safer services karl-tamminen-humber-trust
TRANSCRIPT

CPI European conference 2014
SAFER services:Defining our own pathways to reduction goals.
Karl TamminenHumber Trust

Practice innovation.
What is this presentation about? Dispelling a few myths. Challenging a few assumptions. Not about teaching people how “to suck
eggs”, but discussing alternative perspectives.
Ideas for changes in the ways service users and staff work together.
A pathway to closer, more productive working relationships between service users and staff which serves to reduce engagement in restraint .

….But first a couple of questions….

Question 1:
What do the following things have in common?
Question 2:
What do these people have in common?
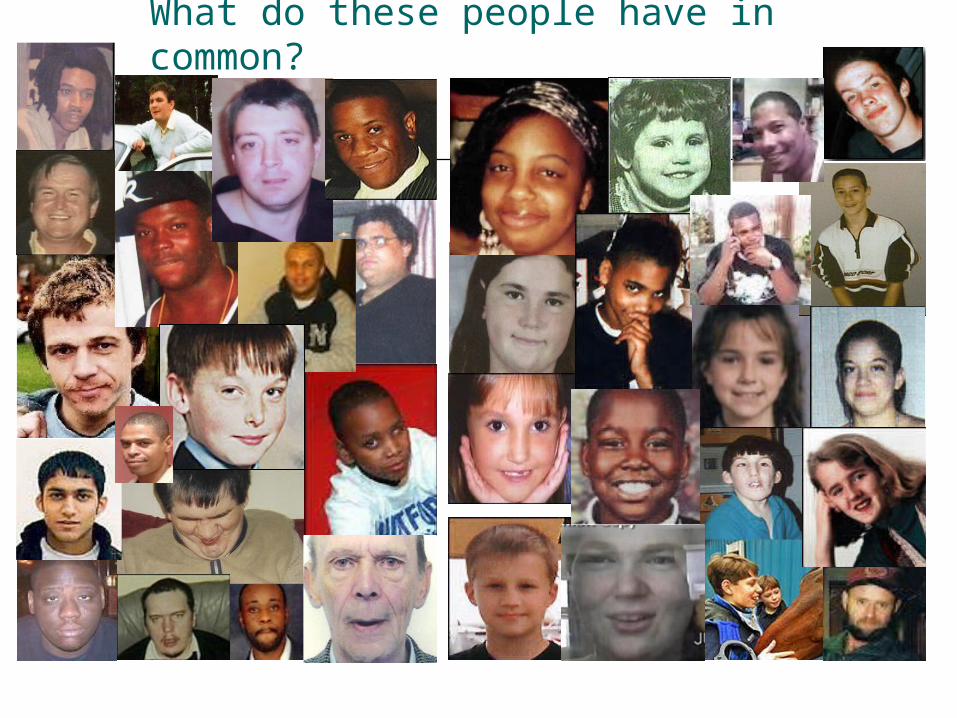
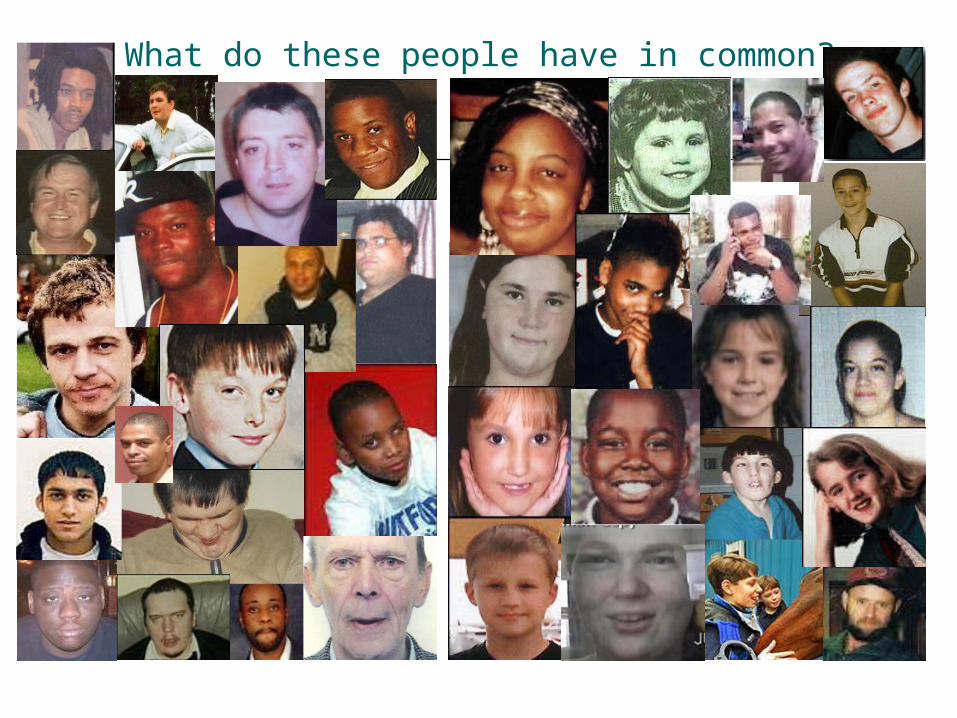
What do these people have in common?
The quiz answers:What do they have in common?
Answer one: These are all reasons people have been restrained,
Answer two: These are all people who have tragically died, following restraint (initiated for the above reasons).Was that a surprise?

Which are valid reasons to engage in restraint?
What do these people have in common?

Myth or true?
Restraint and seclusion are never used as punishment.
Restraint and seclusion are always used as a last resort.
Restraint and seclusion are a valid treatment option.
Restraint and seclusion are the main tools we have to maintain a safe environment.
When we utilise restraint or seclusion we are always acting within the legislation.
Professional practice is about developing and improving the way we use restraint and seclusion.
There is no evidenced based alternative to restraint and seclusion

who Age/ when
where why outcome
Adam Rickwood
14(2004)
Hassockfield Secure Training Centre in County Durham UK.
Refused to move from the table he was sitting at with friends
Psychological impact of restraint. Nose punch technique. Terrified child. Found dead by hanging in his bed space after resolution of restraint/ seclusion.
Angelika Arndt 7.(2006)
Children's Hospital in Minneapolis (US)
Refused to stop gargling milk. Fell asleep in seclusion, restrained to ensure she “learned her lesson” Restraint as a consequence. Restraint to reinforce positive behaviour and disincentives negative
complications from chest compression asphyxiation and said the restraint hold used by the staff at the centre may have contributed to her death.
Gareth Myatt. 15(2004)
Rainsbrook Secure Training Centre (UK)
Refused to clean out a toaster when directed by prison staff
Positional asphyxia

who Age/ when
where why outcome
David (Rocky) Bennet
41 (1998) UK Altercation with fellow patient around phone use. Racist language used
." Mr Bennett's capacity to breathe was restricted and the restraint "continued for substantially longer than was safe".
Jacob Michael 25 (2011) UK Called police for support, he refused to come out of his bedroom and threatened when police responded
Up to eleven police personnel. Pronounced dead when taken into custody. Verdict misadventure
Faith Finlay 17 (2008) US Damaging her own property in her own room
Prone restraint. Positional asphyxiation
Edith Campos 15 (1998) US Refused to hand over family photograph (personal possessions against policy)
Positional asphyxiation
What are the facts in the British cases? The People Who Died: ● The people who died ranged in age from 9 to 95 years old. ● Nearly one-third of those who died were over the age of 65, with 14
seniors over the age of 80 at the time of their deaths. ● The four youngest children to die in restraints were 9 years old. ● Almost three-quarters of those who died were male. ● Nearly 75% of those who died had a psychiatric history, with the most
common known diagnoses being schizophrenia, other psychotic disorders and mood disorders.
● More than half of those individuals admitted with a psychiatric diagnosis had been admitted for psychiatric treatment on three or more prior occasions.
● Twenty-five percent of those who died had a history of intellectual disabilities, learning disorders or other developmental disabilities.
● Nearly half of those who died had limited or no communication skills, due to medical circumstances that limited their awareness or consciousness.
SOURCE: (NATIONAL REVIEW OF RESTRAINT RELATED DEATHS OF CHILDREN AND ADULTS WITH DISABILITIES: The Lethal Consequences of Restraint (2011))

The IAP reported that between the 1st January 1999 and the 31st December 2009, there were 6,151 deaths in state custody in all services. In 22 of these cases, restraint was involved
Table 1 Deaths by age range
setting No of restraint related deaths
Age range 11-20
21-30
31-40
41-50
51-60
61-70
71-80
prisons 1 0 1 0 0 0 0 0Secure Young People’s
estates 1 1 0 0 0 0 0 0
Immigration Removal Centres 0 0 0 0 0 0 0 0
Police 15 0 1 6 3 2 1 1
In-pt mental health setting 5 0 2 3 0 0 0 0
TOTAL 22 1 4 9 3 2 1 1


Why do we need to change?
People die whilst being secluded and restrained. People are injured whilst being restrained and
secluded. People suffer harmful psychological affects whilst
being restrained and secluded. People have “flash backs” about restraint and
seclusion. For the main part neither staff or service users
like to engage in restraint or seclusion. Restraint and seclusion, as a measure of risk, can
keep people in Mental Health services longer.
I am here today to talk about the ingredients of a restraint and seclusion reduction programme.
Restraint and seclusion is seen as a normal, expected and natural part of every day life within a mental health unit…do you think that is how it has to be?

What is the current and predominant approach to restraint? 1. Have we trained people correctly to avoid
injuries and to give people the tools to maintain a safe and effective working environment?
2.Do we have the paper work necessary for defensible practice?
In short do we do it right and can we evidence it was done correctly?
… That’s fine as far as it goes, but what we seldom ask is “why did we end up restraining in the first place?”
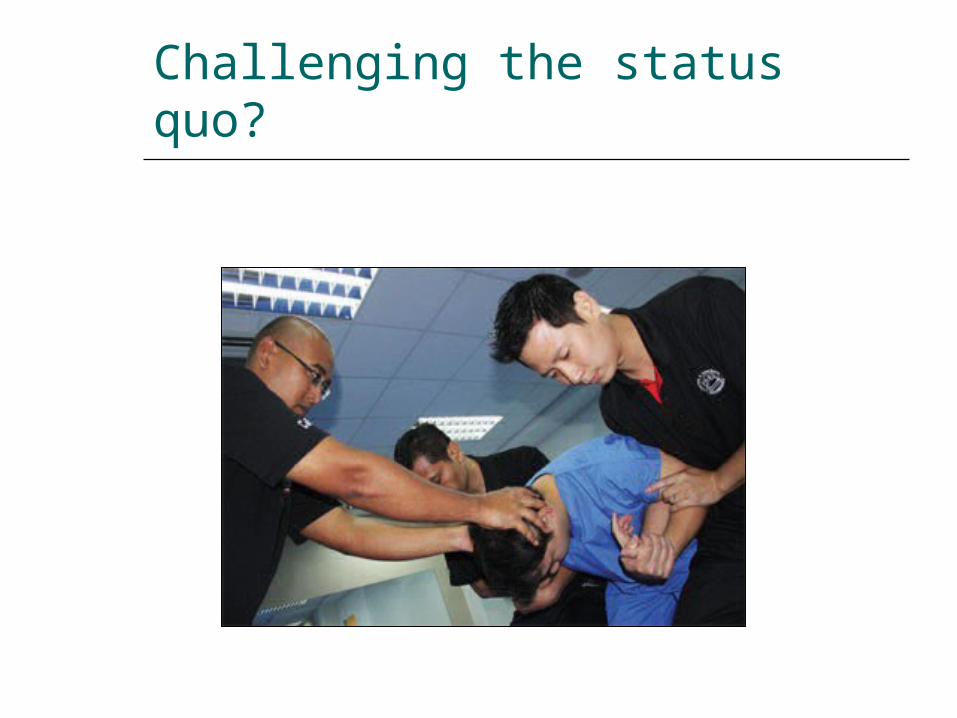
Challenging the status quo?

Is this a case of “its not broke so don’t fix it?”
If the training and the paper work is “correct”…

No. It cant be.

People ask me the same question:
“You know about restraint and seclusion Karl, got any tricks we could use to change the patients behaviour?”

The answer?
The “trick”, if there is one, is to change the question, its not about changing the way patients behave…
…..Its about changing the way we behave.

Is there another way?
Yes…
Who has written about “other” ways?
Dr Bennington Davis and Dr Tim Murphy “pathway to restraint free services” (engagement and empowerment model)
Dr Sandra Bloome “finding sanctuary (recovery focussed model)
Ann Alty and Tom Mason “break with the past (1994)
Joy Duxbury,

Empowerment and engagement model is used in the Salem Hospital Oregon and the recovery focussed models are used across all the hospitals in Pennsylvania and Oregon.
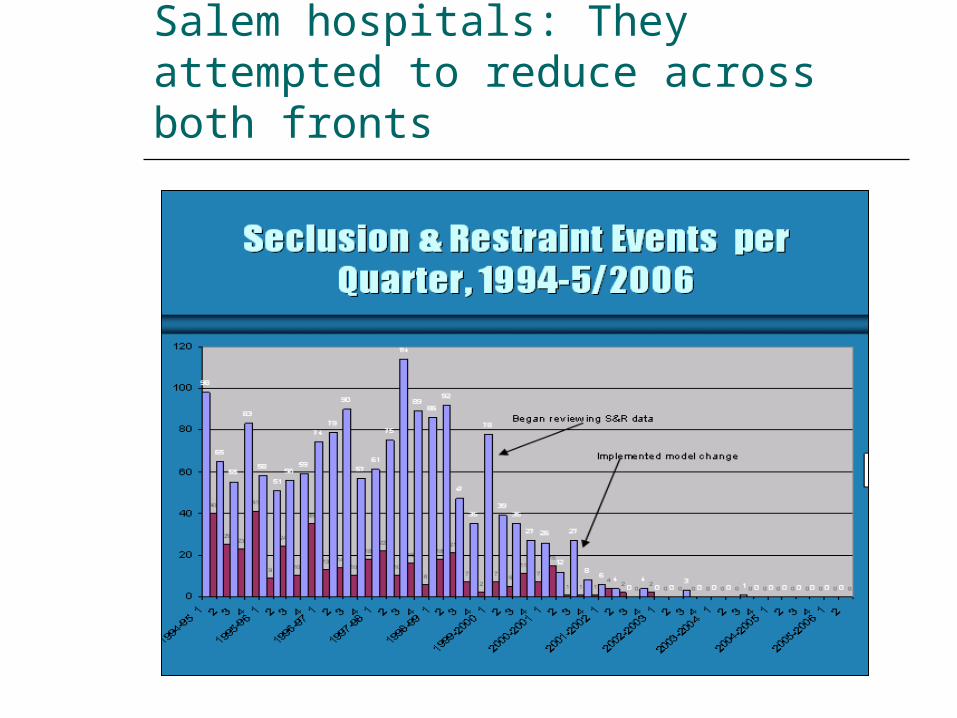
Salem hospitals: They attempted to reduce across both fronts

The changing trend from 1994
301
222
309
287
368
291
96
53
10 3 1 0 0 00
50
100
150
200
250
300
350
400
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Number of Seclusions by Year, 1994 through 9/2007 at Salem Hospital Psychiatry
Implemented model, 2001
Reviewed data & recovery/ trauma model 1999-2000

The Salem Oregon project
1450
260.7
36.85 2.25 0.25 0 0 00
200
400
600
800
1000
1200
1400
1600
Hours
2000 2001 2002 2003 2004 2005 2006 2007
Year
Total Annual Hours of Seclusion, 2000-9/2007 at Salem Hospital Psychiatry

Pennsylvania: across all hospitals and fronts: area one

Area two: mechanical restraints

Area three: physical restraint

So where do we start?
Owning change? Who needs to own it? Trust board? Clinicians? Service
Users? Families and carers? In short…..We all need to own it and
champion it in what ever way we can. If we don’t all make the process of change our own…then it will not happen.

Identifying the layers of change
Policy and procedure (embedding change) Daily rituals of practice Engagement of staff and service Users Approaches to restraint Avoiding inappropriate restraint Remaining empowered to restrain as a last resort
measure Utilising data to inform practice Education and training Support and reflection Creating a learning, sharing system

Pathway to restraint free services:what are the ingredients?
Reclassify: restraint and seclusion are not treatment options they represent treatment failures and breakdowns
Intensify: Scrutinise restraint. (use evidence and data to learn/ develop improve) feed that data into practice.
Choices: Give staff alternatives and service users more meaningful choices.

Pathway to restraint free services:what are the ingredients? Cont. Clinical focus: engage with Service Users and Care
plan for a restraint and seclusion free therapeutic environment.
Practice focus: examine the daily lives of our service Users, identify points of avoidable conflict and develop new ways of running wards
Operational focus: directors and managers need to get behind the change, own it and support it.
Reflect and relearn: Where it does happen, learn from it and plan try different approaches to avoid in the future. (restraint and seclusion reduction group)
Break the mould: Dare to be different.
Pathway to restraint free services:what are the ingredients? Cont.
Reinvent: Be the pioneers for services by introducing innovative, ground breaking, evidence based approaches to violence and aggression management which sets the tone for all other services.
Archaeology: Take up the challenge to unearth the evidence and generate the evidence that this approach works.

Pathway to restraint free services:what are the ingredients? Cont.
Support: Management and clinical leads need to support staff in innovative approaches as alternatives to restraint and seclusion.
Empower: Empower and engage with service users in new and innovative ways which do not blur boundaries
New philosophy: Move away from staff total control to shared responsibility for maintaining a safe environment. (within the professional envelope we retain responsibility for)

Why us? Why here?
There is at least twenty years of evidence out there that the foundations of and the ingredients to alternative approaches which we have discussed here is sound.
Its not easy, there are no magical solutions, successes are born out of hard work, positive risk taking, making mistakes, learning from them and addressing the challenges again and again

Why us? Why here?
There is no step by step guide that cam take us through each aspect on a guaranteed pathway to seclusion and restraint reduction and elimination….. but there is a framework.
We have the skills to do this. We are ready for the challenge. We are ready for change.

So what about the Humber Centre project?
We know where we want to get to~ the position where seclusion and restraint are indeed a last resort intervention.
We want to minimise “last resort” scenarios existing.
We know where the evidence is of what works and we will use it to build our new approach.
We want to work collaboratively with our service users to develop new approaches which are embraced by staff and service users, and are effective for us.

We are treading our own pathways to restraint and seclusion free services…
…….can you see yours?
Any questions?