serial assessment of peak expiratory flows jean-luc malo md chest physician université de montréal...
TRANSCRIPT
Serial assessment of peak expiratory flows
Jean-Luc Malo MD
Chest Physician
Université de Montréal and Hôpital du Sacré-Coeur
and Center for Asthma in the Workplace
Hôpital du Sacré-Cœurde Montréal
Université de Montréal
Axe de rechercheen santé respiratoire
Centre asthme et travailCenter for Asthma in the Workplace

Chronic Obstructive Pulmonary Diseases
Definition (functional)
Diseases characterized by a reduction in
expiratory flow rates caused by either
bronchial obstruction (bronchial involvement per se)
or a loss in the elastic support of the bronchi
by emphysema (destruction of the lung parenchyma)
(peribronchial involvement).
Manifestations: reduction of expiratory flow rates
Functional indices:
1. Forced expiratory volume-one second (FEV1)
2. FEV1/forced vital capacity (“Tiffeneau Index”, 1947)
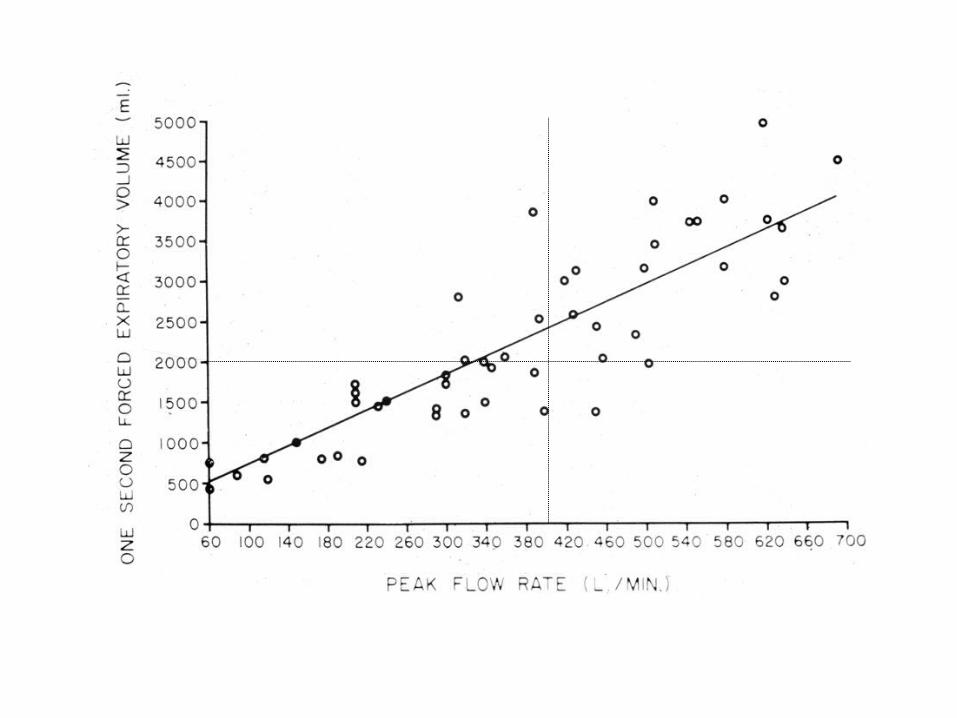
3. Peak Expiratory Flows (Rates):
Wright and McKerrow 1959
Chronic Obstructive Pulmonary Diseases

flow (volume / time)
peak expiratory flow
one second time
ma
xim
um
insp
ira
tory
ca
pac
ity(v
ital c
apa
city
)FEV1 forced vital
capacity

Origin of the assessment of peak expiratory flows (PEF)in Asthma and Occupational Asthma
In asthma Daily peak flow measurements in the assessment of
steroid therapy for airway obstruction.Epstein SW, Fletcher CM, Oppenheimer EA.
BMJ 1969 On observing patterns of airflow obstruction in chronic asthma.Turner-Warwick M.
Br J Dis Chest 1977
Identification of three patterns: 1. Brittle asthmatic;
2. Morning dipper; 3. Pseudo irreversible asthmatic. Comparison of normal and asthmatic circadian rhythms in peak expiratory flow rate.
Hetzel MR, Clark TJH. Thorax 1980. Action plans based on PEF.
In occupational asthma Burge PS et al. 1979 onwards

Interest, advantages
assessment with portable, cheap instruments
provides serial assessment of airway caliber
(relevant for asthma diagnosis and management)
Disadvantages
effort-dependent manoeuver
reflects large airway caliber
(discredit from lung physiologists who focused
on «small airways»)


To assess peak expiratory flows :
Portable peak flow meters : standard (cheap) andelectronic (storage of data)
Predicted values(as a function of age, sex, heightand racial origin)
Normal valuesIn men: 500 to 700 L/minIn women: 350-500 L/min


Number of recordings/day:In asthma: morning value (before medication)In occupational asthma: at least four times a day
How many values at each time ?3 times, 2 best values within 20 L/min
Significant changes ?50 L/min
In occupational asthma, for how long ?Two weeks at work, two weeks off-work
Indications
In asthmaAcute: essential in ER (FEV1 or PEF) and in
GP officeChronic: Poor perception of airflow limitation
Brittle asthma Discrepancy between symptoms and
need for medication: excludehyperventilation
To identify flare-upsIn occupational asthma
As a screening test : negative tracingand absence of airway hyper-responsiveness at work
Diagnostic ?In rhinitis
Nasal peak flows can be assessed.

Examples of tracings



Development of an expert system for interpretation of PEFby Burge PS and coworkers *
Two methods for assessing PEF:
1. Visual examination by experts:
satisfactory within- and between-
observers’ reproducibility
2. Interpretation by discriminant analysis (OASYS)
* Burge PS et al. Occup Environ Med 1999; 56:758-764
Pitfalls
Compliance: poor (50%) in asthma and in occupational asthma (Quirce & Chan-Yeung 1995)
Falsification of data : 20% of values are invented
Interpretation of data: visual vs computed- assisted method (OASYS) ?
contamination of results in field studies
variable figures for sensitivity and specificity by comparison
with specific inhalation challenges (gold standard)

Girard D et al. Am J Respir Crit Care Med 2004; 170: 845-850Girard F et al. Am J Respir Crit Care Med 2004
Conclusion
Advantages assess subjects in a natural setting simplicity: inexpensive and handy devices readily available as a screening test, more to exclude than to confirm the diagnosis
Limitations subject’s motivation and honesty long monitoring may be necessary return to work without supervision interpretation of results

Compatible clinical historyand exposure to possible causal agents
Skin testing and/orspecific IgE assessment
(if possible)
Assessment of bronchial responsivenessto pharmacologic agents
Normal Increased
Subject stillat work
Subject no longerat work
Subject stillat work
Laboratory challengeswith the suspectedoccupational agent
Positive Negative
Consider return to work
Workplace or laboratory challengeswith the suspected occupational
agent, peak expiratory flowmonitoring, or both
Positive Negative
No asthma Occupational asthma
Nonocccupational asthma
Chan Yeung M, Malo JL. NEJM 1995; 333:107