section 12 claims - gateway insurance
TRANSCRIPT

Section 12
Claims

To ensure prompt and efficient service, please list all policy numbers when filing a claim.
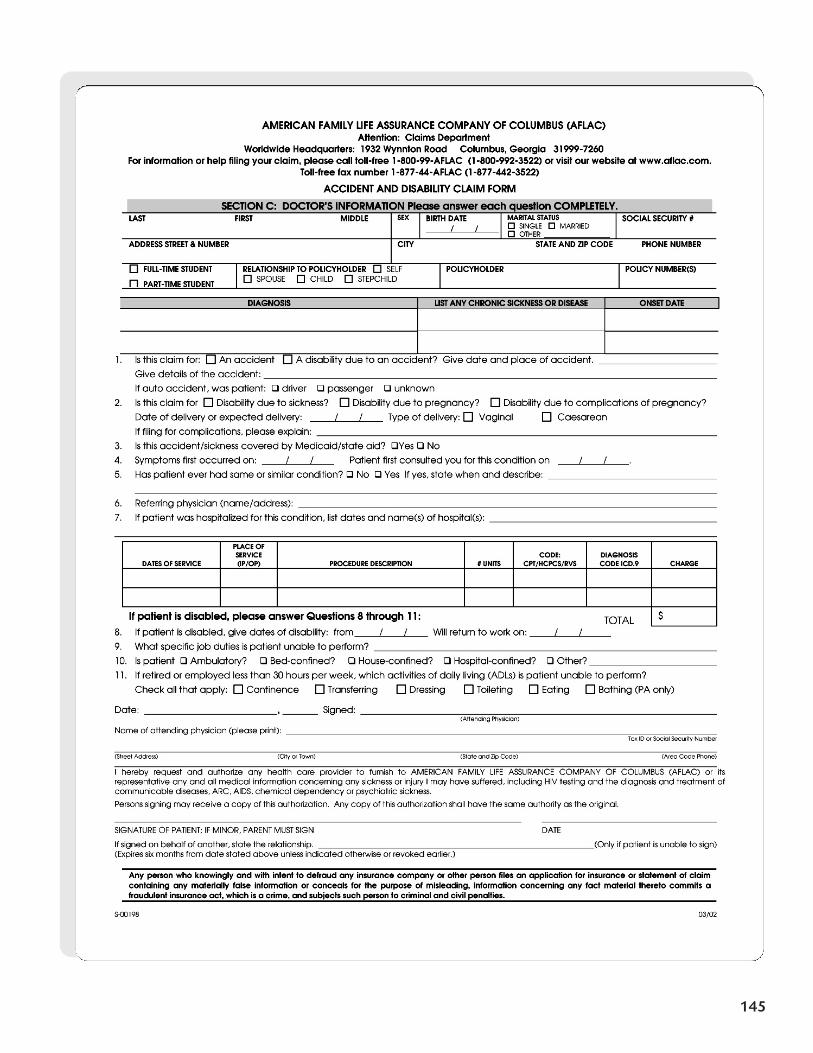
• Claims for accident, sickness, or initial disability will require Form S-00198.
• Claims for continuing disability, whether due to accident or sickness, will require Form S-13270.1.
• Continuing disability claims should be submitted every 30 days.
143
Claims

144
145

146
AMERICAN FAMILY LIFE ASSURANCE COMPANY OF COLUMBUS (AFLAC) Attention: Claims Department
Worldwide Headquarters: 1932 Wynnton Road Columbus, GA 31999-7260 For information or help filing your claim, please call toll-free 1-800-99-AFLAC (1-800-992-3522) or visit our Web site at www.aflac.com
Toll-free fax number 1-877-44AFLAC (1-877-442-3522)
CLAIM FORM FOR CONTINUING DISABILITY ONLY
(If filing first claim for disability, use Form S-00198)
PART A: PATIENT’S INFORMATION LAST FIRST MIDDLE ADDRESS - STREET & NUMBER
CITY STATE/ZIP CODE BIRTH DATE AREA CODE & PHONE NO.
POLICY NO. SOCIAL SECURITY NO.
Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime, and subjects such person to criminal and civil penalties.
PART B: DOCTOR’S INFORMATION FOR CONTINUING DISABILITY ONLY Please answer each question as completely as possible.
Is this claim for continuation of a previous disability? Yes No What is the diagnosis?
Is disability due to: An accident? A sickness? Pregnancy? Complications of pregnancy?
If due to an accident, when did the accident occur? / / If due to a sickness, symptoms first occurred on: / /
Patient first consulted you for this condition on / / Date of initial disability due to this diagnosis: / /
Date of last treatment: / / Type and frequency of treatment:
If pregnant, expected date of delivery: / /
If filing for pregnancy post-partum, what was delivery date? / / Was delivery Vaginal Caesarean
Is patient released to return to work?
Yes – May return to work on: / / List any work restrictions:
No – Date expected to return to work: / /
DATE SIGNATURE (attending physician) TAX ID or SOCIAL SECURITY NUMBER
PRINT NAME OF ATTENDING PHYSICIAN TELEPHONE
STREET ADDRESS CITY OR TOWN STATE ZIP CODE
PART C: EMPLOYER’S INFORMATION FOR CONTINUING DISABILITY ONLY To be completed by Human Resources/Payroll Department
Please answer each question as completely as possible.
Is this claim for continuation of a previous disability? Yes No If yes, date employee was first out for this disability: / /
Is disability due to an accident that occurred on the job? Yes No
Is claimant still employed? Yes No If no, date of termination: / /
Has employee returned to work?
No Date expected to return to work: / /
Yes Date returned to work: / / Full-time Part-time Light duty
If yes, is the employee’s current salary at least 80% of his or her previous salary? Yes No Number of hours worked per week:
Is employee performing all job duties? Yes No If no, what job duties is insured unable to perform, and what percentage of the day
do these duties require? %
%
Will you continue to remit the employee’s premiums during this disability? Yes No
Are disability insurance premiums paid with pre-tax dollars? Yes No
If yes, indicate if employee is exempt from the following deductions: Social Security Medicare
Does employer pay a portion of the disability premiums? Yes No If yes, what percent? %
SIGNATURE of EMPLOYER TITLE DATE
PLEASE PRINT FULL NAME TELEPHONE
STREET ADDRESS CITY or TOWN STATE ZIP CODE
S-13270.1 03/02