sepsis case study 2017 denise hinge & jo kelly · overview of case study •time line •issues...
TRANSCRIPT

Sepsis Case Study 2017 Denise Hinge & Jo Kelly

Overview of case study
• Time line
• Issues identified
• Multiple handovers
– Pre hospital
– 2 hospital sites
– ED to ward
– Ward to ICU

Day 0 Pre hospital 39 year old patient NHS 111 call
Called ambulance 12:49 Paramedic response at scene 12:58
• No past medical history
• c/o generally feeling unwell, hiccups, loose stools, bloated, jaundice.
• 6 days ago started to feel unwell
• 4 days ago went to OOH-stated a virus 24-48 hours
• 2 days ago went to GP-stated a virus 48-72 hours
• Initial assessment: – Airway-patent/talking in sentences
– Respirations- 20 resp per min
– Saturations- 98% on air
– Heart rate 104 bpm
– BP 122/84
– Temperature 38.8○C
• Blood glucose 10.8 mmol / Paramedic administered 1g Paracetamol
• Temperature reduced to 37.7 ○C . All other observations remained the same.

Day 0 Emergency department
• 15:47 patient self presented in private transport accompanied by his partner to PRH – Partner noticed patient to be slightly jaundiced
• 15:58 RR 36 on air, temp 36.6, SpO2 97%, BP 134/69, Pulse 109
• Seen by Dr (no time noted) – o/e Jaundice ?biliary ?hepatitis – VBG- lactate 2.2 – USS completed
• 16:59 Antibiotics given • 17:00 Fluids commenced

Day 0 Emergency department
• 17:30 review by on call medical SHO – Clerked – AKI noted (Creatinine 376, Urea 16.3, Na 126, K 3.5, CRP 424.9, WCC 15.9, Bilirubin
163) – Catheter requested – d/c with ITU SHO advised to rpt U&E, VBG in night and contact if deteriorates (not
for filtration at present) – CT requested, further bloods, viral swabs, ECG, CXR – DW on call medical consultant – Renal SPR r/v requested
• 19: 33 Decision to admit • 21:00 S/B reg
– Impression intra-abdominal sepsis/biliary sepsis – Possible transfer to RSCH – For ITU r/v

Continued
• 2200 Seen by SPR medical on call
– Contacted ITU SPR
– Should be under the medics
– Advised repeat ABG at 01:00 & monitor UO
– If patient becomes more unwell contact ITU again
• 2300
– Transferred to medical ward

Day 0

Day 1
• 02:30 review ITU registrar – ABG pH 7.49 lactate 1.7 base excess -5 – Plan-fluid replacement, monitor UO, rpt bloods/ABG review in
morning
• 08:45 post take ward round – Imp biliary sepsis & AKI 2’ sepsis – 7 litres of fluid since admission noted – Plan: monitor/continue, d/w renal, gastro r/v
• 09:20 CT1 – D/w renal unlikely primary renal problem – Plan-d/c gastro & surgeons, RSCH, no beds on renal but liaise. – Continue IV fluids , monitor renal function

Day 1
• 09:20 CT1 medical team D/w Gastro SPR – Plan NBM, NGT, liver screen, accepted under
gastro.
• 11:10 CT1 discussed with Surgical SPR – CT scan reviewed
– They will see on arrival to RSCH
– NGT ASAP
– CT to have GI radiologist – CT1 asked hot reporting to action this.

• 11:35 Frontline transport booked (within 2 hours) • 11:45 CCOT r/v
– NGT inserted (700ml bile) – Deteriorating AKI
• 12:30 CT1 r/v – VBG pH 7.46, Lactate 1.9, Base excess 5.3 – CT review ?mechanical small bowel obstruction – D/w surgeon will see patient on arrival-bleep when at RSCH. – D/w results with Gastro -still transfer under them if no surgical
input required they will see.
• 12:40 Transport changed to blue light transfer (within 30 minutes)

Day 1
• Arrived at RSCH at 15:20 • Single clerking:
– Transfer from PRH ?SBO, comfortable currently. Plan: surgical review
– RR16, SpO2 95%, Pulse 111, BP 131/65, Temp 131/65 alert / orientated NEWS 3
– Fluid balance • Input 5350 mls since MN • Output 1005 (including NG aspirate)
• No name of Dr. No further clerking completed.

2000 Transferred to Ward
– RR28, SpO2 96% on 28% oxygen, temp 37.5, BP 125/60, Pulse 105 Alert , NEWS 5
– ABG 0137 & 0414
– Bloods Creatinine 545 despite aggressive fluid management
No medical documentation until 00:30

Day 2
0030 Medical SPR review DW surgical SPR 0510 Lab phone results – creatinine 545 Medical team informed 0930 Gastro ward round AKI – Infectious disease and renal advice Surgical review ? Time Renal ? Time creat 545 despite 14 litres fluid in 48 hours Suggests may need ICU setting Stops IV fluids – repeat bloods

Day 2
15:30 Phone from microbiology
Blood cultures grown strep pyogenes; group strep A unknown source
Full examination (skin etc nil found)
1620 Infectious diseases review – antibiotics changes
16:24 Further surgical review
17:40 Seen by CCOT – referred by ward staff
SOBOE RR 22 SpO2 96% on 28% oxygen, BP 11/60, Pulse 85, Temp 37.2
Repeat ABG: pH 7.46, PO2 9.6, PCO24.3, lactate 0.8, BE -1
Input 4255, Output 1630
DW ICU consultant
18:30 Seen by ICU accepted for admission
2200 Transferred to ICU for ongoing monitoring / potential haemofiltration

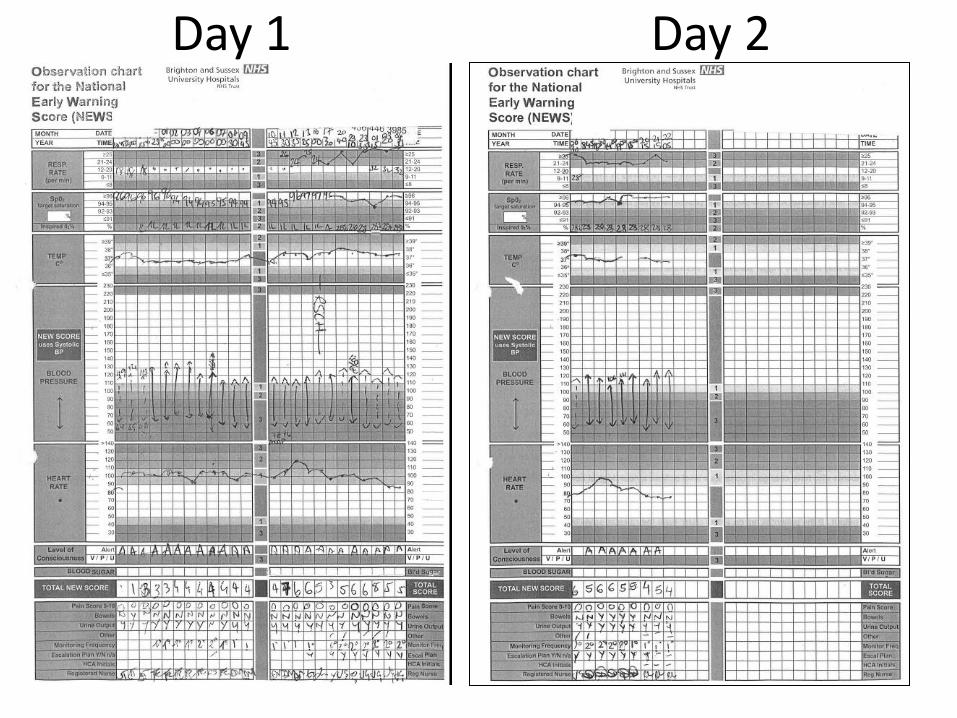
Day 1 Day 2
ICU 12 days
• CVVH (citrate ) • CT AP & contrast – dilated & thickened small
bowel- unlikely ischaemia • Conservative management • IVIg • OGD – distal ½ severely inflamed • PICC line for TPN • Laproscopy – free fluid , adhesions, no obvious
cause infection / blockage • ICU delirium –unpleasant hallucinations


Red flags/ increased risk • Fluid balance (NG loss / Urine output )
• Breathless on exertion
• Increased oxygen requirements
• Renal function not improving
• Multiple teams involved – Who has ownership
– Transfer between hospital sites
– Escalation plan
• Multiple handovers

• Severe Group Strep A streptococcal infection
• Patient experience – Sepsis
– Feeling unwell – multiple staff involved
• Technology : – Limitations of paper based escalation NEWS / fluid
charts
