rubine de beer physiotherapist - university of pretoria · rubine de beer physiotherapist ... steps...
TRANSCRIPT

Rubine de BeerPhysiotherapist
Steve Biko Academic HospitalFebruary 2014

Mobilisation Asher 1947
“Teach us to live that we may dread unnecessary timein bed. Get people up and we may save our patients from an early grave.”
(Grosselink et al. 2008)

What is Mobilisation in ICU?Physical activity sufficient to elicit acutephysiological effects that enhance
Ventilation,
Central and Peripheral Perfusion,
Circulation,
Muscle metabolism,
Alertness,
Are counter measures for venous stasis and DVT.(Walsham et al. 2009)

Effects of Immobility in ICU CNS Cardiovascular Respiratory Gastro-Intestinal Urinary Tract Dermatological Psychological Musculoskeletal Functional Independence Cost of Care Length of hospital stay

CNS Decrease Perception
Decrease Proprioception / Co-ordination
Decrease Balance
Decrease / Increase muscle tone

Cardiovascular Decrease Cardiac Output, Stroke Volume, Peripheral
Vascular Resistance
Venous stasis
Orthostatic intolerance
Increase risk of venous thrombosis and Pulmonary Emboli
Decrease total cardiac and left ventricular size

Respiratory Decrease ant / post diameter → Decrease alveolar
size → Decrease gas exchange
Decrease in functional residual capacity
Decrease lung compliance
Retained secretions → Pneumonia (VAP)
Atelectasis
Respiratory muscle weakness
Decrease exercise tolerance

Gastro Intestinal Decrease bowel function
Abnormal fluid distribution

Urinary Tract Kidney stones
Increase excretion of Nitrogen, Calcium, Magnesium and Potassium

Dermatological Pressure sore formation

Psychological Depression
Anxiety
Decrease Cognition
Delirium

Musculoskeletal Decrease muscle protein synthesis Muscle atrophy (30% loss in week) Decrease muscle strength (40% loss in week) Contractures Decreased Range of motion (ROM) Loss of bone density – Osteoporosis Neuromuscular weakness
Critical Illness Polyneuropathy or Myopathy
Decrease Quality of Life (5 years post ICU)

Critical IllnessCritical Illness
↑ Reactive O2 Species Bed Rest Malnutrition↑ Inflammatory Cytokines
Neuromuscular Abnormalities
Muscle Weakness
↑ Mechanical Ventilation Time ↑ ICU / Hospital Stay ↓ Physical Function ↓ QOL
(Truyong et al. 2009)

CIP & CIM CIP
Decrease sensation
Distal weakness > Proximal weakness
Deep tendon reflex absent
CIMNormal sensation
Proximal weakness > Distal weakness
Hypoactive deep tendon reflex
(Khan et al. 2006)

When to Start Mobilisation 24-48 hours after ICU admission
Physiological StabilityNeurologically (Conscious)
Cardiovascular (HR <50% age predicted Max HR,Normal BP, Normal ECG)
Respiratory (SaO2 >90%, Respiratory pattern)
Haematologically (HB >7, Platelet count, Glucoselevels 3.5 – 20mmol/L)
Sufficient perfusion to maintain normal organ function
(Dean & Ross, 1994)

Steps of MobilisationPassive or active limb exercises in
bedSitting over side of bed with or without
support
T/F from bed to chair with partial mechanical assistance
T/F from bed to chair without mechanical assistance
Standing and walking on the spot with mechanical assistance
Walking without mechanical assistance
(Walsham et al. 2009)

Mobilisation Techniques Limb exercises (passive, active assisted,
active and resistant)
Active / passive moving or turning in bed
Hoist
Slide board
Motomed
Walking Aid (Walking frame)

Effects of mobilisation Psychological
Central nervous system - Consciousness
Cardiovascular
Respiratory - Improve airway clearance
- Improve lung volumes
Gastro Intestinal
Musculoskeletal – Functional Independence
(Stiller K. 2007)

When to Stop Mobilisation SaO2 <88%
Hypotension associated with dizziness
Heart rate >max heart rate
Change in heart rhythm
Increased respiratory rate
Chest pain
Excessive pallor of flushing skin

Mobilisation Team Medical staff
Nursing staff
Physiotherapist

Current Treatment Passive exercises
Active Assisted
Active exercises
Resistant exercises
Sitting over side of bed
Sit in chair with hoist
Standing / walking with hoist
Walk with assistive device
Motomed

Motomed Exercise Machine in ICU
Passive exercises
Active exercises
Resistant exercises
Upper limb and Lower limb
Feedback to the patient

Motomed

Motomed General weakness
COPD
Brain Injury / CVI
Paraplegia
Cancer
Awake and orientated
Contra Indications for mobilisation

Different Studies Australian Journal of Physiotherapy – 2004
Physiological responses to the early mobilisation of the intubated, ventilated abdominal surgery patient.
Study was done in Sydney Australia, took ABG before and after mobilisation. Mobilise patient into supine, sit, stand, walk on the spot for 1 minute and sit in chair for 20 minutes. Study showed physiological changes due to change in position from supine to sit / stand. No changes from sit / stand – 20 min sit.

Studies Cont.

Studies Cont.

Studies Cont. Physical Therapy – September 2006
Effects of physical training on functional status in patients with prolonged mechanical ventilation – 6 week training program (active and resistant UL and LL exercises)
Function, QOL and Psychological improvement
Critical Care Medicine – 2007Treatment group received OT and PT during daily wake
up. Control group received standard care. Treatment group had shorter ventilation days, decrease delirium and quicker recovery.

Studies Cont. American Journal of Critical Science - 2011
Questionnaire send 12 months after DC from hospital for patients with respiratory failure – patients not mobilised early - readmission / passed away
Critical Care Research and Practise – July 2012
Randomised control study of 90 patients. Treatment group ride bicycle for 5 days, 20 min per day – Mobiliseindependantly with D/C. Control group need rehab

Case Study: SBAH Surgery ICU19 Year old female patient. Diagnosed with achalasia,
leiomyopathy, diabetes and asthma. She presented with
an unknown syndrome. The patient presented during
May 2013 with abdominal pain. She had several
laparotomies for bowl obstruction. Fistula was formed.
3 months on TPN, with no oral intake.
Admitted in ICU 26 July 2013 – 46 days in ICU

Daily Physiotherapy Rx Chart
Date Treatment Date Treatment
26/7 Chest Physiotherapy 05/8 Mobilise bedside
27/7 - 06/8 Mobilise chair
28/7 - 07/8 Stand – with assistance
29/7 Mobilise bedside 08/8 Motomed exercise
30/7 Bed exercise 09/8 -
31/7 Stand – with assistance 10/8 -
01/8 Motomed exercise 11/8 -
02/8 Mobilise bedside 12/8 Bed exercise
03/8 - 13/8 Bed exercise
04/8 - 14/8 -

Daily Physiotherapy Rx Chart
Date Treatment Date Treatment
15/8 Stand, walk next to bed 25/8 -
16/8 Motomed 26/8 Motomed exercise
17/8 - 27/8 Sit w/chair outside
18/8 - 28/8 -
19/8 - 29/8 Bed exercise
20/8 Motomed exercise 30/8 Walk with walking frame
21/8 Bed exercise 31/8 -
22/8 Stand with assistance 01/9 -
23/8 Motomed exercise 02/9 Bed exercise
24/8 - 03/9 Mobilise bedside

Daily Physiotherapy Rx Chart
Date Treatment
04/9 Mobilise in chair
05/9 Motomed exercise, Stand, Sit outside
06/9 Mobilise with ventilator
07/9 -
08/9 -
09/9 Mobilise in chair
10/9 Motomed exercise

Motomed ChartPatient Info 08/08 16/08 20/8 05/9 10/9
Mode of ventilation
SIMV SIMV SIMV SIMV CPAP
FiO2 40% 40% 40% 40% 40%
PEEP 10 8 6 5 5
PSV 24 10 12 18 8
Set Rate 10 10 8 1 0
SaO2 97% 91% 96% 98% 98%
Type of feeding TPN = 60 TPN = 60Intestimine
= 8
TPN = 60Survimed
= 10
Survimed= 40
Survimed= 40
Weight 29 kg 25 kg 25 kg 30 kg 30 kg
Type of Exercise Arms Arms Arms Arms Arms
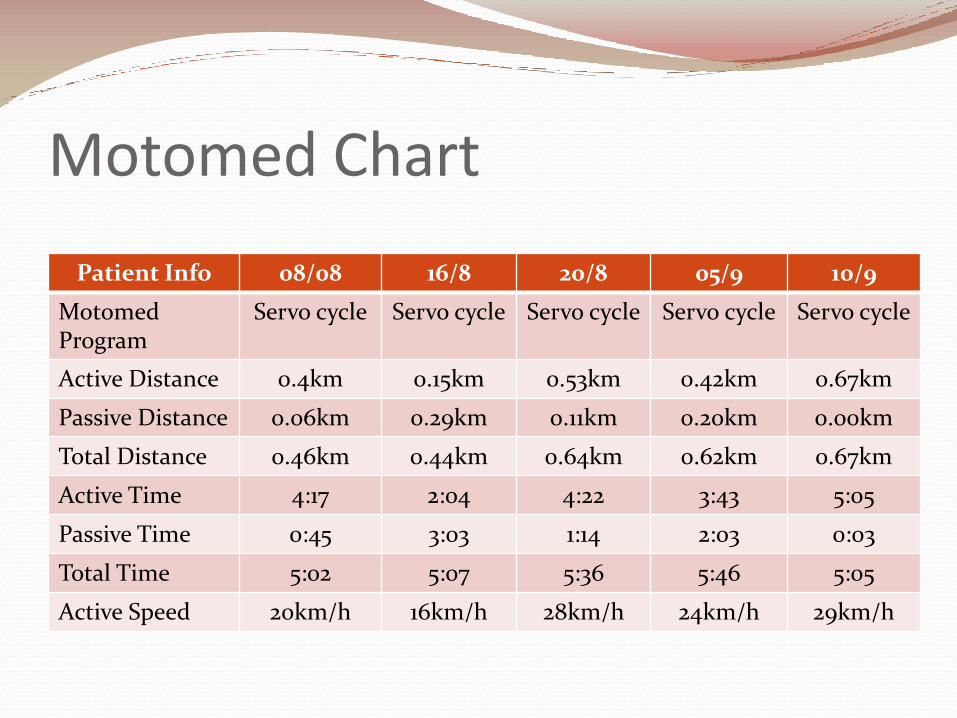
Motomed Chart
Patient Info 08/08 16/8 20/8 05/9 10/9
MotomedProgram
Servo cycle Servo cycle Servo cycle Servo cycle Servo cycle
Active Distance 0.4km 0.15km 0.53km 0.42km 0.67km
Passive Distance 0.06km 0.29km 0.11km 0.20km 0.00km
Total Distance 0.46km 0.44km 0.64km 0.62km 0.67km
Active Time 4:17 2:04 4:22 3:43 5:05
Passive Time 0:45 3:03 1:14 2:03 0:03
Total Time 5:02 5:07 5:36 5:46 5:05
Active Speed 20km/h 16km/h 28km/h 24km/h 29km/h

Motomed Chart
Patient Info 08/8 16/8 20/8 05/9 10/9
Total Energy 3.7kcal 1.8kcal 3.8kcal 3.2kcal 4.5kcal
Energy 15.5KJ 7.5KJ 15.8KJ 13.5KJ 19.0KJ
Symmetry 35/65 42/58 56/44 48/52 52/48
Muscle Tone - 1 - 0 -
Muscle Spasm 0 0 1 0 0
Peak Performance
- - 1 0 1

Conclusion Early mobilisation is beneficial to critically ill patients
Decrease duration of mechanical ventilation
Decrease delirium
Decrease length of stay
Improve Functional independency
Safe money
Inter-professional team work is essential

Conclusion Mobilise…
Mobilise…
Mobilise….


References Adam S. ABC of ICU. BMJ. 1999;319:175-178 Chiang L. Effects of Physical Training on Functional Status
in patients with prolonged mechanical ventilation. Physical Therapy. 2006;86(9):1271-1281
Clini E. Early physiotherapy in the respiratory ICU. Respiratory Medicine. 2005;99:1096-1104
Clark E. Effectiveness of an early mobilization protocol in TBICU: Retrospective cohort study. Journal of the American Physical Therapy Association. 2013; 93:186-196
Dale M. Mobilizing patients in the ICU. JAMA. 2008;300:1685-1690
Grosselink R. Physiotherapy for adult patients with critical illness. Intensive Care Medicine. 2008;34:1188-1199
Khan J. Acquired weakness in the ICU. Minerva Anestesiol. 2006;7:401-405

References Parker A. The importance of early rehabilitation and
mobility in the ICU. 2013 Perme C. Early mobility and walking program for
patients in ICU. AJCC. 2009;18:212-221 Ruth M. How early should we mobilize ICU patients?
Medscape. 2011 Stiller K. Physiotherapy in ICU. Chest. 2000;118:1801-
1813 Stiller K. Safety aspects of mobilising acutely ill
inpatients. Physiotherapy Theory and Practice. 2003;19:239-257
Truyong A. Bench-to-bedside review: Mobilizing patients in ICU – from pathophysiology to clinical trials. Critical Care. 2009;13:216

References Van Aswegen H. Physiotherapy in ICU. 2011 Walsham J. Should we mobilise critically ill patients?
Critical Care And Resusitation. 2009;11:290-300
Zafiropoulos B. Physiological responses to the early mobilisation of intubated, ventilated abdominal surgery patients. Australian Journal of Physiotherapy. 2004;50:95-99
Zomorodi M. Developing a mobility protocol for early mobilisation of patients in a surgical / trauma ICU. Critical Care Research and Practise. 2012

QUESTIONS ????