role of telemedicine in rop screening in rural india sfnm.pdf
TRANSCRIPT

lable at ScienceDirect
Seminars in Fetal & Neonatal Medicine xxx (2015) 1e11
Contents lists avai
Seminars in Fetal & Neonatal Medicine
journal homepage: www.elsevier .com/locate/s iny
Review
Role of tele-medicine in retinopathy of prematurity screening in ruraloutreach centers in India e A report of 20,214 imaging sessions in theKIDROP program
Anand Vinekar a, *, Chaitra Jayadev a, Shwetha Mangalesh a, b, Bhujang Shetty a,Dharmapuri Vidyasagar c, d
a Narayana Nethralaya Postgraduate Institute of Ophthalmology, Bangalore, Indiab Duke University, Durham, NC, USAc University of Illinois, Chicago, IL, USAd M.S. Ramaiah Medical College, Bangalore, India
Keywords:Retinopathy of prematurityRuralOutreachScreeningLaserTelemedicineIndia
* Corresponding author. Address: Narayana NethraOphthalmology, Bangalore, India. Fax: þ91 80 233773
E-mail address: [email protected] (A. Vin
http://dx.doi.org/10.1016/j.siny.2015.05.0021744-165X/© 2015 Elsevier Ltd. All rights reserved.
Please cite this article in press as: Vinekar AIndia e A report of 20,214 imaging sessionsj.siny.2015.05.002
s u m m a r y
Middle-income countries such as India are suffering from the third epidemic of retinopathy of prema-turity (ROP). Improved survival and lower infant mortality rates have resulted in an increased number ofpreterm survivors in rural areas that unfortunately lack ROP specialists. We report our experience of apubliceprivate partnership in rural India of an ongoing telemedicine program Karnataka InternetAssisted Diagnosis of Retinopathy of Prematurity program KIDROP that provides ROP screening by non-physicians. The analysis of 20,214 imaging sessions of 7106 from 36 rural centers in 77 months of activityare presented. The overall incidence of any stage and treatment requiring ROP was 22.39% and 3.57%respectively. We found a higher incidence of severe ROP in private (7.1%) vs government centers (1.7%).Fifty of the 254 babies (19.69%) who underwent treatment were outside the American screeningguidelines cut-off. The report compares other “real-world” tele-ROP programs, summarizes the impact,and provides future strategies for outreach ROP screening in middle-income countries.
© 2015 Elsevier Ltd. All rights reserved.
1. Introduction
Retinopathy of prematurity (ROP) is one of the leading causes ofpreventable infant blindness worldwide [1,2]. Since the 1990s thefocus of ROP as a public health problem has shifted from theindustrialized world to middle-income nations [1,2]. Countrieswith improving economies and standard of living have also shownrapid improvement in the survival of their infants. Infant mortalityrates in India have fallen in the past two decades resulting inincreased numbers of survivors, even in the rural areas. Withdecreasing mortality, emphasis on “intact survival” is now the newbenchmark of neonatal quality of life in government-based childhealth programs [3,4]. Despite this, factors such as a high birth rate,declining infant mortality, improved survival of low-birth-weightbabies, and lack of uniform neonatal care increase the
laya Postgraduate Institute of29.ekar).
, et al., Role of tele-medicinein the KIDROP program, Sem
vulnerability of these babies to unscreened ROP blindness in ruralareas [5,6]. If detected on time, ROP blindness is largely preventableand has thus gained public importance in countries such as India,which have mandated ROP and universal screening [3]. Yet, theoperational guidelines and road map remain incomplete and theinfrastructure to execute these services remains grossly inadequate.
Countries such as India and China together account for morethan half of the total number of premature infants born, with Indiaalone accounting for 3.5 million preterm infants annually [4].Whereas the incidence of ROP in India varies from 38% to 52% of“at-risk” babies in urban areas [7e13], rural ROP has recently beenreported to be comparable [14e16]. The incidence of treatable ROPis ~5e10% and this accounts for >60,000 infants annually who mayprogress to treatment requiring disease in India alone [17]. With<100 ROP specialists, most of whom practice in the cities, the vastmajority of rural preterm infants remain unscreened, or arescreened too latewhen they present with stage 5 disease to tertiarycare centers in larger cities [18].
The Karnataka Internet Assisted Diagnosis of Retinopathy ofPrematurity program (KIDROP) is a telemedicine project initiated in
in retinopathy of prematurity screening in rural outreach centers ininars in Fetal & Neonatal Medicine (2015), http://dx.doi.org/10.1016/
A. Vinekar et al. / Seminars in Fetal & Neonatal Medicine xxx (2015) 1e112
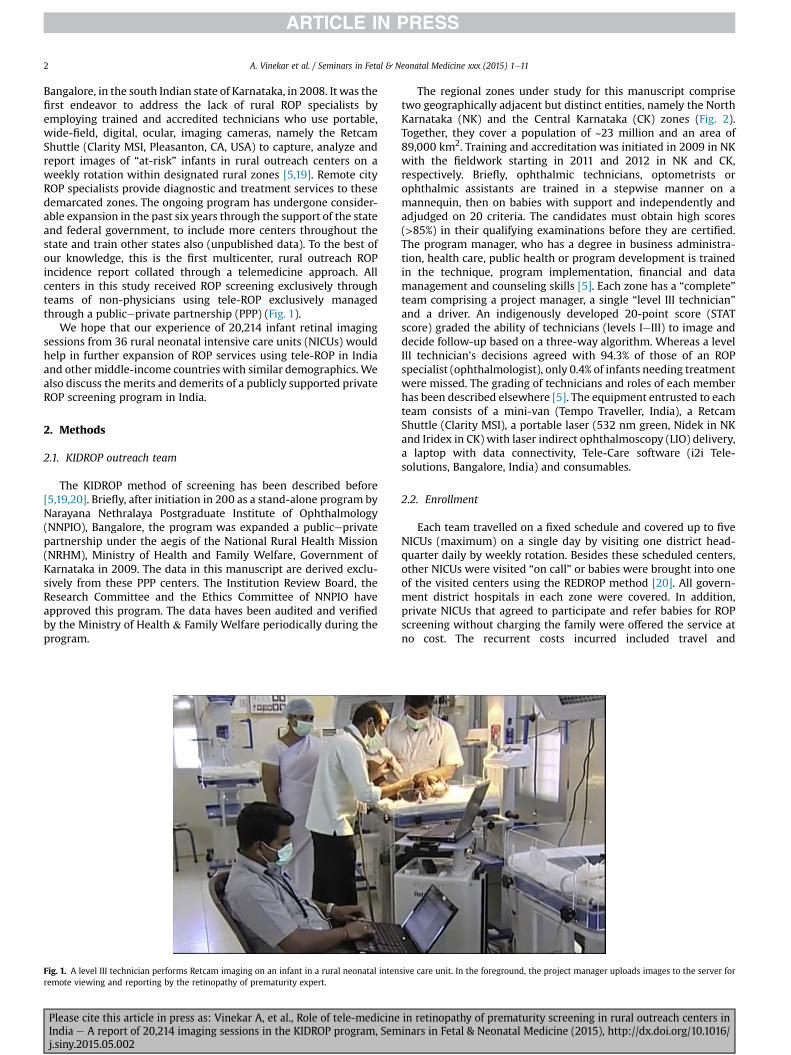
Bangalore, in the south Indian state of Karnataka, in 2008. It was thefirst endeavor to address the lack of rural ROP specialists byemploying trained and accredited technicians who use portable,wide-field, digital, ocular, imaging cameras, namely the RetcamShuttle (Clarity MSI, Pleasanton, CA, USA) to capture, analyze andreport images of “at-risk” infants in rural outreach centers on aweekly rotation within designated rural zones [5,19]. Remote cityROP specialists provide diagnostic and treatment services to thesedemarcated zones. The ongoing program has undergone consider-able expansion in the past six years through the support of the stateand federal government, to include more centers throughout thestate and train other states also (unpublished data). To the best ofour knowledge, this is the first multicenter, rural outreach ROPincidence report collated through a telemedicine approach. Allcenters in this study received ROP screening exclusively throughteams of non-physicians using tele-ROP exclusively managedthrough a publiceprivate partnership (PPP) (Fig. 1).
We hope that our experience of 20,214 infant retinal imagingsessions from 36 rural neonatal intensive care units (NICUs) wouldhelp in further expansion of ROP services using tele-ROP in Indiaand other middle-income countries with similar demographics. Wealso discuss the merits and demerits of a publicly supported privateROP screening program in India.
2. Methods
2.1. KIDROP outreach team
The KIDROP method of screening has been described before[5,19,20]. Briefly, after initiation in 200 as a stand-alone program byNarayana Nethralaya Postgraduate Institute of Ophthalmology(NNPIO), Bangalore, the program was expanded a publiceprivatepartnership under the aegis of the National Rural Health Mission(NRHM), Ministry of Health and Family Welfare, Government ofKarnataka in 2009. The data in this manuscript are derived exclu-sively from these PPP centers. The Institution Review Board, theResearch Committee and the Ethics Committee of NNPIO haveapproved this program. The data haves been audited and verifiedby the Ministry of Health & Family Welfare periodically during theprogram.
Fig. 1. A level III technician performs Retcam imaging on an infant in a rural neonatal intenremote viewing and reporting by the retinopathy of prematurity expert.
Please cite this article in press as: Vinekar A, et al., Role of tele-medicineIndia e A report of 20,214 imaging sessions in the KIDROP program, Semj.siny.2015.05.002
The regional zones under study for this manuscript comprisetwo geographically adjacent but distinct entities, namely the NorthKarnataka (NK) and the Central Karnataka (CK) zones (Fig. 2).Together, they cover a population of ~23 million and an area of89,000 km2. Training and accreditation was initiated in 2009 in NKwith the fieldwork starting in 2011 and 2012 in NK and CK,respectively. Briefly, ophthalmic technicians, optometrists orophthalmic assistants are trained in a stepwise manner on amannequin, then on babies with support and independently andadjudged on 20 criteria. The candidates must obtain high scores(>85%) in their qualifying examinations before they are certified.The program manager, who has a degree in business administra-tion, health care, public health or program development is trainedin the technique, program implementation, financial and datamanagement and counseling skills [5]. Each zone has a “complete”team comprising a project manager, a single “level III technician”and a driver. An indigenously developed 20-point score (STATscore) graded the ability of technicians (levels IeIII) to image anddecide follow-up based on a three-way algorithm. Whereas a levelIII technician's decisions agreed with 94.3% of those of an ROPspecialist (ophthalmologist), only 0.4% of infants needing treatmentwere missed. The grading of technicians and roles of each memberhas been described elsewhere [5]. The equipment entrusted to eachteam consists of a mini-van (Tempo Traveller, India), a RetcamShuttle (Clarity MSI), a portable laser (532 nm green, Nidek in NKand Iridex in CK) with laser indirect ophthalmoscopy (LIO) delivery,a laptop with data connectivity, Tele-Care software (i2i Tele-solutions, Bangalore, India) and consumables.
2.2. Enrollment
Each team travelled on a fixed schedule and covered up to fiveNICUs (maximum) on a single day by visiting one district head-quarter daily by weekly rotation. Besides these scheduled centers,other NICUs were visited “on call” or babies were brought into oneof the visited centers using the REDROP method [20]. All govern-ment district hospitals in each zone were covered. In addition,private NICUs that agreed to participate and refer babies for ROPscreening without charging the family were offered the service atno cost. The recurrent costs incurred included travel and
sive care unit. In the foreground, the project manager uploads images to the server for
in retinopathy of prematurity screening in rural outreach centers ininars in Fetal & Neonatal Medicine (2015), http://dx.doi.org/10.1016/
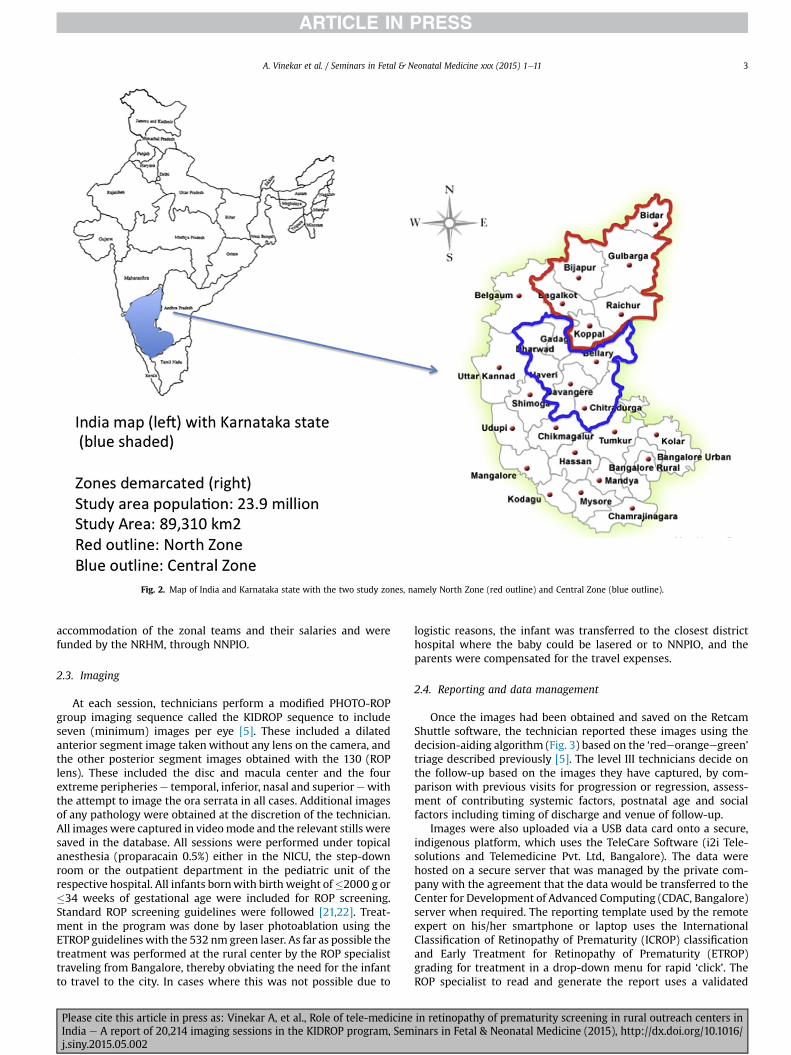
Fig. 2. Map of India and Karnataka state with the two study zones, namely North Zone (red outline) and Central Zone (blue outline).
A. Vinekar et al. / Seminars in Fetal & Neonatal Medicine xxx (2015) 1e11 3
accommodation of the zonal teams and their salaries and werefunded by the NRHM, through NNPIO.
2.3. Imaging
At each session, technicians perform a modified PHOTO-ROPgroup imaging sequence called the KIDROP sequence to includeseven (minimum) images per eye [5]. These included a dilatedanterior segment image taken without any lens on the camera, andthe other posterior segment images obtained with the 130 (ROPlens). These included the disc and macula center and the fourextreme peripheriese temporal, inferior, nasal and superiorewiththe attempt to image the ora serrata in all cases. Additional imagesof any pathology were obtained at the discretion of the technician.All images were captured in videomode and the relevant stills weresaved in the database. All sessions were performed under topicalanesthesia (proparacain 0.5%) either in the NICU, the step-downroom or the outpatient department in the pediatric unit of therespective hospital. All infants bornwith birth weight of�2000 g or�34 weeks of gestational age were included for ROP screening.Standard ROP screening guidelines were followed [21,22]. Treat-ment in the program was done by laser photoablation using theETROP guidelines with the 532 nm green laser. As far as possible thetreatment was performed at the rural center by the ROP specialisttraveling from Bangalore, thereby obviating the need for the infantto travel to the city. In cases where this was not possible due to
Please cite this article in press as: Vinekar A, et al., Role of tele-medicineIndia e A report of 20,214 imaging sessions in the KIDROP program, Semj.siny.2015.05.002
logistic reasons, the infant was transferred to the closest districthospital where the baby could be lasered or to NNPIO, and theparents were compensated for the travel expenses.
2.4. Reporting and data management
Once the images had been obtained and saved on the RetcamShuttle software, the technician reported these images using thedecision-aiding algorithm (Fig. 3) based on the ‘redeorangeegreen’triage described previously [5]. The level III technicians decide onthe follow-up based on the images they have captured, by com-parison with previous visits for progression or regression, assess-ment of contributing systemic factors, postnatal age and socialfactors including timing of discharge and venue of follow-up.
Images were also uploaded via a USB data card onto a secure,indigenous platform, which uses the TeleCare Software (i2i Tele-solutions and Telemedicine Pvt. Ltd, Bangalore). The data werehosted on a secure server that was managed by the private com-pany with the agreement that the data would be transferred to theCenter for Development of Advanced Computing (CDAC, Bangalore)server when required. The reporting template used by the remoteexpert on his/her smartphone or laptop uses the InternationalClassification of Retinopathy of Prematurity (ICROP) classificationand Early Treatment for Retinopathy of Prematurity (ETROP)grading for treatment in a drop-down menu for rapid ‘click’. TheROP specialist to read and generate the report uses a validated
in retinopathy of prematurity screening in rural outreach centers ininars in Fetal & Neonatal Medicine (2015), http://dx.doi.org/10.1016/
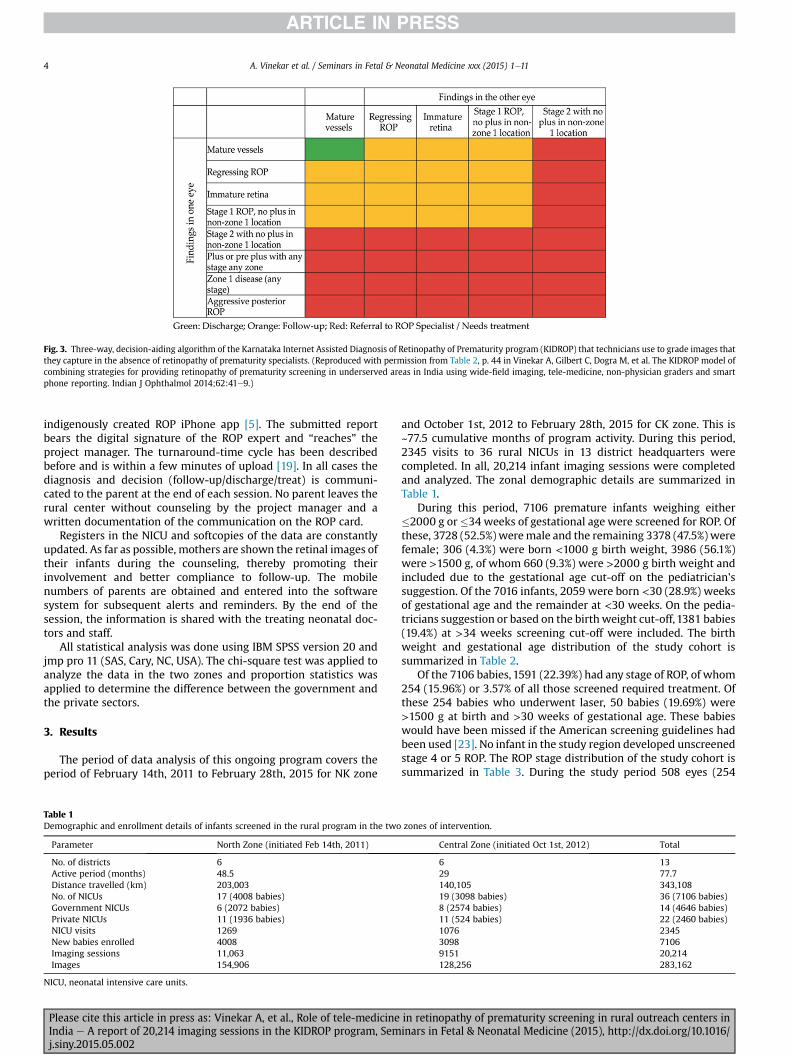
Fig. 3. Three-way, decision-aiding algorithm of the Karnataka Internet Assisted Diagnosis of Retinopathy of Prematurity program (KIDROP) that technicians use to grade images thatthey capture in the absence of retinopathy of prematurity specialists. (Reproduced with permission from Table 2, p. 44 in Vinekar A, Gilbert C, Dogra M, et al. The KIDROP model ofcombining strategies for providing retinopathy of prematurity screening in underserved areas in India using wide-field imaging, tele-medicine, non-physician graders and smartphone reporting. Indian J Ophthalmol 2014;62:41e9.)
A. Vinekar et al. / Seminars in Fetal & Neonatal Medicine xxx (2015) 1e114
indigenously created ROP iPhone app [5]. The submitted reportbears the digital signature of the ROP expert and “reaches” theproject manager. The turnaround-time cycle has been describedbefore and is within a few minutes of upload [19]. In all cases thediagnosis and decision (follow-up/discharge/treat) is communi-cated to the parent at the end of each session. No parent leaves therural center without counseling by the project manager and awritten documentation of the communication on the ROP card.
Registers in the NICU and softcopies of the data are constantlyupdated. As far as possible, mothers are shown the retinal images oftheir infants during the counseling, thereby promoting theirinvolvement and better compliance to follow-up. The mobilenumbers of parents are obtained and entered into the softwaresystem for subsequent alerts and reminders. By the end of thesession, the information is shared with the treating neonatal doc-tors and staff.
All statistical analysis was done using IBM SPSS version 20 andjmp pro 11 (SAS, Cary, NC, USA). The chi-square test was applied toanalyze the data in the two zones and proportion statistics wasapplied to determine the difference between the government andthe private sectors.
3. Results
The period of data analysis of this ongoing program covers theperiod of February 14th, 2011 to February 28th, 2015 for NK zone
Table 1Demographic and enrollment details of infants screened in the rural program in the two
Parameter North Zone (initiated Feb 14th, 2011)
No. of districts 6Active period (months) 48.5Distance travelled (km) 203,003No. of NICUs 17 (4008 babies)Government NICUs 6 (2072 babies)Private NICUs 11 (1936 babies)NICU visits 1269New babies enrolled 4008Imaging sessions 11,063Images 154,906
NICU, neonatal intensive care units.
Please cite this article in press as: Vinekar A, et al., Role of tele-medicineIndia e A report of 20,214 imaging sessions in the KIDROP program, Semj.siny.2015.05.002
and October 1st, 2012 to February 28th, 2015 for CK zone. This is~77.5 cumulative months of program activity. During this period,2345 visits to 36 rural NICUs in 13 district headquarters werecompleted. In all, 20,214 infant imaging sessions were completedand analyzed. The zonal demographic details are summarized inTable 1.
During this period, 7106 premature infants weighing either�2000 g or�34 weeks of gestational age were screened for ROP. Ofthese, 3728 (52.5%) weremale and the remaining 3378 (47.5%) werefemale; 306 (4.3%) were born <1000 g birth weight, 3986 (56.1%)were >1500 g, of whom 660 (9.3%) were >2000 g birth weight andincluded due to the gestational age cut-off on the pediatrician'ssuggestion. Of the 7016 infants, 2059 were born <30 (28.9%) weeksof gestational age and the remainder at <30 weeks. On the pedia-tricians suggestion or based on the birth weight cut-off, 1381 babies(19.4%) at >34 weeks screening cut-off were included. The birthweight and gestational age distribution of the study cohort issummarized in Table 2.
Of the 7106 babies, 1591 (22.39%) had any stage of ROP, of whom254 (15.96%) or 3.57% of all those screened required treatment. Ofthese 254 babies who underwent laser, 50 babies (19.69%) were>1500 g at birth and >30 weeks of gestational age. These babieswould have been missed if the American screening guidelines hadbeen used [23]. No infant in the study region developed unscreenedstage 4 or 5 ROP. The ROP stage distribution of the study cohort issummarized in Table 3. During the study period 508 eyes (254
zones of intervention.
Central Zone (initiated Oct 1st, 2012) Total
6 1329 77.7140,105 343,10819 (3098 babies) 36 (7106 babies)8 (2574 babies) 14 (4646 babies)11 (524 babies) 22 (2460 babies)1076 23453098 71069151 20,214128,256 283,162
in retinopathy of prematurity screening in rural outreach centers ininars in Fetal & Neonatal Medicine (2015), http://dx.doi.org/10.1016/
Table 2Birth weight and gestational age distribution of the study cohort (n ¼ 7106 infants).
Parameter North Zone Central Zone Total
No. of babies 4008 3098 7106Sex (M:F) 2177:1831 1551:1547 P < 0.001Birth weight (% of all babies, n ¼ 7106)�1000 g 168 138 306 (4.3%)1001e1500 g 1619 1195 2814 (39.6%)1501e1750 g 969 787 1756 (24.71%)1751e2000 g 832 738 1570 (22.09%)�2001 g 420 240 660 (9.3%)
Gestational age (% of all babies, n ¼ 7106)�30 weeks 1134 925 2059 (28.98%)31e32 weeks 941 844 1785 (25.12%)33e34 week 1002 879 1881 (26.47%)�35 weeks 931 450 1381 (19.43%)
Table 3Retinopathy of prematurity (ROP) stage distribution of the study cohort (n ¼ 7106infants).
Parameter North Zone(n ¼ 4008)
Central Zone(n ¼ 3098)
Total(n ¼ 7106)
No ROP 3026 (75.5%) 2489 (80.34%) 5515 (77.61%)Any stage ROP 982 (24.5%) 609 (19.66%) 1591 (22.39%)Treated ROP 181 (4.52%) 73 (2.36%) 254 (3.57%)ROP stage distribution (% of all ROP)Stage 1 378 127 505 (31.74%)Stage 2 493 463 956 (60.1%)Stage 2 with plus 10 0 10 (0.63%)Stage 3 65 17 82 (5.13%)Stage 4 0 0 0Stage 5 0 0 0
APROP 32 6 38 (2.4%)
APROP, aggressive posterior retinopathy of prematurity.
A. Vinekar et al. / Seminars in Fetal & Neonatal Medicine xxx (2015) 1e11 5
babies) underwent primary laser. Of these, three babies (six eyes)were lost to follow-up before complete regression could be docu-mented, one baby progressed to stage 5 ROP in one eye followingtreatment, and two babies had unfavorable outcome in both eyesfollowing laser treatment. Thus, 11 eyes had unfavorable outcomesand the remaining 497 eyes had favorable structural outcomesaccounting for 97.83%.
Table 4Government vs private center comparison of study cohort.
Parameter Government centers
Centers 14Visits 1328Sessions 12,175New babies 4646Male:female 2329:2317Birth weight (g)<1000 2061001e1500 18041501e1750 11531751e2000 1114�2001 369
Gestational age (weeks)<30 130931e32 111233e34 1279�35 946
ROP stagesAll stages 770Any stage ROP 770/4646 (16.57%)Treatment requiring ROP (%) 79/4646 (1.7%)Proportion of treatment requiring ROP to all ROP 79/770 (10.23%)
ROP, retinopathy of prematurity.
Please cite this article in press as: Vinekar A, et al., Role of tele-medicineIndia e A report of 20,214 imaging sessions in the KIDROP program, Semj.siny.2015.05.002
3.1. Comparison of experience in government vs private centers
We performed a sub-analysis to compare the distribution andoutcome between the government and private centers. Of the 36NICUs, 14 (38.9%) were government and the remaining 22 (61.1%)were private hospitals. There were more visits to the governmentcenters than the private hospitals (1328 vs 1017). The governmentcenters always had patients for screening or review and hencewerevisitedmore frequently, whichwas not the case in private hospitals,which scheduled appointments for both screenings and reviews.This also translated to higher new enrollments from the govern-ment compared to private centers (4646 vs 2460 respectively,P < 0.001). A greater proportion of males were screened in privatehospitals compared to the government centers (private, mal-e:female 1.32 vs government, male:female 1.00; P < 0.001). Thesmallest birth weights (<1000 g) and the lowest gestational age(<30 weeks) were screened in the government centers (67.3% and63.6% respectively, P < 0.001). The incidence of ROP (all stages) was16.57% (770/4646) in the government compared to 33.38% in theprivate centers (P < 0.001). The incidence of treatment requiringdisease of all those screened was also more in the private centerscompared to the government centers (7.11% vs 1.7% respectively,P < 0.001) and more infants with the disease progressed to treat-ment requiring ROP in private compared to the government babies(21.32% vs 10.23% respectively, P < 0.001). The details of this sub-analysis are represented in Table 4.
4. Discussion
The World Health Organization's “Born too soon” report hasshifted the focus of care of premature infants from industrializedcountries to middle-income nations such as India, which currentlyleads the order of countries with the highest burden of prematurity[4]. Unfortunately, ROP screening programs have not been able tokeep up with improving neonatal care practices and remainedgrossly inadequate. In India today, there are very few ROP spe-cialists and they only cater to a handful of NICUs in the main cities,exposing the vast majority of unscreened rural Indian prematureinfants to a risk of ROP-related blindness.
Thus far, indirect ophthalmoscopy (IO) has been considered thegold standard in ROP screening. It assumes competency of the
Private centers Total P-value
22 361017 2345 <0.0018038 20,214 <0.0012460 71061399:1061 <0.001
100 306 <0.0011010 2814603 1756456 1570291 660 0.0024
750 2059 <0.001673 1785602 1881435 1381
821 1591821/2460 (33.38%) 1591/7106 (22.4%) <0.001175/2460 (7.11%) 254/7106 (3.57%) <0.001175/821 (21.32%) 254/1591 (15.96%) <0.001
in retinopathy of prematurity screening in rural outreach centers ininars in Fetal & Neonatal Medicine (2015), http://dx.doi.org/10.1016/
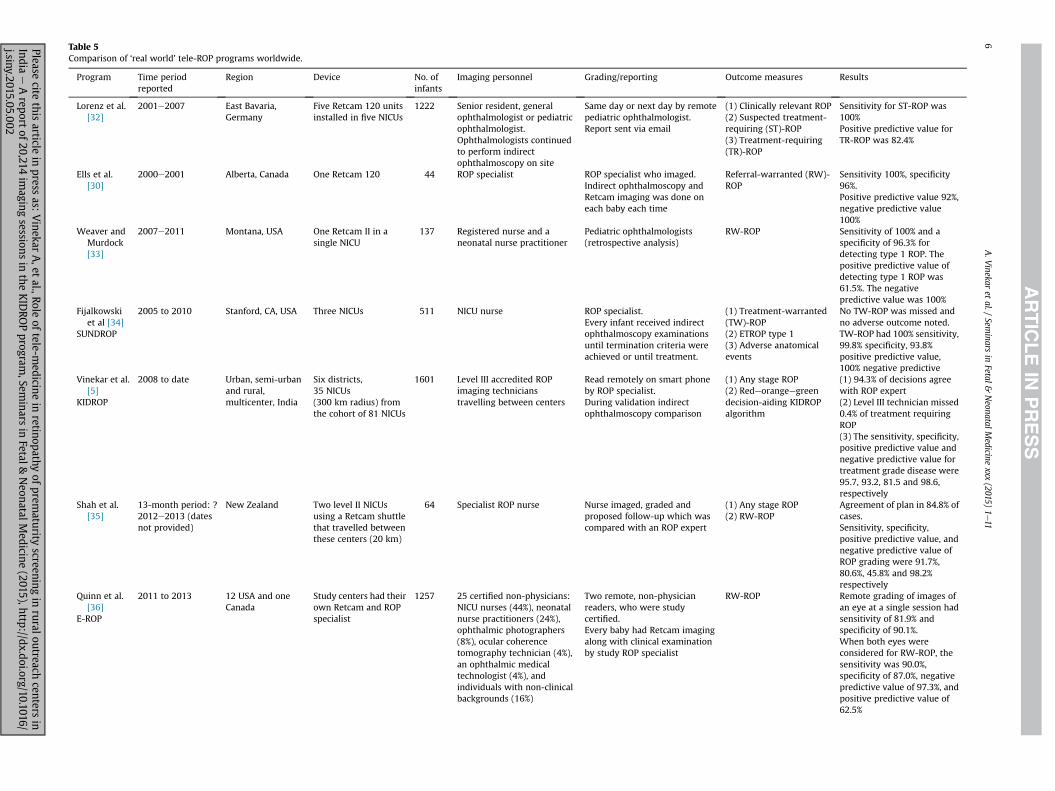
Table 5Comparison of ‘real world’ tele-ROP programs worldwide.
Program Time periodreported
Region Device No. ofinfants
Imaging personnel Grading/reporting Outcome measures Results
Lorenz et al.[32]
2001e2007 East Bavaria,Germany
Five Retcam 120 unitsinstalled in five NICUs
1222 Senior resident, generalophthalmologist or pediatricophthalmologist.Ophthalmologists continuedto perform indirectophthalmoscopy on site
Same day or next day by remotepediatric ophthalmologist.Report sent via email
(1) Clinically relevant ROP(2) Suspected treatment-requiring (ST)-ROP(3) Treatment-requiring(TR)-ROP
Sensitivity for ST-ROP was100%Positive predictive value forTR-ROP was 82.4%
Ells et al.[30]
2000e2001 Alberta, Canada One Retcam 120 44 ROP specialist ROP specialist who imaged.Indirect ophthalmoscopy andRetcam imaging was done oneach baby each time
Referral-warranted (RW)-ROP
Sensitivity 100%, specificity96%.Positive predictive value 92%,negative predictive value100%
Weaver andMurdock[33]
2007e2011 Montana, USA One Retcam II in asingle NICU
137 Registered nurse and aneonatal nurse practitioner
Pediatric ophthalmologists(retrospective analysis)
RW-ROP Sensitivity of 100% and aspecificity of 96.3% fordetecting type 1 ROP. Thepositive predictive value ofdetecting type 1 ROP was61.5%. The negativepredictive value was 100%
Fijalkowskiet al [34]
SUNDROP
2005 to 2010 Stanford, CA, USA Three NICUs 511 NICU nurse ROP specialist.Every infant received indirectophthalmoscopy examinationsuntil termination criteria wereachieved or until treatment.
(1) Treatment-warranted(TW)-ROP(2) ETROP type 1(3) Adverse anatomicalevents
No TW-ROP was missed andno adverse outcome noted.TW-ROP had 100% sensitivity,99.8% specificity, 93.8%positive predictive value,100% negative predictive
Vinekar et al.[5]
KIDROP
2008 to date Urban, semi-urbanand rural,multicenter, India
Six districts,35 NICUs(300 km radius) fromthe cohort of 81 NICUs
1601 Level III accredited ROPimaging technicianstravelling between centers
Read remotely on smart phoneby ROP specialist.During validation indirectophthalmoscopy comparison
(1) Any stage ROP(2) Redeorangeegreendecision-aiding KIDROPalgorithm
(1) 94.3% of decisions agreewith ROP expert(2) Level III technician missed0.4% of treatment requiringROP(3) The sensitivity, specificity,positive predictive value andnegative predictive value fortreatment grade disease were95.7, 93.2, 81.5 and 98.6,respectively
Shah et al.[35]
13-month period: ?2012e2013 (datesnot provided)
New Zealand Two level II NICUsusing a Retcam shuttlethat travelled betweenthese centers (20 km)
64 Specialist ROP nurse Nurse imaged, graded andproposed follow-up which wascompared with an ROP expert
(1) Any stage ROP(2) RW-ROP
Agreement of plan in 84.8% ofcases.Sensitivity, specificity,positive predictive value, andnegative predictive value ofROP grading were 91.7%,80.6%, 45.8% and 98.2%respectively
Quinn et al.[36]
E-ROP
2011 to 2013 12 USA and oneCanada
Study centers had theirown Retcam and ROPspecialist
1257 25 certified non-physicians:NICU nurses (44%), neonatalnurse practitioners (24%),ophthalmic photographers(8%), ocular coherencetomography technician (4%),an ophthalmic medicaltechnologist (4%), andindividuals with non-clinicalbackgrounds (16%)
Two remote, non-physicianreaders, who were studycertified.Every baby had Retcam imagingalong with clinical examinationby study ROP specialist
RW-ROP Remote grading of images ofan eye at a single session hadsensitivity of 81.9% andspecificity of 90.1%.When both eyes wereconsidered for RW-ROP, thesensitivity was 90.0%,specificity of 87.0%, negativepredictive value of 97.3%, andpositive predictive value of62.5%
A.V
inekaret
al./Sem
inarsin
Fetal&
NeonatalM
edicinexxx
(2015)1e11
6Pleasecite
thisarticle
inpress
as:Vinekar
A,et
al.,Roleof
tele-medicine
inretinopathy
ofprem
aturityscreening
inruraloutreach
centersin
Indiae
Areport
of20,214im
agingsessions
inthe
KID
ROPprogram
,Seminars
inFetal&
NeonatalM
edicine(2015),http://dx.doi.org/10.1016/
j.siny.2015.05.002

Curren
treport
2011
todate
Rural,multicen
ter,
India
36ruralN
ICUs,60
0e80
0km
radius,tw
ozo
nes
ofsixdistricts
each
7106
Twoteam
swithleve
lIII
tech
nicianan
dproject
man
ager
each
trav
ellin
gwithin
resp
ective
zones
Theresp
ective
imag
ing
tech
nicianson
site.
Imag
esview
edan
dva
lidated
remotelyby
ROPex
pert
(1)Anystag
eROP
(2)Trea
tmen
tgrad
eROP
(3)Decisionto
disch
arge
from
ROPscreen
ing
Tech
niciansva
lidated
asper
KID
ROPalgo
rithm.
Gov
ernmen
tvs
priva
tehospital,reg
ional
variations
discu
ssed
ROP,
retinop
athyof
prematurity;NICU,n
eonatal
intensive
care
unit.
A. Vinekar et al. / Seminars in Fetal & Neonatal Medicine xxx (2015) 1e11 7
Please cite this article in press as: Vinekar A, et al., Role of tele-medicineIndia e A report of 20,214 imaging sessions in the KIDROP program, Semj.siny.2015.05.002
examining surgeon, which is unfortunately difficult to assess. Be-sides, IO has several problems even among the “ROP experts”. In thelandmark CRYO ROP study, the initial diagnosis of threshold diseasein 12% of eyes was overruled on subsequent examination withinthree days by another examiner [24]. Inter-observer variation couldbe minimized if experts opined on an image rather than on a livepatient [25]. Furthermore, with ROP training not being mandatoryin medical college curricula in India and only few postgraduatecourses in ophthalmology imparting indirect ophthalmoscopytraining to residents and fellows, the so-called “gold standard” forROP screening appears to be an inadequate tool in tackling thecurrent burden, even as its relevance is being questioned the worldover [26].
Alternate methods of screening in outreach centers thereforeneeded exploration. Retinal imaging and telemedicine models offerviable options. Wide-field digital imaging (WFDI) for ROP screeningwas first suggested in 1999 [27] and a proof of concept demon-strated in 2000 [28]. Images were read remotely by readers. Therewas difficulty in commenting on zone 3 disease, perhaps due to thelimitations of the older devices [29]. However, WFDI fared betterthan conventional examinationswith indirect ophthalmoscopy (IO)in giving a more accurate longitudinal follow-up [30]. In the USA,WFDI as the primary means of screening was demonstrated in theStanford University Network for Diagnosis of Retinopathy of Pre-maturity (SUNDROP) program. The program used indirectophthalmoscopy only if the Retcam image was diagnosed to have a“referral-warranted ROP” or the babywas discharged from theNICU[31]. The program since then has demonstrated the utility of thestore-and-forward, hub-and-spoke method in which the remoteexpert opined on the images captured by trained nurses [32].
The KIDROP tele-ROP program in India was initiated in 2008. Ittrained and employed accredited cadres of Retcam trained tech-nicians who used an indigenously created triage algorithm todetermine on site whether the baby needed follow-up, neededtreatment, or could be discharged. A summary of “real-world” tele-ROP programs is detailed in Table 5. This is the first program from amiddle-income country to implement tele-ROP in a rural area. Inthe study region, there was no ROP screening prior to the inter-vention, making the KIDROP program the only means of providingROP screening to these infants. The program is undergoingexpansion to other Indian states through the national task on ROP,supported by the Government of India.
There were three unique aspects of the program: (1) non-physicians (level IeIII technicians) were allowed to report andanalyze the images as the first point of contact, thereby providingthe diagnosis and decision to the rural mother before she left thecenter; (2) there were no mandated indirect ophthalmoscopy ex-aminations at any point either to continue follow-up or to termi-nate screening. This strategy has allowed the onus of screening careto be shifted to the rural center, thereby obviating the dependenceon the limited few experts from the cities; (3) the program aims atdetecting any stage, not just treatment requiring disease. This dif-fers from other programs that used referral-warranted criteria astheir end-point [33e37]. This multicenter report summarizes datafrom the initial 77.5 months of program activity exclusively fromrural centers. In all the centers under study, there was no ROPprogram prior to KIDROP's intervention and none of their babiesunderwent any ROP screening.
Our experience provides new insights into ROP screening inrural villages as well as the feasibility and sustenance of a tele-medicine program for outreach centers. There are six major find-ings on ROP demographics of our study. (1) Rural ROP incidence inthis rural multicenter study was 22.39% and treatment-requiringROP was 3.57%. This is lower than that for a single rural districthospital that we reported earlier [14] (41.5% and 10.2%
in retinopathy of prematurity screening in rural outreach centers ininars in Fetal & Neonatal Medicine (2015), http://dx.doi.org/10.1016/

Fig. 4. A frequent scenario in rural, public neonatal intensive care units, which lack infrastructure and are overburdened with large number of admissions.
A. Vinekar et al. / Seminars in Fetal & Neonatal Medicine xxx (2015) 1e118
respectively), but is comparable to some urban centers [9], sug-gesting that ROP is a significant rural problem. Urban centers maybe reporting higher ROP either because of the sicker infants theymanage or because they may be using a higher concentration ofoxygen. This needs further research and will need the analysis ofoxygen and other neonatal care practices in rural vs urban centers.(2) The data suggest that 4% of all admissions are <1000 g and thatup to 29% of babies enrolled are born <30 weeks of gestational age,indicating the improved survival of these at-risk infants in ruralcenters. (3) There appear to be regional differences in the severityand type of ROP documented. North Karnataka centers have moreaggressive posterior ROP (84% of all cases of APROP) compared tothe central zone. Since the former is more backwardwith respect tohuman developmental indices, further investigation on correlatingthe level of neonatal care in these centers vis-�a-vis the moredeveloped central zone is needed. (4) Private hospitals appear to bedealing with a greater incidence of any stage ROP (33% vs 16%) andsevere disease (7.1% vs 1.7%) needing treatment compared to gov-ernment centers. This is not because “lighter” and “younger” babiesare being managed in the former (Table 4) but could be due tohigher systemic comorbidities in these babies or because of moreaggressive preterm management in the private hospitals. Theseassociations need further investigation. (5) The data suggest that
Fig. 5. Continuum of care of a preterm baby to prevent or reduce the occurrence a
Please cite this article in press as: Vinekar A, et al., Role of tele-medicineIndia e A report of 20,214 imaging sessions in the KIDROP program, Semj.siny.2015.05.002
there is a bias towards the male child. Whereas the governmentcentres show a more even gender ratio distribution, private hos-pitals show a higher proportion of males enrolled (Table 4,P < 0001). We have reported this unfortunate trend from a city-based public hospital, and it is likely that parents would prefer-entially use financial resources for the treatment of a male child in aprivate hospital or because practitioners could be more aggres-sively managing male infants [20]. (6) Our data show that 20% ofbabies who required treatment would have been missed forscreening if the American screening guidelines (1500 g and 30weeks) [23] had been used. This suggests that middle-incomecountries such as India need to develop their own screeningguidelines based on their regional variability and data [10,21].
The program has also provided insights into the feasibility of atelemedicine program for unscreened rural outreach centers. First,the mechanism of implementation through a publiceprivatepartnership appears to be a good approach. The advantages arethat a large part of the capital expenditure and running costs areborne by the government. There is also a better “buy-in” of thegovernment health care system into childhood blindness, thelarge deserving government hospitals which struggle with inad-equate infrastructure and a heavy case load (Fig. 4). The PPPsupport could also translate into its integration with the
nd severity of retinopathy of prematurity. NICU, neonatal intensive care unit.
in retinopathy of prematurity screening in rural outreach centers ininars in Fetal & Neonatal Medicine (2015), http://dx.doi.org/10.1016/

Fig. 6. Mothers wait with their infants being dilated for retinopathy of prematurity (ROP) screening on the Retcam in a rural center. This opportunity is used to promote awarenessabout ROP as well as immunization, breastfeeding, and well-baby practices.
A. Vinekar et al. / Seminars in Fetal & Neonatal Medicine xxx (2015) 1e11 9
government insurance schemes making ROP screening moreuniversally acceptable and accessible. The PPP also providesincreased program visibility and advocacy. The disadvantages ofthe PPP in our experience lie in the fact that there are frequentchanges and transfers of the bureaucracy, leading to delays inprogram implementation. There is also need to protect intellectualproperty especially where there are innovations in program stra-tegies, technology used and ideologies implemented. SeveralKIDROP centers that were being offered free ROP screening wereauctioned to third parties as part of the tendering process of thegovernment. Whereas integration into the government system isinevitable, the mechanism of such technology and skill transfermust be documented and executed to safeguard the interests ofthe program handlers. Further, delays in implementation andreimbursement of salaries and running costs place a considerablefinancial burden on the private organization that supports ormanages the program. Further, the program needs increasedparticipation from ophthalmologists in the government sector. Aspecial cadre of Team B ophthalmologists was trained at theinitiation of the program, but the involvement has been subopti-mal. Finally, the maternal and child health department rather thanthe department of ophthalmology should head an ROP program asit provides wider coverage, better integration into the child healthclinics and better utilization of the resources.
With the Government of India expanding neonatal care throughthe backbone of public-hospital-based “special newborn careunits” (SNCUs), the role of the pediatrician and neonatologist inROP screening has become paramount. Strategies must beenhanced to sensitize and train SNCU nurses on good oxygensupplementation practices, setting the right alarm, need for pulseoximetry, judicious use of oxygen during admission and transfer toanother SNCU and strict adherence to the written protocol for in-clusion into ROP screening. The involvement of the obstetrician inROP management must also be strengthened through awarenessand training including avoiding multifecundity, use of antenatalsteroids, impressing the parents about the dangers of prematurityincluding ROP and communicating the same with the treatingneonatologist (Fig. 5) Through the KIDROP program we haveattempted nurse sensitization in all centers where screening isperformed and have attempted collaboration with the treating
Please cite this article in press as: Vinekar A, et al., Role of tele-medicineIndia e A report of 20,214 imaging sessions in the KIDROP program, Semj.siny.2015.05.002
obstetric units and public health departments where available, topromote healthy newborn care practices including immunization,kangaroo mother care, and breastfeeding. This is performed whilethe mothers are waiting with their infants during dilatation, asthey are more receptive to such advice from the health carepractitioners (Fig. 6).
The limitations of the study lie in the fact that the denominatorof the total number of “at-risk” babies from each hospital are notascertained. This is largely due to the fact that registers are notmaintained in most hospitals in these outreach zones. Our teamshave attempted to collect data from the labor ward/birth register todetermine the total number of at-risk babies at each visit. Second,neonatal and maternal risk factors are not reliably documented inthe inpatient or discharge summary, making it difficult to deter-mine the risk factor analysis in the study cohort.
In conclusion, ROP screening in the rural outreach is possiblewith a telemedicine program that is managed by non-physiciansprovided they are accredited, monitored and accountable at alllevels of care. The debate about utilizing trained non-physicians ortechnicians in this important task and their ability to diagnose ROPcorrectly is relevant, but must be viewed in light of the fact thatthese rural infants have no screening mechanism in the absence ofthe current strategy. In the USA, 86e100% [38,39] of malpracticeclaims in ROP were due to screening failure and follow-up at thecenter and in the community [40]. More recently, the E-ROP studyin North America supported the validity of remote evaluation bynon-physicians to read referral-warranted ROP, but the delay in thereports which they found would make it difficult in a programwhich KIDROP which relies solely on this strategy [36].
The ideal strategy for middle-income nations would be the useof low-cost wide-field infant retinal cameras which can be usedonsite by the resident nursing or medical staff, a cloud-based imagereservoir which can be accessed and reported by ROP experts, and aprompt referral system to treat those infants whose disease pro-gresses. Only a paradigm shift in the way we currently manage ROPcan prevent blindness in the millions of premature infants bornworldwide. Strategies to integrate ROP into universal screening arealready being piloted in India [41]. A greater awareness and trainingamong pediatricians, obstetricians, ophthalmologists, nurses andparents is required to tackle this burden of ROP blindness.
in retinopathy of prematurity screening in rural outreach centers ininars in Fetal & Neonatal Medicine (2015), http://dx.doi.org/10.1016/
Practice points
� This is the first multicenter rural retinopathy of prematu-
rity (ROP) study and covers a population of >23 million.
� Non-physician technicians can use wide-field digital im-
aging to screen for ROP as the primary method of
screening.
� Technicians can be trained to capture images as well as
grade and report the disease, obviating the need for the
scarce ROP specialist in the outreach.
� There is a large proportion of premature infants born <30weeks of gestational age and <1000 g at birth who are
surviving in rural centers.
� There is considerable regional variation in the severity of
ROP within the same state and this could be related to
neonatal care and overall developmental indices.
� Private NICUs appear to have a higher incidence of any
stage of ROP as well as severe disease compared to their
government counterparts.
� A larger proportion of males are cared for in private
hospitals compared to females, suggesting a gender bias.
This is not evidenced in the public hospitals.
� Nearly 20% of babies undergoing treatment were outside
the American screening guidelines and would have been
missed.
� There was no case of unscreened stage 5 ROP in any
center during the study period.
Research directions
� The cost/benefit utility analysis of this telemedicine pro-
gram for ROP screening in rural outreach centers needs to
be assessed.
� Innovations in low-cost infant retinal cameras that can be
situated in each center and connected to a central cloud-
based server managed by ROP specialists or trained
technicians or image readers would increase the
coverage and accessibility of the program.
� The impact of this program in training of health care
personnel, including obstetricians, pediatricians, nursing
and paramedical staff in the NICUs and special newborn
care units in the judicious use of oxygen and monitoring
of ROP needs to be studied.
A. Vinekar et al. / Seminars in Fetal & Neonatal Medicine xxx (2015) 1e1110
Conflict of interest statement
None declared.
Funding sources
The rural outreach component of KIDROP is supported through apublic-private partnership between the The National Rural HealthMission, Government of India and Government of Karnataka withNarayana Nethralaya Postgraduate Institute of Ophthalmology,Bangalore, India.
Acknowledgements
We acknowledge the following for their support in this pro-gram: North Karnataka team: Dr Siddesh Kumar, Mr Muralidhar
Please cite this article in press as: Vinekar A, et al., Role of tele-medicineIndia e A report of 20,214 imaging sessions in the KIDROP program, Semj.siny.2015.05.002
Gayakwad, Mr Ravishankar Kandagal, Mr Sudendra Babu; CentralZone team: Dr Prakash Suranagi, Mr Madhava Prasad Padaki, MrSomeshwara Matad, Mr Manjunatha Kalleshappa; KIDROP's head-quarter team: Mr Praveen Sharma, Mr Sivakumar Munusamy, MrKrishnan Narasimha, Mr Srinivas Gowda.
References
*[1] Gilbert C, Rahi J, Eckstein M, O'Sullivan J, Foster A. Retinopathy of prematurityin middle-income countries. Lancet 1997;350:12e4.
*[2] Gilbert C, Fielder A, Gordillo L, Quinn G, Semiglia R, Visintin P, et al. Inter-national NO-ROP Group. Characteristics of infants with severe retinopathy ofprematurity in countries with low, moderate, and high levels of develop-ment: implications for screening programs. Pediatrics 2005;115:e518e25.
[3] Child health screening andearly intervention services underNRHMMinistryofHealth and Family Welfare. Operational guidelines for Rashtriya Bal SwasthyaKaryakram. 2013. Available at:, http://mdm.nic.in/Files/School%20Health%20Programme/Nutrition_Support/Rastriya_Bal_Swaasthya_Karyakram.pdf.
*[4] United Nations. Born too soon. The global action report on preterm birth.2012. Available from:, http://www.who.int/pmnch/media/news/2012/201204_borntoosoon-report.pdf.
*[5] Vinekar A, Gilbert C, Dogra M, Kurian M, Shainesh G, Shetty B, et al. TheKIDROP model of combining strategies for providing retinopathy of prema-turity screening in underserved areas in India using wide-field imaging, tele-medicine, non-physician graders and smart phone reporting. Indian J Oph-thalmol 2014;62:41e9.
[6] Gilbert CE, Anderton L, Dandona L, Foster A. Prevalence of visual impairmentin children: a review of available data. Ophthalmic Epidemiol 1999;6:73e82.
[7] Charan R, Dogra MR, Gupta A, Narang A. The incidence of retinopathy ofprematurity in a neonatal care unit. Indian J Ophthalmol 1995;43:123e6.
[8] Gopal L, Sharma T, Ramachandran S, Shanmugasundaram R, Asha V. Reti-nopathy of prematurity: a study. Indian J Ophthalmol 1995;43:59e61.
[9] Maheshwari R, Kumar H, Paul VK, Singh M, Deorari AK, Tiwari HK. Incidenceand risk factors of retinopathy of prematurity in a tertiary care newborn unitin New Delhi. Natl Med J India 1996;9:211e4.
[10] Vinekar A, Dogra MR, Sangtam T, Narang A, Gupta A. Retinopathy of pre-maturity in Asian Indian babies weighing greater than 1250 grams at birth:ten year data from a tertiary care center in a developing country. Indian JOphthalmol 2007;55:331e6.
[11] Shah PK, Narendran V, Kalpana N, Gilbert C. Severe retinopathy of prematurityin big babies in India: history repeating itself? Indian J Pediatr 2009;76:801e4.
[12] Jalali S, Kesarwani S, Hussain A. Outcomes of a protocol-based managementfor zone 1 retinopathy of prematurity: the Indian Twin Cities ROP ScreeningProgram report number 2. Am J Ophthalmol 2011;151:719e24.
[13] Azad R. Prevention of blindness due to retinopathy of prematurity: a nationalmovement. Indian J Pediatr 2014;81:1373e5.
[14] Hungi B, Vinekar A, Datti N, Kariyappa P, Braganza S, Chinnaiah S, et al.Retinopathy of prematurity in a rural neonatal intensive care unit in SouthIndia e a prospective study. Indian J Pediatr 2012;79:911e5.
[15] Keerthi BJ, Babu S, Vinekar A, Goud N, Bullappa A. Retinopathy of prematurityscreening of 500 infants in a level II neonatal intensive care unit at a medicalcollege hospital in Southern Karnataka. J EvolMed Dent Sci 2014;3:10665e72.
[16] Vinekar A, Avadhani K, Braganza S, Shetty B, Dogra M, Gilbert C. Outcomes ofa protocol-based management for zone 1 retinopathy of prematurity: theIndian Twin Cities ROP Screening Program report number 2. Am J Oph-thalmol 2011;152:712. author reply 713.
[17] Vinekar A. IT-enabled innovation to prevent infant blindness in rural India:the KIDROP experience. J Indian Business Res 2011;3:98e102.
[18] Sanghi G, Dogra MR, Katoch D, Gupta A. Demographic profile of infants withstage 5 retinopathy of prematurity in North India: implications for screening.Ophthalmic Epidemiol 2011;18:72e4.
[19] Vinekar A, Jayadev C, Bauer N. Need for telemedicine in retinopathy of pre-maturity in middle-income countries: e-ROP vs KIDROP. JAMA Ophthalmol2015;133:360e1.
[20] Vinekar A, Avadhani K, Dogra M, Sharma P, Gilbert C, Braganza S, et al.A novel, low-cost method of enrolling infants at risk for retinopathy ofprematurity in centers with no screening program: the REDROP study.Ophthalmic Epidemiol 2012;19:317e21.
[21] Pejaver RK, Vinekar A, Bilagi A. National Neonatology Foundation's EvidenceBased Clinical Practice Guidelines 2010. Retinopathy of Prematurity (NNFIndia, Guidelines). 2010. p. 253e62.
[22] Vinekar A, Jayadev C, Bilagi A, Pejaver R, Dhaded SM, Battu RR. Screening andprevention of ROP: practical pearls for the ophthalmologist and the pedia-trician. Perinatology 2014;15:97e9.
[23] Anonymous. Screening examination of premature infants for retinopathy ofprematurity. A joint statement of the American Academy of Pediatrics, theAmerican Association for Pediatric Ophthalmology and Strabismus, and theAmerican Academy of Ophthalmology. Pediatrics 1997;100(2 Pt 1):273.
[24] Reynolds JD, Dobson V, Quinn GE, Fielder AR, Palmer EA, Saunders RA, et al.CRYO-ROP and LIGHT-ROP Cooperative Study Groups. Evidence-basedscreening criteria for retinopathy of prematurity: natural history data fromthe CRYO-ROP and LIGHT-ROP studies. Arch Ophthalmol 2002;120:1470e6.
in retinopathy of prematurity screening in rural outreach centers ininars in Fetal & Neonatal Medicine (2015), http://dx.doi.org/10.1016/
A. Vinekar et al. / Seminars in Fetal & Neonatal Medicine xxx (2015) 1e11 11
[25] Wilson PJ, Ellis JD, MacEwen CJ, Ellingford A, Talbot J, Leese GP. Screening fordiabetic retinopathy: a comparative trial of photography and scanning laserophthalmoscopy. Ophthalmologica 2010;224:251e7.
[26] Trese MT. What is the real gold standard for ROP screening? Retina2008;28(3 Suppl):S1e2. Erratum in: Retina 2009;29:127.
[27] Lorenz B, Bock M, Müller HM, Massie NA. Telemedicine based screening ofinfants at risk for retinopathy of prematurity. Stud Health Technol Inform1999;64:155e63.
[28] Schwartz SD, Harrison SA, Ferrone PJ, Trese MT. Telemedical evaluation andmanagement of retinopathy of prematurity using a fiberoptic digital funduscamera. Ophthalmology 2000;107:25e8.
[29] Roth DB, Morales D, Feuer WJ, Hess D, Johnson RA, Flynn JT. Screening forretinopathy of prematurity employing the retcam 120: sensitivity andspecificity. Archs Ophthalmol 2001;119:268e72.
*[30] Ells AL, Holmes JM, Astle WF, Williams G, Leske DA, Fielden M, et al. Tele-medicine approach to screening for severe retinopathy of prematurity: apilot study. Ophthalmology 2003;110:2113e7.
[31] Murakami Y, Jain A, Silva RA, Lad EM, Gandhi J, Moshfeghi DM. StanfordUniversity Network for Diagnosis of Retinopathy of Prematurity (SUNDROP):12-month experience with telemedicine screening. Br J Ophthalmol 2008;92:1456e60.
*[32] Lorenz B, Spasovska K, Elflein H, Schneider N. Wide-field digital imagingbased telemedicine for screening for acute retinopathy of prematurity (ROP).Six-year results of a multicentre field study. Graefes Arch Clin Exp Oph-thalmol 2009;247:1251e62.
[33] Weaver DT, Murdock TJ. Telemedicine detection of type 1 ROP in a distantneonatal intensive care unit. J AAPOS 2012;16:229e33.
Please cite this article in press as: Vinekar A, et al., Role of tele-medicineIndia e A report of 20,214 imaging sessions in the KIDROP program, Semj.siny.2015.05.002
*[34] Fijalkowski N, Zheng LL, Henderson MT, Wang SK, Wallenstein MB, Leng T,et al. Stanford University Network for Diagnosis of Retinopathy of Prema-turity (SUNDROP): five years of screening with telemedicine. OphthalmicSurg Lasers Imaging Retina 2014;45:106e13.
*[35] Shah SP, Wu Z, Iverson S, Dai S. Specialist Nurse Screening for Retinopathy ofPrematurityVA Pilot Study. Asia-Pac J Ophthalmol 2013;2:300e4.
*[36] Quinn GE, Ying GS, Daniel E, Hildebrand PL, Ells A, Baumritter A, et al. e-ROPCooperative Group. Validity of a telemedicine system for the evaluation ofacute-phase retinopathy of prematurity. JAMA Ophthalmol 2014;132:1178e84.
[37] Silva RA, Murakami Y, Lad EM, Moshfeghi DM. Stanford University networkfor diagnosis of retinopathy of prematurity (SUNDROP): 36-month experi-ence with telemedicine screening. Ophthalmic Surg Lasers Imaging 2011;42:12e9.
[38] Day S, Menke AM, Abbott RL. Retinopathy of prematurity malpractice claims:the Ophthalmic Mutual Insurance Company experience. Arch Ophthalmol2009;127:794e8.
[39] Reynolds JD. Malpractice and the quality of care in retinopathy of prematu-rity (an American Ophthalmological Society thesis). Trans Am OphthalmolSoc 2007;105:461e80.
[40] Kemper AR, Wallace DK. Neonatologists' practices and experiences in ar-ranging retinopathy of prematurity screening services. Pediatrics 2007;120:527e31.
*[41] Vinekar A, Govindaraj I, Jayadev C, Kumar AK, Sharma P, Mangalesh S,et al. Universal ocular screening of 1021 term infants using wide-fielddigital imaging in a single public hospital in India e a pilot study.Acta Ophthalmol 2015 Feb 26. http://dx.doi.org/10.1111/aos.12685.
in retinopathy of prematurity screening in rural outreach centers ininars in Fetal & Neonatal Medicine (2015), http://dx.doi.org/10.1016/