short-term outcomes and long-term prognosis in oral cavity
TRANSCRIPT

Yale UniversityEliScholar – A Digital Platform for Scholarly Publishing at Yale
Yale Medicine Thesis Digital Library School of Medicine
January 2016
Short-Term Outcomes And Long-Term PrognosisIn Oral Cavity CancerZachary Gregg SchwamYale University, [email protected]
Follow this and additional works at: http://elischolar.library.yale.edu/ymtdl
This Open Access Thesis is brought to you for free and open access by the School of Medicine at EliScholar – A Digital Platform for ScholarlyPublishing at Yale. It has been accepted for inclusion in Yale Medicine Thesis Digital Library by an authorized administrator of EliScholar – A DigitalPlatform for Scholarly Publishing at Yale. For more information, please contact [email protected].
Recommended CitationSchwam, Zachary Gregg, "Short-Term Outcomes And Long-Term Prognosis In Oral Cavity Cancer" (2016). Yale Medicine ThesisDigital Library. 2079.http://elischolar.library.yale.edu/ymtdl/2079

1
SHORT-TERM OUTCOMES AND LONG-TERM PROGNOSIS
OF ORAL CAVITY CANCER
A Thesis Submitted to the
Yale University School of Medicine
in Partial Fulfillment of the Requirements for the
Degree of Doctor of Medicine
by
Zachary G. Schwam and Benjamin L. Judson (advisor)1
1Department of Surgery, Section of Otolaryngology, Yale University School
of Medicine, New Haven, CT
2016

2
SHORT-TERM OUTCOMES AND LONG-TERM PROGNOSIS OF ORAL CAVITY
CANCER. Zachary G. Schwam, Benjamin L. Judson (advisor). Section of
Otolaryngology, Department of Surgery, Yale University School of Medicine, New
Haven, CT.
We sought to characterize short-term morbidity and mortality outcomes as well as
long-term changes in prognosis for oral cancer patients. We predicted that clinical and
demographic variables would affect short- and long-term outcomes. Retrospective
analyses of the National Surgical Quality Improvement Program (NSQIP) and National
Cancer Database (NCDB) were performed on 408 and 13,655 patients, respectively. Chi-
square, Kaplan Meier, logistic regression, and Cox proportional hazards regression were
performed. In the NSQIP, the overall adverse event and mortality rates were 20.3% and
1.0%, respectively. The most common complications were reoperation, infection, and
respiratory complications. Over 90% of post-discharge complications occurred by post-
discharge day (PDD) 14, but the majority of surgical-site infections and dehiscences
occurred by PDD 7. Neck dissection, smoking, and weight loss were associated with
several complications in multivariate analysis. In the NCDB, three-year overall survival
increased by 36.2% and 16.0% for patients with early and late stage disease (LSD),
respectively. In LSD patients, adjuvant chemoradiotherapy increased from 8.3% to 36.4%.
Later year of diagnosis (hazard ratio [HR] 0.76), neck dissection (HR 0.90), and negative
margins (HR 1.00) were associated with better overall survival (all p≤.002). Many
patients with oral cavity cancers experience postoperative complications, some of which
occur post-discharge. Early follow-up should be sought for high-risk patients. Long-term
prognosis for oral cancers has increased dramatically, as has the administration of
adjuvant chemoradiotherapy in LSD. Numerous sociodemographic, clinical, and
treatment variables may account for this difference in survival.

3
Acknowledgements:
I would like to thank Dr. Benjamin L. Judson for his mentorship and guidance,
the department of surgery for their generous financial support, and the section of
otolaryngology for demonstrating the interplay of research, education, and clinical
medicine at the highest levels. Additionally, the members of the office of student research,
namely Mae Geter and Donna Carranzo, have been instrumental in securing funding and
ensuring that my research needs have been met throughout the years. I would also like to
thank my family and friends for their support and understanding throughout my academic
career. These projects were funded by the NCATS CTSA-TL1 and James D. Hirsch
Medical Student Research Fellowships. Two published manuscripts serve as the basis for
this work, with permissions to reproduce text and images secured by the publishers:
Schwam ZG, Sosa JA, Roman SA, Judson BL. Complications and mortality
following surgery for oral cavity cancer. Laryngoscope 2015;125:1869-73 (1).
Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity
squamous cell carcinoma: Analysis of the National Cancer Database 1998-2006.
Oral Oncol 2016;52:45-51 (2).

4
Table of Contents
Introduction………………………………………………………………………...p.1-11
Purpose and Aims…………………………………….…………………………...p.11-12
Methods…………...…………………………………………………………….…p.12-18
Results……………………….…………………………….……………………….p.18-42
Discussion……………………………………………………………………….....p.42-52
Conclusions……………………………………….…………………………….....p.52-53
References…………………………………………………………………………p.54-77

1
Introduction
Sub-sites and lymphatic drainage patterns of the oral cavity
The oral cavity is composed of seven sub-sites, namely the lip, oral tongue,
alveolar ridge, retromolar trigone, floor of mouth, buccal mucosa, and hard palate (3).
While the anatomy and lymphatic drainage of the oral cavity is varied and complex, some
patterns have emerged in terms of sites of nodal metastases from oral cancers. In a
review of 1,081 patients at Memorial Sloan Kettering Cancer Center undergoing radical
neck dissections between 1965 and 1986, 562 neck dissections were performed for oral
cavity malignancies (4). In those patients, lymph node metastases were found to
predominate in cervical lymph node levels I, II, and III, and were rarely found in levels
IV or V. “Skip lesions” were also not observed, in that any patients with level V nodal
metastases also had metastases in levels I-IV.
Epidemiology of oral cancer
It is estimated that 59,340 new primary cancers of the head and neck were
diagnosed in the United States in 2015, with 12,290 associated deaths (5). Primary
tumors of the oral cavity were estimated to cause over 30,000 of those cases (51%) and
nearly 6,000 (49%) deaths. Oral cavity cancer is also common worldwide, and is the
fifteenth most common malignancy according to the World Health Organization (6). Oral
cancers are more common in men, which is thought to be secondary to higher rates of
tobacco and alcohol use, as well as greater exposure to sunlight via outdoor occupations
in the case of lip cancer (7). Oral cancer is predominantly a disease of middle age, with
only 6% of cases reported in patients under 45 years of age (8). The median age at

2
diagnosis in the United States was 62.0 years between years 2000 and 2004 (6,9),
although there are reports of an increasing incidence of oral tongue squamous cell
carcinoma in young white males aged 20-44 years (10).
Risk factors for developing oral cavity squamous cell carcinoma
Risk factors for the development of oral cavity cancer have been well-
characterized, and overlap with those of many of the other head and neck sub-sites.
Tobacco and alcohol use have been associated with the development of many head and
neck cancers, and have been estimated to cause nearly three-quarters of oral cavity cancer
cases (11). Tobacco is found in many forms, with cultural differences in its consumption
related to distinct anatomic locations of lesions within the oral cavity. Dipping snuff is
common in the Southern United States, and has been associated with a 50-fold higher
incidence of buccal and gingival lesions (12). Similarly, the large percentage of the
population in Bombay, India that chews pan, a tobacco derivative, contributes to very
high rates of buccal cancers (13). Additionally, hard palate carcinomas are particularly
common amongst Indian women who engage in “reverse chutta smoking,” in which the
lit end of a cigar is placed inside the mouth (14). Smoking cigarettes, pipes, and cigars
have also linked to the development of oral cavity cancers, with pipe and cigar smokers at
higher risk of developing oral cancers than cigarette smokers (15). Tobacco products all
exhibit a dose-response tumorigenic effect (16), with polycyclic aromatic hydrocarbons
(PAHs), nicotine-derived nitrosamine ketones (NNKs), and N-nitrosonornicotine (NNN)
creating DNA adducts in addition to oxidative damage by nitric oxide and quinones (17).
Tobacco use is not only linked to development of head and neck squamous cell
3
carcinomas, but is also associated with more aggressive disease; patients with a history of
tobacco use are more likely to have regional metastases and extracapsular spread when
compared to those without such a history (18).
Worldwide, 3.6% of cancers are related to alcohol consumption, notably the oral
cavity, pharynx, larynx, liver, breast, esophagus, and colon (19). Ethanol consumption
has been observed to have a dose-response effect, with a progressively higher relative
risk of developing oral cancer with increasing ethanol intake. In certain case-control
studies, drinking ≥6 whiskey-equivalents daily had a higher relative risk than did
smoking ≥40 cigarettes daily on the development of oral carcinomas (20). While the
exact mechanism behind ethanol’s association is as of yet unknown, it is thought to
behave synergistically with tobacco through a direct topical effect (13,21). Mechanisms
proposed include mucosal exposure to high concentrations of acetaldehyde, a breakdown
product of ethanol generated by oral bacteria (19,22) that interferes with DNA synthesis
and repair by binding to enzymes involved in cytosine methylation and glutathione
production (19,23,24). Acetaldehyde also binds to DNA, forming mutagenic adducts
(25). Oral acetaldehyde concentrations have been found to be higher in smokers, with the
theory that smoking somehow shifts the native flora to more acetaldehyde-producing
species (26). Cigarette smoke itself has also been found to have rather high
concentrations of acetaldehyde.
Cancers of the lip have a distinct epidemiological pattern when compared to those
of the oral cavity, with additional risk factors including exposure to sunlight, pipe

4
smoking, fair complexion (27), and immunosuppression (28). Pipe smoking is thought to
cause lip cancer through multiple mechanisms, including mechanical irritation, thermal
injury, and chemical exposure (3,29). In Australia, Canada, and Spain, lip cancer is the
most common sub-site of the oral cavity (30). It is important to distinguish cancers of the
lip from surrounding sub-sites, notably the buccal mucosa and adjacent skin.
Additional risk factors for cancer of the oral cavity include poor dental hygiene,
(specifically not brushing one’s teeth every day) and wearing ill-fitting dentures that have
caused sores (31). While the effects of poor dentition can be measured, they tend to be
greatly outweighed by the effects of tobacco and alcohol (32).
Histology common to oral cancers
In an analysis of the National Cancer Database (NCDB) examining 58,976
patients with oral cancer, the most common subtypes were found to be squamous cell
carcinoma (86.3%), adenocarcinoma (5.6%), and verrucous carcinoma (2.0%). The
remaining were split evenly by carcinoma not otherwise specified, lymphoma, Kaposi
sarcoma, and “other” (33).
While conventional squamous cell carcinoma is the most common subtype,
multiple variants can be found within the oral cavity, including sarcomatoid, basaloid,
and verrucous squamous cell carcinoma (3). Sarcomatoid squamous cell carcinoma stains
positively for keratin, has squamous cells intermingling with spindle-type cells, and has a
similar overall survival to that of conventional squamous cell carcinoma. There is,

5
however, a higher rate of locoregional recurrence (34). Basaloid squamous cell
carcinomas typically have basaloid cells, prominent peripheral nuclear palisading (35),
and have a predilection for the oral tongue (36). Basaloid lesions tend to have similar
survival curves to moderate to poorly differentiated squamous cell carcinomas (36). In
verrucous lesions, which are commonly found on the buccal mucosa, there is typically a
thick zone of non-proliferating and non-keratinizing cells. It is considered low-grade in
nature and resistant to radiation (3). Numerous additional pathologies of the oral cavity
may be found, including minor salivary gland tumors, melanoma, sarcomas (including
Kaposi’s sarcoma), lymphoma, and granulomas.
Treatment options and factors affecting treatment
The treatment of oral cavity (including lip) cancers is guided by clinical and
pathological staging information, presence of high-risk pathologic features, and success
of surgical resection. Surgical resection of the primary is the backbone of treatment, with
elective or therapeutic neck dissection based on presence of clinically positive nodes,
tumor thickness, or the results of sentinel lymph node biopsy. Adjuvant radiotherapy can
be considered in the case of having one positive node without having adverse features,
but is indicated and frequently combined with chemotherapy if there is extracapsular
extension, positive margins, or other adverse features such as pathologic T3/T4
classification, N2/N3 nodal disease, nodal disease in levels IV or V, as well as perineural
and lymphovascular invasion. Definitive radiotherapy is also an option in the case of
small lesions without nodal metastases, with salvage surgery reserved for recurrence (37).

6
Presence of nodal metastasis is an important prognostic factor in oral cancers; as a
result, there has been much effort to determine predictors of occult nodal metastases in
the clinically negative neck (38,39), with rates of occult nodal metastases in T1/T2
lesions as high as 27-40% (40,41,42). Tumor thickness is thought to reflect proximity to
lymphatic and vascular structures (43) and to approximate aggressiveness of tumor
growth (44). It has also been postulated that tumor emboli are more apt to spread along
the wider lymphatic channels located in the deeper aspects of the tissue (45). Tumor
thickness ≥4mm is considered to be an indication for elective neck dissection, as 4.5% of
patients are expected to have occult metastases with a thickness of 4mm, while 16.6%
have them with a cutoff of 5mm (46). A recent randomized control trial of node-negative
oral cancer patients demonstrated a superior overall and disease-free survival for patients
undergoing elective as compared to therapeutic neck dissection (47).
Reconstruction after oncologic resection
For small lesions of the oral cavity, primary closure, placement of a split-
thickness skin graft, or healing by secondary intention may be considered. Larger lesions
may require free-tissue transfer or a regional pedicle flap, and are dependent on surgeon
preference and ability as well as patient expectations (3).
Effects of disease and treatment on quality of life
The oral cavity is an integral anatomic region, playing important roles in speech,
deglutition, taste, salivation, and mastication. As a result, tumor-induced dysfunction as
well as treatment-related effects may have a profound impact on a patient’s day-to-day

7
functioning. Numerous factors have been found to affect quality of life in oral cavity
cancer patients, including the site of tumor, tumor size, depressive symptoms, pre-
operative performance status, method of reconstruction, and whether a patient underwent
neck dissection (48). While there have been articles reporting no effect of tumor site on
quality of life, it has also been demonstrated that more posterior tumors may have a
profound effect based on the impact on deglutition (49). Similarly, larger tumors and
overall stage are often associated with worse pain and physical symptoms, especially
when treated with multimodality therapy (48, 50). Anxiety and depression are prevalent
among those with oral cancers (51), and disfigurement often leads to changes in self-
perception, isolation, and problems with partners (52).
Much attention has been paid to the effect of surgical reconstruction on quality of
life, with some authors reporting that primary closure and laser surgery have superior
outcomes to free-flap reconstruction one year post-operatively (48,49). In a prospective
trial examining quality of life after free tissue transfer for oropharyngeal cancer
reconstruction, an initial decline in performance was observed, but recovered by 6
months. Mental health and emotional indices were superior to pre-treatment levels at one
year post-operatively (53). No differences in quality of life measures have been noted in
post-maxillectomy patients undergoing reconstruction with a free flap versus obturator
(54), or for bony free flap versus marginal mandibulectomy in resection of large
mandibular tumors (55). Extent of neck dissection has also been related to postoperative
shoulder dysfunction and pain, most notably in patients undergoing bilateral neck
dissections of levels I-IV or any dissection including level V (56).

8
Synchronous and metachronous tumors
Patients with head and neck squamous cell carcinomas have or develop a second
primary in 10-40% of cases, with common sites including the head and neck, esophagus,
and lung (57). Synchronous lesions are those that are diagnosed within 6 months of the
initial cancer, and metachronous lesions occur after the 6-month window has passed.
Panendoscopy of the upper aerodigestive tract and the tracheobronchial tree at the time of
diagnosis routinely yields a second primary tumor in 9-14% of cases (58,59). Up to 33%
of patients with oral cavity primaries have been found to have second primaries, with
most being found in the oral cavity, pharynx, larynx, lung, and esophagus (58). The risk
of developing a second oral cancer is highest in patients with primaries of the gingiva,
floor of mouth, and buccal mucosa, with gingival and floor of mouth primaries most
likely to have their second lesions in the lung (60,61,62). Identification of a second
primary was linked to a substantial decrease in five-year overall survival from 26.9% to
15.2% in one series (63).
Role of adjuvant therapy in treating oral cancer
Before 2004, locoregionally advanced head and neck squamous cell carcinoma
was typically treated with surgical resection and adjuvant radiotherapy. With this
treatment algorithm, rates of locoregional recurrence, distant metastasis, and five-year
overall survival rates were 30%, 25%, and 40%, respectively (64,65). The Radiation
Therapy Oncology Group (RTOG) 9501 and European Organization for Research and
Treatment of Cancer (EORTC) 22931 trials, which were both published in 2004, showed

9
a significant improvement in disease-free survival and locoregional control for high-risk
and late stage head and neck cancer patients. The two trials, however, had discordant
results with respect to overall survival, with EORTC 22931 showing a significant
improvement, and RTOG 9501 only demonstrating minimal improvement (2,66,67).
While different end-outcomes and definitions of “high risk” were used, a combined
follow-up analysis demonstrated the greatest benefit of adjuvant chemoradiotherapy to be
in those with positive margins or ECE (2,65).
Effect of screening in oral cancer
Currently, the United States Preventive Services Task Force maintains that there
is insufficient evidence for routine oral cancer screening in asymptomatic adults (68).
While routine oral cancer screening has not gained traction in the United States, there has
been some success on an international level. In a longitudinal screening program in
Kerala, India, nearly 200,000 people were randomized to either undergo serial visual
screenings or be placed in a control group over a thirteen-year period. While a reduction
of 12% in oral cancer mortality did not reach significance when all patients were
combined, tobacco/alcohol users in the serial screening group had a 38% lower incidence
of oral cancer and 81% lower oral cancer mortality when compared to patients in the
control group (69). Other efforts have focused on salivary biomarker detection in high-
risk patients (70), as well as autofluorescence visualization devices, cytological brush
tests (71), and differential gene expression using microarrays (72).
Current literature on short term outcomes and long term prognosis

10
The five-year relative survival rates for many head and neck cancers have
improved over the years, with increases from 53% (1975-77) to 66% (2004-10) for oral
cavity and pharyngeal primaries (5). This is in contrast to laryngeal primaries, which
have seen a significant decrease in their five-year relative survival from 66% to 63% over
the same period. This may be due to roughly two-thirds of head and neck cancer patients
presenting with advanced disease (73), and between 4-25% eventually developing distant
metastases. It has been found that between 7% and 12% have distant metastases at
presentation (73,74,75). Even in light of advances in diagnostic imaging and methods
and increased awareness, the proportion of head and neck cancer patients presenting with
Stage IV disease has not changed appreciably since 1990 (76).
Data on changes in prognosis of oral cavity malignancies are varied, with some
reports stating that the five-year survival rate has remained relatively stable over several
decades at 50-55%, with variations based on several variables including race and gender
(77,78,79). Oral cavity sub-site has also been shown to have prognostic value, with
cancers of the oral tongue showing a worse overall and cause-specific survival when
compared to other oral sub-sites (80). The long-term prognosis for lip cancer, however,
is excellent, with five-year survival rates of 95% (77,79). These data are in contrast to an
international cohort study from seven leading cancer centers that demonstrated a
significant improvement in survival for oral cancer patients (81), and a report from
Memorial Sloan Kettering Cancer Center showing a significant increase in survival for
oral tongue cancers between 1978 and 1987 (82).

11
Unfortunately, postoperative complications are rather common in head and neck
cancer patients, with reported complication rates as high as 53% (83,84,85,86). Wound
infections at the surgical site are the most common (85) in the literature, with risk factors
including neoadjuvant therapy (86), advanced disease (83,84,85), comorbidity, and neck
dissection (83). In a retrospective review of 1,693 Taiwanese oral cavity cancer patients
undergoing primary resection, the wound infection rate was found to be 19.8%, with risk
factors including diabetes, flap reconstruction, and low postoperative serum albumin
level (83). Thirty-day readmission and mortality has been reported using the NCDB for
patients with oral cavity squamous cell carcinoma (87), and Chen et al. have examined
postdischarge complications for all otolaryngology procedures in the NSQIP (88). As
postdischarge complications are one of the most important contributors to readmission
(89) and may delay the receipt of critical adjuvant therapies, investigating them remains
critical.
Purpose, aims, and hypotheses
The purpose of this study was multifold, and included characterizing both short-
term morbidity and mortality outcomes as well as long-term changes in prognosis for
patients with cancers of the oral cavity using large administrative datasets. We
hypothesized that clinical and demographic variables such as age and various
comorbidities would affect short-term postoperative morbidity and mortality, and sought
to characterize modifiable risk factors to predict which patient populations were at
highest risk. It was also our aim to characterize the time course of postoperative and post-
discharge complications (1). While we anticipated the majority of complications to occur

12
during admission, we believed that certain adverse events would tend to occur after
discharge. In identifying risk factors for postoperative adverse events, we predicted that
more preoperative comorbidity would be re associated with more morbidity and mortality
postoperatively. In investigating the long-term prognosis for patients with oral cavity
squamous cell carcinoma, we predicted that three-year overall survival would increase
over the study period, and would likely be associated with the administration of adjuvant
therapies, superior surgical techniques as measured by rates of negative margins, as well
as socio-demographic and oncologic variables such as age, cancer stage, and the category
of treatment center (2).
Methods
Division of responsibility
All procedures, methods, and statistical analyses were performed principally by
the first author. This included selecting the cohort, choosing inclusion and exclusion
criteria, recoding and redefining variables, univariate and multivariate analysis, creation
of tables and figures, and authorship of the manuscript. Data interpretation was chiefly
performed by the first author with assistance from the faculty advisor.
Description of the National Surgical Quality Improvement Program§
To characterize and determine the timing of postoperative complications
following oncologic resection of oral cavity malignancies, we utilized the American
§Adapted with permissions from: Schwam ZG, Sosa JA, Roman SA, Judson BL. Complications and mortality
following surgery for oral cavity cancer: analysis of 408 cases. Laryngoscope 2015;125:1869-73.

13
College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP)
Participant Use Data File (PUF) to examine data from patients undergoing surgery
between 2005 and 2010 (1). The NSQIP collects data from over 400 participating sites,
and is prospective, risk-adjusted, and validated against claims data in recording major
postoperative complications (1,90,91). The NSQIP is the only national dataset of its kind.
Data on 135 variables detailing preoperative patient characteristics and comorbid
conditions, intraoperative processes, and postoperative morbidity and mortality are
carefully recorded by a Surgical Clinical Nurse Reviewer at each site, and data are not
limited to in-hospital events (1,92,93,94). Due to a robust auditing and training process,
the inter-rater reliability of variables in the database has improved over the years,
ensuring standardization of data inputs (95). The NSQIP clinical reviewers rely on an
eight-day cycle in which representative cases are selected from the operative logs to
ensure lack of bias in selection; using this process, cases “have an equal chance of being
selected from each day of the week (96).”
Description of the National Cancer Database†
The NCDB was used to determine changes in long-term prognosis of patients
with oral cavity squamous cell carcinoma diagnosed between years 1998-2006. The
NCDB is a joint venture of the American Cancer Society and the Commission on Cancer
(CoC) of the American College of Surgeons, and has been in existence since 1989 (2,97).
It accounts for more than 1440 CoC-approved cancer program registries (2,76,98),
approximately 75% of cancers diagnosed in the United States, and is the pre-eminent
†Adapted with permissions from Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity squamous
cell carcinoma: analysis of the National Cancer Database 1998-2006. Oral Oncol 2016;52:45-51.

14
oncologic database in the United States. The NCDB uses the same definitions and
standards as federal cancer registry systems (99), with coding guidelines found in the
Registry Operations and Data Standards (100) and Facility Oncology Registry Data
Standards manuals (2,101). Data is collected on socio-demographic, clinical, oncologic,
and treatment-related variables.
Selection criteria using the ACS NSQIP§
The NSQIP was queried by International Classification of Diseases-9th edition
(ICD-9) codes (102), selecting for malignant lesions of the oral cavity: 141.1-141.5,
144.0, 144.1, 144.8, 144.9, 145.0-145.2, 145.6, 145.8, and 145.9 (1). The following
Current Procedural Terminology (CPT) codes were then included in the analysis either as
the principal or concurrent procedure: 21025, 21026, 21034, 21040, 21044, 21045, 21050,
21198, 21299 (bony excision), 21557 (radical tumor resection), 31225 (maxillectomy),
41116 (excision from floor of mouth), 40810, 40812, 40814, 40816, 40899 (excision
from vestibule of mouth), 41110, 41112, 41114, 41120, 41130, 41135, 41140, 41145,
41599 (excision of tongue lesion, glossectomy with or without neck dissection), 41150,
41153, 41155 (glossectomy as part of composite procedure, with or without neck
dissection), 41825, 41827, 41830 (excision of dento-alveolar structures), 42104, 42106,
42107, 42120, 42140, 42160, 42299 (excision or destruction palatal or uvular lesion),
42415 (excision of parotid tumor), 42842, 42844, and 42845 (radical resection of
retromolar trigone with or without flap reconstruction) (1,103).
§Adapted with permissions from: Schwam ZG, Sosa JA, Roman SA, Judson BL. Complications and mortality
following surgery for oral cavity cancer: analysis of 408 cases. Laryngoscope 2015;125:1869-73.

15
Preoperative and intraoperative variables in the NSQIP§
Definitions of variables included in the database are described in the ACS-NSQIP
user guide (104) with several modifications (1). “Pulmonary comorbidity” was defined
as having dyspnea on exertion or at rest, a history of chronic obstructive pulmonary
disease, or being ventilator-dependent. “Cardiovascular comorbidity” was defined as a
history of congestive heart failure, angina, myocardial infarction (MI), peripheral
vascular disease, percutaneous coronary intervention, or cardiac surgery. “Poor
functional status” prior to surgery was defined as being either partially or totally
dependent on others for activities of daily living. Neck dissection was determined by the
following CPT codes (1,103): 38542 (dissection of deep jugular nodes), 38700, 41153
(suprahyoid neck dissection), 38720, 38724, 41135, 41155, and 42426 (includes
complete lymphadenectomy, modified radical neck dissection, radical neck dissection, or
neck dissection in addition to another procedure). Cases in which neck dissection was the
only procedure performed were excluded from analysis (1).
Postoperative outcomes in the NSQIP§
Complications and adverse events analyzed included surgical-site (superficial,
deep, and organ-space, and wound-dehiscence), infectious (urinary tract infection,
pneumonia, sepsis, and septic shock), respiratory (re-intubation, failure to wean, or
ventilator use >48 hours), renal (acute renal insufficiency or acute renal failure), and
cardiovascular complications (myocardial infarction, cardiac arrest, or stroke), as well as
flap failure, venous thromboembolism (deep venous thrombosis or pulmonary embolism),
§Adapted with permissions from: Schwam ZG, Sosa JA, Roman SA, Judson BL. Complications and mortality
following surgery for oral cavity cancer: analysis of 408 cases. Laryngoscope 2015;125:1869-73.
16
reoperation, and death (1,105).
Selection Criteria using the NCDB†
We extracted oral cancer patient data from the NCDB using the following
International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) (2,106)
topography codes: C00.0, 00.1, 00.2, 00.3, 00.4, 00.5, 00.6, 00.8, 00.9 (Lip), 02.0, 02.1,
02.2, 02.3, 02.8, 02.9 (oral tongue), 03.0, 03.1, 03.9 (gingiva and alveolus), 04.0, 04.1,
04.8, 04.9 (floor of mouth), 05.0, 05.8, 05.9 (hard palate), 06.0, 06.1 (buccal mucosa),
06.2 (retromolar trigone), 06.8, and 06.9 (other and unspecified mouth). We then
selected for patients with squamous cell carcinomas using the following ICD-O-3
morphology codes 8051, 8052, 8070-8076, 8078, 8083, and 8084 (2,105). Patients with
T0, TX, Tis, and NX lesions as well as those with Stage 0 disease were excluded.
Staging information reflects the American Joint Committee on Cancer (AJCC) staging
system, 5th (1998-2002) and 6th editions (2003-2006) (107,108). Patients with incomplete
information for the following variables of interest were not included in our analyses:
patient gender, age, race, Hispanic origin, insurance status, facility type, TNM
classifications and overall stage, information on first course of treatment (surgery,
chemotherapy, radiation, surgical margins, scope of regional lymph node surgery), last
contact/death, and vital status at follow-up (2).
Variable definitions in the NCDB†
†Adapted with permissions from Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity squamous
cell carcinoma: analysis of the National Cancer Database 1998-2006. Oral Oncol 2016;52:45-51.
†Adapted with permissions from Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity squamous
cell carcinoma: analysis of the National Cancer Database 1998-2006. Oral Oncol 2016;52:45-51.
17
Variable definitions are as defined in the NCDB data dictionary (109), with some
exceptions. Patients were coded as diagnosed in years 1998-2003 or 2004-2006, as the
landmark RTOG 9501 and EORTC 22931 trials involving the use of adjuvant therapy in
head and neck cancer were first published in 2004 (2,65,66,67). Hispanic origin was
combined with race, and those of Hispanic origin were labeled “Hispanic.” Insurance
status was stratified into private, uninsured/Medicaid, and Medicare/other government.
Facility type was divided into Academic/Research Cancer Programs (ARPs) and non-
ARPs (87). Facility volume was categorized as high or low, with high-volume centers
treating ≥22 patients (≥90th percentile) over the study period. All patients underwent
surgical resection of the primary site, and some received adjuvant radiation or
chemoradiation. Surgical margins were characterized as being negative
(microscopically) or positive (micro- or macroscopically, or unspecified). Patients who
underwent regional lymph node surgery were coded as having received a neck dissection
(87). High-risk pathologic features such as tumor depth, perineural invasion, and
extracapsular extension are not available for the vast majority of patients in the database;
therefore these variables could not be analyzed. Data regarding Charlson comorbidity
index was only available for patients diagnosed years 2003-2006, and was therefore not
examined (2).
Statistical analysis§†
§†Adapted with permissions from:
Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity squamous cell carcinoma: analysis of the
National Cancer Database 1998-2006. Oral Oncol 2016;52:45-51.
Schwam ZG, Sosa JA, Roman SA, Judson BL. Complications and mortality following surgery for oral cavity cancer:
analysis of 408 cases. Laryngoscope 2015;125:1869-73.

18
Statistical analysis was performed with SPSS version 22.0.0 (Chicago, IL).
Standard descriptive statistics were used to summarize patient demographic and disease-
related data. Cases with missing data for variables of interest (<5%) were removed from
the NSQIP cohort. Extreme outliers were removed in calculating summary statistics if
values fell three times the interquartile distance from the 75th percentile value. Chi-square,
Kaplan-Meier, and Cox proportional hazards regression analyses were performed, and
only variables with p≤.10 in univariate analyses were included in multivariate models.
All tests were two-sided, and final threshold for significance was set at p≤.05. Temporal
trends in the first course of treatment and three-year overall survival were depicted using
Prism Graphpad 6.0 (La Jolla, CA), and Pearson product-moment correlation coefficients
were calculated to determine the temporal associations between different treatment
modalities and overall survival. Correlation coefficients range from -1 to +1, which
represent perfect negative and positive linear correlations, respectively. This study was
granted exemption by our institutional review board, as both the NSQIP and NCDB are
de-identified datasets (1,2).
Results
Patient demographics and clinical characteristics in the NSQIP
In querying the NSQIP to identify cases of oral cavity cancer undergoing primary
resection in addition to other procedures, 408 cases were identified. The oral tongue
(40.7%), floor of mouth (21.8%), buccal mucosa (7.1%), retromolar trigone (6.1%), and
hard palate (4.9%) were the most common oral cavity sub-sites (1).

19
The majority of patients were male, between the ages of 45-79 years, and
Caucasian (Table 1). Many had significant comorbid conditions, including diabetes,
tobacco use within the year prior to surgery, heavy alcohol use, prior strokes/transient
ischemic attacks, and hypertension. Few patients received neoadjuvant chemotherapy or
radiotherapy for their disease. Steroids for a chronic condition and poor functional status
prior to surgery were uncommon comorbidities. Weight loss greater than 10% over the
six months prior to surgery occurred in just under 7% of patients, and 3% of patients had
a procedure performed within the 30 days prior to surgery. Neck dissection was
performed in 38.2% of cases (1).

20
Table 1. Patient demographics and clinical characteristics from the NSQIPA
% (N=408)B
Sex
Male 60.0 (245)
Female 40.0 (163)
Age (years)
18-44 7.8 (32)
45-64 43.4 (177)
65-79 34.6 (141)
≥80 14.2 (58)
Race
Caucasian 83.8 (295)
Black 10.2 (36)
Hispanic 2.6 (9)
Asian 3.4 (12)
BMI
<18.5 22.3 (90)
18.5-24.9 38.6 (156)
25.0-29.9 33.7 (136)
≥30.0 5.4 (22)
ASA classification
1 2.5 (10)
2 29.7 (121)
3 63.7 (260)
4 4.2 (17)
A Reproduced with permission from: Schwam ZG, Sosa JA, Roman SA, Judson BL. Complications and mortality
following surgery for oral cavity cancer: analysis of 408 cases. Laryngoscope 2015;125:1869-73. B Numbers may not add to total due to missing data

21
Diabetes 11.8 (48)
Current smoker 32.8 (134)
Heavy alcohol use 9.1 (37)
Pulmonary comorbidity 15.7 (64)
Cardiovascular
comorbidity
11.5 (47)
Hypertension 52.5 (214)
Prior stroke/TIA 8.3 (34)
Neoadjuvant
chemotherapy
1.0 (4)
Neoadjuvant XRT 2.0 (8)
Chronic steroids 3.2 (13)
Coagulopathy 2.7 (11)
Poor functional status 4.2 (17)
Significant weight loss
prior to surgery
6.6 (27)
Operation within prior
30 days
3.0 (12)
Abbreviations: NSQIP=National Surgical Quality Improvement Program, BMI=body mass index,
ASA=American Society of Anesthesiologists, TIA=transient ischemic attack, XRT=radiotherapy

22
30-day postoperative complications and adverse events
The overall thirty-day complication rate was 20.3%, and four patients (1.0%) died within
30 days of surgery (Table 2). The most common adverse events were reoperation as well
as infectious, respiratory, and surgical-site complications. Graft failure, venous
thromboembolism, cardiovascular, and renal complications occurred infrequently.
Unfortunately, detailed information regarding the type of graft (split-thickness skin graft
versus pedicle or free flap) was not available in the database. The majority of
complications occurred between postoperative day (POD) two and ten, although most
venous thromboembolic events and renal insufficiency occurred much later (median 22.0
and 22.5 days, respectively) (1).

23
Table 2. Complications and adverse events within 30 days of surgeryA
% (n)B
Overall 20.3 (83)
Reoperation 9.6 (39)
Infectious 6.6 (27)
Respiratory 5.1 (21)
Surgical-site 4.7 (19)
Flap failure 2.2 (9)
VTE 1.7 (7)
Cardiovascular 1.5 (6)
Renal 1.2 (5)
Death 1.0 (4)
Abbreviations: VTE=venous thromboembolism
A Reproduced with permissions from: Schwam ZG, Sosa JA, Roman SA, Judson BL. Complications and mortality
following surgery for oral cavity cancer: analysis of 408 cases. Laryngoscope 2015;125:1869-73. B Numbers do not add to total due to some patients experiencing multiple complications

24
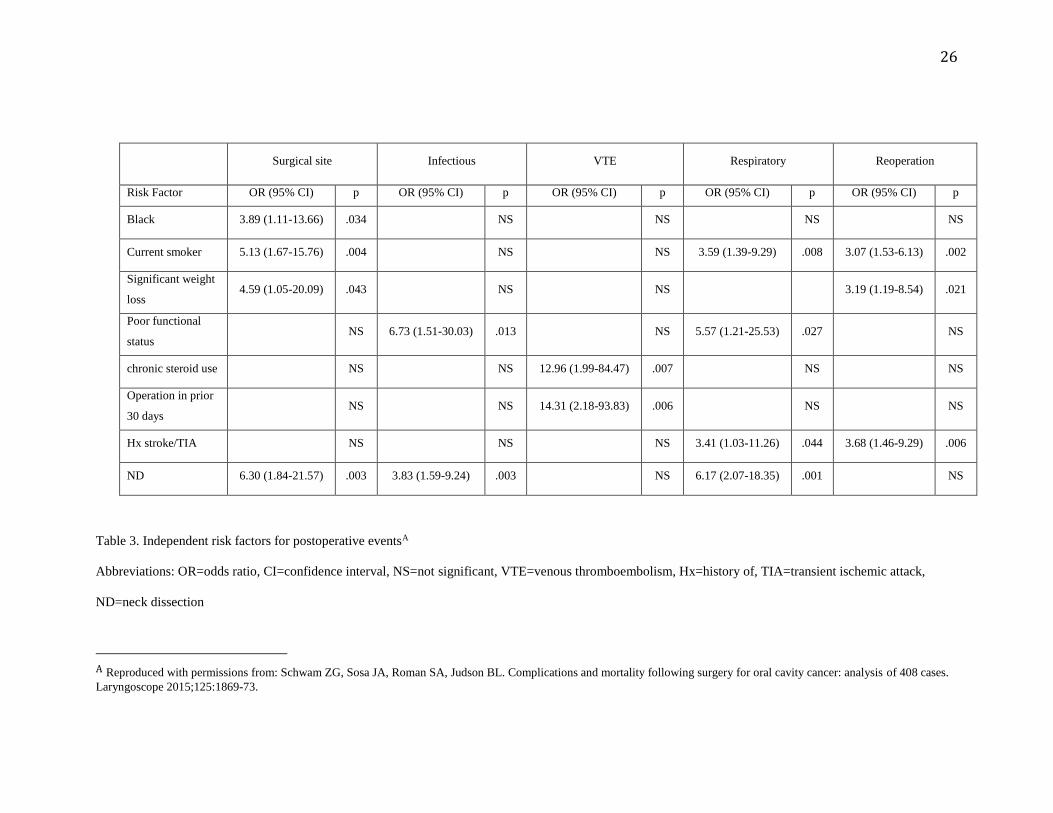
Preoperative risk factors for 30-day postoperative adverse events
While several preoperative variables were identified as risk factors for
experiencing an adverse event postoperatively, some were linked to a variety of
complications in multivariable analysis (Table 3). Being a smoker within the year prior
to surgery was associated with surgical-site and respiratory complications as well as
reoperation. Undergoing neck dissection was associated with graft failure [odds ratio
[OR] 16.97, 95% confidence interval [CI] 1.78-161.44], surgical-site, infectious, and
respiratory complications, and was associated with an adverse event of any type in
univariate analysis (32.7% versus 12.7%, p<.001). Poor functional status predisposed
patients to infectious and respiratory events, and steroid use for a chronic condition was
the only risk factor for thirty-day mortality (OR 56.44, 95% CI 2.03-1569.28]. There
were no independent risk factors identified for cardiovascular or renal complications (1).
Length-of-stay and post-discharge complications
The median and mean length-of-stay were found to be 3.0 and 4.8 days,
respectively. Patients who experienced an in-hospital adverse event had a significantly
longer inpatient admission (mean 14.8 versus 3.1 days, p<.001). While most adverse
events occurred within the hospital, twenty patients (4.9%) experienced 17.3% of all
complications in the post-discharge time period. A significant proportion of surgical-site
complications (42.1%), sepsis (20.0%), flap failure (22.2%), deep venous thrombosis
(33.3%), and death (25.0%) occurred after admission. While the vast majority (91.3%) of
post-discharge complications occurred by post-discharge day 14, 52% of post-discharge

25
wound dehiscences and 67% of surgical site infections occurred by post-discharge day 7
(1).
26
Table 3. Independent risk factors for postoperative eventsA
Abbreviations: OR=odds ratio, CI=confidence interval, NS=not significant, VTE=venous thromboembolism, Hx=history of, TIA=transient ischemic attack,
ND=neck dissection
A Reproduced with permissions from: Schwam ZG, Sosa JA, Roman SA, Judson BL. Complications and mortality following surgery for oral cavity cancer: analysis of 408 cases.
Laryngoscope 2015;125:1869-73.
Surgical site Infectious VTE Respiratory Reoperation
Risk Factor OR (95% CI) p OR (95% CI) p OR (95% CI) p OR (95% CI) p OR (95% CI) p
Black 3.89 (1.11-13.66) .034 NS NS NS NS
Current smoker 5.13 (1.67-15.76) .004 NS NS 3.59 (1.39-9.29) .008 3.07 (1.53-6.13) .002
Significant weight
loss 4.59 (1.05-20.09) .043 NS NS 3.19 (1.19-8.54) .021
Poor functional
status NS 6.73 (1.51-30.03) .013 NS 5.57 (1.21-25.53) .027 NS
chronic steroid use NS NS 12.96 (1.99-84.47) .007 NS NS
Operation in prior
30 days NS NS 14.31 (2.18-93.83) .006 NS NS
Hx stroke/TIA NS NS NS 3.41 (1.03-11.26) .044 3.68 (1.46-9.29) .006
ND 6.30 (1.84-21.57) .003 3.83 (1.59-9.24) .003 NS 6.17 (2.07-18.35) .001 NS

27
Changes in patient demographics, clinical characteristics, and survival by year of
diagnosis in the NCDB
After applying the several inclusion and exclusion criteria to patient records from
the NCDB, 13,655 patient records were available for analysis. Patients were divided into
two cohorts based on year of diagnosis: those diagnosed 1998-2003 (n=7,734) and those
diagnosed in 2004-2006 (n=5,921). The overall median follow-up time was 43.6 months
(range 0.0-176.2 months), while the median follow-up times for those diagnosed 1998-
2003 and 2004-2006 were 33.9 months (range 0.0-176.2 months) and 55.1 months (0.0-
106.9 months), respectively (2).
Patients diagnosed in the later cohort were younger, more often had private
insurance, and received their care in academic/research facilities and high volume centers
(Table 4). Patients diagnosed in 2004-2006 also had a higher proportion of T≤2 lesions,
N0 nodal disease, and early stage disease (Stages I and II). Negative surgical margins,
neck dissections, and adjuvant chemoradiotherapy were more often administered to
patients diagnosed in 2004-2006 (2).
Observed three-year overall survival improved significantly from 1998 to 2006
(21.7% to 50.9%, p<.001). Patients diagnosed from 2004-2006 were found to have a
median estimated survival of 88.2 months (95% CI 84.2-92.2 months), compared to 52.2
months (95% CI 49.6-54.7 months) in univariate Kaplan-Meier analysis (Figure 1) (2).

28
Table 4. Patient demographics and facility data stratified by year of diagnosisB
1998-2003 2004-2006
% (n=7,734) % (n=5,921) p
Sex
Male 62.6 61.3
.131
Female 37.4 38.7
Age (years)
18-64 50.8 56.4
<.001
≥65 49.2 43.6
Race
White 88.0 88.3
<.001
Black 6.0 4.3
Hispanic 2.1 3.0
Asian 3.4 3.7
Other 0.6 0.7
Insurance
Private 40.5 45.0
<.001
Uninsured/Medicaid 11.9 12.3
Medicare/other
government
47.5 42.6
Facility Type
ARP 42.4 51.7
<.001
Non-ARP 57.6 48.3
Facility Volume
Low 54.9 45.7 <.001
B Reproduced with permissions from Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity
squamous cell carcinoma: analysis of the National Cancer Database 1998-2006. Oral Oncol 2016;52:45-51.

29
High 45.1 54.3
T-classification
1 42.1 45.2
<.001
2 32.2 32.1
3 10.1 7.2
4 15.6 15.5
N-classification
0 78.2 79.6
.006
1 10.7 9.1
2 10.4 10.8
3 0.7 0.5
M-classification
0 99.6 99.6
.846
1 0.4 0.4
Overall Stage
I 39.4 42.4
<.001
II 24.7 25.0
III 13.5 10.7
IV 22.4 21.9
Treatment Regimen
Surgery alone 64.8 66.9
<.001 Surgery + RT 29.7 21.6
Surgery + CRT 5.4 11.5
Surgical Margins
Negative 85.8 88.2
<.001
Positive 14.2 11.8
Neck Dissection

30
No 49.6 47.2
.006
Yes 50.4 52.8
Abbreviations: ARP-Academic/Research Program, RT-Radiation Therapy, CRT-
Chemoradiation Therapy

31
Figure 1. Overall survival of all patients stratified by year of diagnosisB
B Reproduced with permissions from Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity
squamous cell carcinoma: analysis of the National Cancer Database 1998-2006. Oral Oncol 2016;52:45-51.
32
Changes in treatment patterns and survival by year of diagnosis and disease stage
Patients were characterized as having early or late stage (Stages III and IV)
disease, with the proportion of patients being diagnosed with early stage disease
increasing from 64.1% to 67.4% between the two time-based cohorts (p<.001). Patients
presenting with late stage disease were significantly different from early stage patients in
terms of demographics and several treatment variables; patients with later stage disease
were more frequently <65 years of age (57.8% versus 50.9%), uninsured/Medicaid
(18.8% versus 8.6%), non-white (17.3% versus 9.0%), and received their treatment in
high volume centers (59.0% versus 43.9%) (all p<.001) (2).
Treatment patterns for patients with early stage disease remained stable between
1998 and 2006 (Figure 2a); there was a 3.8% increase in the administration of adjuvant
chemoradiotherapy, and a 1.9% decrease in the administration of adjuvant radiotherapy.
Surgery followed by adjuvant radiotherapy had a negative temporal correlation with
three-year overall survival (Pearson coefficient -0.77, p=.016), whereas adjuvant
chemoradiotherapy was positively correlated with three-year overall survival (Pearson
coefficient 0.88, p=.002). There was a significant improvement for patients with early
stage disease in three-year overall survival from 23.5% to 59.7% over the study period
(p<.001) (2).
Early stage disease patients diagnosed in 1998-2003 had higher rates of positive
margins (11.0% versus 8.3%), treatment in a low volume center (61.1% versus 50.0%),

33
and age ≥65 years (52.1% versus 45.4%) (all p<.001). Neck dissections increased from
22.8% to 37.6% over the study period (p<.001) (2).
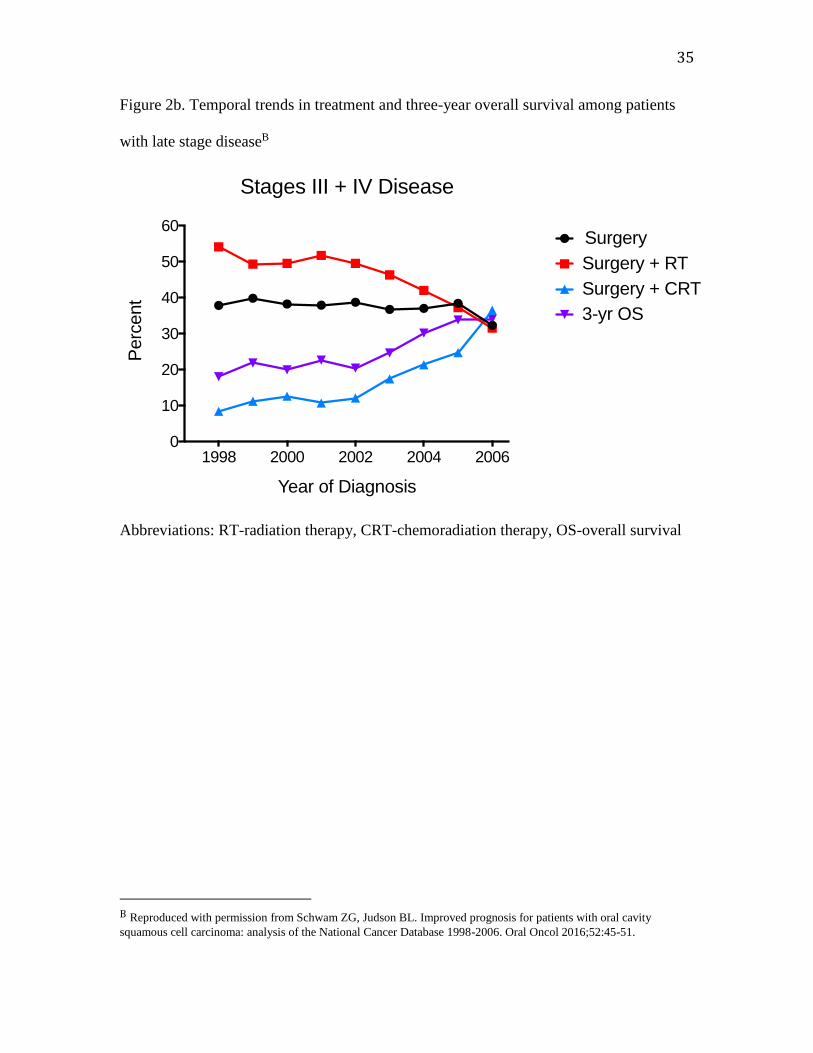
Patients with late stage disease saw a similar improvement in three-year overall
survival from 17.9% to 33.9% over the study period (Figure 2b). A strong, positive
temporal correlation was found between administration of adjuvant chemoradiotherapy,
which increased from 8.3% to 36.4%, and three-year overall survival (Pearson coefficient
0.92, p<.001). Receipt of adjuvant radiotherapy was observed to fall from 54.0% to
31.4%, and was negatively associated with survival (Pearson coefficient=-0.95, p<.001)
(2).
Late stage disease patients diagnosed from 2004 to 2006 were more often <65
years old (60.2% versus 56.0%, p=.004), more commonly had private insurance (40.9%
versus 37.5%, p=.008), received treatment in a high volume facility (63.1% versus 56.1%,
p<.001), and presented with Stage IV disease (67.0% versus 62.4%, p=.001). No
statistical difference was found in surgical margin status between the two periods
(p=.341) (2).

34
Figure 2a. Temporal trends in treatment and three-year overall survival among patients
with early stage diseaseB
Abbreviations: RT-radiation therapy, CRT-chemoradiation therapy, OS-overall survival
B Reproduced with permission from Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity
squamous cell carcinoma: analysis of the National Cancer Database 1998-2006. Oral Oncol 2016;52:45-51.
1998 2000 2002 2004 20060
10
20
30
40
50
60
70
80
90
100
Year of Diagnosis
Perc
ent
Stages I + II Disease
Surgery
Surgery + RT
Surgery + CRT
3-yr OS
35
Figure 2b. Temporal trends in treatment and three-year overall survival among patients
with late stage diseaseB
Abbreviations: RT-radiation therapy, CRT-chemoradiation therapy, OS-overall survival
B Reproduced with permission from Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity
squamous cell carcinoma: analysis of the National Cancer Database 1998-2006. Oral Oncol 2016;52:45-51.
1998 2000 2002 2004 20060
10
20
30
40
50
60
Year of Diagnosis
Perc
ent
Stages III + IV Disease
Surgery
Surgery + RT
Surgery + CRT
3-yr OS

36
Long-term prognostic factors in multivariable analysis
Several independent risk factors for mortality were identified in multivariable
analysis. Older age, insurance status, year of diagnosis, later stage at diagnosis,
administration of adjuvant chemoradiotherapy, and the presence of positive margins were
all associated with increased mortality in early and late stage disease patients, but also
when these two disease-based cohorts were combined (Table 5). Receiving treatment in
a high volume facility and undergoing neck dissection were associated with better overall
survival in early stage disease patients and when all patients were combined, but not in
late stage disease patients. Being treated in an academic/research program was linked to
improved prognosis when all patients were combined, but not for a particular staging
group. Compared to surgery alone, receiving adjuvant radiotherapy was associated with
greater risk of death in early stage disease patients and when all patients were combined.
The year of diagnosis was associated with improved overall survival (Hazard ratio [HR]
0.76, 95% CI 0.72-0.80) in multivariable models, and those diagnosed 2004-2006 had a
significantly higher three-year overall survival rate as compared to those diagnosed in the
earlier cohort (48.4% versus 29.2%, p<.001) (2).

37
Table 5. Independent risk factors for mortality stratified by disease-stateB Early Stage (I, II) Late Stage (III, IV) All Stages (I-IV)
HR (95% CI) p HR (95% CI) p HR (95% CI) p
Sex
Male (Ref) 1.00 1.00 1.00
Female 1.00 (0.93-1.07) .943 0.92 (0.85-0.99) .020 0.95 (0.91-1.01) .062
Age (years)
18-64 (Ref) 1.00 1.00 1.00
≥65 1.80 (1.62-1.99) <.001 1.41 (1.26-1.58) <.001 1.59 (1.48-1.72) <.001
Race
White (Ref) 1.00 1.00 1.00
Black 1.43 (1.21-1.69) <.001 0.99 (0.87-1.12) .866 1.10 (0.99-1.21) .078
Hispanic 1.00 (0.79-1.69) .998 0.85 (0.66-1.08) .173 0.91 (0.77-1.08) .271
Asian 0.71 (0.57-0.89) .003 0.85 (0.70-1.02) .075 0.78 (0.68-0.90) .001
Other 0.96 (0.59-1.54) .859 0.87 (0.57-1.32) .503 0.88 (0.64-1.21) .444
Insurance
Private (Ref) 1.00 1.00 1.00
Uninsured/Medicaid 1.54 (1.35-1.76) <.001 1.34 (1.32-1.49) <.001 1.52 (1.40-1.64) <.001
Medicare/other
government
1.58 (1.43-1.76) <.001 1.29 (1.15-1.44) <.001 1.45 (1.35-1.57) <.001
Facility Type
ARP (Ref) 1.00 1.00 1.00
Non-ARP 1.05 (0.97-1.15) .121 1.08 (0.98-1.18) .123 1.07 (1.01-1.14) .030
Facility Volume
Low (Ref) 1.00 1.00 1.00
B Reproduced with permission from Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity
squamous cell carcinoma: analysis of the National Cancer Database 1998-2006. Oral Oncol 2016;52:45-51.

38
High 0.84 (0.79-0.90) <.001 0.97 (0.88-1.06) .470 0.91 (0.85-0.97) .002
Year of Diagnosis
1998-2003 (Ref) 1.00 1.00 1.00
2004-2006 0.67 (0.63-0.72) <.001 0.87 (0.81-0.94) <.001 0.76 (0.72-0.80) <.001
Stage
I (Ref) 1.00 -- -- 1.00
II 1.49 (1.39-1.60) <.001 -- -- 1.49 (1.40-1.60) <.001
III (Ref) -- -- 1.00 1.96 (1.80-2.14) <.001
IV -- -- 1.22 (1.13-1.32) <.001 2.44 (2.26-2.64) <.001
Treatment Regimen
Surgery (Ref) 1.00 1.00 1.00
Surgery + RT 1.39 (1.38-1.51) <.001 1.00 (0.92-1.08) .999 1.18 (1.11-1.25) <.001
Surgery + CRT 1.80 (1.48-2.18) <.001 1.13 (1.02-1.26) .021 1.41 (1.29-1.54) <.001
Neck Dissection
No (Ref) 1.00 1.00 1.00
Yes 0.80 (0.75-0.87) <.001 1.00 (0.91-1.11) .952 0.90 (0.84-0.95) <.001
Surgical Margins
Negative (Ref) 1.00 1.00 1.00
Positive 1.39 (1.26-1.53) <.001 1.55 (1.43-1.69) <.001 1.50 (1.41-1.60) <.001
Abbreviations: HR-Hazard Ratio, CI-Confidence interval, Ref-Referent category, ARP-
Academic/Research Program, RT-Radiation Therapy, CRT-Chemoradiation Therapy

39
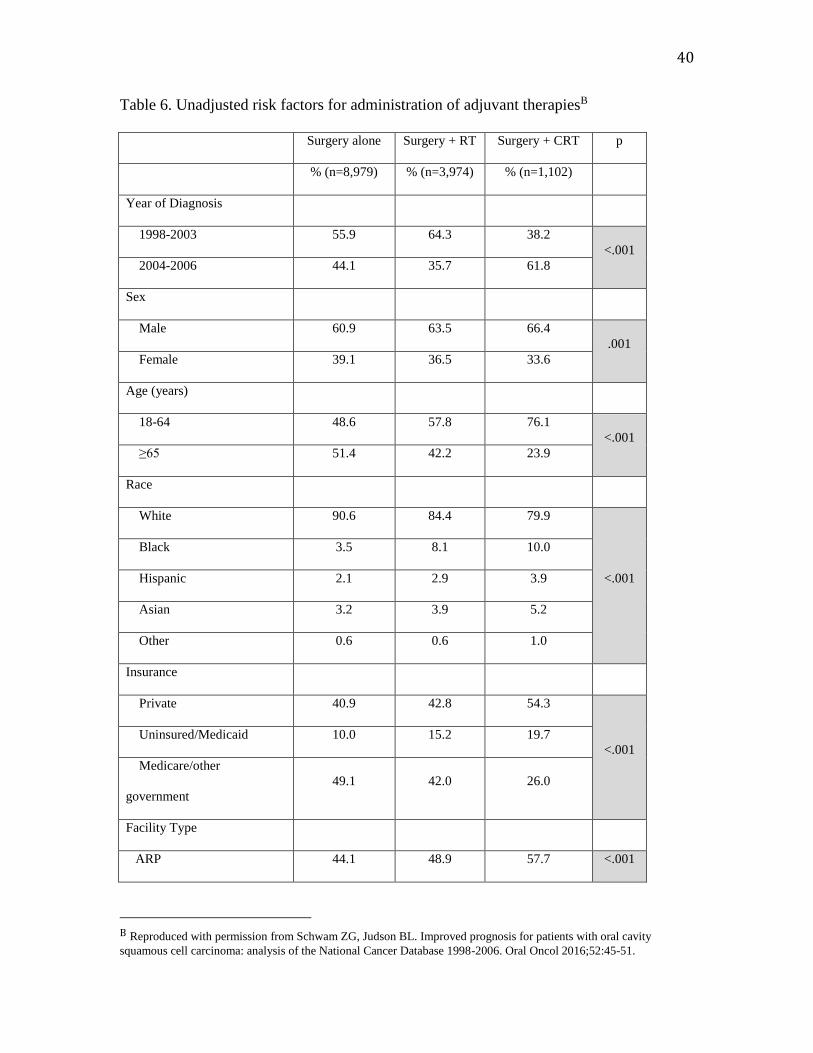
Factors associated with receipt of adjuvant therapies
When all patients were combined, 65.7% received surgery alone, 29.1% received
adjuvant radiotherapy, and 8.1% received adjuvant chemoradiotherapy. In univariate
analysis, later year of diagnosis, younger age, black race, private insurance, getting
treated in an academic program or high volume facility, T4 lesions, higher overall stage,
positive margins, and undergoing neck dissection were all associated with the receipt of
adjuvant chemoradiotherapy (Table 6) (2).
Nearly one in six patients receiving adjuvant chemoradiotherapy did not undergo
neck dissection, and 76.1% had negative surgical margins. Data regarding dose of
radiotherapy were scant, being present for only 21.1% of our cohort. In those patients for
whom data were available, the median dose was 56.0 Gray (Gy), and 18.2% received
doses between 60.0 and 66.0 Gy. The median dose increased over the study period from
52.0 Gy (1998-2003) to 59.4 Gy (2004-2006). No data were available regarding type,
dose, or adequacy of chemotherapeutic agents (2).
40
Table 6. Unadjusted risk factors for administration of adjuvant therapiesB
Surgery alone Surgery + RT Surgery + CRT p
% (n=8,979) % (n=3,974) % (n=1,102)
Year of Diagnosis
1998-2003 55.9 64.3 38.2
<.001
2004-2006 44.1 35.7 61.8
Sex
Male 60.9 63.5 66.4
.001
Female 39.1 36.5 33.6
Age (years)
18-64 48.6 57.8 76.1
<.001
≥65 51.4 42.2 23.9
Race
White 90.6 84.4 79.9
<.001
Black 3.5 8.1 10.0
Hispanic 2.1 2.9 3.9
Asian 3.2 3.9 5.2
Other 0.6 0.6 1.0
Insurance
Private 40.9 42.8 54.3
<.001
Uninsured/Medicaid 10.0 15.2 19.7
Medicare/other
government
49.1 42.0 26.0
Facility Type
ARP 44.1 48.9 57.7 <.001
B Reproduced with permission from Schwam ZG, Judson BL. Improved prognosis for patients with oral cavity
squamous cell carcinoma: analysis of the National Cancer Database 1998-2006. Oral Oncol 2016;52:45-51.

41
Non-ARP 55.9 51.1 42.3
Facility Volume
Low 51.5 51.9 42.6
<.001
High 48.5 48.1 57.4
T-classification
1 56.7 19.7 12.6
<.001
2 29.2 39.3 32.6
3 5.3 14.6 18.7
4 8.8 26.4 35.1
N-classification
0 90.1 62.9 38.5
<.001
1 5.5 17.9 21.2
2 4.1 18.6 37.3
3 0.2 0.7 3.0
M-classification
0 99.7 99.6 99.1
.003
1 0.3 0.4 0.9
Overall Stage
I 55.2 15.2 5.8
<.001
II 25.4 26.5 14.4
III 7.9 20.6 20.9
IV 11.4 37.7 58.9
Surgical Margins
Negative 92.2 76.8 76.1
<.001
Positive 7.8 23.2 23.9
Neck Dissection
No 60.0 30.0 15.9 <.001

42
Yes 40.0 70.0 84.1
Abbreviations: RT-radiation therapy, CRT-chemoradiation therapy, ARP-
Academic/Research Program
Discussion
There is a scarcity of multi-institutional level data characterizing the postoperative
complications following oral cavity cancer surgery, the risk factors for them, and the
time-course over which they occur (1). While changes in prognosis have been reported
in oral cancer in international cohorts (81), there is a similar lack of multi-institutional
data from the United States (2).
In measuring thirty-day morbidity and mortality following primary resection for
oral cavity cancer, the overall complication rate was 20.3% and mortality occurred in
1.0% of patients. In their comparison of clinical registry and administrative data from
355 oral cavity cancer patients treated at Memorial Sloan-Kettering Cancer Center, Awad
et al. found that all major complications, one-third of total complications, and 27% of
patients were found in the NSQIP, in comparison to their own administrative records (90).
They found a significantly higher overall adverse rate of 62.0%, but were also able to
track many procedure-specific complications including orocutaneous fistula, trismus, and
chyle leak that are not found in the NSQIP. Awad et al. tracked only complications
occurring during admission, and stopped tracking them after 45 days (1).

43
Awad’s group found that 34% of patients undergoing neck dissection experienced
a complication (90), while we measured a very similar value of 33%. The rate of
complications after neck dissection ranges in the literature between 7-16% for major
complications and up to 38% in total (110,111,112,113,114), although pre-neck
dissection therapy such as radiation, chemotherapy, or prior surgery must be taken into
consideration in addition to extent of neck dissection. In one prospective trial of elective
modified radical (MRND) versus supraomohyoid (SOH) neck dissection for T2-T4 oral
cavity malignancies, the MRND group had a significantly higher complication rate (41%
versus 25%, p=.043) and a longer median length of stay (9 days versus 7 days) when
compared to the SOH group (115). In our study, we found that undergoing neck
dissection was a risk factor for several postoperative complications, including surgical-
site, infectious, and respiratory complications. While the neck dissection itself may
increase the likelihood of complications by prolonging operative times, extending
incisions, and putting critical neurovascular structures at risk, we believe it to be a proxy
variable for more advanced disease (37) in the NSQIP, which does not track oncologic
variables such as TNM classifications or overall stage of disease (1).
We found that the rate of neck dissections increased significantly between 1998
and 2006, particularly for patients with early stage disease. It was also noted that
undergoing neck dissection was associated with better overall survival in early stage
disease patients and when all patients were combined (2). A recent randomized control
trial from Tata Memorial Centre evaluated the role of elective versus therapeutic neck
dissection in 596 patients with T≤2, clinically N0 lateralized oral cancers (47). The

44
investigators found several benefits to elective node dissection, including significantly
fewer recurrences, a three-year overall survival rate of 80.0% compared to 67.5%, a
hazard ratio for mortality of 0.64 (95% CI 0.45-0.92), and a significantly higher rate of
three-year disease-free survival (69.5% versus 45.9%). Adverse event rates were
relatively low, with 6.6% of the elective group and 3.6% of the therapeutic group having
complications.
In addition to neck dissection as a significant risk factor for multiple
complications, we found that cigarette smoking within the year prior to surgery and
weight loss ≥10% within the six months prior to surgery were associated with surgical-
site complications. Perioperative smoking cessation is frequently recommended due to its
known association with impaired wound healing (116,117,118) and surgical site
infections (1,119,120). Weight loss resulting in physiologic impairments has been
associated with postoperative septic complications (1,121). In our study, we believe that
significant weight loss most likely reflects cancer-induced inflammation as well as
difficulties with eating as a result of the lesion’s location in the oral cavity (1).
Furthermore, it has been shown that systemic inflammation and weight loss affect
albumin concentration (122,123), which was associated with wound complications in a
NSQIP study of over two thousand patients undergoing laryngectomy (1,124).
Minimizing readmission after surgery has become a quality of care initiative
(125), especially in light of its ability to influence Medicare reimbursements (126).
While the NSQIP does not track readmission rates, Luryi et al. found a 3.5% readmission
45
rate following surgery for oral cancers (87) using the National Cancer Database. In the
same study, neck dissection, male gender, and T3 tumor classification were associated
with unplanned readmission. In our cohort, we measured thirty-day reoperation
occurring in 9.6% of patients, with risk factors including cigarette smoking, recent weight
loss, and history of stroke/TIA. As these very same risk factors were also noted to be
associated with surgical-site and respiratory complications, reoperation may have been to
create or revise a tracheostomy stoma. Cigarette smoking in the two weeks prior to
surgery has also been linked to major flap complications requiring return to the operating
room (127), and may explain some of the reoperations in our study (1).
Post-discharge complications are a huge source of hospital readmissions, with
nearly one in seven surgical patients experiencing a preventable adverse event leading to
unintended readmission (105,128). In our study, we found that 4.9% of patients
experienced 17.3% of all complications after leaving the hospital, and that over 90% of
them occurred within 14 days of discharge. Many superficial wound infections and much
of the dehiscence occur within 7 days of discharge, however. This compares favorably to
the NSQIP analysis of 21 groups of general surgery procedures by Kazaure and
colleagues, in which 41.5% of all complications occurred in the post-discharge timeframe
(105). In using the NSQIP to examine over 48,000 patients undergoing a diverse range
of otolaryngologic procedures, Chen et al. had similar findings, showing that about three-
quarters of post-discharge complications occurred by post-discharge day 14, with many
of them concerning the surgical-site or systemic infections (1,88).

46
In order to maximize short-term well-being and to minimize healthcare spending
on unintended readmissions, the literature shows that early clinical follow-up is essential
(1). It has been reported that half of patients readmitted for post-discharge complications
had not seen a physician within the month after discharge (128). Using the Surveillance,
Epidemiology, and End Results (SEER) database, Tuggle et al. showed that seeing a
healthcare provider in the 30 days after surgery could reduce re-hospitalization rates by
55% (absolute decrease of 6.3%) in elderly patients undergoing thyroidectomy (129).
Similarly, Robles was able to show that hiring a nurse practitioner in a surgical practice
not only increased telephone communication and therapy services, but also reduced
unnecessary emergency room visits by 48% (absolute reduction of 12%) (130). As many
of the post-discharge complications occurred within the one to two weeks after leaving
the hospital, early intervention would likely play an important role in minimizing
morbidity and unnecessary healthcare spending (1).
Our data from the National Cancer Database demonstrate a large increase in
three-year overall survival for patients with oral cavity squamous cell carcinomas using
multi-institutional data from hundreds of participating centers throughout the United
States. In a 20-year retrospective study of 2,738 oral cavity cancer patients from seven
leading international cancer centers, Amit et al. found an 11% improvement in five-year
overall survival and a 12% increase in disease-specific survival when all patients were
examined together (81). Surgery alone was performed in 31% of their cohort, adjuvant
radiotherapy was administered in 51%, and adjuvant chemoradiotherapy in 18%.
Additionally, 60% of patients underwent elective neck dissection, and 40% received

47
therapeutic neck dissection. When splitting the study population into two time-of-
diagnosis based cohorts (1990-2000 and 2001-2011), the authors found that the later
cohort presented at an earlier age, with more advanced disease and extracapsular
extension, and more often had negative margins. A limited, selective neck dissection was
also more frequently performed in the later group. The decade of diagnosis was an
important predictor of survival, with patients diagnosed 2001-2011 having better overall,
disease-specific, and disease-free survival in multivariate analyses. In a study by Pulte et
al. using the SEER database to examine trends in prognosis of head and neck cancers, the
investigators similarly found a 14.4% increase in overall survival for patients with lesions
of the oral tongue between 1992-1996 and 2002-2006 (131). We found a much larger
improvement in overall survival than found in the Amit and Pulte studies, which may be
due to either changes in patterns of follow-up by the NCDB or heterogeneity of the
participating sites; the NCDB includes hospital registry data from over 1500 participating
sites (97), while Amit and colleagues tracked patients only from seven leading cancer
hospitals throughout the world. We found period of diagnosis to be associated with
improved overall survival, and found that those presenting later more often were younger
and had early stage disease; this may be explained by greater access to healthcare, more
effective disease screening, or increased awareness (2).
Receiving treatment in a high-volume center took place more often in 2004-2006,
and was associated with improved overall survival in patients with early stage disease
and when all patients were analyzed together. This was closely mirrored by an increase
in patients receiving care in academic/research programs. These changes in treatment

48
setting may be from some degree of regionalization of cancer care, shifts in referral
patterns, or more physicians going to work for larger hospital systems (2). Facility
volume has been shown to be a positive factor in head and neck cancer prognostication
using multiple databases (133,134) and government registries (135,136). Surgical
resection of the primary tumor is often the first therapeutic step in the treatment of oral
cavity malignancies (37), and higher-volume centers may be more facile with larger
ablative procedures requiring free tissue transfer as part of the reconstruction. Higher
volume centers may also have a more formal way of approaching oncologic treatment
decision making in the way of tumor boards, which have been shown to intensify
proposed head and neck cancer treatment and up-stage disease (2,136). We found that
nearly 80% of high volume facilities were academic/research programs, which have been
largely superior to non-academic facilities in terms of process measures and risk-adjusted
mortality for complex patients in the literature (137). We labeled a facility “high volume”
if it was in the ≥90th percentile, and did not determine the minimum percentile for which
there was a survival benefit (2).
In addition to treatment in a high volume facility, this study found positive
surgical margins to be a poor prognostic factor for patients with oral cavity squamous cell
carcinoma. Positive margins are more commonly found in the oral cavity when
compared to other head and neck sub-sites (138), are an important determinant in the
decision to administer adjuvant treatment (37), and put patients at higher risk of disease
recurrence and compromised disease-specific survival (2,139). We found a significant
decrease in the rate of patients with positive margins and a steady increase in patients

49
receiving adjuvant therapy; this is likely due to high-risk pathologic features not
accounted for in the database, such as extracapsular spread and perineural invasion. In
using the NCDB to examine over 20,000 early stage oral cavity cancer patients, Luryi et
al. observed positive margins in 7.5% of the study population, with a range of 0.0-43.8%
(140). The authors found that more advanced disease and receiving treatment in a lower
volume or non-academic facility to be risk factors for positive surgical margins. While
we did not examine risk factors for positive margins, we did see a corresponding decrease
in both presentation with late stage disease and treatment in low volume/non-academic
facilities to accompany the decrease in rate of positive margins (2).
Receipt of adjuvant chemoradiotherapy was associated with worse overall
survival in all patients, regardless of disease stage. This is in contrast to its strong,
positive temporal correlation with three-year overall survival in late stage patients.
Administration of adjuvant chemoradiotherapy became increasingly popular after the
publication of two noteworthy trials, RTOG 9501 (66) and EORTC 22931 (67), which
compared the efficacy of adjuvant chemoradiotherapy to adjuvant radiotherapy in high-
risk and late stage head and neck cancer, respectively. Both studies reported superior
locoregional control and a more serious toxicity profile in the chemoradiotherapy group.
The two trials differed slightly with respect to survival analyses; RTOG 9501 reported
that chemoradiotherapy was associated with improved disease-free survival, but not
overall survival, while EORTC 22931 demonstrated better progression-free and overall
survival in the chemoradiotherapy group. When the authors pooled their data in a follow-
up analysis, they concluded that adjuvant chemoradiotherapy was best suited for those

50
with extracapsular extension or positive margins (2,65). In our cohort, nearly one in six
patients receiving adjuvant chemoradiotherapy did not undergo neck dissection, and over
three-quarters receiving such therapy had negative margins. Additionally, many patients
with positive margins did not receive adjuvant therapy. While we were unable to account
for certain high-risk pathologic features that are currently indications for adjuvant
treatment, the appropriateness of certain treatment regimens must be called into question
(2). Unfortunately, the reason for non-administration of therapy was lacking for the
majority of patients, and could not be analyzed in a meaningful way. It is possible that
patients had significant comorbidities precluding them from receiving treatment, or that
they refused recommended therapy. The majority of patients were also diagnosed and
treated prior to the publication of those two trials. In analyzing the adequacy of
radiotherapy, we found that the median regional dose to be 56.0 Gy, with only 18.2% of
patients for whom there was data receiving doses in line with the trial protocols.
Adequacy of chemotherapy or systemic therapies was not possible to measure in the
database, and toxicity from adjuvant therapy as a cause for mortality cannot be excluded
(2).
Several additional limitations must be taken into account when analyzing the
results of our data concerning both short- and long-term prognosis of oral cavity
malignancies. In terms of thirty-day morbidity and mortality, many complications of
interest may not be tracked in the NSQIP, potentially underestimating the true
complication rate. Patients in our cohort also underwent a variety of concurrent
procedures, from free flaps to parotidectomies, with each procedure having a different
51
adverse event profile. Furthermore, the NSQIP does not keep track of oncologic
variables, hospital or surgeon volume, prior surgery, or rationale/timing of reoperation (1).
Several other variables were not adjusted for, and may impact our results: including
trainee involvement, length of procedure, surgeon skill, postoperative nursing care, and
patient compliance with prescribed regimens. While we were able to give a timecourse
over which complications occurred, there is wide variation in admission and discharge
practices amongst facilities. An important variable not recorded in the NSQIP is time
from hospital discharge to outpatient follow-up, as this may be an important avenue for
intervention. Additionally, some complications in the NSQIP may not be as specific as
desired; for example, return to the operating room is listed, but without cause. Returning
because of postoperative hemorrhage and returning to obtain negative margins are very
different events. Additionally, we selected a cohort in which data for the variables of
interest were present, introducing potential bias, unless one assumes that data is missed at
random. While the NSQIP collects data from its hundreds of participating sites, entry
requirements including a large subscription fee and the cost of employing a SCNR; this
may be prohibitive for smaller facilities or may skew the dataset to representing
institutions with a strong desire to study and improve outcomes.
In analyzing changes in long-term prognosis, we were unable to analyze Charlson
comorbidity scores, relative timing of adjuvant treatment, and a host of high-risk
pathologic features that are associated with worse prognosis in oral cancers. The NCDB
also limits analysis to overall survival, as cause of death is not available. Individual
patient income and level of education are not available, which may impact treatment

52
decisions. Undergoing neck dissection was not one of our inclusion criteria, which may
have led to under-staging for certain patients. We limited our analysis to patients
diagnosed between 1998 and 2006 due to data availability; if extended in either direction,
a more pronounced change in prognosis may have been observed (2). Additionally, the
NCDB has additional limitations that should further inform the results of our study. As it
currently stands, only CoC-approved cancer centers are allowed to report their results to
the NCDB (141,142); criteria for CoC-approval include having a wide range of oncologic
services and specialists, and must participate in several quality-improvement activities
(141). CoC-approved hospitals have been found to be more likely associated with
residency programs and medical schools, more frequently accredited by the Joint
Commission, less frequently in rural areas, and tend to have higher volume surgical
facilities and more comprehensive oncologic services (141). As the vast majority of
facilities are not CoC-accredited (142), the NCDB may represent an unrepresentative
cross-section of oral cancer care nationwide.
Conclusions
In examining a multicenter cohort of patients with oral cavity cancer, we
determined that a significant number of patients undergoing primary resection experience
a postoperative adverse event, and determined that a small yet significant minority
experience complications after admission. We identified risk factors that may serve as
potential red flags in the patient history for postoperative complications. Furthermore, we
identified the two weeks after discharge as a high-risk time for vulnerable patients, and
believe that early clinical follow-up may mitigate the morbidity associated with post-

53
discharge complications and prevent costly readmission in high-risk patients (1).
Monitoring our advancements in treatment of oncologic disease is an important task to
undertake, and can be done through examining changes in prognosis for a given disease.
This was the first study showing that the long-term prognosis for patients with oral cavity
squamous cell carcinoma has improved significantly for both early and late stage disease
patients using a nationwide cohort. Similar changes in prognosis have only been
demonstrated in patients with human papillomavirus-positive oropharyngeal squamous
cell carcinoma. This study was the first to show that receipt of adjuvant
chemoradiotherapy has increased substantially in the treatment of oral cavity squamous
cell carcinoma, yet we also found it to be associated with compromised overall survival.
We think this represents a selection bias where patients with high-risk pathologic features
not accounted for in the NCDB were more likely to receive such therapy. We believe
that further work is needed in the way of clinical trials to determine the efficacy of
adjuvant therapies specifically in patients with oral cavity squamous cell carcinoma (2).

54
References
1. Schwam, Z.G., Sosa, J.A., Roman, S.A., Judson, B.L. 2015. Complications and
mortality following surgery for oral cavity cancer. Laryngoscope. 125:1869-73.
2. Schwam, Z.G., Judson, B.L. 2016. Improved prognosis for patients with oral cavity
squamous cell carcinoma: Analysis of the National Cancer Database 1998-2006. Oral
Oncol. 52:45-51.
3. Wein, R.O., Weber, R.S. 2014. Malignant neoplasms of the oral cavity. In Cummings
Otolaryngology: P.W. Flint, B.H. Haughey, V. Lund, J.K. Niparko, T. Robbins, J.R.
Thomas, M.M. Lesperance, editors. Philadelphia: Saunders. 1359-1387.
4. Shah, J.P. 1990. Patterns of cervical lymph node metastases from squamous cell
carcinomas of the upper aerodigestive tract. Am. J. Surg. 160:405-409.
5. Siegel, R.L., Miller, K.D., Jemal, A. 2015. Cancer statistics, 2015. CA: A cancer
journal for clinicians. 65:5-29.
6. World Health Organization Global Agency for Research on Cancer. 2012. World
estimated cancer incidence, all ages: both sexes. Available from URL:
http://globocan.iarc.fr/old/summary_table_pop-
html.asp?selection=224900&title=World&sex=0&type=0&window=1&sort=0&submit=
%C2%A0Execute%C2%A0 [accessed July 4, 2015].
55
7. Warnakulsariya, S. 2009. Global epidemiology of oral and oropharyngeal cancer. Oral
Oncol. 45:309-16.
8. Llewellyn, C.D., Johnson, N.W., Warnakulasuriya, S. 2001. Risk factors for squamous
cell carcinoma of the oral cavity in young people – a comprehensive literature review.
Oral Oncol. 37:401–418.
9. Surveillance epidemiology and end results (SEER). SEER Cancer statistics review
1975–2004. National Cancer Institute. Available from URL:
http://seer.cancer.gov/statfacts/html/oralcav [accessed November 1, 2015].
10. Shiboski, C.H., Schmidt, B.L., Jordan, R.C. 2005. Tongue and tonsillar carcinoma:
increasing trends in the US population ages 20–44 years. Cancer. 103:1843–1849.
11. Chaturvedi, A.K., Engels, E.A., Anderson, W.F., Gillison, M.L. 2008. Incidence
trends for human papillomavirus–related and –unrelated oral squamous cell carcinomas
in the United States. J. Clin. Oncol. 26:612-619.
12. Winn, D.M., Blot, W.J., Shy, C.M., Pickle, L.W., Toledo, A., et al. 1981. Snuff
dipping and oral cancer among women in the southern United States. N. Engl. J. Med.
304:745–9.

56
13. Decker, J., Goldstein, J.C. 1982. Risk factors in head and neck cancer. N. Engl. J.
Med. 306:1151-1155.
14. Reddy, C.R. 1974. Carcinoma of hard palate in India in relation to reverse smoking of
chuttas. J. Natl. Cancer Inst. 53:615-9.
15. Franceschi, S., Talamini, R., Barra, S., Baron A.E., Negri, E. 1990. Smoking and
drinking in relation to cancers of the oral cavity, pharynx, larynx, and esophagus in
northern Italy. Cancer. Res. 15:6502-7.
16. Wynder, E.L., Hoffmann, D. 1976. Tobacco and tobacco smoke. Semin. Oncol. 3:5–
15.
17. Hecht, S.S. 2003. Tobacco carcinogens, their biomarkers and tobacco-induced cancer.
Nat. Rev. Cancer. 3:733-44.
18. Mansour, O.I., Snyderman, C.H., D’Amico, F. 2003. Association between tobacco
use and metastatic neck disease. Laryngoscope. 113:161-166.
19. Seitz, H.K., Stickel, F. 2007. Molecular mechanisms of alcohol-mediated
carcinogenesis. Nat. Rev. Cancer. 7:599-612.

57
20. Mashberg, A., Garfinkel, L., Harris, S. 1981. Alcohol as a primary risk factor in oral
squamous cell carcinoma. CA Cancer J. Clin. 31:146-55.
21. Rothman, K., Keller, A. 1972. The effect of joint exposure to alcohol and tobacco on
risk of cancer of the mouth and pharynx. J. Chronic Dis. 25:711–6.
22. Homann, N., Jousimies-Somer, H., Jokelainen, K., Heine, R., Salaspuro, M. 1997.
High acetaldehyde levels in saliva after ethanol consumption: methodological aspects and
pathogenetic implications. Carcinogenesis. 18:1739–1743.
23. Seitz, H.K., Stickel, F. 2006. Risk factors and mechanisms of hepatocarcinogenesis
with special emphasis on alcohol and oxidative stress. Biol. Chem. 387:349–360.
24. Garro, A.J., Espina, N., Farinati, F., Lieber, C.S. 1986. The effect of chronic ethanol
consumption on carcinogen metabolism and on O6-methylguanine transferase-mediated
repair of alkylated DNA. Alcohol Clin. Exp. 10:73–77.
25. Wang, M., McIntee, E.J., Cheng, G., Shi, Y., Villalta, P.W., et al. 2000. Identification
of DNA adducts of acetaldehyde. Chem Res Toxicol. 13:1149–1157.
26. Bailey, S.M., Cunningham, C.C. 2002. Contribution of mitochondria to oxidative
stress associated with alcohol liver disease. Free. Radic. Biol. Med. 32, 11–16.

58
27. De Visscher, J.G., Van der Waal, I. 1998. Etiology of cancer of the lip: A review. Int.
J. Oral Maxillofac. Surg. 27:199-203.
28. Van Leeuwen, M.T., Grulich, A.E., McDonald, S.P., McCredie, M.R., Amin, J, et al.
2009. Immunosuppression and other risk factors for lip cancer after kidney
transplantation. Cancer Epidemiol. Biomarkers Prev. 18:561-9.
29. Wurman, L.H., Adams, G.L., Meyerhoff, W.L. 1975. Carcinoma of the lip. Am. J.
Surg. 130:470-474.
30. Czerninski, R., Zini, A., Sgan-Cohen, H.D. 2010. Lip cancer: incidence, trends,
histology and survival: 1970-2006. Br. J. Dematol. 162:1103-9.
31. Velly, A.M., Franco, E.L., Schlecht, N., Pintos, J., Kowalski, L.P., et al. 1998.
Relationship between dental factors and risk of upper aerodigestive tract cancer. Oral
Oncol. 34:284-291.
32. Marshall, J.R., Graham, S., Haughey, B.P., Shedd, D., O’Shea, R., et al. 1992.
Smoking, alcohol, dentition and diet in the epidemiology of oral cancer. Oral Oncol.
Euro. J. Cancer. 28B:9-15.

59
33. Funk, G.F., Karnell, L.H., Robinson, R.A., Zhen, W.K., Trask, D.K., et al. 2002.
Presentation, treatment, and outcome of oral cavity cancer: a National Cancer Data Base
report. Head Neck. 24:165-180.
34. Spector, M.E., Wilson, K.F., Light, E.L., McHugh, J.B., Bradford, C.R. 2011.
Clinical and pathologic predictors of recurrence and survival in spindle cell carcinoma.
Otolaryngol. Head Neck Surg. 145:242-247.
35. Raslan, W.F., Barnes, L., Krause, J.R. 1994. Basaloid squamous cell carcinoma of the
head and neck: a clinicopathologic and flow cytometric study of 10 new cases with
review of the English literature. Am. J. Otolaryngol. 15:204-211.
36. de Sampaio Goes, F.C., Oliviera, D.T., Dorta, R.G., Nishimoto, I.N., Landman, G., et
al. 2004. Prognoses of oral basaloid squamous cell carcinoma and squamous cell
carcinoma: a comparison. Arch. Otolaryngol. Head Neck Surg. 130:83-86.
37. Pfister, D.G., Spencer, S., Brizel, D.M., Burtness, B., Busse, P.M., et al. NCCN
Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Head and Neck Cancers
Version 1.2015. ©2015 National Comprehensive Cancer Network, Inc. Available from
URL: www.NCCN.org [accessed February 3, 2015].
38. Fakih, A.R., Rao, R.S., Borges, A.M., Patel, A.R. 1989. Elective versus therapeutic
neck dissection in early carcinoma of the oral tongue. Am. J. Surg. 158:309-313.

60
39. Ferlito, A., Rinaldo, A., Robbins, K.T., Leemans, C.R., Shah, J.P., et al. 2003.
Changing concepts in the surgical management of the cervical node metastasis. Oral
Oncol. 39:429-435.
40. Teichgraeber, J.F., Clairmont. A.A. 1984. The incidence of occult metastases for
cancer of the oral tongue and floor of the mouth: treatment rationale. Head Neck Surg.
7:15-21.
41. Ross, G.L., Soutar, D.S., MacDonald, D.G., Shoaib, T., Camilleri, I.G., et al. 2004.
Improved staging of cervical metastases in clinically node-negative patients with head
and neck squamous cell carcinoma. Ann. Surg. Oncol. 11:213-218.
42. Keski-Santti, H., Atula, T., Tornwall, J., Koivunen, P., Makitie, A. 2006. Elective
neck treatment versus observation in patients with T1/T2 N0 squamous cell carcinoma of
oral tongue. Oral Oncol. 42:96-101.
43. Pentenero, M., Gandolfo, S., Carrozzo, M. 2005. Importance of tumor thickness and
depth of invasion in nodal involvement and prognosis of oral squamous cell carcinoma: a
review of the literature. Head Neck. 27:1080-1091.
44. Moore, C., Kuhns, J.G., Greenberg, R.A. 1986. Thickness as prognostic aid in upper
aerodigestive tract cancer. Arch. Surg. 121:1410-1414.
61
45. DiTroia, J.F. Nodal metastases and prognosis in carcinoma of the oral cavity. 1972.
Otolaryngol. Clin. North Am. 5:333-342.
46. Huang, S.H., Hwang, D., Lockwood, G., Goldstein, D.P., O'Sullivan, B. 2009.
Predictive value of tumor thickness for cervical lymph‐node involvement in squamous
cell carcinoma of the oral cavity. Cancer. 11:1489-1497.
47. D’Cruz, A.K., Vaish, R., Kapre, N., Dandekar, M., Gupta, S., et al. 2015. Elective
versus therapeutic neck dissection in node-negative oral cancer. N. Engl. J. Med.
373:521-529.
48. Chandu, A., Smith, A.C., Rogers, S.N. 2006. Health-related quality of life in oral
cancer: a review. J. Oral. Maxillofac. Surg. 64:495-502.
49. Rogers, S.N., Lowe, D., Brown, J.S., Vaughan, E.D. 1999. The University of
Washington head and neck cancer measure as a predictor of outcome following primary
surgery for oral cancer. Head Neck. 21:394-401.
50. De Graeff, A., de Leeuw, J.R., Ros, W.J., Hordijk, G.J., Blijham, G.H., et al. 1999. A
prospective study on quality of life of patients with cancer of the oral cavity or
oropharynx treated with surgery with or without radiotherapy. Oral Oncol. 35:27-32.

62
51. Hammerlid, E., Silander, R., Hornestam, L., Sullivan, M. 2001. Health-related quality
of life three years after diagnosis of head and neck cancer, a longitudinal study. Head
Neck. 23:113-125.
52. Gamba, A., Romano, M., Grosso, I.M., Tamburini, M., Cantu, G., et al. 1992.
Psychosocial adjustment of patients surgically treated for head and neck cancer. Head
Neck.14:218-223.
53. Netscher, D.T., Meade, R.A., Goodman, C.M., Alford, E.L., Stewart, M.G. 2000.
Quality of life and disease-specific functional status following microvascular
reconstruction for advanced (T3 and T4) oropharyngeal cancers. Plast. Reconstr. Surg.
105,1628-1634.
54. Rogers, S.N., Devine, J., Lowe, D., Shokar, P., Brown, J.S., et al. 2004. Longitudinal
health related quality of life after mandibular resection for oral cancer: A comparison
between rim and segment. Head Neck. 26:54-62.
55. Rogers, S.N., Lowe, D., McNally, D., Brown, J.S., Vaughan, E.D., 2003. Health
related quality of life after maxillectomy: A comparison between prosthetic obturation
and free flap. J. Oral. Maxillofac. Surg. 61:174-181.

63
56. Laverick, S., Lowe, D., Brown, J.S., Vaughan, E.D., Rogers, S.N. 2004. The impact
of neck dissection on health-related quality of life. Arch. Otolaryngol. Head Neck Surg.
130:149-154.
57. Licciardello, J.T., Spitz, M.R., Hong, W.K. 1989. Multiple primary cancer in patients
with cancer of the head and neck: Second cancer of the head and neck, esophagus, and
lung. Internat. J. Radiat. Oncol. Biol. Phys. 17:467-476.
58. Cohn, A.M., Peppard, S.B. 1980. Multiple primary malignant tumors of the head and
neck. Am. J. Otolaryngol. 1:411-417.
59. Shapshay, S.M., Wong, W.K., Fried, M.P., Sismanis, A., Vaughn, C.W., Strong, M.S.
1980. Simultaneous carcinomas of the esophagus and upper aerodigestive tract.
Otolaryngol. Head Neck Surg. 8:373-377.
60. Berg, J.W., Schottenfeld, D., Ritter, F. 1970. Incidence of multiple primary cancers.
Ill. Cancers of the respiratory and upper digestive system as multiple primary cancers. J.
Natl. Cancer Inst. 44:263-270.
61. Tepperman, B.S., Fitzpatrick, P.J. 1981. Second respiratory and upper digestive tract
cancers after oral cancer. Lancet. 2:547-549.

64
62. Winn, D.M., Blot, W.J. 1985. Second cancer following cancers of the buccal cavity
and pharynx in Connecticut, 1935-1982. In Multiple primary cancers in Connecticut and
Denmark. J.D. Boice, Jr., editor. Bethesda: Department of Health and Human Services.
25-46.
63. Gluckman, J.L., Crissman, J.D. 1983. Survival rates in 548 patients with multiple
neoplasms of the upper aerodigestive tract. Laryngoscope. 93:71-74.
64. Laramore, G.E., Scott, C.B., Al-Sarraf, M., Haselow, R.E., Ervin, T.J., et al. 1992.
Adjuvant chemotherapy for resectable squamous cell carcinomas of the head and neck:
report on Intergroup Study 0034. Int. J. Radiat. Oncol. Biol. Phys. 23: 706–713.
65. Bernier, J., Cooper, J.S., Pajak, T.F., van Glabbeke, M., Bourhis, J., et al. 2005.
Defining risk levels in locally advanced head and neck cancers: A comparative analysis
of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931)
and RTOG (# 9501). Head Neck. 27:843-850.
66. Cooper, J.S., Pajak, T.F., Forastiere, A.A., Jacobs, J., Campbell, B.H., et al. 2004.
Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell
carcinoma of the head and neck. N. Engl. J. Med. 350:1937-1944.

65
67. Bernier, J., Domenge, C., Ozsahin, M., Matuszewska, K., Lefebvre, J.L., et al. 2004.
Postoperative irradiation with or without concomitant chemotherapy for locally advanced
head and neck cancer. N. Engl. J. Med. 350:1945-1952.
68. U.S. Preventive Services Task Force. Oral Cancer: Screening. Available from URL:
http://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/oral
-cancer-screening1 [accessed December 20, 2015].
69. Sakararanarayana, R., Ramadas, K., Thara, S., Muwonge, R., Thomas, G., et al. 2012.
Long term effect of visual screening on oral cancer incidence and mortality in a
randomized trial in Kerala, India. Oral Oncol. 49:314-321.
70. Elashoff, D., Zhou, H., Reiss, J., Wang, J., Xiao, H., et al. 2012. Prevalidation of
salivary biomarkers for oral cancer detection. Cancer Epidemiol. Biomarkers Prev.
21:664-72.
71. Rethman, M.P., Carpenter, W., Cohen, E.E., Epstein, J., Evans, C.A., et al. 2010.
Evidence-based clinical recommendations regarding screening for oral squamous cell
carcinomas. J. Am. Dent. Assoc. 141:509-520.
72. Ziober, A.F., Patel, K.R., Alawi, F., Gimotty, P., Weber, R.S., et al. 2006.
Identification of a gene signature for rapid screening or oral squamous cell carcinoma.
Clin. Cancer Res. 12:5960-71.

66
73. de Bree, R., Deurloo, E.E., Snow, G.B., Leemans, C.R. 2000. Screening for distant
metastases in patients with head and neck cancer. Laryngoscope. 110:397-401.
74. Dennington, M.L., Carter, D.R., Meyers, A.D. 1980. Distant metastases in head and
neck epidermoid carcinoma. Laryngoscope. 90:196-201.
75. Black, R.J., Gluckman, J.L., Shumrick, D.A. 1984. Screening for distant metastases
in head and neck cancer patients. Aust. N. Z. J. Surg. 54:527-530.
76. Cooper, J.S., Porter, K., Mallin, K., Hoffman, H.T., Weber, R.S., et al. 2009. National
Cancer Database report on cancer of the head and neck: 10‐year update. Head Neck.
31:748-758.
77. Silverman, S. Jr. 2001. Demographics and occurrence of oral and pharyngeal cancers.
The outcomes, the trends, the challenge. J. Am. Dent. Assoc. 132:7S–11S.
78. Ries, L.A.G., Hankey, B.F., Miller, B.A., Hartman, A.M., 1991. Edwards, B.K.
Cancer Statistics Review 1973–1988. Bethesda: National Cancer Institute. 91-2789.
79. Neville, B.W., Day, T.A. 2002. Oral Cancer and precancerous lesions. CA: A cancer
journal for clinicians. 52:195-215.

67
80. Rusthoven, K., Ballonoff, A., Raben, D., Chen, C. 2007. Poor prognosis in patients
with stage I and II oral tongue squamous cell carcinoma. Cancer. 112:345-51.
81. Amit, M., Yen, T.C., Liao, C.T., Chaturvedi, P., et al. 2013. Improvement in survival
of patients with oral cavity squamous cell carcinoma: An international collaborative
study. Cancer. 119:4242-4248.
82. Franceschi, D., Gupta, R., Spiro, R.H., Shah, J.P. 1993. Improved survival in the
treatment of squamous cell carcinoma of the oral tongue. Am. J. Surg. 166:360-65.
83. Liu, S.A., Wong, Y.K., Poon, C.K., Wang, C.C., Wang, C.P., et al. 2007. Risk factors
for wound infection after surgery in primary oral cavity cancer patients. Laryngoscope.
117:166-171.
84. Agra, I.M., Carvalho, A.L., Pontes, E., Campos, O.D., Ulbrich, F.S., et al. 2003.
Postoperative complications after en bloc salvage surgery for head and neck cancer. Arch.
Otolaryngol. Head Neck Surg. 2003;129:1317–1321.
85. de-Melo, G.M., Ribeiro, K.C., Kowalski, L.P., Deheinzelin, D. 2001. Risk factors for
postoperative complications in oral cancer and their prognostic implications. Arch.
Otolaryngol. Head Neck Surg. 127:828–833.

68
86. Penel, N., Fournier, C., Lefebvre, D., Lefebvre, J.L. 2005. Multivariate analysis of
risk factors for wound infection in head and neck squamous cell carcinoma surgery with
opening of mucosa. Study of 260 surgical procedures. Oral Oncol. 41:294–303.
87. Luryi, A.L., Chen, M.M., Mehra, S., Roman, S.A., Sosa, J.A., et al. 2014. Hospital re-
admission and 30-day mortality following surgery for oral cavity cancer: Analysis of
21,681 cases. Head Neck. In press.
88. Chen, M.M., Roman, S.A., Sosa, J.A., Judson, B.L. 2013. Postdischarge
Complications Predict Reoperation and Mortality after Otolaryngologic Surgery.
Otolaryngol. Head Neck Surg. 149:865-872.
89. Morris, M.S., Deierhoi, R.J., Richman, J.S., Altom, L.K., Hawn, M.T. 2014. The
Relationship Between Timing of Surgical Complications and Hospital Readmission.
JAMA Surg. 149:348-354.
90. Awad, M.I., Shuman, A.G., Montero, P.H., Palmer, F.L., Shah, J.P., et al. 2015.
Accuracy of administrative and clinical registry data in reporting postoperative
complications following surgery for oral cavity squamous cell carcinoma. Head Neck.
37:851-861.
91. Sullivan, M.C., Roman, S.A., Sosa, J.A. 2012. Does chemotherapy prior to
emergency surgery affect patient outcomes? Examination of 1912 Patients. Ann. Surg.

69
Oncol. 19:11-18.
92. Gupta, P.K., Smith, R.B., Gupta, H., Forse, R.A., Fang, X., et al. 2012. Outcomes
after thyroidectomy and parathyroidectomy. Head Neck. 34:477-484.
93. Khuri, S.F., Daley, J., Henderson, W., Hur, K., Demakis, J., et al. 1998. The
Department of Veterans Affairs' NSQIP: the first national, validated, outcome-based,
risk-adjusted, and peer-controlled program for the measurement and enhancement of the
quality of surgical care. National VA Surgical Quality Improvement Program. Ann. Surg.
228:491-504.
94. American College of Surgeons National Surgical Quality Improvement Program.
User Guide for the 2010 Participant Use Data File. June 24, 2010. Available at:
http://site.acsnsqip.org/wp-content/uploads/2012/03/2010-User-Guide_FINAL.pdf.
[Accessed June 1, 2012].
95. Shiloach, M., Frencher, S.K. Jr, Steeger, J.E., Rowell, K.S., Bartzokis, K., et
al. 2010. Toward robust information: data quality and inter-rater reliability in the
American College of Surgeons National Surgical Quality Improvement Program. J. Am.
Coll. Surg. 210:6-16.
96. American College of Surgeons. User guide for the 2013 ACS NSQIP Paticipant Use
Data File (PUF). 2014. Available from URL:

70
https://www.facs.org/~/media/files/quality%20programs/nsqip/acs_nsqip_puf_user_guide
_2013.ashx [accessed November 29, 2015].
97. American College of Surgeons. National Cancer Data Base. Available from URL:
https://www.facs.org/quality%20programs/cancer/ncdb [accessed January 4, 2014].
98. Jesup, J.M., Menck, H.R., Winchester, D.P., Hundhal, S.A., Murphy, J.P. 1996. The
National Cancer Data Base report on hospital reporting. Cancer. 78:1829-1837.
99. Raval, M.V., Bilmoria, K.Y., Stewart, A.K., Bentrem, D.J., Ko, C.Y. 2009. Using the
NCDB for cancer care improvement: an introduction to available quality assessment
tools. J. Surg. Oncol. 99:488-490.
100. Commission on Cancer. Registry Operations and Data Standards (ROADS). 1996.
Available from URL:
https://www.facs.org/~/media/files/quality%20programs/cancer/coc/roads/roads1996.ash
x [accessed June 20, 2014].
101. Commission on Cancer. Facility Oncology Registry Data Standards (FORDS). 2003.
Available from URL: http://www.facs.org/cancer/coc/fords/fordsoriginal2003.pdf
[accessed June 20, 2014].

71
102. World Health Organization. 2015. International Classification of Diseases (ICD).
Available from URL: http://www.who.int/classifications/icd/en/ (Accessed December 1,
2015).
103. American Medical Association. 2015. cpt® Code/Relative Value Search. Available
from URL: https://ocm.ama-
assn.org/OCM/CPTRelativeValueSearch.do?submitbutton=accept. [Accessed June 14,
2014].
104. American College of Surgeons National Surgical Quality Improvement Program.
User Guide for the 2010 Participant Use Data File. 2010. Available from URL:
http://site.acsnsqip.org/wp-content/uploads/2012/03/2010-User-Guide_FINAL.pdf.
[Accessed June 1, 2012].
105. Kazaure, H.S., Roman, S.A., Sosa, J.A. 2012. Association of postdischarge
complications with reoperation and mortality in general surgery. Arch. Surg. 147:1000-
1007.
106. Fritz, A., Percy, C., Jack, A., Shanmugaratnam, K., Sobin, L., et al. 2000.
International Classification of Diseases for Oncology, ICD-O. 3rd ed. Geneva: World
Health Organization, 242 pp.

72
107. Fleming, I.D., Cooper, J.S., Henson, D.E., Hutter, R.V., Kennedy, B.J., et al., editors.
1997. American Joint Committee on Cancer (AJCC) cancer staging manual. 5th edition.
Philadelphia: J. B. Lippincott. 294pp.
108. Greene FL, Page DL, Fleming ID, et al., eds. 2002. AJCC Cancer Staging
Handbook. 6th ed. New York: Springer-Verlag. 199pp.
109. American College of Surgeons. National Cancer Data Base data dictionary.
Available from URL: http://ncdbpuf.facs.org/?q=print-pdf-all [accessed June 13, 2014].
110. Stenson, K.M., Haraf, D.J., Pelzer, H., Recant, W., Kies, M.S., et al. 2000. The role
of cervical lymphadenectomy adter aggressive concomitant chemoradiotherapy: The
feasibility of selective neck dissection. Arch. Otolaryngol. Head Neck Surg. 126:950-956.
111. Mendenhall, W.M., Villaret, D.B., Amdur, R.J., Hinerman, R.W., Mancuso, A.A.
2002. Planned neck dissection after definitive radiotherapy for squamous cell carcinoma
of the head and neck. Head Neck. 24:1012-1018.
112. Mendenhall, W.M., Million, R.R., Cassisi, N.J. 1986. Squamous cell carcinoma of
the head and neck treated with radiation therapy: the role of neck dissection for clinically
positive neck nodes. Int. J. Radiat. Oncol. Biol. Phys. 12:733-740.

73
113. McGuirt, W.F., McCabe, B.F. 1980. Bilateral neck dissections. Arch. Otolaryngol.
106:427-429.
114. Brizel, D.M., Prosnitz, R.G., Hunter, S. 2004. Necessity for adjuvant neck dissection
in setting of concurrent chemoradiation for advanced head and neck cancer. Int. J. Radiat.
Oncol. Biol. Phys. 58:1418-1423.
115. Brazilian Head and Neck Cancer Study Group. 1998. Results of a prospective trial
on elective modified radical classical versus supromohyoid neck dissection in the
management of oral squamous carcinoma. Am. J. Surg.176:422-427.
116. Mosely, L.H., Finseth, F., Goody, M. 1978. Nicotine and its effect on wound
healing. Plast. Reconstr. Surg. 61:570-575.
117. Silverstein, P. 1992. Smoking and wound healing. Am. J. Med. 93:22S-24S.
118. Møller, A.M., Villebro, N., Pederson, T., Tønneson, H. 2002. Effect of preoperative
smoking intervention on postoperative complications: a randomised clinical trial. Lancet.
359:114-117.
119. Lotfi, C.J., Cavalcanti Rde, C., Costa e Silva, A.M, Latorre Mdo, R., Ribeiro Kde,
C., et al. 2008. Risk factors for surgical-site infections in head and neck cancer surgery.
Otolaryngol. Head Neck Surg. 138:74-80.

74
120. Sørensen, L.T., Hørby, J., Friis, E., Pilsgard, B., Jørgensen, T. 2002. Smoking as a
risk factor for wound healing and infection in breast cancer surgery. Euro. J. Surg. Oncol.
28:815-820.
121. Windsor, J.A., Hill, G.L. 1988. Weight loss with physiologic impairment. A basic
indicator of surgical risk. Ann. Surg. 207: 290-296.
122. Scott, H.R., McMillan, D.C., Forrest, L.M., Brown, D.J.F., McArdle, C.S., et al.
2002. The systemic inflammatory response, weight loss, performance status and survival
in patients with inoperable non-small cell lung cancer. Br. J. Cancer. 87:264-267.
123. McMillan, D.C., Watson, W.S., O'Gorman, P., Preston, T., Scott, H.R., et al. 2001.
Albumin concentrations are primarily determined by the body cell mass and the systemic
inflammatory response in cancer patients with weight loss. Nutr. Cancer. 39:210-213.
124. Schwartz, S.R., Yueh, B., Maynard, C., Daley, J., Henderson, W., et al. 2004.
Predictors of wound complications after laryngectomy: a study of over 2000 patients.
Otolaryngol. Head Neck Surg. 131: 61-68.
125. Benbassat, J., Taragin, M. 2000. Hospital readmissions as a measure of quality of
health care: advantages and limitations. Arch. Intern. Med. 160:1074-1081.

75
126. Centers for Medicare & Medicaid Services. Readmissions Reduction Program.
2014. Available from URL: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-
Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. [Accessed February
20, 2015].
127. Haughey, B.H., Wilson, E., Kluwe, L., Piccirillo, J., Frederickson, J., et al. 2001.
Free flap reconstruction of the head and neck: analysis of 241 cases. Otolaryngol. Head
Neck Surg.125:10-17.
128. Jencks, S.F., Williams, M.V., Coleman, E.A. 2009. Rehospitalizations among
patients in the Medicare fee-for-service program. N. Engl. J. Med. 360:1418-1428.
129. Tuggle, C.T., Park, L.S., Roman, S., Udelsman, R., Sosa, J.A. 2010.
Rehospitalization among elderly patients with thyroid cancer after thyroidectomy are
prevalent and costly. Ann. Surg. Oncol. 17:2816-2823.
130. Robles, L., Slogoff, M., Ladwig-Scott, E., Zank, D. 2011. The addition of a nurse
practitioner to an inpatient surgical team results in improved use of resources. Surgery.
150:711-717.
131. Pulte, D., Brenner, H. 2010. Changes in survival in head and neck cancers in the late
20th and 21st century: a period analysis. Oncologist. 15:994-1001.
76
132. Chen, M.M., Roman, S.A., Yarbrough, W.G., Burtness, B.A., Sosa, J.A., et al. 2014.
Trends and variations in the use of adjuvant therapy for patients with head and neck
cancer. Cancer. 120:3353-3360.
133. Sharma, A., Schwartz, S.M., Mendez, E. 2013. Hospital volume is associated with
survival but not multimodality therapy in Medicare patients with advanced head and neck
cancer. Cancer. 119:1845-1852.
134. Cheung, M.C., Koniaris, L.G., Perez, E.A., Molina, M.A., Goodwin, W.J., et al.
2009. Impact of hospital volume on surgical outcome for head and neck cancer. Ann.
Surg. Oncol. 16:1001-1009.
135. Eskander, A., Irish, J., Groome, P.A., Freeman, J., Gullane, P., et al. 2014. Volume-
outcome relationships for head and neck cancer surgery in a universal health care system.
Laryngoscope. 124:2081-8.
136. Wheless, S.A., McKinney, K.A., Zanation, A.M. 2010. A prospective study of the
clinical impact of a multidisciplinary head and neck tumor board. Otolaryngol. Head
Neck Surg. 143:650-654.
137. Kupersmith, J. 2005. Quality of care in teaching hospital: a literature review. Acad.
Med. 80:458-66.
77
138. Jones, A.S., Bin Hanafi, Z., Nadapalan, V., Poland, N.J., Kinsella, A., et al. 1996.
Do positive resection margins after ablative surgery for head and neck cancer adversely
affect prognosis? A study of 352 patients with recurrent carcinoma following
radiotherapy treated by salvage surgery. Br. J. Cancer. 74:128-132.
139. Joo, Y.H., Yoo, I.R., Cho, K.J., Park, J.O., Nam, I.C., et al. 2013. Standardized
uptake value and resection margin involvement predict outcomes in pN0 head and neck
cancer. Otolaryngol. Head Neck Surg. 149:721-726.
140. Luryi, A.L., Chen, M.M., Mehra, S., Roman, S.A., Sosa, J.A. 2014. Positive
Surgical Margins in Early Stage Oral Cavity Cancer An Analysis of 20,602 Cases.
Otolaryngol. Head Neck Surg. 151:984-990.
141. Bilimoria, K.Y., Stewart, A.K., Winchester, D.P., Ko, C.Y. 2008. The National
Cancer Data Base: A powerful initiative to improve cancer care in the United States. Ann.
Surg. Oncol. 15:683–690.
142. Bilimoria, K.Y., Bentrem, D.J., Stewart, A.K., Winchester, D.P., Ko, C.Y. 2009.
Comparison of Commission on Cancer–Approved and –Nonapproved Hospitals in the
United States: Implications for Studies That Use the National Cancer Data Base. J. Clin.
Oncol. 27:4177-4181.