rigshospitalet fludarabin/cykofosfamid/rituximab forsøgs arm … · 2: bone marrow aspiate/biopsy...
TRANSCRIPT

Rigshospitalet Hæmatologisk afdeling
Fludarabin/Cykofosfamid/Rituximab CLL13
Forsøgs arm FCR ≤ 65 år
Navn CPR
___________
Cyklus (28 dage) Cyklus 1 Cyklus 2 Cyklus 3 Cyklus 4 Cyklus 5 Cyklus 6
EOT
Behandlingsdag 11 2 3 15 1 2 3 1 2 3 1 2 og 3 1 2 og 3 1 2 og 3
28 d
age
efte
r sta
rt a
CY6
Dato Visit window ±/1 ±1 ±1 ±1 ±1 ±1 ±1 Medicin Tabl. Tavegyl 1 mg 0 0 0 0 0 0 Tabl. Pamol 0 0 0 0 0 0 IV. Solomedrol pn IV. Fludarabin 25/m2 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 IV. Cykofosfamid 250 mg/m2 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 IV. Rituximab 375 mg/m2 0 IV. Rituximab 500 mg/m2 0 0 0 0 0 Allopurinol 300 mg 0 0 0 0 Sullfatrim 2 tbl 2 0 Dokumenteres Anamnese og medicinstatus 0 0 0 0 0 0 0 ECOG + b symptomer 0 0 0 0 0 0 0 Sygdomsstatus/resp.eval 0 0 AE’er på AE skema 0 0 0 0 0 0 0 Undersøgelser Objektiv undersøgelse 0 0 0 0 0 0 0 Knoglemarv / biopsi 2 CT-scanning3 Højde og vægt 0 0 0 0 0 0 0 BT, tp, p 0 0 0 0 0 0 0 Quality of life4 0 0 Labka CLL135 0 0 0 0 0 0 0 Standard blpr6 (0) FISH cytogenetics +TP53+IGHV7
HBV test8 0 Graviditetstest9 0 0 0 0 0 0 0 Accompanying scientific progr10 0 MRD blood sample 11 0 0
CLL13 forsøgsarm FCR > 65 år Version 1 August 2016

Rigshospitalet Hæmatologisk afdeling
Fludarabin/Cykofosfamid/Rituximab CLL13
Forsøgs arm FCR ≤ 65 år
Navn CPR
___________
1: Treatment must be stated within 14 days after randomization.
2: Tabl Sulfatrim indtages hver mandag og torsdag, indtil patienten når måned 15.
2: Bone marrow aspiate/biopsy must be performed together with measurement of MDR from the bone marrow at final restaging, preferably together with MRD-testing of peripheral blood at MRD-staging ( to be send to the central lab in Kiel)
3: Radiological assessment of lymphadenopathy , liver and spleen using imaging techniques(CT/MRI) must be performed at final restaging (if abnormal at screening)
4: EORTC QLQ-C30 and EORTC QOL-CLL16 questionnaires.
5: Hæmatologi :(LEU,DIFFMAS, THROM, RETIC, HB) Biokemi: (CREA,BILI,ALAT,ASAT,LDH,NA,K,CL,PHOS,HCO3,CA,URAT,CARB) ( ved EOT tillægges immunoglobulins (IgA, IgM, IgG, IgE) and direct antiglobulin Coombs test.
6: Assessment is recommended, but not needed at cycle 1 day 15, following cycles only if considered indicated. Standard = (HB,TROM,LEU,CRP,K,CREA,NA)
7: To be send in case of progression only (central lab Ulm)
8: Only for patients who are HBsAg negative /anti –HBc positive with negative PCR for HBV DNA (with a lower limit of detection of the order of 10 who IU/ml) at screening; in this case HBV-DNA PCR must be performed every month until 1 year after last dosage of rituximab. If the HbV dNa assay becomes positive, the patient should pre-emptively be treated with nucleoside analog (i.e.lamivudine) for at least 12 months after the last cycle of therapy or be referred to gastroenterologist for management.
9: ≤ 7 days before start of study treatment and on day 1 in every treatment cycle, in all woman of childbearing potential.
10: To be send to Keil and Ulm
11: To be send to Keil
CLL13 forsøgsarm FCR > 65 år Version 1 August 2016

Rigshospitalet Hæmatologisk afdeling
Fludarabin/Cykofosfamid/Rituximab CLL13
Forsøgs arm FCR ≤ 65 år
Navn CPR
___________
Dose and schedule modifications
Before starting treatment on day 1 of every cycle, the following retreatment criteria must be fulfilled:
• No active infection • no CTC grade III/IV AEs (except hematological AEs that are due to bone marrow involvement of the CLL, these must be recovered to at least baseline value)
If these criteria are not met treatment must be delayed for up to 14 days.
Afterwards the patient must continue with a reduced dose of 75% of the normal dose of fludarabine, cyclophosphamide or bendamustine.
The rituximab dose will not be reduced (except for dose reductions of 100% that may occur due to side effects), but will be delayed by the same amount.
If the patient does not meet the retreatment criteria within the 14-day-period again a further delay of 14 days (resulting in a total delay of 28 days) is permitted.
The patient will than continue with a reduced dose of 50% of the normal dose of the fludarabine, cyclophophamide or bendamustine respectively. Again, the rituximab dose will not be reduced.
The reduced dosage must be applied in all consecutive treatment cycles.
If the retreatment criteria are not met after 4 weeks, the study treatment must be permanently discontinued.
If, after the first dose reduction to 75%, retreatment criteria are not met by day 1 of one of the following treatment courses, treatment can be delayed again for up to 2 weeks with a following reduction to 50% of fludarabine and cyclophosphamide or bendamustine respectively for subsequent cycles. The rituximab dose will not be reduced. Further delay is not permitted.
If the retreatment criteria are not met on day 1 of the subsequent cycles after dose reduction to 50%, treatment can be delayed again for up to 2 weeks without further dose reduction. If the event does not resolve after two additional weeks, the study treatment has to be discontinued.
Besides the above described circumstances for permanent discontinuation of standard chemoimmunotherapy it must be performed in the following cases:
• CTC grade 4 infections • Treatment related autoimmune disease
CLL13 forsøgsarm FCR > 65 år Version 1 August 2016

Rigshospitalet Hæmatologisk afdeling
Fludarabin/Cykofosfamid/Rituximab CLL13
Forsøgs arm FCR ≤ 65 år
Navn CPR
___________
• ≥ grade 3 non-hematological toxicity related to study treatment
Dose modifications of fludarabine and cyclophosphamide due to decreased renal function
Both fludarabine and cyclophosphamide are excreted mainly via the kidneys. If a decrease of renal function occurs during therapy (creatinine clearance < 70 ml/min) the dose of fludarabine and cyclophosphamide has to be adjusted (See Table 5). A dose reduction of fludarabine to 80% and of cyclophosphamide to 75% must be instituted when the creatinine clearance is within the range from 30 to 70 ml/min. If creatinine clearance falls to < 30 ml/min, FC should be discontinued.
Table 3: Dose adjustments for fludarabine and cyclophosphamide in renal impairment
No furthertreatment
No furthertreatment
< 30
187 (75%)2030 - 70
25025> 70
Cyclophosphamide(mg/m2/day)
Fludarabine(mg/m2/day)
Creatinin-Clearance(ml/min)
CLL13 forsøgsarm FCR > 65 år Version 1 August 2016

Rigshospitalet Hæmatologisk afdeling
Rituximab + Bendamustine CLL13
Forsøgs arm BR > 65 år
Navn CPR
Godkendt af læge_____________
Cyklus (28 dage) Cyklus 1 Cyklus 2 Cyklus 3 Cyklus 4 Cyklus 5 Cyklus 6
EOT
Behandlingsdag 11 2 15 1 2 15 1 2 15 1 2 1 2 1 2
28 d
age
efte
r sta
rt a
CY6
Dato Visit window ±1 ±1 ±1 ±3 ±1 ±3 ±1 Medicin T. Tavegyl 1 mg 0 0 0 0 0 0 T. Panodil 1000 mg 0 0 0 0 0 0 IV. Solumedrol pn IV. Bendamustine0 70mg/m2 0 0 0 0 0 0 0 0 0 0 0 0 IV. Rituximab 375 mg/m2 0 IV. Rituximab 500 mg/m2 0 0 0 0 0 Dokumenteres Anamnese og medicinstatus 0 0 0 0 0 0 0 ECOG + b symptomer 0 0 0 0 0 0 0 Sygdomsstatus/resp.eval 0 0 AE’er på AE skema 0 0 0 0 0 0 0 Úndersøgelser Objektiv undersøgelse 0 0 0 0 0 0 0 Knoglemarv/MRD / biopsi 2 CT-scanning3 Højde og vægt 0 0 0 0 0 0 0 BT, tp, p 0 0 0 0 0 0 0 0 0 0 Quality of life4 0 0 Labka CLL135 0 0 0 0 0 0 0 Standard blpr6 (0) FISH cytogenetics + TP53+IGHV7
HBV test8 (0) (0) (0) (0) 0 Graviditetstest9 0 0 0 0 0 0 0 Accompanying scientfic program10 0
MRD blood sample 11 0 0
CLL13 forsøgsarm BR > 65 år Version 1. August 2016
Rigshospitalet Hæmatologisk afdeling
Rituximab + Bendamustine CLL13
Forsøgs arm BR > 65 år
Navn CPR
Godkendt af læge_____________
0: Såfremt der vurderes betydende risiko for tumorlyse må der gives probenecid i cyklus 1 (allopurinol kontraindiceret grundet risiko for Steven-Johnson sammen med bendamustin), alternativt er oral hydrering 2 l pr dag.
1: Treatment must be stated within 14 days after randomisation.
2: Bone marrow aspiate/biopsy must be perfomed together with measurement of MDR from the bone marrow at final restaging, preferably together with MRD-testing of peripheral blood at MRD-staging ( to be send to the central lab in Kiel)
3: Radiological assessement of lymphadenopathy , liver and spleen using imaging techniques(CT/MRI) must be performed at final restaging (if abnormal at screening)
4: EORTC QLQ-C30 and EORTC QOL-CLL16 questionnaires.
5: Hæmatologi :(LEU,DIFFMAS, THROM, RETIC, HB) Biokemi: (CREA,BILI,ALAT,ASAT,LDH,NA,K,CL,PHOS,HCO3,CA,URAT,CARB)
6: 6: Assessment is recommended, but not needed at cycle 1 day 15, following cycles only if considered indicated. Standard = (HB,TROM,LEU,CRP,K,CREA,NA)
7: To be send in case of progression only (central lab Ulm)
8: Only for patients who are HBsAg negative /anti –HBc positive with negative PCR for HBV DNA (with a lower limit of detection of the order of 10 who IU/ml) at screening; in this case HBV-DNA PCR must be performed every month until 1 year after last dosage of rituximab. If the HbV dNa assay becomes positive, the patient should pre-emptively be treated with nucleoside analog (i.e.lamivudine) for at least 12 months after the last cycle of therapy or be referred to gastroenterologist for management.
9: ≤ 7 days before start of study treatment and on day 1 in every treatment cycle, in all woman of childbearing potential.
10: To be send to Keil and Ulm
11: To be send to Keil
CLL13 forsøgsarm BR > 65 år Version 1. August 2016

Rigshospitalet Hæmatologisk afdeling
Rituximab + Bendamustine CLL13
Forsøgs arm BR > 65 år
Navn CPR
Godkendt af læge_____________
Dose and schedule modifications for treatment
In case of emerging adverse events during treatment, the following should be fol-lowed:
Hematologic toxicity
(unless directly attributable to the underlying CLL)
Event Dose delay or dose modification
Neutropenia (with or without fever and infection) CTC Grade 3 or 4
• Withhold treatment for at least 7 days • Administer G-CSF or growth factors for neutropenia as indicated • When counts recover to ANC ≥ 1 x109/l resume at one dose level reduction
CLL13 forsøgsarm BR > 65 år Version 1. August 2016

Rigshospitalet Hæmatologisk afdeling
Rituximab + Bendamustine CLL13
Forsøgs arm BR > 65 år
Navn CPR
Godkendt af læge_____________
Thrombocytopenia CTC Grade 4 and/or symptomatic bleeding
• Withhold treatment • Platelets may be transfused at the discretion of the investigator • When platelet level rises to > 50x109/l without transfusional support for 5 consecutive days, restart
treatment at previous dose
For a second episode:
o Withhold treatment o When platelet level rises to > 50 x10^9/l without transfusional support for 5 consecutive
days, restart treatment at one dose level reduction
For subsequent episodes:
o Withhold treatment o When platelet level rises to > 50 x10^9/l without transfusional support for 5 consecutive
days, restart treatment at one dose level reduction
For recurrent episodes please consult the GCLLSG study office.
Non-hematologic events (e.g. infections)
CTC Grade Dose delay or dose modification
Grade 3 or 4 • Delay treatment for a maximum of 28 days. • First episode: If improvement to Grade ≤ 1 or baseline, resume previous doses of treatment. • For subsequent episodes: If improvement to Grade ≤ 1 or baseline, restart treatment at one dose level
reduction.
CLL13 forsøgsarm BR > 65 år Version 1. August 2016

Rigshospitalet Hæmatologisk afdeling
Rituximab + Bendamustine CLL13
Forsøgs arm BR > 65 år
Navn CPR
Godkendt af læge_____________
Certain treatment emergent non-hematologic adverse events (e.g., venous thromboembolic events) may be managed and become clinically stable following medical intervention but may not improve to Grade ≤ 1 according to the NCI CTCAE definitions. In such cases resumption of study drug may be possible after consultation with the GCLLSG study office.
Grade 2 • Delay treatment until resolution to Grade ≤ 1 (or baseline status) for a maximum of 28 days. • After resolution, resume full dose.
Grade 1 • No dose reduction or delay
CLL13 forsøgsarm BR > 65 år Version 1. August 2016

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Rituximab + Venetoclax (RVe) NAVN: CPR:
År: Dato:
Scr
eeni
ng d
ag-2
8-0
Serie Serie 1 Serie 2 Serie 3 Serie 4 Serie 5 Serie 6
Behandlingsuge 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Behandlingsdag
1
15 22 1 8 15 22 1 1 1 1
Behandling: Præ pamol tavegyl solu-medrol pn 0 0 0 Rituximab 375 mg/ m2 0 Rituximab 500 mg/m2 0 0 0 0 0 Allopurinol1 300 mgx1 d.-3-end 6.serie 0 0 0 0 0 0 0 Venetoclax, 20 mg 2 02 Venetoclax, 50 mg 2 02 Venetoclax, 100 mg 2 02 Venetoclax, 200 mg 2 02 Venetoclax, 400 mg 2 02 0 0 0 0 Sulfatrim 2 tbl man og tors TOM month 15
0 0 0 0 0 0
Undersøgelser
Medicin status 0 0 0 0 0 0 Sygdomsstatus/ response evaluering.
0 TLS risiko vurdering3 0 0 0 0 0 0 0 0 0 0 Objektiv undersøgelse4 0 0 AE registering 0 0 0 0 0 0 CT scanning5 ECOG + B symptomer 0 0 ECG6 0 Livskvalitetsskema7 0 Vitale værdier 0 0 0 0 0 Højde, vægt 0 0 0 0 0 0
BLODPRØVER Labka :CLL138 0 0 0 0 0 0 Standard blpr9 (0) Tumorlyseprøver10 0 0 0 0 0 HBV testing11 (0) (0) (0) (0) (0) (0)
HcG (fødedygtige kvinder)12 0 0 0 0 0 0
Protokol prøver / PK MRD/ FISH
Accompanying scientfic program13 0 MRD from peripheral blood14 0 0 MRD from bone marrow15 FISH cytogenetics, TP53 and IGHV.16
CLL13 forsøgsarm RVe version 1. August 2016 Side 1 af 6

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Rituximab + Venetoclax (RVe) NAVN: CPR:
0) Treatment must be started within 14 days after randomisation.
1) Allopurinol must be started 3 days before cycle 1 day 1, and be stopped after cycle 6.
2) Laboratory assessments regarding to Venetoclax are required on the first day of each dose level (i.e. 20
mg, 50 mg, 100 mg, 200 mg and 400 mg venetoclax) pre-dose as well as 6-8 and 24 hours post-dose. Pre-existing electrolyte abnormalities should be corrected before initiation of treatment. For 100 mg, 200 mg and 400 mg ramp up in patients without increased risk of tumor lysis, pre-dose sampling can be done up to 24 h ahead of dosing at home.
3) Overnight hospitalization is recommended for patients at increased risk of TLS (high tumor burden (e.g.,
any lymph node with a diameter ≥5 cm or high absolute lymphocyte count [ALC ≥25 x 109/L]), splenomegaly, renal dysfunction (CrCl < 80 mL/min), the presence of pre-treatment clinical chemistry abnormalities, or the presence of other co-morbidities) in order to allow more intensive prophylaxis and monitoring through the first 24 hours after initiating treatment with venetoclax. ( separat venotoclax skema for ramp-up perioden )
4) Objektiv undersøgelse inkluderer: hoved, øjne, ører, næse, hals, cardiovaskulær, dermatologisk, muskulatur, respiratorisk, gastroentestinal.
5) ) Radiological assessment of lymphadenopathy, liver and spleen using imaging techniques (CT or MRI) is mandatory at final restaging (if abnormal at screening). The modality of staging in one patient should not be changed. Further imaging (even with ultrasound) can be performed at the investigator’s discretion, e.g. in case of a suspected PD.
6) Assessment recommended and to the investigator’s , but are not documented in the CRF.
7) EORTC QLQ-C30, EORTC QOL-CLL16 and questionnaires
8) Hæmoglobin:( LEU,DIFFMAS, THROM, RETIC, HB)
Biokemi:(CREA,BILI,ALAT,ASAT,LDH,NA,K,CL,PHOS,HCO3,CA,URAT,CARB)
9) Assessment is recommended, but not needed at cycle 1 day 15, following cycles only if considered indicated. Standard = (HB,TROM,LEU,CRP,K,CREA,NA)
10) Tumorlyseprøver:( CAI, PHOS, K, CARB,CREA,LDH,MG,NA,URAT)
11) Only for patients who are HBsAg negative/anti-HBc positive with negative PCR for HBV DNA (with a lower limit of detection of the order of 10 WHO IU/mL) at screening; in this case HBV-DNA PCR must be
CLL13 forsøgsarm RVe version 1. August 2016 Side 2 af 6

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Rituximab + Venetoclax (RVe) NAVN: CPR:
performed every month until 1 year after last dosage of rituximab or obinutuzumab respectively. If the HBV DNA assay becomes positive, patients should pre-emptively be treated with a nucleoside analog (i.e. lamivudine) for at least twelve months after the last cycle of therapy or be referred to a gastroenterologist for management.
12) ≤7 days before start of study treatment and on day 1 of every treatment cycle (monthly) in all women of
childbearing potential
13) Additional samples for accompanying scientific program should be sent to Kiel and Ulm on cycle 2 day 1, (and in case of progression)
14) Samples for MRD testing should be sent to central lab in Kiel on cycle 1 day 1 and cycle 2 day 1
15) Bone marrow aspirate/biopsy must be performed together with measurement of MRD from the bone
marrow at final restaging, preferably together with MRD-testing of peripheral blood at MRD-staging 1(to be sent to the central lab in Kiel)
16) To be sent in case of progression only!
Dose modifications for Rituximab : No dose modifacication will be performed for Rituximab Rituximab should be held in case of: - febrile infection - any CTC gradeIII/IV AEs (except hematological AEs that are due to bone marrow involvement of the CLL and thrombocytopenia during the first cycle, see below) In case of a febrile infection or CTC grade III/IV AEs, a weekly monitoring should be performed until the event resolves. Rituximab or obinutuzumab can be postponed for a maximum of 4 weeks (but please note that the appropriate treatment cycle won’t be prolonged). The last application of obinutuzumab or rituximab may not be performed after cycle 12 day 28. All antibody infusions that were not given until this timepoint must be skipped. Permanent discontinuation of rituximab or obinutuzumab is necessary in case of the following, however, treatment with venetoclax (and ibrutinib if applicable) may be continued: - CTC grade IV infusion related reaction, - IRR with acute life-threatening respiratory symptoms - CTC grade III infusion related reaction at re-challenge or prolonged or recurrent infusion reac-tions - anaphylaxis, acute respiratory distress - patients with <20 x109/l platelets and administration platelet inhibitors: temporary hold of platelet inhibitor is recommended2 Dose and schedule modifications for venetoclax In case of emerging adverse events during treatment with venetoclax, the following should be fol-lowed: Hematologic toxicity (unless directly attributable to the underlying CLL) Event Dose delay or dose modification
CLL13 forsøgsarm RVe version 1. August 2016 Side 3 af 6

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Rituximab + Venetoclax (RVe) NAVN: CPR: Neutropenia (with or without fever and infection) CTC Grade 3 or 4
• Withhold venetoclax for at least 7 days • Administer G-CSF or growth factors for neutropenia as indicated • When counts recover to ANC ≥ 1 x109/l resume venetoclax at one dose
level reduction Thrombocytopenia CTC Grade 4 and/or symptomatic bleeding
• Withhold venetoclax • Platelets may be transfused at the discretion of the investigator • When platelet level rises to > 50x109/l without transfusional support for 5
consecutive days, restart venetoclax at previous dose For a second episode:
o Withhold venetoclax o When platelet level rises to > 50 x10^9/l without transfusional
support for 5 consecutive days, restart venetoclax at one dose level reduction
For subsequent episodes:
o Withhold venetoclax o When platelet level rises to > 50 x10^9/l without transfusional
support for 5 consecutive days, restart venetoclax at one dose level reduction
For recurrent episodes please consult the GCLLSG study office.
Non-hematologic events (e.g. infections) CTC Grade Dose delay or dose modification Grade 3 or 4 • Delay venetoclax for a maximum of 28 days.
• First episode: If improvement to Grade ≤ 1 or baseline, resume previous doses of venetoclax.
• For subsequent episodes: If improvement to Grade ≤ 1 or baseline, restart venetoclax at one dose level reduction.
Certain treatment emergent non-hematologic adverse events (e.g., venous thromboembolic events) may be managed and become clinically stable following medical intervention but may not improve to Grade ≤ 1 according to the NCI CTCAE definitions. In such cases resumption of study drug may be possible after consultation with the GCLLSG study office.
Grade 2 • Delay treatment with venetoclax until resolution to Grade ≤ 1 (or baseline status) for a maximum of 28 days.
• After resolution, resume full dose of venetoclax
Grade 1 • No dose reduction or delay
First dose of Venetoclax or dose escalation
• Within the first 24 hours after either the first dose or dose escalation, if any laboratory criteria below
are met, the patient should be hospitalized for monitoring and the investigator notified. No additional GDC-0199 doses should be administered until resolution. A rapidly rising serum potassium level is a medical emergency.
• Nephrology (or acute dialysis service) must be consulted/contacted on admission (per institutional standards to ensure emergency dialysis is available).
CLL13 forsøgsarm RVe version 1. August 2016 Side 4 af 6

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Rituximab + Venetoclax (RVe) NAVN: CPR:
• Intravenous (IV) fluids (e.g., D5 1/2 normal saline) should be initiated at a rate of at least 1 mL/kg/h rounded to the nearest 10 mL (target 150 to 200 mL/hr; not < 50 mL/hr). Modification of fluid rate should also be considered for individuals with specific medical needs.
• Monitor for symptoms or signs of tumor lysis syndrome (TLS) (e.g., fever, chills, tachycardia, nausea, vomiting, diarrhea, diaphoresis, hypotension, muscle aches, weakness, paresthesias, mental status changes, confusion, and seizures). If any clinical features are observed, recheck potassium, phosphorus, uric acid, calcium, and creatinine within 1 hour STAT.
• Vital signs should be taken at time of all blood draws or any intervention.
• The management recommendations below focus on the minimum initial responses required. If a diagnosis of TLS is established, ongoing intensive monitoring and multidisciplinary management will be as per institutional protocols.
In addition to the recommendations in the table below, for patients with chronic lymphocytic leukemia (CLL)/ small lymphocytic lymphoma (SLL) receiving first dose of GDC-0199:
• For potassium increase ≥ 0.5 mmol/L from baseline, or any value > 5.0 mmol/L, recheck potassium, phosphorus, uric acid, calcium, and creatinine within 1 hour STAT and follow first guideline.
• For phosphorus increase of >0.162 mmol/l AND >1,454 mmol/l, administer phosphate binder and recheck potassium, phosphorus, uric acid, calcium, and creatinine within 1 hour STAT.
CLL13 forsøgsarm RVe version 1. August 2016 Side 5 af 6

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Obinutuzumab (GVe) NAVN: CPR:
År: Dato:
Scr
eeni
ng d
ag-2
8-0
Serie Serie 1 Serie 2 Serie 3 Serie 4 Serie 5 Serie 6
Behandlingsuge 1 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Behandlingsdag 1 2 8 15 22 1 8 15 22 1 1 1 1
Behandling: PRÆ tavegyl pamol solumedrol, solumedrol pn efter 1. gang
0 0 0 0 0 0
Obinutuzumab 100 mg 0 Obinutuzumab 900 mg 0 Obinutuzumab 1000mg 0 0 0 0 0 0 0 Allopurinol1 300 mgx1 d.-3-end 6.serie 0 0 0 0 0 0 0 0 0 0 0 0 0
Venetoclax, 20 mg 2 02 Venetoclax, 50 mg 2 02 Venetoclax, 100 mg 2 02 Venetoclax, 200 mg 2 02 Venetoclax, 400 mg 2 02 0 0 0 0 Sulfatrim 2 tbl man og tors TOM month 15
0 0 0 0 0 0
Undersøgelser
Medicin status 0 0 0 0 0 0 Sygdomsstatus/ response evaluering.
0
TLS risiko vurdering3 0 0 0 0 0 0 0 0 0 0 Objektiv undersøgelse4 0 0 AE registering 0 0 0 0 0 0 ECOG + B symptomer 0 0 ECG/LEVF6 0 Livskvalitetsskema7 0 Vitale værdier 0 0 0 0 0 Højde, vægt 0 0 0 0 0 0
BLODPRØVER Labka :CLL138 0 0 0 0 0 0 Standard blpr9 (0) (0) Tumorlyseprøver2 0 0 0 0 0 0 0 HBV testing9 (0) (0) (0) (0) (0) (0) HcG (fødedygtige kvinder)10
0 0 0 0 0 0
Protokol prøver / PK MRD/ FISH
Accompanying scientfic program11 0 MRD from peripheral blood12 0 0
CLL13 forsøgsarm GVe version 1 August 2016 Side 1 af 5

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Obinutuzumab (GVe) NAVN: CPR:
0) Treatment must be started within 14 days after randomisation.
1) Allopurinol must be started 3 days before cycle 1 day 1, and be stopped after cycle 6.
2) Laboratory assessments regarding to Venetoclax are required on the first day of each dose level (i.e. 20
mg, 50 mg, 100 mg, 200 mg and 400 mg venetoclax) pre-dose as well as 6-8 and 24 hours post-dose. Pre-existing electrolyte abnormalities should be corrected before initiation of treatment. For 100 mg, 200 mg and 400 mg ramp up in patients without increased risk of tumor lysis; pre-dose sampling can be done up to 24 h ahead of dosing at home.
Tumorlyse blodpr: (CAI, PHOS, K, CARB, CREA, LDH, MG, NA, URAT)
3) Overnight hospitalization is recommended for patients at increased risk of TLS (high tumor burden (e.g., any lymph node with a diameter ≥5 cm or high absolute lymphocyte count [ALC ≥25 x 109/L]), splenomegaly, renal dysfunction (CrCl < 80 mL/min), the presence of pre-treatment clinical chemistry abnormalities, or the presence of other co-morbidities) in order to allow more intensive prophylaxis and monitoring through the first 24 hours after initiating treatment with venetoclax. ( separat venotoclax skema for ramp-up perioden )
4) Objektiv undersøgelse inkluderer: hoved, øjne, ører, næse, hals, cardiovaskulær, dermatologisk, muskulatur, respiratorisk, gastroentestinal, neurologisk
5) ) Radiological assessment of lymphadenopathy, liver and spleen using imaging techniques (CT or MRI) is mandatory at final restaging (if abnormal at screening). The modality of staging in one patient should not be changed. Further imaging (even with ultrasound) can be performed at the investigator’s discretion, e.g. in case of a suspected PD.
6) Assessment recommended and to the investigator’s , but are not documented in the CRF.
7) EORTC QLQ-C30, EORTC QOL-CLL16 and questionnaires
8) Hæmatologi (LEU,DIFFMAS, THROM, RETIC, HB)
Biokemi: (CREA,BILI,ALAT,ASAT,LDH,NA,K,CL,PHOS,HCO3,CA,URAT,CARB)
9) Assement is recommended, but needed at cycle 1 day 15, following cycles only if considered indicated. Standard = (HB,TROM,LEU,CRP,K,CREA,NA)
10) Only for patients who are HBsAg negative/anti-HBc positive with negative PCR for HBV DNA (with a lower
limit of detection of the order of 10 WHO IU/mL) at screening; in this case HBV-DNA PCR must be performed every month until 1 year after last dosage of rituximab or obinutuzumab respectively. If the HBV DNA assay becomes positive, patients should pre-emptively be treated with a nucleoside analog (i.e.
CLL13 forsøgsarm GVe version 1 August 2016 Side 2 af 5

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Obinutuzumab (GVe) NAVN: CPR:
lamivudine) for at least twelve months after the last cycle of therapy or be referred to a gastroenterologist for management.
11) ≤7 days before start of study treatment and on day 1 of every treatment cycle (monthly) in all women of
childbearing potential
12) Additional samples for accompanying scientific program should be sent to Kiel and Ulm on cycle 2 day 1, (and in case of progression)
13) Samples for MRD testing should be sent to central lab in Kiel on cycle 1 day 1 and cycle 2 day 1
14) Bone marrow aspirate/biopsy must be performed together with measurement of MRD from the bone
marrow at final restaging, preferably together with MRD-testing of peripheral blood at MRD-staging 1(to be sent to the central lab in Kiel)
15) To be sent in case of progression only!
Dose modifications for Obinutuzumab : No dose modifacication will be performed for Obinutuzumab Obinutuzumab should be held in case of: - febrile infection - any CTC gradeIII/IV AEs (except hematological AEs that are due to bone marrow involvement of the CLL and thrombocytopenia during the first cycle, see below) In case of a febrile infection or CTC grade III/IV AEs, a weekly monitoring should be performed until the event resolves. Rituximab or obinutuzumab can be postponed for a maximum of 4 weeks (but please note that the appropriate treatment cycle won’t be prolonged). The last application of obinutuzumab or rituximab may not be performed after cycle 12 day 28. All antibody infusions that were not given until this timepoint must be skipped. Permanent discontinuation of rituximab or obinutuzumab is necessary in case of the following, however, treatment with venetoclax (and ibrutinib if applicable) may be continued: - CTC grade IV infusion related reaction, - IRR with acute life-threatening respiratory symptoms - CTC grade III infusion related reaction at re-challenge or prolonged or recurrent infusion reac-tions - anaphylaxis, acute respiratory distress Thrombocytopenias with obinutuzumab during the first cycle With obinutuzumab severe and life-threatening thrombocytopenias and even fatal hemorrhagic events were observed during the first 28 days of treatment. Therefore, patients should be closely monitored, especially during the first infusions. Dose delays should be considered in case of severe or life-threatening thrombocytopenia. Transfusion of blood products (i.e. platelet transfusion) according to institutional practice is at the discretion of the treating physician. All concomitant therapies, which could possibly worsen the thrombocytopenia itself or related events such bleedings (e.g. platelet inhibitors and anticoagulants), should also be rethought and discontinuation or dose reductions of these concomitant therapies should be taken into account. In case of severe thrombocytopenia on day 8 and 15, as defined as: - platelets < 10 x109/l, - platelets < 20 x109/l in patients with concomitant anticoagulant/platelet inhibitors and/or - symptomatic bleeding
CLL13 forsøgsarm GVe version 1 August 2016 Side 3 af 5

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Obinutuzumab (GVe) NAVN: CPR: The following guidelines should be followed: - hold obinutuzumab until the event resolves but do not skip any doses of obinutuzumab for sake of maintaining the schedule - patients with <20 x109/l platelets and administration of low molecular weight heparin (LMWH): hold of dose-reduction of LMWH is recommended - patients with <20 x109/l platelets and administration platelet inhibitors: temporary hold of platelet inhibitor is recommended2 Dose and schedule modifications for venetoclax In case of emerging adverse events during treatment with venetoclax, the following should be fol-lowed: Hematologic toxicity (unless directly attributable to the underlying CLL) Event Dose delay or dose modification Neutropenia (with or without fever and infection) CTC Grade 3 or 4
• Withhold venetoclax for at least 7 days • Administer G-CSF or growth factors for neutropenia as indicated • When counts recover to ANC ≥ 1 x109/l resume venetoclax at one dose
level reduction Thrombocytopenia CTC Grade 4 and/or symptomatic bleeding
• Withhold venetoclax • Platelets may be transfused at the discretion of the investigator • When platelet level rises to > 50x109/l without transfusional support for 5
consecutive days, restart venetoclax at previous dose For a second episode:
o Withhold venetoclax o When platelet level rises to > 50 x10^9/l without transfusional
support for 5 consecutive days, restart venetoclax at one dose level reduction
For subsequent episodes:
o Withhold venetoclax o When platelet level rises to > 50 x10^9/l without transfusional
support for 5 consecutive days, restart venetoclax at one dose level reduction
For recurrent episodes please consult the GCLLSG study office.
Non-hematologic events (e.g. infections) CTC Grade Dose delay or dose modification Grade 3 or 4 • Delay venetoclax for a maximum of 28 days.
• First episode: If improvement to Grade ≤ 1 or baseline, resume previous doses of venetoclax.
• For subsequent episodes: If improvement to Grade ≤ 1 or baseline, restart venetoclax at one dose level reduction.
Certain treatment emergent non-hematologic adverse events (e.g., venous thromboembolic events) may be managed and become clinically stable following medical intervention but may not improve to Grade ≤ 1 according to the NCI CTCAE definitions. In such cases resumption of study drug may be possible after consultation with the GCLLSG study office.
CLL13 forsøgsarm GVe version 1 August 2016 Side 4 af 5

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Obinutuzumab (GVe) NAVN: CPR: Grade 2 • Delay treatment with venetoclax until resolution to Grade ≤ 1 (or baseline
status) for a maximum of 28 days. • After resolution, resume full dose of venetoclax
Grade 1 • No dose reduction or delay
First dose of Venetoclax or dose escalation
• Within the first 24 hours after either the first dose or dose escalation, if any laboratory criteria below
are met, the patient should be hospitalized for monitoring and the investigator notified. No additional GDC-0199 doses should be administered until resolution. A rapidly rising serum potassium level is a medical emergency.
• Nephrology (or acute dialysis service) must be consulted/contacted on admission (per institutional standards to ensure emergency dialysis is available).
• Intravenous (IV) fluids (e.g., D5 1/2 normal saline) should be initiated at a rate of at least 1 mL/kg/h rounded to the nearest 10 mL (target 150 to 200 mL/hr; not < 50 mL/hr). Modification of fluid rate should also be considered for individuals with specific medical needs.
• Monitor for symptoms or signs of tumor lysis syndrome (TLS) (e.g., fever, chills, tachycardia, nausea, vomiting, diarrhea, diaphoresis, hypotension, muscle aches, weakness, paresthesias, mental status changes, confusion, and seizures). If any clinical features are observed, recheck potassium, phosphorus, uric acid, calcium, and creatinine within 1 hour STAT.
• Vital signs should be taken at time of all blood draws or any intervention.
• The management recommendations below focus on the minimum initial responses required. If a diagnosis of TLS is established, ongoing intensive monitoring and multidisciplinary management will be as per institutional protocols.
In addition to the recommendations in the table below, for patients with chronic lymphocytic leukemia (CLL)/ small lymphocytic lymphoma (SLL) receiving first dose of GDC-0199:
• For potassium increase ≥ 0.5 mmol/L from baseline, or any value > 5.0 mmol/L, recheck potassium,
phosphorus, uric acid, calcium, and creatinine within 1 hour STAT and follow first guideline.
• For phosphorus increase of >0.162 mmol/l AND >1,454 mmol/l, administer phosphate binder and recheck potassium, phosphorus, uric acid, calcium, and creatinine within 1 hour STAT.
CLL13 forsøgsarm GVe version 1 August 2016 Side 5 af 5

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Ibrutinib + Obinutuzumab (GIVe) NAVN: CPR:
År: Dato:
Scr
eeni
ng d
ag-
28-0
Serie Serie 1 Serie 2 Serie 3 Serie 4 Serie 5 Serie 6 Behandlingsuge 1 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Behandlingsdag 1 2 8 15 22 1 8 15 22 1 1 1 1
Behandling: PRÆ tavegyl pamol solumedrol, solumedrol pn efter 1. gang
0 0 0 0 0 0 0 0 0
Obinutuzumab 100 mg 0 Obinutuzumab 900 mg 0 Obinutuzumab 1000mg 0 0 0 0 0 0 0 Allopurinol1 300 mgx1 d.-3-end 6.serie 0 0 0 0 0 0 0 0 0 0 0 0 0 Ibrutinib dag 2 420 mg, kontinuerligt fra dag 1 0 0 0 0 0 0 0 0 0 0 0 0 0 Venetoclax, 20 mg 3 03 Venetoclax, 50 mg 3 03 Venetoclax, 100 mg 3 03 Venetoclax, 200 mg 3 03 Venetoclax, 400 mg 3 03 0 0 0 0 Sulfatrim 2 tbl man og tors TOM month 15
0 0 0 0 0 0
Undersøgelser Medicin status 0 0 0 0 0 0 Sygdomsstatus/ response evaluering.
0 TLS risiko vurdering4 0 0 0 0 0 0 0 0 0 Objektiv undersøgelse5 0 0 AE registering 0 0 0 0 0 0 ECOG + B symptomer 0 0 ECG/LEVF7 0 Livskvalitetsskema8 0 Vitale værdier 0 0 0 0 0 Højde, vægt 0 0 0 0 0 0 BLODPRØVER Labka :CLL139 0 0 0 0 0 0 Standard blpr10 0 0 Tumorlyseprøver3 0 0 0 0 0 0 0 HBV testing11 (0) (0) (0) (0) (0) (0) HcG (fødedygtige kvinder)12
0 0 0 0 0 0
Protokol prøver / PK MRD/ FISH
Accompanying scientfic program13 0 MRD from peripheral blood14 0 0
CLL13 forsøgsarm GIVe version 1 August 2016 Side 1 af 7

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Ibrutinib + Obinutuzumab (GIVe) NAVN: CPR:
0) Treatment must be started within 14 days after randomisation.
1) Allopurinol must be started 3 days before cycle 1 day 1, and be stopped after cycle 6.
2) For GIVe arm only; Ibrutinib will be started on cycle 1 day 1 (in the morning before breakfast) with a daily
oral intake of 420mg until MRD-negativity is reached in patients with CR or a maximum of 36 month or new CLL treatment or progression, whatever occurs first.
3) Laboratory assessments regarding to Venetoclax are required on the first day of each dose level (i.e. 20
mg, 50 mg, 100 mg, 200 mg and 400 mg venetoclax) pre-dose as well as 6-8 and 24 hours post-dose. Pre-existing electrolyte abnormalities should be corrected before initiation of treatment. For 100 mg, 200 mg and 400 mg ramp up in patients without increased risk of tumor lysis, pre-dose sampling can be done up to 24 h ahead of dosing at home.
Tumorlyseprøver:( CAI, PHOS, K, CARB,CREA,LDH,MG,NA,URAT)
4) Overnight hospitalization is recommended for patients at increased risk of TLS (high tumor burden (e.g.,
any lymph node with a diameter ≥5 cm or high absolute lymphocyte count [ALC ≥25 x 109/L]), splenomegaly, renal dysfunction (CrCl < 80 mL/min), the presence of pre-treatment clinical chemistry abnormalities, or the presence of other co-morbidities) in order to allow more intensive prophylaxis and monitoring through the first 24 hours after initiating treatment with venetoclax. ( separat venotoclax skema for ramp-up perioden )
5) Objektiv undersøgelse inkluderer: hoved, øjne, ører, næse, hals, cardiovaskulær, dermatologisk, muskulatur, respiratorisk, gastroentestinal, neurologisk
6) ) Radiological assessment of lymphadenopathy, liver and spleen using imaging techniques (CT or MRI) is mandatory at final restaging (if abnormal at screening). The modality of staging in one patient should not be changed. Further imaging (even with ultrasound) can be performed at the investigator’s discretion, e.g. in case of a suspected PD.
7) Assessment recommended and to the investigator’s , but are not documented in the CRF.
8) EORTC QLQ-C30, EORTC QOL-CLL16 and MARS questionnaires
9) Hæmatologi (LEU,DIFFMAS, THROM, RETIC, HB)
Biokemi: (CREA,BILI,ALAT,ASAT,LDH,NA,K,CL,PHOS,HCO3,CA,URAT,CARB)
CLL13 forsøgsarm GIVe version 1 August 2016 Side 2 af 7

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Ibrutinib + Obinutuzumab (GIVe) NAVN: CPR:
10) Assessment is recommended, but not needed at cycle 1 day 15, following cycles only if considered indicated. Standard = (HB,TROM,LEU,CRP,K,CREA,NA)
11) Only for patients who are HBsAg negative/anti-HBc positive with negative PCR for HBV DNA (with a lower limit of detection of the order of 10 WHO IU/mL) at screening; in this case HBV-DNA PCR must be performed every month until 1 year after last dosage of rituximab or obinutuzumab respectively. If the HBV DNA assay becomes positive, patients should pre-emptively be treated with a nucleoside analog (i.e. lamivudine) for at least twelve months after the last cycle of therapy or be referred to a gastroenterologist for management.
12) ≤7 days before start of study treatment and on day 1 of every treatment cycle (monthly) in all women of
childbearing potential
13) Additional samples for accompanying scientific program should be sent to Kiel and Ulm on cycle 2 day 1, (and in case of progression)
14) Samples for MRD testing should be sent to central lab in Kiel on cycle 1 day 1 and cycle 2 day 1
15) Bone marrow aspirate/biopsy must be performed together with measurement of MRD from the bone
marrow at final restaging, preferably together with MRD-testing of peripheral blood at MRD-staging 1(to be sent to the central lab in Kiel)
16) To be sent in case of progression only!
Dose modifications for Obinutuzumab : No dose modifacication will be performed for Obinutuzumab Obinutuzumab should be held in case of: - febrile infection - any CTC gradeIII/IV AEs (except hematological AEs that are due to bone marrow involvement of the CLL and thrombocytopenia during the first cycle, see below) In case of a febrile infection or CTC grade III/IV AEs, a weekly monitoring should be performed until the event resolves. Rituximab or obinutuzumab can be postponed for a maximum of 4 weeks (but please note that the appropriate treatment cycle won’t be prolonged). The last application of obinutuzumab or rituximab may not be performed after cycle 12 day 28. All antibody infusions that were not given until this timepoint must be skipped. Permanent discontinuation of rituximab or obinutuzumab is necessary in case of the following, however, treatment with venetoclax (and ibrutinib if applicable) may be continued: - CTC grade IV infusion related reaction, - IRR with acute life-threatening respiratory symptoms - CTC grade III infusion related reaction at re-challenge or prolonged or recurrent infusion reac-tions - anaphylaxis, acute respiratory distress Thrombocytopenias with obinutuzumab during the first cycle With obinutuzumab severe and life-threatening thrombocytopenias and even fatal hemorrhagic events were observed during the first 28 days of treatment. Therefore, patients should be closely monitored, especially during the first infusions. Dose delays should be considered in case of severe or life-threatening thrombocytopenia. Transfusion of blood products (i.e. platelet transfusion) according to institutional practice is at the discretion of the
CLL13 forsøgsarm GIVe version 1 August 2016 Side 3 af 7
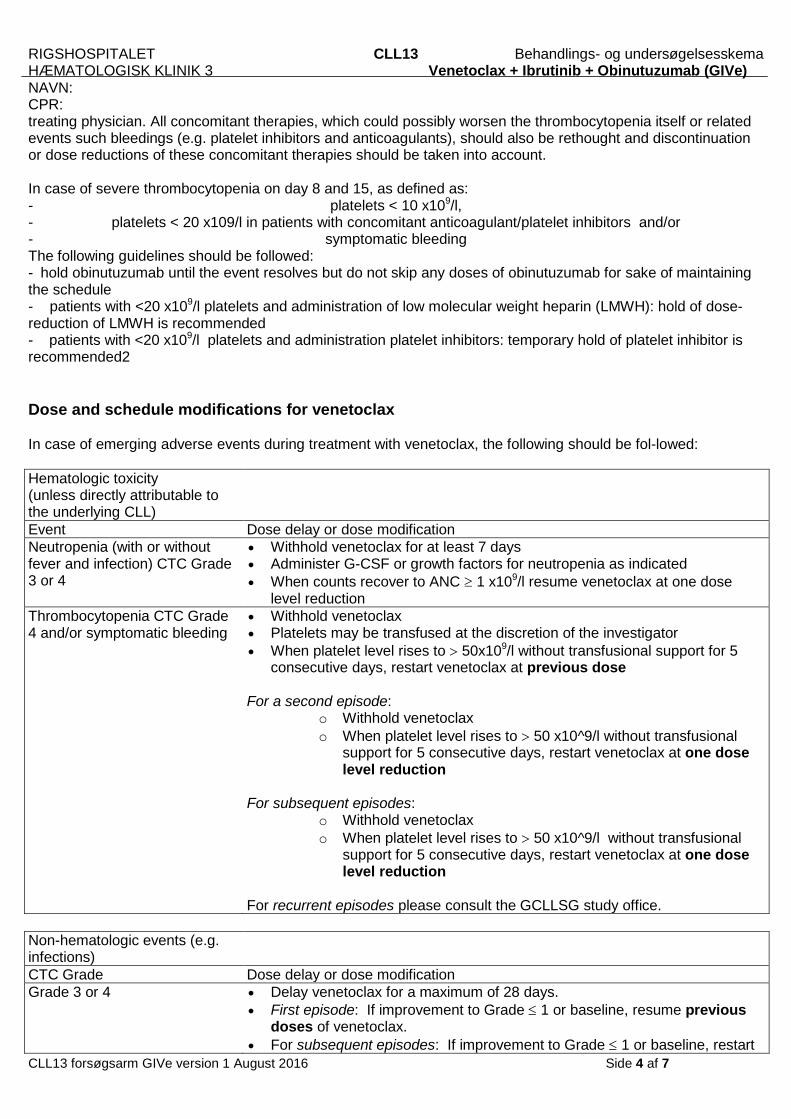
RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Ibrutinib + Obinutuzumab (GIVe) NAVN: CPR: treating physician. All concomitant therapies, which could possibly worsen the thrombocytopenia itself or related events such bleedings (e.g. platelet inhibitors and anticoagulants), should also be rethought and discontinuation or dose reductions of these concomitant therapies should be taken into account. In case of severe thrombocytopenia on day 8 and 15, as defined as: - platelets < 10 x109/l, - platelets < 20 x109/l in patients with concomitant anticoagulant/platelet inhibitors and/or - symptomatic bleeding The following guidelines should be followed: - hold obinutuzumab until the event resolves but do not skip any doses of obinutuzumab for sake of maintaining the schedule - patients with <20 x109/l platelets and administration of low molecular weight heparin (LMWH): hold of dose-reduction of LMWH is recommended - patients with <20 x109/l platelets and administration platelet inhibitors: temporary hold of platelet inhibitor is recommended2 Dose and schedule modifications for venetoclax In case of emerging adverse events during treatment with venetoclax, the following should be fol-lowed: Hematologic toxicity (unless directly attributable to the underlying CLL) Event Dose delay or dose modification Neutropenia (with or without fever and infection) CTC Grade 3 or 4
• Withhold venetoclax for at least 7 days • Administer G-CSF or growth factors for neutropenia as indicated • When counts recover to ANC ≥ 1 x109/l resume venetoclax at one dose
level reduction Thrombocytopenia CTC Grade 4 and/or symptomatic bleeding
• Withhold venetoclax • Platelets may be transfused at the discretion of the investigator • When platelet level rises to > 50x109/l without transfusional support for 5
consecutive days, restart venetoclax at previous dose For a second episode:
o Withhold venetoclax o When platelet level rises to > 50 x10^9/l without transfusional
support for 5 consecutive days, restart venetoclax at one dose level reduction
For subsequent episodes:
o Withhold venetoclax o When platelet level rises to > 50 x10^9/l without transfusional
support for 5 consecutive days, restart venetoclax at one dose level reduction
For recurrent episodes please consult the GCLLSG study office.
Non-hematologic events (e.g. infections) CTC Grade Dose delay or dose modification Grade 3 or 4 • Delay venetoclax for a maximum of 28 days.
• First episode: If improvement to Grade ≤ 1 or baseline, resume previous doses of venetoclax.
• For subsequent episodes: If improvement to Grade ≤ 1 or baseline, restart CLL13 forsøgsarm GIVe version 1 August 2016 Side 4 af 7

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Ibrutinib + Obinutuzumab (GIVe) NAVN: CPR:
venetoclax at one dose level reduction. Certain treatment emergent non-hematologic adverse events (e.g., venous thromboembolic events) may be managed and become clinically stable following medical intervention but may not improve to Grade ≤ 1 according to the NCI CTCAE definitions. In such cases resumption of study drug may be possible after consultation with the GCLLSG study office.
Grade 2 • Delay treatment with venetoclax until resolution to Grade ≤ 1 (or baseline status) for a maximum of 28 days.
• After resolution, resume full dose of venetoclax
Grade 1 • No dose reduction or delay
Dose and schedule modifications for ibrutinib
The below actions should be taken for the following toxicities unless they are directly attributable to the underlying CLL by the judgment of the investigator:
• Grade 4 neutropenia (ANC <0.5 x 109/L) for >14 days
• Grade 3 thrombocytopenia (platelets <50 x 109/L) in the presence of ≥ Grade 2 bleeding
• Grade 4 thrombocytopenia (platelets <25 x 109/L)
• Grade 3 or 4 nausea, vomiting, or diarrhea (if persistent despite optimal antiemetic or anti-diarrhea therapy)
• any Grade 3 toxicity that is not resolving with medical management
• any other Grade 4 toxicity
4 Dose reduction and modification guidelines for ibrutinib
Occurrence of the same AE/SAE
Action
First hold ibrutinib until recovery to Grade ≤1 or baseline; may restart at original dose level
Second hold ibrutinib until recovery to Grade ≤1 or baseline; restart at 1 dose level lower (280 mg daily)
Third hold ibrutinib until recovery to Grade ≤1 or baseline; restart at 1 dose level lower (140 mg daily)
Fourth discontinue ibrutinib
Ibrutinib may be held for a maximum of 28 consecutive days. After 28 days the investigator may decide to continue treatment after consultation of the GCLLSG study office.
No reescalation of ibrutinib in case of dose reductions and especially no dose escalation to more than 3 capsules/day (= above 420 mg) is permitted in this study.
CLL13 forsøgsarm GIVe version 1 August 2016 Side 5 af 7

RIGSHOSPITALET CLL13 Behandlings- og undersøgelsesskema HÆMATOLOGISK KLINIK 3 Venetoclax + Ibrutinib + Obinutuzumab (GIVe) NAVN: CPR:
First dose of Venetoclax or dose escalation
• Within the first 24 hours after either the first dose or dose escalation, if any laboratory criteria below are met, the patient should be hospitalized for monitoring and the investigator notified. No additional GDC-0199 doses should be administered until resolution. A rapidly rising serum potassium level is a medical emergency.
• Nephrology (or acute dialysis service) must be consulted/contacted on admission (per institutional standards to ensure emergency dialysis is available).
• Intravenous (IV) fluids (e.g., D5 1/2 normal saline) should be initiated at a rate of at least 1 mL/kg/h rounded to the nearest 10 mL (target 150 to 200 mL/hr; not < 50 mL/hr). Modification of fluid rate should also be considered for individuals with specific medical needs.
• Monitor for symptoms or signs of tumor lysis syndrome (TLS) (e.g., fever, chills, tachycardia, nausea, vomiting, diarrhea, diaphoresis, hypotension, muscle aches, weakness, paresthesias, mental status changes, confusion, and seizures). If any clinical features are observed, recheck potassium, phosphorus, uric acid, calcium, and creatinine within 1 hour STAT.
• Vital signs should be taken at time of all blood draws or any intervention.
• The management recommendations below focus on the minimum initial responses required. If a diagnosis of TLS is established, ongoing intensive monitoring and multidisciplinary management will be as per institutional protocols.
In addition to the recommendations in the table below, for patients with chronic lymphocytic leukemia (CLL)/ small lymphocytic lymphoma (SLL) receiving first dose of GDC-0199:
• For potassium increase ≥ 0.5 mmol/L from baseline, or any value > 5.0 mmol/L, recheck potassium, phosphorus, uric acid, calcium, and creatinine within 1 hour STAT and follow first guideline.
• For phosphorus increase of >0.162 mmol/l AND >1,454 mmol/l, administer phosphate binder and recheck potassium, phosphorus, uric acid, calcium, and creatinine within 1 hour STAT
CLL13 forsøgsarm GIVe version 1 August 2016 Side 6 af 7