ruptur hepar
DESCRIPTION
managementTRANSCRIPT
HistoryHistory
�� Basic data: Basic data:
�� 姓名:林姓名:林**伯伯
�� 4545歲,男性歲,男性
�� AdmissionAdmission date: 2007/09/12date: 2007/09/12
�� Chief complaint: Chief complaint:
diffuse abdominal pain after traffic accidentdiffuse abdominal pain after traffic accident
�� Present illness:Present illness:
�� On Sep. 12 about 21:40, he drove a car and hit On Sep. 12 about 21:40, he drove a car and hit
against traffic island. According to the first aider, against traffic island. According to the first aider,
there was alcoholic odor on his body and blood in there was alcoholic odor on his body and blood in
his oral and nasal cavity. There was no open his oral and nasal cavity. There was no open
wound and active bleeding in appearance.wound and active bleeding in appearance.
�� PE:PE:
�� TPR: 35.2 / 80 / 18 ; BP: 92/63 mmHgTPR: 35.2 / 80 / 18 ; BP: 92/63 mmHg
�� Consciousness: E3M6V5, drowsyConsciousness: E3M6V5, drowsy
�� Abdomen: soft and distension, diffuse tenderness, Abdomen: soft and distension, diffuse tenderness,
rebounding pain(+), hypoactive bowel soundrebounding pain(+), hypoactive bowel sound
�� Lab Data:Lab Data:
�� Blood gas: pH=7.295, pCO2=32.6, HCO3=15.4, Blood gas: pH=7.295, pCO2=32.6, HCO3=15.4,
pO2=57.1, pO2=57.1, ABEcABEc==--9.7, 9.7, SBEcSBEc==--9.89.8
�� GOT/GPT= 297/230, GOT/GPT= 297/230,
�� U/A: OB=2+U/A: OB=2+
�� Bedside abdominal echo: Bedside abdominal echo:
�� No fluid seenNo fluid seen
�� Abdominal CT:Abdominal CT:
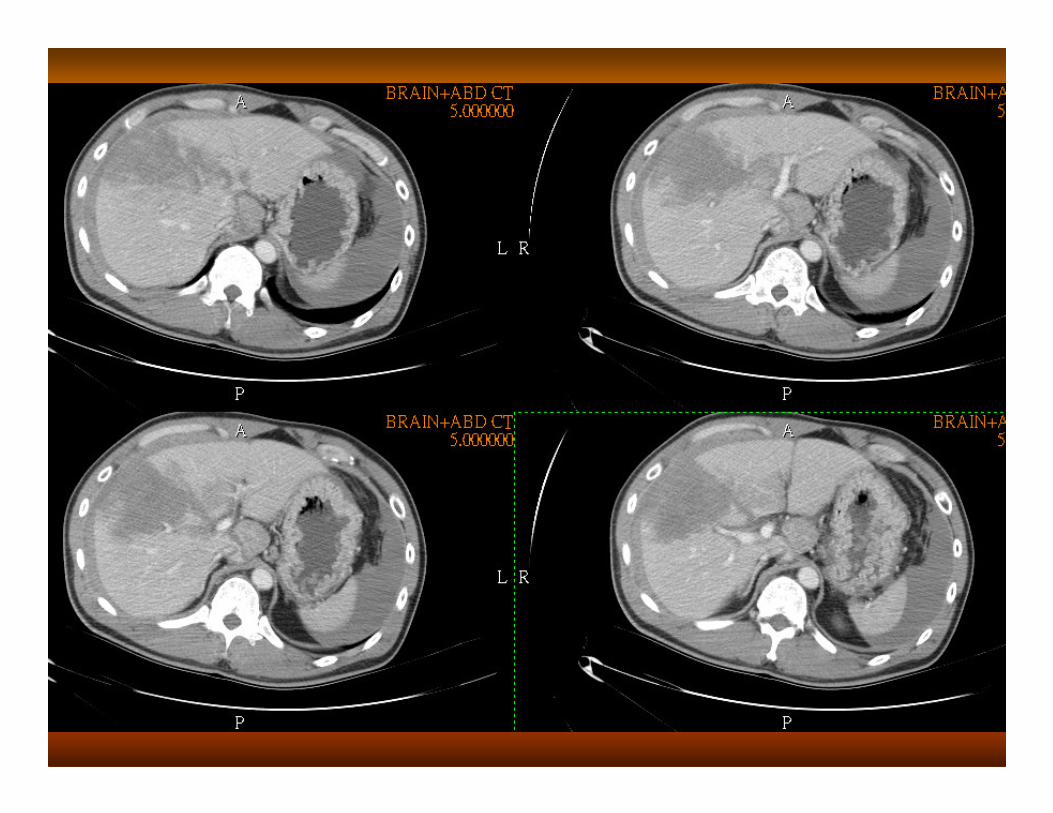
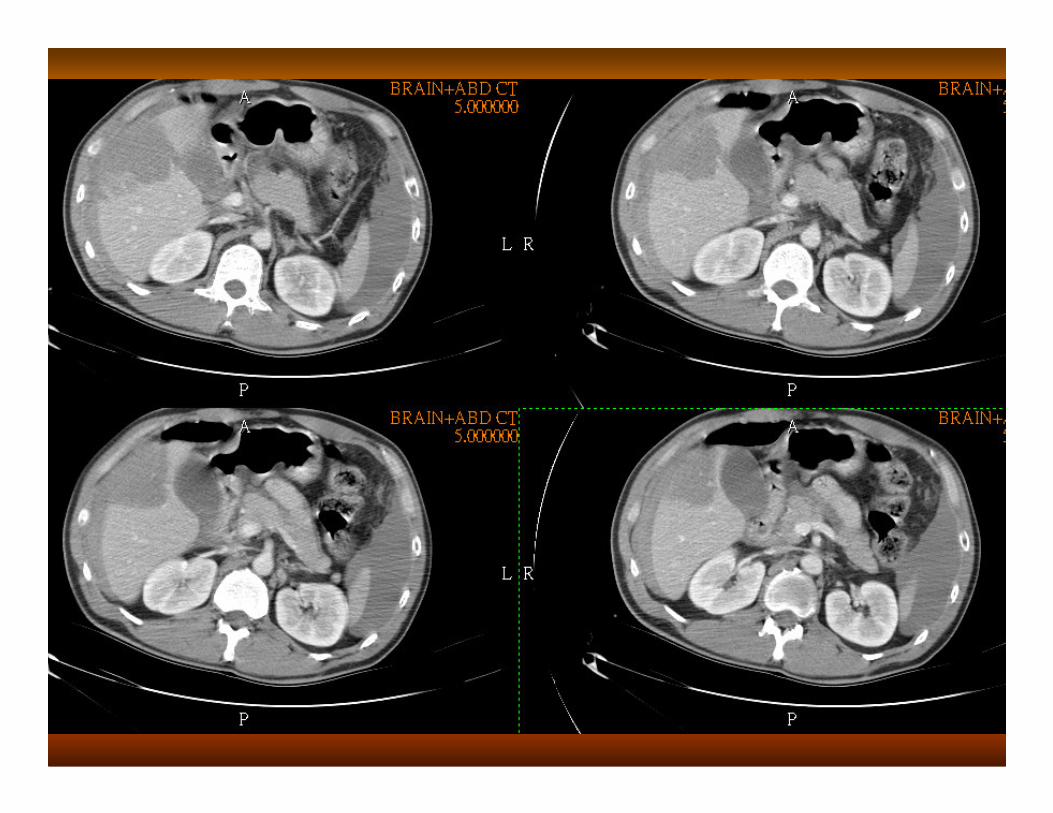
�� Impression: liver laceration, grade IVImpression: liver laceration, grade IV
�� Treatment: Treatment:
�� Sep. 13th, 2:35AMSep. 13th, 2:35AM�� hepatorrhaphyhepatorrhaphy + repair of + repair of
portal vein and hepatic veinportal vein and hepatic vein
liver laceration of S4~S7liver laceration of S4~S7
�� Sep. 13th, 9:50AMSep. 13th, 9:50AM�� Partial Partial segmentectomysegmentectomy
(S4~S6)(S4~S6)
�� Died on Sep. 14th, 10:40AMDied on Sep. 14th, 10:40AM

DiscussionDiscussion
Mechanism of liver injuryMechanism of liver injury
�� 2 categories of blunt liver trauma:2 categories of blunt liver trauma:
�� Deceleration trauma Deceleration trauma –– fall from heightfall from height
create fissure in the hepatic parenchyma, typically between create fissure in the hepatic parenchyma, typically between
right posterior and right anterior sector, may involve major right posterior and right anterior sector, may involve major
vesselsvessels
�� Crush injury Crush injury –– direct trauma to the abdomen over liver direct trauma to the abdomen over liver
areaarea
�� Penetrating trauma may not associate with Penetrating trauma may not associate with parenchymalparenchymal
disruption, but life threatening hemorrhage if major disruption, but life threatening hemorrhage if major
vessel is transectedvessel is transected
Symptoms & SignsSymptoms & Signs
�� Shock, hypotensionShock, hypotension
�� Abdominal distensionAbdominal distension
�� Anterior abdominal wall bruisingAnterior abdominal wall bruising
�� Abdominal painAbdominal pain
�� Peritoneal signsPeritoneal signs
�� Shoulder tip pain (Shoulder tip pain (subdiaphragmaticsubdiaphragmatic hematoma causing hematoma causing phrenicphrenic
nerve irritation) nerve irritation)
�� Penetrating low thoracic woundPenetrating low thoracic wound
�� Posterior penetrating wound below scapulaPosterior penetrating wound below scapula
�� Abdominal Abdominal sonographysonography: : intraperitonealintraperitoneal fluidfluid
�� Diagnostic peritoneal Diagnostic peritoneal lavagelavage (DPL): blood(DPL): blood
�� CT: blood, collapsed cava, shock CT: blood, collapsed cava, shock nephrogramnephrogram, small , small hypodensehypodense
spleen (gold stander)spleen (gold stander)
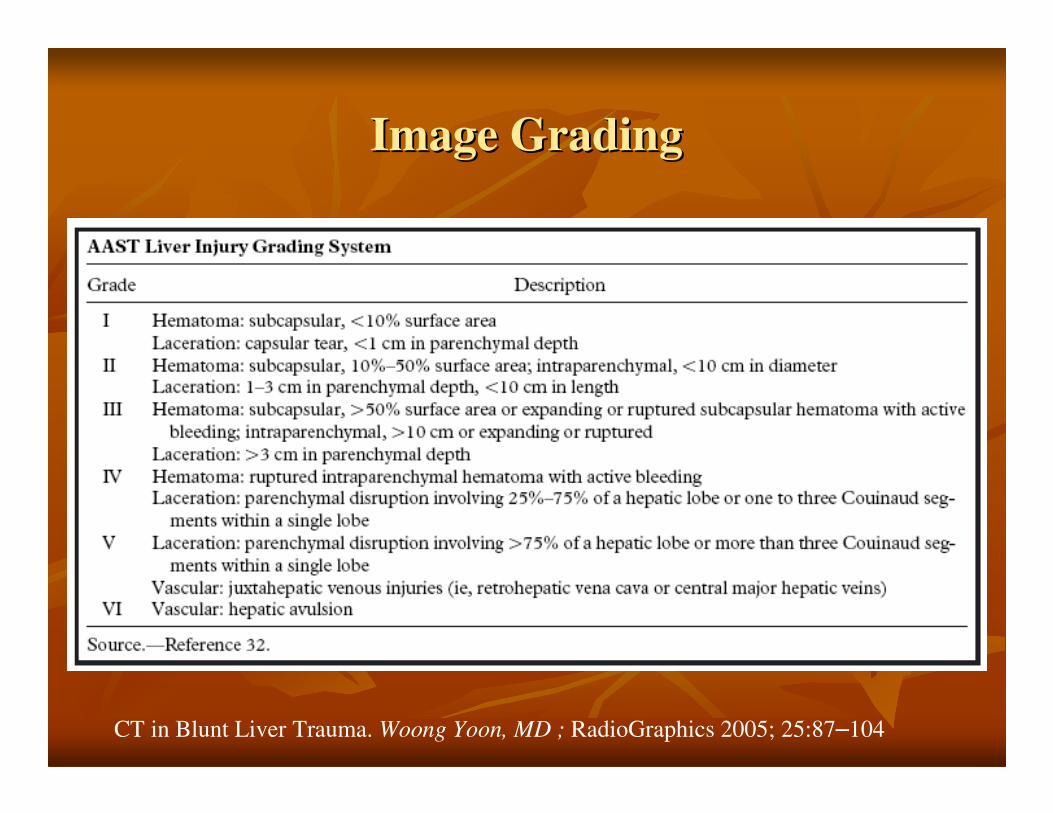
Image GradingImage Grading
CT in Blunt Liver Trauma. Woong Yoon, MD ; RadioGraphics 2005; 25:87–104
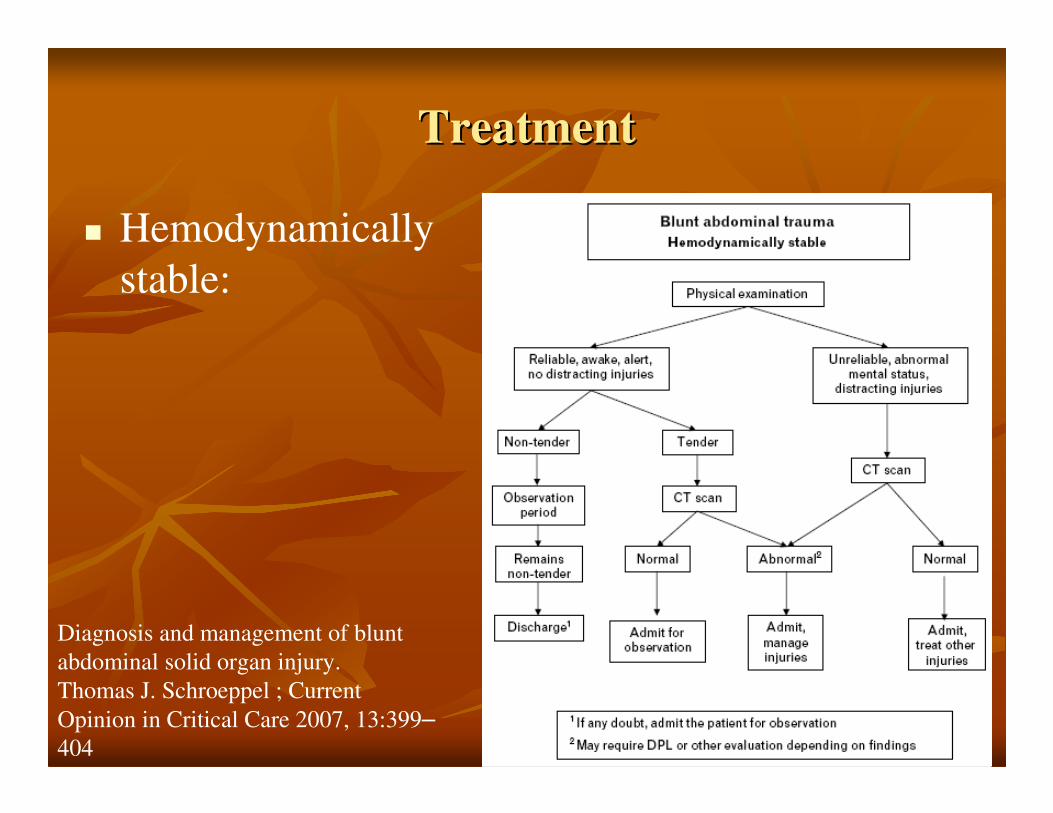
TreatmentTreatment
� Hemodynamically
stable:
Diagnosis and management of blunt
abdominal solid organ injury.
Thomas J. Schroeppel ; Current
Opinion in Critical Care 2007, 13:399–
404

�� IVF challengeIVF challenge
�� Blood transfusionBlood transfusion
�� Angiographic Angiographic embolizationembolization
�� Monitor Monitor HctHct and vital signsand vital signs
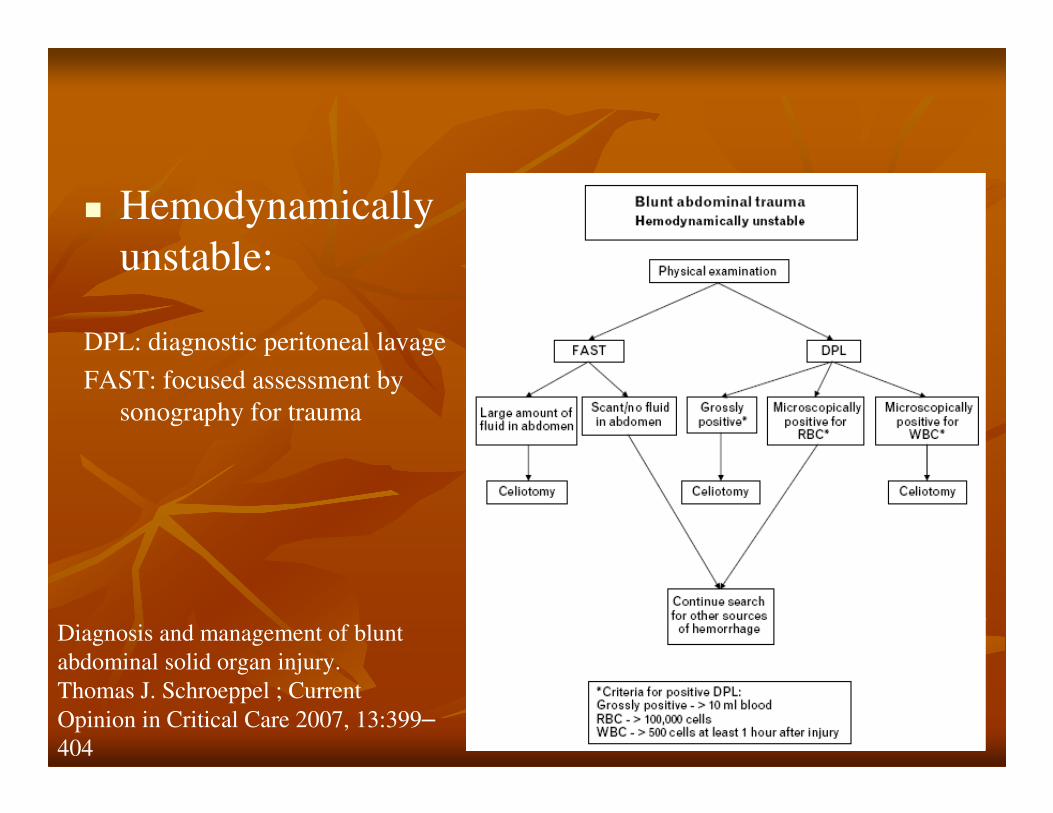
� Hemodynamically
unstable:
DPL: diagnostic peritoneal lavage
FAST: focused assessment by
sonography for trauma
Diagnosis and management of blunt
abdominal solid organ injury.
Thomas J. Schroeppel ; Current
Opinion in Critical Care 2007, 13:399–
404
�� Operation: Operation:
�� Principles: control of bleeding, removal of Principles: control of bleeding, removal of
devitalized tissue, adequate drainagedevitalized tissue, adequate drainage
�� Simple suture with or without Simple suture with or without hemostatichemostatic agentsagents
�� Deep mattress sutureDeep mattress suture
�� PackingPacking
�� DebridementDebridement
�� ResectionResection
�� Mesh Mesh hepatorrhaphyhepatorrhaphy
PrognosisPrognosis
�� Overall mortality rate: 8~10% ; morbidity rate: Overall mortality rate: 8~10% ; morbidity rate:
18~30%18~30%
�� NonoperativeNonoperative management:management:
�� Grade 1~3: success rate near 95%Grade 1~3: success rate near 95%
�� Grade 4~5: success rate 75~80%Grade 4~5: success rate 75~80%
�� Complication rate 11%: Complication rate 11%: most could be managed with most could be managed with
angioembolizationangioembolization for contrast for contrast extravasationextravasation, CT, CT--guided guided
drainage for hepatic abscess and drainage for hepatic abscess and bilomasbilomas, laparoscopy for bile , laparoscopy for bile
peritonitis, and endoscopic retrograde peritonitis, and endoscopic retrograde
cholangiopancreatographycholangiopancreatography (ERCP) for persistent bile leaks.(ERCP) for persistent bile leaks.
�� Operative management:Operative management:
�� Operative mortality is 20Operative mortality is 20––43%43%
�� Complication: postoperative bleeding(10%), intraComplication: postoperative bleeding(10%), intra--
abdominal abscess(7.2%), abdominal abscess(7.2%), biliarybiliary fistula (7~10%), fistula (7~10%),
hemobilia(rarehemobilia(rare))
ReferencesReferences
�� SabistonSabiston: textbook of surgery. 17th ed.: textbook of surgery. 17th ed.
�� Emergency Emergency imageingimageing. R. Brooke Jeffery, 1st ed.. R. Brooke Jeffery, 1st ed.
�� HepatobiliaryHepatobiliary and pancreatic surgery. O. James and pancreatic surgery. O. James Garden, 2nd ed.Garden, 2nd ed.
�� Diagnosis and management of blunt abdominal solid Diagnosis and management of blunt abdominal solid organ injury. Thomas J. organ injury. Thomas J. SchroeppelSchroeppel ; Current Opinion ; Current Opinion in Critical Care 2007, 13:399in Critical Care 2007, 13:399––404404
�� CT in Blunt Liver Trauma. CT in Blunt Liver Trauma. WoongWoong Yoon, MD ; Yoon, MD ; RadioGraphicsRadioGraphics 2005; 25:872005; 25:87––104104
�� Advances and Changes in the Management of Liver Advances and Changes in the Management of Liver Injuries. SEONG K. LEE ; THE AMERICAN Injuries. SEONG K. LEE ; THE AMERICAN SURGEON March 2007, 201SURGEON March 2007, 201--206206