rtog lung cancer committee 2012 clinical trial...
TRANSCRIPT

1
RTOG Lung Cancer Committee
2012 Clinical Trial Update
Wally Curran
RTOG Group Chairman

2
RTOG Lung Committee: Active Trials
• Small Cell Lung Cancer
– Limited Stage (Intergroup Trial)
– Extensive Stage (RTOG 0937)
• Early Stage NSCLC
– In-operable (0813 and 0915)
– Operable (RTOG 1021 / ACOSOG Z4099)
• Locally advanced NSCLC
– Stage IIIA with minimal N2 disease (0839)
– Stage IIIA –Individualized RT Rx with PET-adapted boost (1106)

3
Phase III Comparison of Thoracic
Radiotherapy Regimens in Limited-
stage Small Cell Lung Cancer
CALGB 30610
RTOG 0538
Principal Investigator: Jeff Bogart, MD
RTOG PI: Ritsuko Komaki, MD

CDDP VP-16
CDDP VP-16
CDDP VP-16
CDDP VP-16
70 Gy Gy, 2.0 Gy QD
61.2 Gy, 1.8 Gy QD FB Con bst
CDDP VP-16
CDDP VP-16
CDDP VP-16
CDDP VP-16
PCI
45 Gy 1.5 Gy BID
CDDP VP-16
CDDP VP-16
CDDP VP-16
CDDP VP-16
R
A
N
D
O
M
I
Z
E
CALGB 3060/RTOG 0538
(months)
0 4 8 12 16 20 24 28 32 36
0
10
20
30
40
50
60
70
80
90
100
PCI
Control
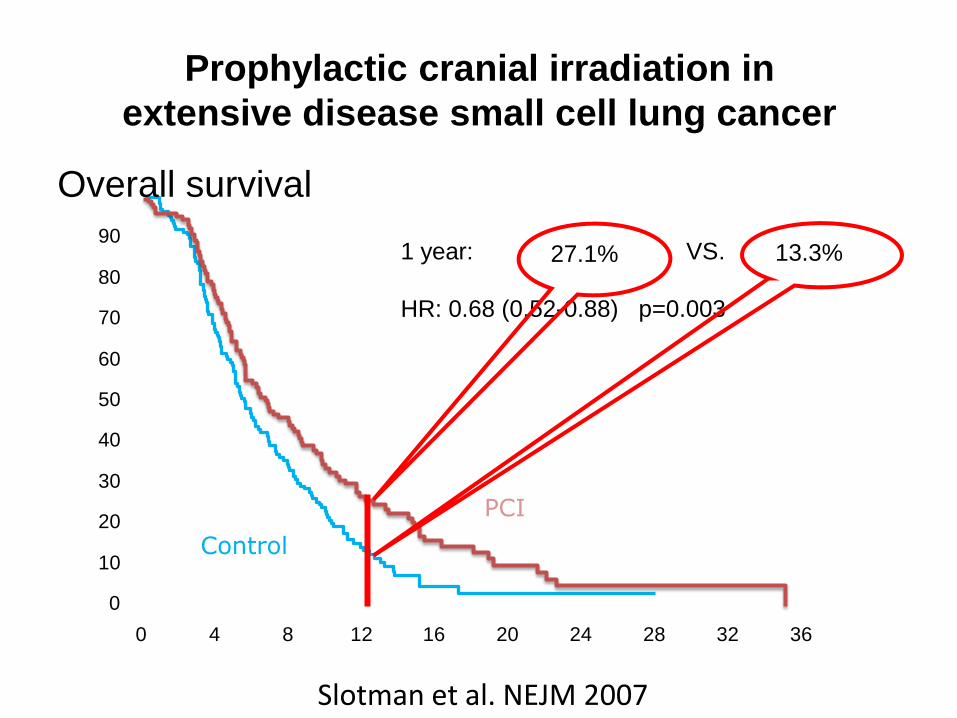
1 year: VS.
HR: 0.68 (0.52-0.88) p=0.003
Overall survival
Prophylactic cranial irradiation in
extensive disease small cell lung cancer
13.3% 27.1%
Slotman et al. NEJM 2007

6
Study Design
PCI
25 Gy in 10 fx
RT to
Chest and
Other Sites
Random Any response Chemotherapy
(4-6 cycles)
Phase II Study of PCI and consolidative
Extra-Cranial Radiation for ED-SCLC
RTOG 0937
Observation
PI: Elizabeth Gore, MD
Stratify:
PR vs CR
1 vs 2-3 mets

7
RTOG 0937 Specifics
• Primary Objective: To compare 1-year median survival
• Eligibility:
– ES-SCLC, excluding brain metastases AND
– Only 1-3 metastatic sites prior to platinum-based
chemotherapy AND
– Radiographic PR or CR
• Sample size = 154
• Radiation therapy dosing
– PCI given in 2.5 Gy fractions to 25 Gy
– Metastases dosing is 3 Gy fractions to 45 Gy
– Acceptable alternative is 4 Gy fractions to 40 Gy

8
RTOG Lung Committee
• Small Cell Lung Cancer
– Limited Stage (Intergroup Trial)
– Extensive Stage (RTOG 0937)
• Early Stage NSCLC
– In-operable
– Operable (RTOG 1021 / ACOSOG Z4099)
• Locally advanced NSCLC
– Stage IIIA with minimal N2 disease (0839)
– Stage IIIA with PET-adapted boost (1106)

9
Physical Targeting with SBRT
RTOG 0813
Phase I/II study of SBRT for early stage centrally located NSCLC in medically
inoperable pts

10
RTOG 0813 - SBRT Dose Levels
Level 5 10.0 Gy x 5 50.0. Gy
Level 6 10.5 Gy x 5 52.5 Gy
Level 7 11.0 Gy x 5 55.0 Gy
Level 8 11.5 Gy x 5 57.5 Gy
Level 9 12.0 Gy x 5 60.0 Gy

11
RTOG 0915-SBRT for early stage
medically inoperable lung cancer
12 Gy x 4
R
e
g
i
s
t
e
r
34 Gy X 1 Primary Endpoint
> grade 3 rates of Toxicity Respiratory
Soft tissue/chest wall
Skin
Secondary Endpoints
LC/OS/DFS
PET response
PFTs
Biomarkers
R
a
n
d
o
m
i
z
e
VS.
PI: Videtic
12 Gy X 4

12
• Medically Inoperable Early Stage NSCLC
RTOG SBRT Plan
Randomize III
SBRT 34 Gy X 1
SBRT 12Gy X4
SBRT (18 Gy X 3)
Altered Fx SBRT
Randomize II
RTOG 0915

13
Histological
confirmed
Stage I
NSCLC Registration
and
Randomization
ARM 1:
Sublobar
Resection ±
Brachytherapy
(SR)
ARM 2:
Stereotactic
Body
Radiation
Therapy
(SBRT) 18 Gy
X 3 = 54 Gy
F
O
L
L
O
W
U
P
ACOSOG Z4099/ RTOG 1021
H. Fernando, MD (ACOSOG);
R. Timmerman, MD (RTOG)
Activated June 2011
14
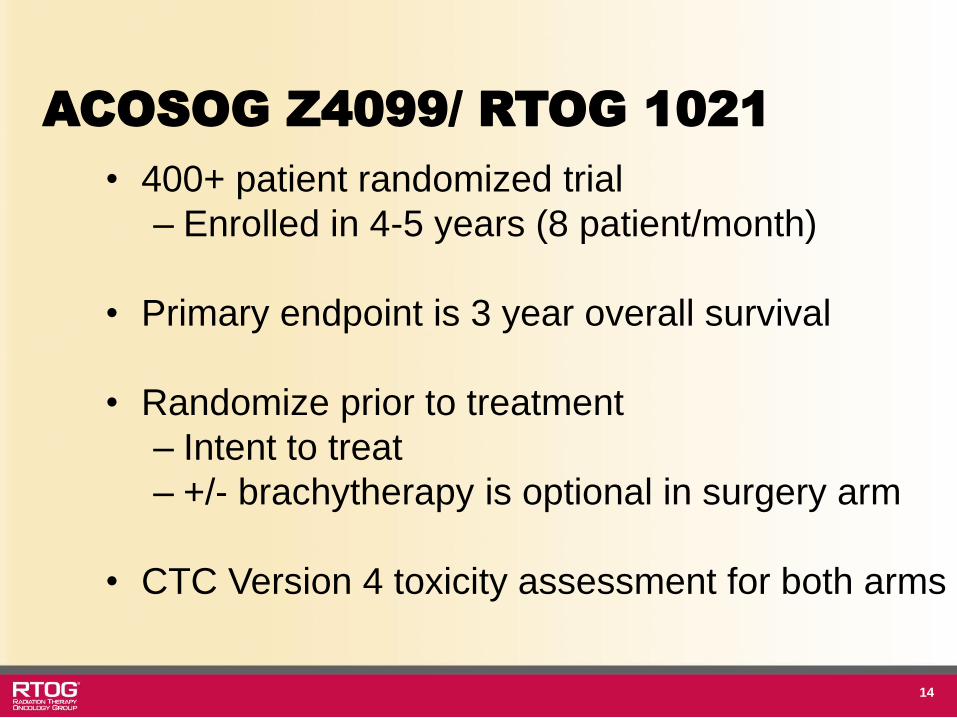
ACOSOG Z4099/ RTOG 1021
• 400+ patient randomized trial
– Enrolled in 4-5 years (8 patient/month)
• Primary endpoint is 3 year overall survival
• Randomize prior to treatment
– Intent to treat
– +/- brachytherapy is optional in surgery arm
• CTC Version 4 toxicity assessment for both arms

15
RTOG Lung Cancer Strategy
• Small Cell Lung Cancer
– Limited Stage
– Extensive Stage
• Early Stage NSCLC
– In-operable
– Operable
• Locally advanced NSCLC
– Stage IIIA with minimal disease
– Stage IIIA with PET-adapted boost

16
RTOG 0229: Phase II Trial of Concurrent Chemo and Full
Dose RT Followed by Surgical Resection and Consolidative
Tx for LA NSCLC
Induction Chemo-RT Paclitaxel and Carboplatin 1x/week for 6 weeks plus Concurrent RT to 61.2 Gy
Reassessment of Mediastinum: 4 weeks post Induction Chemoradiation
Resection Within 2 wks of Reassessment
Not Resectable
Consolidation Chemotherapy No later than 10 weeks post-surgery Pacilitaxel and Carboplatin q
21 days x 2
(Prophylactic Cranial Irradiation, if indicated)
17
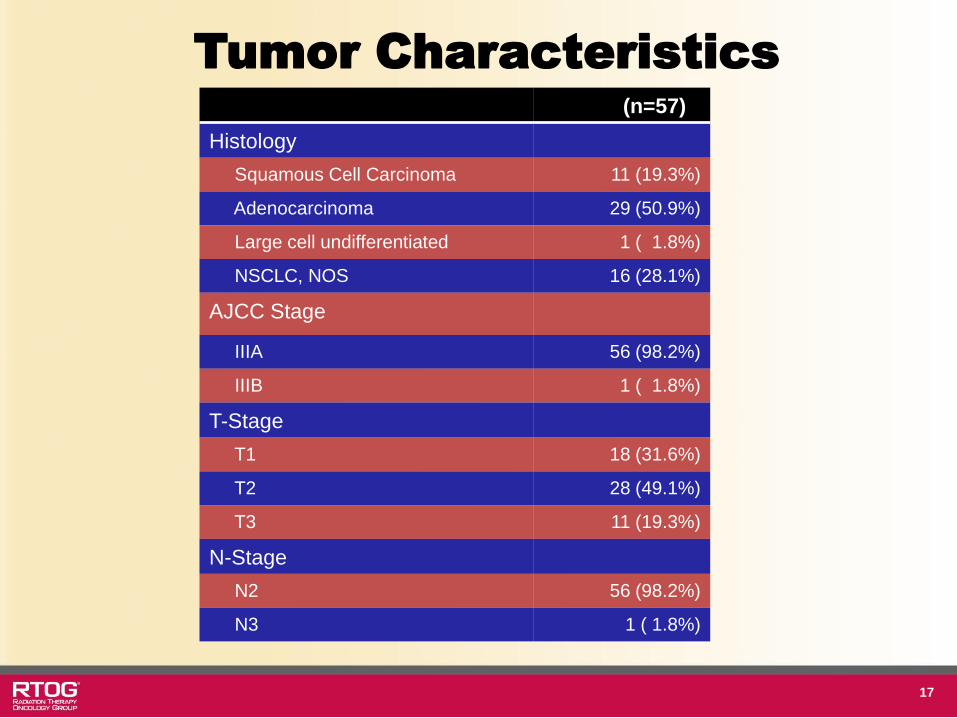
Tumor Characteristics
(n=57)
Histology
Squamous Cell Carcinoma 11 (19.3%)
Adenocarcinoma 29 (50.9%)
Large cell undifferentiated 1 ( 1.8%)
NSCLC, NOS 16 (28.1%)
AJCC Stage
IIIA 56 (98.2%)
IIIB 1 ( 1.8%)
T-Stage
T1 18 (31.6%)
T2 28 (49.1%)
T3 11 (19.3%)
N-Stage
N2 56 (98.2%)
N3 1 ( 1.8%)

18
Mediastinal Nodal Clearance
Residual Mediastinal Disease
Mediastinal nodal clearance
Patients Eligible for Assessment of Primary Endpoint
Surgery Performed
Reasons for No Surgery
Residual Mediastinal Nodes
Primary Unresectable
Medical contraindications
MD refusal
Died prior to Surgery
Progressive disease
Other
(N=43*)
16 (37%)
27 (63%)
43 Pts
37 pts
20 pts
6 pts
2 pts
5 pts
1 pt
1 pt
1 pt
4 pts

19
Survival
Time (Months)
Overall Survival
% Alive (95% Cl) # at Risk
Progression-Free Survival
%Alive (95% Cl) # at Risk
0
6
12
18
24
100% 57
87.7% (76.0, 93.9) 50
77.2% (64.0, 86.1) 43
66.4% (52.5, 77.1) 37
53.8% (40.0, 65.8) 29
100% 57
75.4% (62.1, 84.7) 43
50.8% (37.2, 62.9) 28
38.1% (25.6, 50.5) 21
32.7% (20.9, 45.0) 17
Fail/Total
Median
(95% Cl)
32/57
26.6 months
(18.5, ∞)
45/57
12.9 months
(8.0, 18.8)

20
Overall Survival by Mediastinal
Nodal Clearance Status
Time (Months)
No Mediastinal Nodal
Clearance
% Alive (95% Cl) # at Risk
Mediastinal Nodal
Clearance
% Alive (95% Cl) # at Risk
0
6
12
18
24
100 % 16
87.5% (58.6, 96.7) 14
81.3% (52.5, 93.5) 12
60.9% (32.7, 80.3) 9
54.2% (27.1, 75.0) 8
100% 27
100% 27
92.6% (73.5, 98.1) 25
81.5% (61.1, 91.8) 22
66.7% (45.7, 81.1) 17
Fail/Total
Median Survival
Time (95% Cl)
8/16
32.7 months (13.8, ∞)
12/27
Not Reached
21
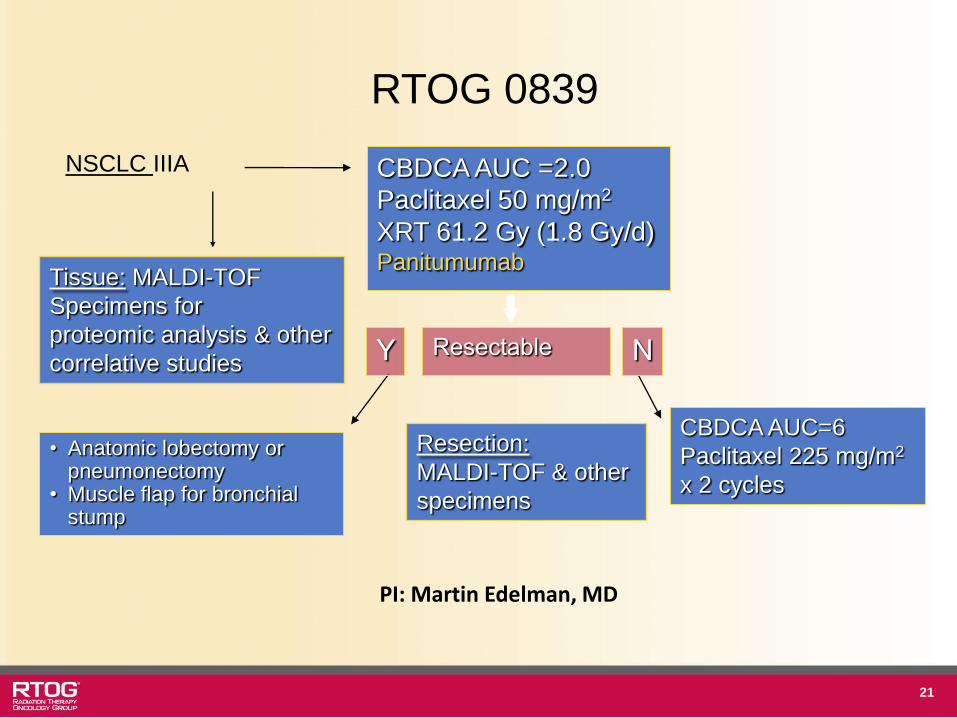
NSCLC IIIA CBDCA AUC =2.0
Paclitaxel 50 mg/m2
XRT 61.2 Gy (1.8 Gy/d) Panitumumab
Resectable Y N
• Anatomic lobectomy or pneumonectomy
• Muscle flap for bronchial stump
CBDCA AUC=6
Paclitaxel 225 mg/m2
x 2 cycles
Tissue: MALDI-TOF
Specimens for
proteomic analysis & other
correlative studies
Resection:
MALDI-TOF & other
specimens
RTOG 0839
PI: Martin Edelman, MD
22
Thinking newer strategies
• Personalized medicine – AM4/ALK and EGFR mutation trial
– Wild-type (non mutant) trial
• Adaptive XRT (RTOG 1106) – Mid-treatment FDG-PET based target volumes
adapted radiation therapy
– Isoeffect radiation dose prescriptions
– Why? • PET tumor volumes shrink during XRT
• May incorporate all Stage III patients, not just those selected to get 74 Gy based on NTCP

23
RTOG 1210/ Alliance 31101
Submitted to NCI 7/12
Stage III NSCLC With either EGFR TK mutation or ALK Fusion
ALK Fusion +: Crizotinib 3 months
A Randomized Phase II Trial
EGFR Mutation + Erlotinib 3 months followed by
ChemoRT* Alk Fusion +
Crizotinib 3 months followed by ChemoRT*
*Pemetrexed 500 mg/m2 q 3 weekly x 4 Carboplatin AUC 5 (4 cycles) with Thoracic Radiation 64 Gy
EGFR Mutation+/Alk Fusion+ ChemoRT* ONLY
Experimental
Control

24
PET-based Adaptive RT for Stage III
NSCLC
RTOG 1106: Just Activated!!
R E G I S T E R
ChemoRT 44 Gy FDG-PET
SD/Response
PD
FDG-PET
Off Study – D/C RT
RT to 64 Gy
R A N D O M I Z E
RT to 64 Gy + 10+ Gy boost based on FDG-PET

Tumor Volume Reduced During-RT
(UMCC 2003-76, UMCC 2006-040)
Change in PET-MTV
04080
120160200240280320360400
Pre-RT During-RT Post-RT
PE
T-M
TV
(cc)
Change in CT-GTV
0
50
100
150
200
250
300
350
400
450
500
Pre-RT During-RT Post-RT
CT
-GT
V (
cc)
020406080
100120140160180200
PE
T-M
TV
(%
)
Pre-RT During-RT Post-RT
Change in PET-MTV based on Pre-RT Change in CT-GTV based on Pre-RT
0
25
50
75
100
125
150
175
200
225
250
Pre-RT During-RT Post-RT
CT
-GT
V (
%)

During-RT PET-CT adapted composite plan: 17.2% lung NTCP~ 86 Gy to during-RT PET-PTV
(102 ED2 lung, ~92 Gy ED2 tumor, ~120 Gy BED for a/b=10).
Pre-RT PET-CT based plan: 17.2% lung NTCP~ 70 Gy
9.8% NTCP ~ 50 Gy
Pre-RT
During-RT

RTOG 0617 (CALGB, NCCTG)
Phase III Trial of Standard-Dose (60 Gy) Versus High-Dose
(74 Gy) Conformal RT w Concurrent & Consolidation Cb/P
in Stage III NSCLC
Primary Endpoint – Survival (n=512)
Stage IIIA/B
PS 0-1
FEV1 ≥1.5L; V20 <37%
No Supraclav LNs
PET recommended
R
A
N
D
O
M
I
Z
E
Concurrent ChemoRT Paclitaxel 45 mg/m2 Carboplatin AUC 2 Weekly x7
RT 60 Gy (2 Gy/d)
+ Cetuximab
Concurrent ChemoRT Paclitaxel 45 mg/m2 Carboplatin AUC 2 Weekly x7
RT 74 Gy (2 Gy/d)
+ Cetuximab
Consolidation Paclitaxel 200mg/m2 Carboplatin AUC 6 q3wks x2 cycles

28
Research RFP for RTOG 0617
RTOG 0617
512 Pts Enrolled
Banked Specimens on 50%
Formal RFP for Translational Proposals
IALSC and ASTRO broadcast
25 Applicants
External Peer Review Ongoing

29
RTOG Lung Committee Future
NRG Oncology
Will Have 7 Disease Site Committees
Lung Cancer Committee will be One
HQ in Philadelphia
Lung Cancer Biobanking at UCSF
Seeking Links with SPORES/P30/P01’s