risk factors for post-pancreaticoduodenectomy bleeding and finding an innovative approach to...
TRANSCRIPT

Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Dig Surg 2009;26:297–305 DOI: 10.1159/000228245
Risk Factors for Post-Pancreaticoduodenectomy Bleeding and Finding an Innovative Approach to Treatment
Hung-Kuang Wei a Shin-E Wang a Yi-Ming Shyr a Hsiuo-Shan Tseng b
Wan-Chen Tsai b Tien-Hua Chen a Cheng-Hsi Su a Chew-Wun Wu a
Wing-Yiu Lui a
Departments of a Surgery, Taipei Veterans General Hospital, and b Radiology, Koo Foundation Sun Yat-SenCancer Center and Taipei Veterans General Hospital, National Yang Ming University, Taipei , Taiwan
failure. Conclusions: The placement of metallic clips on the gastroduodenal artery stump during a pancreaticoduode-nectomy is helpful in identifying overlooked intermittent sentinel bleeding during angiography. Transarterial emboli-zation for gastroduodenal artery bleeding could not guaran-tee against hepatic failure. The intravascular placement of a covered stent is the preferred procedure to avoid the com-plete interruption of arterial blood supply to the liver.
Copyright © 2009 S. Karger AG, Basel
Introduction
Surgical mortality after pancreaticoduodenectomy has decreased to under 5% in most high-volume centers, but morbidity remains high, ranging from 18 to 52% [1–4] . The most frequent causes of morbidity are delayed gastric emptying and pancreatic leakage [1–2] . The inci-dence of pancreatic leakage has been reported to be 3.7–25%, with an average of 13.6% [4] . Pancreatic leakage of-ten carries a mortality rate of 8–40% because this may result in further serious complications, e.g. intra-abdom-inal abscess, sepsis and bleeding [3–8] . Post-pancreatico-duodenectomy bleeding is the major concern once pan-creatic leakage occurs [3, 9] . According to the literature, the outcome of post-pancreaticoduodenectomy bleeding
Key Words
Post-pancreaticoduodenectomy bleeding � Gastroduodenal artery � Transarterial embolization � Covered stent
Abstract
Background: This study is to determine the risk factors and outcome for post-pancreaticoduodenectomy bleeding, and to assess the roles of surgery and intravascular intervention in its management. Methods: Post-pancreaticoduodenecto-my data of 628 patients were analyzed with regards to post-pancreaticoduodenectomy bleeding. Results: Post-pancre-aticoduodenectomy bleeding occurred in 58 patients (9.2%) and led to death in 23 patients. Pancreatic leakage and intra-abdominal abscess were independent risk factors for both extraluminal and intraluminal post-pancreaticoduodenec-tomy bleeding. The most common source of bleeding was the gastroduodenal artery (n = 9, 24.3%), and 8 of these pa-tients (88.9%) experienced gastroduodenal artery bleeding in late post-pancreaticoduodenectomy bleeding. Hemo-stasis for post-pancreaticoduodenectomy bleeding was achieved by surgery in 22 patients (78.6%) and intravascular intervention in 7 patients (58.3%). Transarterial embolization for gastroduodenal artery bleeding did not deteriorate liver function in most patients except for 1 who died of hepatic
Received: October 17, 2008 Accepted: March 28, 2009 Published online: July 11, 2009
Yi-Ming Shyr, MD Division of General Surgery, Department of SurgeryVeterans General Hospital, 201 Section 2 Shih-Pai Road Taipei 112 (Taiwan) Tel. +886 2 2875 7652, Fax +886 2 2875 7537, E-Mail [email protected]
© 2009 S. Karger AG, Basel0253–4886/09/0264–0297$26.00/0
Accessible online at:www.karger.com/dsu

Wei /Wang /Shyr /Tseng /Tsai /Chen /Su /Wu /Lui
Dig Surg 2009;26:297–305298
is often unfavorable, with a mortality rate of about 60% [3, 5, 9, 10] . Deciding on the optimal management of life-threatening post-pancreaticoduodenectomy bleeding is difficult, especially for late bleeding. Management of post-pancreaticoduodenectomy bleeding is often dictat-ed by the clinical status of each individual patient, avail-able medical equipment and institutional preferences. The endoscopic approach is feasible mainly for gastroin-testinal (intraluminal) bleeding; reoperation is tradition-ally reserved for intra-abdominal (extraluminal) bleed-ing, but carries substantial morbidity and mortality for late bleeding [3, 10] . Intravascular intervention, such as transarterial embolization or the placement of covered stents to occlude the orifice of the bleeding vessel, is a minimally invasive procedure and can be considered as a good alternative to reoperation [2–3, 5, 9–20] . Therefore, determining the risk factors for post-pancreaticoduode-nectomy bleeding and accumulating treatment experi-ence is of utmost importance for pancreatic surgeons.
The aims of this study are to determine the risk factors and outcome for post-pancreaticoduodenectomy bleed-ing. We also assess the roles of surgery and intravascular intervention by transarterial embolization or the place-ment of a covered stent in the management of post-pan-creaticoduodenectomy bleeding.
Materials and Methods
Clinical data were retrieved for analysis from our prospec-tively collected computer database of 628 patients with resectable periampullary lesions who underwent a pancreaticoduodenecto-my between January 1980 and December 2007. Detailed data re-garding the time and source of post-pancreaticoduodenectomy bleeding were also retrospectively assessed by a thorough review of medical records when possible. Based on the definitions and classifications of postpancreatectomy hemorrhage proposed by the International Study Group of Pancreatic Surgery (ISGPS) [21] , the cases were classified into ISGPS grades A, B and C, and cate-gorized into intraluminal or extraluminal, mild or severe, and early or late groups. Intraluminal post-pancreaticoduodenecto-my bleeding referred to bleeding inside the gastrointestinal tract, and extraluminal post-pancreaticoduodenectomy bleeding was in tra-abdominal bleeding outside the gastrointestinal tract. Ear-ly post-pancreaticoduodenectomy bleeding was defined as bleed-ing within 24 h after the pancreaticoduodenectomy, and latepost-pancreaticoduodenectomy bleeding was defined as bleeding more than 24 h after the pancreaticoduodenectomy.
The incidence, treatment modality and outcome of post-pan-creaticoduodenectomy bleeding were evaluated. A variety of risk factors for post-pancreaticoduodenectomy bleeding were deter-mined for univariate and multivariate analysis, including the type of pancreatic anastomosis, consistency of pancreas paren-chyma, pancreatic duct stenting, the diameter of pancreatic duct,
surgeon volume, patients’ age, pancreatic leakage, bile leakage, gastrojejunostomy leakage, intra-abdominal abscess formation, a primary periampullary lesion and serum levels of total bilirubin. To provide direct evidence of pancreatic anastomosis leakage, up-per gastrointestinal studies (oral intake of 2 ml of methylene blue dye plus 200 ml of water) or a fistulogram were performed in cases in which pancreatic leakage were suspected. Pancreatic leakage was defined as a leak of methylene blue dye into a drain or positive fistulogram findings during the postoperative period [4, 22] . Pancreas texture was determined by gross examination and significant fibrotic change by microscopic examination.
Surgical Technique Pancreaticoduodenectomiy was performed with either a pylo-
rus-preserving modification or a classic resection including an-trectomy. Pancreatic reconstruction could be done by a pancreati-cogastrostomy or pancreaticojejunostomy. The surgical technique (pancreaticogastrostomy or pancreaticojejunostomy) was selected according to the surgeon’s preference. In the pancreaticogastros-tomy group, the pancreatic stump was anastomosed and invagi-nated into the midbody posterior wall of the stomach with inter-rupted 2-layer sutures: 3-0 silk for the outer layer placed between the pancreatic capsule and seromuscular layer of the posterior gas-tric wall, and 3-0 polyglactin (Vicryl; Ethicon Inc., Somerville, N.J., USA) for the inner layer placed between the cut edge of the pan-creas and the full thickness of the posterior gastric wall. Pancre-atic duct stents were not used in the pancreaticogastrostomies. In the pancreaticojejunostomy group, pancreatico jejunostomies were performed by end-to-side, 2-layer sutures, using the same suture materials as for the pancreaticogastrostomies. The 1st layer suture was a duct-to-mucosa anastomosis with 6–8 sutures, and the 2nd layer suture was between the cutting edge of the pancreas and the seromuscular edge of the jejunum. A pancreatic duct stent was usu-ally used in the pancreaticojejunostomies. Two latex closed-suction tubes were used to drain the areas near the pancreatic anastomosis. For accurate and prompt localization of gastroduodenal artery bleeding, the gastroduodenal artery stump was routinely marked by 2 metallic clips after dividing it, starting in the year 2000.
Statistical Analysis Statistical analysis was carried out using the SPSS 16.0 soft-
ware program (Statistic Package for Social Sciences; SPSS Inc., Chicago, Ill., USA). All continuous data were presented as median and range. Categorical variables were compared by a � 2 test or Fisher’s exact test. A Mann-Whitney U test or Wilcoxon test was used to compare the continuous variables. Logistic regression multivariate analysis was carried out to determine the indepen-dent risk factors for post-pancreaticoduodenectomy bleeding. A p value ! 0.05 was considered statistically significant.
Results
Post-pancreaticoduodenectomy bleeding occurred in 58 of 628 patients (9.2%) who underwent a pancreatico-duodenectomy, including 21 intraluminal (36.2%) and 37 extraluminal (63.8%) types. There were 45 males and 13 females with a median age of 67 years (range 36–84).

Post-Pancreaticoduodenectomy Bleeding Dig Surg 2009;26:297–305 299
Overall, pancreaticoduodenectomy resulted in surgi-cal mortality in 7.0% of the patients (44/628), with 3.2% (10/309) in the pancreaticogastrostomy group and 10.7% (34/319) in the pancreaticojejunostomy group (p = 0.000). The mortality rate was 39.7% (23/58) for all patientswith post-pancreaticoduodenectomy bleeding, including 28.6% for the intraluminal type (6/21) and 45.9% for the extraluminal type (17/37; p = 0.194). Therefore, 52.3% (23/44) of the patients died as a result of post-pancre-aticoduodenectomy bleeding. Using univariate analy-sis, pancreatic leakage, bile leakage, gastrojejunostomy leakage and intra-abdominal abscess were risk factorsfor overall post-pancreaticoduodenectomy bleeding ( ta-ble 1 ). Post-pancreaticoduodenectomy bleeding occurred in 15 of the 61 patients (24.6%) with pancreatic leakage, 5 of the 19 patients (26.3%) with bile leakage, 3 of the 6 pa-tients (50.0%) with gastrojejunostomy leakage and 25 of the 69 patients (36.2%) with an intra-abdominal abscess. Although the overall incidence of pancreatic head cancer was highest among the periampullary cancers, the num-ber (246) of resected ampullary cancers was higher than that of resected pancreatic head cancers with lower re-sectability (174). Among the 58 patients with post-pan-creaticoduodenectomy bleeding, 25.9% were associated with pancreatic leakage, 8.6% with bile leakage, 5.2% with gastrojejunostomy leakage and 43.1% with intra-ab-dominal abscess. For extraluminal post-pancreaticoduo-denectomy bleeding, the type of pancreatic anastomosis, pancreatic leakage, gastrojejunostomy leakage and intra-abdominal abscess were risk factors. Pancreatic leakage and intra-abdominal abscess were risk factors for in-traluminal post-pancreaticoduodenectomy bleeding ( ta-ble 2 ).
After multivariate analysis ( table 3 ), pancreatic leak-age, gastrojejunostomy leakage and intra-abdominal abscess were still independent risk factors for overall post-pancreaticoduodenectomy bleeding and extralumi-nal post-pancreaticoduodenectomy bleeding. Pancreatic leakage and intra-abdominal abscess were independent risk factors for intraluminal post-pancreaticoduodenec-tomy bleeding.
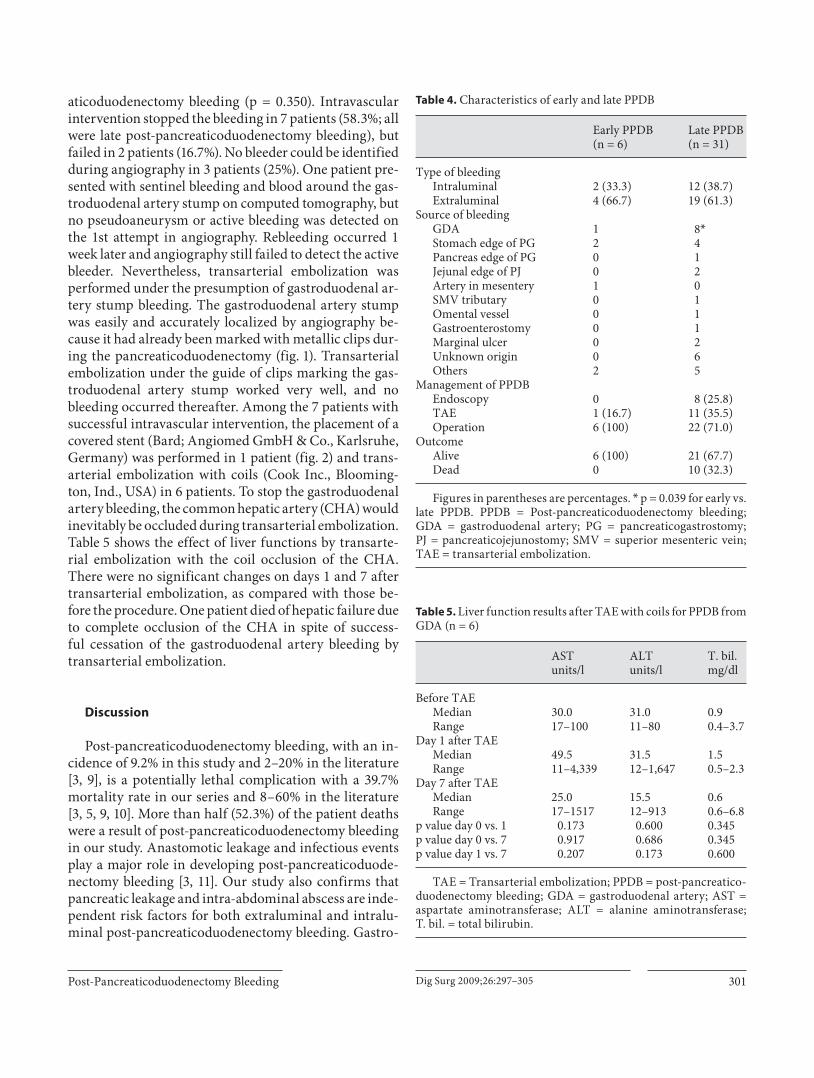
Among the 58 patients with post-pancreaticoduode-nectomy bleeding, determining the accurate time and lo-cation of the bleeding could be retrospectively assessed on 37 patients by a thorough review of their medical records, consisting of 6 early and 31 late post-pancreati-coduodenectomy bleeding cases ( table 4 ). According to ISGPS definition, our 37 cases of post-pancreaticoduo denectomy bleeding were classified into 1 grade A, 16grade B and 20 grade C cases. Ten belonged to mild post-
Table 1. Univariate analysis of risk factors for overall PPDB
Risk factor Overall PPDB pvalueno yes
Type of anastomosis 0.082PG (n = 309) 286 (92.6) 23 (7.4)PJ (n = 319) 284 (89.0) 35 (11.0)Pancreas texture 0.128Soft (n = 262) 239 (91.2) 23 (8.8)Hard (n = 168) 159 (94.6) 9 (5.4)Pancreatic duct stenting 0.342With (n = 183) 171 (93.4) 12 (6.6)Without (n = 247) 227 (91.9) 20 (8.1)Pancreatic duct 0.461Dilated (>5 mm) (n = 112) 103 (92.0) 9 (8.0)Nondilated (≤5 mm) (n = 318) 295 (92.8) 23 (7.2)Surgeon volume 0.370Low (<10) (n = 64) 55 (85.9) 9 (14.1)Medium (10–20) (n = 36) 33 (91.7) 3 (8.3)High (>20) (n = 528) 482 (91.3) 46 (8.7)Age 0.490≤65 years (n = 288) 262 (91.0) 26 (9.0)>65 years (n = 340) 308 (90.6) 32 (9.4)Pancreatic leakage 0.000Yes (n = 61) 46 (75.4) 15 (24.6)No (n = 567) 524 (92.4) 43 (7.6)Bile leakage 0.024Yes (n = 19) 14 (73.7) 5 (26.3)No (n = 609) 556 (91.3) 53 (8.7)Gastrojejunostomy leakage 0.012Yes (n = 6) 3 (50.0) 3 (50.0)No (n = 622) 567 (91.2) 55 (8.8)Intra-abdominal abscess 0.000Yes (n = 69) 44 (63.8) 25 (36.2)No (n = 559) 526 (94.1) 33 (5.9)Primary lesions 0.128Ampullary cancer (n = 246) 217 (88.2) 29 (11.8)Duodenal cancer (n = 37) 33 (89.2) 4 (10.8)Distal CBD cancer (n = 54) 46 (85.2) 8 (14.8)Pancreatic head cancer (n = 174) 165 (94.8) 9 (5.2)IPMN (n = 27) 23 (85.2) 4 (14.8)Chronic pancreatitis (n = 38) 37 (97.4) 1 (2.6)Others (n = 52) 49 (94.2) 3 (5.8)Total serum bilirubin level 0.331≥15 mg/dl (n = 320) 289 (90.3) 31 (9.7)<15 mg/dl (n = 102) 90 (88.2) 12 (11.8)
Figures in parentheses are percentages. PPDB = Post-pancre-aticoduodenectomy bleeding; PG = pancreaticogastrostomy; PJ = pancreaticojejunostomy; CBD = common bile duct; IPMN = in-traductal papillary mucinous neoplasm.

Wei /Wang /Shyr /Tseng /Tsai /Chen /Su /Wu /Lui
Dig Surg 2009;26:297–305300
pancreaticoduodenectomy bleeding and 27 belonged to severe post-pancreaticoduodenectomy bleeding. There were no deaths from early post-pancreaticoduodenec-tomy bleeding, but 10 deaths (32.3%) from late post-pancreaticoduodenectomy bleeding (p = 0.127). In early
post-pancreaticoduodenectomy bleeding cases, there were 2 intraluminal (33.3%) and 4 extraluminal bleeding (66.7%) cases. In late post-pancreaticoduodenectomy bleeding cases, there were 12 intraluminal (38.7%) and 19 extraluminal bleeding (61.3%). The most common source of post-pancreaticoduodenectomy bleeding was the gas-troduodenal artery occurring in 24.3% of the cases (9/37), of which 88.9% (8/9) were late post-pancreaticoduode-nectomy bleeding (p = 0.039). While the gastroduodenal artery (25.8%) was the most common site of late post-pancreaticoduodenectomy bleeding, the stomach edgeof the pancreaticogastrostomy (33.3%) was the most common site in early post-pancreaticoduodenectomy bleeding. 28 patients (75.7%) underwent reoperation for post-pancreaticoduodenectomy bleeding, and 12 patients (32.4%) received intravascular intervention. All 6 patients (100%) with early post-pancreaticoduodenectomy bleed-ing eventually underwent an operation for bleeding, while only 22 patients (71.0%) with late post-pancreatico-duodenectomy bleeding were treated so (p = 0.162). Sur-gery achieved hemostasis in 22 patients (78.6%; 6 early bleeding, 16 late bleeding) and failed in 4 (14.3%). No bleeder could be found during operation in 2 patients (7.1%). Intravascular intervention was attempted in 1 pa-tient (16.7%) with early post-pancreaticoduodenectomy bleeding and 11 patients (35.5%) with late post-pancre-
Table 2. Univariate analysis of risk factors for extraluminal and intraluminal PPDB
Risk factor Extraluminal PPDB p value Intraluminal PPDB p value
no yes no yes
Type of anastomosis 0.040 0.055PG (n = 309) 296 (95.8) 13 (4.2) 299 (96.8) 10 (3.2)PJ (n = 319) 294 (92.2) 25 (7.8) 299 (93.7) 20 (6.3)
Pancreatic leakage 0.000 0.000Yes (n = 61) 49 (80.3) 12 (19.7) 51 (83.6) 10 (16.4)No (n = 567) 541 (95.4) 26 (4.6) 547 (96.5) 20 (3.5)
Bile leakage 0.101 0.229Yes (n = 19) 16 (84.2) 3 (15.8) 17 (89.5) 2 (10.5)No (n = 609) 574 (94.3) 35 (5.7) 581 (95.4) 28 (4.6)
Gastrojejunostomy leakage 0.046 0.255Yes (n = 6) 4 (66.7) 2 (33.3) 5 (83.3) 1 (16.7)No (n = 622) 586 (94.2) 36 (5.8) 593 (95.3) 29 (4.7)
Intra-abdominal abscess 0.000 0.000Yes (n = 69) 49 (71.0) 20 (29.0) 57 (82.6) 12 (17.4)No (n = 559) 541 (96.8) 18 (3.2) 541 (96.8) 18 (3.2)
Figures in parentheses are percentages. PPDB = Post-pancreaticoduodenectomy bleeding; PG = pancreati-cogastrostomy; PJ = pancreaticojejunostomy.
Table 3. Independent risk factors for PPDB by multivariate anal-ysis
Risk factors p value OR CI
Overall PPDBPancreatic leakage 0.000 3.579 1.789–6.123Bile leakage 0.235 2.051 0.627–6.706Gastrojejunostomy leakage 0.017 9.183 1.493–56.494Intra-abdominal abscess 0.000 7.828 4.231–14.481
Extraluminal PPDBOperation type 0.888 1.058 0.484–2.312Pancreatic leakage 0.002 3.850 1.636–9.061Gastrojejunostomy leakage 0.026 9.344 1.315–66.408Intra-abdominal abscess 0.000 11.073 5.317–23.057
Intraluminal PPDBPancreatic leakage 0.000 4.947 2.253–10.860Intra-abdominal abscess 0.000 4.539 2.071–9.951
PPDB = Post-pancreaticoduodenectomy bleeding; OR = odds ratio; CI = 95% confidence interval.
Post-Pancreaticoduodenectomy Bleeding Dig Surg 2009;26:297–305 301
aticoduodenectomy bleeding (p = 0.350). Intravascular intervention stopped the bleeding in 7 patients (58.3%; all were late post-pancreaticoduodenectomy bleeding), but failed in 2 patients (16.7%). No bleeder could be identified during angiography in 3 patients (25%). One patient pre-sented with sentinel bleeding and blood around the gas-troduodenal artery stump on computed tomography, but no pseudoaneurysm or active bleeding was detected on the 1st attempt in angiography. Rebleeding occurred 1 week later and angiography still failed to detect the active bleeder. Nevertheless, transarterial embolization was performed under the presumption of gastroduodenal ar-tery stump bleeding. The gastroduodenal artery stump was easily and accurately localized by angiography be-cause it had already been marked with metallic clips dur-ing the pancreaticoduodenectomy ( fig. 1 ). Transarterial embolization under the guide of clips marking the gas-troduodenal artery stump worked very well, and no bleeding occurred thereafter. Among the 7 patients with successful intravascular intervention, the placement of a covered stent (Bard; Angiomed GmbH & Co., Karlsruhe, Germany) was performed in 1 patient ( fig. 2 ) and trans-arterial embolization with coils (Cook Inc., Blooming-ton, Ind., USA) in 6 patients. To stop the gastroduodenal artery bleeding, the common hepatic artery (CHA) would inevitably be occluded during transarterial embolization. Table 5 shows the effect of liver functions by transarte-rial embolization with the coil occlusion of the CHA. There were no significant changes on days 1 and 7 after transarterial embolization, as compared with those be-fore the procedure. One patient died of hepatic failure due to complete occlusion of the CHA in spite of success-ful cessation of the gastroduodenal artery bleeding by transarterial embolization.
Discussion
Post-pancreaticoduodenectomy bleeding, with an in-cidence of 9.2% in this study and 2–20% in the literature [3, 9] , is a potentially lethal complication with a 39.7% mortality rate in our series and 8–60% in the literature [3, 5, 9, 10] . More than half (52.3%) of the patient deaths were a result of post-pancreaticoduodenectomy bleeding in our study. Anastomotic leakage and infectious events play a major role in developing post-pancreaticoduode-nectomy bleeding [3, 11] . Our study also confirms that pancreatic leakage and intra-abdominal abscess are inde-pendent risk factors for both extraluminal and intralu-minal post- pancreaticoduodenectomy bleeding. Gastro-
Table 4. Characteristics of early and late PPDB
Early PPDB(n = 6)
Late PPDB(n = 31)
Type of bleedingIntraluminal 2 (33.3) 12 (38.7)Extraluminal 4 (66.7) 19 (61.3)
Source of bleedingGDA 1 8*Stomach edge of PG 2 4Pancreas edge of PG 0 1Jejunal edge of PJ 0 2Artery in mesentery 1 0SMV tributary 0 1Omental vessel 0 1Gastroenterostomy 0 1Marginal ulcer 0 2Unknown origin 0 6Others 2 5
Management of PPDBEndoscopy 0 8 (25.8)TAE 1 (16.7) 11 (35.5)Operation 6 (100) 22 (71.0)
OutcomeAlive 6 (100) 21 (67.7)Dead 0 10 (32.3)
Figures in parentheses are percentages. * p = 0.039 for early vs. late PPDB. PPDB = Post-pancreaticoduodenectomy bleeding; GDA = gastroduodenal artery; PG = pancreaticogastrostomy;PJ = pancreaticojejunostomy; SMV = superior mesenteric vein; TAE = transarterial embolization.
Table 5. Liver function results after TAE with coils for PPDB from GDA (n = 6)
ASTunits/l
ALTunits/l
T. bil.mg/dl
Before TAEMedian 30.0 31.0 0.9Range 17–100 11–80 0.4–3.7
Day 1 after TAEMedian 49.5 31.5 1.5Range 11–4,339 12–1,647 0.5–2.3
Day 7 after TAEMedian 25.0 15.5 0.6Range 17–1517 12–913 0.6–6.8
p value day 0 vs. 1 0.173 0.600 0.345p value day 0 vs. 7 0.917 0.686 0.345p value day 1 vs. 7 0.207 0.173 0.600
TAE = Transarterial embolization; PPDB = post-pancreatico-duodenectomy bleeding; GDA = gastroduodenal artery; AST = aspartate aminotransferase; ALT = alanine aminotransferase;T. bil. = total bilirubin.

Wei /Wang /Shyr /Tseng /Tsai /Chen /Su /Wu /Lui
Dig Surg 2009;26:297–305302
Patient CHA with a covered stent
GDA bleeding
X2 Distance: 5.90 mm X2
X1 Distance: 6.96 mmX1
GDA stump marked with clipsTAE with coils for CHA andGDA stump marked with clips
Fig. 1. No active bleeder or pseudoaneurysm could be identified during the 1st angiographic attempt for an episode of sentinel bleeding. Note that the gastroduodenal artery (GDA) stump was marked by clips (left pic-ture). Transarterial embolization (TAE) was still successfully performed for the intermittent bleeding of the GDA stump clearly marked by clips (right picture).
Fig. 2. A pseuodoaneurysm with bleeding from the GDA stump marked with clips was noted on angiography (left picture). Angiography of a patient’s CHA with a covered stent (right picture).

Post-Pancreaticoduodenectomy Bleeding Dig Surg 2009;26:297–305 303
jejunostomy leakage is another independent risk factor for extraluminal post-pancreaticoduodenectomy bleed-ing.
Patients with post-pancreaticoduodenectomy bleed-ing are divided into early and late groups because the pathogenesis and optimal management might differ. Management of the early group is usually more straight-forward with a better outcome compared to the late group [1, 3, 9] . In our series, bleeding from the stomach edge of the pancreaticogastrostomy (33.3%) was the most com-mon site in the early group. Additionally, all early group patients and 71.0% of the late group patients eventually underwent reoperation. The outcome seemed favorable in the early group as no deaths occurred, but mortality was 32.3% in the late group. Early post-pancreaticoduo-denectomy bleeding was more likely to be related to some surgical mishap [3, 9] . The common sites for early post-pancreaticoduodenectomy bleeding could be the suture line of the anastomosis, the pancreatic cut surface, a stress or marginal ulcer, a slipped ligature or a large oozing raw area of the operative site. Therefore, patients with early massive post-pancreaticoduodenectomy bleeding should undergo prompt surgical reintervention until proven otherwise [1, 3, 9] . We propose a management algorithm
for early post-pancreaticoduodenectomy bleeding as shown in figure 3 .
Late post-pancreaticoduodenectomy bleeding is often associated with anastomotic leakage, especially from pancreatic anastomosis, and intra-abdominal infection [1–3, 9, 11, 23, 24] . Approximately two thirds of the re-ported cases of late arterial post-pancreaticoduodenec-tomy bleeding are found to have an underlying fluid col-lection or anastomotic leakage, with a pseudoaneurysm formation identified in approximately one third of the cases [3, 10] . It is hypothesized that late post-pancreatico-duodenectomy bleeding might be caused by erosion of the vasculature resulting from intra-abdominal contam-ination of enteric, pancreatic or bile juice in the area adjacent to the surgical anastomosis [2, 3, 9, 11, 23, 24] . Surgery has always been the treatment of choice for late post-pancreaticoduodenectomy bleeding [10, 25, 26] . However, a surgical approach to late post-pancreaticodu-odenectomy bleeding is often unsuccessful due to severe adhesion, extensive oozing, edematous tissue and inac-cessibility to these vessels, owing to adjacent pancreatic anastomosis [3, 5, 27] . Moreover, suture control of the eroded bleeding vessels is difficult due to local sepsis, se-vere peripancreatic inflammation and friable tissue and vessel walls [3, 27] . Incidence of rebleeding after ligation of the bleeding vessels is as high as 63%, and remains the main cause of death in such patients [3, 20, 27] .
A pretreatment diagnosis would be helpful in the se-lection of the optimal treatment for late post-pancreati-coduodenectomy bleeding [9] , and interventional angi-ography has recently emerged as a safe and effective first-line tool [1–3, 5, 9–11] . Encouraging results have been reported with intravascular intervention as it offers a minimally invasive approach in obtaining hemostasis with a success rate between 63 and 85% [2, 3, 5, 28] . As shown in this study and the literature, the most common site of late post-pancreaticoduodenectomy bleeding is the gastroduodenal artery stump. Its bleeding can be easily detected and effectively resolved by intravascular inter-vention [3, 5, 9, 10, 12, 13, 25] . One would think that an-giography should be the most sensitive and specific diag-nostic test for pseudoaneurysms and late post-pancreati-coduodenectomy bleeding. However, 25% of the bleeders in our post-pancreaticoduodenectomy bleeding cases could not be identified during angiography. It might be hypothesized that there is a clot in the pseudoaneurysm that obscures visualization even when the patient is ac-tively bleeding [9] , or the bleeding is intermittent in na-ture [3] . To improve the identification rate of the gastro-duodenal artery stump during angiography, we routinely
Early PPDB (<1st postoperative day)
Intraluminal Extraluminal
Endoscopy Surgery
PPDB control PPDB not control
Angiography
PPDB control PPDB not control
Surgery
Fig. 3. Management algorithm for early post-pancreaticoduode-nectomy bleeding (PPDB).

Wei /Wang /Shyr /Tseng /Tsai /Chen /Su /Wu /Lui
Dig Surg 2009;26:297–305304
mark the gastroduodenal artery stump with metallic clips during the pancreaticoduodenectomy. We believe this prevents gastroduodenal artery bleeding from being overlooked, and successful intravascular intervention can still be performed under the guide of clips on the gas-troduodenal artery stump. Our successful experience of intravascular intervention in the patients presenting with sentinel bleeding and rebleeding confirms this policy and encourages us to continue to do so in the future. In agree-ment with other authors [5] , we strongly suggest that an emergency angiography should be considered for all pa-tients who develop either sentinel or massive late post-pancreaticoduodenectomy bleeding, with the added ben-efit that intravascular intervention might prevent the need for a high-risk emergency operation ( fig. 4 ).
Transarterial embolization with a coil occlusion of the CHA may lead to a complete interruption of arterial blood supply to liver, which might result in cholangitis, biliary ischemia, a hepatic abscess or fatal hepatic failure as occurred in 1 of our patients [2, 19, 29] . Our cases also show that the recent use of covered stents may prove to be a successful solution to resolve this issue. A covered stent makes it possible to arrest the bleeding while preserving
the patency of the vessels [3, 10, 12, 15–17] . Potential dis-advantages of the covered stent include a longer duration to achieve hemostasis as compared to transarterial embo-lization, risk of arterial rupture due to low flexibility and fragile vascular walls, and technical difficulties in nego-tiating with torturous arteries [3] .
In conclusion, post-pancreaticoduodenectomy bleed-ing continues to be a potentially lethal complication and is the major cause of surgical mortality after a pancreati-coduodenectomy. Intra-abdominal abscess and anasto-motic leakage, such as pancreatic and gastrojejunostomy leakage, are independent risk factors for post-pancreati-coduodenectomy bleeding. Placement of metallic clips on the gastroduodenal artery stump during a pancreatico-duodenectomy is very helpful in the identification of an overlooked pseudoaneurysm or intermittent sentinel bleeding from the gastroduodenal artery stump during angiography. Although transarterial embolization of the CHA is safe in most patients with gastroduodenal artery bleeding, it cannot guarantee against hepatic failure. The intravascular placement of a covered stent is a preferred solution to avoid a complete interruption of arterial blood supply to liver.
Late PPDB (after 1st postoperative day)
Intraluminal
Endoscopy
PPDB control PPDB not control
Angiography
Surgery
PPDB control PPDB not control
Extraluminal
(either sentinel of massive)
Angiography
Bleeder
visualizable
TAE or covered
stent
Bleeder not
visualizable
Covered stent
at GDA stump
if highly
suspected
Surgery
PPDB control PPDB not control
Fig. 4. Management algorithm for late PPDB.

Post-Pancreaticoduodenectomy Bleeding Dig Surg 2009;26:297–305 305
References
1 Yekebas EF, Wolfram L, Cataldegirmen G, et al: Postpancreatectomy hemorrhage: diag-nosis and treatment: an analysis in 1,669 consecutive pancreatic resections. Ann Surg 2007; 246: 269–280.
2 de Castro SM, Kuhlmann KF, Busch OR, et al: Delayed massive hemorrhage after pan-creatic and biliary surgery: embolization or surgery? Ann Surg 2005; 241: 85–91.
3 Jagad RB, Koshariya M, Kawamoto J, Chude GS, Neeraj RV, Lygidakis NJ: Postoperative hemorrhage after major pancreatobiliary surgery: an update. Hepatogastroenterology 2008; 55: 729–737.
4 Fang WL, Shyr YM, Su CH, Chen TH, Wu CW, Lui WY: Comparison between pancre-aticojejunostomy and pancreaticogastrosto-my after pancreaticoduodenectomy. J For-mos Med Assoc 2007; 106: 717–727.
5 Sato N, Yamaguchi K, Shimizu S, et al: Coil embolization of bleeding visceral pseudo-aneurysms following pancreatectomy. Arch Surg 1998; 133: 1099–1102.
6 Sato N, Yamaguchi K, Chijiiwa K, Tanaka M: Risk analysis of pancreatic fistula after pan-creatic head resection. Arch Surg 1998; 133: 1094–1098.
7 Van Berge Henegouwen MI, De Wit LT, Van Gulik TM, Obertop H, Gouma DJ: Inci-dence, risk factors, and treatment of pancre-atic leakage after pancreaticoduodenec tomy: drainage versus resection of the pancreatic remnant. J Am Coll Surg 1997; 185: 18–24.
8 Shyr YM, Wang SE, Chen TH, Su CH, Wu CW: Pancreaticogastrostomy after pancre-aticoduodenectomy. Formos J Surg 2008; 41: 81–85.
9 Ellison EC: Evidence-based management of hemorrhage after pancreaticoduodenecto-my. Am J Surg 2007; 194: 10–12.
10 Khorsandi SE, Limongelli P, Jackson JE, Tait P, Williamson RC, Habib NA, Jiao LR: Man-agement of delayed arterial hemorrhage af-ter pancreaticoduodenectomy. A case series. JOP 2008; 9: 172–178.
11 Tien YW, Lee PH, Yang CY, Ho MC, Chiu YF: Risk factors of massive bleeding related to pancreatic leak after pancreaticoduode-nectomy. J Am Coll Surg 2005; 201: 554–559.
12 Mansueto G, D’Onofrio M, Iacono C, Roz-zanigo U, Serio G, Procacci C: Gastroduode-nal artery stump haemmorrhage following pylorus-sparing Whipple procedure: treat-ment with covered stents. Dig Surg 2002; 19: 237–240.
13 Strigler B, von Rahden BHA, Weiss W, Stein HJ: Interventional radiology for manage-ment of celiac trunk bleeding after pancre-atic surgery. J Am Coll Surg 2006; 202: 1018–1019.
14 Blanc T, Cortes A, Goere D, et al: Hemor-rhage after pancreaticoduodenectomy: when is surgery still indicated? Am J Surg 2007; 194: 3–9.
15 Kaw LL Jr, Saeed M, Brunson M, Delaria GA, Dilley RB: Use of a stent graft for bleeding hepatic artery pseudoaneurysm following pancreaticoduodenectomy. Asian J Surg 2006; 29: 283–286.
16 Heiss P, Bachthaler M, Hamer OW, et al: De-layed visceral arterial hemorrhage following Whipple’s procedure: minimally invasive treatment with covered stents. Ann Surg On-col 2008; 15: 824–832.
17 Stoupis C, Ludwig K, Inderbitzin D, Do DD, Triller J: Stent grafting of acute hepatic ar-tery bleeding following pancreatic head re-section. Eur Radiol 2007; 17: 401–408.
18 Wente MN, Shrikhande SV, Kleeff J, et al: Management of early hemorrhage from pan-creatic anastomoses after pancreaticoduo-denectomy. Dig Surg 2006; 23: 203–208.
19 Yoon YS, Kim SW, Her KH, et al: Manage-ment of postoperative hemorrhage after pan-creatoduodenectomy. Hepatogastroenterol-ogy 2003; 50: 2208–2212.
20 Santoro R, Carlini M, Carboni F, Nicolas C, Santoro E: Delayed massive arterial hemor-rhage after pancreaticoduodenectomy for cancer. Management of a life-threatening complication. Hepatogastroenterology 2003; 50: 2199–2204.
21 Wente MN, Veit JA, Bassi C, et al: Postpan-createctomy hemorrhage (PPH): an Interna-tional Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007; 132: 20–25.
22 Shyr YM, Su CH, Wu CW, Lui WY: Does drainage fluid amylase reflect pancreatic leakage after pancreaticoduodenectomy? World J Surg 2003; 27: 606–610.
23 Choi SH, Moon HJ, Heo JS, Joh JW, Kim YI: Delayed hemorrhage after pancreaticoduo-denectomy. J Am Coll Surg 2004; 199: 186–191.
24 Koukoutsis I, Bellagamba R, Morris-Stiff G, Wickremesekera S, Coldham C, Wigmore SJ, et al: Haemorrhage following pancreati-coduodenectomy: risk factors and the im-portance of sentinel bleed. Dig Surg 2006; 23: 224–228.
25 Brodsky JT, Turnbull AD: Arterial hemor-rhage after pancreatoduodenectomy. The ‘sentinel bleed’. Arch Surg 1991; 126: 1037–1040.
26 van Berge Henegouwen MI, Allema JH, van Gulik TM, Verbeek PC, Obertop H, Gouma DJ: Delayed massive haemorrhage after pan-creatic and biliary surgery. Br J Surg 1995; 82: 1527–1531.
27 Balachandran P, Sikora SS, Raghavendra Rao RV, Kumar A, Saxena R, Kapoor VK: Haemorrhagic complications of pancreati-coduodenectomy. ANZ J Surg 2004; 74: 945–950.
28 Okuno A, Miyazaki M, Ito H, et al: Nonsur-gical management of ruptured pseudoaneu-rysm in patients with hepatobiliary pancre-atic disease. Am J Gastroenterol 2001; 96: 1067–1071.
29 Noun R, Zeidan S, Tohme-Noun C, Smayra T, Sayegh R: Biliary ischemia following em-bolization of a pseudoaneurysm after pan-creaticoduodenectomy. JOP 2006; 7: 427–431.