s. michael marcy memorial lecture how to communicate with
TRANSCRIPT

S. Michael Marcy Memorial Lecture How to communicate with vaccine hesitant
parents April 22, 2017
Children’s Hospital Los Angeles
• Following this presentation attendees will be able to… – provide knowledge to parents regarding the
tremendous burden that vaccine preventable diseases were in the pre-vaccine era.
– distinguish between parents who have unfounded fears or concerns about vaccine from those who have philosophical objection so as to be able to spend the appropriate amount of time with the encounter.
– understand how to discuss immunizations with hesitant parents
Objectives

JAMA 2007; 298: 2156


IMMUNIZATION SCHEDULE FOR PERSONS 0- 6 YEARS OF AGE: 1985
DTP DTP DTP DTP DTP
OPV OPV OPV OPV OPV
MMR

IMMUNIZATION SCHEDULE FOR PERSONS 0- 6 YEARS OF AGE:
1995
-------HBV1---- -- HBV2 -- ---------------HBV-------------
DTP DTP DTP ---- DTaP or DTP---- DTaP
Hib Hib Hib ------Hib------
OPV OPV ----------------OPV---------------
MMR



So what happened??!!!?

Vaccine refusal in schools for PBE*: Washington NEJM 2009;360:1981-1988
*Personal belief exemption

Vaccine refusal in schools for PBE: California 2009

Kindergarten Immunization Rates in California
2012to2013
2013to2014
2014to2015
2015to2016
ALL Public Priv ALLPublic Priv ALL Public Priv All Public Priv
School#
8220 5865 2355 7684 2355 2355 7738 5895 1843 8467 6275 2192
AllReq’dvac%
90.3 90.8 85.8 90.2 90.6 85.4 90.4 90.7 86.6 92.9 93.2 86.6
PBEs 2.79 2.55 5.2 3.15 2.92 5.88 2.54 2.31 5.33 2.37 2.16 4.93
MMR 92.7 93.2 88.2 92.3 92.7 87.6 92.6 92.9 88.8 94.5 94.9 90.5
12

“I took away the fear.”
Fear of disease displaced by fear of vaccines

• National Immunization Survey 2003-2004 (CDC)
• 3924 parents responded
Understanding parents’ fears Pediatrics 2008;122:718

Understanding parents’ fears Pediatrics 2008;122:718

No doubt indicators 71.7% Unsure, delayed or both 22.4% Refused 5.9%
Understanding parents’ fears Pediatrics 2008;122:718

Gust, D. A. et al. Pediatrics 2008;122:718-725
FIGURE 3 Main reasons parents who planned to delay or not to get a vaccine for their child changed their minds

CDC National Immunization Survey: The Problems Kennedy A, et al: Pediatrics 2011; 127 (Supp 1): S92-S99
• 40% of parents delayed or refused an
immunization in 2008…vs 20% in 2003.
• 33% thought too many shots were needed
• 25% questioned whether vaccines were effective
• 25% were concerned about autism
• 25% said they feared side effects or thought vaccines were unsafe.
18

CDC National Immunization Survey: Primary Sources of Information
Kennedy A, et al: Pediatrics 2011; 127 (Supp 1): S92-S99
19
Child’s healthcare provider 80%
Family 50%
Child’s other parent 25%
Friends 25%
American Academy of Pediatrics 20%
Centers for Disease Control 15%
Internet 10%

Most Recent NIS Results for Children 19-35 months of Age MMWR 2015;33:889-896
• Over all immunization rates remain high in the US, with target rates of 90% were met for > 3 doses of IPV, MMR, and HBV & > 1 dose of varicella vaccine BUT: – Targets for DTaP, HibV, HBV birth dose, PCV, HepAV and
complete rotavirus vaccine were missed – Disparity among non-Hispanic black children of other
ethnicities
• Top 10 in MMRV: Mississippi (>99.2%), Maryland (99.1%), No. Carolina (98.5%), New York State (98.2%), West Virginia (97.6%), Texas (97.4%), So. Dakota (97.1%), Connecticut (97.0%), Louisiana & Wyoming (96.8%), and Montana (Montana (96.0%)
• California is 27th (92.6%)
20
Measles in US, January 4-April 2, 2015M MMWR 2015;64:373-376
• Four outbreaks (including Disneyland) involving 159 patients – 155 US citizens and 4 visitors – Occurred in 18 states but 70% were associated with D-land exposure – Most cases were in California – Vaccination status:
• 45% were unvaccinated (68 US residents, 3 visitors) • Of the 68 US cases:
– 43% were unvaccinated due to PB or religion – 40% were ineligible, – 4% had missed opportunities, and – 13% had other reasons
• Measles cases cluster among unimmunized individuals especially where exemption rates are higher
21
Understanding parents’ fears Amer J Clin Epidemiol 2005;58:1081; J Amer Acad Nurse Pract
2007;19:15
• Concern about side effects • Pain and discomfort due to vaccines • Distrust of vaccines; conspiracy theories
– Preservatives, heavy metals, long term effects
• Infants’ immune systems will be overwhelmed by vaccines
• Risk of infection low; diseases are not that bad • Other barriers:
– Cost – Transportation – Inconvenience – Parental issues: drug use, lack of knowledge, motivation

Vaccine-preventable diseases Loss of “institutional memory”
“Those who cannot remember the past are condemned to repeat it.”
George Santayana

Vaccine-preventable diseases in US Myers MG, Pineda D 2008
Disease # cases pre-vaccine
Year of vaccine
# cases 2006
Small pox 48,164 Early 1900s 0
Diphtheria 175,885 Mid 1940s 0
Pertussis 142,721 Mid 1940s 15,632
Paralytic Polio 16,316 1955 0
Measles 503,282 1963 55
Congen Rubella 823 1969 1
Invasive Hib 20,000 1985 29
Hepatitis B 26,107 1986 4,713
Varicella 4,000,000 1995 48,445

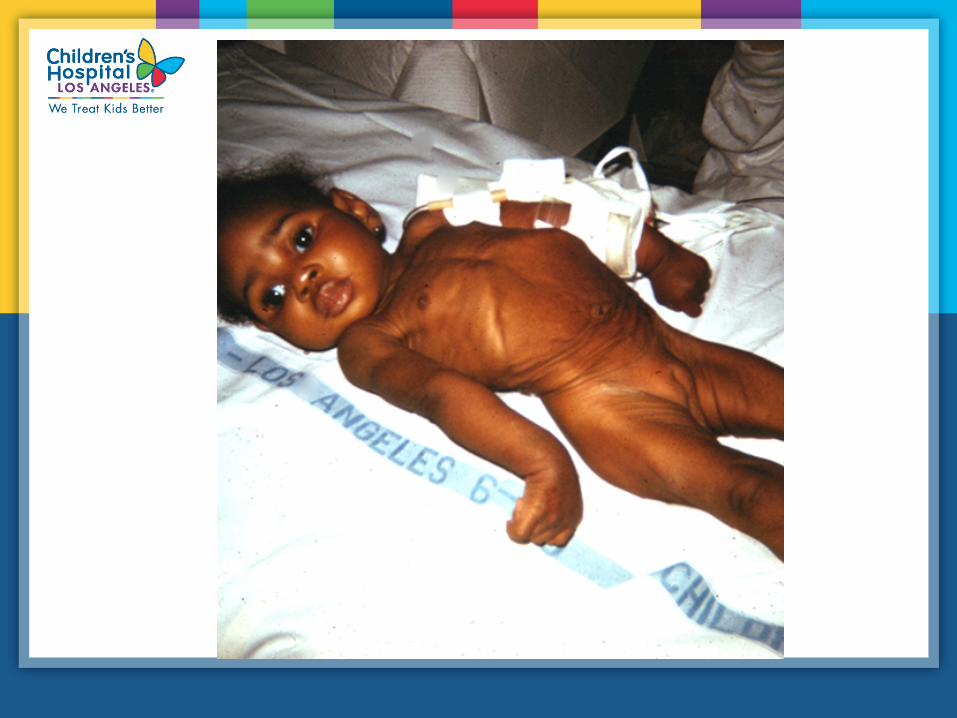
Measles
• Highly contagious viral illness • First described in 7th century • Near universal infection of
childhood in pre-vaccination era • In pre-vaccine era:
– 3-4 million cases/year – 28,000 hospitalizations – 450 deaths – 1000 children with chronic
disabilities MMWR 2008;57:203

0100200300400500600700800900
1950 1960 1970 1980 1990 2000
Cas
es (t
hous
ands
)Measles cases 1950-2000
CDC-MMWR
MMR

Measles Resurgence— United States, 1989-1991
• Cases 55,622
• Age group affected Children <5 yrs
• Hospitalizations >11,000
• Deaths 123
• Direct medical costs >$150 million

Measles Resurgence: Children’s Hospital Los Angeles, 1989-1991
PIDJ 1993;12:42-48
• Cases 440
• Age group affected 90% children <5 yrs
• Hospitalizations 195 (44.3%)
• Deaths 3
• Direct medical costs $1.7 million

Measles Resurgence: Children’s Hospital Los Angeles, 1989-1991
PIDJ 1993;12:42-48
Complications # %
Otitis media 276 63
Diarrhea 197 45
Dehydration 171 39
Pneumonia 160 36
Croup 82 19
Bacteremia 4 1

0
5
10
15
20
25
30
<5 5-19 20+
Age group (yrs)
Perc
ent
Pneumonia Hospitalization
Measles Complications by Age Group


32
Laryngotracheobronchitis Ross et al J Pediatr 1992;121:511-515
• 82/440 patients had croup
• Age: 15 months vs. 25 months
• Hospitalized 92% vs. 44%
• ICU care: 13 cases (17%)
• Intubation: 9 cases (11%)

Crude herd (community) immunity thresholds
Disease Crudeherdimmunitythreshold(%)
Diphtheria 85
Influenza 30-75
Measles 92-94
Mumps 75-86
Pertussis 92-94
Polio 50-93
Rubella 83-85
Smallpox 80-85
From:Plotkin,OrensteinandOffitVaccinesfiWhed.2004
33
Haemophilus influenzae type B and Hib Vaccine
Epidemiology and Prevention of Vaccine-Preventable Diseases
National Immunization Program
Centers for Disease Control and Prevention Revised December 2004

• Severe bacterial infection, primarily in infants
• Peak incidence was 41 cases/100,000 < 5 y/o in 1987
• 1 in 200 children < 5y/o had invasive Hib disease before the vaccine; 50-60% had meningitis
Haemophilus influenzae type b

Cellulitis6%
Arthritis8% Bacteremia
2%
Meningitis50%
Epiglottitis17%
Pneumonia15%
Osteomyelitis2%
Haemophilus influenzae type b Clinical Manifestations

• Accounted for approximately 50%-65% of cases
• Hearing impairment or neurologic sequelae in 15%-30%
• Case fatality rate 2%-5% in spite of effective antimicrobial therapy
Haemophilus influenzae type b Meningitis

Estimated Incidence* of Invasive Hib Disease, 1987-2000
*Rate per 100,000 children <5 years of age
l Hibvaccine

Haemophilus influenzae type b—United States, 1996-2000
• Incidence has fallen 99% since pre-vaccine era
• 341 confirmed Hib cases reported during 1996-2000 (average of 68 cases per year)
• Most recent cases in unvaccinated or incompletely vaccinated children
• Jan. 30, 2009 MMWR: 5 cases of Hib disease in Minnesota-3/5 were unimmunized MMWR 2009;58:58

Polio and Polio Vaccine
Epidemiology and Prevention of Vaccine-Preventable Diseases
National Immunization Program
Centers for Disease Control and Prevention Revised December 2004

Poliomyelitis
• First described by Michael Underwood in 1789
• First outbreak described in U.S. in 1843
• 21,000 paralytic cases reported in the U. S. in 1952
• Global eradication in near future?
l First described by Michael Underwood in 1789
l First outbreak in U.S. in 1843
l 21,000 cases of paralytic disease in the U.S. in 1952
l Eradication expected in ?


0
5000
10000
15000
20000
25000
1950 1956 1962 1968 1974 1980 1986 1992 1998
Cases
Poliomyelitis—United States, 1950-2002
Live oral vaccine Last indigenous case
Salk vaccine l Salk
l Sabin

0
2
4
6
8
10
12
14
1980 1984 1988 1992 1996 2000
Cases
VAPP Imported
Poliomyelitis—United States, 1980-2002

Polio Vaccination Recommendations
• Exclusive use of IPV recommended in 2000
• OPV no longer routinely available in the United States
• VAPP eliminated

Polio Eradication
• Last case in United States in 1979
• Western Hemisphere certified polio free in 1994
• Global eradication goal by ?
l Last case in the U.S. in 1979
l The Western Hemisphere certified polio free in 1984
l World eradication ?

Endemic Polio Countries
48

Spreading polio cases prompts Emergency Alert from WHO, May 5,
2014
49

Why get vaccinated?
• Because the microbes are still with us
Why get vaccinated?
• Because vaccine-preventable diseases are still here and/or are just a plane ride away – Measles in San Diego (Switzerland) – Measles in California (Philippines) – Measles in Texas, Michigan, & Pennsylvania (Japan) – Mumps (United Kingdom) – Chicken pox (USA) – Pertussis (USA) – Haemophilus influenzae type b (USA) – Meningococcal infections (USA)

Vaccine refusal is held to be ironic by some
52

Countering anti-vaccination attitudes PNAS 2015;112:10321-10324
• Rather than focusing on how effective and safe vaccines are; emphasize how bad the diseases were, and still are, and the risk they pose to the children. – Emphasizing the vaccines actually had a “backfire”
effect Pediatrics 2014;133:e835-e842; Vaccine 2015;33:459-464
• RCT showing information to parents and non-parents both with negative views on vaccines – Developed an attitude scale to measure effect – 3 groups: “disease risk”, “autism correction”, “control group”
53
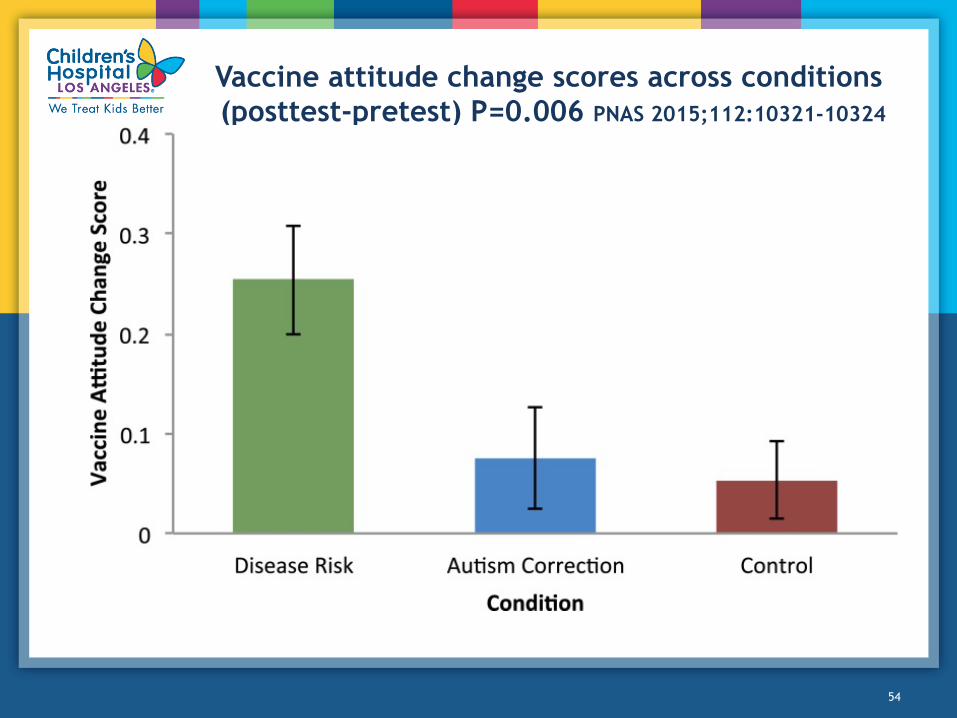
Vaccine attitude change scores across conditions (posttest-pretest) P=0.006 PNAS 2015;112:10321-10324
54

Comparison of parents with negative attitudes to non-parents PNAS 2015;112:10321-10324
55

Understanding parents’ fears Amer J Clin Epidemiol 2005;58:1081; J Amer Acad Nurse Pract
2007;19:15
• Concern about side effects • Pain and discomfort due to vaccines • Distrust of vaccines; conspiracy theories
– Preservatives, heavy metals, long term effects
• Infants’ immune systems will be overwhelmed by vaccines
• Risk of infection low; diseases are not that bad • Other barriers:
– Cost – Transportation – Inconvenience – Parental issues: drug use, lack of knowledge, motivation

Thimerosal and Autism What’s the Evidence?
• Population-based cohort study from Denmark 01/01/90 to 12/31/96 linked vaccine records to autism dx. – Ethyl-Hg (E-Hg) was removed from vaccines in 1993 – Of 467,450 children, 1227 had autism but no
association with E-Hg was found. • VSD study in the US-no association with E-Hg found • Ecologic studies from Denmark (2) and Sweden showed
autism increasing after E-Hg was removed from vaccines • California Department of Health study JAMA 2003;290:1763; Pediatrics 2003;112:1039; Arch Gen Psychiatry 2007;65:19

Increases in Autism Reported to California’s Developmental Services System Archive
GenPsychiatry 2007;65:19
l Thimerosalremovedfromchildhoodvaccines

• Aluminum is the third most abundant element on the earth’s surface, and the most abundant metal
• As a consequence, aluminum is in the air we breathe, the food we eat, and the water we drink
Aluminum ad hoc hypothesis

• Aluminum and infant formulas • By 6 months of age: Vaccines 4 mg Breast milk 10 mg Infant formula 30 mg Soy formula 120 mg
Aluminum in Food

Vaccines overwhelm the immune system
Infants are exposed to numerous new immuno-genic proteins and polysaccharides daily
DPT whole-cell contained about 3000 antigens
Today, exposure to routine immunizations through 5 years of age would be ~150 antigens
On-time receipt of all vaccines during infancy has no adverse effect on neuropsych outcomes
61

1900 1960 1980 2000 2010
Vaccine Prot. Vaccine Prot. Vaccine Prot. Vaccine Prot. Vaccine Prot.
Smallpox ~ 200 Smallpox ~ 200 Diphtheria 1 Diphtheria 1 Diphtheria 1
Diphtheria 1 Tetanus 1 Tetanus 1 Tetanus 1
Tetanus 1 WC Pertussis ~ 3000 AC Pertussis 2-5 AC Pertussis 2-5
WC Pertussis ~ 3000 Polio 15 Polio 15 Polio 15
Polio 15 Measles 10 Measles 10 Measles 10
Mumps 9 Mumps 9 Mumps 9
Rubella 5 Rubella 5 Rubella 5
Hib conj. 2 Hib conj. 2
Varicella 69 Varicella 69
Pneumo conj. 8 Pneumo conj. 8
Hepatitis B 1 Hep A and B 5
Rotavirus 15
Influenza 8
1 ~ 200 5 ~ 3217
7 ~ 3041
11 123-126
14 150-153
Immunogenic Proteins and Polysaccharides in Vaccines

CAPACITY OF IMMUNE SYSTEM RESPONSE
63
• Based on the number of antigens in vaccines, the total number of lymphocytes capable of responding to these antigens, and the amount of antibody they can produce….
• Theoretically, an individual could respond to up to 10 million antigens given at one time


• Not science-based or evidence-based • More likely to induce needle phobia • Increase time during which children are
susceptible to vaccine-preventable diseases
• Responsibility to the waiting room • No benefit
Harm in Alternative Schedule

Remember parents’ concerns differ in content and intensity Vaccine 2005;23:2486-2493
• Four different parent types: – Believer (less time)
• Highest commitment to immunization • May want to know about safety and side effects • Lowest information needs
– Relaxed (less time) • High commitment to immunization • Less likely to ask questions • May need to probe for unanswered questions • Low to moderate information needs
– Conscientious objector (less time) • Refusers-low or no information needs • Is decision firm? • Accepts consequences: exclusion from school, risk of quarantine,
warn PCP of illness, etc
67

Remember parents’ concerns differ in content and intensity Vaccine 2005;23:2486-2493
• Four different parent types: – Cautious (more time)
• High emotional involvement with child • Rigid thought patterns • May have concerns re specific vaccines • Moderate to low commitment to immunization • Believe in disease protection Encourage dialogue • Discuss risks and benefits • Stress risks of disease/complications Possible questions • Is protection necessary? • Benefits of “natural” disease?
68

Kaiser Permanente: A new approachNor. Cal.
• The goal is to immunize, not win a debate. • Belief defeats science and evidence; e.g. belief eats
science and evidence for lunch • To non-vaccinators, vaccine refusal is the social norm. • Parents have the best intentions for their children. • Hesitant parents can be influenced by physicians
proportional to the degree of trust they have in them. • Words matter, e.g. protect rather than vaccinate • It is acceptable to disagree.
69

Kaiser Permanente: A new approach
Rhetorical tools • Cognitive ease
– Create comfortable, receptive state; unhurried, calm, confident, friendly
– Do no confront with a difficult choice
• The natural assumption – Assume that vaccines will be given – Vaccine as default, parents will go with the flow
• Identity strategy – Identify as excellent parents – Both parents and physician want safety and protection for the
child
• Advantageous terms- safety, protection; repetition
70

Algorithm for discussion
71
Createcogni]veease
Unsure parents l Trust the provider l Open to discussion
l Natural assumption
l Identity as good parents
l Address concerns
l Emotional appeal
Delaying parents Less trust
Social networks define identity
l Natural assumption
l Identity as good parents
l Address concerns with caution
l Forge common identity
Refusing parents • Little trust • Resistant to discuss
• Don’t debate, build trust
• Put at ease • Realistic goals • Establish common
ground • Define, accept
disagreement • Reinforce bond l Active choice=risk of disease
l No action=protection by vaccine

Take-Home Points • Vaccines save hundreds of thousands of lives
every year • Scientific evidence has proven vaccines are safe • Despite proof, parents are more anxious than
ever but all parents with concerns are not the same, i.e. relaxed, fence sitters, refusers
• We must speak plainly, directly, and passionately, emphasizing: – The terrible impact vaccine preventable diseases
had before vaccines were available – The need to vaccinate each and every child – The safety of vaccines

Vaccine information resources
• Allied Vaccine Group – www.vaccine.org
• Centers for Disease Control and Prevention (CDC) – www.cdc.gov/vaccines
• American Academy of Pediatrics – www.cispimmunize.org
• Immunization Action Coalition – www.immunize.org & www.vaccineinformation.org
• Nat’l Network for Immunization Information – www.immunizationinfo.org
• Vaccine Education Center at CHOP – www.vaccine.chop.edu
• California Immunization Coalition – www.immunizeca.org (Shot by Shot)
74

Selected bibliography • Salmon D, Pavia A, Gellin B: Vaccine safety throughout the product
life cycle. Pediatrics 2011; 127: S1-S137
• Offit P, Moser C A: The problem with Dr Bob’s alternative vaccine schedule. Pediatrics 2009; 123: e164-e169
• Offit P A: Deadly Choices: How the Anti-VaccineMovement Threatens us All. New York City, Basic Books, 2011.
• Plotkin S, Orenstein W, Offit P: Vaccines, 5th Ed. Elsevier, 2008
• Price C S, et al: Prenatal and infant exposure to thimerosal from vaccines and immune globulins and risk of autism. Pediatrics, 126: 656-64
• Thompson W W, et al: Early thimerosal exposure and neuropsychological outcomes at 7 and 10 years. New Engl J Med 2007; 357: 1281-92
75