acs: bleeding risk, bleeding and clinical outcomes · acs: bleeding risk, bleeding and clinical...
TRANSCRIPT
ACS: Bleeding Risk, Bleeding and Clinical Outcomes
Joaquin E. Cigarroa, MDClinical Chief of Cardiology
Clinical Professor of MedicineOHSU
Conflict of Interest
• I DO Not Have any relevant financial relationships to disclose.
• I will stay within evidence-based guidelines and away from commercial recommendations.
Clinical Case
• 76 year old woman admitted with intermittent chest discomfort
• Past Med Hx: diabetes, dyslipidemia, obesity, TIA
• Outpatient medications:Aspirin 81 mg dailySimvastatinMetforminGlipizide
• Physical exam:Vitals: 185 lbs, HR 92, BP 148/80Clear lungsCor: nonpalpable PMI, RRR, quiet S1 and S2,
no murmurs, normal JVPAbd: obeseExt: no edema, 1 plus pulses
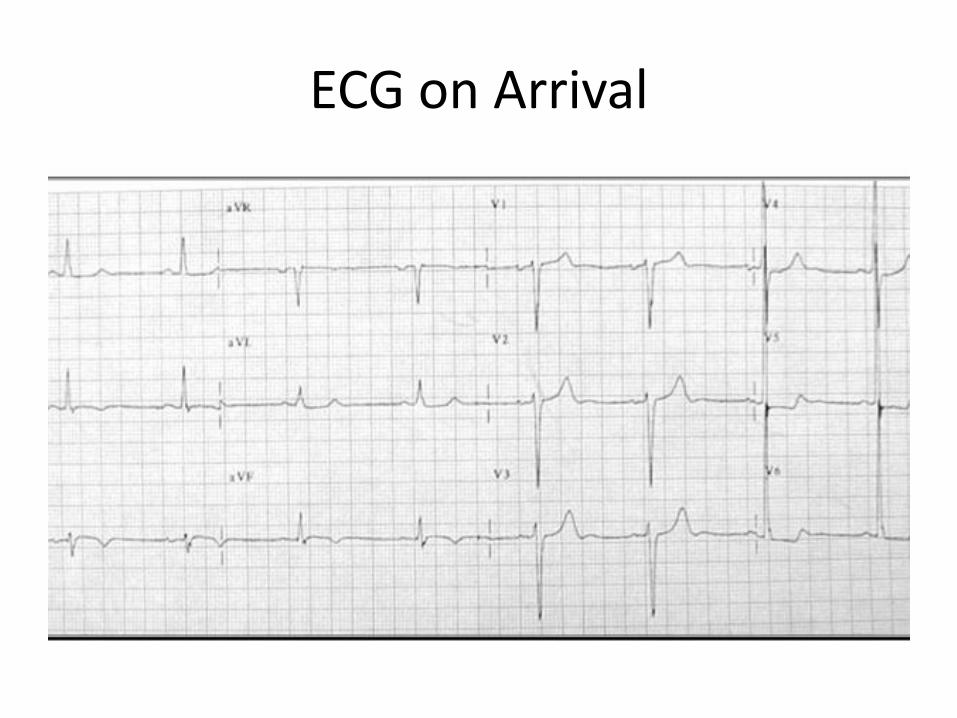
ECG on Arrival
• Labs:troponin I 5.6HCT 32%Platelets 168,000Creat 1.4 (creat clearance of 30 ml/min)
Management Strategy
• What medical therapies?1. Antiplatelet:
a. Aspirinb. Clopidogrelc. Prasugreld. Ticagrelore. iv glycoprotein 2b/3a
inhibitor
• Antithrombotic therapies?1. Unfractionated Heparin2. Low molecular Heparin3. Fondaparinux4. Bivalirudin
What is Her Bleeding Risk
• 1. <2%
• 2. 2-5%
• 3. 5-10%
• 4. 11-15%
• 5. > 15%
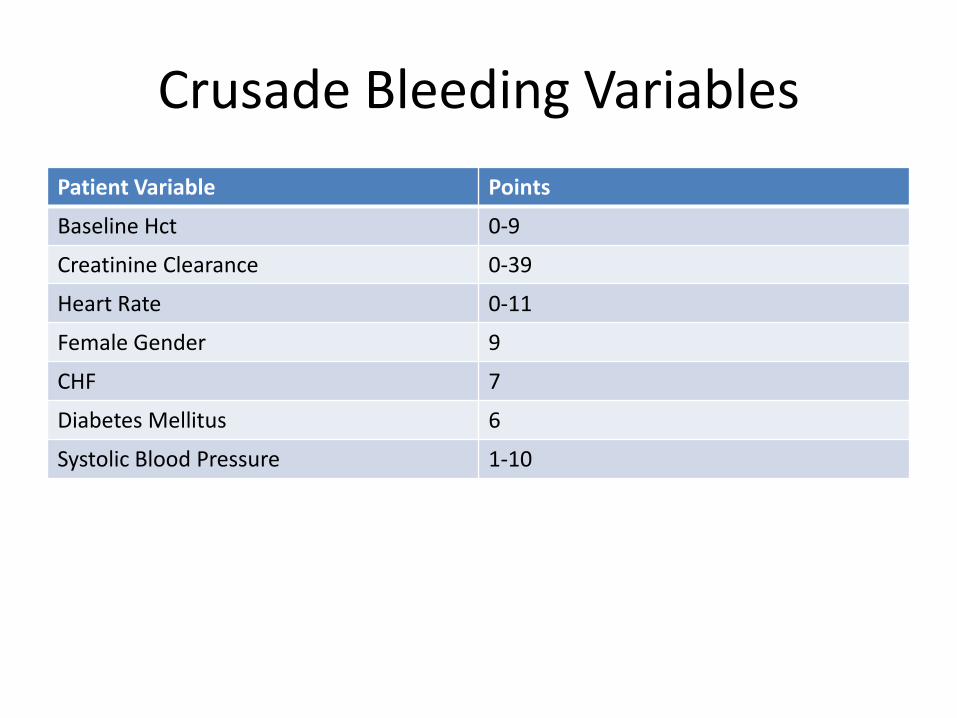
Crusade Bleeding Variables
Patient Variable Points
Baseline Hct 0-9
Creatinine Clearance 0-39
Heart Rate 0-11
Female Gender 9
CHF 7
Diabetes Mellitus 6
Systolic Blood Pressure 1-10
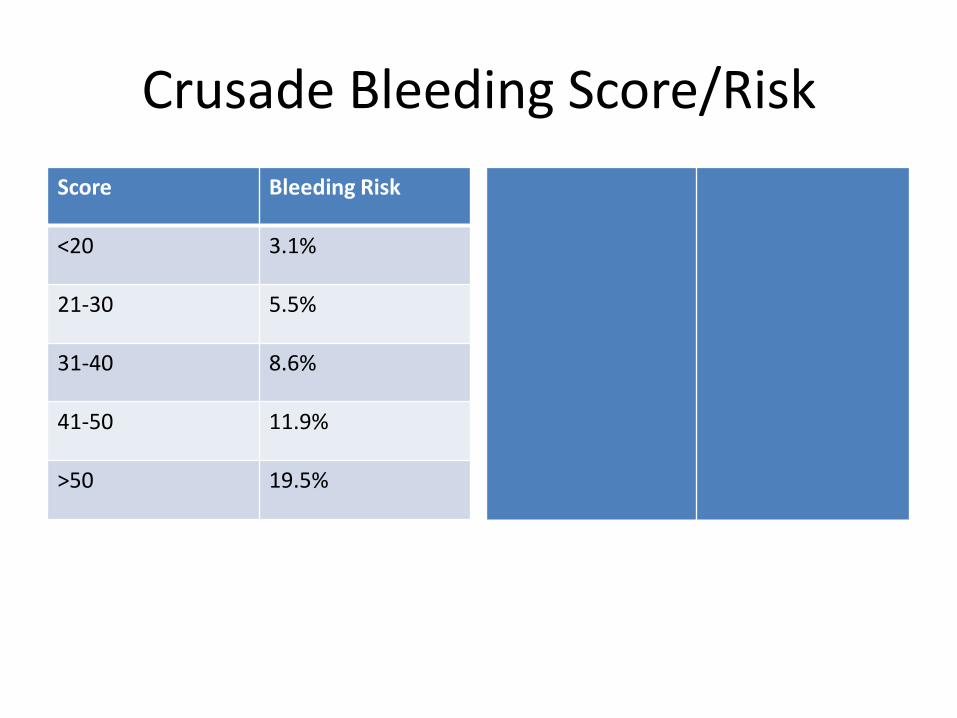
Crusade Bleeding Score/Risk
Score Bleeding Risk
<20 3.1%
21-30 5.5%
31-40 8.6%
41-50 11.9%
>50 19.5%
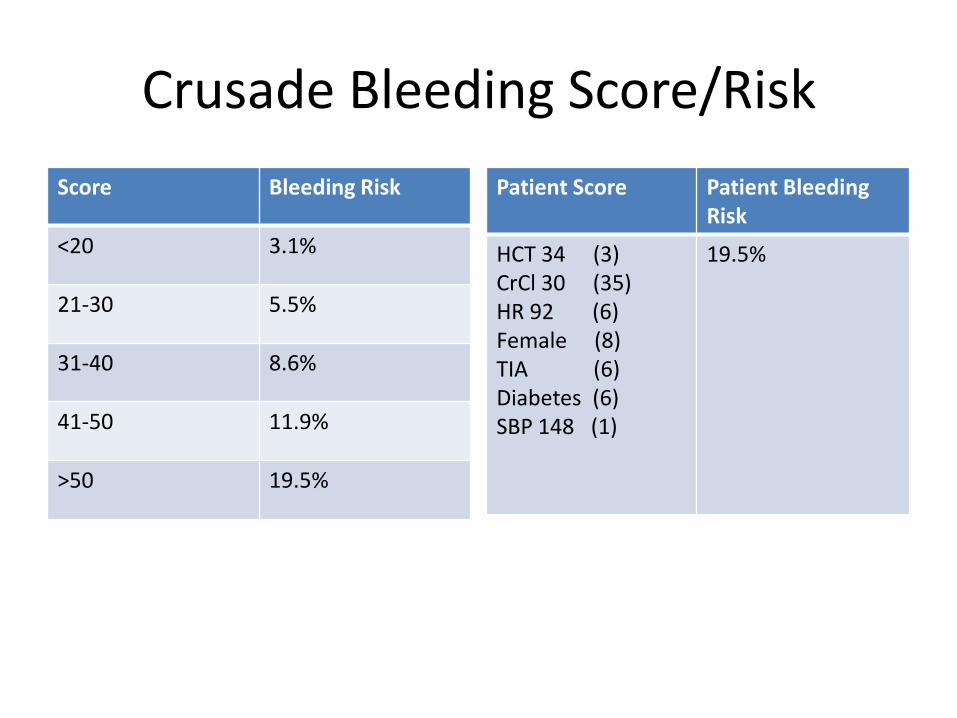
Crusade Bleeding Score/Risk
Score Bleeding Risk
<20 3.1%
21-30 5.5%
31-40 8.6%
41-50 11.9%
>50 19.5%
Patient Score Patient Bleeding Risk
HCT 34 (3)CrCl 30 (35)HR 92 (6)Female (8)TIA (6)Diabetes (6)SBP 148 (1)
19.5%
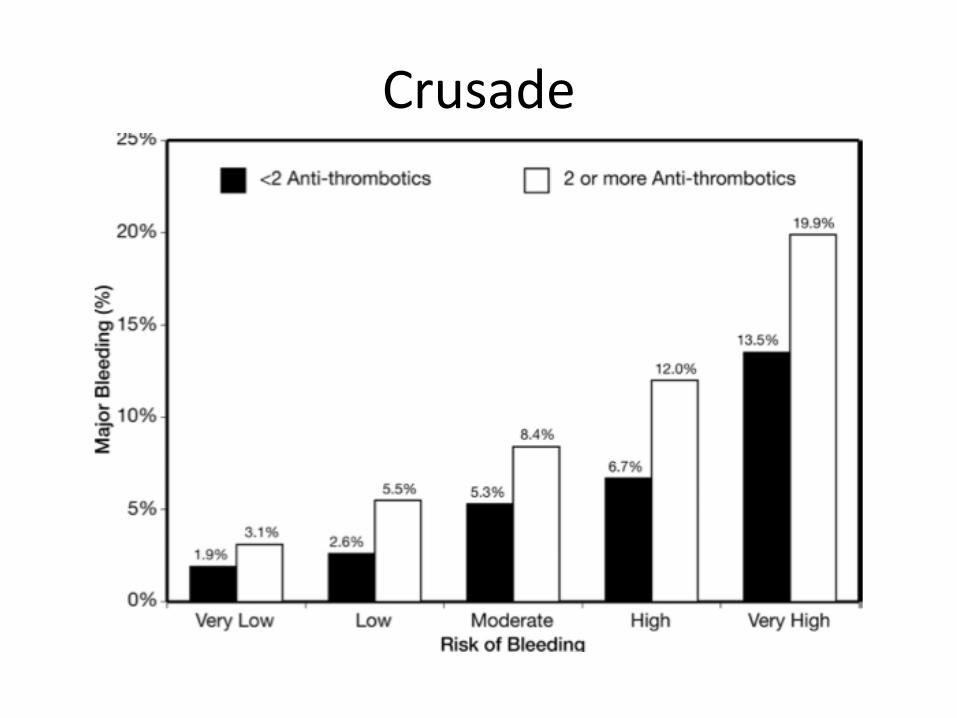
Crusade
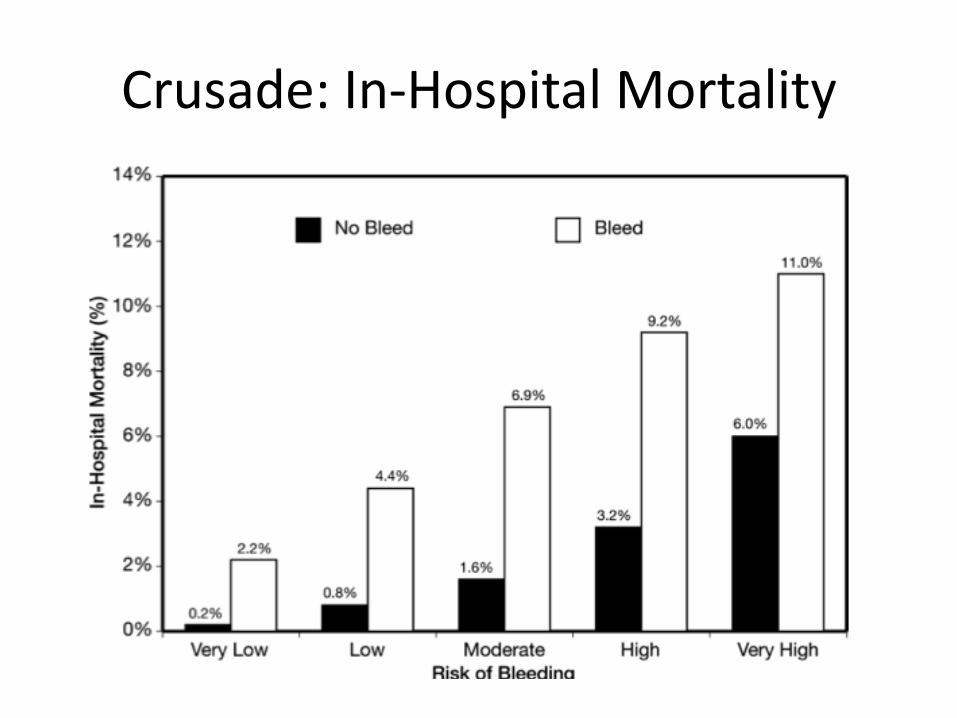
Crusade: In-Hospital Mortality
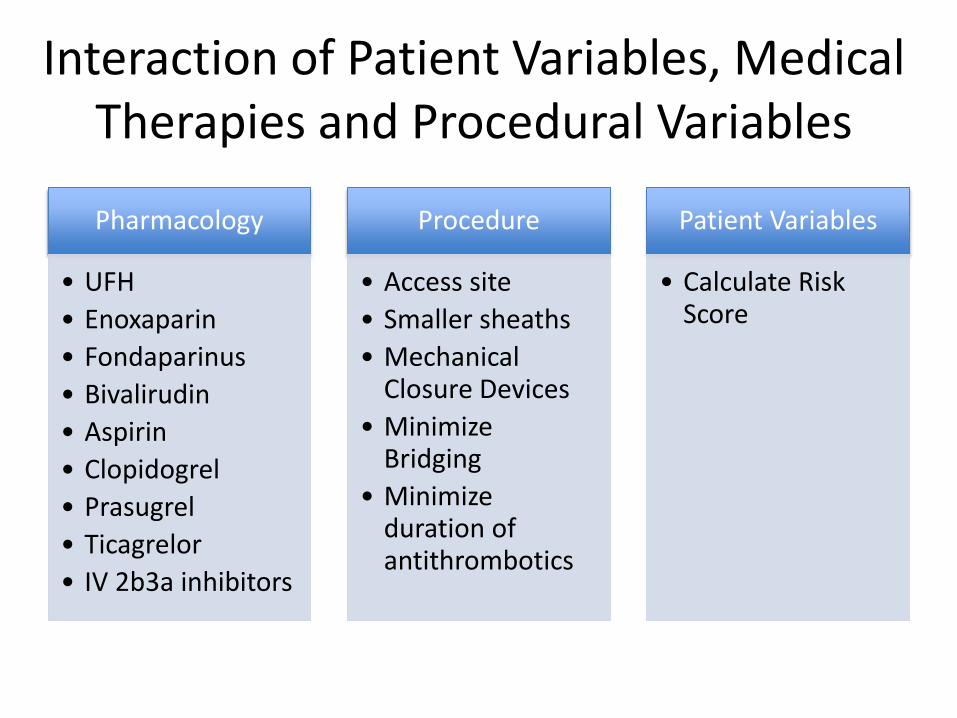
Interaction of Patient Variables, Medical Therapies and Procedural Variables
Pharmacology
• UFH
• Enoxaparin
• Fondaparinus
• Bivalirudin
• Aspirin
• Clopidogrel
• Prasugrel
• Ticagrelor
• IV 2b3a inhibitors
Procedure
• Access site
• Smaller sheaths
• Mechanical Closure Devices
• Minimize Bridging
• Minimize duration of antithrombotics
Patient Variables
• Calculate Risk Score
• What medical therapies would you recommend on this patient?
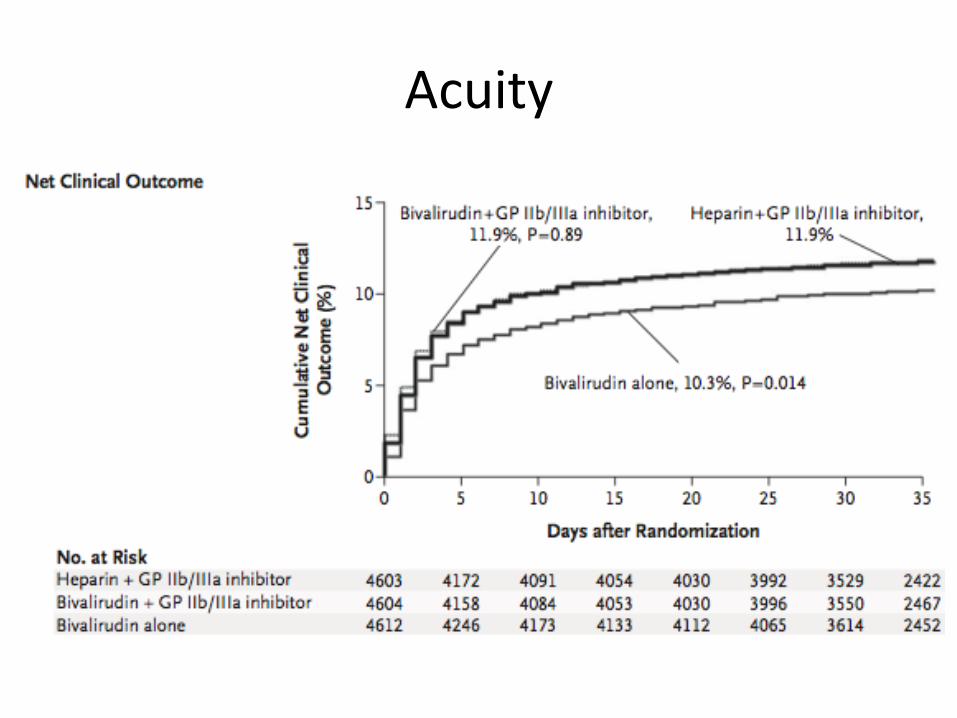
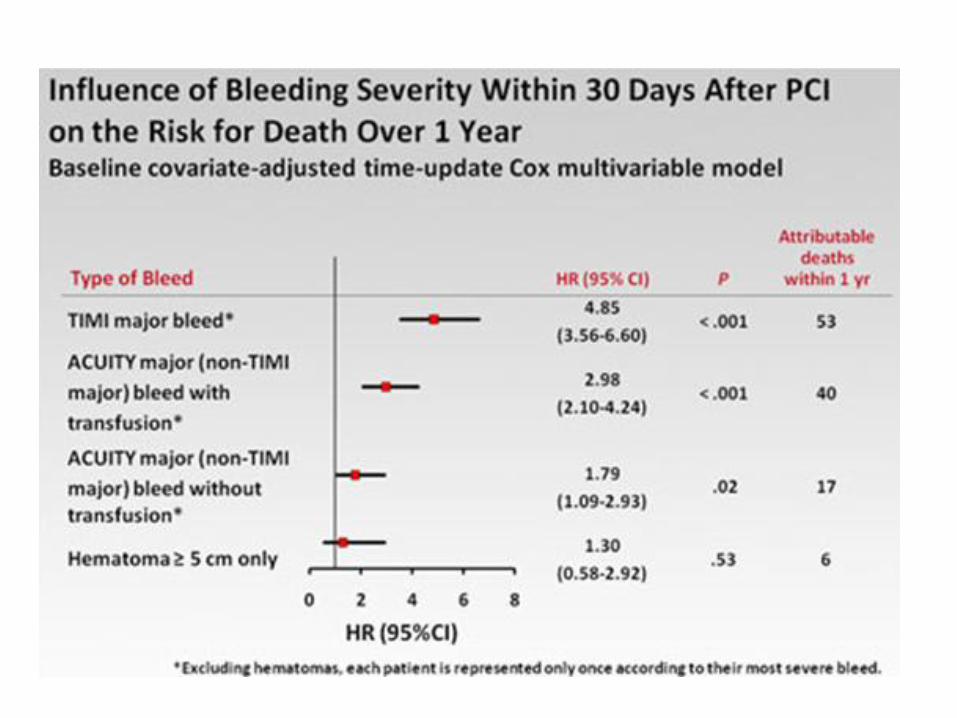
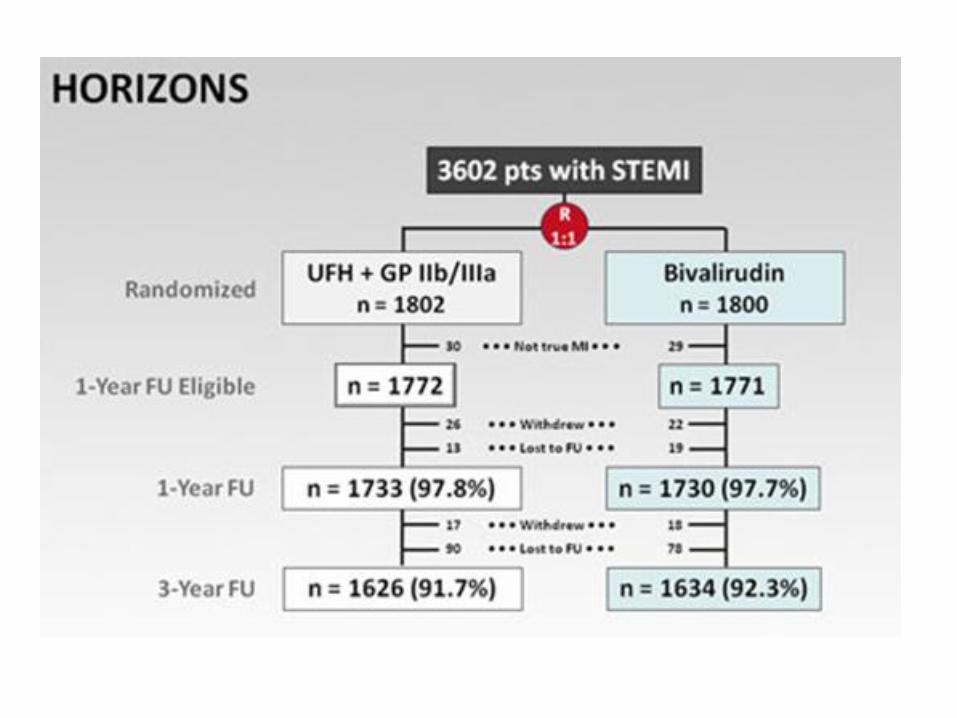
Acuity
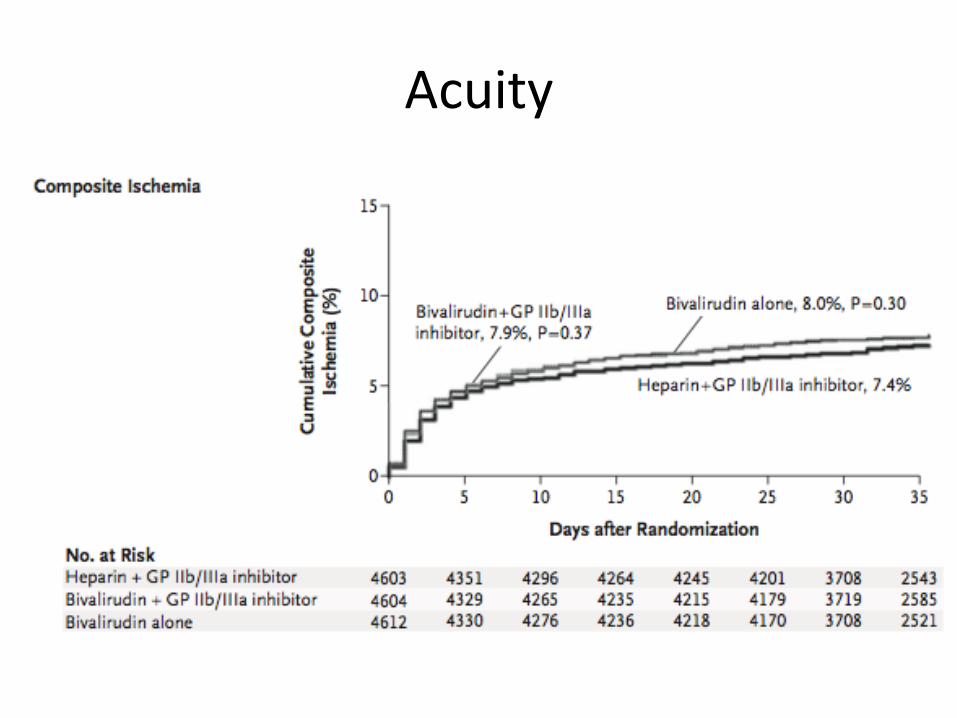
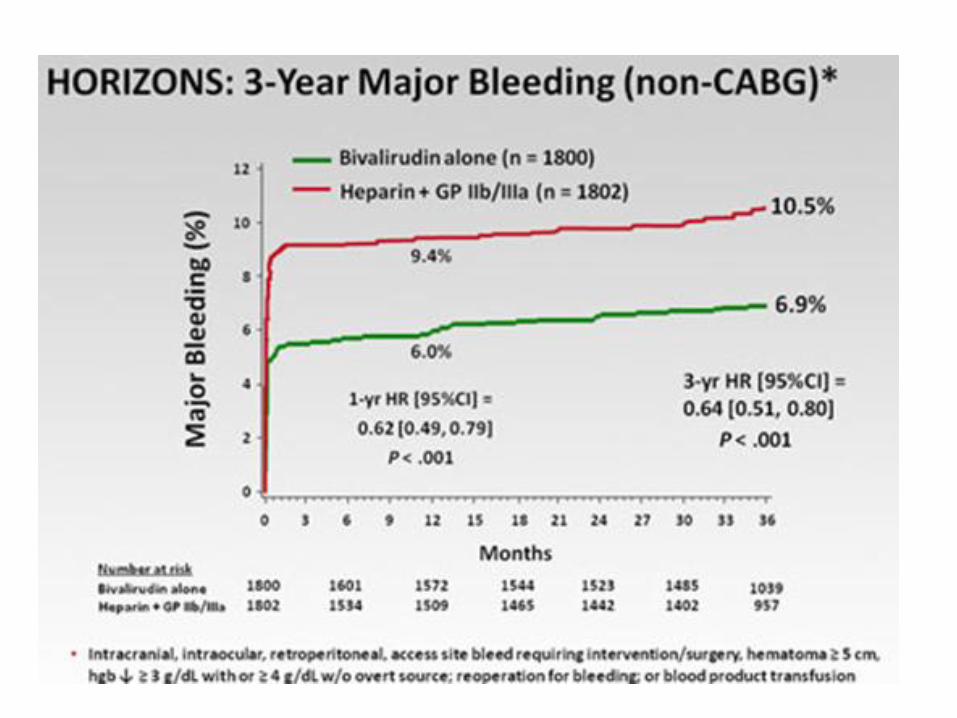
Acuity
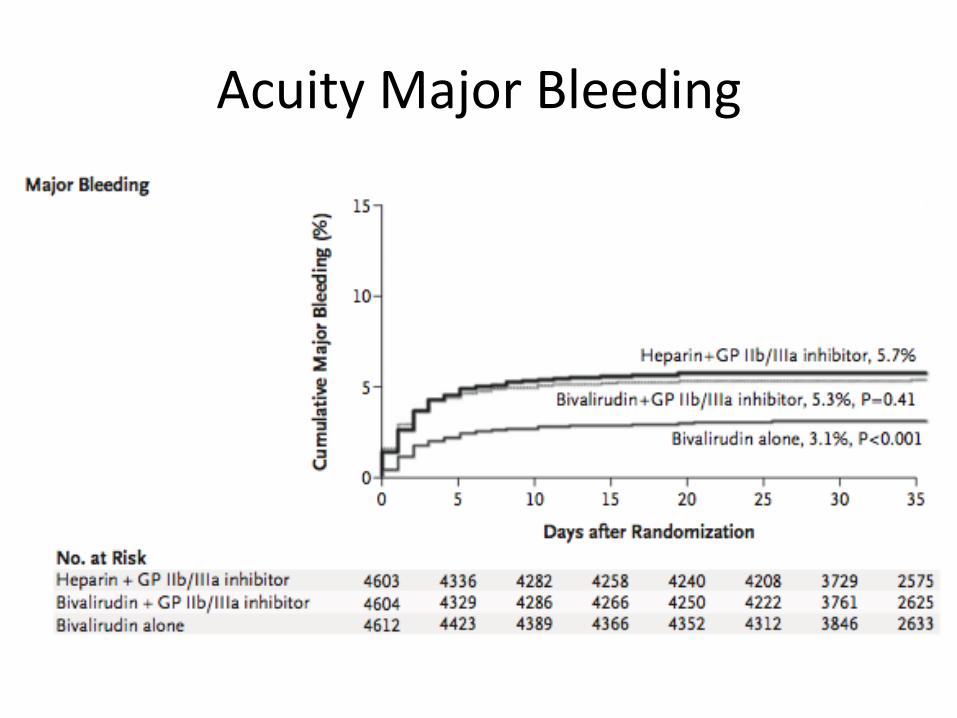
Acuity Major Bleeding
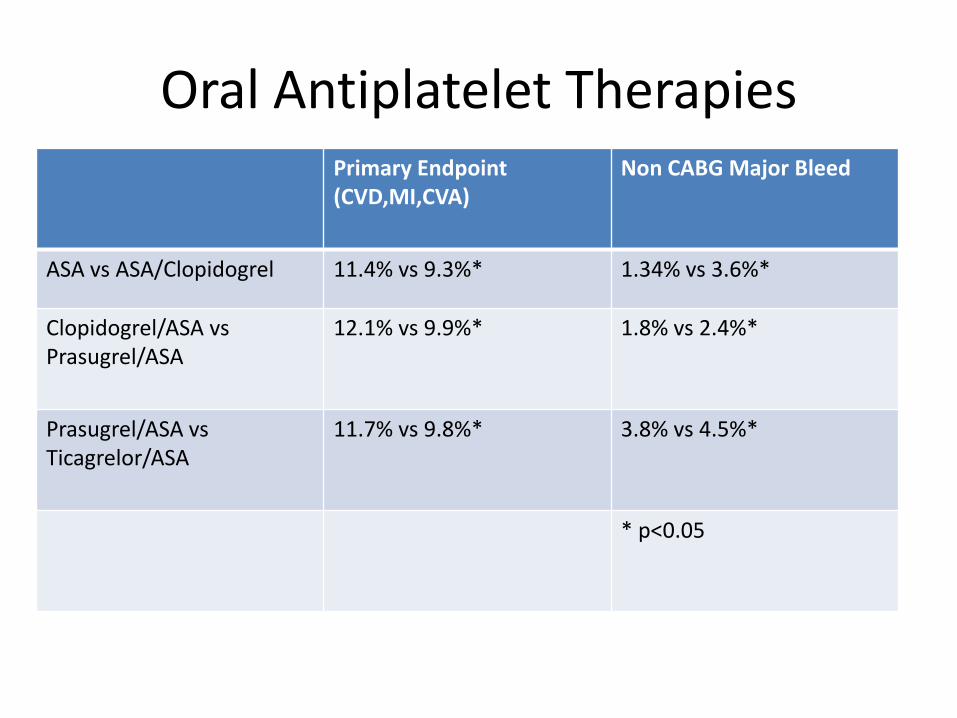
Oral Antiplatelet TherapiesPrimary Endpoint (CVD,MI,CVA)
Non CABG Major Bleed
ASA vs ASA/Clopidogrel 11.4% vs 9.3%* 1.34% vs 3.6%*
Clopidogrel/ASA vsPrasugrel/ASA
12.1% vs 9.9%* 1.8% vs 2.4%*
Prasugrel/ASA vsTicagrelor/ASA
11.7% vs 9.8%* 3.8% vs 4.5%*
* p<0.05
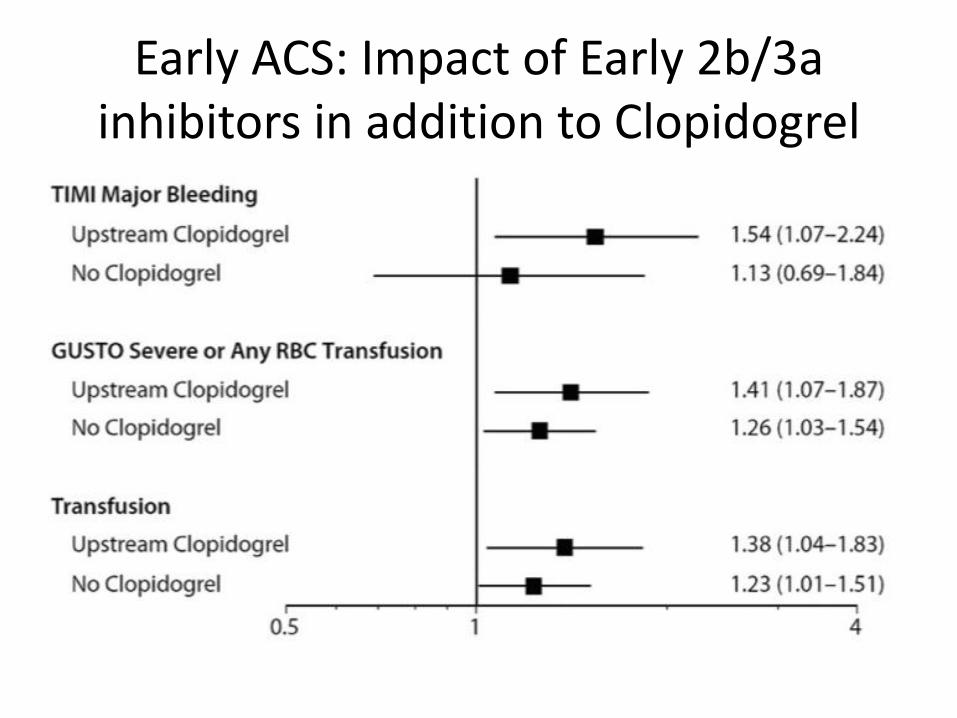
Early ACS: Impact of Early 2b/3a inhibitors in addition to Clopidogrel
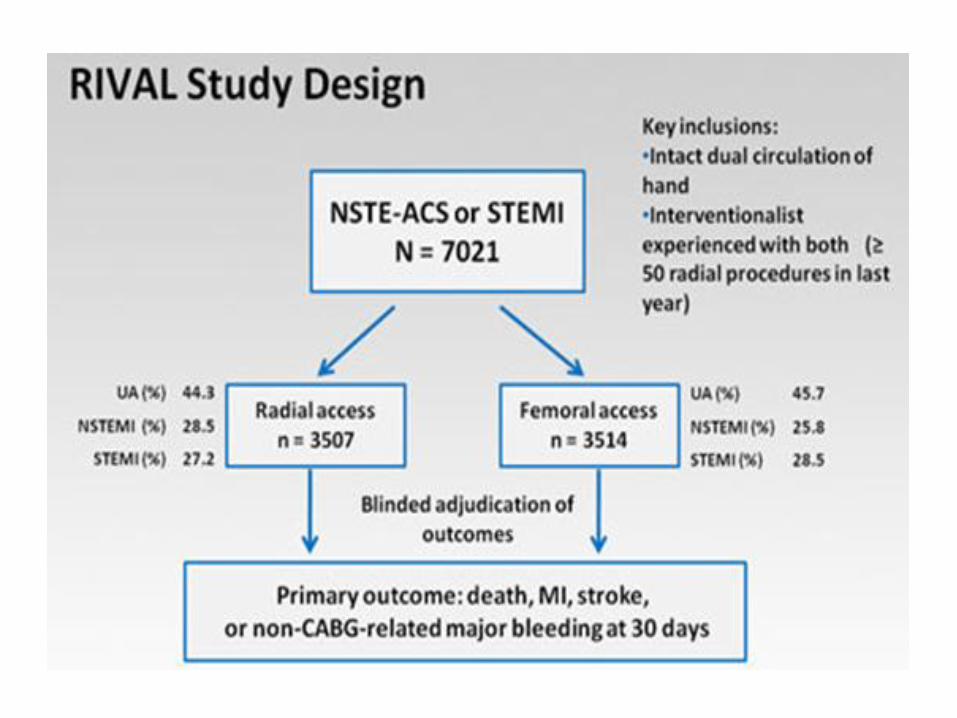
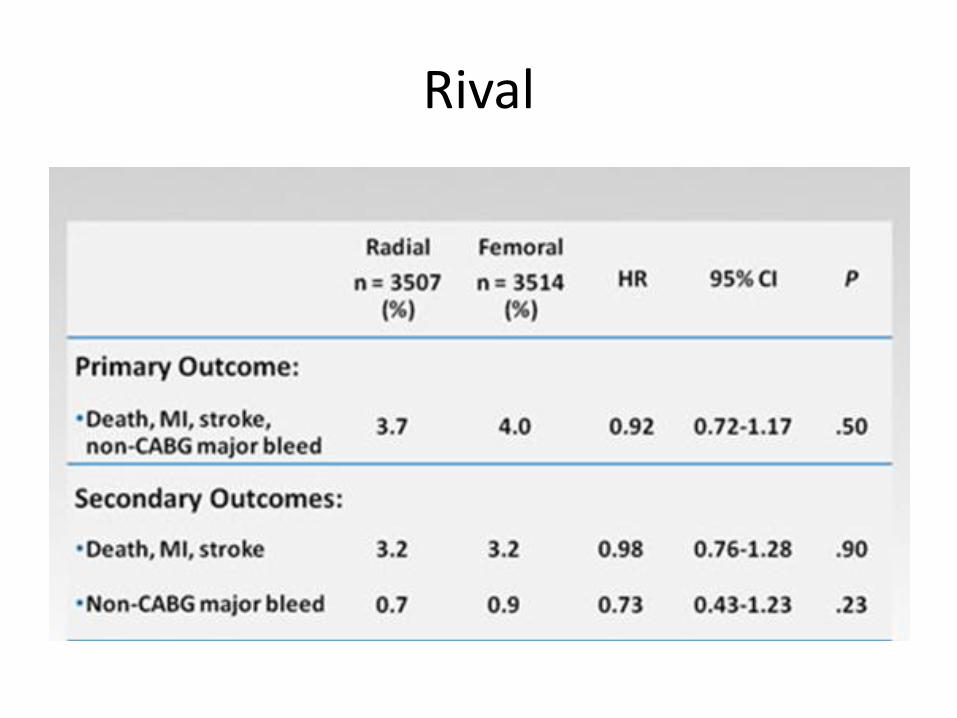
Rival
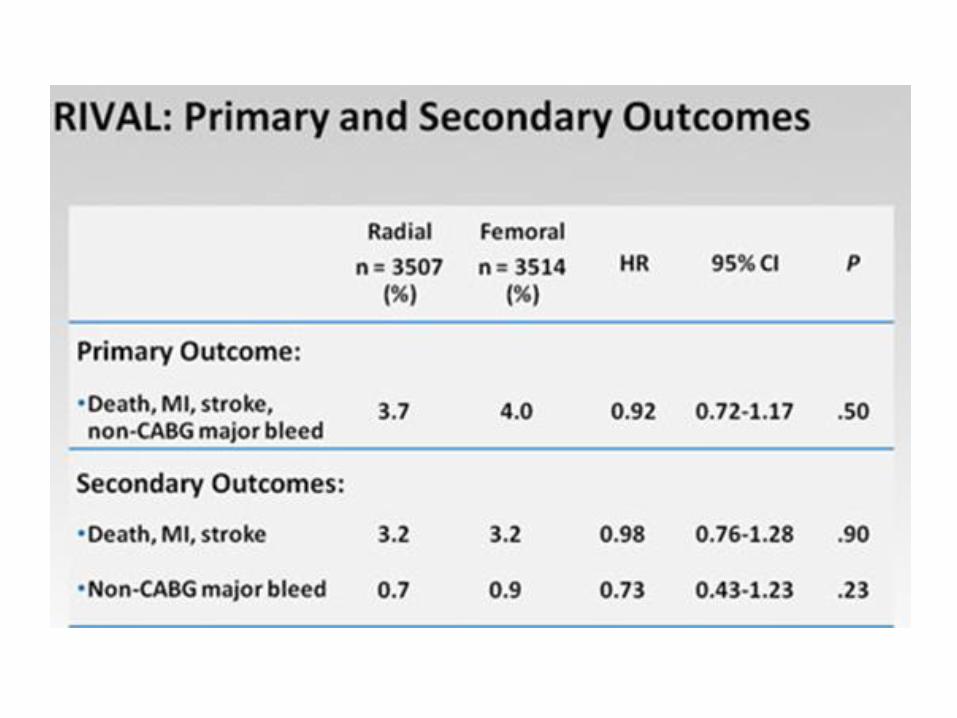
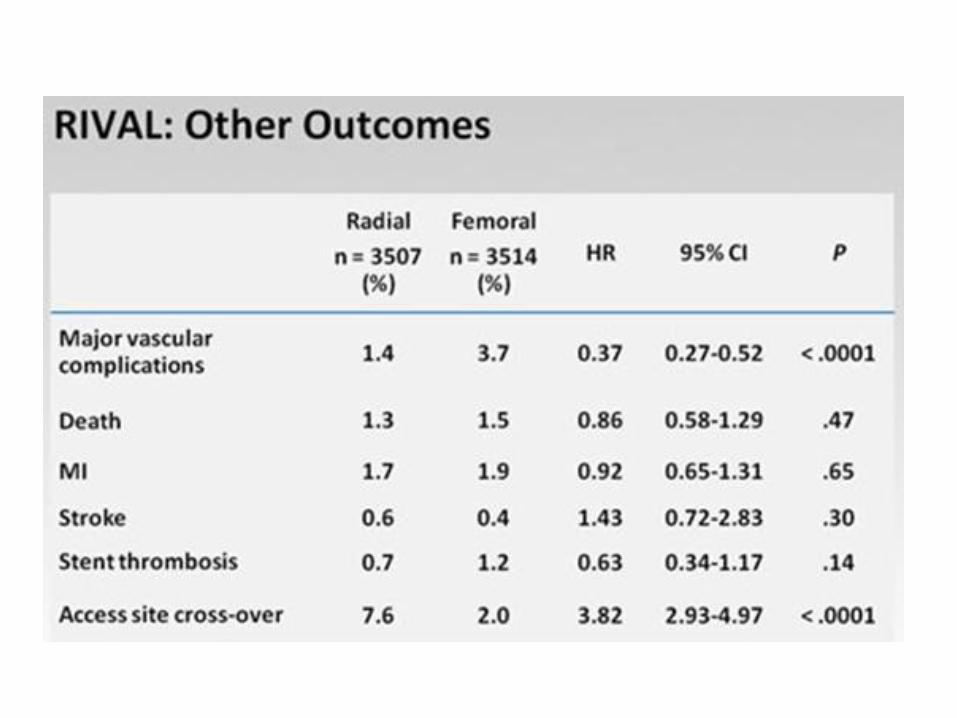
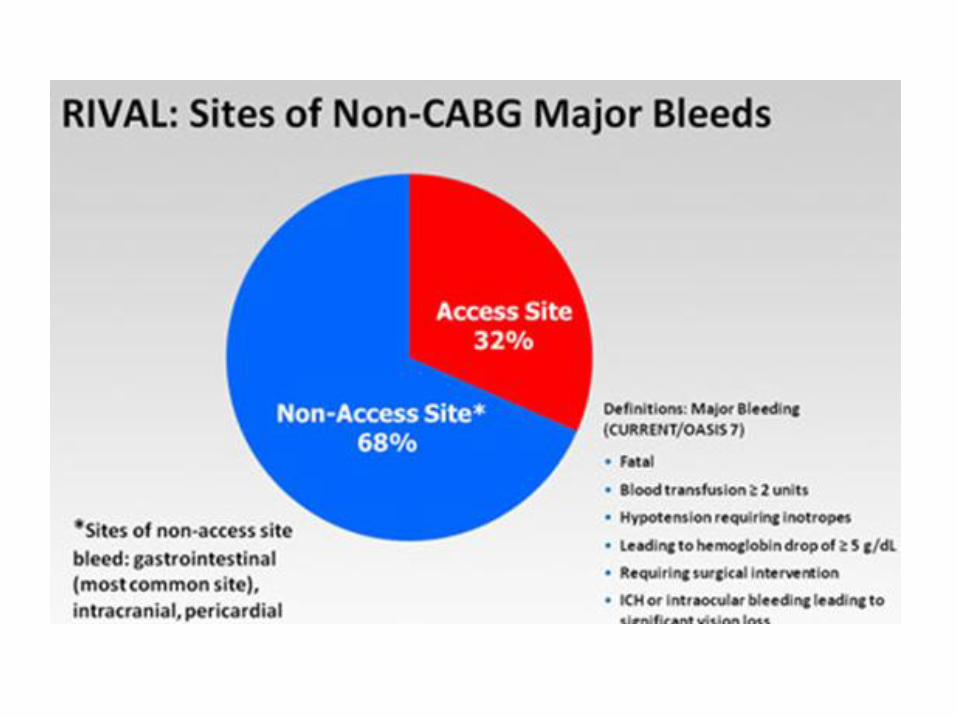
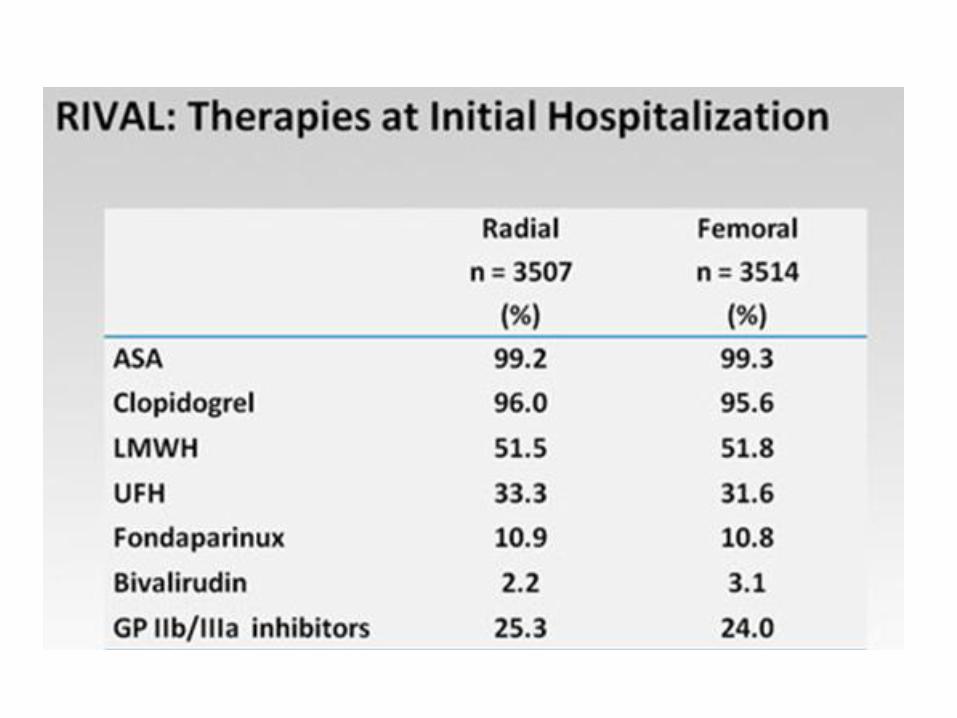
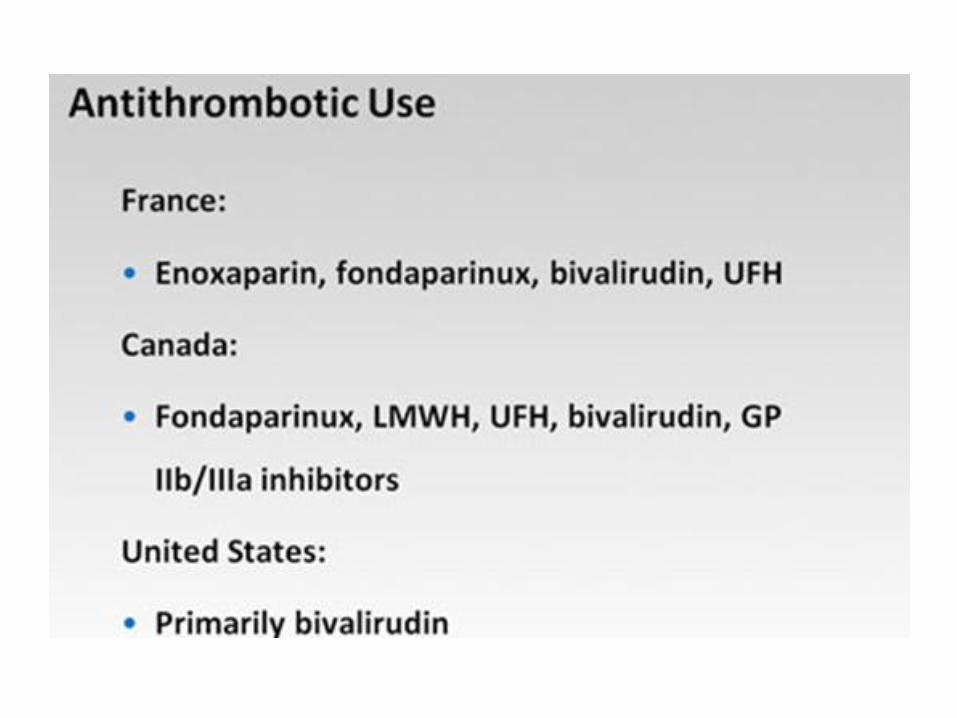
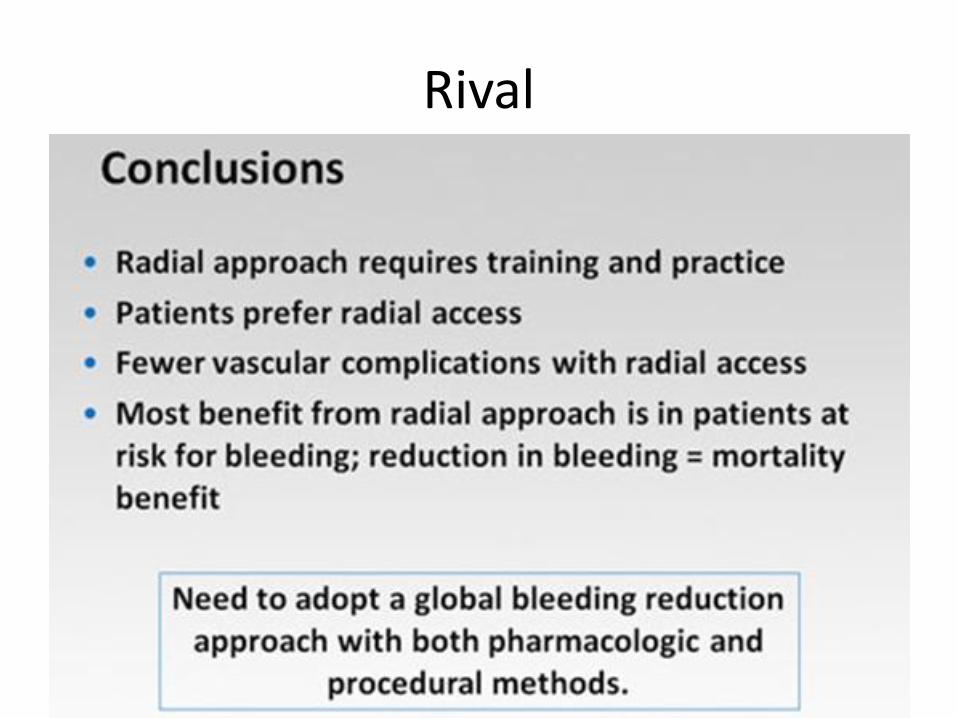
Rival
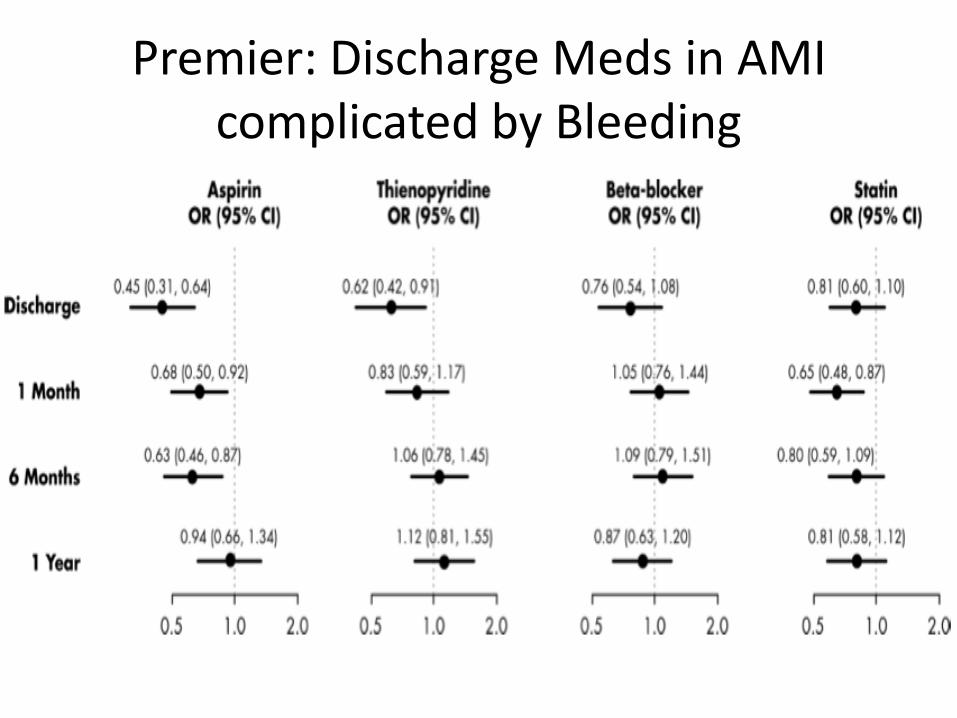
Premier: Discharge Meds in AMI complicated by Bleeding
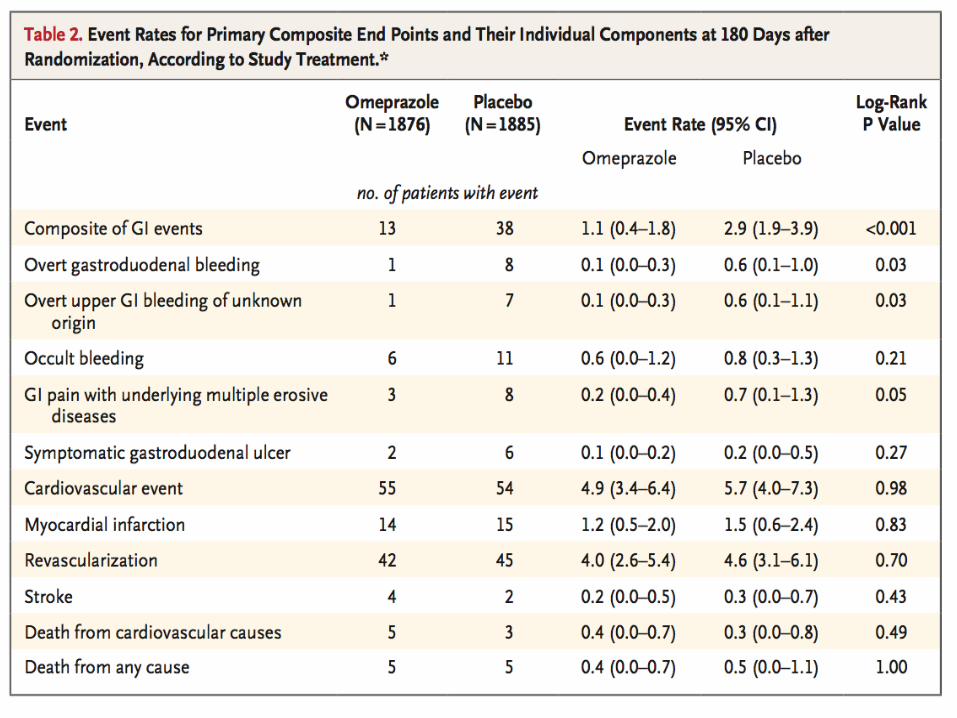
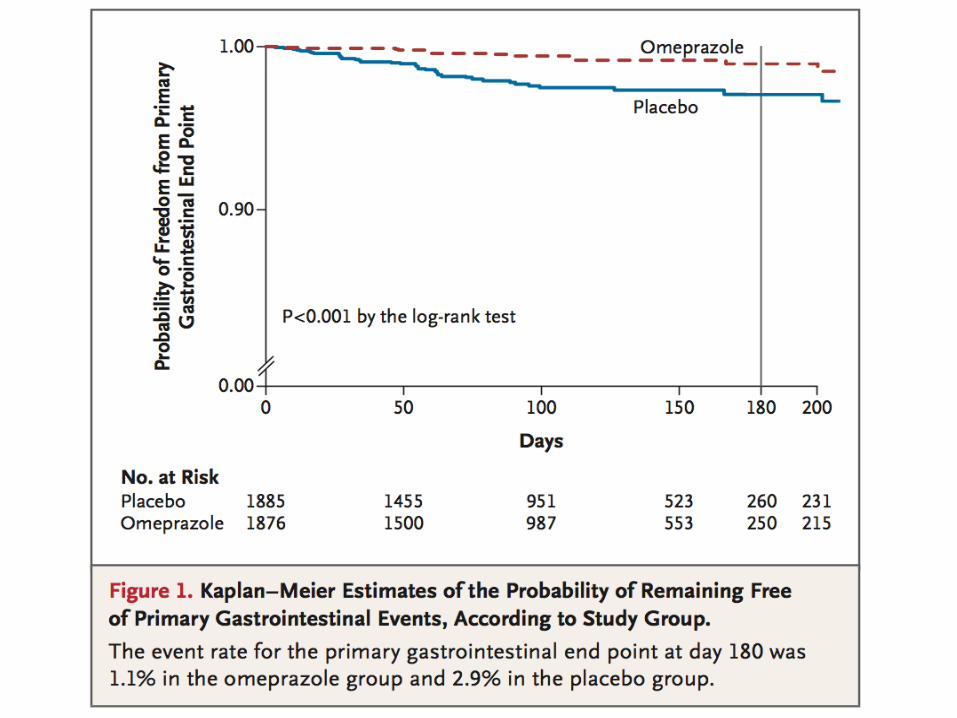
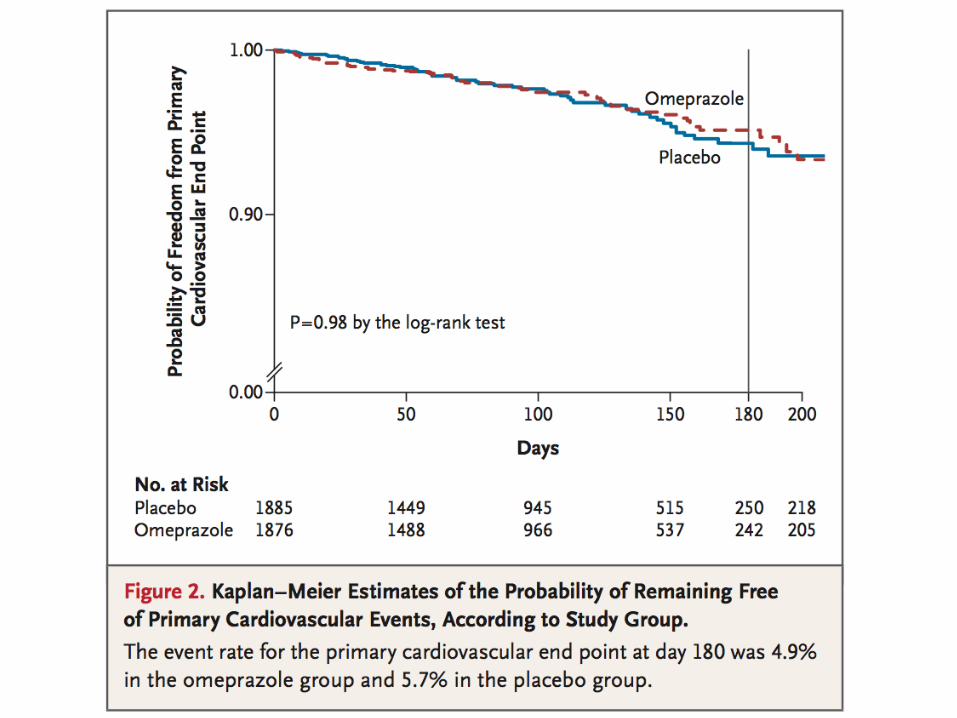
Clopidogrel and Omeprazole in CAD
NEJM 363;20
• Patients receiving dual antiplatelet tx were randomized to omeprazole or placebo.
• Primary endpoint: first occurrence of upper GI clinical events including:a. UGI bleedb. Confirmed ulcerc. Gastroduodenal erosions/obstructiond. Perforation
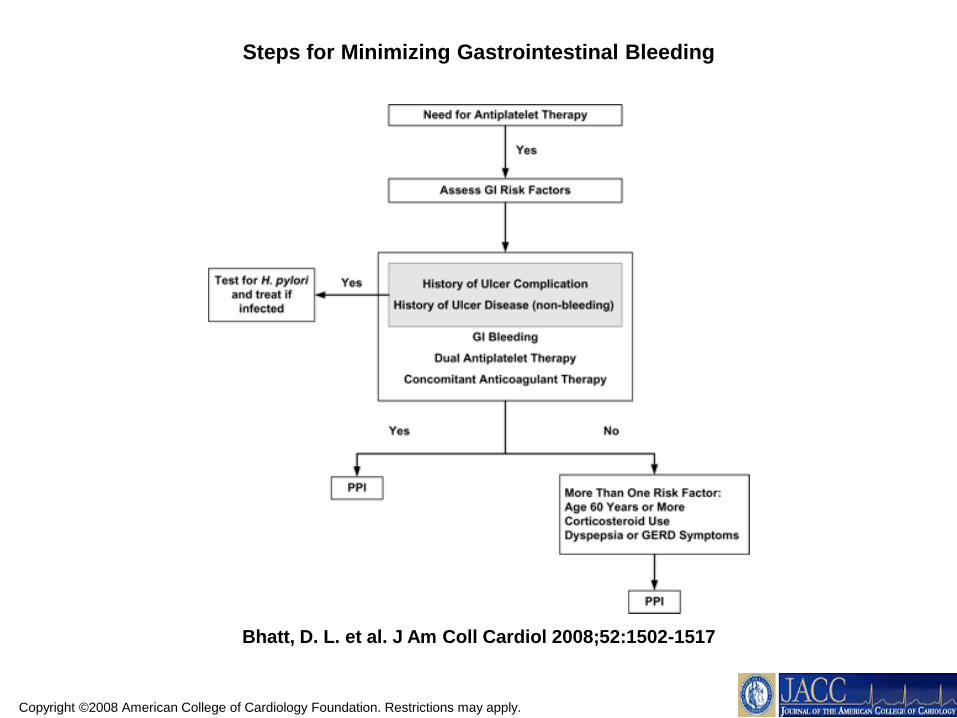
Copyright ©2008 American College of Cardiology Foundation. Restrictions may apply.
Bhatt, D. L. et al. J Am Coll Cardiol 2008;52:1502-1517
Steps for Minimizing Gastrointestinal Bleeding
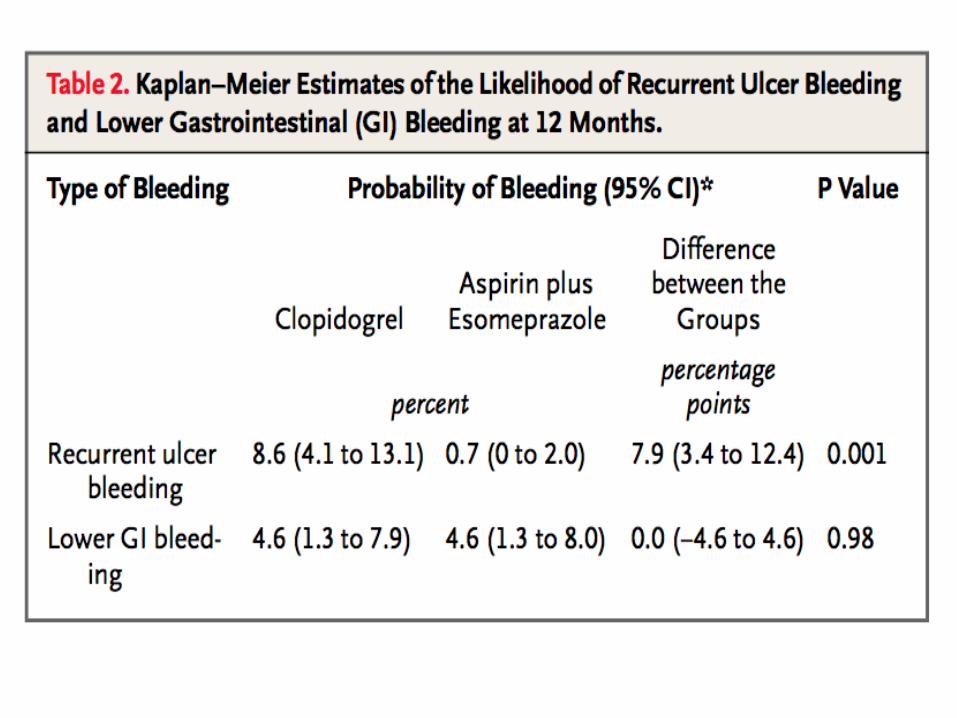
Clopidogrel vs ASA and Esomeprazole to Prevent Recurrent Ulcer Bleeding
NEJM 2005;353:238
• Patients on ASA for CV prevention, presented with ulcer bleeding and healed were randomized to clopidogrel vs ASA plus esomeprazole.
• 90% of patients had CAD or PAD
• Primary endpoint: recurrent bleeding during 12 months follow up.
Conclusion
• Patient risk of bleeding is important in selecting best therapies for treating ACS.
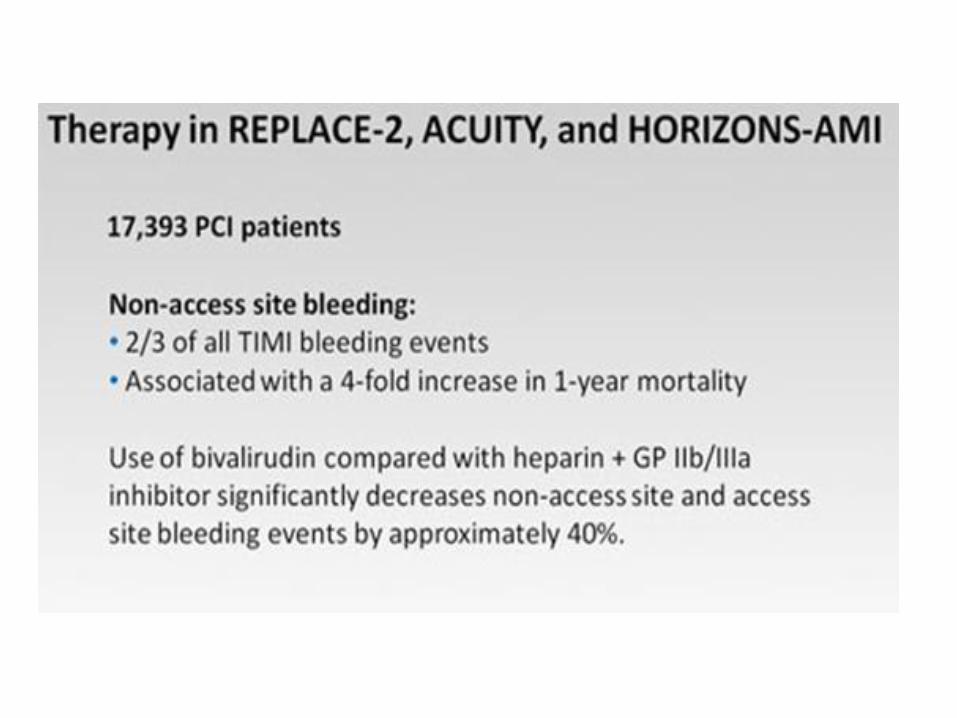
• Bleeding occurs more often in non access sites than access sites.
• Minimize dual antiplatelet therapy coupled with antithrombotic therapy.
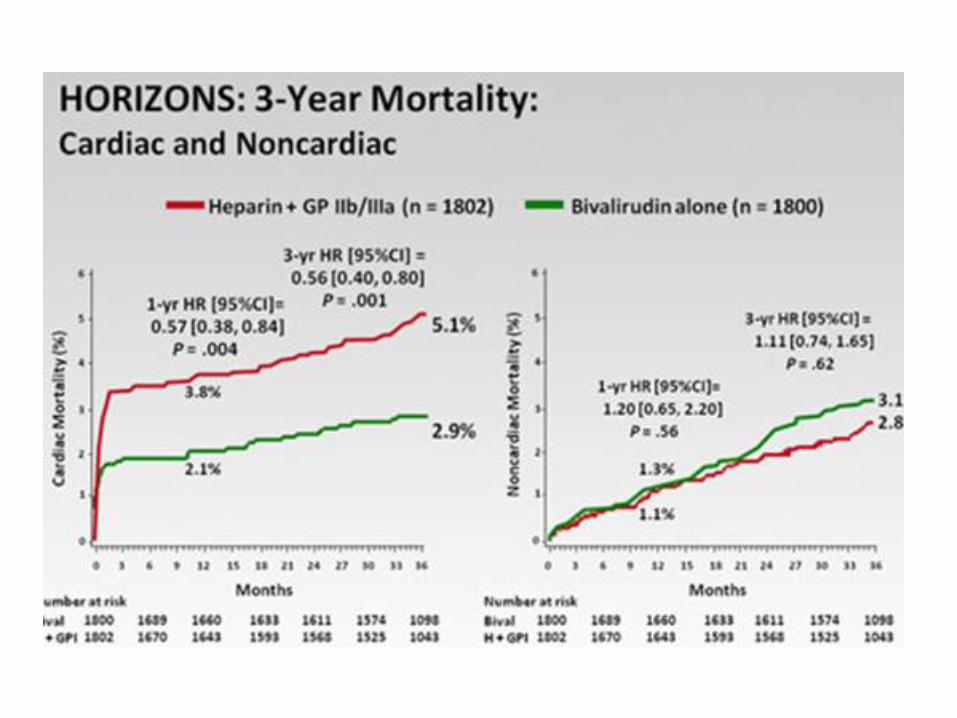
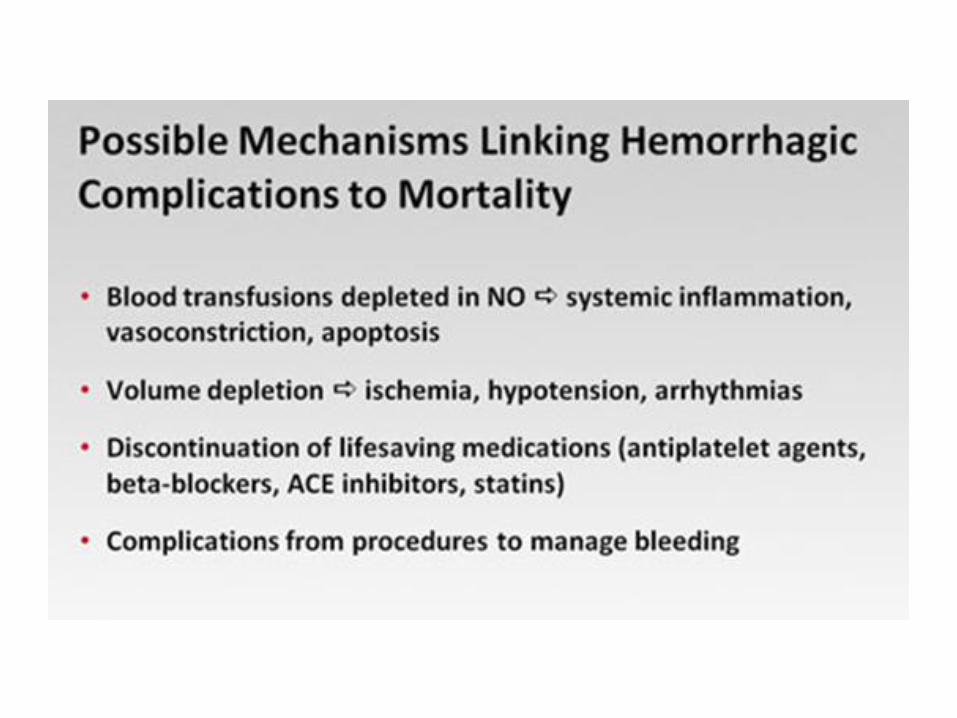
• Minimize lovenox “bridging”.• Bleeding is associated with increase in ischemic
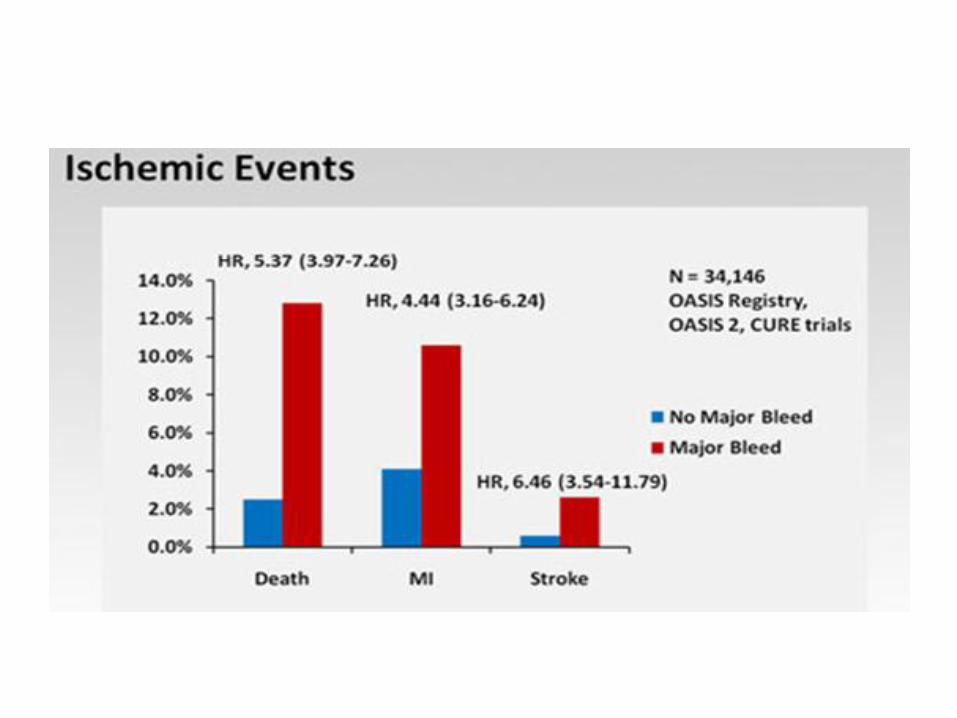
events and an increase in mortality.• Clinical decision making in this patient population
has become complex.