safety digest 3/04 - assets.publishing.service.gov.uk · safety digest lessons from marine accident...
TRANSCRIPT

SAFETY DIGESTLessons from Marine
Accident Reports3/2004
is an
INVESTOR IN PEOPLE
MA
RIN
E A
CC
IDE
NT
INV
EST
IGA
TIO
N B
RA
NC
H
SAFETY DIGESTLessons from Marine Accident Reports
No 3/2004
MARINE ACCIDENT INVESTIGATION BRANCH
is an
INVESTOR IN PEOPLE
Department for TransportEland HouseBressenden PlaceLondon SW1E 5DUTelephone 020 7944 3000Web site: www.dft.gov.uk
© Crown copyright 2004
This publication, excluding any logos, may be reproduced free of charge in any format or mediumfor research, private study or for internal circulation within an organisation. This is subject to itbeing reproduced accurately and not used in a misleading context. The material must beacknowledged as Crown copyright and the title of the publication specified.
Further copies of this report are available from:MAIB1st FloorCarlton HouseCarlton PlaceSouthamptonSO15 2DZ
Printed in Great Britain. Text printed on material containing 100% post-consumer waste.Cover printed on material containing 75% post-consumer waste and 25% ECF pulp.November 2004

MARINE ACCIDENTINVESTIGATION BRANCH
The Marine Accident Investigation Branch (MAIB) is an independent part of the Department forTransport, the Chief Inspector of Marine Accidents being responsible directly to the Secretary ofState for Transport. The offices of the Branch are located at Carlton House, Carlton Place,Southampton, SO15 2DZ.
This Safety Digest draws the attention of the marine community to some of the lessons arising frominvestigations into recent accidents. It contains facts which have been determined up to the time ofissue.
This information is published to inform the shipping and fishing industries, the pleasure craftcommunity and the public of the general circumstances of marine accidents and to draw out thelessons to be learned. The sole purpose of the Safety Digest is to prevent similar accidents happeningagain. The content must necessarily be regarded as tentative and subject to alteration or correction ifadditional evidence becomes available. The articles do not assign fault or blame nor do theydetermine liability. The lessons often extend beyond the events of the incidents themselves to ensurethe maximum value can be achieved.
Extracts can be published without specific permission providing the source is duly acknowledged.
The Editor, Jan Hawes, welcomes any comments or suggestions regarding this issue.
The Safety Digest and other MAIB publications can be obtained by applying to the MAIB.
If you wish to report an accident or incidentplease call our 24 hour reporting line
023 8023 2527
The telephone number for general use is 023 8039 5500.
The Branch fax number is 023 8023 2459.The e-mail address is [email protected]
Summaries (pre 1997), and Safety Digests are available on the Internet:www.maib.gov.uk
Crown copyright 2004

Extract fromThe Merchant Shipping
(Accident Reporting and Investigation)Regulations 1999
The fundamental purpose of investigating an accident under these Regulations is to determine itscircumstances and the causes with the aim of improving the safety of life at sea and the avoidance ofaccidents in the future. It is not the purpose to apportion liability, nor, except so far as is necessary toachieve the fundamental purpose, to apportion blame.
The role of the MAIB is to contribute to safety at sea by determining the causes andcircumstances of marine accidents, and working with others to reduce the likelihood of suchcauses and circumstances recurring in the future.
MARINE ACCIDENT INVESTIGATION BRANCH
GLOSSARY OF TERMS AND ABBREVIATIONS 6
INTRODUCTION 7
PART 1 – MERCHANT VESSELS 8
1. Exposure to a Potential Killer 10
2. Collision in Fog 12
3. I Know Where I am, But Where am I Going? 13
4. Rule of the Road – What’s that? 16
5. Routine Maintenance Causes Engine Failure – Are Your Instructions Adequate? 18
6. Another Near Miss! – Coaster and Fishing Vessel 20
7. Too Close for Comfort 22
8. It Only Takes One Slip Up to Cause a Fatal Accident 23
9. Blackout! 25
10. Fatal Balancing Act 26
11. Risk of Collision Revisited 27
12. Working Under Pressure 28
13. When Things are Meant to go Wrong 29
14. Breakfast May Be Late 30
15. Offset in the Mediterranean 31
PART 2 – FISHING VESSELS 35
16. Are You Alone? 36
17. Deckhand Dragged Overboard and Lost While Shooting Creels 38
18. Own Goal 40
19. Another Unchecked Flooding 41
20. Fire on Unmanned Crabber 42
21. Down the Fish Room 44
22. Flooding – A Positive Outcome 47
23. Fire-Fighting Training Saves the Day 49
INDEX
PART 3 – LEISURE CRAFT 51
24. Three Family Members Lost on Angling Trip 52
25. Leisure Craft and Commercial Vessels – a Conflict of Interests? 55
26. Fishing for Disaster 56
MAIB NOTICEBOARD 58
APPENDICES 60
Appendix A – Preliminary examinations and investigations started in the 60period 01/07/2004 to 31/10/2004
Appendix B – Reports issued in 2004 60
Glossary of Terms and AbbreviationsAB – Able Seaman
ARPA – Automatic Radar Plotting Aid
CCTV – Closed Circuit Television
CO2 – Carbon Dioxide
CPA – Closest Point of Approach
FRC – Fast Rescue Craft
GPS – Global Positioning System
GT – Gross tons
HS – Hydrogen Sulphide
IR – Infrared
LSA – Lifesaving Apparatus
“Mayday” – Spoken distress signal
MCA – Maritime and Coastguard Agency
OOW – Officer of the Watch
RIB – Rigid Inflatable Boat
RNLI – Royal National Lifeboat Institution
Ro-Ro – Roll on – roll off
TSS – Traffic Separation Scheme
VHF – Very High Frequency
VTS – Vessel Traffic Services
Herewith another batch of salutary tales from thesea. Please take the time to read them – we allfall into bad habits; complacency is probably thegreatest danger at sea. Hopefully these articleswill remind mariners of every kind that ours isnot a forgiving environment, so we must allconstantly be alive to hazards.
Yet again, there are a number of collisions,groundings and near misses in this edition. EionLyons, in his excellent introduction to theMerchant Vessel section, stresses officers of thewatch making wrong decisions. I echo hissentiments. But nearly all officers of the watch,including all those involved in these incidents,know and appreciate “the Rules”, so why are theynot being universally and appropriately applied?Here we must consider two factors: the growingplethora of things to distract the OOW on thebridge, and fatigue. The former is something thatcompanies, masters and OOWs must address –the OOW must not be distracted from his primetask. The latter is still poorly understood. Toomany mariners consider that the only effect offatigue that they need to be concerned about isfalling asleep. This is patently nonsense. Fatigueaffects a person’s alertness, comprehension,decision making abilities, judgment, awareness ofdanger and many other capabilities essential tothe OOW. Our Bridge Watchkeeping Safety Study(published in July 2004 and available on ourwebsite or in hard copy from MAIB) identifiesfatigue as a major causal factor in collisions andgroundings. This has to be addressed.
In the Fishing Vessel section, it is heartening toread two good news stories (cases 22 and 23). Inboth cases, potentially lethal situations weredealt with most professionally, so that vessels andcrews were saved. Forethought, good equipment,training and calm leadership carried the day.Would you be ready to deal with such situationsin your boat?
In the Leisure Craft section, there are two tragiccases involving sea anglers. For fishermen, theboat is merely the means of enjoying their sport,so it often does not receive the attention andcare that is essential.
Please pass these articles on to sea anglers thatyou know, so that they can enjoy their sport insafety.
Stephen MeyerChief Inspector of Marine AccidentsDecember 2004
Introduction
7MAIB Safety Digest 3/2004
When approached by Stephen Meyer with aninvitation to provide an introduction to theMerchant Vessel section of this edition of theSafety Digest, I felt both flattered and privilegedbecause of the opportunity that was presented tome. During the last few years, the Safety Digesthas evolved significantly and is now renownedthroughout the industry for the positivecontribution it provides to improving safetyawareness and performance within the UK fleetand far beyond. However, the Digest is mainlydependent upon the source material, and thecontinued submission of comprehensive incidentreports is therefore actively encouraged.
Consistently, the Safety Digest has providedreaders with a broad selection of reportsdemonstrating the sometimes horrifyingconsequences of our errors or omissions, and thisedition is no different. Although the incidentsare only a very small sample of those reported tothe Marine Accident Investigation Branch, andrecognising that the reports published in theDigest are not selected on any statistical merit, itis nevertheless disturbing and disheartening tonote that almost half occurred because of failuresto properly adhere to the Collision Regulations.Whether this is evidence of a developing trendor not, I am provided with ample justification forreminding all seafarers charged with theresponsibilities of bridge watchkeeping duties tomaintain their knowledge of and adherence tothe provisions of the COLREGS. There has beenmuch debate over recent years during which ithas been suggested that the regulations requireyet further amendment and revision to take
account of ever-evolving technology andworking practices. Whilst that debate willundoubtedly continue ad infinitum, I wouldsuggest that the fundamental problem is not withthe regulations, but with the failure of somewatchkeeping officers to properly adhere tothem. Whether it is failing to maintain aneffective lookout (Another Near Miss!!), actingon the basis of inadequate information (I KnowWhere I Am, But Where Am I Going?), passingat an inappropriately close distance (Too CloseFor Comfort; Risk of Collision Revisited!),failing to take full account of the prevailingcircumstances and conditions (Collision in Fog)or blatant failure to comply with the most basicrequirements of the COLREGS (Rule of theRoad – What’s That?), it is clear that on toomany occasions officers of the watch are makingthe wrong decision. In every one of theseincidents, the difference between what actuallyhappened and a major incident was purely goodfortune. It is incumbent on all of us in positionsof responsibility within the industry; regulators,educational establishments, ship operators,shipmasters and watchkeeping officers alike, tomake every possible effort to ensure betterunderstanding and implementation of the Rulesof the Road.
Obviously the saddest incident reports appearingin the Safety Digest are those during whichsomeone loses their life. There are three suchincidents in this edition, all of which could havebeen avoided if only the risks involved had beenproperly assessed and appropriate preventativemeasures put in place. Whilst neither scientificnor definitive, the evidence available from myown fleet indicates that in excess of 90% of allsafety related failures are entirely avoidable, ifonly greater care and attention had been devotedto the planning, execution and monitoring of thetask being undertaken.
Whilst the other incidents are all important, onein particular struck a familiar chord with my ownexperiences. Several years ago, in order to satisfythe requirements of a contract, it was necessaryfor my company to purchase a vessel. Except for
8
Part 1 – Merchant Vessels
MAIB Safety Digest 3/2004
initial inspection, access to the vessel was deniedand a handover to our incoming crew was notallowed. Investigation of a potentially seriousincident that occurred soon after purchaseidentified that the vessel could not have beenoperating under previous ownership inaccordance with the procedures left on board attime of sale. An effective familiarisation periodwould have identified this anomaly andprevented the incident. “Blackout” highlightsthe importance of ships’ staff having theopportunity to become familiar with theirworking environment. When this involves theacquisition of an existing vessel, it is essentialthat every effort is made to ensure cooperationbetween the leaving and joining crew.
It is the responsibility of all seafarers and shore-based managers to promote and develop aneffective safety culture within individual ships,shipping companies and thereby across the entireindustry. This cannot be done independentlywithout reference to events and initiativeselsewhere within the industry. Consultation andexchange of information are essential to best aidthe reduction in safety related incidents and Icommend this edition of the Safety Digest to youas an effective part of that improvement process.
MAIB Safety Digest 3/2004 9
Eion Lyons
Eion Lyons is Marine Director and Head of Technical Department of F.T. Everard & Sons Limited. Based atDartford in Kent, Everard operate a fleet of petroleum product tankers around the UK, Ireland and closecontinent. Eion went to sea in 1977 with Hunting & Son, joined Bolton Maritime Management in 1981gaining command in 1988 before spending some time with Sealink. His sea service encompassed tankers, bulkcarriers, ro-ro passengers and OBOs. He joined Everard as an Assistant Marine Superintendent, progressedto Quality Manager and was promoted to his current role in 1995.
A Fellow and Council Member of the Nautical Institute, Eion is an Elder Brother and Assistant MarineDirector of the Corporation of the Newcastle Upon Tyne Trinity House. He represents Everard on panels atthe UK Chamber of Shipping and at other industry organisations.

Narrative
On board a passenger ship, a crossover linebetween the port and starboard ballast/treatedblack water/grey water tanks passed through anadjacent cofferdam. The pipework in thecofferdam had suffered corrosion, and thisallowed sewage to build up in the tank. Ship’sstaff were aware of the problem, and permanentrepairs were planned for the next refit which wasdue within a few months.
Because of the amount of liquid that had leakedinto the cofferdam, it was decided to empty thecontents using a portable salvage pump. Thecofferdam had been opened on a number ofoccasions without cause for concern.
The appropriate tank rescue equipment wasassembled in the vicinity of the tank lid, inaccordance with the company’s ‘Permit to Work– Entry into Confined Spaces’ procedures. Tworatings removed the port aft lid to ventilate the
tank, so that the senior first officer could test theatmosphere and complete the Permit to Work.Immediately on lifting the lid, the ratingsnoticed a strong smell of sewage. They insertedthe fan extension hose into the tank and vacatedthe area.
A short while later, the senior first officer arrivedto conduct the routine atmosphere test. Whileapproaching the tank, his multi-gas detectorregistered an alarm and recorded a hydrogensulphide (HS) reading of 98 parts per million.The compartment was immediately evacuatedand the watertight access doors closed.
The cofferdam lid was re-secured 15 minuteslater by a rating wearing full compressed airbreathing apparatus.
The ship’s senior doctor examined the tworatings who had removed the cofferdam lid, andtreated them for exposure to hydrogen sulphide.They remained fit for duty.
10
Exposure to a Potential Killer
MAIB Safety Digest 3/2004
CASE 1
11MAIB Safety Digest 3/2004
CASE 1
The Lessons
1. Over-exposure to the potentially lethaltoxic gases was prevented because theratings vacated the area immediatelyafter opening the cofferdam lid. Thesenior first officer fully recognised thedangers, and understood the meaning ofthe multi-gas detector alarm and readinglevels. His direction to fully isolate thecompartment stabilised the situation andprevented the possible contamination ofother areas.
2. The need to quickly replace thecofferdam lid was recognised, and thiswas achieved in a controlled, safemanner, making use of the compressedair breathing apparatus to provide safetyto personnel.
3. Strict adherence to the company’s Permitto Work procedures ensured that allappropriate safety equipment wasimmediately available, and procedureswere followed which reduced the risksassociated with this potentiallydangerous activity.
4. It is advisable to test the atmosphere onopening tank lids, because potentiallylethal levels of HS can be released if tanklevels are high and the surface isdisturbed by the ship’s movement. Inaddition, it is prudent to don breathingapparatus when opening tank lids if theatmosphere in the compartment isunknown.
5. Whenever corrosion or componentfailure compromises the integrity ofsewage systems, every effort should bemade to repair the defect as soon aspossible to prevent exposure to toxic HSgases. If sewage systems, orcompartments suspected of containingsewage, are opened, there will be adanger from the release of HS gas.Concentrations as low as 10 parts permillion are toxic, as indicated in MarineGuidance Note 33 (M+F). It should alsobe noted that HS might be released fromstagnant bilge areas that contain animal,vegetable or mineral oils which havebeen mixed with salt water, especiallywhen the surface has been disturbed.
Narrative
A ship was on a river passage with a pilotembarked. As the visibility was about one cable,the bridge organisation was configured toconduct blind pilotage. Also, the navigationlights were switched on, a fog lookout waspositioned on the forecastle, engines were readyfor immediate manoeuvre and speed wasmoderated to 8 knots. On the advice of the pilot,sound signals were not sounded.
As the ship approached a container terminal,visibility improved to about one mile, so the foglookout was stood down and speed increased to
12 knots. Minutes later, however, the visibilitydeteriorated, and speed was reduced again to 8knots. A tug pushing three barges loaded withcontainers was then seen at about one cable onthe ship’s head. At about the same time, theVTS advised that a tug was one cable ahead, anda small radar target was seen separating from theclutter in the vicinity of one of the containervessels berthed alongside. Full astern wasordered, quickly followed by emergency fullastern.
Fortunately, although the ship’s starboard bowhit the tug’s port quarter, neither vessel wasdamaged and there were no casualties.
12
Collision in Fog
MAIB Safety Digest 3/2004
CASE 2
The Lessons
1. When navigating in river ports, notablyin Europe, where many have docksextending for several miles and a lot ofbarge traffic, small vessels such as tugsand tows are likely to pop up frombehind moored vessels or side entranceswithout warning. This is particularlydangerous in restricted visibility when aVTS is often unable to control suchvessels, or to give adequate warning oftheir approach, due to limitations of itsown radar coverage. As always,therefore, self-help through a sharpvisual and radar lookout is the best firstline of defence against this danger.
2. Operating in confined waters, theforward mooring team is normally athand to let go the anchor if required, andit is logical to use these people aslookouts when the situation dictates. Inthick fog, a lookout in the eyes of a shipshould see and hear other vessels aheadbefore anyone on the bridge, and theseconds saved might just be enough tomake any action taken in order to avoida collision successful.
3. Don’t be caught out by relaxing theprecautions taken for restricted visibilitytoo hastily. Fog is a wonderfullyfrustrating phenomenon, which can becompletely unpredictable. Whenvisibility appears to be improving, stayon your guard, it can deteriorate twice asquickly and without warning.
4. Despite the requirement of the collisionregulations, it is increasingly apparentthat consideration of stopping distance isnot at the top of a master’s prioritieswhen determining safe speed.Consequently, when suddenly faced withanother vessel at close range, many shipswould be unable to avoid a collision byjust stopping. As few other alternativesare available in restricted waters,collisions are inevitable. Stoppingdistances are important whendetermining safe speed. Themanoeuvring data provided on bridgebulkheads is not a decoration, it is thereto be used.
Narrative
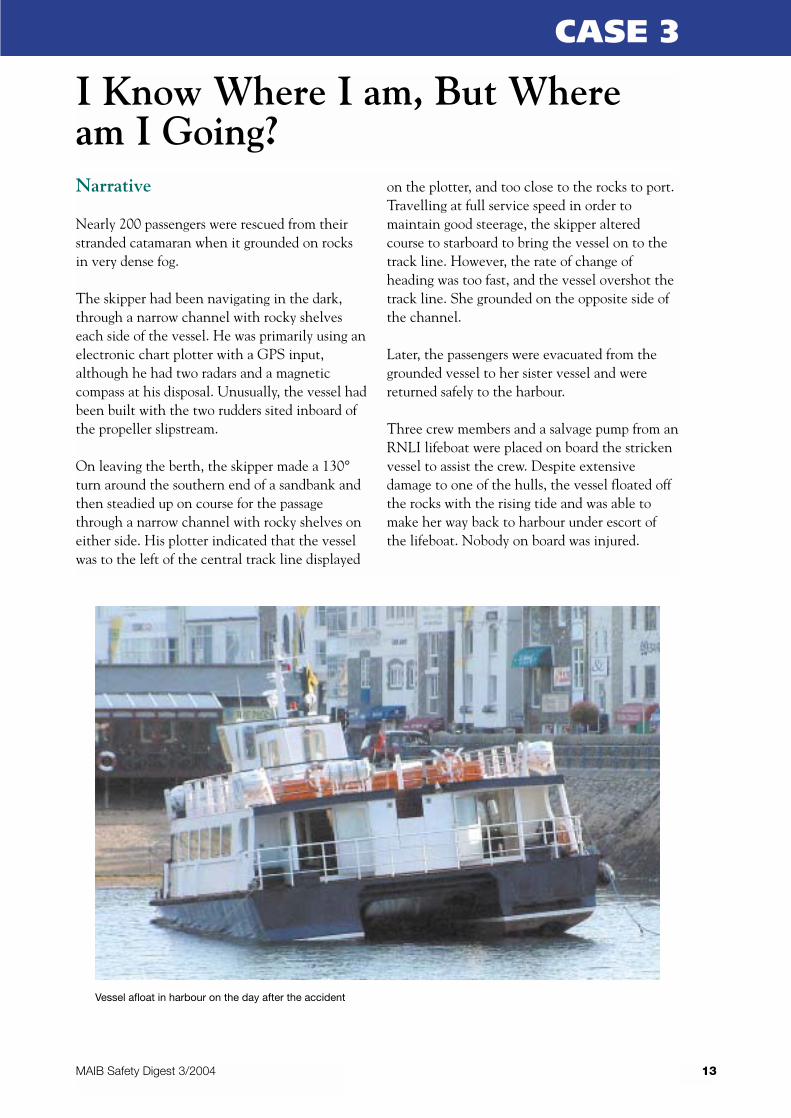
Nearly 200 passengers were rescued from theirstranded catamaran when it grounded on rocksin very dense fog.
The skipper had been navigating in the dark,through a narrow channel with rocky shelveseach side of the vessel. He was primarily using anelectronic chart plotter with a GPS input,although he had two radars and a magneticcompass at his disposal. Unusually, the vessel hadbeen built with the two rudders sited inboard ofthe propeller slipstream.
On leaving the berth, the skipper made a 130°turn around the southern end of a sandbank andthen steadied up on course for the passagethrough a narrow channel with rocky shelves oneither side. His plotter indicated that the vesselwas to the left of the central track line displayed
on the plotter, and too close to the rocks to port.Travelling at full service speed in order tomaintain good steerage, the skipper alteredcourse to starboard to bring the vessel on to thetrack line. However, the rate of change ofheading was too fast, and the vessel overshot thetrack line. She grounded on the opposite side ofthe channel.
Later, the passengers were evacuated from thegrounded vessel to her sister vessel and werereturned safely to the harbour.
Three crew members and a salvage pump from anRNLI lifeboat were placed on board the strickenvessel to assist the crew. Despite extensivedamage to one of the hulls, the vessel floated offthe rocks with the rising tide and was able tomake her way back to harbour under escort ofthe lifeboat. Nobody on board was injured.
13
I Know Where I am, But Wheream I Going?
MAIB Safety Digest 3/2004
CASE 3
Vessel afloat in harbour on the day after the accident

14 MAIB Safety Digest 3/2004
CASE 3
Photographs of hull showing position of propeller and offset rudder
MAIB Safety Digest 3/2004
The Lessons
1. Blind pilotage, which relies totally oninstrumentation when navigating in fog,should be practised regularly to ensurethat bridge personnel are familiar with,and practised in, the interpretation ofthe critical navigational displays that areused during this process.
2. Total reliance on only one navigationalaid (the chart plotter in this case) in fogis insufficient; skippers shouldfrequently scan the other navigationalaids (radar, compass, rate-of-turnindicator) to obtain a greater andconstant sense of orientation.
3. The design feature of the siting of therudders outside the propeller stream hadthe knock-on effect of making the vesseldifficult to manoeuvre at less than fullspeed. This was not ideal whennavigating through a narrow channelwith rocks each side, in fog. Followingthis accident, the owners changed thearrangement of the rudders to improvethe vessel’s manoeuvrability at lowspeed.
4. A high standard of subdivision can keepa grounded vessel afloat long enough toallow passengers to be evacuated and/orto enable the vessel to reach a safehaven.
CASE 3
15
Narrative
A ferry was crossing the Dover Traffic SeparationScheme (TSS) on passage from Dover, with theintention of passing close west of the MPC buoy.A tanker was crossing the north-east traffic lane,intending to pass to the east of the MPC buoyand to then join the south-west traffic lane. Itwas daylight with good visibility.
Instead of following the planned track, thetanker’s master altered course to port to pass tothe south of the MPC buoy. This caused thevessel to cross the north-east traffic lane at anoblique angle.
The vessels were now on a collision course, withthe tanker about 30° on the ferry’s port bow. Theferry gave a series of short flashes. On receivingno response, these were repeated.
The tanker’s master called the ferry on VHFradio channel 16, enquiring about the ferry’sintentions and indicating that he intended toalter course to port.
With no action being taken by the tanker, theferry altered course to starboard. The tanker thenaltered course to starboard around the ferry’sstern.
16
Rule of the Road – What’s that?
MAIB Safety Digest 3/2004
CASE 4
The Lessons
1. The decision taken by the tanker’smaster, to alter course to port whilecrossing the north-east traffic lane,resulted in the vessel following a trackfar removed from that intended, and incontravention of Rule 10(c) of theCollision Regulations.
2. It was while on this latter course that arisk of collision developed with the ferry.The ferry was on the tanker’s starboardbow. It was therefore a crossingsituation, with the tanker the give-way
vessel. However, rather than takingaction in accordance with Rule 15, thetanker’s master decided to alter course toport. This would have caused the tankerto cross ahead of the ferry, incontravention of that rule.
3. The incident could have been avoidedhad the tanker crossed the TSS asoriginally planned, or taken early actionto avoid collision in accordance withRule 16 and exercised the precaution ofkeeping clear of the MPC buoy inaccordance with Rule 2(a).

17MAIB Safety Digest 3/2004
CASE 4
Narrative
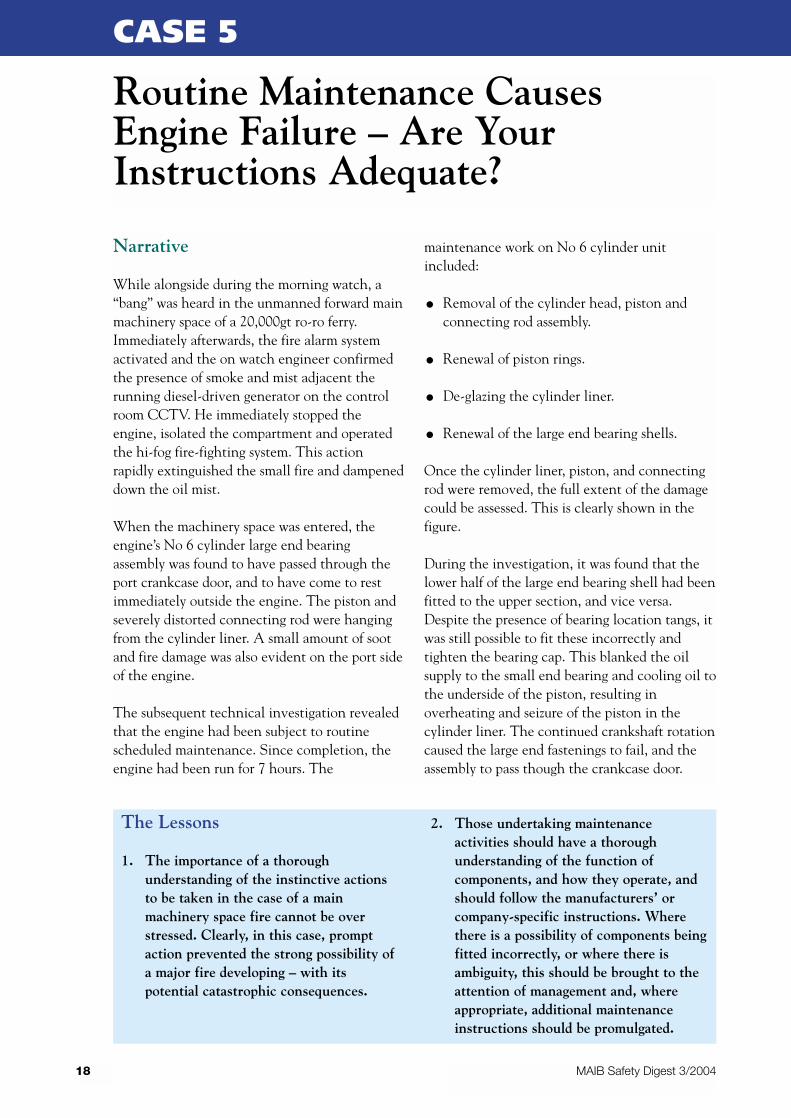
While alongside during the morning watch, a“bang” was heard in the unmanned forward mainmachinery space of a 20,000gt ro-ro ferry.Immediately afterwards, the fire alarm systemactivated and the on watch engineer confirmedthe presence of smoke and mist adjacent therunning diesel-driven generator on the controlroom CCTV. He immediately stopped theengine, isolated the compartment and operatedthe hi-fog fire-fighting system. This actionrapidly extinguished the small fire and dampeneddown the oil mist.
When the machinery space was entered, theengine’s No 6 cylinder large end bearingassembly was found to have passed through theport crankcase door, and to have come to restimmediately outside the engine. The piston andseverely distorted connecting rod were hangingfrom the cylinder liner. A small amount of sootand fire damage was also evident on the port sideof the engine.
The subsequent technical investigation revealedthat the engine had been subject to routinescheduled maintenance. Since completion, theengine had been run for 7 hours. The
maintenance work on No 6 cylinder unitincluded:
• Removal of the cylinder head, piston andconnecting rod assembly.
• Renewal of piston rings.
• De-glazing the cylinder liner.
• Renewal of the large end bearing shells.
Once the cylinder liner, piston, and connectingrod were removed, the full extent of the damagecould be assessed. This is clearly shown in thefigure.
During the investigation, it was found that thelower half of the large end bearing shell had beenfitted to the upper section, and vice versa.Despite the presence of bearing location tangs, itwas still possible to fit these incorrectly andtighten the bearing cap. This blanked the oilsupply to the small end bearing and cooling oil tothe underside of the piston, resulting inoverheating and seizure of the piston in thecylinder liner. The continued crankshaft rotationcaused the large end fastenings to fail, and theassembly to pass though the crankcase door.
18
Routine Maintenance CausesEngine Failure – Are YourInstructions Adequate?
MAIB Safety Digest 3/2004
CASE 5
The Lessons
1. The importance of a thoroughunderstanding of the instinctive actionsto be taken in the case of a mainmachinery space fire cannot be overstressed. Clearly, in this case, promptaction prevented the strong possibility ofa major fire developing – with itspotential catastrophic consequences.
2. Those undertaking maintenanceactivities should have a thoroughunderstanding of the function ofcomponents, and how they operate, andshould follow the manufacturers’ orcompany-specific instructions. Wherethere is a possibility of components beingfitted incorrectly, or where there isambiguity, this should be brought to theattention of management and, whereappropriate, additional maintenanceinstructions should be promulgated.

19MAIB Safety Digest 3/2004
CASE 5
Damage to No 6 Cylinder Components

Narrative
A 1,700gt products tanker was on a south-easterly course 3 miles off the Yorkshire coast.The master was on watch and was alone on thebridge. He was steering by autopilot, there was anorth-westerly wind force 4 to 5 blowing and a1.5 to 2m swell. The visibility was good.
Towards the end of his watch, the masterdetected visually, and soon after using binoculars,a small vessel approximately 2.5 miles ahead. Hethen attempted to acquire the target on thevessel’s ARPA, but was unable to obtain anaccurate fix.
Based on his visual assessment, he assumed theother vessel to be on a course similar to that ofhis own. He also assumed he was the overtakingvessel and would pass clear to the east. Confidentof his assumption, he went to the chart table,which was positioned in the aft part of thebridge, and began plotting a position on thechart.
On board the other vessel, a 10m fishing vesselengaged in trawling on a north-westerly course,the skipper detected the coaster at a distance ofapproximately 3 to 4 miles ahead, on or near acollision course. As the distance decreased, hebecame concerned and called the coaster severaltimes on channel 16 VHF radio, but received noreply. As the distance decreased further, theskipper realised the coaster would not be able totake avoiding action in ample time, and beganaltering course hard to starboard.
At that instance, the master on the coasterreturned to the forward part of the bridge anddetected the fishing vessel 5 to 6 cables ahead.He then altered course hard to starboard. Bothvessels passed each other within a distance of1 cable.
The somewhat shaken skipper of the fishingvessel reported the incident to the coastguard.
The fishing vessel was displaying the correctsignal for a vessel engaged in trawling.
20
Another Near Miss! – Coaster andFishing Vessel
MAIB Safety Digest 3/2004
CASE 6
The Lessons
1. This incident is another one of the manynear misses the MAIB receives betweencoastal vessels and vessels engaged infishing. When navigating in coastalwaters, always be aware that the majorityof fishing vessels, while engaged infishing, are hampered by their gear andwill be slow to react when alteringcourse, whether it be through evasiveaction or not. The best solution is to givethese vessels a wide berth at all times.Resist the temptation to get close.
2. It is impossible to both maintain a properlookout and work at the chart table forany length of time. In accordance withRule 5 of the Collision Regulations, aproper lookout should have beenmaintained at all times by all availablemeans. An additional person shouldalways be employed on the bridge as adedicated lookout when the officer of thewatch has other duties to attend to.Doing so, would have averted this nearmiss.

21MAIB Safety Digest 3/2004
CASE 6
Photograph of fishing vessel and coaster showing relative sizes
Narrative
The watchkeeping officer of a feeder containervessel detected, by ARPA, a group of fishingvessels ahead at a distance of approximately11 miles.
As the distance between them decreased, thewatchkeeping officer altered course 30° to portto leave the group of fishing vessels clear on hisstarboard side. However, one fishing vessel,which was trawling away from the group,remained on the container vessel’s port side at adistance considered safe by the watchkeepingofficer. She was trawling in a north-westerlydirection at a speed of approximately 2.5 knots,5 miles from the coast, when her skipper firstdetected the container vessel at a distance ofapproximately 4 miles. She was displaying theappropriate daytime signals for a vessel engagedin trawling. The visibility was good.
When the distance between the two vesselsdecreased to approximately 1 mile, the fishingvessel’s skipper became concerned because thecontainer vessel appeared to be taking noavoiding action. He called the container vesselon VHF radio channel 16 to attract herattention. He received no reply. The fishingvessel was constrained from altering course tostarboard for fear of coming fast on two nearbywrecks.
The container vessel still had the remainingfishing vessels on her starboard side. Thankfully,and just in the nick of time, the container vesseldid alter course to starboard. The two vesselspassed each other at a distance of approximately30 metres.
22
Too Close for Comfort
MAIB Safety Digest 3/2004
CASE 7
The Lessons
1. The MAIB receives regular incidentreports from the coastguard of nearmisses between coastal vessels andvessels engaged in fishing. It is an all toofamiliar situation.
However tempting it might be to getclose to fishing vessels, for whateverreason, whether intending minimumdeviation from track, or just out of sheercuriosity, a fishing vessel engaged infishing is the stand-on vessel under theCollision Regulations. This means theyshould be given a wide berth at all times,especially in coastal areas where vesselstend to fish in a fleet. Most fishingvessels have a variety of gear, oftenextending into the seaway by half a mileor more. In addition to this, their course
and speed can be unpredictable,especially when they are hauling andshooting their gear.
2. Consideration for other users of the seais a must. Think ahead, and recognisehow your actions might affect others.Had this been done, this incident couldhave been avoided.
3. In this instance, there was a lack ofunderstanding of each other’s limitations.The container vessel was hampered bythe other fishing vessels on her starboardside, and the fishing vessel was restrictedby seabed obstructions. Had each beenfully aware of the other’s limitations,more substantial avoiding action couldhave been taken at a much earlier stage –before the situation became far too closefor comfort.
Narrative
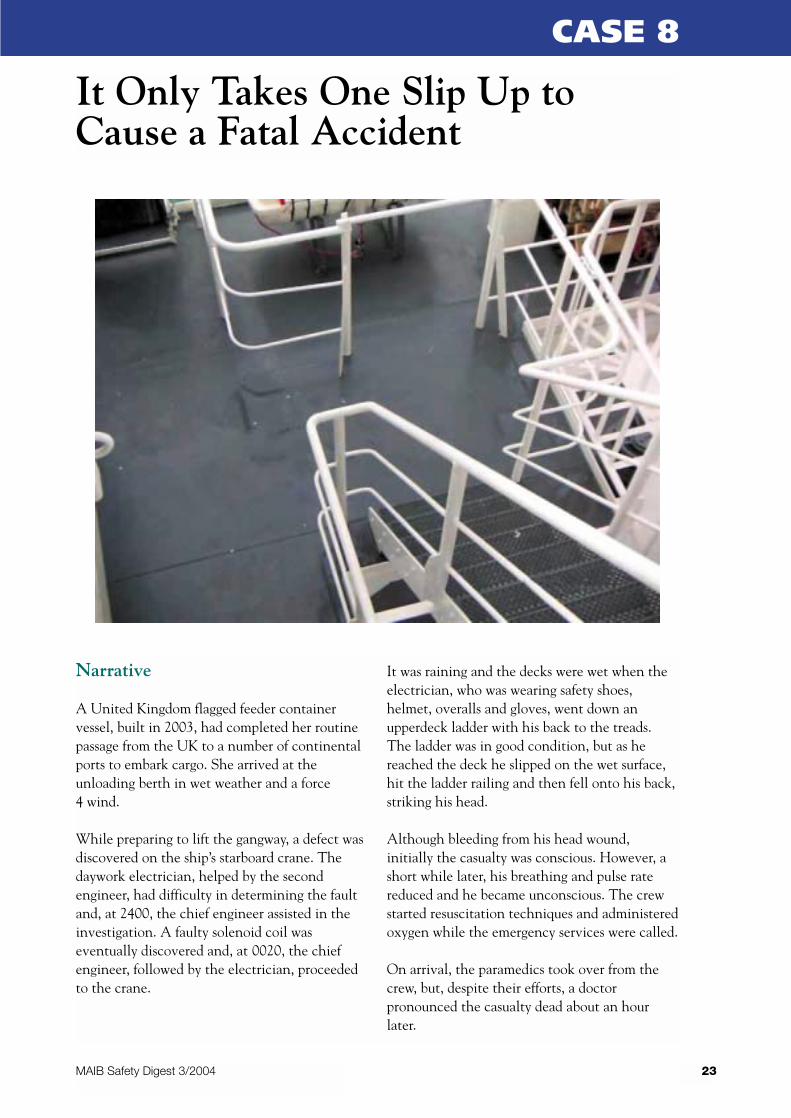
A United Kingdom flagged feeder containervessel, built in 2003, had completed her routinepassage from the UK to a number of continentalports to embark cargo. She arrived at theunloading berth in wet weather and a force4 wind.
While preparing to lift the gangway, a defect wasdiscovered on the ship’s starboard crane. Thedaywork electrician, helped by the secondengineer, had difficulty in determining the faultand, at 2400, the chief engineer assisted in theinvestigation. A faulty solenoid coil waseventually discovered and, at 0020, the chiefengineer, followed by the electrician, proceededto the crane.
It was raining and the decks were wet when theelectrician, who was wearing safety shoes,helmet, overalls and gloves, went down anupperdeck ladder with his back to the treads.The ladder was in good condition, but as hereached the deck he slipped on the wet surface,hit the ladder railing and then fell onto his back,striking his head.
Although bleeding from his head wound,initially the casualty was conscious. However, ashort while later, his breathing and pulse ratereduced and he became unconscious. The crewstarted resuscitation techniques and administeredoxygen while the emergency services were called.
On arrival, the paramedics took over from thecrew, but, despite their efforts, a doctorpronounced the casualty dead about an hourlater.
23
It Only Takes One Slip Up toCause a Fatal Accident
MAIB Safety Digest 3/2004
CASE 8
24 MAIB Safety Digest 3/2004
CASE 8
The Lessons
1. When conducting risk assessments, dueregard should be paid to the condition ofladders and to the immediate deck area,which may become slippery anddangerous when wet, especially in heavyseaways. Careful consideration shouldalso be given to applying non-slip paint,or using other methods to improve thetraction in these risk areas.
2. Although, ultimately, the crew wereunable to save their badly injuredcolleague, the regular drills which hadbeen conducted on board their vessel,helped them deal with the situationquickly and confidently. Byadministering first-aid to the electrician,they were able to stabilise him until theemergency services arrived.
Narrative
A coaster, recently purchased by new owners,completed unloading her bulk cargo at a berth ina small harbour. She did not take on a freshcargo, and in order to catch the tide left herberth without taking on any ballast.
While manoeuvring from her berth, asternengine movements caused aeration of the wateraround her stern sufficient to affect the coolingwater intake to her port side generator, whichwas running. As a result, this began to show signsof overheating.
The motorman attempted to start the starboardgenerator, but found its starting batteries flat. Asthe batteries on the starboard generator weretotally independent of those on the port sideunit, he disconnected one on the port generatorwith the aim of using it on the starboard unit.
As the motorman was making these changes, thevessel was about to clear the harbour entranceand began making a starboard turn to follow thechannel. Coinciding with this were indicationsin the wheelhouse that the vessel had suffered acomplete electrical failure, including the 24voltemergency system. However, no alarms soundedand all warning lights went out because thesewere supplied by the 24volt system.
The master changed over to emergency steering.Although the main engine continued to run, hewas unable to prevent the vessel grounding,partly due to the hand-powered emergencysteering being very heavy. The falling tideprevented her from being refloated until severalhours later, fortunately without serious damage.
25
Blackout!
MAIB Safety Digest 3/2004
CASE 9
The Lessons
1. Taking on ballast before departure wouldhave given both the propeller andgenerator cooling water intake greaterimmersion, and would have reduced theeffects of propeller wash on the portgenerator’s cooling system. Ballastingoperations should be part of the vessel’sstandard departure procedures and safetymanagement system.
If a tide is missed because essentialsafety-related operations have to becompleted, then an owner, and others,must accept that safety is the priority.
2. The motorman, who had been on thevessel only a few days, was unaware thatthe 24volt system was supplied from thebatteries on the port generator, and thatthis system also held closed the breakerson the main 220volt system. Breaking
into the battery system on the generatorcaused total loss of electrical power onboth 24volt and 220volt systems. Theimportance of the 24volt system to thesafety of the vessel should be indicatedby warnings, in the form of signs postedon the batteries and an entry in thevessel’s safety management system.These will assist new crew members infuture.
3. The crew had been on board for only afew days before these events took place,and had little opportunity to becometotally familiar with the vessel. This wascompounded by limited technicaldocumentation being passed from theprevious owners. It is important that allcrew new to a vessel have theopportunity to become familiar with heressential safety-dependent systems beforebeing required to sail her.
Narrative
A fast rescue craft (FRC) returned to its mothervessel, with supplies from ashore which includedfour large gas bottles used for welding and metalcutting. The crew on board the FRC comprisedthe skipper, engineer and cook.
When the FRC came alongside the vessel, theengineer and cook climbed out of it, and theengineer removed his lifejacket. The skipperconnected up the lifting hook from the vessel’scrane to the FRC. The FRC’s painter was tiedloosely to the vessel’s guardrail.
The skipper stayed on board the FRC as it washoisted from the water and raised level with thevessel’s deck. The engineer assisted with thestores transfer but, during the unloadingoperation, the loose gas bottles rolled, thepainter released and the FRC began to dip at thebow and ship water.
To counteract the increasing trim of the FRC bythe bow, the engineer jumped into the stern ofthe FRC. This caused it to tip vertically and thestern to come into contact with the lifting strop.
In an effort to stabilise the FRC, it was loweredback to the water. As the bow re-entered thewater, it further unbalanced the FRC, the gasbottles were lost over the bow and the FRCbegan to flip through 180°. The skipper managedto cling to the lifting strop. The engineer,however, was washed off and swept away.
Time was of the essence, as the crew, desperate tosave their colleague fighting against a strong tide,attempted to restart the FRC’s engine.Unfortunately, it had become submerged whenthe FRC flipped over, putting it out of action.The crew started the mother vessel’s engine, cutthrough the anchor chain and hurriedly threw alifebelt to their colleague. But it was too late.Before the engineer was able to grab it, he driftedaway from them. His body was recovered 2 weekslater.
26
Fatal Balancing Act
MAIB Safety Digest 3/2004
CASE 10
The Lessons
1. No risk assessments had been carried outfor operations involving the FRC. Hadthey been, the following risks might havebeen exposed:
• Transfer of crew and stores to/fromthe FRC;
• Lifting operation of the FRC withcrew/stores on board;
• Carrying heavy stores;
• Suitable survival clothing;
• Man overboard.
2. Had the heavy gas bottles been suitablysecured in the FRC, or removed before itwas hoisted, loose heavy loads would nothave moved around and destabilised theFRC.
3. The engineer probably decided – on thespur of the moment – to jump onto theFRC from the vessel, to prevent thestores being lost overboard. It was aselfless action, but one that cost him hislife. Everyone needs to place safety first.
Narrative
A cargo vessel was steering 260° at 8.5 knots. Itwas daylight with good visibility. A fishing vesselwas trawling in a northerly direction at 2.2knots.
The cargo vessel’s master was on watch. He sawthe fishing vessel on his port bow, interpretedfrom his ARPA that she would pass 0.5 mileahead, and initially decided to maintain courseand speed.
The fishing vessel’s skipper, however, concludedthat a risk of collision existed, and expected thecargo vessel to take avoiding action. With noaction apparent, he attempted to contact thecargo vessel by VHF radio, without success.
The cargo vessel then altered course to starboardand passed close ahead of the fishing vessel.
27
Risk of Collision Revisited
MAIB Safety Digest 3/2004
CASE 11
The Lessons
1. The cargo vessel’s master interpretedthat a risk of collision did not exist. Hebased this interpretation on the fact thatthe fishing vessel was expected to crossahead at a range of 0.5 mile. However, inview of their respective tracks, her CPAwould have been only 0.1 mile.Therefore, it is hardly surprising that thefishing vessel’s skipper felt vulnerable,and wished the cargo vessel to takeavoiding action.
Rule 7 of the Collision Regulationsrequires all available and appropriatemeans to be used in determining if a riskof collision exists, and warns of thedangers of misinterpretation and ofmaking assumptions based on scantyinformation.
In this case, the cargo vessel should haveexercised caution, and should have takenavoiding action at an early stage.
2. When the cargo vessel’s mastereventually decided to take action, hechose to alter course to starboard. Atthis late stage, this was unwise for tworeasons: firstly, the alteration effectivelyincreased the risk of collision initiallyand, secondly, it resulted in his vesselpassing ahead of the other, which wouldhave done nothing to alleviate theanxiety held by the fishing vesselskipper.
At this stage, an alteration of course toport would have immediately increasedthe fishing vessel’s CPA, and given theskipper an assurance that a risk ofcollision had been eliminated.
Narrative
A third officer was in charge of the deck of aproduct tanker while loading motor spirit. Hewas accompanied by an extra third officer and anAB, and had received written instructions fromthe chief officer.
The plan was to load No 3 wing tanks, followedby No 1 centre tank. The pumping rate was800m3 per hour, and as the No 3 wing tanksneared their intended level, the third officerinstructed the AB to open the intermediate valveto No 1 centre tank. The AB, however, openedthe intermediate valve to No 2 centre tank.
The AB was then instructed to open the tankvalve on No 1 centre. Unwittingly, the AB
opened the valve to No 2 centre, but his errorwent unnoticed as he was obscured from theofficers’ view. On hearing the AB’s report thatthe valve was open, the third officer closed thevalve to No 3 port. Moments later, the extrathird officer closed the tank valve on No 3starboard, and because of the configuration ofthe pumping arrangements, this was against thefull flow of the shore pump.
At that point, the centre deck line in way of theVJ coupling, ruptured, causing approximately6m3 of motor spirit to spill onto the deck. Theloading was immediately stopped, the generalalarm was sounded, and the accommodationvents shut down. The engine room was alsoadvised. The spill was successfully cleared and nopollution resulted.
28
Working Under Pressure
MAIB Safety Digest 3/2004
CASE 12
The Lessons
1. Everybody is prone to an occasional lapsein concentration, and it only requiresone basic error during the loading of oiland gas products to spoil everyone’s day.Mistakes, however, need not end indisaster, provided they are spotted early.Cross-checking by a second person is oneof the simplest – yet most effective –ways of doing this, and should be doneregardless of how routine a task, or howcompetent an individual. It is not a slighton a person’s ability, but is a provensafety procedure used to good effect bymany industries and professionals,including aircraft pilots.
2. When cargo is coming on board at highpressure, it pays dividends not to close atank until after verifying that there is aflow into another tank. Otherwise,something has to give, and the resultingsound will be more than just the masterblowing his top!
Narrative
A sophisticated, newly completed, twin screwvessel was on builders’ trials. She had completeda seagoing phase of her trials and was to return toher berth at the builder’s yard. During thesetrials, one of the processors serving themachinery management system failed. Thisprocessor was switched off but, as a result, thecontrol panel’s warning light remained on.
The approach to her berth was along a river andbuoyed channel. Shortly after the pilot boarded,a signal on the machinery monitoring systemindicated a fault with one main engine togearbox clutch. However, the clutch appeared tobe performing correctly and the chief engineerdecided the problem was due to aninstrumentation fault. The vessel continued itspassage upriver.
As the vessel entered a narrow part of thechannel, the pilot requested a slight change ofheading to port. The helmsman brought the
head around and applied starboard helm tosteady her on her new heading.
However, the vessel’s head continued to pay offto port. In spite of applying more starboard helm,the helmsman was unable to stop the headpaying off to port even more rapidly.
Both propellers were put on to astern pitch andhelm hard to starboard. Despite these efforts, thehead continued to swing to port. However, speedcame off the vessel, but not before she touchedbottom. She remained grounded for nearly 7hours when, with the aid of tugs, she was floatedfree and towed to her berth.
Initial investigation established that the portpropeller had spontaneously moved to full asternpitch just, coincidentally, as the initial courseadjustment was made, as requested by the pilot.Tests showed that connections in a cableconnector were intermittently poor and hadresulted in the port propeller misbehaving.
29
When Things are Meant to goWrong
MAIB Safety Digest 3/2004
CASE 13
The Lessons
1. Among other objectives, builders’ trialsare for highlighting defects in a vesseland its systems. At these times, failuresmust be expected, and provision made toensure the vessel’s safety. The earlierproblems with the processor and clutchinstrumentation suggest that there weresufficient warnings of possible problemsbefore the river passage began. Until alltests and trials are satisfactory, the closeattendance of tugs, when in restrictedwaters, is a prudent provision.
2. A continuously shown alarm rapidlybecomes an ignored alarm. Theilluminated single alarm lamp on thiscontrol panel made it difficult to give anysubsequent alarm condition its properstatus, and confer on it the appropriatelevel of urgency. Great care needs to beapplied to the configuration of machineryalarm systems to ensure each is given theconsideration it deserves.
Narrative
During his preparations for cooking breakfast, acook switched on a large electrically heatedhotplate, used for cooking food in bulk, andcoated it with cooking oil to ready it for grilling.
As its temperature increased, the cooking oil onthe hotplate ignited.
The cook smothered the flames, using theintegral hinged hood of the hotplate, and cooledthe unit using a clean water supply.
Once cooled, the hotplate was examined. It wasfound that one of its three electric heatingelements was defective. This was the elementclosest to the unit’s single thermostat.
Because the unit’s thermostat was adjacent to thefailed heating element, it was sensing the coolestarea of the hotplate. The two working elementscontinued to heat the remaining part of thehotplate but, because the thermostat was sensinga low temperature, the increasing and excessivetemperature was not being sensed. This unevenheating process continued until the coating ofcooking oil reached its auto-ignition temperatureand burst into flames.
30
Breakfast May Be Late
MAIB Safety Digest 3/2004
CASE 14
The Lessons
1. Defects in any electrically heatedequipment should be rectified as soon asthey are detected.
2. A second, sensibly placed, thermostatcould have prevented the localisedexcessive heating.
3. Using water to tackle an oil or fat fire isnot advisable. In this case, water wasused to cool the exterior of the hotplate,after its integral lid had been closed tosmother the fire and the electrical supplyisolated. Water was thus separated fromthe hot oil and any live conductors.

Narrative
A tanker was approaching a Mediterranean port.On contacting the Port Authority at 0045, theship was assigned an anchorage. The mastercame to the bridge at 0115, and confirmed withthe second officer the assigned anchorage.Although the course to the anchorage wasdetermined, no plan was made to monitor theship’s approach to the anchorage position.
The arrival checklists were completed by 0130,and end of passage rung at 0136. The mastertook the con at 0140 from the second officer,who was the OOW. The master asked the secondofficer to put the anchor position on the radar.This was done using the latitude and longitudereadout of the radar cursor using the co-ordinatesof the centre of the anchorage circle from thechart. No allowance was included for thedistance of the radar scanner from the bow, norwas the datum shift, which was indicated on thechart, applied. The datum shift accounted for anerror of 140 metres to the north-east, and thebridge to bow distance added an additional 130metres, also to the north-east. This put the dropposition on the radar a total of 270 metres north-east of the required position, and nearer thecoast.
The engine was successfully tested astern at 0150with 1.7 miles to run to the anchorage. Themaster intended to put the engines astern when6 cables from the anchor position. Experiencetold him that this would bring the ship to a stopat the required point. The ‘go astern’ positionwould be 12 cables off the coast ahead of thevessel.
At approximately 0200, with the vessel 12 cablesfrom the shore, and where the master intended
to ring slow astern, he noted that the let goposition on the radar appeared to be too close tothe land. He asked the second officer to checkthe radar mark. This distraction delayed theastern movement until 0204. The master stillexpected to be able to stop the vessel in time, buthad failed to recognise that the astern movementwas applied 3 cables further on than intended.
At 0210, the second officer plotted another GPSfix on the chart, again failing to apply the datumshift, but this time incorrectly plotting theposition some 160 metres south-west of the givenco-ordinates. The position indicated that thevessel (bridge) was still 40 metres inside theanchorage circle on the chart. In fact, with thedatum shift applied, and the position correctlyplotted, the vessel was 240 metres outside thecircle, and already across the 20-metre depthcontour, putting the bow 90 metres from acharted 10.3 metre obstruction. The masteridentified the log speed at this time to be aboutzero, and using the 0210 position as a guide,considered that although the ship had overrunthe anchorage, they could continue astern toregain the required anchor position.
At 0212, the master, still misled by the 0210plotted position, noted that the vessel was stillnot gathering sternway, and increased to halfastern. At 0218, the position was again plottedwithout the datum shift, and at 0220 the enginewas stopped in the realisation that the vessel wasaground. No one onboard noticed any bump orlist as the ship had taken the ground.Throughout the approach to the anchorage theecho-sounder had not been monitored.
After discharging ballast from the forepeak, thevessel refloated some 5 hours later without theassistance of tugs.
31
Offset in the Mediterranean
MAIB Safety Digest 3/2004
CASE 15
32 MAIB Safety Digest 3/2004
CASE 15
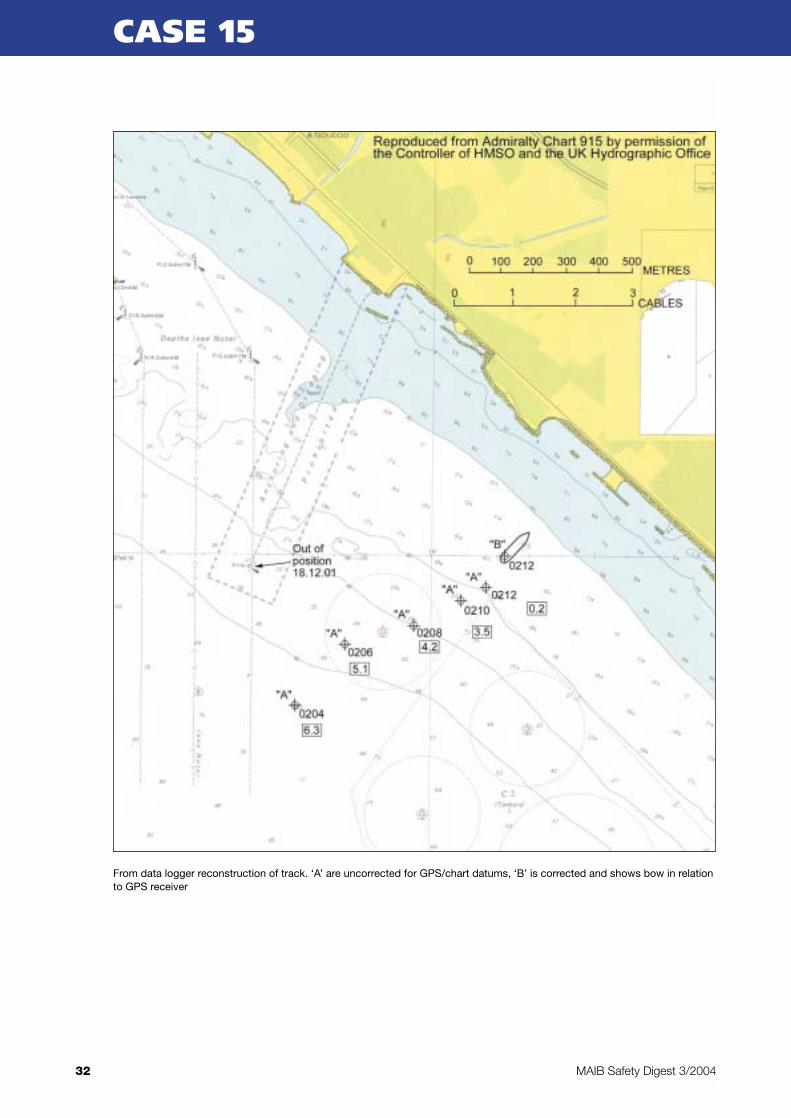
From data logger reconstruction of track. ‘A’ are uncorrected for GPS/chart datums, ‘B’ is corrected and shows bow in relationto GPS receiver
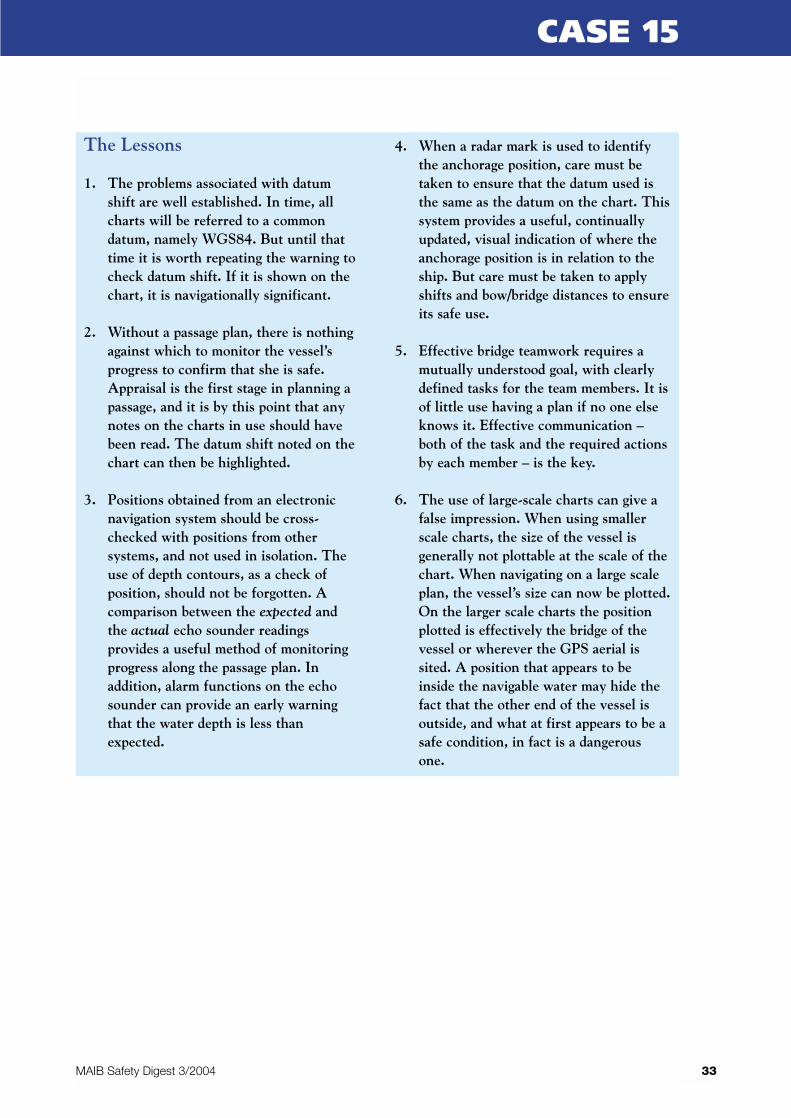
The Lessons
1. The problems associated with datumshift are well established. In time, allcharts will be referred to a commondatum, namely WGS84. But until thattime it is worth repeating the warning tocheck datum shift. If it is shown on thechart, it is navigationally significant.
2. Without a passage plan, there is nothingagainst which to monitor the vessel’sprogress to confirm that she is safe.Appraisal is the first stage in planning apassage, and it is by this point that anynotes on the charts in use should havebeen read. The datum shift noted on thechart can then be highlighted.
3. Positions obtained from an electronicnavigation system should be cross-checked with positions from othersystems, and not used in isolation. Theuse of depth contours, as a check ofposition, should not be forgotten. Acomparison between the expected andthe actual echo sounder readingsprovides a useful method of monitoringprogress along the passage plan. Inaddition, alarm functions on the echosounder can provide an early warningthat the water depth is less thanexpected.
4. When a radar mark is used to identifythe anchorage position, care must betaken to ensure that the datum used isthe same as the datum on the chart. Thissystem provides a useful, continuallyupdated, visual indication of where theanchorage position is in relation to theship. But care must be taken to applyshifts and bow/bridge distances to ensureits safe use.
5. Effective bridge teamwork requires amutually understood goal, with clearlydefined tasks for the team members. It isof little use having a plan if no one elseknows it. Effective communication –both of the task and the required actionsby each member – is the key.
6. The use of large-scale charts can give afalse impression. When using smallerscale charts, the size of the vessel isgenerally not plottable at the scale of thechart. When navigating on a large scaleplan, the vessel’s size can now be plotted.On the larger scale charts the positionplotted is effectively the bridge of thevessel or wherever the GPS aerial issited. A position that appears to beinside the navigable water may hide thefact that the other end of the vessel isoutside, and what at first appears to be asafe condition, in fact is a dangerousone.
33MAIB Safety Digest 3/2004
CASE 15

Never having had the misfortune of findingmyself overboard, I can only imagine the panicand terror that would ensue.
The wearing of lifejackets has long beenpromoted as the only safe means of protectingoneself. Indeed, there is some substance to thistheory and I would certainly endorse the wearingof buoyancy aids. But there are no absolutes.Having said that, may I offer the suggestion ofimproved working practices, so that you canavoid finding yourself in this position in the firstplace.
When all said and done, your vessel is yourprimary lifesaving appliance. And it is yourvessel which ultimately holds the key to yoursurvival.
We all know that accidents happen – they are afact of life, as demonstrated in many of thearticles in this edition of the Safety Digest. Yetthis should not deter us from attempting toreduce the risks by applying simple commonsense. A greater awareness of the dangers lurkingon board every vessel, combined with improvedworking practices, will significantly reduce therisk of accidents, including man overboard.
Some lifejackets can be cumbersome,uncomfortable and, occasionally, impractical towear. But the fact remains that by wearing oneyou will substantially increase your chances ofsurvival in an MOB situation. Perhaps a lifelineor a harness may be the preferred alternative ofsome fishermen.
Here are my suggestions to maximise your safety:
1. Ensure work areas are as free fromobstructions as possible, and remember:
“Tidy Ships Reduce Falls and Slips”
2. Let people ashore know your plans – whereyou are fishing and when you expect toreturn.
3. Compile a risk assessment of your vessel, andinclude the crew; they may have noticedsomething which you have not.
On a final note: safety is everyone’s concern,including your family and friends. They want youto come home safe too!
35
Part 2 – Fishing Vessels
MAIB Safety Digest 3/2004
Alan Piggott
Alan’s 36 years in the industry began as a fisherman sailing out of Grimsby. He then worked on theenforcement side, as a warranted British sea fisheries officer for the Scottish Office. After working in theShetland Islands as a Production Manager, Alan returned to his roots by becoming the Safety and TrainingOfficer of the National Federation of Fishermen’s Organisations.
Narrative
A small 6m open fishing boat was single linecreel fishing close inshore on the Scottish coast.The creels were recovered by hand as there wasno hauler onboard. The weather was good withonly a force 2 south-westerly wind. The skipper,who normally fished alone, put to sea every day,weather permitting, to check his creels andretrieve any catch. He had fished for many years,both on his own and with others, in small fishingboats. On the day of the accident he departedfrom the harbour and headed off to the furthestcreel so that he could work his way back towardshome. He never returned.
During the late afternoon, the skipper fell overthe side of his boat. The boat was washed up onto rocks, intact and with the throttle still ahead,although the engine had stopped. The skipper’s
body was retrieved 2 days later, close to wherethe boat was found.
The skipper was a non swimmer and was notwearing a lifejacket. He had believed that, onbalance, he was better off not wearing one, eventhough family members had tried to persuadehim otherwise. He even had prior experience of a‘near-miss’, where he was forced to jump out ofhis boat as it neared rocks without any enginepower. Luckily, that time, he landed in wateronly waist deep, and waded ashore.
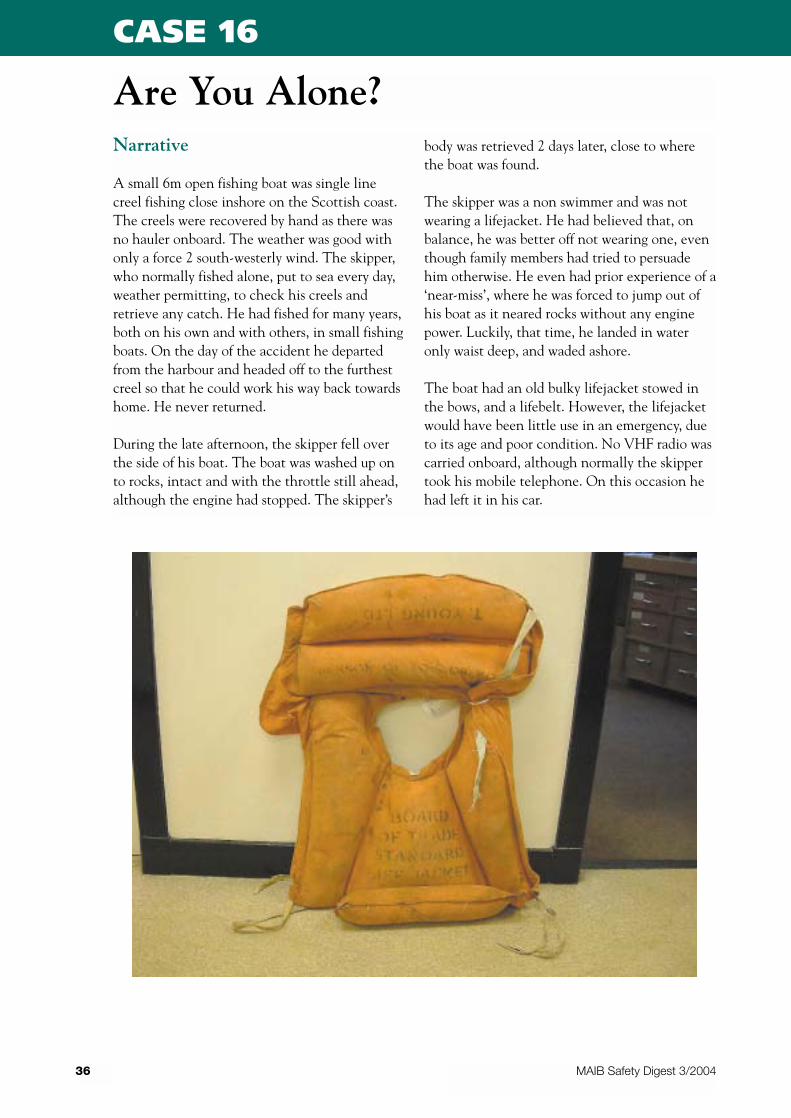
The boat had an old bulky lifejacket stowed inthe bows, and a lifebelt. However, the lifejacketwould have been little use in an emergency, dueto its age and poor condition. No VHF radio wascarried onboard, although normally the skippertook his mobile telephone. On this occasion hehad left it in his car.
36
Are You Alone?
MAIB Safety Digest 3/2004
CASE 16
37MAIB Safety Digest 3/2004
CASE 16
The Lessons
1. There is no need for single-handedfishing to be any more dangerous thanother types of fishing, so long as a properrisk assessment has been conducted andconsequential safety measures put inplace. Just because you have not yetsuffered an accident, is not grounds forcontinuing unsafe working practices.Planning for the unthinkable, andcarrying the appropriate equipment, willensure you have every chance ofreturning home to your loved ones afteryour fishing trips. Don’t becomecomplacent!
2. Wear a lifejacket! It could save your life.There are plenty of different typesavailable which will allow you to conducthauling and other fishing operations
without undue hindrance. Althoughwearing one is a personal choice,consider, also, the concerns of thosearound you.
3. There was a regulatory requirement tocarry a fixed or portable VHF radio onthe vessel involved in this tragedy. AVHF radio, in a waterproof pouch kepton your person, will dramaticallyimprove your chance of survival if youend up in the water. Carrying a mobiletelephone is not a satisfactoryalternative.
4. There is plenty of guidance andregulatory information freely availablefrom the MCA. Don’t wait to beinspected to find out. Take action nowand be safe!
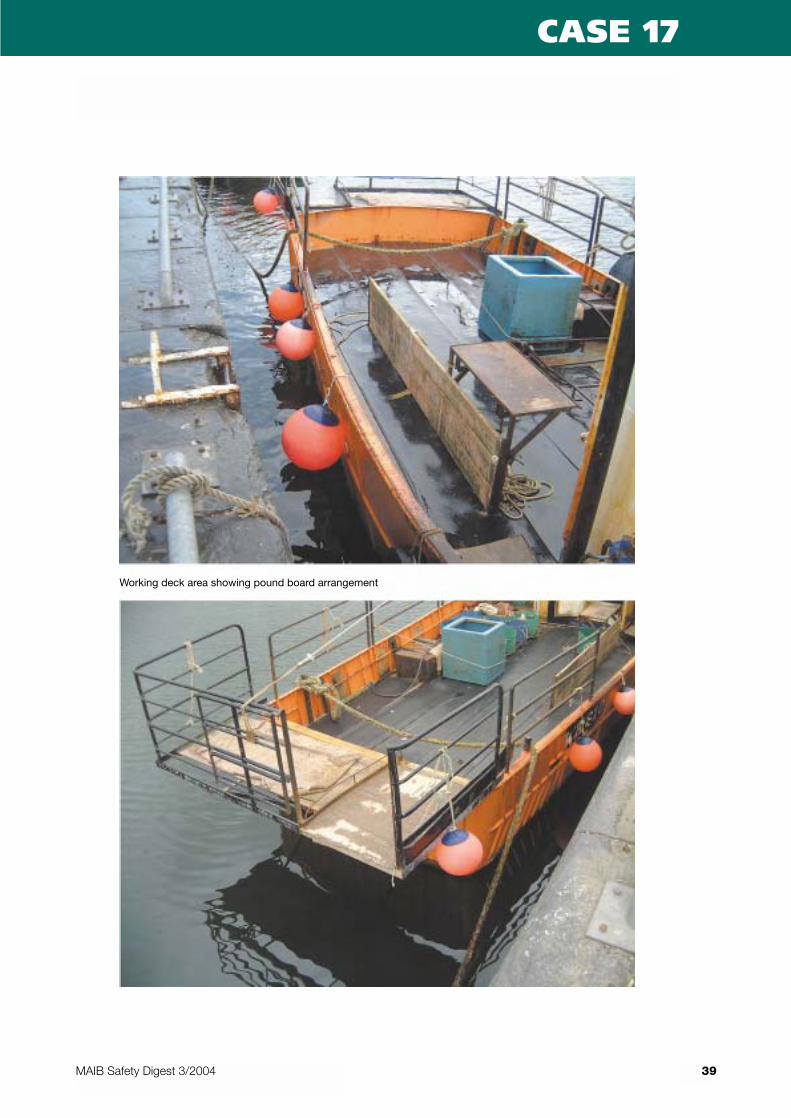
Narrative
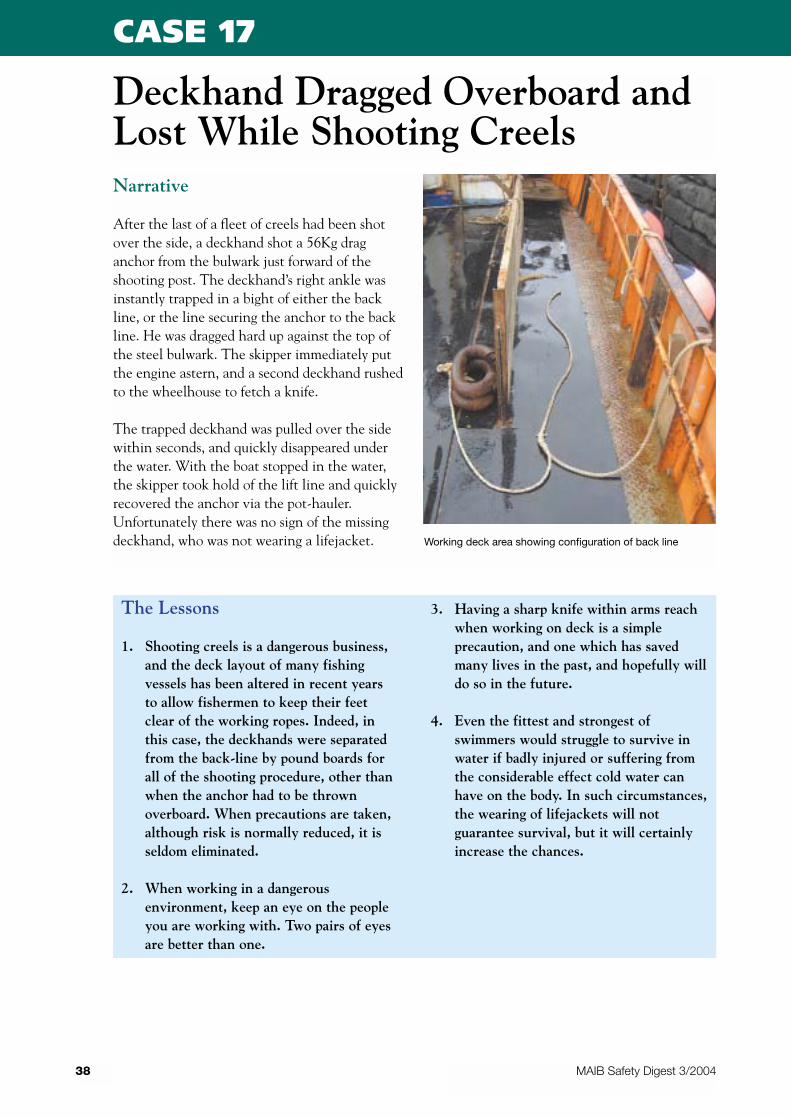
After the last of a fleet of creels had been shotover the side, a deckhand shot a 56Kg draganchor from the bulwark just forward of theshooting post. The deckhand’s right ankle wasinstantly trapped in a bight of either the backline, or the line securing the anchor to the backline. He was dragged hard up against the top ofthe steel bulwark. The skipper immediately putthe engine astern, and a second deckhand rushedto the wheelhouse to fetch a knife.
The trapped deckhand was pulled over the sidewithin seconds, and quickly disappeared underthe water. With the boat stopped in the water,the skipper took hold of the lift line and quicklyrecovered the anchor via the pot-hauler.Unfortunately there was no sign of the missingdeckhand, who was not wearing a lifejacket.
38
Deckhand Dragged Overboard andLost While Shooting Creels
MAIB Safety Digest 3/2004
CASE 17
The Lessons
1. Shooting creels is a dangerous business,and the deck layout of many fishingvessels has been altered in recent yearsto allow fishermen to keep their feetclear of the working ropes. Indeed, inthis case, the deckhands were separatedfrom the back-line by pound boards forall of the shooting procedure, other thanwhen the anchor had to be thrownoverboard. When precautions are taken,although risk is normally reduced, it isseldom eliminated.
2. When working in a dangerousenvironment, keep an eye on the peopleyou are working with. Two pairs of eyesare better than one.
3. Having a sharp knife within arms reachwhen working on deck is a simpleprecaution, and one which has savedmany lives in the past, and hopefully willdo so in the future.
4. Even the fittest and strongest ofswimmers would struggle to survive inwater if badly injured or suffering fromthe considerable effect cold water canhave on the body. In such circumstances,the wearing of lifejackets will notguarantee survival, but it will certainlyincrease the chances.
Working deck area showing configuration of back line
39MAIB Safety Digest 3/2004
CASE 17
Working deck area showing pound board arrangement

Narrative
While trawling, a vessel’s main engine suddenlystopped when her propeller was fouled by
discarded fishing gear from a beam trawler. Thevessel had to be towed back into port; fortunatelythere was no damage to the main engine orgearbox.
40
Own Goal
MAIB Safety Digest 3/2004
CASE 18
The Lessons
1. Throwing worn and unwanted fishinggear over the side might be the simplestway of solving a problem for one vessel,but apart from harming the marineenvironment, it can also cause seriousdamage to others.
2. Many fishermen already struggle to makea living, and can do without own goalslike this. Don’t be selfish, think of them,and dispose of all unwanted gear ashorein the appropriate manner.
Photograph of propeller fouled by discarded fishing gear

Narrative
A modern, steel, 24 metre fishing vessel wastowing in deep water with the skipper on watchin the wheelhouse. The high-level bilge alarmsounded. Before going to the engine room toinvestigate, the skipper woke one of the otherfour crewmen and told him to go to thewheelhouse to keep an eye on things.
By the time the skipper reached the engineroom, floodwater was covering the floor platesand was well up towards the top of the mainengine. All handwheels for closing the sea inletvalves were already considerably below waterlevel and inaccessible. However, he noticed astream of bubbles in the water over one of themain sea inlet strum boxes. This suggested thatthe cover of the strum box had failed or beendisplaced.
He returned to the accommodation, alerted theremainder of the crew and told them to assemblein the wheelhouse.
Back in the engine room, the skipper found thewater level over the main engine, which then
stopped. However, an auxiliary engine, beinghigher than the main engine, remained runningand maintained the 240-volt system.
Recognising the difficulty of the situation, a“Mayday” was broadcast. This was picked up byanother fishing vessel only a few miles away,which offered to assist. At this stage the 240voltsystem failed, suggesting floodwater had reachedthe level of the auxiliary engine.
All five men donned lifejackets, and a liferaftwas thrown overboard and inflated. One manalso put on his survival suit. The others also hadsurvival suits, but did not put them on.
By this stage the vessel was listing to 25o to 30o
and it was decided that all five men should boardthe liferaft.
Once the liferaft was clear of the vessel, thesurvivors were able to watch her sink by thestern. A short while later they were picked up bythe fishing vessel that had earlier responded totheir “Mayday”. All five men were later landedsafely, with few ill effects other than somediscomfort due to the cold.
41
Another Unchecked Flooding
MAIB Safety Digest 3/2004
CASE 19
The Lessons
1. High-level bilge alarms are vital pieces ofequipment for alerting crews topotentially serious problems. However,unless other important systems aredesigned so that worthwhile remedialaction can be taken, the value of bilgealarms is diminished. In this case, anability or system to allow sea inlet valvesto be closed from a high position, such asby having extended spindles reachingwell above floor plate level, could havetaken advantage of the warning given bythe alarm and stopped the ingress ofwater.
2. Although survival suits were readilyavailable to all five men, only one choseto wear his. All were sufficientlydisciplined to wear their lifejackets, butit would have been prudent for them tohave linked the need to put on alifejacket with the need also to put on asurvival suit.
Narrative
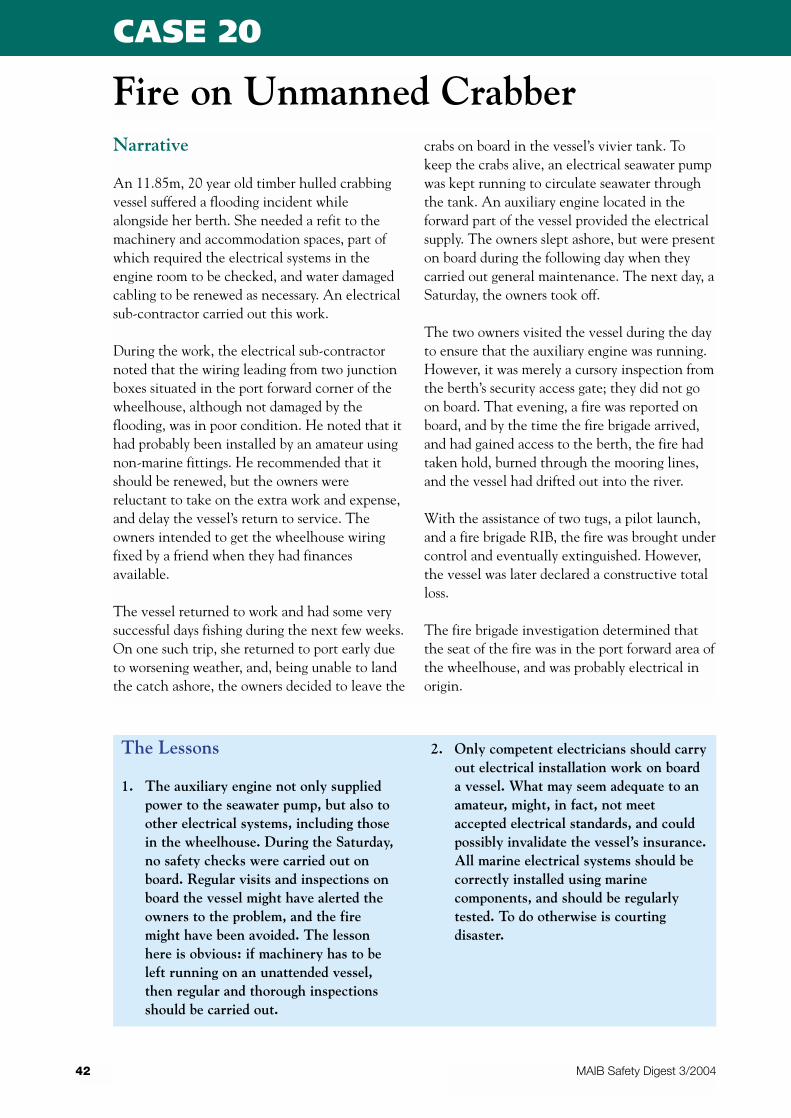
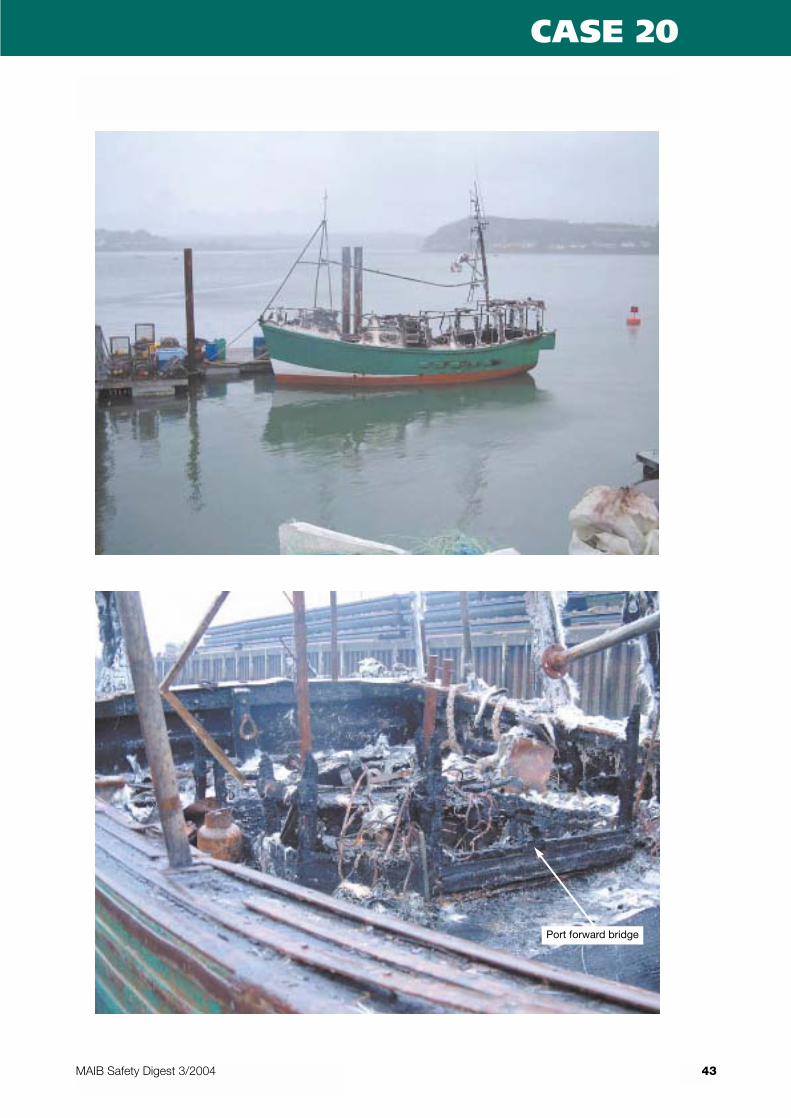
An 11.85m, 20 year old timber hulled crabbingvessel suffered a flooding incident whilealongside her berth. She needed a refit to themachinery and accommodation spaces, part ofwhich required the electrical systems in theengine room to be checked, and water damagedcabling to be renewed as necessary. An electricalsub-contractor carried out this work.
During the work, the electrical sub-contractornoted that the wiring leading from two junctionboxes situated in the port forward corner of thewheelhouse, although not damaged by theflooding, was in poor condition. He noted that ithad probably been installed by an amateur usingnon-marine fittings. He recommended that itshould be renewed, but the owners werereluctant to take on the extra work and expense,and delay the vessel’s return to service. Theowners intended to get the wheelhouse wiringfixed by a friend when they had financesavailable.
The vessel returned to work and had some verysuccessful days fishing during the next few weeks.On one such trip, she returned to port early dueto worsening weather, and, being unable to landthe catch ashore, the owners decided to leave the
crabs on board in the vessel’s vivier tank. Tokeep the crabs alive, an electrical seawater pumpwas kept running to circulate seawater throughthe tank. An auxiliary engine located in theforward part of the vessel provided the electricalsupply. The owners slept ashore, but were presenton board during the following day when theycarried out general maintenance. The next day, aSaturday, the owners took off.
The two owners visited the vessel during the dayto ensure that the auxiliary engine was running.However, it was merely a cursory inspection fromthe berth’s security access gate; they did not goon board. That evening, a fire was reported onboard, and by the time the fire brigade arrived,and had gained access to the berth, the fire hadtaken hold, burned through the mooring lines,and the vessel had drifted out into the river.
With the assistance of two tugs, a pilot launch,and a fire brigade RIB, the fire was brought undercontrol and eventually extinguished. However,the vessel was later declared a constructive totalloss.
The fire brigade investigation determined thatthe seat of the fire was in the port forward area ofthe wheelhouse, and was probably electrical inorigin.
42
Fire on Unmanned Crabber
MAIB Safety Digest 3/2004
CASE 20
The Lessons
1. The auxiliary engine not only suppliedpower to the seawater pump, but also toother electrical systems, including thosein the wheelhouse. During the Saturday,no safety checks were carried out onboard. Regular visits and inspections onboard the vessel might have alerted theowners to the problem, and the firemight have been avoided. The lessonhere is obvious: if machinery has to beleft running on an unattended vessel,then regular and thorough inspectionsshould be carried out.
2. Only competent electricians should carryout electrical installation work on boarda vessel. What may seem adequate to anamateur, might, in fact, not meetaccepted electrical standards, and couldpossibly invalidate the vessel’s insurance.All marine electrical systems should becorrectly installed using marinecomponents, and should be regularlytested. To do otherwise is courtingdisaster.
43MAIB Safety Digest 3/2004
CASE 20
Port forward bridge

Narrative
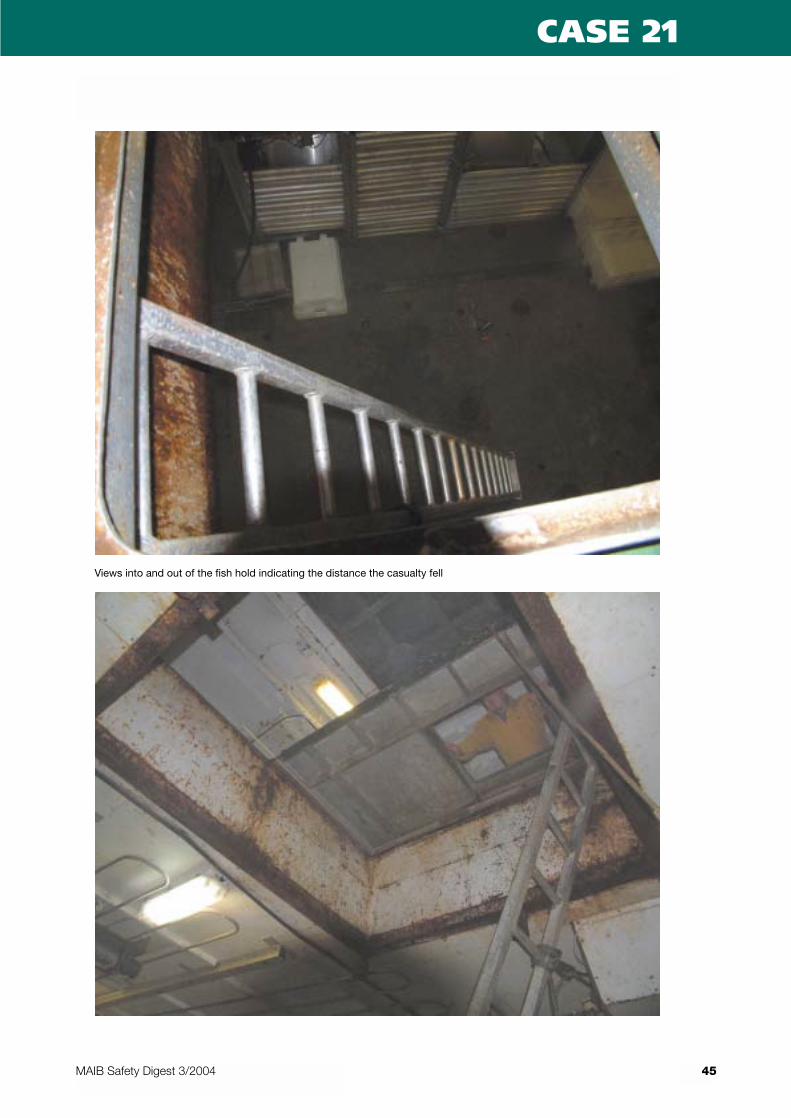
A 34m vessel was trawling when one of her crewfell down into the fish room through the openhatch from the deck above.
At the time of the accident, the casualty was ondeck in the fish preparation area, helpinganother crew member. They were transferringempty bins, which were stowed on the deckforward, down into the fish room. Two othercrew members were in the fish room ready toreceive them.
The additional bins were required below to storethe catch. Normally, sufficient empty bins werekept in the fish room, but on this occasion, manywere being used to store ice. Whenever extrabins were required, it was usual practice tomanhandle them from their stowed positionforward, and lower them down into the fish roomusing a line and pulley attached to the deckheadabove the hatch opening.
At the time of the accident, the casualty waspulling on one of the bins which had becomelodged behind a fixed pound board. He was
standing next to the open hatch when he lost hisgrip on the bin and fell down the open hatch. Hewas not wearing a hard hat. The height from thedeck to the fish room floor was 4.15m. Thedeckhands in the fish room saw him fall, butwere unable to do anything. He sustained seriousinjuries to his head and shoulder.
A short time later, he was airlifted off by ahelicopter and rushed to hospital. He is expectedto make a full recovery following a lengthyperiod in hospital.
A risk assessment had been conducted andrecords were kept on board. However, it hadbeen done by a shore-based consultant who hadnever been to sea on the vessel. Consequently,an assessment of the risks for this operation wasnever carried out.
The risk assessment did identify the hazardpresented by unprotected openings. Thesuggested control measures were: to exerciseextra caution, to have open hatches guarded andto display warnings. However, the risk wasconsidered low and the control measures werenot implemented.
44
Down the Fish Room
MAIB Safety Digest 3/2004
CASE 21
45MAIB Safety Digest 3/2004
CASE 21
Views into and out of the fish hold indicating the distance the casualty fell
46 MAIB Safety Digest 3/2004
CASE 21
The Lessons
1. Whenever working close to openhatches, always ensure safety measuresare in place, such as portable guard rails.If that is not possible, use a safetyharness attached to a point which willprevent a person working close to anopen hatch from falling down. It’s also agood idea to wear a hard hat with achinstrap, just in case.
2. Contrary to popular belief, theassessment of risk is not a complicated
exercise. It requires all concerned in anyoperation to stand back, for a fewminutes only, and consider the risksassociated with that particular operation.If hazards are identified, often, simplecontrol measures can be put in place toprevent accidents from happening.
3. The best people to carry out riskassessments are the skipper and his crew.It is they who know their vessel betterthan anyone else, and it is they,therefore, who are able to more readilyidentify risks.
Bin being lifted into fish hold
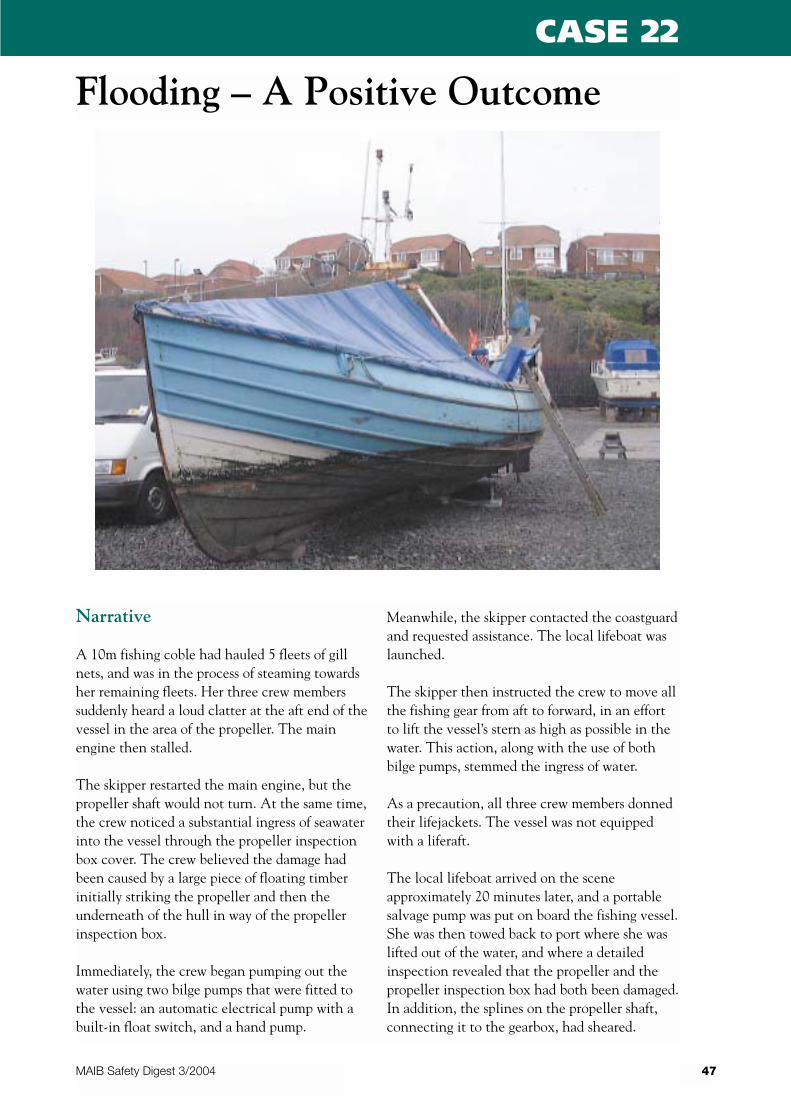
Narrative
A 10m fishing coble had hauled 5 fleets of gillnets, and was in the process of steaming towardsher remaining fleets. Her three crew memberssuddenly heard a loud clatter at the aft end of thevessel in the area of the propeller. The mainengine then stalled.
The skipper restarted the main engine, but thepropeller shaft would not turn. At the same time,the crew noticed a substantial ingress of seawaterinto the vessel through the propeller inspectionbox cover. The crew believed the damage hadbeen caused by a large piece of floating timberinitially striking the propeller and then theunderneath of the hull in way of the propellerinspection box.
Immediately, the crew began pumping out thewater using two bilge pumps that were fitted tothe vessel: an automatic electrical pump with abuilt-in float switch, and a hand pump.
Meanwhile, the skipper contacted the coastguardand requested assistance. The local lifeboat waslaunched.
The skipper then instructed the crew to move allthe fishing gear from aft to forward, in an effortto lift the vessel’s stern as high as possible in thewater. This action, along with the use of bothbilge pumps, stemmed the ingress of water.
As a precaution, all three crew members donnedtheir lifejackets. The vessel was not equippedwith a liferaft.
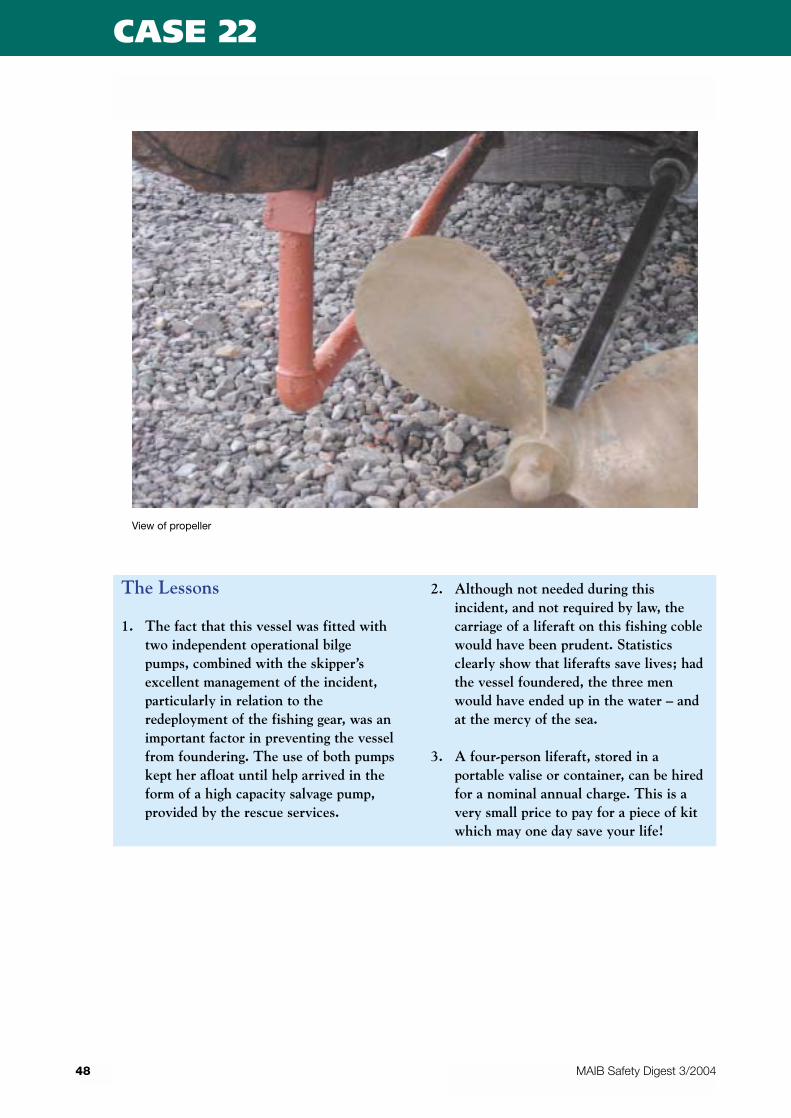
The local lifeboat arrived on the sceneapproximately 20 minutes later, and a portablesalvage pump was put on board the fishing vessel.She was then towed back to port where she waslifted out of the water, and where a detailedinspection revealed that the propeller and thepropeller inspection box had both been damaged.In addition, the splines on the propeller shaft,connecting it to the gearbox, had sheared.
47
Flooding – A Positive Outcome
MAIB Safety Digest 3/2004
CASE 22
48 MAIB Safety Digest 3/2004
CASE 22
The Lessons
1. The fact that this vessel was fitted withtwo independent operational bilgepumps, combined with the skipper’sexcellent management of the incident,particularly in relation to theredeployment of the fishing gear, was animportant factor in preventing the vesselfrom foundering. The use of both pumpskept her afloat until help arrived in theform of a high capacity salvage pump,provided by the rescue services.
2. Although not needed during thisincident, and not required by law, thecarriage of a liferaft on this fishing coblewould have been prudent. Statisticsclearly show that liferafts save lives; hadthe vessel foundered, the three menwould have ended up in the water – andat the mercy of the sea.
3. A four-person liferaft, stored in aportable valise or container, can be hiredfor a nominal annual charge. This is avery small price to pay for a piece of kitwhich may one day save your life!
View of propeller

Narrative
A 13.6m steel construction beam trawler wasfishing off the south coast when her skippernoticed back smoke coming from the engineroom ventilators. As he “cracked” open theengine room hatch, he was confronted by denseblack acrid smoke. He closed the hatchimmediately and alerted the crew.
Conscious of the need to isolate the oxygensupply, and potential fuel supply to the fire, heblocked the engine room ventilators, and shutdown the engine room fans, main engine andgenerator. The skipper re-assessed the situationand considered it safe to “crack” the engine roomhatch and discharge two CO2 extinguishersdown the hatchway. This had little effect. Hethen dogged the hatch closed and alerted hisshore manager and the coastguard.
The coastguard helicopter arrived within 5minutes and, using the on board infrared (IR)equipment, was able to identify to the skipperthat the seat of the fire was in the starboard aftercorner of the engine room. The only equipmentin this area was a plastic cased portable high-pressure washer, stowed adjacent the starboardfuel tank.
The lifeboat arrived shortly after and transferreda fire pump, which the trawler and lifeboat crewused to boundary cool the deck area above thefire. After about 10 minutes, the helicopterreported that the heat source was reducing. Thedeck water had also stopped steaming. Theengine room hatch was again “cracked open” andthe fire hose directed at the seat of the fire.
When the fire appeared to be extinguished, theskipper cautiously entered the engine room,wearing a lifeline and accompanied by a memberof the crew, and dampened down the area.Following a damage assessment, the generatorand fans were re-started and the remainingsmoke cleared.
After further checks, the main engine wasstarted, fishing gear recovered and, under herown power, the trawler returned to her homeport.
The trawler engine room suffered significantsmoke staining, some electrical fittings in thevicinity of the fire were badly damaged and therewas a large area of damaged paintwork. The highpressure water washer was completely destroyed.
49
Fire-Fighting Training Saves theDay
MAIB Safety Digest 3/2004
CASE 23
50 MAIB Safety Digest 3/2004
CASE 23
The Lessons
1. Having recently attended a fire-fightingcourse, the skipper was able to effectivelyand calmly assess the risks and tackle thefire confidently during this potentiallycatastrophic incident. He fullyappreciated the need to isolate the air andadditional fuel supply from the fire.
2. Although the trawler was not fitted withdedicated ventilator closures, the skipperused his initiative in utilising materials tofurther isolate the air supply. He alsorecognised the need to boundary cool thedeck in the vicinity of the fire to reducethe heat required to sustain the fire. Thebenefits of being properly trained in fire-fighting techniques clearly influenced themanner in which the skipper dealt withthe fire.
3. The co-ordination of the helicopter IRfacilities, lifeboat, and trawler crewresources was first class, and undoubtedlyprevented the fire from spreading, withthe possible loss of the vessel.
4. Extreme caution must be exercised whenaccessing a compartment where a fire hasoccurred, or the condition of thecompartment is unknown, in case thesudden air supply causes re-ignition. Inaddition, where it is suspected thatcombustion-related toxic fumes mightexist, the compartment should beaccessed wearing breathing apparatus –even after it has been ventilated.
5. Portable electrical appliances should befully isolated when not in use, unlessdirected otherwise in the manufacturer’sinstructions.
All of us who take small craft to sea, whether forrecreation or commercially, are relieved not toappear as a ‘case study’ in this publication.
We all make errors of judgment and occasionallythe boat’s equipment lets us down. Fortunately insmall craft the result is usually embarrassmentand, if unlucky, a trip to the chandlers, howeverwhere the outcome is more serious it isinvaluable for us to study the reasons.
The RYA regularly uses these reports as a basisfor discussion at its many conferences forcommercial and amateur yachtsmen. Many ofthe lessons apply equally to sail and powerskippers, both inshore and offshore.
Occasionally, the RYA syllabus is revised as aresult of an MAIB investigation. Following thepublication of the report of the inversion of theyacht Ocean Madam in the Bay of Biscay, a basicknowledge of stability was introduced into theYachtmaster shorebased syllabus.
The smallest of mishaps can sometimes trigger asequence of events that can lead to the tragicoutcomes seen in the following pages. Goodseamanship is about knowing what to do in avariety of circumstances. Equally important isknowing what not to do. Good training andthese pages provide an insight into both options.
51
Part 3 – Leisure Craft
MAIB Safety Digest 3/2004
Jon MendezRYA Chief Power/Motor Boat Instructor
Jon’s keen interest in boats started at a young age with friends and family, motor cruising on the RiverThames. He has run a successful business and has spent time employed as a freelance instructor on the southcoast. Between 1990 and 1992, Jon worked full-time for Sealine Sea School on the River Hamble. He is nowChief Power and Motorboat Instructor for the RYA, where he is responsible for the training course contentand instructor training for motor cruising, powerboating, inland cruising and personal watercraft. He is aYachtmaster instructor and examiner, and is also a powerboat trainer.
Narrative
On a bright, warm, summer day, four members ofone family and a family friend launched arecently bought, second hand, 15' speedboat in asea loch for an angling trip. The owner of theboat, who had brought his father and two sonsalong, had minimal boat handling experience, sohad requested the friend to accompany them andprovide advice.
The safety equipment on board was limited to aspare outboard engine, three lifejackets and threeflares. The owner also had a buoyancy jacket andhe carried a mobile telephone. The othersonboard wore mostly lightweight clothing.
After launching in the morning from the westernshore of the loch, they motored out to theentrance, searching for fish with a finder. Afterfishing to the west of the loch entrance in themorning, they crossed to the eastern shore in theafternoon and began drift angling.
By late afternoon, the weather conditions hadbegun to deteriorate. They had a good catch offish and, as one of the sons had begun to feelseasick, they decided to make their way back.
The family friend was at the helm. As theyheaded into the choppy sea they saw a ferryleaving the ferry terminal within the loch. Awareof the problems associated with wash waves fromthe high-speed and conventional ferries that
operated through the loch, they held back untilthe ferry had passed. They rode the wash and,probably, took some water over the bow.
They speeded up and continued to cross theloch, but a little time later, when nearly midwayacross, they were swamped by several waves thatcame over the starboard quarter. Although thebilge pump was started, and two of those onboard attempted to bail out the water using fishboxes, the boat was unable to withstand theadditional weight of the water and it sank rapidlyby the stern. As it sank, the father hurriedly putlifejackets on his sons and attempted,unsuccessfully, to make a telephone call.
The boys’ ill-fitting lifejackets inflated, and theyand their father began to drift away from thegrandfather and friend, under the influence ofthe wind. The bow of the boat then bobbed up,and the grandfather and friend were able to tiethemselves to it with a rope.
Although a number of ferries and other craftpassed quite close to them, it wasn’t until nearly4 hours later that the grandfather and friendwere seen by a passing yacht. The watertemperature was 10°C.
An extensive search for the father and sonsbegan immediately, and about an hour later, thebodies of the father and one son were found,along with the two lifejackets. The other son’sbody was not found until nearly 6 weeks later.
52
Three Family Members Lost onAngling Trip
MAIB Safety Digest 3/2004
CASE 24
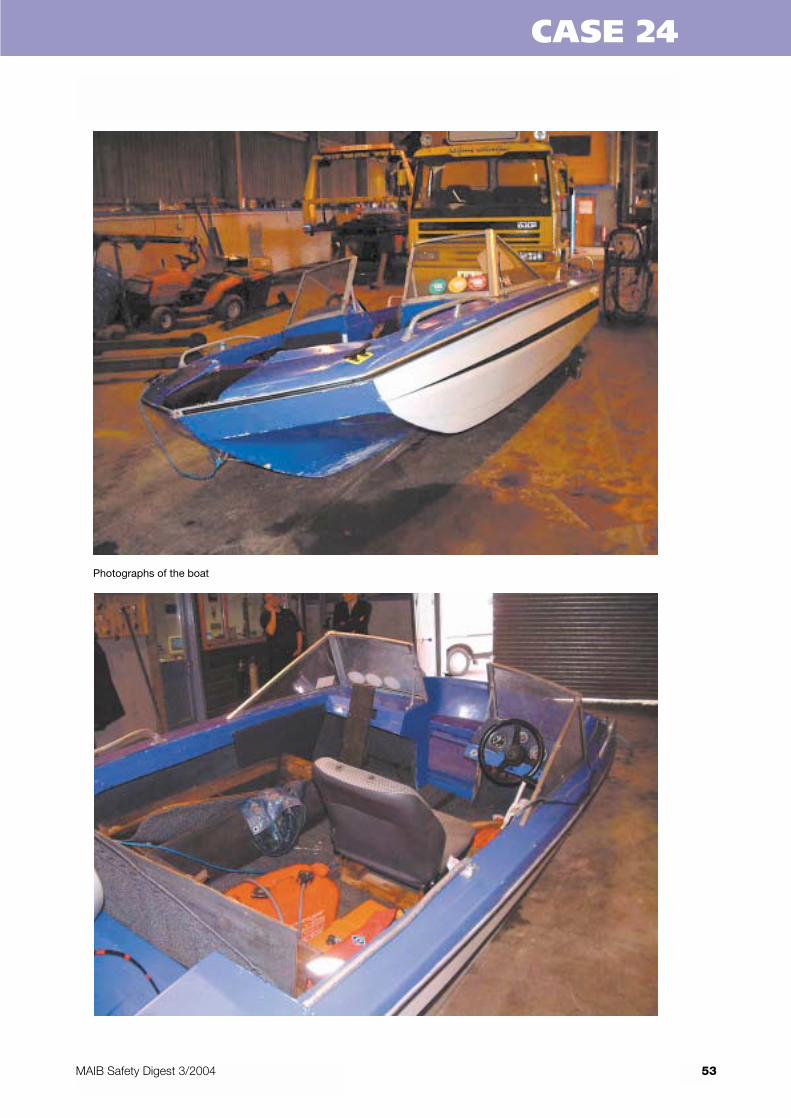
53MAIB Safety Digest 3/2004
CASE 24
Photographs of the boat
54 MAIB Safety Digest 3/2004
CASE 24
The Lessons
1. The boat, which was nearly 30 years old,had had multiple owners and had beenmodified and poorly repaired such that itno longer met the original design criteria.Many boats like this are for sale on thesecond-hand market, and their conditionis not regulated. A boat caninadvertently become a death trap whenmodifications are carried out inexpertly.Before buying a second-hand boat makesure you know:
• the boat’s history• that it is suitable for the intended
purpose, and• that any repairs or modifications have
been carried out by a competentperson.
If you are unsure about any of the above,DON’T buy it – no matter how much ofa bargain it might appear to be.
2. In this case, the new owner took theboat out fully loaded into what was,effectively, open sea conditions on itsfirst trip. It would have been prudent tohave experimented with it first, in acontrolled and sheltered environment, toestablish its capabilities. Sensiblepreparation, particularly on a previouslyuntried boat, will pay dividends if anunexpected event occurs during the trip.
3. The group did not take adequatelifesaving equipment on the trip, andwhat they had was not used to goodadvantage. Lifejackets should have beenavailable for each of the crew – and theyshould have been worn. Accidents occureven in benign conditions, and it is oftentoo late to don lifejackets properly afterthe event. Plentiful advice is availablefrom various sea safety organisations.The RNLI provides a free safetyequipment advice service (SEACheck),and will come to you. All you have to dois call them (0800 328 0600).
4. A mobile telephone has receptionlimitations, especially when usedoffshore, and there can be crucial delaysin connecting to the coastguard. Amarine VHF radio allows for directcommunication in an emergency, and isthe recommended communicationmethod. Be prepared, use the propercommunications equipment, and makesure that you can contact the emergencyservices and other vessels if needed.
5. Although the weather conditions at thetime of launching were benign, the seatemperature was cold. The twosurvivors, who were wearing lightweightclothing, said later that their extremitieshad numbed soon after immersion. Thedangers of cold-water immersion, such ascold water shock, are commonlymisunderstood. Although survival timesdepend on different criteria, and can varyconsiderably, research indicates that only50% of fully clothed men can beexpected to survive more than 2 hours ina water temperature of 10C. Warmclothing and buoyancy aids help toprolong the survival times.
6. Operating a small craft near mainshipping routes should only beundertaken with caution. Wash waves,that are hazardous to small craft, can beproduced by large vessels, particularlyhigh-speed craft. These wash waves canbe particularly dangerous in shallowwater or on the shoreline. Wash wavescan also be a problem in deeper water ifthey approach a vulnerable craft fromastern. Be alert to the problem and takeappropriate action.
7. If you do not know the sea area in whichyou intend to use your boat, take advicefrom the local RNLI, harbourmaster orboating club. And/or gain experience ofthe area with qualified boat usersthrough boating clubs or other similarorganisations.
Narrative
A sailing club arranged a two day Open RaceMeeting, which was held over a summerweekend, and which involved some 80 RS Classracing dinghies. The open water was accessed viaa busy river channel that was also used byfishermen, other pleasure craft and was subject tofrequent car/passenger ferry sailings. The sailingclub advised the ferry company of the roughareas of intended racing about a month beforethe event, but did not identify the “box”co-ordinates.
Two courses were set up to the east and west ofthe river channel entrance. During the first day’sracing, the sailing club carefully moved theracing marks, having taken due note of thecourses the ferries were taking. One ferry,however, passed close to one of the marks andhad cause to raise concern about the position ofthe mark with the race officers in the safety boat.This concern was also raised with the sailing clubthe following day.
On the second day of racing, during the floodtide, the marks were reset with the agreement ofone of the ferry masters, although there were norecords of these co-ordinates. Later that day, onan ebb tide and in good visibility, a ferry wasmaking her regular crossing when sheinexplicably passed inside one of the racingmarks, having taken a slightly more westerlycourse than normal.
At about the same time, a dinghy rounded themark, and in doing so became dismasted. Theferry master appeared to be concentrating onavoiding the racing marks that he believed wereon his course, when he suddenly became aware ofa large number of dinghies on a course crossingahead. Astern power was applied and three shortblasts sounded. The ferry was quickly surroundedby the fast racing yachts; they had to takeavoiding action to prevent colliding with her.
Fortunately there were no casualties.
55
Leisure Craft and CommercialVessels – a Conflict of Interests?
MAIB Safety Digest 3/2004
CASE 25
The Lessons
1. Regular meetings between water spaceusers (ferry companies, sailing clubs,harbour commissioners etc) will help allparties to appreciate individual needs andhelp resolve conflicting interests.
2. During occasions when there are largesailing races, careful considerationshould be given to posting lookouts onpassing vessels.
3. When proposed racing area informationis passed to interested parties, it isextremely helpful to include the “box”co-ordinates so that concerns can beraised, especially where these are in closeproximity to regular ferry routes.
4. Whenever possible, racing marks shouldbe positioned well clear of regular ferryroutes, and sometimes it may beappropriate to agree a temporary “no gozone” for both ferries and yachts duringlarge regattas.
5. Inviting ferry masters to participate indinghy racing, and yachtsmen onto thebridge of ferries during a busy yachtrace, enables both parties to appreciateeach other’s concerns and to see the“landscape” from a different perspective.

Narrative
An amateur fisherman and his teenageneighbour set out on a pre-dawn mid winterfishing trip in a recently acquired and repaired,5 metre long, relatively old speedboat. Theylaunched in a relatively sheltered area, but hadintended to move out to a more exposed positionon the coast to fish. They wore warm clothing,waders and old solid buoyancy aids. They alsocarried a spare outboard engine and a torch.
When the two men set out, within the shelteredarea a 25 knot wind was blowing, gusting to 35knots, there was a significant wave height of0.8m and the sea was between 6 and 8°C. Thetide was on the ebb.
About 40 minutes after launching the boat, a999 call was made from the fisherman’s mobiletelephone. The caller requested the telephoneoperator to put him through to the coastguard.He provided no information to the operator onhis location.
The call was quickly transferred to the localcoastguard station, but the station officers couldhear only the noise of the wind and sea during
the brief remaining time of the call. Theyattempted to return the call, but without success.Without any further information available, andbearing in mind hoax and accidental calls arenot uncommon, no further action was taken.
Later that day, the family of the fisherman raisedthe alarm that he had not returned at theexpected time. A large-scale search and rescueoperation began immediately, involving manysearch and rescue units over a considerable area.Only scant information was available on theprobable destination of the fishing trip, and thelength of time involved between the two menlaunching the speedboat and the time of thealarm being raised, meant that the area to becovered by the search units was extensive.Despite the efforts of the rescue services, thesearch was unsuccessful, and the two men werenot found.
A day and a half later, a buoyancy aid was foundwashed ashore, which was identified by thefamily of the fisherman. About 10 days later, thebody of the teenager was washed ashore, stillwearing his buoyancy aid and chest-high waders.
The fisherman and his boat are still missing.
56
Fishing for Disaster
MAIB Safety Digest 3/2004
CASE 26

57MAIB Safety Digest 3/2004
CASE 26
The Lessons
1. The fisherman and his friend wereinexperienced in boat operations. Theboat’s history was unknown; what isknown, however, is that repairs had beencarried out to its hull and engine.Without any trials having been carriedout in a safe environment, it waslaunched in darkness, in mid winter andin poor weather conditions. Also, theboat did not carry the requirednavigation lights. The decision to launchit was, at the very least, unwise.
2. Survival equipment consisted of warmclothing, old solid buoyancy aids and atorch. Additionally, a spare engine wascarried on board. The waders that wereworn, probably to protect the fishermenfrom the cold and sea spray, would havecounteracted any useful buoyancyafforded by the old buoyancy aids. Theboat was not properly equipped for theplanned activity.
3. A relative had been told when the twofishermen were expected home, about 10hours after their launching time. Thisalerted the coastguard to their plight andis good practice. It would have beenbetter, however, if the skipper had agreedto call in every hour throughout the day.
4. The mobile telephone was the onlymethod of communication available tothe pair. This was inadequate and is not
advised for maritime use because itcauses genuine difficulties for theemergency services. A VHF radio cantransmit emergency calls via channel 16(the emergency channel) directly to thecoastguard, and a quick response can beassured. Other methods of raising thealarm include personal locator beacons,which are readily available and arebecoming increasingly cheaper.
5. The RNLI provides a free, friendly andconfidential sea safety advice(SEACheck) service, which is availablecountrywide through a system of co-ordinators and volunteers. This servicecan provide guidance on effectivelifesaving apparatus (LSA), and otherequipment that would prove useful indifferent sea conditions, as well asdistress and emergency procedures.Other free guidance for leisure craftusers is available from the Maritime andCoastguard Agency (MCA).
6. It’s not always easy to cancel a plannedand eagerly awaited fishing trip at thelast moment, but commonsense and goodseamanship must prevail. The decision tolaunch should be based on such things asthe weather, sea conditions, experienceof the crew, state of the boat andadequacy of the equipment. Whendifficult decisions need to be taken,never ever forget that the power anddanger of the sea should be respected atall times.
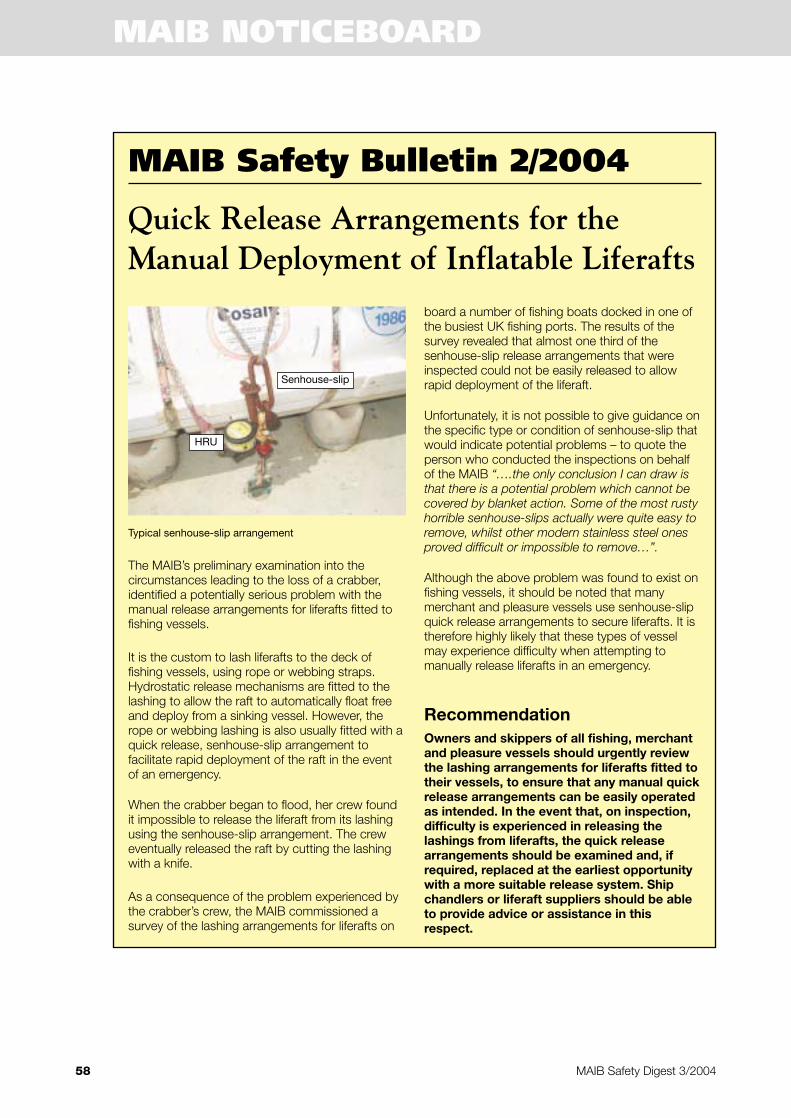
The MAIB’s preliminary examination into thecircumstances leading to the loss of a crabber,identified a potentially serious problem with themanual release arrangements for liferafts fitted tofishing vessels.
It is the custom to lash liferafts to the deck offishing vessels, using rope or webbing straps.Hydrostatic release mechanisms are fitted to thelashing to allow the raft to automatically float freeand deploy from a sinking vessel. However, therope or webbing lashing is also usually fitted with aquick release, senhouse-slip arrangement tofacilitate rapid deployment of the raft in the eventof an emergency.
When the crabber began to flood, her crew foundit impossible to release the liferaft from its lashingusing the senhouse-slip arrangement. The creweventually released the raft by cutting the lashingwith a knife.
As a consequence of the problem experienced bythe crabber’s crew, the MAIB commissioned asurvey of the lashing arrangements for liferafts on
board a number of fishing boats docked in one ofthe busiest UK fishing ports. The results of thesurvey revealed that almost one third of thesenhouse-slip release arrangements that wereinspected could not be easily released to allowrapid deployment of the liferaft.
Unfortunately, it is not possible to give guidance onthe specific type or condition of senhouse-slip thatwould indicate potential problems – to quote theperson who conducted the inspections on behalfof the MAIB “….the only conclusion I can draw isthat there is a potential problem which cannot becovered by blanket action. Some of the most rustyhorrible senhouse-slips actually were quite easy toremove, whilst other modern stainless steel onesproved difficult or impossible to remove…”.
Although the above problem was found to exist onfishing vessels, it should be noted that manymerchant and pleasure vessels use senhouse-slipquick release arrangements to secure liferafts. It istherefore highly likely that these types of vesselmay experience difficulty when attempting tomanually release liferafts in an emergency.
RecommendationOwners and skippers of all fishing, merchantand pleasure vessels should urgently reviewthe lashing arrangements for liferafts fitted totheir vessels, to ensure that any manual quickrelease arrangements can be easily operatedas intended. In the event that, on inspection,difficulty is experienced in releasing thelashings from liferafts, the quick releasearrangements should be examined and, ifrequired, replaced at the earliest opportunitywith a more suitable release system. Shipchandlers or liferaft suppliers should be ableto provide advice or assistance in thisrespect.
58
MAIB Safety Bulletin 2/2004
MAIB Safety Digest 3/2004
Quick Release Arrangements for theManual Deployment of Inflatable Liferafts
Typical senhouse-slip arrangement
Senhouse-slip
HRU
MAIB NOTICEBOARD
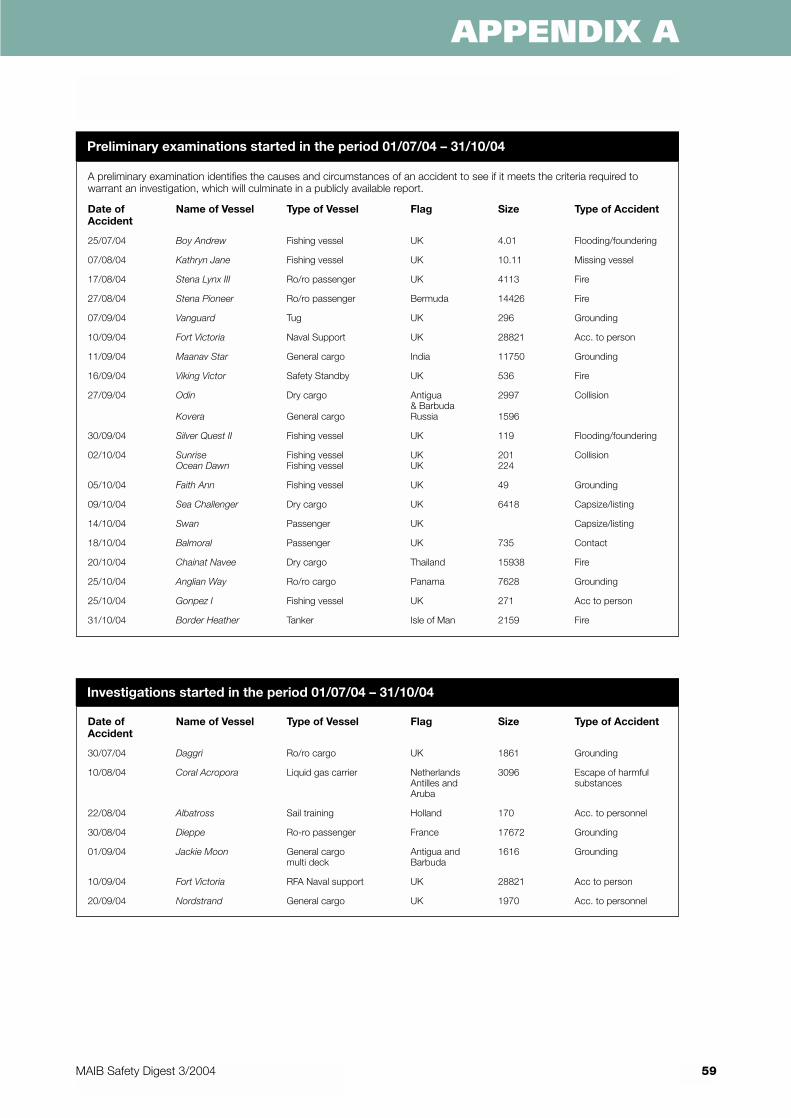
59MAIB Safety Digest 3/2004
APPENDIX A
A preliminary examination identifies the causes and circumstances of an accident to see if it meets the criteria required towarrant an investigation, which will culminate in a publicly available report.
Date of Name of Vessel Type of Vessel Flag Size Type of AccidentAccident
25/07/04 Boy Andrew Fishing vessel UK 4.01 Flooding/foundering
07/08/04 Kathryn Jane Fishing vessel UK 10.11 Missing vessel
17/08/04 Stena Lynx III Ro/ro passenger UK 4113 Fire
27/08/04 Stena Pioneer Ro/ro passenger Bermuda 14426 Fire
07/09/04 Vanguard Tug UK 296 Grounding
10/09/04 Fort Victoria Naval Support UK 28821 Acc. to person
11/09/04 Maanav Star General cargo India 11750 Grounding
16/09/04 Viking Victor Safety Standby UK 536 Fire
27/09/04 Odin Dry cargo Antigua 2997 Collision& Barbuda
Kovera General cargo Russia 1596
30/09/04 Silver Quest II Fishing vessel UK 119 Flooding/foundering
02/10/04 Sunrise Fishing vessel UK 201 CollisionOcean Dawn Fishing vessel UK 224
05/10/04 Faith Ann Fishing vessel UK 49 Grounding
09/10/04 Sea Challenger Dry cargo UK 6418 Capsize/listing
14/10/04 Swan Passenger UK Capsize/listing
18/10/04 Balmoral Passenger UK 735 Contact
20/10/04 Chainat Navee Dry cargo Thailand 15938 Fire
25/10/04 Anglian Way Ro/ro cargo Panama 7628 Grounding
25/10/04 Gonpez I Fishing vessel UK 271 Acc to person
31/10/04 Border Heather Tanker Isle of Man 2159 Fire
Preliminary examinations started in the period 01/07/04 – 31/10/04
Date of Name of Vessel Type of Vessel Flag Size Type of AccidentAccident
30/07/04 Daggri Ro/ro cargo UK 1861 Grounding
10/08/04 Coral Acropora Liquid gas carrier Netherlands 3096 Escape of harmfulAntilles and substancesAruba
22/08/04 Albatross Sail training Holland 170 Acc. to personnel
30/08/04 Dieppe Ro-ro passenger France 17672 Grounding
01/09/04 Jackie Moon General cargo Antigua and 1616 Groundingmulti deck Barbuda
10/09/04 Fort Victoria RFA Naval support UK 28821 Acc to person
20/09/04 Nordstrand General cargo UK 1970 Acc. to personnel
Investigations started in the period 01/07/04 – 31/10/04
Breakaway 5 – capsize of Breakaway 5, RiverBure, Norfolk on 19 July 2003Published 12 February 2004
Chelaris J – investigation of the capsize andsinking of the fishing vessel Chelaris J and loss ofall crew members, Banc de la Schole (nearAlderney) 1 October 2003Published 16 July 2004
Chelaris J – French version of above report sent12 August 2004
Dart 8 – injury to person while vessel berthingat Europort Terminal, River Thames on 21March 2004Published 30 September 2004
Donald Redford – investigation of the aggregatesdredger Donald Redford colliding with Hythe Pier,Southampton Water on 1 November 2003Published 6 May 2004
Elegance – investigation into 2 engine roomfires, subsequent flooding and foundering of thefishing vessel Elegance 30 miles north-west ofShetland on 30 January 2004 and 8.5 miles westof Shapinsay on 5 March 2004Published 11 August 2004
Elhanan T- flooding and foundering of thefishing vessel Elhanan T on 14 August 2003Published 4 March 2004
HC Katia – investigation of the grounding ofHC Katia while undergoing sea trials in theSolent on 3 December 2003Published 30 July 2004
Hoo Finch/Front Viewer – investigation into thenear collision between Hoo Finch and FrontViewer off the River Humber on 25 February2004Published 25 August 2004
Loch Ryan – swamping of unnamed cabincruiser in Lady Bay on Loch Ryan, 3 September2003, and associated wave generation issuesPublished 22 April 2004
Loch Ryan – swamping and foundering of a 4.6mgrp open sports boat with the loss of three liveson Loch Ryan south-west Scotland 12 July 2003Published 22 April 2004
Reno and Ocean Rose – collision off Whitby,North SeaPublished 12 October 2004
Scot Venture – contact with number 16 buoy,Drogden Channel, Denmark on 29 January 2004Published 15 September 2004
Trident VI – investigation of grounding of theinter-island passenger vessel Trident VI in PercéePassage, off Herm island near Guernsey in theChannel Islands 23 August 2003Published 30 January 2004
Annual Report 2003 Published June 2004
Leisure Craft Safety Digest Published January2004
Safety Digest 1/2004 Published April 2004
Safety Digest 2/2004 Published August 2004
A full list of all publications available from theMAIB can be found on our website atwww.maib.gov.uk
60
Reports issued in 2004
MAIB Safety Digest 3/2004
APPENDIX B
