role of low placental share in twin–twin transfusion syndrome complicated by intrauterine growth...
TRANSCRIPT

lable at ScienceDirect
Placenta 32 (2011) 616e618
Contents lists avai
Placenta
journal homepage: www.elsevier .com/locate/placenta
Role of low placental share in twinetwin transfusion syndromecomplicated by intrauterine growth restrictionq
B.H. Grubbs a, K. Benirschke b, L.M. Korst a, A. Llanes a, L. Yedigarova a, R.H. Chmait a,*aDivision of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Keck School of Medicine, University of Southern California,1300 North Vermont Avenue, Suite 706, Los Angeles, CA 90027, USAbDepartment of Pathology, University of California San Diego, San Diego, CA, USA
a r t i c l e i n f o
Article history:Accepted 22 May 2011
Keywords:Placental shareIntrauterine growth restrictionTwinetwin transfusion syndrome
q Previously presented: Portions of this manuscrip#393 Poster Session III at the Society for Maternal-Meeting, San Francisco, California on February 11, 201* Corresponding author. Tel.: þ1 323 361 6074; fax
E-mail address: [email protected] (R.H. Chmait).
0143-4004/$ e see front matter � 2011 Elsevier Ltd.doi:10.1016/j.placenta.2011.05.009
a b s t r a c t
Objectives: Prior studies have demonstrated that donor twin survival following treatment of twinetwintransfusion syndrome (TTTS) was highly associated with donor intrauterine growth restriction (IUGR).Here, we hypothesized that donor IUGR may be attributed in part to low placental share.Study design: The study population consisted of all patients who underwent laser treatment for TTTS ata single institution between 2006-2010. Only those pregnancies with dual survival at birth were includedso that placental share information could be interpreted. We examined the relationships betweenQuintero Stage (with separate analysis of Stage III patients with critically abnormal donor Dopplerfindings) and low placental share (defined as � 30%) with IUGR (<10th percentile) using chi-squareanalysis and multivariable logistic regression modeling.Results: Of 210 patients treated, 159 (75.7%) had dual survivors at birth. Of these, placental share wasdocumented in 90 cases (56.6%). Twenty-seven (30.0%) had low placental share, and 37 (41.1%) had IUGR.IUGR was associated with low placental share (63.0% vs. 31.7%, P ¼ 0.0116). IUGR was also associated withStage III patients (57.4% vs. 23.3%, P ¼ 0.0021), and in particular with Stage III patients with donorinvolvement (77.8% vs. 25.4%, P < 0.0001). In logistic regression modeling, both low placental share andStage III with donor involvement were independent risk factors for IUGR (OR ¼ 3.5 [1.2e10.3],P ¼ 0.0206, and OR ¼ 10.1 [3.3e30.6], P < 0.0001, respectively).Conclusions: Donor IUGR in TTTS pregnancies appears to be associated, in part, with low placental share.
� 2011 Elsevier Ltd. All rights reserved.
1. Introduction
In the USFetus study, which described stage-based perinataloutcomes of 682 consecutive cases of twinetwin transfusionsyndrome (TTTS) treated with selective laser photocoagulation ofcommunicating vessels, the presence of intrauterine growthrestriction (IUGR) in the donor twin appeared to be a strong riskfactor for donor demise [1]. A potential explanation for theobserved post-operative decreased donor survival among gesta-tions with donor IUGR is that affected donors may have relativelydecreased individual placental territory. It has been proposed thatunequal placental share may occur if trophoblastic and/or inner cellmass segregate into two groups of cells composed of different cell
t were presented in AbstractFetal Medicine, 31st Annual1.: þ1 323 361 6099.
All rights reserved.
numbers during the monozygotic twinning process [2]. Lowplacental share has been associated with IUGR in monochorionictwins [3e5], including those complicated by TTTS [6e8].
The purpose of this study was to assess whether a low placentalshare in TTTS pregnancies is associated with donor IUGR.
2. Methods
We analyzed data collected prospectively from all patients undergoing lasertherapy for the treatment of TTTS at the Los Angeles Fetal Therapy Program,University of Southern California (USC), between 2006 and 2010. At initial assess-ment, all patients with monochorionic-diamniotic multiple gestations underwenta complete ultrasonographic examination, and the diagnosis of TTTS was made andprospectively classified according to the Quintero Staging System [9]. Stage III donor-involved patients included those Stage III pregnancies in which only the donor(Stage III donor) and those in which both the donor and recipient (Stage III Donor/Recipient) manifested abnormal Doppler studies. Abnormal Doppler findings weredefined as persistent absent or reversed end diastolic flow in the umbilical artery,persistent reversed flow of the ductus venosus a-wave, or pulsatile umbilical venousflow. These Stage III donor-involved patients were compared to those without donorinvolvement (Stage III Recipient). No patients were upstaged based on echocardio-graphic findings.

B.H. Grubbs et al. / Placenta 32 (2011) 616e618 617
Patients categorized as Quintero Stage I through IV were offered laser surgery ifthey were diagnosed with TTTS between 16 and 26 weeks’ gestation. Women whochose laser surgery gave written informed consent, and underwent the procedureusing the surgical techniques described previously [1]. The stage-based perinataloutcomes of the 210 patients in this study were included in the USFetus study [1].Monoamniotic twins were excluded from the analysis. Patients with triplet preg-nancies and patients with a short cervix were not excluded. At the time of treatment,patients with donor IUGRwere identified via ultrasound as having a donor twinwithan estimated fetal weight (EFW) less than the 10th percentile for the stated gesta-tional age [10].
After treatment, patients returned to their referring physicians to be subse-quently managed and delivered. At the time of delivery, the referring physician wasinstructed to send the placenta to University of California, San Diego, for gross andmicroscopic pathological review by one of the authors (KB). Placentas were sentfresh after delivery from the referring centers via express mail in a watertightcontainer. They were weighed to obtain the total placental mass, and the individualplacental territory was determined. The avascular zone on the chorionic fetal surfacethat divided the placenta into two territories between both cord insertions wasidentified as the anatomic vascular equator, and the placenta was cut along this line.Each placental portionwas thenweighed separately, yielding an individual placentalmass (IPM). Individual placental territory (IPT) was calculated as [(IPM divided bytotal placental mass) � 100]. The IPT was calculated for the donor and the recipienttwin. A subset of patients with placental information was analyzed, and “lowplacental share”was defined as an IPT less than 30% [8]. Because an intrauterine fetaldemise (IUFD) could affect placental weight at birth, only gestations with bothfetuses born alive were included in this investigation.
To estimate the effect of bias created by the necessity of looking only at dual fetalsurvivors, we described the Quintero Stage distribution and gestational age atdelivery for those gestations inwhich both fetuses were and were not born alive. Forthose cases with dual survivors, we then described the Quintero Stage distributionand gestational age at delivery for those who did and did not have a placentalexamination, to assure that no other obvious biases existed in the final studypopulation.
Because IUGR gestations appear to be at risk for donor demise, we wished todetermine whether low placental share was associated with IUGR, as a potentialcausal factor. Thus, our primary relationship of interest is between IUGR and lowplacental share. Because, as reported in the USFetus study [1], Quintero Stage IIIdonor-involved gestations were at increased risk for donor demise, and may havea common causal factor (low placental share), we included Quintero Stage in theanalyses. We then examined the relationships between Quintero Stage and lowplacental share with IUGR using chi-square analysis and multivariable logisticregression modeling, including an interaction term. Odds ratios (OR) and their 95%Confidence Intervals (CI) are expressed for logistic regression results. This study wasapproved by the Institutional Review Board at USC’s Health Sciences Campus, LosAngeles, California.
3. Results
Of the 210 consecutive TTTS patients that underwent lasersurgery, 159 (75.7%) had dual survivors at birth. The majority ofpatients who were excluded because of this criterion were largelycategorized as Stage III donor-involved (Table 1). Those gestationswith dual survivors at birth did not demonstrate any difference ingestational age at delivery compared to those who were excluded:(median [range]) 32.0 (20.1e39.2) weeks vs. 33.7 (23.1e38.4)weeks, P ¼ 0.6462.
Of the 159 gestations with dual survivors at birth, placentalshare was documented in 90 cases (56.6%). The Stage distributionfor those who did and did not have a placental examination isshown in Table 1. Those gestations with placental examinations didnot demonstrate any difference in gestational age at delivery:
Table 1Quintero Stage distribution of laser treated TTTS patients excluded from analysis becaus
Both fetuses born alive (Total N ¼ 210) Stage I Stage II
Yes 159 (75.7%) 25 (15.7%) 32 (20.1%)No 51 (24.3%) 2 (3.9%) 10 (19.6%)
Dual Survivors with PlacentalExamination (Total N ¼ 159)
Yes 90 (56.6%) 15 (16.7%) 19 (21.1%)No 69 (43.4%) 10 (14.5%) 13 (18.8%)
(median [range]) 33.8 (23.1e38.0) weeks vs. 33.6 (24.0e38.4)weeks, P ¼ 0.8037. For this final study population of 90 cases, theStage distribution was: Stage I (N ¼ 15); Stage II (N ¼ 19); Stage III(N ¼ 47) of which 27 (57.4%) had donor involvement; and Stage IV(N ¼ 9).
In these final 90 patients, low placental share was identified in27 (30%) and IUGR was identified in 37 (41%). Of the 47 patientswith low placental and/or IUGR, 10 (21%) had low placental shareonly, 20 (43%) had IUGR only, and 17 (36%) had both low placentalshare and IUGR. Of the patients with low placental share, 14/27(51.9%) had a velamentous cord insertion vs. 22/63 (34.9%) in thosewithout a low placental share (p ¼ 0.20). IUGR was associated withthose gestations in which the donor twin had a low placental sharevs. those gestations in which the placental share was not classifiedas low (17/27 [63.0%] vs. 20/63 [31.7%], P ¼ 0.0116).IUGR was alsoassociated with Stage III patients when compared to all otherpatients (27/47 [57.4%] vs. 10/43 [23.3%], P ¼ 0.0021), and wasespecially prevalent among Stage III donor-involved patients whencompared to all other patients (21/27 [77.8%] vs. 16/63 [25.4%],P < 0.0001). Although Stage III patients with donor involvementappeared more likely to demonstrate a low placental share, thisrelationship did not reach statistical significance (11/27 [40.7%] vs.16/63 [25.4%], P ¼ 0.2283). A logistic regression model for donorIUGR was constructed using low placental share and Stage III donorinvolvement (reference all other patients), and included an inter-action term for the two variables. Both low placental share andStage III with donor involvement were strong risk factors for donorIUGR (OR ¼ 3.54 [95% CI 1.21e10.32], P ¼ 0.0206, and OR ¼ 10.09[95% CI 3.33e30.57], P < 0.0001, respectively). The interaction termwas non-contributory.
These same relationships were confirmed in a sub-analysis of allStage III patients only, comparing those with Stage III donorinvolvement to those with recipient involvement only (lowplacental share OR ¼ 11.41 [95% CI 1.78e73.18, P ¼ 0.0102], Stage IIIdonor-involved OR ¼ 9.44 [95% CI 2.05e43.49, P ¼ 0.0040]). Theinteraction term was non-contributory.
4. Discussion
Donor fetus IUGR is not an uncommon finding in TTTS, and isassociated with relatively high risk of donor demise post lasersurgery [1]. The etiology of donor IUGR may be due to “nutritionaldepletion” because of transfusion to the recipient twin and/or“placental insufficiency” due to poor placental share inherent in thepregnancy [7]. In this study of placental share among dual TTTSsurvivors after laser surgery, we found a strong associationbetween low placental share and donor IUGR. However, QuinteroStage III, particularly Quintero Stage III with donor involvement,was also positively associated with donor IUGR. Logistic regressionmodeling found that both low placental share and Quintero StageIII were independently associated with IUGR in the donor.
Laser surgery is widely accepted as the treatment of choice inthe setting of TTTS, due to improved survival and neurological
e: (1) both fetuses did not survive; or (2) the placenta was not examined.
Stage IIIdonor-involved
Stage III Recipientonly involved
Stage IV P value
49 (30.8%) 35 (22.0%) 18 (11.3%) 0.016828 (54.9%) 7 (13.7%) 4 (7.8%)
27 (30.0%) 20 (22.2%) 9 (10.0%) 0.964622 (31.8%) 15 (21.7%) 9 (13.0%)
B.H. Grubbs et al. / Placenta 32 (2011) 616e618618
outcomes compared to other treatment modalities [11]. The elim-ination of vascular communications via laser ablation treats TTTS byeffectively creating a dichorionic placenta. However, the placentamust be “split” according to the vascular anatomy. Thus, lasersurgery can cure TTTS, but cannot correct unequal placental sharethat may be inherent in any given monochorionic twin pregnancy.In cases where nutritional depletion is the primary source of donorIUGR, laser surgery would be expected to significantly improveoutcomes in the donor fetus. In fact, laser surgery has been shownto result in “catch-up” growth in a subgroup of surviving donorfetuses with IUGR [8]. However, in those cases of donor IUGRcomplicated by low placental share, laser surgery may not preventpoor perinatal outcomes, as was seen in the USFetus study [1]. Webelieve that both factors (nutritional depletion and placentalinsufficiency) play an important role in donor IUGR and outcomes.
A relationship between placental share and fetal growth in TTTShas been described in prior studies. Quintero demonstrated thatdonors tended to have a smaller placental share when compared torecipients [6]. This study additionally showed that donor survivalfollowing laser surgery was expected if placental share was greaterthan 18%, and that donors could survive with as little as 10%placental share. Placental share was determined using the samemethods as used by our study, and also carried the limitation of thestudy population to dual survivors. Habli reported on TTTS affectedby "placental insufficiency", which was defined as estimated fetalweight < 10th percentile with an increased head circumference toabdominal circumference ratio, and estimated fetal weight discor-dance >20% [12]. All cases also had abnormal Doppler studiesdefined as the presence of any of the following: pulsatile umbilicalvenous flow, umbilical artery (UA) absent or reversed end diastolicflow, systolic to diastolic (S/D) ratio >3.0 or resistance index>0.622, reversed flow in the ductus venosus, or elevated middlecerebral artery resistance index or peak systolic velocity. Donors inthis series had a mean fetoscopically estimated placental share of26% and a significantly higher rate of marginal ormembranous cordinsertion as demonstrated by magnetic resonance imaging, ultra-sound, and/or fetoscopy. Importantly, this series lacked informationregarding placental pathology.
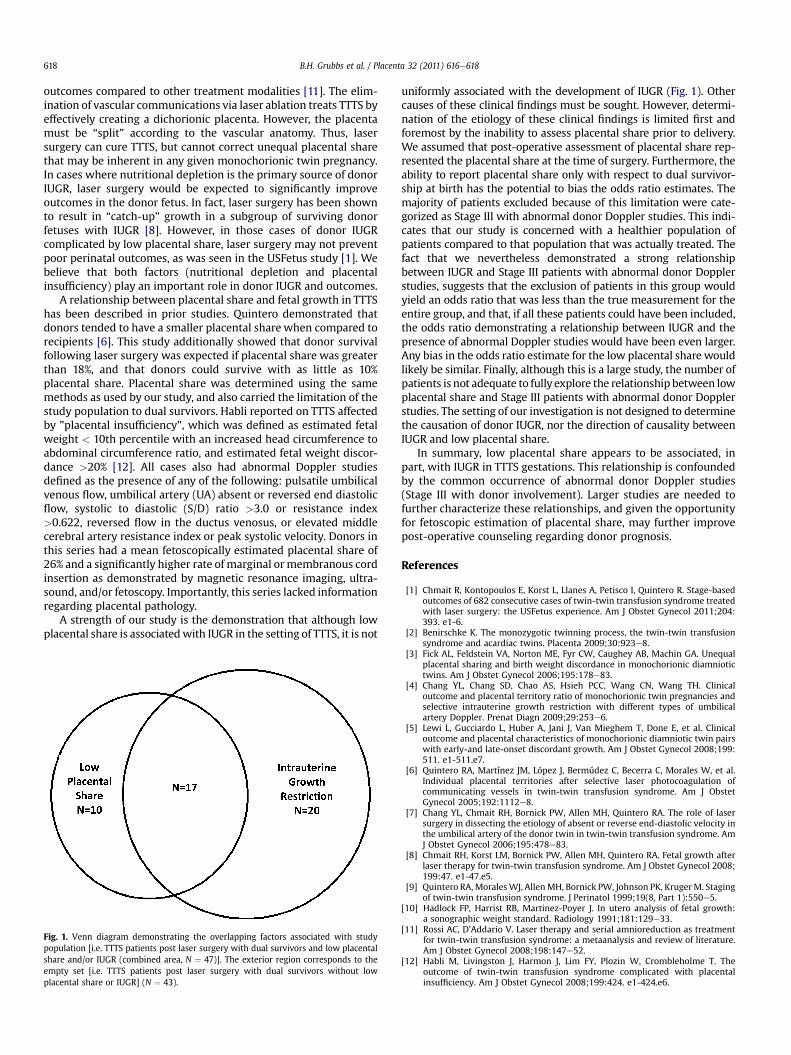
A strength of our study is the demonstration that although lowplacental share is associatedwith IUGR in the setting of TTTS, it is not
Fig. 1. Venn diagram demonstrating the overlapping factors associated with studypopulation [i.e. TTTS patients post laser surgery with dual survivors and low placentalshare and/or IUGR (combined area, N ¼ 47)]. The exterior region corresponds to theempty set [i.e. TTTS patients post laser surgery with dual survivors without lowplacental share or IUGR] (N ¼ 43).
uniformly associated with the development of IUGR (Fig. 1). Othercauses of these clinical findings must be sought. However, determi-nation of the etiology of these clinical findings is limited first andforemost by the inability to assess placental share prior to delivery.We assumed that post-operative assessment of placental share rep-resented the placental share at the time of surgery. Furthermore, theability to report placental share only with respect to dual survivor-ship at birth has the potential to bias the odds ratio estimates. Themajority of patients excluded because of this limitation were cate-gorized as Stage III with abnormal donor Doppler studies. This indi-cates that our study is concerned with a healthier population ofpatients compared to that population that was actually treated. Thefact that we nevertheless demonstrated a strong relationshipbetween IUGR and Stage III patients with abnormal donor Dopplerstudies, suggests that the exclusion of patients in this group wouldyield an odds ratio that was less than the true measurement for theentire group, and that, if all these patients could have been included,the odds ratio demonstrating a relationship between IUGR and thepresence of abnormal Doppler studies would have been even larger.Any bias in the odds ratio estimate for the low placental share wouldlikely be similar. Finally, although this is a large study, the number ofpatients is not adequate to fully explore the relationship between lowplacental share and Stage III patients with abnormal donor Dopplerstudies. The setting of our investigation is not designed to determinethe causation of donor IUGR, nor the direction of causality betweenIUGR and low placental share.
In summary, low placental share appears to be associated, inpart, with IUGR in TTTS gestations. This relationship is confoundedby the common occurrence of abnormal donor Doppler studies(Stage III with donor involvement). Larger studies are needed tofurther characterize these relationships, and given the opportunityfor fetoscopic estimation of placental share, may further improvepost-operative counseling regarding donor prognosis.
References
[1] Chmait R, Kontopoulos E, Korst L, Llanes A, Petisco I, Quintero R. Stage-basedoutcomes of 682 consecutive cases of twin-twin transfusion syndrome treatedwith laser surgery: the USFetus experience. Am J Obstet Gynecol 2011;204:393. e1-6.
[2] Benirschke K. The monozygotic twinning process, the twin-twin transfusionsyndrome and acardiac twins. Placenta 2009;30:923e8.
[3] Fick AL, Feldstein VA, Norton ME, Fyr CW, Caughey AB, Machin GA. Unequalplacental sharing and birth weight discordance in monochorionic diamniotictwins. Am J Obstet Gynecol 2006;195:178e83.
[4] Chang YL, Chang SD, Chao AS, Hsieh PCC, Wang CN, Wang TH. Clinicaloutcome and placental territory ratio of monochorionic twin pregnancies andselective intrauterine growth restriction with different types of umbilicalartery Doppler. Prenat Diagn 2009;29:253e6.
[5] Lewi L, Gucciardo L, Huber A, Jani J, Van Mieghem T, Done E, et al. Clinicaloutcome and placental characteristics of monochorionic diamniotic twin pairswith early-and late-onset discordant growth. Am J Obstet Gynecol 2008;199:511. e1-511.e7.
[6] Quintero RA, Martínez JM, López J, Bermúdez C, Becerra C, Morales W, et al.Individual placental territories after selective laser photocoagulation ofcommunicating vessels in twin-twin transfusion syndrome. Am J ObstetGynecol 2005;192:1112e8.
[7] Chang YL, Chmait RH, Bornick PW, Allen MH, Quintero RA. The role of lasersurgery in dissecting the etiology of absent or reverse end-diastolic velocity inthe umbilical artery of the donor twin in twin-twin transfusion syndrome. AmJ Obstet Gynecol 2006;195:478e83.
[8] Chmait RH, Korst LM, Bornick PW, Allen MH, Quintero RA. Fetal growth afterlaser therapy for twin-twin transfusion syndrome. Am J Obstet Gynecol 2008;199:47. e1-47.e5.
[9] Quintero RA, MoralesWJ, AllenMH, Bornick PW, Johnson PK, KrugerM. Stagingof twin-twin transfusion syndrome. J Perinatol 1999;19(8, Part 1):550e5.
[10] Hadlock FP, Harrist RB, Martinez-Poyer J. In utero analysis of fetal growth:a sonographic weight standard. Radiology 1991;181:129e33.
[11] Rossi AC, D’Addario V. Laser therapy and serial amnioreduction as treatmentfor twin-twin transfusion syndrome: a metaanalysis and review of literature.Am J Obstet Gynecol 2008;198:147e52.
[12] Habli M, Livingston J, Harmon J, Lim FY, Plozin W, Crombleholme T. Theoutcome of twin-twin transfusion syndrome complicated with placentalinsufficiency. Am J Obstet Gynecol 2008;199:424. e1-424.e6.