnom Penh 50 11 22 Siem Reap 61.54 16 26 Svay Rieng 30.95 13 42 Pousat 41.67 15 36 Kampot 43.90 18 41
*** Additional data on Buddhist Pagoda Socio-Economic-Status (SES) was not informative for the purposes of this Survey Summary. Please contact the authors of this report if interested in these statistics.

Appendix 4 – Survey Questionnaires Buddhist Monk Questionnaire
Buddhist Monk Behavior Regarding Tobacco's 2004 (for monk only)
Date:...................../......................2004 Nº................... Interviewer:................................................ Village:.........................................................Commune............................................................... District....................................................... Province.........................................Pagoda Name:......................................................................
READ INTRODUCTION STATEMENT TO EACH MONK AND OBTAIN CONSENT
Monk Selection Method (1=small pagoda: all monks called to meeting hall, 2=large pagoda: monk houses and beds randomly selected) Result of interview (1=completed, 2=Buddhist Monk not present at time of visit; rescheduled for ………..., 3=Refused) 1 Age?
2 # of years of formal schooling 3 a, # of years as a monk b, # of years of Buddhist education c, What is your rank as a monk? (1=peitkou 2=samunei 3=teacher 4=student 5=chief monk) 4 What do you think the teaching of Buddha has to say about smoking?(1= nothing, 2=smoking is ok, 3= smoking is not ok, 4= other (write in)) 5 Do you think that people should offer cigarettes to monks? (1= yes 2= no) 6a Are you exposed to the smoke of other people's cigarettes on a daily basis? (1=yes 2= no) 6b How are you exposed to cigarette smoking? (1=prayer hall, 2=eating hall, 3=bedroom, 4=classroom, 5=all of the above, 6=other (write in)
6c Do community members or Achaa smoke during worship? (1= yes, 2= no) 7 Should monks smoke a ciggarette? (1= yes 2= no) (i.e. "be allowed to") 8 What is the average # of cigarette packages you receive monthly as gifts? (#packages/month) 9a What do you do with the tobacco gift packages? [any;no prompt] (1= smoke myself 2= give away 3= other) 9b How much do you think the tobacco cigarettes that are given as offerings are worth each month? (riel) 9c Have you ever refused offerings of cigarettes in the past three years? (1=yes, 2=no) if no skip to 9e 9d Why did you refuse the offerings? (1=ban at the pagoda, 2=health reasons, 3=recommendation from other monk, 4=other) 9e Is there any cigarette smoking ban which keeps people from smoking in your pagoda? (1=yes, 2=no)(if no skip to 10) 9f Is that cigarette smoking ban effective in your pagoda? (1=yes, 2=no) 10 Is smoking bad for health? (1=yes 2=no) (if no, skip to 14)
What are the diseases related to smoking? [any; no prompting] (1= lung CA, 2=heart disease, 3=stroke, 4=hypertension 11 5=impotence, 6=eye disease, 7= vascular disease, 8=mouth/throat CA, 9=Other[write in])
Where have you heard about the dangers of smoking? [any; do not prompt] (1=ADRA Cambodia 2=other health programs 12a 3=media 4=poster/brochure 5=school 6=Buddhist studies 7=other [write in], 8=ministry ciruculation/announcement) (if #3, go to 12b) 12b If media, what kind (any;prompt) 1=tv spot, 2=radio spot, 3=daily news, 4=radio talk show, 5= print media, 6=monk preaching, 7=cigarette packaging, 8=other(write in) 13 Would you be willing to teach people about the effects of smoking? (1= yes 2= no 3= not sure)

SFCC 2004 Survey Summary. March 21, 2005 65
14 Is smoking addictive? (1=yes 2=no) 15 Does smoking cause harm to others around smokers ? (1=yes, 2=no, 3=don't know) 16 How do you feel when you are near the smoker? (1= like it, 2=Do not like it) 17 Should there be a health warning on all tobacco products? (1=yes, 2=no) 18a Should cigarette advertising be allowed in Cambodia ? (1=yes, 2=no) 18b Should the government put a tax increase on tobacco sales? (1=yes, 2=no) 19a Have you ever smoked at least 100 cigarettes or the equivalent amount of tobacco in your lifetime? (1= yes 2= no) 19b Are you a former smoker who quit? (1=yes, 2=no) if yes continue to next question 19c How long ago did you quit smoking (months/years ago) 19d Why did you quit? (1=health problem, 2=money, 3=policy, 4=other) 19e How did you quit? (1=SCP, 2=awareness, 3=counceling, 4=other) 20a Are you currently a regular smoker? (1= yes 2=no) (smokes at least one cigarette / month) (ask everyone) 20b How often do you smoke? (1=daily, 2=few / week, 3=few/month, 4=never) (ask everyone; prompt) 20c Do you chew tobacco or bitter leafe? 1=chew tobacco, 2=bitter leaf, 3=chew tobacco and bitter leaf, 4=other[write in] 5=no [any: no prompt]
SMOKERS ONLY (if 20a=yes, and if 20b=1-3) 21 About how many cigarettes do you smoke every day? ( _____ cigarettes) 22 For how many years have you smoked? (.........years) 23 At what age did you try your first cigarette? (.......years)
Where do your cigarettes or tobacco come from? [any; no prompting] 24 1=Offerings from community 2=Other monks/friends 3=I buy them 4=all of the above 5=other [write in] 25 Do you want to quit smoking? (1= yes 2= no 3= not sure) If no, end survey
Why do you want to quit? [any; no prompting] 26 (1= health 2= waste of money 3= waste of time 4=Buddhist beliefs 5=peer pressure 6=other [write in]) 27 If a program was offered in your pagoda to help monks stop smoking would you attend? (1= yes 2=no)
28 Do you smoke within 20 minutes of waking up each day? (1 = yes 2=no)
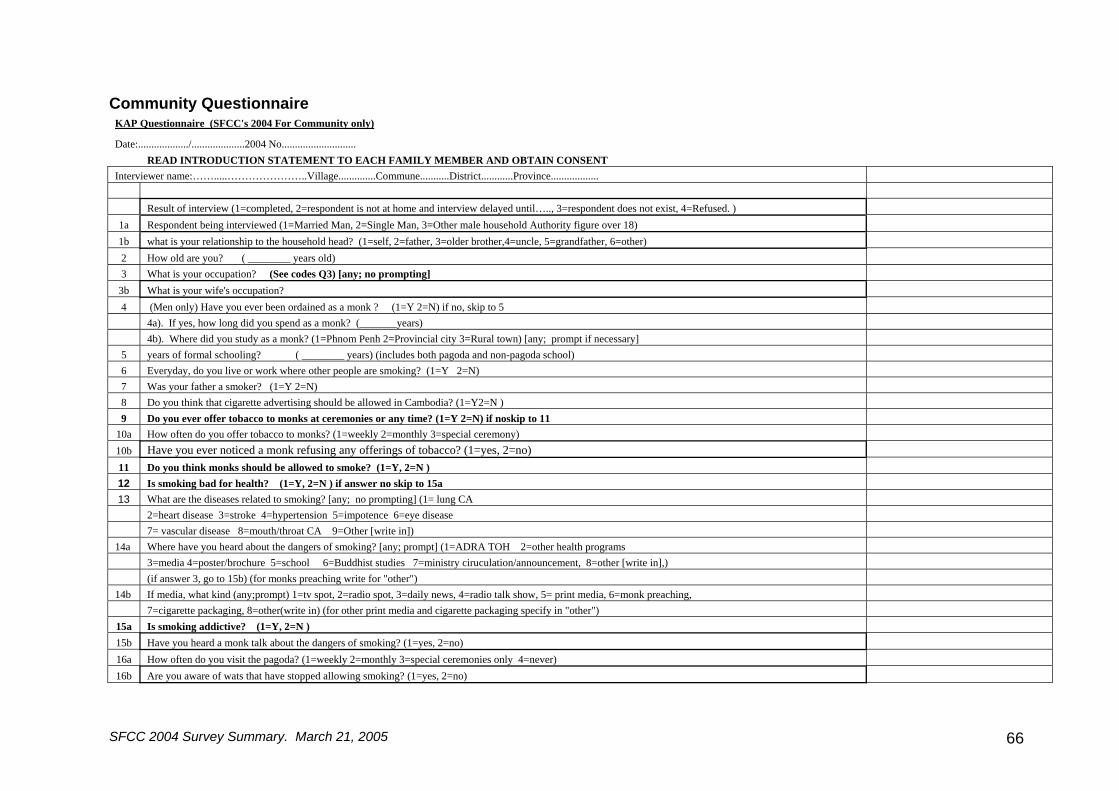
SFCC 2004 Survey Summary. March 21, 2005 66
Community Questionnaire KAP Questionnaire (SFCC's 2004 For Community only)
Date:.................../....................2004 No............................ READ INTRODUCTION STATEMENT TO EACH FAMILY MEMBER AND OBTAIN CONSENT
Interviewer name:…….....…………………..Village..............Commune...........District............Province.................. Result of interview (1=completed, 2=respondent is not at home and interview delayed until….., 3=respondent does not exist, 4=Refused. )
1a Respondent being interviewed (1=Married Man, 2=Single Man, 3=Other male household Authority figure over 18) 1b what is your relationship to the household head? (1=self, 2=father, 3=older brother,4=uncle, 5=grandfather, 6=other) 2 How old are you? ( ________ years old) 3 What is your occupation? (See codes Q3) [any; no prompting]
3b What is your wife's occupation? 4 (Men only) Have you ever been ordained as a monk ? (1=Y 2=N) if no, skip to 5 4a). If yes, how long did you spend as a monk? (_______years) 4b). Where did you study as a monk? (1=Phnom Penh 2=Provincial city 3=Rural town) [any; prompt if necessary] 5 years of formal schooling? ( ________ years) (includes both pagoda and non-pagoda school) 6 Everyday, do you live or work where other people are smoking? (1=Y 2=N) 7 Was your father a smoker? (1=Y 2=N) 8 Do you think that cigarette advertising should be allowed in Cambodia? (1=Y2=N ) 9 Do you ever offer tobacco to monks at ceremonies or any time? (1=Y 2=N) if noskip to 11
10a How often do you offer tobacco to monks? (1=weekly 2=monthly 3=special ceremony) 10b Have you ever noticed a monk refusing any offerings of tobacco? (1=yes, 2=no) 11 Do you think monks should be allowed to smoke? (1=Y, 2=N ) 12 Is smoking bad for health? (1=Y, 2=N ) if answer no skip to 15a 13 What are the diseases related to smoking? [any; no prompting] (1= lung CA 2=heart disease 3=stroke 4=hypertension 5=impotence 6=eye disease 7= vascular disease 8=mouth/throat CA 9=Other [write in])
14a Where have you heard about the dangers of smoking? [any; prompt] (1=ADRA TOH 2=other health programs 3=media 4=poster/brochure 5=school 6=Buddhist studies 7=ministry ciruculation/announcement, 8=other [write in],) (if answer 3, go to 15b) (for monks preaching write for "other") 14b If media, what kind (any;prompt) 1=tv spot, 2=radio spot, 3=daily news, 4=radio talk show, 5= print media, 6=monk preaching, 7=cigarette packaging, 8=other(write in) (for other print media and cigarette packaging specify in "other") 15a Is smoking addictive? (1=Y, 2=N ) 15b Have you heard a monk talk about the dangers of smoking? (1=yes, 2=no) 16a How often do you visit the pagoda? (1=weekly 2=monthly 3=special ceremonies only 4=never) 16b Are you aware of wats that have stopped allowing smoking? (1=yes, 2=no)
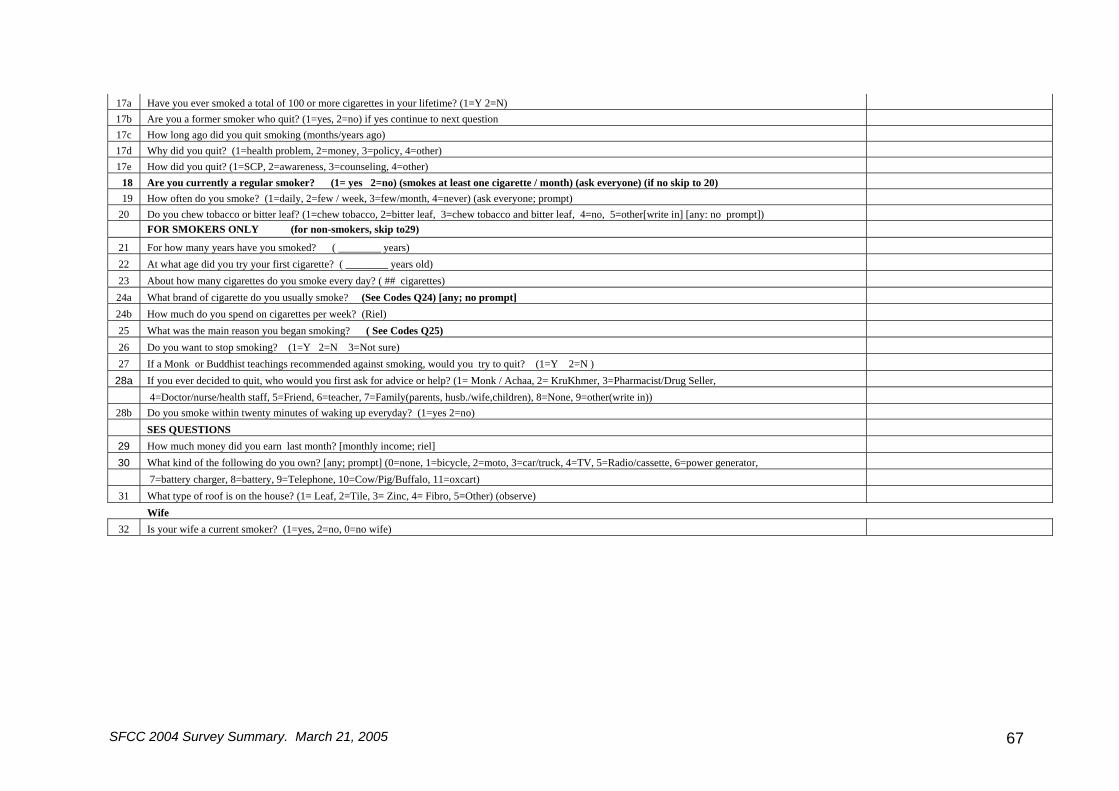
SFCC 2004 Survey Summary. March 21, 2005 67
17a Have you ever smoked a total of 100 or more cigarettes in your lifetime? (1=Y 2=N) 17b Are you a former smoker who quit? (1=yes, 2=no) if yes continue to next question 17c How long ago did you quit smoking (months/years ago) 17d Why did you quit? (1=health problem, 2=money, 3=policy, 4=other) 17e How did you quit? (1=SCP, 2=awareness, 3=counseling, 4=other)
18 Are you currently a regular smoker? (1= yes 2=no) (smokes at least one cigarette / month) (ask everyone) (if no skip to 20) 19 How often do you smoke? (1=daily, 2=few / week, 3=few/month, 4=never) (ask everyone; prompt)
20 Do you chew tobacco or bitter leaf? (1=chew tobacco, 2=bitter leaf, 3=chew tobacco and bitter leaf, 4=no, 5=other[write in] [any: no prompt]) FOR SMOKERS ONLY (for non-smokers, skip to29)
21 For how many years have you smoked? ( ________ years) 22 At what age did you try your first cigarette? ( ________ years old) 23 About how many cigarettes do you smoke every day? ( ## cigarettes) 24a What brand of cigarette do you usually smoke? (See Codes Q24) [any; no prompt] 24b How much do you spend on cigarettes per week? (Riel) 25 What was the main reason you began smoking? ( See Codes Q25) 26 Do you want to stop smoking? (1=Y 2=N 3=Not sure) 27 If a Monk or Buddhist teachings recommended against smoking, would you try to quit? (1=Y 2=N )
28a If you ever decided to quit, who would you first ask for advice or help? (1= Monk / Achaa, 2= KruKhmer, 3=Pharmacist/Drug Seller, 4=Doctor/nurse/health staff, 5=Friend, 6=teacher, 7=Family(parents, husb./wife,children), 8=None, 9=other(write in))
28b Do you smoke within twenty minutes of waking up everyday? (1=yes 2=no) SES QUESTIONS
29 How much money did you earn last month? [monthly income; riel] 30 What kind of the following do you own? [any; prompt] (0=none, 1=bicycle, 2=moto, 3=car/truck, 4=TV, 5=Radio/cassette, 6=power generator, 7=battery charger, 8=battery, 9=Telephone, 10=Cow/Pig/Buffalo, 11=oxcart)
31 What type of roof is on the house? (1= Leaf, 2=Tile, 3= Zinc, 4= Fibro, 5=Other) (observe) Wife
32 Is your wife a current smoker? (1=yes, 2=no, 0=no wife)
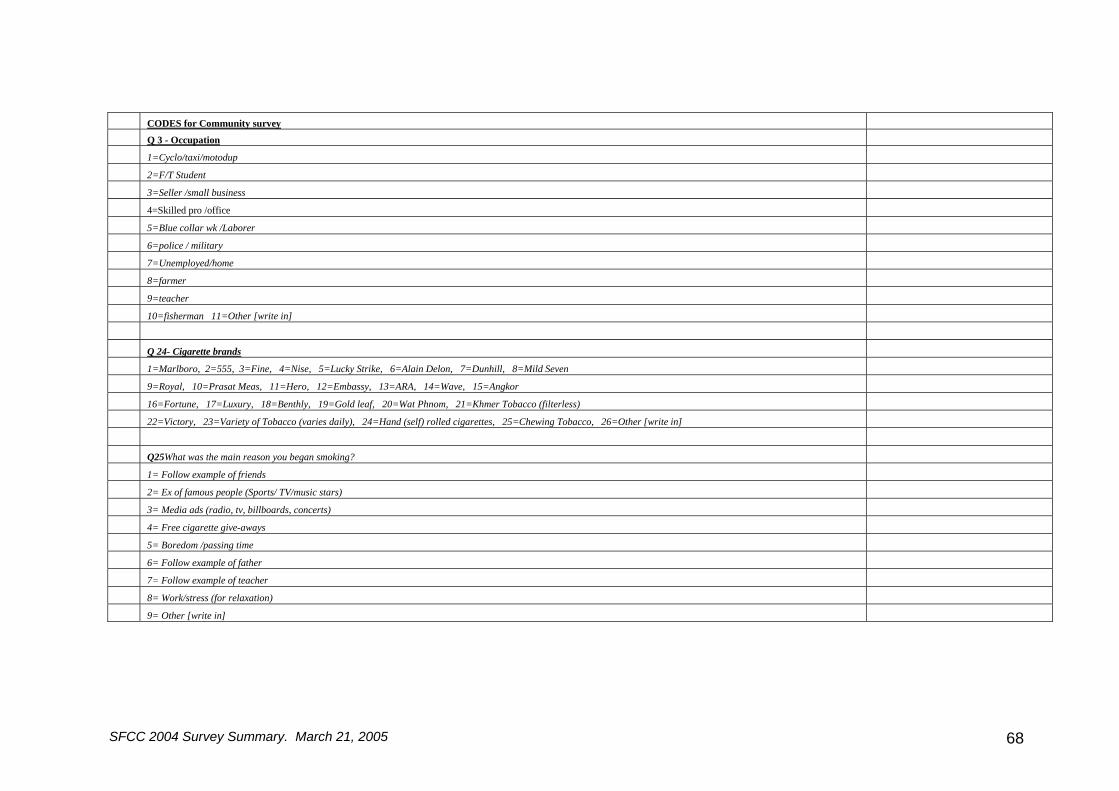
SFCC 2004 Survey Summary. March 21, 2005 68
CODES for Community survey Q 3 - Occupation 1=Cyclo/taxi/motodup 2=F/T Student 3=Seller /small business 4=Skilled pro /office 5=Blue collar wk /Laborer 6=police / military 7=Unemployed/home 8=farmer 9=teacher 10=fisherman 11=Other [write in] Q 24- Cigarette brands 1=Marlboro, 2=555, 3=Fine, 4=Nise, 5=Lucky Strike, 6=Alain Delon, 7=Dunhill, 8=Mild Seven 9=Royal, 10=Prasat Meas, 11=Hero, 12=Embassy, 13=ARA, 14=Wave, 15=Angkor 16=Fortune, 17=Luxury, 18=Benthly, 19=Gold leaf, 20=Wat Phnom, 21=Khmer Tobacco (filterless) 22=Victory, 23=Variety of Tobacco (varies daily), 24=Hand (self) rolled cigarettes, 25=Chewing Tobacco, 26=Other [write in] Q25What was the main reason you began smoking? 1= Follow example of friends 2= Ex of famous people (Sports/ TV/music stars) 3= Media ads (radio, tv, billboards, concerts) 4= Free cigarette give-aways 5= Boredom /passing time 6= Follow example of father 7= Follow example of teacher 8= Work/stress (for relaxation) 9= Other [write in]
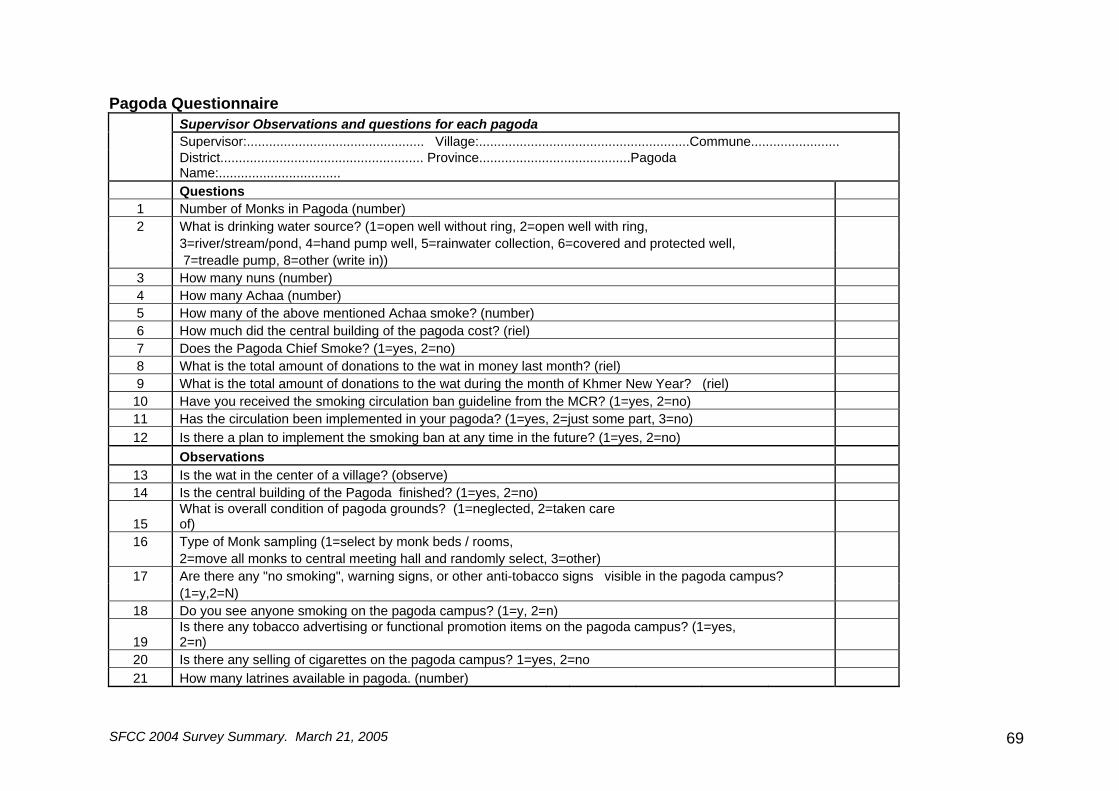
SFCC 2004 Survey Summary. March 21, 2005 69
Pagoda Questionnaire Supervisor Observations and questions for each pagoda Supervisor:................................................ Village:.........................................................Commune........................
District....................................................... Province.........................................Pagoda Name:.................................
Questions 1 Number of Monks in Pagoda (number) 2 What is drinking water source? (1=open well without ring, 2=open well with ring, 3=river/stream/pond, 4=hand pump well, 5=rainwater collection, 6=covered and protected well, 7=treadle pump, 8=other (write in)) 3 How many nuns (number) 4 How many Achaa (number) 5 How many of the above mentioned Achaa smoke? (number) 6 How much did the central building of the pagoda cost? (riel) 7 Does the Pagoda Chief Smoke? (1=yes, 2=no) 8 What is the total amount of donations to the wat in money last month? (riel) 9 What is the total amount of donations to the wat during the month of Khmer New Year? (riel) 10 Have you received the smoking circulation ban guideline from the MCR? (1=yes, 2=no) 11 Has the circulation been implemented in your pagoda? (1=yes, 2=just some part, 3=no) 12 Is there a plan to implement the smoking ban at any time in the future? (1=yes, 2=no)
Observations 13 Is the wat in the center of a village? (observe) 14 Is the central building of the Pagoda finished? (1=yes, 2=no)
15 What is overall condition of pagoda grounds? (1=neglected, 2=taken care of)
16 Type of Monk sampling (1=select by monk beds / rooms, 2=move all monks to central meeting hall and randomly select, 3=other)
17 Are there any "no smoking", warning signs, or other anti-tobacco signs visible in the pagoda campus? (1=y,2=N)
18 Do you see anyone smoking on the pagoda campus? (1=y, 2=n)
19 Is there any tobacco advertising or functional promotion items on the pagoda campus? (1=yes, 2=n)
20 Is there any selling of cigarettes on the pagoda campus? 1=yes, 2=no 21 How many latrines available in pagoda. (number)

SFCC 2004 Survey Summary. March 21, 2005 70
SFCC 2004 Survey Summary. March 21, 2005 71
Appendix 5 - References 1 Brundtland GH (1999). Speech delivered to the International Policy Conference on Children and Tobacco, 18 March 1999, Washington, DC. 2 WHO World Health Report (1998). Statistics on HIV AIDS. 3 Peto, R, A. Lopez, J. Boreham et al. (1997). Mortality From Smoking in Developed Countries 1950=2000. Oxford, ICRF and WHO. Oxford University Press. 4 Townsend, Jay. (1998) The Role of Taxation Policy in Tobacco Control. Abedian, Iraj, et. al. editors. The Economics of Tobacco Control: Toward and Optimal Policy Mix. Applied Fiscal Research Center, Cape Town. 6 Slama, Karen. (1998). Tobacco Control and Prevention: A guide for low income countries. International Union Against Tobacco and Lung Disease. Paris. 7 Ministry of Health. 2000. Tobacco Control Country Profile. Phnom Penh, Ministry of Health. 9 ADRA Cambodia. Smoke Free Buddhist Monk Survey Questionnaire. Survey Summary. 2001 10 Kalton, Graham. Introduction to Survey Sampling, Sage Publications, 1983 11 Epi Info, Database and statistics software for public health professionals. Centers for Disease Control. Version 3.2. 2004 12 Rosner, Bernard. Fundamentals of Biostatistics. 5th edition. Duxbury, 2000. pg 386. 13 Guidlines for controlling and monitoring the Tobacco Epidemic. World Health Organization. 1998. 14 Smith, Marshall Tobacco Control smoking Budhist monks. 1995