skin necrosis following prolonged administration of coumarin in a patient with inherited protein s...
TRANSCRIPT

American Journal of Hematology 38:64-66 (1991)
Skin Necrosis Following Prolonged Administration of Coumarin in a Patient With Inherited Protein S Deficiency
Stuart L. Goldberg, Carolyn L. Orthner, Barbara L. Yalisove, Mervyn L. Elgart, and Craig M. Kessler
Division of Hematology and Oncology (S.L.G., C.M.K.) and Department of Dermatology (B.L.Y., M.L.E.), George Washington University Medical Center, Washington, D.C.; Jerome H. Holland Laboratory, American Red Cross (C.L.O.), Rockville, Maryland
Depression of the vitamin K-dependent modulators of coagulation during the initial phase of oral anticoagulant therapy may lead to a transient hypercoagulable state and skin necrosis. We report a case of skin necrosis associated with inherited protein S deficiency following prolonged coumarin therapy. As a result of a stasis ulceration causing a rise in c4b binding protein and concurrent treatment with topical sulfonamide, we hypothesize that a precipitous decrease in free protein S led to skin necrosis. Progression of the necrosis was halted with unactivated prothrombin complex concentrate. This case confirms the rare association between coumarin induced skin necrosis and protein S deficiency and emphasizes potential drug interactions.
Key words: protein S, hypercoagulable states, vitamin K-dependent modulators
INTRODUCTION
Coumarin necrosis, a rare complication of oral anti- coagulant therapy, typically occurs between the third and tenth days of therapy and involves infarction of skin and subcutaneous tissues secondary to diffuse thrombosis of small venules [l]. Its etiology may be related to an iatrogenic hypercoagulable state induced during the ini- tiation of coumarin therapy by significant decreases in protein C, a vitamin K-dependent protein with a rela- tively short half-life [2,3]. Protein S, a cofactor of activated protein C, also may be reduced by coumarin and precipitate a hypercoagulable state with skin necro- sis. However, the longer half-life of protein S compared to protein C and other vitamin K-dependent proteins may provide a margin of safety during coumarin initiation by allowing the development of an anticoagulated state to occur first [4]. Four cases of skin necrosis have been described following initiation of anticoagulant therapy in patients with protein S deficiency, including two with a concurrent lupus anticoagulant [5-71. We report a case of inherited protein S deficiency in which skin necrosis occurred after 15 years of cournarin therapy.
REPORT OF THE CASE
A 38-year-old white male presented with a history of multiple thromboembolic events occurring over a 15 year 0 1991 Wiley-Liss, Inc.
period despite oral anticoagulant therapy. There was a strong family history of thromboembolic events occur- ring in his father and paternal second cousin.
Several months before presentation, the patient devel- oped an extensive lower extremity stasis ulceration. Hyperbaric oxygenation, bedrest with elevation, oral antibiotics, and an Una boot resulted in incomplete healing. Topical silvadene cream was applied liberally over the entire ulceration during the 6 weeks prior to presentation.
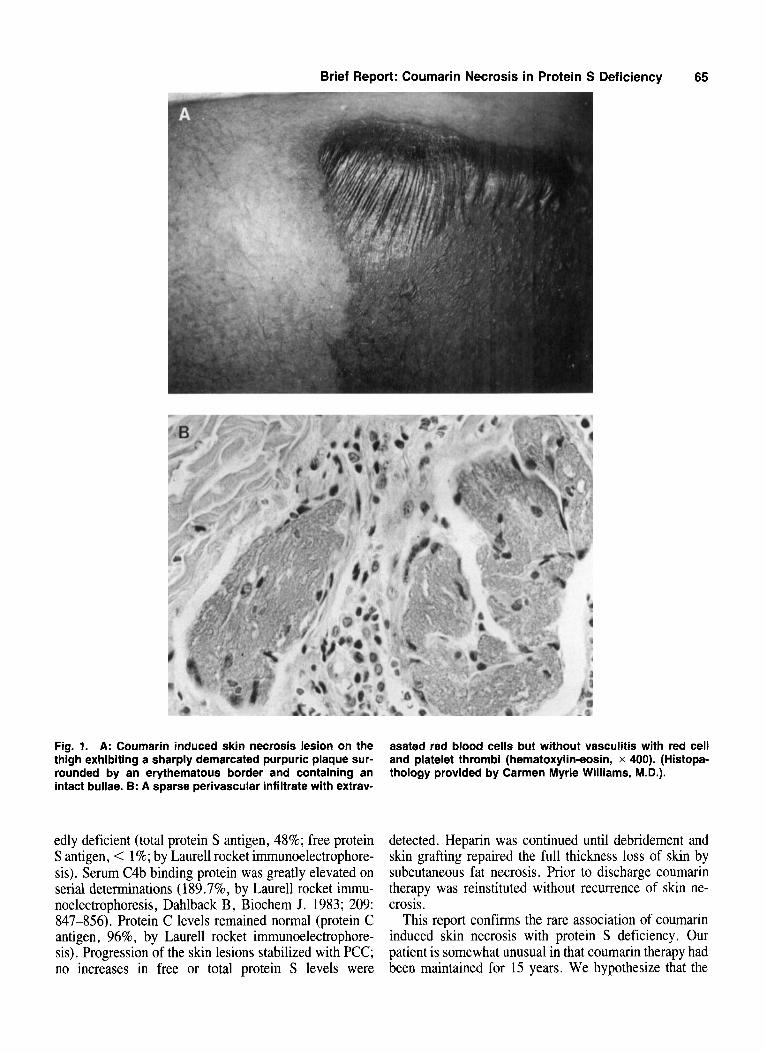
Painful escharified lesions, circumscribed by discrete erythematous borders and containing scattered bullae, developed suddenly over the patient’s legs and buttocks (Fig. 1). The lesions progressed despite discontinuation of the coumarin. An unactivated prothrombin complex concentrate (PCC, containing proteins C and S) was administered 25 units Factor IX/kg bolus followed by 20 units/kg continuous infusion for 2 days. Continuous intravenous heparin at 1,000 unitsihr was administered concurrently. Pre-treatment protein S levels were mark-
Received for publication January 16, 1991; accepted February 14, 1991.
Address reprint requests to Craig M . Kessler, M.D., Division of Hematology and Oncology, George Washington University Medical Center, 21 50 Pennsylvania Avenue, NW, Suite 3-428, Washington, DC 20037.
Brief Report: Coumarin Necrosis in Protein S Deficiency 65
Fig. 1. A: Coumarin induced skin necrosis lesion on the thigh exhibiting a sharply demarcated purpuric plaque sur- rounded by an erythematous border and containing an intact bullae. 6: A sparse perivascular infiltrate with extrav-
asated red blood cells but without vasculitis with red cell and platelet thrombi (hematoxylin-eosin, x 400). (Histopa- thology provided by Carmen Myrie Williams, M.D.).
edly deficient (total protein S antigen, 48%; free protein S antigen, < 1%; by Laurell rocket immunoelectrophore- sis). Serum C4b binding protein was greatly elevated on serial determinations (189.7%, by Laurell rocket immu- noelectrophoresis, Dahlback B, Biochem J. 1983; 209: 847-856). Protein C levels remained normal (protein C antigen, 96%, by Laurell rocket immunoelectrophore- sis). Progression of the skin lesions stabilized with PCC; no increases in free or total protein S levels were
detected. Heparin was continued until debridement and skin grafting repaired the full thickness loss of skin by subcutaneous fat necrosis. Prior to discharge coumarin therapy was reinstituted without recurrence of skin ne- crosis.
This report confirms the rare association of coumarin induced skin necrosis with protein S deficiency. Our patient is somewhat unusual in that coumarin therapy had been maintained for 15 years. We hypothesize that the

66
liberal application of silvadene cream with systemic absorption of the sulfa compound through the open wound may have upset the delicately balanced modula- tion of coagulation. Sulfa compounds potentiate antico- agulant effects by displacing coumarin from albumin [8]. This additional coumarin effect may have exacerbated preexisting decreases in free and total protein S levels. Alternatively, or concurrently, the markedly increased levels of C4b binding protein, an acute phase reactant rising in response to the inflammatory venous stasis ulceration, could have mediated the development of the skin necrosis since only the free unbound protein S modulates coagulation [9]. We speculate that increased circulating levels of coumarin and C4b binding protein produced a sudden uncompensated decrease in the free protein S level, leading to transient hypercoagulability and skin necrosis. This case illustrates a rare but serious complication of coumarin therapy in patients with under- lying hypercoagulable states, and serves to emphasize the importance of recognizing potential drug interactions with coumarin therapy.
Brief Report: Goldberg et al.
ACKNOWLEDGMENTS
The authors thank Marvin Chadab, M.D., for referring the patient. We also thank J.D. McGriff and Ciro
Berdeguez for technical assistance in performing the coagulation assays.
REFERENCES
1.
2 .
3.
4.
5.
6 .
7.
8.
9.
Horn JR, Danziger LH, Davis RJ: Warfarin-induced skin necrosis. A report of four cases. Am J Hosp Pharm 38:1763-1768, 1981. Broekmans AW, Bertina RM, Loeliger EA, Hofrnann V, Klingemann HG: Protein C and the development of skin necrosis during anticoag- ulant therapy. Thromb Haemost 49:244, 1983. McGehee WG, Klotz TA, Epstein DJ, Rapaport SI: Coumarin necrosis associated with hereditary protein C deficiency. Ann Intern Med 101:59,60, 1984. D’Angelo A, Vigano-D’Angelo S, Esrnon CT, Comp PC: Acquired deficiencies of protein S. J Clin Invest 81~1445-1454, 1988. Grimaudo V , Gueissaz F, Hauert J , Sarraji A, Kruithof EKO, Bach- mann F: Necrosis of skin induced by coumarin in a patient deficient in protein S. Br Med J [Clin Res] 298~233-234, 1989. Moreb J, Kitchens CS: Acquired functional protein S deficiency, cerebral venous thrombosis, and coumarin skin necrosis in association with antiphospholipid syndrome: Report of two cases. Am J Med 87:207-2 10, 1989. Friedman KD, Marlar RA, Houston JG, Montgomery RR: Warfarin- induced skin necrosis in a patient with protein S deficiency. (abstr) Blood 68(Suppl 1):33A, 1986. Peterson CE, Kwaan HC: Current concepts of warfarin therapy. Arch Intern Med 146~581-584, 1986. Boerger LM, Morris PC, Thurnau GR, Esmon CT, Comp PC: Oral contraceptives and gender affect protein S status. Blood 69592-694, 1987.