safe entry and how to avoid complications
TRANSCRIPT


Safe Entry and How to avoid Safe Entry and How to avoid complicationscomplications? ?
؟
Mahmoud ZakherahProf. Obstertris and Gynecology
15-2-2014E-mail: .mszakhera@yahoo com

IntroductionIntroduction Laparoscopy is a very common
procedure in gynaecology. Access to the abdomen is the one
challenge of laparoscopic surgery.It was noted that complications of
laparoscopic surgery are mostly entry related and independent on complexity of surgery .
3

IntroductionIntroduction To minimize entry related injuries,
several techniques, instruments, and approaches have been introduced.
The life-threatening complications include injury to the bowel, bladder, major abdominal vessels, and anterior abdominal-wall vessel.
4

IntroductionIntroduction Other less serious complications
can also occur, such as post-operative infection, subcutaneous emphysema and extraperitoneal insufflation.
Laparoscopic procedures are minimal invasive surgically minimal invasive surgically but not not minimally invasive physiologically.minimally invasive physiologically.
5

Laparoscopic EntryLaparoscopic EntryAccess is the Key of Success
6

Laparoscopic EntryLaparoscopic EntryAccess is the Key of SuccessAccess is the Key of Success
Entry into the peritoneal cavity is the most dangerous part of the procedureBe careful…be careful…be
careful…The pneumoperitoneum The pneumoperitoneum – a continuing mistake in laparoscopy
7

Laparoscopic EntryLaparoscopic Entry
A. Closed access * Blind Insufflated Veress Needle Entry(1932) Non-insufflated Direct Trocar
Entry(1978) * Visual Optical Trocar insertion(1994)
( Layer by layer)
8

Laparoscopic EntryLaparoscopic Entry
B- Open access Hasson Technique 1978 Radially Expanding Access System
(1996) Visual Entry Systems Disposable Optical Trocars Endopath Optiview optical Trocar Visiport optical trocars EndoTIP visual cannula

Veress Needle EntryVeress Needle Entry
10

Veress Needle EntryVeress Needle Entry Pneumoperitoneum
instillation of gas into the peritoneal cavity
11

Veress Needle ModificationsVeress Needle Modifications
Pressure-sensor-equipped Veress needle
Optical Veress needle (minilaparoscopy)
12

Sites of Veress Needle EntrySites of Veress Needle Entry
1-Trans-umbilical :Intra-umblical
Sub or supra umbilical (smiling incision(
11-Extraumbilical
13

1-Trans-umbilical :
Veress needle insertion Towards uterus (forgives) Away from vessels (do not
forgives) angle 45
14

Checking springChecking spring
15

1-Trans-umbilical Clean
Incise
16
Realign the umbilicus prior to entry to regain“anatomical” positioning

1-Trans-umbilical Insertion
17
Like a dart


1-Trans-umbilical
In every case, theumbilicus was locatedcephalad to where thecommon iliac veincrossed the midline
19

Normal : BMI < 25 use angle < 45°
Non obese Mean location of the umbilicus was 0.4 cm caudal to the aortic bifurcation

Overweight BMI 25-30 use angle 45°- 90°
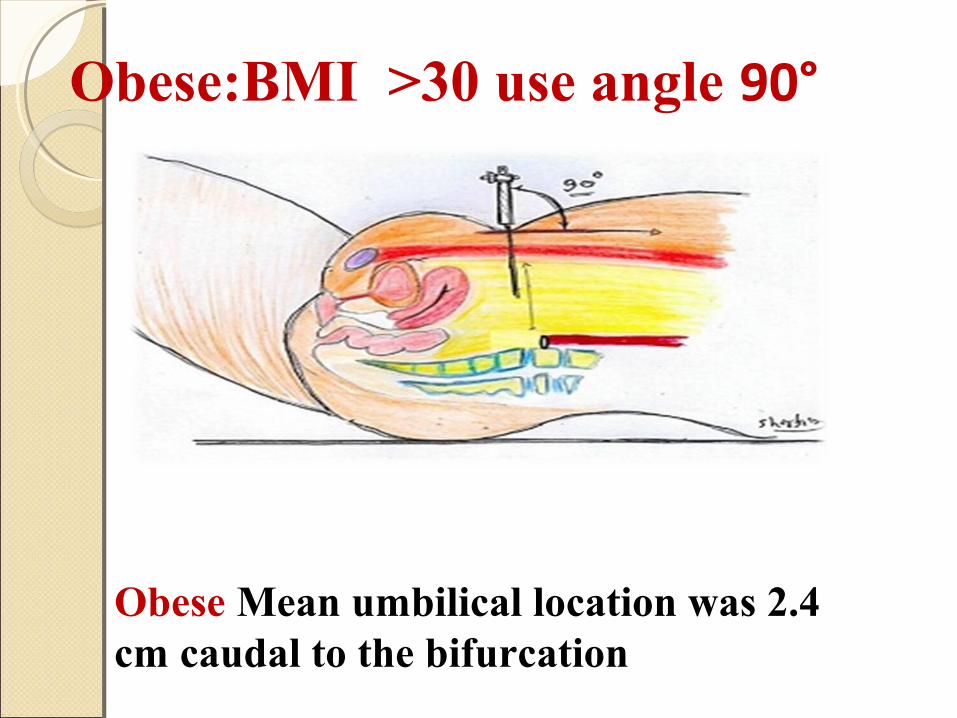
Obese:BMI >30 use angle 90°
Obese Mean umbilical location was 2.4 cm caudal to the bifurcation

Incorrect IncorrectCorrect
Midsagittal Plane Insertion

Veress needle safety testsVeress needle safety tests
(Tests for peritoneal entry)The “hiss” sound test Double click sound of the Veress needle Irrigation test (the syringe test.) Aspiration test (Palmer test) Hanging drop of saline test Insufflation of gas test Needle movement test

Veress needle safety Veress needle safety teststests
Irrigation test Aspiration test
25

Veress needle safety testsVeress needle safety tests
Hanging drop test HISS TEST
26

Number of Veress needle insertions Number of Veress needle insertions attemptsattempts Complication rates were as follows: one attempt, 0.8% to 16.3%; at 2 attempts, 16.31% to 37.5%; 3 attempts, 44.4% to 64%;
More than 3 attempts, 84.6% to 100%.
Complications were extraperitoneal insufflation, omental and bowel injuries, and failed laparoscopy.

11-Extraumbilical1.1. Left upper quadrant (LUQ,) Left upper quadrant (LUQ,)
PalmerPalmer’’s points point Ninth or tenth intercostal Ninth or tenth intercostal
spacespace 1.1. Transuterine Veress CO2 Transuterine Veress CO2
insufflationinsufflation2.2. Trans cul-de-sac CO2 Trans cul-de-sac CO2
insufflation(Transvaginal) insufflation(Transvaginal)

29
Palmer’s point just below
9th rib-midclvicular
Palmer’s Technique
3 cm below the left subcostal border in the midclavicular line

LUQ, Palmer’s point
3 cm below the left subcostal border
Elevation Of The Anterior Abdominal Wall
Veress Needle Insertion



Prerequisites:
Emptying of the stomach by nasogastric
suction
No previous splenic or gastric surgery
No significant hepatosplenomegaly
No portal hypertension
No gastropancreatic masses
Left Upper Quadrant (LUQ, Palmer’s) Laparoscopic Entry

Left Upper Quadrant (LUQ, Left Upper Quadrant (LUQ, Palmer’s) Laparoscopic EntryPalmer’s) Laparoscopic Entry
It should be considered in patients with:
Suspected or known periumbilical adhesions
History or presence of umbilical hernia
After three failed insufflation attempts at the umbilicus.
(SOGC Practice Guideline.193, 2007) (L:II-2 G:A)

35

Trocar Entry

Conventional trocar and cannulaConventional trocar and cannula
VALVES trap-door (trumpet )
flapper valveSIZE 5,9,10mm. PRIMARY SECONDARY
Tips pyramidal or
conical tip
37
TROCARS

38
Conventional Trocar and Cannula

Trocar EntryTrocar Entry1-Primary trocar
With pneumopeitoneun (conventional)VNEWithout pneumoperitoneum ( DTE)
2-Secondary trocars
39

Trocar EntryTrocar Entry1-Primary trocar
With pneumopeitoneun (conventional)VNEWithout pneumoperitoneum ( DTE)
2-Secondary trocars
40

Optical access trocarsOptical access trocars
i. Visiport uses a blade that strikes the fascia and peritoneum under laparoscopic guidance.
ii. Optiview uses a conical clear tip that is rotated under laparoscopic vision as it penetrates the fascia and peritoneum
41

Trocar EntryTrocar Entry
42

Trocar EntryTrocar Entry43

44

45

TROCAR INSERTIONTROCAR INSERTION
46

Laparoscopic PearlsLaparoscopic Pearls
Primary ports 45 angle of entry Stay midline Keep patient flatIf the same angle of insertion is used in
the Trendelenburg position, the trocar may be directed at the great vessels
47
Trocar EntryTrocar Entry
Low pressure entry
≤15mmHgHigh pressure entry (Garry
48

High pressure trocar entryHigh pressure trocar entryTemporary higher inflation
pressure (25-30mmHg)The use of transient HIP-Entry does
not adversely affect cardiopulmonary function in healthy women.
↑ separation between viscera and anterior abdominal wall
May therefore reduce risk of injury
49

14 mm Hg 20 -30mm Hg
The High Pressure Entry
The tip of the trocar can injure .abdominal contents The tip of the trocar is away from
abdominal contents.

3 kg force
3 kg force
25 mm Hg15 mm Hg
The tip of the trocartouched abdominal contents
> 4 cm maintained. the tip of the trocar never touched abdominal contents.
Phillips et al Gynaecol Endosc 1999;8:369–74.
Trocar insertion requires 4 to 6 kg of force
Tarney et al . Obstet Gynecol 1999;94:83–8.
< 4 cm
The High Pressure Entry
So the pressure of 25-30 mmHg is required

Trocar EntryTrocar Entry1-Primary trocar
With pneumopeitoneun (conventional)VNEWithout pneumoperitoneum ( DTE)
2-Secondary trocars
52

Direct Trocar EntryWithout pneumoperitoneum
( DTE)
53

Direct Trocar EntryDirect Trocar EntryPneumoperitoneum with Veress
needle insertion has actually three blind steps opposed to one in direct trocar entry.
Several reports pointed out that, direct trocar entry without pneumoperitoneum, is a safe alternative to Veress needle entry (RCOG greentop guideline 2009)
54

Technique of direct trocar entry Technique of direct trocar entry (DTE(DTE((
Intra-umbilical skin incision wide enough to accommodate the diameter of a sharp trocar/cannual system.
The anterior abdominal wall adequately elevated by the hand, and the trocar was inserted directly into the abdominal cavity, aiming towards the pelvic hollow
55

Technique of direct trocar entry Technique of direct trocar entry (DTE(DTE((
After removal of the sharp trocar, the laparoscope was inserted to confirm the presence of omentum or bowel in the visual field then pneumoperitoneum started
56

The advantages of direct trocar The advantages of direct trocar entry areentry areThe avoidance of complications related
to the use of the Veress needle as failed pneumoperitoneum, preperitoneal insufflation, intestinal insufflation, or the more serious CO2 embolism
Faster than any other method of entry.Immediate recognition and rapid
treatment of complications.
57

Succesful Direct Trocar EntrySuccesful Direct Trocar Entry
Relaxation: Adequate General anesthésiaSharp Trocar: the sharper = saferAdequate IncisionElevation of the abdominal wall (not
necessary)
58

59

60

Trocar EntryTrocar Entry1-Primary trocar
With pneumopeitoneun (conventional)VNEWithout pneumoperitoneum ( DTE)
2-Secondary trocars
61

62

How Should Secondary Ports be How Should Secondary Ports be InsertedInserted??
The secondary trocar should be placed in a well-controlled fashion under direct visualization
A suprapubic trocar Lateral lower pelvic ports Transillumination of the abdominal wall will
often identify these superficial vessels and aid in trocar placement. These trocars should be placed under direct visualization
63

How Should Secondary Ports be How Should Secondary Ports be InsertedInserted??
Secondary ports must be inserted under
direct vision perpendicular to the skin,
while maintaining the
pneumoperitoneum at 20–25 mmHg
64
RCOG Guideline No. 49 May 2008

How Should Secondary Ports be How Should Secondary Ports be InsertedInserted??
During insertion of secondary ports, the inferior epigastric vessels should be visualised laparoscopically to ensure the entry point is away from the vessels
65
RCOG Guideline No. 49 May 2008

How Should Secondary Ports be How Should Secondary Ports be InsertedInserted??
Once the tip of the trocar has pierced the peritoneum it should be angled towards the anterior pelvis under careful visual control until the sharp tip has been removed.
66
RCOG Guideline No. 49 May 2008
The “Baseball Diamond ConceptThe “Baseball Diamond Concept
67

Safety Zones for Anterior Safety Zones for Anterior Abdominal WallAbdominal Wall
68
Epigastric vessels are usually located in the area between 4 and 8 cm from the midline. Staying away from this area will determine the safe zone of entry of the anterior abdominal wall.

How Should Secondary Ports be How Should Secondary Ports be InsertedInserted??
Secondary ports must be removed under
direct vision to ensure that any
haemorrhage can be observed and
treated, if present.
69
RCOG Guideline No. 49 May 2008

Injury of Epigastric VesselsInjury of Epigastric Vessels
Managementdirect pressure with the operating portfull-thickness abdominal wall suture
ligationFoley catheter balloon tamponade.Exploration of the wound
70

Elevation of the anterior Elevation of the anterior abdominal wallabdominal wall
Many surgeons advocate elevating the lower anterior abdominal wall by hand or using towel clips at the time of Veress or primary trocar insertion.
Elevation of the anterior abdominal wall at the time of Veress or primary trocar insertion is not routinely recommended, as it does not avoid visceral or vessel injury. (II-2 B

Open Laparoscopic Entry

))Hasson TechniqueHasson Technique((
Particularly useful in previous abdominal surgery or underlying adhesions
73

Complications of laparoscopic Complications of laparoscopic abdominal entryabdominal entry Extraperitoneal insufflation Visceral injury Vascular injury

There are 3 subgroups of patients in whom the creation of a pneumoperitoneum
can be problematic: 1. Obese and thin patients,2. Patients with scars from
previous abdominal surgeries3. patients with failed
insufflations.

Laparoscopic surgery in the obese Laparoscopic surgery in the obese womenwomen
Obesity changes the relationship of the umbilicus to the aortic bifurcation.
In nonobese patients (BMI <25), the umbilicus had a median location 0.4 cm caudal to the bifurcation,.
In overweight (BMI 25 to 30) and obese (BMI >30) patients, the umbilicus had a median location 2.4 and 2.9 cm caudal to the aortic bifurcation, respectively.

Laparoscopic surgery in very thin Laparoscopic surgery in very thin womanwoman
Liable to more complicationsThe Hasson technique or insertion
at Palmer’s point is recommended for the primary entry in women who are very thin and women with morbid obesity
RCOG Guideline No. 49 May 2008 Grade C

AimAim
Safe Laparoscopy
78
Safe Entry

RCOG green top guidelinesRCOG green top guidelinesPrimary incision for laparoscopy
should be vertical from the base of the umbilicus (not in the skin below the umbilicus)
The Veress needle should be sharp, with a good and tested spring action
The operating table should be horizontal (not in the Trendelenburg tilt) at the start of the procedure
79

RCOG green top guidelinesRCOG green top guidelinesAn intra-abdominal pressure of 20–
25 mmHg should be used for gas insufflation before inserting the primary trocar (HPE).
The distension pressure should be reduced to 12–15 mmHg once the insertion of the trocars is complete
80

RCOG green top guidelinesRCOG green top guidelines
During insertion of secondary ports, the inferior epigastric vessels should be visualised laparoscopically to ensure the entry point is away from the vessels..
81

RCOG green top guidelinesRCOG green top guidelines
During insertion of secondary ports, once the tip of the trocar has pierced the peritoneum it should be angled towards the anterior pelvis under careful visual control until the sharp tip has been removed
82

RCOG green top guidelinesRCOG green top guidelines
Secondary ports must be removed under direct vision to ensure that any haemorrhage can be observed and treated, if present.
83

Risk of herniationRisk of herniation Hernias at the site of laparoscopic
ports are significantly more common with 12-mm trocars.
Close fascia, therefore, when you’ve used any type of trocar that is 10 mm or greater in diameter.
Chiong et al .. 2010;75(3):574–580.

RecommendationsRecommendations
Guidelines approved by the Executive and Council of the Society of Obstetricians an Gynecologists of Canada 2007.
85

Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. . Left upper quadrant (LUQ, Palmer’s)
laparoscopic entry should be considered in patients with suspected or known or history or presence of umbilical hernia, or after three failed insufflation attempts at the umbilicus. (II-2 A)
Other sites of insertion, such as transuterine Veress CO2 insufflation, may be considered if the umbilical and LUQ insertions have failed or have been considered and are not an option. (I-A)
The various Veress needle safety tests or checks provide very little useful information on the placement of the Veress needle.
It is therefore not necessary to perform various safety checks on inserting the Veress needle; however, waggling of the Veress needle from side to side must be avoided, as this can enlarge a 1.6 mm puncture injury to 1 cm in viscera or blood vessels,
Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. .

The Veress intraperitoneal (VIP-pressure 10 mm Hg) is a reliable indicator of correct intraperitoneal placement of the Veres needle;therefore, it is appropriate to attach the CO2 source to the Veress needle on entry. (II-1 A)
Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. .

The angle of the Veress needle insertion should vary according to the BMI of the patient, from 45 in non-obese women to 90 in obese women. (II-2 B)
Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. .

Elevation of the anterior abdominal
wall at the time of Veress or primary trocar insertion is not routinely recommended, as it does not avoid visceral or vessel injury. (II-2 B)
Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. .

The volume of CO2 inserted with the Veress needle should depend on the intra-abdominal pressure. Adequate pneumoperitoneum should be determined by a pressure of 20 to 30 mm Hg and not by predetermined CO 2 volume. (II-1 A)
Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. .

In the Veress needle method of entry, the
abdominal pressure may be increased immediately prior to insertion of the first trocar. The high intraperitoneal (HIP-pressure) laparoscopic entry technique does not adversely affect cardiopulmonary function in healthy women. (II-1 A)
Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. .

The open entry technique may be utilized as an alternative to the Veress needle technique, although the majority of gynaecologists prefer the Veress entry.
There is no evidence that the open entry technique is superior to or inferior to the
other entry techniques currently available. (II-2 C)
Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. .

Society of Obstetricians an Society of Obstetricians an Gynecologists of Canada 2007Gynecologists of Canada 2007 No significant risk differences have
been found for bowel and vascular injuries, when comparing the open-entry to the closed-entry technique.
Evidence level A1 [11]
94

20122012
An open-entry technique is associated with a significant reduction in failed entry when compared to a closed-entry technique, with no difference in the incidence of visceral or vascular injury.

Direct insertion of the trocar without prior pneumoperitoneum may bconsidered as a safe alternative to Veress needle technique. (II-2)
Direct insertion of the trocar is associated with less insufflation-related complications such as gas embolism, and it is a faster technique than the Veress needle technique. (I)
Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. .

Significant benefits were noted with the use of a direct-entry technique when compared to the Veress Needle.
The use of the Veress Needle was associated with an increased incidence of failed entry, extraperitoneal insufflation and omental injury; direct-trocar entry is therefore a safer closed-entry technique.
20122012

Shielded trocars may be used in an
effort to decrease entry injuries. There is no evidence that they result in fewer visceral and vascular injuries during laparoscopic access. (II-B)
Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. .

The visual entry cannula system may represent an advantage over traditional trocars, as it allows a clear optical entry, but this advantage has not been fully explored.
The visual entry cannula trocars have the advantage of minimizing the size of the entry wound and reducing the force necessary for insertion. Visual entry trocars are not-superior to other trocars since they do not avoid visceral and vascular injury. (2 B)
Society of Obstetricians an Society of Obstetricians an
Gynecologists of Canada 2007Gynecologists of Canada 2007. .

Arm tuckingArm tucking Avoid brachial plexus injury in
laparoscopic surgery by always tucking the arms, instead of placing them on arm boards that can inadvertently be moved beyond horizontal during the surgery.
Shveiky et al .. 2010;17(4):414–420.

Release of gas CompletelyRelease of gas Completely
Evacuate all gas and instruct the anesthesiologist to perform five manual inflations of the lungs before the patient is taken out of Trendelenburg position.
Phelps P, et al .Obstet Gynecol. 2008;111(5):1155–1160.

RecommendationsRecommendations Surgeons intending to perform
laparoscopic surgery should have appropriate training, supervision and experience.
Surgeons undertaking laparoscopic surgery should be familiar with the equipment, instrumentation and energy sources they intend to use.
102

اللهم سبحانكوبحمدك
انت ال اله ل ان اشهداليك واتوب استغفرك
103

If your only toy is a hammer every problem will look like a
nail