screening: antenatal screening for heamoglobinopathies ... · screening: antenatal screening for...
TRANSCRIPT

Screening: Antenatal screening for Heamoglobinopathies Clinical Guideline
V1.0
October 2018
Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 2 of 21
Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 3 of 21
1. Aim/Purpose of this Guideline
This document provides guidance for midwives to enable them to offer informed choices to
all pregnant women regarding participation in the linked sickle cell and thalassaemia
screening programme and to provide guidance in the event of a couple being identified as
higher risk by screening.
2. The Guidance
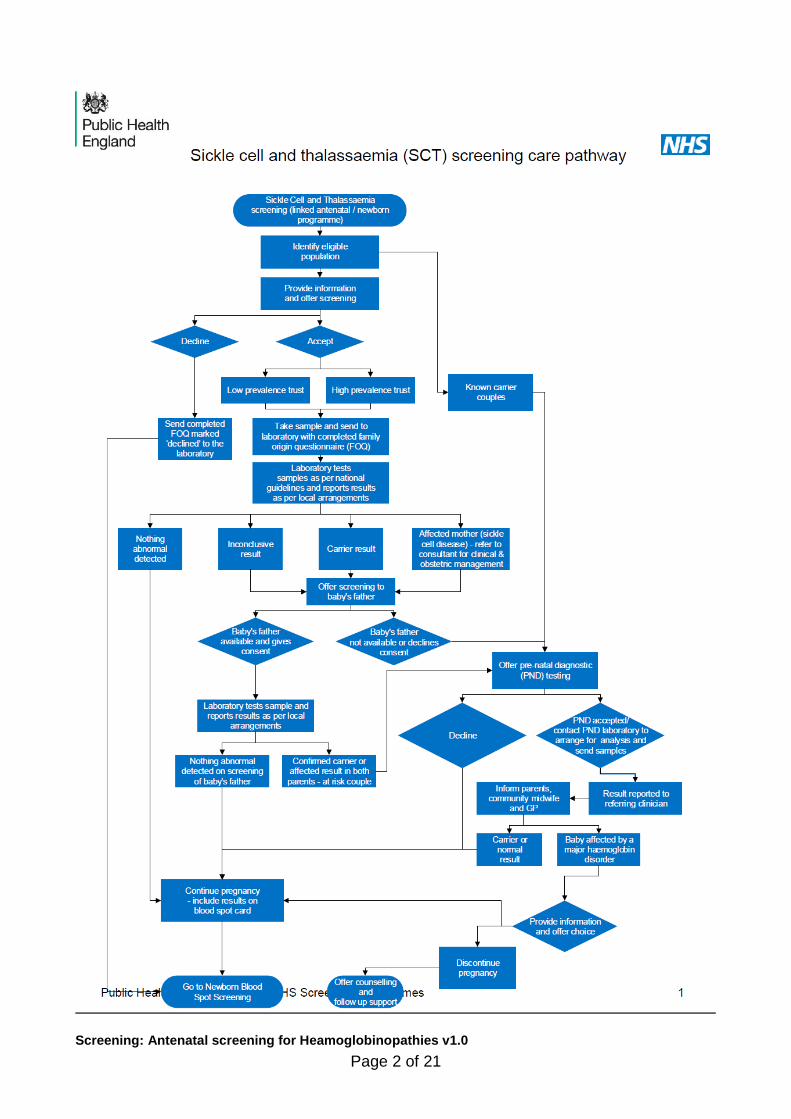
2.1 About the NHS sickle cell and thalassaemia screening programme
This programme is a linked antenatal and newborn programme - neither component should be viewed in isolation. Women and their partners [the baby’s’ biological father] are offered screening for sickle cell and thalassaemia antenatally. All new-borns are offered screening for sickle cell as part of the newborn bloodspot programme
2.2 Aims of the Guideline and Screening Programme
To offer all pregnant women screening for sickle cell and thalassaemia by 10+0 weeks of pregnancy
If the pregnant woman is identified as, or known to be a carrier - offer screening to the baby’s father as soon as possible so that the identification of those couples at risk of having a baby with a major haemoglobinopathy can be offered early prenatal diagnosis [PND] by 12+0 weeks
To perform PND by 12+6 days
To ensure all babies are offered screening for sickle cell disease as part of the newborn bloodspot screening programme in order to allow early diagnosis and to improve outcomes through early treatment and care
2.3 Background
Haemoglobinopathies are a group of disorders in which there is an abnormal haemoglobin molecule. Sickle cell and thalassaemia are autosomal recessive conditions of the blood. Inheritance of an altered gene variant from both parents results in a seriously affected baby, and inheritance of only one altered gene variant results in a minimally affected carrier. Sickle originated in West Africa and the thalassaemia’s [alpha and beta] extend from the Mediterranean to the Far East. They are most commonly found in people whose ethnicity is derived from these areas but migration over many centuries has resulted in dispersion of these genes throughout the world.

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 4 of 21
2.4 Screening Approach The Family Origin Questionnaire [FOQ], together with the initial screening Full Blood Count [FBC] is used to assess risk and determine further testing. Accurate and complete information in the FOQ is essential. There are two approaches to the offer of screening depending on whether a Trust is defined as either high prevalence (HP) or low prevalence (LP) High prevalence trusts are those where sickle cell diseases are estimated to affect over 1.5 pregnancies per 10,000 births. Information from the FOQ is used to interpret the blood results Low prevalence trusts are those where sickle cell diseases are estimated to affect less than 1.5 pregnancies per 10,000 births. The FOQ is used to screen women and the baby’s father and assess the risk of haemoglobin variants and sickle cell disease
RCHT is defined as a low prevalence Trust
2.5 Key Messages for screening in low prevalence areas:
Screening involves the combined use of the Full Blood Count sample and the Family Origin Questionnaire
Thalassaemia screening takes place in the haematology lab using the FBC sample to check certain red blood cell indices
Sickle Cell screening is initiated by the haematology lab according to the FOQ. If the woman or the father of the baby is from a high risk group, screening is performed on the FBC sample using the electrophoresis.
Low risk women will not be automatically tested for Sickle Cell but the red cell indices may identify a Thalassaemia trait
The FOQ (Appendix 3) is used in the lab as the basis of determining which women to test for the haemoglobin variants and helps in the interpretation of laboratory results. Therefore careful attention to the complete provision of accurate information of the FOQ is important
2.6 Antenatal screening processes for sickle cell and thalassaemia at RCHT
2.6.1 Pre-booking
Prior to booking the woman will be given the booklet: ‘Screening tests
for you and your Baby’ Translations are available in 11 languages
and can be accessed from:
https://www.gov.uk/government/publications/screening-tests-for-you-
Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 5 of 21
and-your-baby-description-in-brief
2.6.2 Booking timings
Women should be offered the screening test by 10+0 weeks of
pregnancy; however, women who present later in pregnancy should
still be offered screening
This early booking appointment allows the opportunity for the father
of the baby to be tested, allowing prenatal diagnosis [PND] to be
offered by 12+0 weeks and completed by 12+6 weeks.
If prenatal diagnosis is required, couples should be given results
within 5 working days of the result being available
2.6.3 Information giving
In order for the woman to make an informed choice, the midwife should
discuss the following points:
The benefits of screening for herself and her baby and the management of a
screen positive result including referral to a haemoglobinopathy specialist and
obstetrician.
That low risk women will not automatically be tested for sickle cell but the
routine analysis of the full blood count sample [FBC] may identify them as a
possible thalassaemia carrier [see FOQ].
The results procedure, including the feedback of the results and the possibility
of a false negative or false positive result.
The role of the Family Origin Questionnaire, which should be completed by
the midwife with the woman, ticking the relevant boxes should ensure that at
least three generations are considered
The basic principles of recessive inheritance of sickle cell and thalassaemia.
More information can be found at sct.screening.nhs.uk
2.6.4 Testing women in subsequent pregnancies
The most recent recommendations issued in the National SCT Screening
Laboratory Handbook 2017
[https://www.gov.uk/government/publications/sickle-cell-and-thalassaemia-
screening-handbook-for-laboratories] is to offer testing in every pregnancy,
even if women have been found to have a variant or thalassaemia previously.
We follow this policy at RCHT.
2.6.5 Testing the baby’s father if he has been tested previously
If the baby’s father has been tested for sickle cell and thalassaemia
previously, the same protocol should be used as for a previously tested
mother. We follow the ‘Test every time’ policy at RCHT.
2.6.6 Situations requiring particular care: Fertility Treatment

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 6 of 21
If the pregnancy has been achieved by the use of a donor egg then the screening results on the woman will not be informative so the baby’s father should always be tested to ensure that this is not a high risk pregnancy.
Careful completion of the FOQ section H will initiate father of the baby testing by the laboratory in liaison with the screening coordinators.
If donor sperm has been used then it may be appropriate to refer back to the fertility clinic if the screening results on the woman show that she is a carrier for a haemoglobinopathy.
The haematology laboratory will advise in these circumstances.
If a pregnancy has been achieved by donor egg and donor sperm then the fertility clinic should be contacted to ascertain whether the donors were screened before donation. It is useful for the lab to have this information although it is understood if this is not always possible.
The haematology laboratory will advise in these circumstances.
2.6.7 Taking the blood
If the offer of screening for haemoglobinopathy is accepted, the laboratory
should be sent a single lavender tube [FBC] specimen to arrive to the lab within
one working day.
In order to identify the specimen as an antenatal screening sample, the blood
bottle should be labeled as per Trust standards and put into a clear specimen
bag with the white copy of a fully completed FOQ.
The requestor’s signature should be clear and legible.
The gestation at the time of the blood MUST be documented on the FOQ
The middle [pink] copy of the FOQ should go in the maternal hand held notes
The bottom [yellow] copy of the FOQ should go in the hospital case notes
2.6.8 If the laboratory receives incomplete information on FOQ or FBC:
The lab will contact the Screening Coordinators by email requesting that the
named midwife with responsibility for the woman [or a midwife with
responsibility for the woman if the named midwife is absent] is contacted to
request a new FOQ to be sent or that the midwife contacts the haematology
lab on ex 2502 with the information they require.
The screening coordinators will continue to check their failsafe system weekly
to ensure a result is available.
Similarly, if the lab receives a FOQ without an adequate FBC sample, they
will contact the screening coordinators to request a new sample is drawn. The
Screening Coordinators will then contact the appropriate midwife by email
initially and then by phone to ensure samples are sent in a timely manner.

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 7 of 21
2.6.9 Documentation
The midwife should document the following in the in the woman’ hand held
notes:
The date the screening was offered
Whether haemoglobinopathy screening was accepted or declined
The date the sample was taken
The result and date it was given
2.6.10 If Screening is Declined:
The top copy of the FOQ should be sent to the laboratory with the declined
box ticked and the reason for the decline given if possible. The middle copy of
the FOQ should be placed in the maternal hand held notes and the bottom
copy added to the case notes.
Explain that the blood sample taken for FBC antenatal assessment may
reveal abnormalities on the red cell indices which may lead to a request for
further testing for SCT.
If the woman declines further testing despite an identified abnormality in the
red cell indices, write ‘HPLC declined’ on FBC form, send to lab and
document in hand held notes and hospital records.
If screening is declined it should be noted in the hand-held notes and
recorded on the maternity IT/E3 system.
2.6.11 Results
The laboratory will report the results of the specimen in accordance with
national guidance and enter them onto the Pathology system.
The responsible midwife will review the results within the pathology system
within 10 days of the bloods being taken.
The results should be entered onto the maternity E3 system
If the result shows no evidence of thalassaemia or abnormal haemoglobin, the
result should be reported to the woman at her next antenatal visit (usually 16
weeks) by the community midwife and documented in the hand held notes.
In the event of a positive result, two scenarios are possible;
1. The woman is a carrier of a haemoglobinopathy
2. The woman has a haemoglobinopathy
Father of the baby testing will be initiated in both cases
2.6.12 If maternal results show a carrier status:

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 8 of 21
The laboratory will provide interpretation of the results and the requirement for
any onward testing. The laboratory will contact the screening coordinators and
the following pathway will be initiated:
The screening coordinator will contact the woman and inform her of her
healthy carrier status
If father of the baby testing is required, the screening coordinator will contact
the woman to offer counselling and testing within 3 days of the available
maternal result
The screening coordinator will document the discussion and outcomes on the
maternity E3 system and in the woman’s handheld notes.
When the blood sample is obtained the coordinators must ensure that the father of the baby test specimen can be linked with the maternal sample. This is done by ensuring both parents details are on the form (Maternal CR number and maternal name) and informing the laboratory when the sample is taken so that they can expect it. A yellow alert sticker should be applied to the blood form and the lab phoned to inform them that the sample is on its way.
Ideally, this should be completed by 12+0 weeks of pregnancy.
The screening coordinators will check for the result daily.
2.6.13 If the father of the baby test result is negative:
The screening coordinator will inform him of his result initially by phone and then in writing within 2 weeks of the result. The results will then be recorded in the hospital case notes, on the maternity E3 system and relayed in writing to the community midwife and GP, for documenting in the maternal hand-held notes with partner consent.
The screening coordinators will send an Alert Form to Bristol Newborn Blood Spot lab to inform them of the results and provide the linkage into the postnatal Newborn Blood Spot screening programme.
2.6.14 If the father of the baby is a carrier of a haemoglobinopathy or
is affected with a haemoglobinopathy:
The Screening Coordinators will inform the father of the baby of his
status by telephone. Urgent appointments will be arranged by the screening
coordinators for specialist counselling for the woman and her partner.
At this appointment the offer of prenatal diagnosis will be made depending on
the ancestral origins from the FOQ. The offer of prenatal diagnosis, whether
accepted or declined, should be recorded in the handheld and hospital
records.
Ideally this should be completed by 12+6 weeks of pregnancy.
Additionally, father of the baby status is documented in the handheld and
hospital records, Maternity E3 system with partner consent. Also, it should be

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 9 of 21
noted under ‘Special considerations’ of the postnatal page so that it can be
recorded on the new-born bloodspot card for the baby by community midwife.
2.6.15 If the father of the baby is unavailable for testing (and mother is a
carrier or affected by haemoglobinopathy):
An urgent appointment should be arranged for the woman with the Screening
Coordinators/Fetal Medicine Consultant to determine whether prenatal
diagnosis should be offered in view of ancestral origins of the father of the baby
and information provided on the FOQ.
The offer of prenatal diagnosis, whether accepted or declined, should be
recorded in the handheld and hospital records. Additionally, the father of the
baby status should be documented in the handheld and hospital records.
Additionally, it should be noted under ‘Special considerations of the postnatal
page so that it can be recorded on new-born bloodspot card for the baby.
The Screening Coordinators will send an Alert Form to Bristol New-born Blood
Spot lab to inform them of the results and provide the linkage into the New-
born Blood Spot screening programme
2.6.16 If a woman has full haemoglobinopathy:
The Screening Coordinators will inform the woman of her status and arrange
urgent joint maternal medicine/haematology appointment.
A plan of care must be documented in the maternal handheld and hospital
records. Additionally, the mother’s status will be documented in the hospital
records and on the maternity IT system by the Screening Coordinators. The
result should also be noted under ‘Special considerations’ of the postnatal
page so that it can be recorded on new-born bloodspot card for the baby by
community midwife.
Where a woman fails to attend an appointment for a high risk result, the
Screening Coordinator will contact the woman and ensure that she has all the
information required to make a fully informed decision about her on-going care.
This will be documented on E3 and in the woman’s hand held notes and
hospital notes.
Father of the baby testing will be initiated and results and procedures followed
according to the circumstances as outlined above.
2.7 Alpha Thalassaemia
Alpha thalassaemia varies in severity.
People with Alpha Thalassaemia + do not usually have any problems, though may be slightly anaemic. The children of women who have Alpha Thalassemia + are

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 10 of 21
not usually at risk of a severe disorder.
People with Alpha Thalassaemia 0 [most often of Far Eastern ethnicity] are more affected [with anaemia] and children of those with Alpha Thalassaemia 0 are at risk of a severe disorder [death in utero or Hydrops Foetalis is possible].
Alpha thalassemia [unlike Beta] cannot be diagnosed on haemoglobin
electrophoresis [the test which is used after a FBC to confirm both sickle cell and
beta thalassemia]. The screening FBC result in people with Alpha thalassaemia trait
looks very similar to that in people with iron deficiency anaemia. Therefore, Alpha
Thalassemia trait is assumed to be present ONLY when iron deficiency has been
excluded.
Therefore if a woman has a report identifying ‘possible alpha + thalassaemia
carrier and/or iron deficiency’
1. Investigate a possible anaemia by requesting a ferritin level. If iron deficiency is
identified, review with GP and treat as appropriate.
2. Re-test for haemoglobinopathy status at completion of iron therapy in conjunction
with laboratory advice
If a woman has a report identifying a ‘possible alpha thalassaemia zero and/or
iron deficiency’
1. Investigate a possible anaemia by requesting an urgent ferritin level. If a
deficiency is identified, review with GP and treat as appropriate
2. The Laboratory will liaise with screening coordinators to initiate father of the baby
testing as appropriate
3. Re-test for haemoglobinopathy status at completion of iron therapy in conjunction
with laboratory advice
2.7.1 Pre natal diagnosis
Where prenatal diagnostic is offered it should be undertaken in a timely manner with the aim of CVS being undertaken following appropriate counselling regarding the benefits and risks of an invasive procedure. This will usually be undertaken by the Screening Coordinator and Fetal Medicine Consultant, in liaison with the haematology team.
2.7.2 Linked Programme Alert
Where the mother or the father of the baby is identified as a haemoglobinopathy carrier, the Screening Coordinator will inform the new-born blood spot laboratory in Bristol in the antenatal period via an Alert Form. Details will also be entered onto the Maternity Screening Tracker
2.7.3 Postnatal newborn results
Where an affected new-born is identified through new-born bloodspot screening, the lab will contact the Screening Coordinator who will review the parental result. If any inappropriate/missing actions in the antenatal period are identified a datix must be completed and the incident investigated as per Trust and National Screening Committee process.

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 11 of 21
2.8 ROLES AND RESPONSIBILITIES
2.8.1 Antenatal screening coordinator (ANSCO)
Monitor failsafe and contact community midwifery (CMW) staff where there are concerns relating to antenatal screening for haemoglobinopathies including follow up of missing or incomplete FOQ’s
Inform CMW if screened woman has a result requiring further action as detailed in this guidance
Receive any results requiring further investigation, via the generic screening e-mail account
Contact the woman and arrange for further testing/father of the baby testing, within 3 working days
Track the results where repeat or father of the baby samples have been requested
Arrange for counselling of affected couples and commence high risk pathway
Complete New-born alert proforma and send to Newborn screening lab as per instructions on form
Provide annual updates for midwives on all ante natal and newborn screening
Monitor and complete quarterly key performance indicators (KPI)
Complete the annual report including SCT
Monitoring/audit of screening programmes annually 2.8.2 Midwives responsiblity
Comply with this and all current associated guidance
relating to sickle cell and thalassaemia screening
Ensure the woman receives the leaflet ‘screening tests
for you and your baby’ in advance of her booking
appointment
Ensure the information is available in a format to suit the
needs of the woman, e.g. if English is not the first language
or the woman has a disability
At the booking appointment ensure a discussion takes place with the
woman and her partner about the reasons for testing and gain consent for
testing
Complete the Family Origin Questionnaire (FOQ). If the woman
declines testing the FOQ should still be completed and sent to the lab
Ensures a fit for purpose sample arrives in the haematology
department and obtain a result within 7-10 days
Ensure the woman is aware of the test result
Ensure any positive results are managed in accordance with this guidance with involvement of the local antenatal screening coordinator
Report any adverse events using the Trust Datix system
Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 12 of 21
2.8.3 Laboratory
Appropriate accreditation with a nationally approved scheme e.g. United Kingdom Accreditation Services (UKAS)
Ensure a senior staff member at consultant level (medical or clinical scientist) is responsible for the haemoglobinopathy screening service with defined levels of accountability
Ensure the adoption of the national testing algorithm
Ensure the adoption of the guidelines for standard of reporting screening results
Ensure there is a standard operating procedure for the antenatal sickle cell and thalassaemia programme from receipt of the specimen until the dispatching of the report.
Ensure the provision of a report or interim report within 3 working days of receipt of specimen in the laboratory
Participation in local or national audit relating to the screening programme.
Willing to release of information on screening performance to national screening Committee and its representatives There must be a documented risk management policy for laboratory aspects of Haemoglobinopathy screening
Laboratory must participate in External Quality assurance scheme, Sensitivity of testing protocol >95% detection of carriers/ affected individuals
Failsafe policy and arrangements in laboratory and Maternity services for acting on and reviewing positive screening results. Laboratory to work with Maternity Unit to ensure a joint review of positive results on a regular basis. Participate in regular audit meeting to review accountability and responsibility and screen positive results
Referral of specimens risk assessed for all aspects of the process (responsibility, transfer, receipt of results in a timely manner and reporting) Reports received from third parties/referral laboratories are transcribed into the internal laboratory information systems in a full and exact copy of the report

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 13 of 21
3. Monitoring compliance and effectiveness
Element to be monitored
Key performance indicators (KPI) for antenatal screening to include:
Sickle cell and Thalasseamia screening
Lead Screening Coordinators Jenny Stevenson and Jeanne Clarkson
Tool National KPI tool
ST1 identifies coverage: that SCT screening is offered to the eligible population and each woman accepting screening has a screening result available at the day of the report
ST2 identifies the proportion of women having antenatal SCT screening for whom a result is available by 10+0 days gestation
ST4 measures the timely offer of prenatal diagnosis (PND) to women at risk of having an affected infant. The risk associated with ‘at risk women’ and ‘at risk couples’ is different therefore this KPI is in 2 parts:
1. At risk women offered PND by 12 weeks and 0 days gestation (ST4a).
2. At risk couples offered PND by 12 weeks and 0 days gestation (ST4b).
Frequency Quarterly KPI reporting Annual Report
Reporting arrangements
Bi- annual Screening Programme Board and regional screening team
Acting on recommendations and Lead(s)
Screening Coordinator and Screening Programme Board
Change in practice and lessons to be shared
As per action plan
4. Equality and Diversity 4.1. This document complies with the Royal Cornwall Hospitals NHS Trust service Equality and Diversity statement which can be found in the 'Equality, Diversity & Human Rights Policy' or the Equality and Diversity website.
4.2. Equality Impact Assessment
The Initial Equality Impact Assessment Screening Form is at Appendix 2.

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 14 of 21
Appendix 1. Governance Information
Document Title
Screening: Antenatal screening for Heamoglobinopathies v1.0
Date Issued/Approved: 10th August 2018
Date Valid From: 10th October 2018
Date Valid To: 10th October 2021
Directorate / Department responsible (author/owner):
Antenatal and Newborn Screening: Jenny Stevenson, Jeanne Clarkson
Contact details: 01872 253092
Brief summary of contents To give local guidance on the screening programme for sickle cell/thalassaemia in pregnancy
Suggested Keywords: SCT, sickle cell, thalassaemia, haemoglobinopathy
Target Audience RCHT CPFT KCCG
Executive Director responsible for Policy:
Medical Director
Date revised: August 2018
This document replaces (exact title of previous version):
Sickle Cell and Thalassaemia (SCT) Screening Clinical Guideline V1.0. This is part of a separation of one large guideline so is a new ‘standalone’ guideline and is therefore v1.0
Approval route (names of committees)/consultation:
Maternity Guidelines Group Obstetrics and Gynaecology Directorate Policy Review Group Divisional Board
Divisional Manager confirming approval processes
Tunde Adewopo
Name and Post Title of additional signatories
Not Required
Name and Signature of Divisional/Directorate Governance
{Original Copy Signed}

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 15 of 21
Lead confirming approval by specialty and divisional management meetings Name: Caroline Amukusana
Signature of Executive Director giving approval
{Original Copy Signed}
Publication Location (refer to Policy on Policies – Approvals and Ratification):
Internet & Intranet Intranet Only
Document Library Folder/Sub Folder Clinical/Midwifery and Obstetrics
Links to key external standards Governance Team can advise
Related Documents:
References: NHS Screening Programmes (2017): Sickle Cell and Thalassaemia. Handbook for laboratories UK National Screening Committee (2017) Key Performance Indicators UK National Screening Committee (2017) NHS Sickle cell and Thalassaemia Screening programme: Failsafe processes.
UK NSC (2017) NHS Sickle Cell and Thalassaemia Screening Programme: Standards for the linked Antenatal and Newborn Screening Programme. 3rd edition
Training Need Identified? NO

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 16 of 21
Version Control Table
Date Version
No Summary of Changes
Changes Made by (Name and Job Title)
01 Dec 15 V1.0 Initial Issue Maggie Denholm
10 Aug 18 V1.0
Streamlined national guidance Updated Alpha Thalassaemia recommendations. Taken from the initial issue as above but is v1.0 of a new stand alone Guideline.
Jenny Stevenson Screening Coordinator
All or part of this document can be released under the Freedom of Information Act 2000
This document is to be retained for 10 years from the date of expiry.
This document is only valid on the day of printing
Controlled Document This document has been created following the Royal Cornwall Hospitals NHS Trust Policy for the Development and Management of Knowledge, Procedural and Web
Documents (The Policy on Policies). It should not be altered in any way without the express permission of the author or their Line Manager.

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 17 of 21
Appendix 2. Initial Equality Impact Assessment Form
This assessment will need to be completed in stages to allow for adequate consultation with the relevant groups.
Name of Name of the strategy / policy /proposal / service function to be assessed
Screening: Antenatal screening for Heamoglobinopathies v1.0
Directorate and service area: Obs & Gynae Directorate
Is this a new or existing Policy? Existing
Name of individual completing assessment: Jenny Stevenson/Jeanne Clarkson
Telephone: 01872 253092
1. Policy Aim*
Who is the strategy / policy / proposal /
service function aimed at?
To give guidance to midwives on how and why to offer screening for sickle cell and thalassaemia to our eligible population of pregnant women and to create a link into the postnatal newborn blood spot screening programme
2. Policy Objectives*
To ensure women are offered screening for sickle cell and thalassaemia in accordance with National Screening Committee guidance
3. Policy – intended Outcomes*
To ensure all women are appropriately offered screening in each pregnancy for sickle cell and thalassaemia and women/couples who are identified at higher risk are entered into care in a timely manner
4. *How will you measure the
outcome?
Compliance Monitoring Tool
5. Who is intended to benefit from the
policy?
All pregnant women in our cohort
6a Who did you consult with b). Please identify the groups who have been consulted about this procedure.
Workforce Patients Local groups
External organisations
Other
X
Please record specific names of groups Maternity Guidelines Group Obstetrics and Gynaecology Directorate Policy Review Group Divisional Board

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 18 of 21
Are there concerns that the policy could have differential impact on: Equality Strands: Yes No Unsure Rationale for Assessment / Existing Evidence
Age X
Sex (male,
female, trans-gender / gender reassignment)
X
Race / Ethnic communities /groups
X
Disability - Learning disability, physical impairment, sensory impairment, mental health conditions and some long term health conditions.
X
Religion / other beliefs
X
Marriage and Civil partnership
X
Pregnancy and maternity
X
Sexual Orientation, Bisexual, Gay, heterosexual, Lesbian
X
You will need to continue to a full Equality Impact Assessment if the following have been highlighted:
You have ticked “Yes” in any column above and
No consultation or evidence of there being consultation- this excludes any policies which have
been identified as not requiring consultation. or
Major this relates to service redesign or development
What was the outcome of the consultation?
Guideline agreed
7. The Impact Please complete the following table. If you are unsure/don’t know if there is a negative impact you need to repeat the consultation step.

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 19 of 21
8. Please indicate if a full equality analysis is recommended. Yes No X
9. If you are not recommending a Full Impact assessment please explain why.
No areas indicated
Signature of policy developer / lead manager / director
Jeanne Clarkson
Date of completion and submission 10th August 2018
Names and signatures of members carrying out the Screening Assessment
1. Jeanne Clarkson
2. Human Rights, Equality & Inclusion Lead
Keep one copy and send a copy to the Human Rights, Equality and Inclusion Lead c/o Royal Cornwall Hospitals NHS Trust, Human Resources Department, Knowledge Spa, Truro, Cornwall, TR1 3HD This EIA will not be uploaded to the Trust website without the signature of the Human Rights, Equality & Inclusion Lead. A summary of the results will be published on the Trust’s web site. Signed Sarah Jane Pedler Date 10th August 2018

Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 20 of 21
Appendix 3.
Screening: Antenatal screening for Heamoglobinopathies v1.0
Page 21 of 21
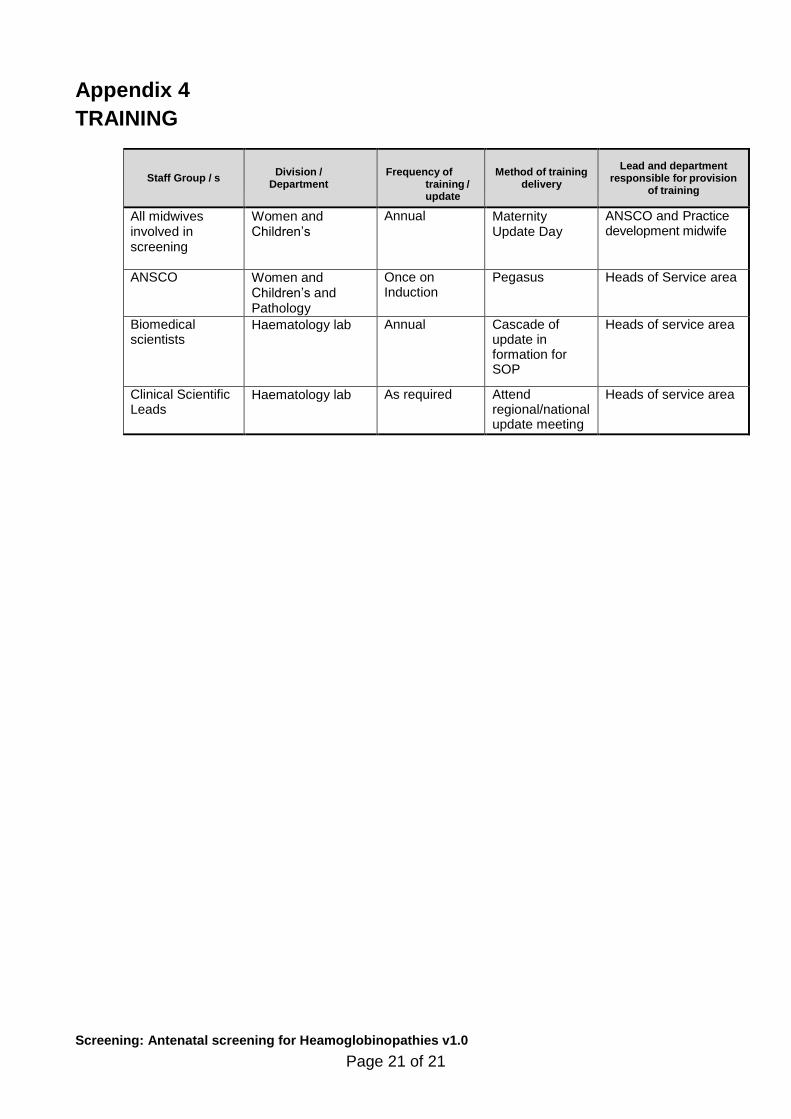
Appendix 4
TRAINING
Staff Group / s
Division /
Department
Frequency of
training / update
Method of training
delivery
Lead and department responsible for provision
of training
All midwives involved in screening
Women and Children’s
Annual Maternity Update Day
ANSCO and Practice development midwife
ANSCO Women and Children’s and Pathology
Once on Induction
Pegasus Heads of Service area
Biomedical scientists
Haematology lab Annual Cascade of update in formation for SOP
Heads of service area
Clinical Scientific Leads
Haematology lab As required Attend regional/national update meeting on scheme
Heads of service area