smile-line aesthetics for edentulous implant patients dentistry, ... are significant considerations...
TRANSCRIPT

Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of
specific product names does not infer endorsement by Dentistry Today. Information contained in CE articles and
courses is not a substitute for sound clinical judgment and accepted standards of care. Participants are urged to
contact their state dental boards for continuing education requirements.
Continuing Education
Smile-Line Aestheticsfor Edentulous Implant
PatientsAuthored by George Priest, DMD
Upon successful completion of this CE activity 1 CE credit hour will be awarded
Volume 33 No. 6 Page 98

ABOUT THE AUTHORDr. Priest maintains a private pros -thodontic practice in Hilton Head Island,SC. He is a Diplomate of the AmericanBoard of Prostho dontics, a Fellow of theAmerican College of Prosthodontists, aFellow of the International College of
Dentists, and a member of the American Academy ofEsthetic Dentistry, and he has been one of DentistryToday’s Leaders in Continuing Education for the past 9years. He is a former professor in graduate prosthodonticsat Emory and lectures internationally on topics includingimplant dentistry, advanced restorative dentistry, andaesthetic excellence. He is a regular contributor to manyacclaimed dental journals, and he can be reached via e-mail at [email protected].
Disclosure: Dr. Priest is a consultant and lecturer for IvoclarVivadent, but he did not receive compensation for writingthis article.
INTRODUCTIONEdentulism results not only in significant loss of function; itnegatively impacts self-esteem.1,2 According to Douglass etal,3 by the year 2020, nearly 38 million Americans will be inneed for treatment of edentulism in at least one arch. Thisdata underscores the continued need for dental treatmentrelated to total tooth loss, to maintain oral function and self-image, for this bourgeoning aging population for theforeseeable future.4
Many edentulous patients are typically re stored withtraditional dentures. Some of these dentures fit and functionacceptably for the life of the prosthesis. Some, however, mayfit poorly, wear prematurely, demonstrate poor opticalproperties, or are visually incompatible with the patient’s ageor facial dimensions. Unstable and poorly retained dentures,
and dentures with improperly sized and arranged teeth, maycause discomfort, sore spots, difficulty in eating or speaking,embarrassment in social situations, and a host of otherproblems.
Implant-retained overdentures and fixed dentalprostheses were developed to address many of theshortcomings of traditional dentures. Placing implants in apatient’s jaw to retain dentures or fixed restorations providesa better, more stable prosthesis, which assists edentulouspa tients with eating, speech, comfort, and confidence.5
Implants also reduce the loss of bone and dental soft tissue,which is vital in helping to maintain facial form.6,7
Today’s patients are more aware of the availability of, andoptions for, a beautiful smile with natural-looking aesthetics,and this includes denture wearers and patients with implantprostheses. Dentists are now able to create dentures andimplant overdentures that are lifelike and stable, unlikedentures of the past. Early dentures made from only unfilledpolymethylmethacrylate resins (PMMA) demonstrated limitedaesthetic potential and poor mechanical properties.8 With theadvent of Bis-GMA in the 1950s, composite resin dentureswith better aesthetics and durability emerged.9 Currentmaterial science has yielded nanohybrid composite resinsthat incorporate nanoparticle filler technology which impartstranslucency, strength, and superior wear characteristics,greatly improving the aesthetics and clinical longevity ofnanohybrid composite dentures and implant prostheses.10
Smile Design for Edentulous Patients When designing a prosthesis for an edentulous patient, theestablished principles of dental and facial aesthetics must betempered with the patient’s individual preferences to deliverpleasing results.11 The lip-line, smile-line, and facial profile willhelp guide the dentist to proper tooth position.12 The size andshape of teeth must be carefully selected to facilitate adequatevertical dimension of occlusion, phonetics, and facialproportions. Tooth shade should appear natural, as selected bythe clinician and patient,13 and the arc of the maxillary teethshould follow the curve of the lower lip, in what is termed aconsonant smile.14 A consonant smile is an aesthetic objectiveas well as a decisive guide to establishment of the correcttransverse angle of the occlusal plane.13 Clinicians can belimited by tooth position of dentate or partially dentate patients,
Continuing Education
1
Smile-Line Aesthetics forEdentulous Implant PatientsEffective Date: 6/1/2014 Expiration Date: 6/1/2017

but edentulous patients present anopen palate, giving the dentist 3-dimensional freedom to placeaesthetic artificial teeth in an optimalposition and arrangement within theconfines of the remaining residualridges. Using a systematic approachcan facilitate the selection of theappropriate teeth. Based on apatient’s specific aesthetic goals andthe dentist’s functional objectives,shade, shape, and wear propertiesare significant considerations intooth selection.
The following 2 clinical examplesillustrate how patients can be rejuv-enated functionally and aestheticallywith a new or restored prosthesisusing SR Phonares II (IvoclarVivadent) denture teeth and denturesmile design principles.
CASE REPORTSCase 1Long-term denture wear resulted in maxillaryridge resorption of a 79-year-old female pa tient(Figure 1). The unstable, nonretentive denturemade it difficult for her to enjoy eating. She rarelywore her uncomfortable mandibular removablepartial denture, further exacerbating her chewingdisability. She also felt that her prostheses madeher look older than her years (Figure 2). Frus -trated with dental compromise, this patientanxiously hoped for new prostheses that were notonly more stable and comfortable, but would alsoim prove her facial appearance.
In the maxillary arch, 3 treatment optionswere discussed: a new complete denture, aremovable implant prosthesis, and a fixed implantprosthesis. A CT scan revealed limited remainingmaxillary bone (Figure 3). The patient preferred amaxillary implant overdenture, but because shewas somewhat frail, she elected not to undergo
Continuing Education
2
Smile-Line Aesthetics for Edentulous Implant Patients
Figure 1. A 79-year-old female presented with amaxillary denture and missing mandibularposterior teeth.
Figure 2. The patient appeared overclosed, thetooth shade was too dark, and she demonstrated anonconsonant smile-line.
Figure 3. Cone-beam radiography revealedminimal yet adequate osseous volume for implantplacement.
Figure 4. Six implants were widely distributed inthe edentulous maxilla.
Figure 5. Jaw relation records withocclusion rims were completed, and castswere mounted on a Stratos 300 (IvoclarVivadent) articulator.
Figure 6. SR Phonares II (Ivoclar Vivadent)denture teeth were selected and arrangedfor their anatomical tooth shape, naturaloptical properties, and strength.
Figure 7. Patient approval was ascertainedat the try-in appointment.
Figure 8. Predicated on tooth position, atitanium implant overdenture bar wasvirtually designed.

recommended grafting procedures. The treatingprosthodontist and periodontist decided therewas minimal but ample bone for implantplacement. Alternatives for the man dibular archincluded replacement anterior crowns with eithera removable partial denture or implantprostheses. The patient selected a conventionalremovable partial denture for budgetary reasons.
Six maxillary implants were widelydistributed in the maxilla, but were relativelyshort and somewhat divergent due to thelimited quantity of bone available (Figure 4).Following successful implant integration, im -pressions were made, jaw relation recordswere completed, and the casts were mountedon a Stratos 300 articu lator (Ivoclar Vivadent)(Figure 5). Nanocomposite denture teeth (SRPhonares II) were selected and ar ranged inwax with the mandibular anterior crowns(Figure 6). These denture teeth were chosenbased on their improved mechanicalproperties, which would better withstand thepotential increased biting forces from theimplants and the abrasive effects of themandibular anterior crowns. Their anatomicalshape and lifelike optical properties wouldfacilitate the aesthetic improvement desired bythe patient. Initially, the patient selected SRPhonares II anterior mold S71, shade D3, butthen changed to the brighter B2 shade. Theauthor’s experience is that most patients wanta more youthful tooth shade and contour.
The accuracy of jaw relation records and aconsonant smile-line were verified during thewax try-in appointment (Figure 7). The patientshould be completely attentive and involved inthis try-in, offering critical positive andnegative feedback at this point as opposed toafter completion of the prosthesis. The dentallaboratory team optically scanned theapproved tooth arrangement and maxillaryimplant cast, and a titanium framework with LOCATORAttachments (ZEST Anchors) was virtually designed within
the confines of the teeth for the removable im plantoverdenture (Figure 8).
Continuing Education
3
Smile-Line Aesthetics for Edentulous Implant Patients
Figure 11. Reinforced with an internalchrome cobalt mesh, 4 red male LOCATORattachments provided adequate retention.
Figure 12. The new prosthesis provided avital and consonant smile.
Figure 13. At the seating appointment, thecompromised facial aesthetics of theexisting prosthesis was evident.
Figure 14. The new overdenturedramatically restored a youthful and vibrantfacial appearance.
Figure 15. Previous repairs and occlusaland incisal wear of an implant overdenturedetracted from the smile of a 62-year-oldfemale patient.
Figure 16. Unrestored anterior teeth andcrowned posterior teeth were present in themandibular arch.
Figure 9. The completed bar with 4 LOCATOR (ZEST Anchors) abutmentswas seated.
Figure 10. An open-palate prosthesis wasprocessed with characterized SR IvocapInjection System resin (Ivoclar Vivadent).

Following computer milling, the strong yetcompact titanium framework was seated andtightened to specified torque (Figure 9).Processed using the SR Ivocap InjectionSystem (Ivoclar Vivadent), an open palateoverdenture was completed (Figure 10). Toprevent acrylic fracture, a metal frameworkwas incorporated within the prosthesis(Figure 11).
During the seating appointment, theprosthodontist made minor chair side refine-ments for the patient’s comfort. Youthful andvibrant denture teeth greatly contributed to anaesthetic smile and happy patient (Figure 12).Wearing the existing maxillary denture to theseating appointment, the patient’s compromisedaesthetics from a reverse smile-line, agedappearing teeth, and a collapsed lower facialprofile were evident (Fig ure 13). At the end of thesame appointment, the patient’s facial aestheticswere completely transformed by re-establishingthe correct occlusal vertical dimension, aconsonant smile, and the vitality of the PhonaresII denture teeth (Figure 14).
Case 2 A 62-year-old female patient was concerned thata new maxillary prosthesis was needed becauseher denture teeth had become worn, and severalhad been repaired or replaced (Figure 15). In themandibular arch, the patient’s teeth and crownswere intact (Figure 16). Her prior dentist hadmeticulously made a hinge-lock maxillaryremovable implant prosthesis that was stillserviceable, but the patient had worn through theresin teeth and base to the metal superstructure(Figure 17). She also stated that food had begun to collect be neath the flange and palatalseal. Relieving the patient’s anxiety about theneed for a completely new rehabilitation, theprosthodontist recommended removing the wornteeth and base and replacement with new teeth
Continuing Education
4
Smile-Line Aesthetics for Edentulous Implant Patients
Figure 19. The intaglio of the prosthesiswas relieved and a new impression wasmade within the overdenture.
Figure 20. SR Phonares II denture teethwere selected to provide improved aesthe-tics and the greater strength required for animplant prosthesis opposing natural teeth.
Figure 21. Occlusion, phonetics, and aesthetics were verified at the try-in appointment.
Figure 22. Characterized SR Ivocap resin was used to process the completedprosthesis.
Figure 23. The renewed intaglio surface provided a passive seal against food entrapment.
Figure 24. The prosthesis demonstratedvivid, anatomical denture teeth and natural-appearing festooning.
Figure 17. The denture teeth had wornthrough to the metal superstructure, andfood was collecting beneath the flanges ofthe resorbing ridge.
Figure 18. Undercuts in the existing substructure were blocked out.
and base while reusing the functional frameworkand superstructure.
Relining a bar-type of prosthesis can bechallenging. Undercuts can trap and tearimpression material and the impression may belocked in place. Using Perma Block (PREATCorp), all spaces and undercuts beneath the barwere very carefully filled in (Figure 18).Approximately 2.0 mm of acrylic resin wasrelieved from the intaglio surface of theprosthesis, adhesive applied, and an impressionwas made, being sure to completely seat the prosthesis andengage the hinge-locks (Figure 19).
SR Phonares II denture teeth, anterior mold S71, shadeB1, were selected for this patient due to her history of wear andfracture, and to optimize the aesthetic outcome (Figure 20).The superstructure with the waxed teeth was tried in forconfirmation of jaw relation records and the patient’s aestheticapproval (Figure 21). Charac terized Ivocap resin (IvoclarVivadent) was used to process the renewed open-palateprosthesis (Figure 22). The re processed base was designed tofit passively yet intimately against the maxillary ridge to providea seal for speech and prevent food collection (Figure 23).
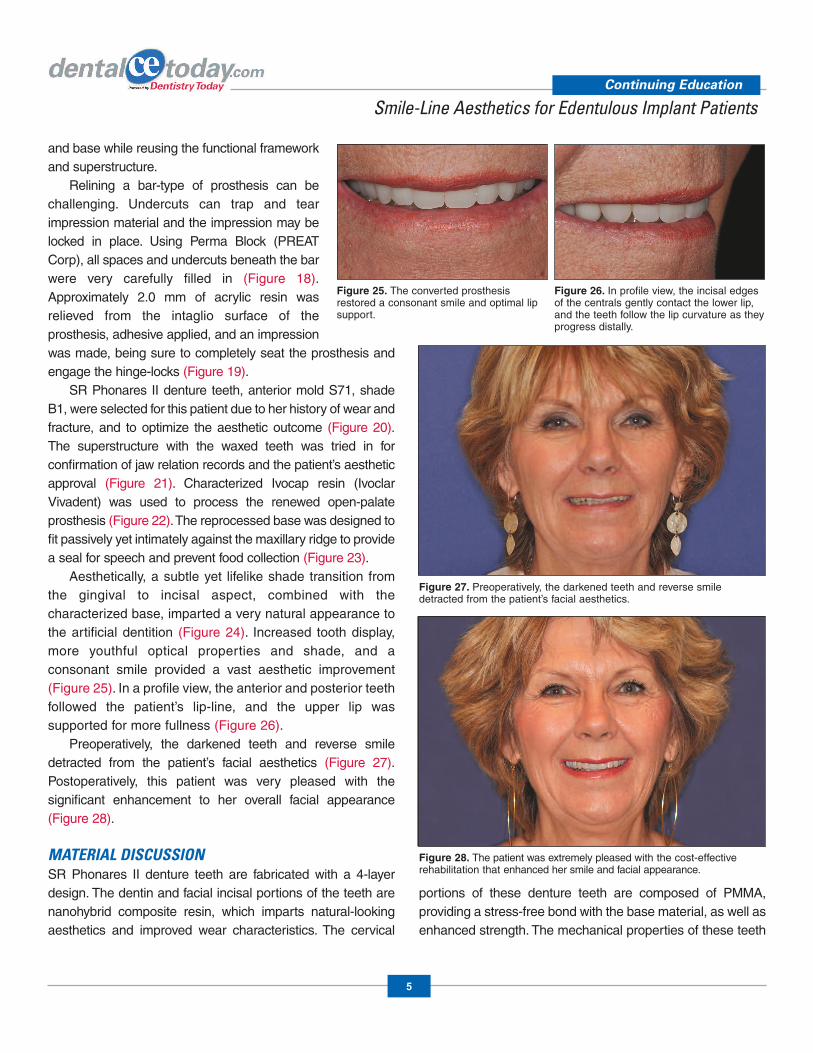
Aesthetically, a subtle yet lifelike shade transition fromthe gingival to incisal aspect, combined with thecharacterized base, imparted a very natural appearance tothe artificial dentition (Figure 24). Increased tooth display,more youthful optical properties and shade, and aconsonant smile provided a vast aesthetic improvement(Figure 25). In a profile view, the anterior and posterior teethfollowed the patient’s lip-line, and the upper lip wassupported for more fullness (Figure 26).
Preoperatively, the darkened teeth and reverse smiledetracted from the patient’s facial aesthetics (Figure 27).Postoperatively, this patient was very pleased with thesignificant enhancement to her overall facial appearance(Figure 28).
MATERIAL DISCUSSIONSR Phonares II denture teeth are fabricated with a 4-layerdesign. The dentin and facial incisal portions of the teeth arenanohybrid composite resin, which imparts natural-lookingaesthetics and improved wear characteristics. The cervical
portions of these denture teeth are composed of PMMA,providing a stress-free bond with the base material, as well asenhanced strength. The mechanical properties of these teeth
Continuing Education
5
Smile-Line Aesthetics for Edentulous Implant Patients
Figure 25. The converted prosthesisrestored a consonant smile and optimal lipsupport.
Figure 26. In profile view, the incisal edgesof the centrals gently contact the lower lip,and the teeth follow the lip curvature as theyprogress distally.
Figure 27. Preoperatively, the darkened teeth and reverse smiledetracted from the patient’s facial aesthetics.
Figure 28. The patient was extremely pleased with the cost-effectiverehabilitation that enhanced her smile and facial appearance.

make them an excellent choice for patients with increasedocclusal forces, such as those with implant-supportedprostheses. Tooth molds are arranged systematically into 2basic shapes, soft (round) and bold (square), and 3 age-specific wear patterns: youthful, universal, and mature.
CLOSING COMMENTSEdentulous patients often have lowered expectations ofdental rehabilitation, with the misconception that their onlychoices are inherently unstable and unaesthetic dentures. Asdemonstrated in these examples, it is possible with today’sadvanced materials and techniques to provide patients withhighly aesthetic solutions that are comfortable, stable, andwhich restore their oral function and self-esteem.
REFERENCES1. Davis DM, Fiske J, Scott B, et al. The emotional effects
of tooth loss: a preliminary quantitative study. Br Dent J.2000;188:503-506.
2. Strassburger C, Kerschbaum T, Heydecke G. Influenceof implant and conventional prostheses on satisfactionand quality of life: a literature review. Part 2: qualitativeanalysis and evaluation of the studies. Int JProsthodont. 2006;19:339-348.
3. Douglass CW, Shih A, Ostry L. Will there be a need forcomplete dentures in the United States in 2020? JProsthet Dent. 2002;87:5-8.
4. Allen PF, McMillan AS. A longitudinal study of quality of lifeoutcomes in older adults requesting implant prosthesesand complete removable dentures. Clin Oral Implants Res.2003;14:173-179.
5. Kent G, Johns R. Effects of osseointegrated implantson psychological and social well-being: a comparisonwith replacement removable prostheses. Int J OralMaxillofac Implants. 1994;9:103-106.
6. LaBarre EE, Ahlstrom RH, Noble WH. Narrow diameterimplants for mandibular denture retention. J Calif DentAssoc. 2008;36:283-286.
7. Wyatt CC. The effect of prosthodontic treatment onalveolar bone loss: a review of the literature. J ProsthetDent. 1998;80:362-366.
8. Powers JM, Sakaguchi RL. Craig’s Restorative DentalMaterials. 12th ed. St. Louis, MO: Mosby Elsevier;2006.
9. Bowen RL, inventor; Bowen RL, assignee. Dental fillingmaterial comprising vinyl silane treated fused silica anda binder consisting of the reaction product of Bis phenoland glycidyl acrylate. US patent 3066112A. November27, 1962.
10. Melander J, Dunn WP, Link MP, et al. Comparison offlexural properties and surface roughness ofnanohybrid and microhybrid dental composites. GenDent. 2011;59:342-347.
11. Witt M, Flores-Mir C. Laypeople’s preferencesregarding frontal dentofacial esthetics: tooth-relatedfactors. J Am Dent Assoc. 2011;142:635-645.
12. Priest G. Optimal smile line esthetics for edentulous anddentate patients. American Journal of Esthetic Dentistry.2012;2:188-198.
13. Dibai N, Caro S. Aesthetics and osseointegration for thecompletely edentulous. J Dent Que. 1990;27:407-411.
14. Passia N, Blatz M, Strub JR. Is the smile line a validparameter for esthetic evaluation? A systematicliterature review. Eur J Esthet Dent. 2011;6:314-327.
Continuing Education
6
Smile-Line Aesthetics for Edentulous Implant Patients

POST EXAMINATION INFORMATION
To receive continuing education credit for participation inthis educational activity you must complete the programpost examination and answer 4 out of 5 questions correctly.
Traditional Completion Option:You may fax or mail your answers with payment to DentistryToday (see Traditional Completion Information on followingpage). All information requested must be provided in orderto process the program for credit. Be sure to complete your“Payment,” “Personal Certification Information,” “Answers,”and “Evaluation” forms. Your exam will be graded within 72hours of receipt. Upon successful completion of the post-exam (answer 4 out of 5 questions correctly), a letter ofcompletion will be mailed to the address provided.
Online Completion Option:Use this page to review the questions and mark youranswers. Return to dentalcetoday.com and sign in. If youhave not previously purchased the program, select it fromthe “Online Courses” listing and complete the onlinepurchase process. Once purchased the program will beadded to your User History page where a Take Exam linkwill be provided directly across from the program title.Select the Take Exam link, complete all the programquestions and Submit your answers. An immediate gradereport will be provided. Upon receiving a passing grade,complete the online evaluation form. Upon submitting the form, your Letter Of Completion will be providedimmediately for printing.
General Program Information:Online users may log in to dentalcetoday.com any time inthe future to access previously purchased programs andview or print letters of completion and results.
POST EXAMINATION QUESTIONS
1. According to the 2010 National Health InterviewSurvey, only 10% of the entire US population, 45years and older, is now completely edentulous.
a. True b. False
2. Implants also reduce the loss of bone and dental softtissue, which is vital in helping to maintain facialform.
a. True b. False
3. With the advent of Bis-GMA in the 1950s,polymethylmethacrylate dentures with betteraesthetics and durability emerged.
a. True b. False
4. A consonant smile is an aesthetic objective as wellas a decisive guide to establishment of the correcttransverse angle of the occlusal plane.
a. True b. False
5. SR Phonares II (Ivoclar Vivadent) denture teeth arefabricated with a 2-layer design.
a. True b. False
Continuing Education
7
Smile-Line Aesthetics for Edentulous Implant Patients
This CE activity was not developed in accordance withAGD PACE or ADA CERP standards.CEUs for this activity will not be accepted by the AGDfor MAGD/FAGD credit.

PROGRAM COMPLETION INFORMATION
If you wish to purchase and complete this activitytraditionally (mail or fax) rather than online, you mustprovide the information requested below. Please be sure toselect your answers carefully and complete the evaluationinformation. To receive credit you must answer 4 of the 5questions correctly.
Complete online at: dentalcetoday.com
TRADITIONAL COMPLETION INFORMATION:Mail or fax this completed form with payment to:
Dentistry TodayDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004
Fax: 973-882-3622
PAYMENT & CREDIT INFORMATION:
Examination Fee: $20.00 Credit Hours: 1
Note: There is a $10 surcharge to process a check drawn on any bank other than a US bank. Should you have additionalquestions, please contact us at (973) 882-4700.
o I have enclosed a check or money order.
o I am using a credit card.
My Credit Card information is provided below.
o American Express o Visa o MC o Discover
Please provide the following (please print clearly):
Exact Name on Credit Card
Credit Card # Expiration Date
Signature
PROGRAM EVAUATION FORMPlease complete the following activity evaluation questions.
Rating Scale: Excellent = 5 and Poor = 0
Course objectives were achieved.
Content was useful and benefited your clinical practice.
Review questions were clear and relevant to the editorial.
Illustrations and photographs were clear and relevant.
Written presentation was informative and concise.
How much time did you spend reading the activity and completing the test?
What aspect of this course was most helpful and why?
What topics interest you for future Dentistry Today CE courses?
Continuing Education
Smile-Line Aesthetics for Edentulous Implant Patients
ANSWER FORM: VOLUME 33 NO. 6 PAGE 98Please check the correct box for each question below.
1. o a. True o b. False
2. o a. True o b. False
3. o a. True o b. False
4. o a. True o b. False
5. o a. True o b. False
PERSONAL CERTIFICATION INFORMATION:
Last Name (PLEASE PRINT CLEARLY OR TYPE)
First Name
Profession / Credentials License Number
Street Address
Suite or Apartment Number
City State Zip Code
Daytime Telephone Number With Area Code
Fax Number With Area Code
E-mail Address
/
8
This CE activity was not developed in accordance withAGD PACE or ADA CERP standards.CEUs for this activity will not be accepted by the AGDfor MAGD/FAGD credit.