right heart failure
TRANSCRIPT

Right Heart Failure
COURTNEY SCHILMILLER, APRN, MSN, ACNP-BCUNIVERSITY OF LOUISVILLE, DEPARTMENT OF
CARDIOVASCULAR AND THORACIC SURGERY

Disclosures:
None

Objectives:
1. Right Heart Hemodynamics
2. Recognizing Right Heart Problems
3. Differentiating Right Heart Failure
4. Treating Right Heart Failure
Why do we care?
Right Heart Failure accounts for 3 - 9% of acute heart failure admissions
In‐hospital mortality 5 - 17%
Mortality as high as LV Failure
75% of our patients have severe right ventricular dysfunction prior to LVAD implant
20-50% of patients post LVAD experience complications
Meineri. M., Rensburg, A., and Vegas. A. (2012). Right ventricular failure after LVAD implantation: prevention and treatment. Retrieved from: https://pubmed.ncbi.nlm.nih.gov/22910091/

Causes of Right Ventricular Failure?
Acute Progressive
Pulmonary Embolism Pulmonary Hypertension
Right Sided MI Left Ventricular Failure

Right Heart Hemodynamics
Cardiac
OutputStroke Volume Heart Rate
Preload
Afterload
Contractility

Right
Heart Contractility
https://www.quizover.com/biology3/course/8-1-heart-anatomy-by-openstax-heart?page=3

Diagnosis of
Right Heart
Failure
Systemic Venous
Congestion
RUQ discomfort,
Epigastric
Fullness
Elevated Central Venous
Pressure
BNP, AST/ALT, T.bili, creatinine,
Elevated lactate
Echo

Echocardiogram

Echocardiogram

Assessing RV Function: TAPSE-
Tricuspid Annular Plane Systolic
Excursion
Bedside echo
Normal is > 2.0 cm
Correlates with RV systolic
functionSchmid, L., Hilbreth, J., Blumenstock.G, Shekar, P., King, S., Sherman. S., Rosenberger. P., & Nowak-Machen. M. (2015). Tricuspid annular plane systolic excursion (TAPSE) predicts poor outcome in patients undergoing acute
pulmonary embolectomy. Heart Lung And Vessels 7(2), 151–158. Retrieved from:https://ubpem.files.wordpress.com/2020/06/tapse.pdf

Assessing RV Function: Pulmonary
Artery Pulsatility Index (PAPi)
PAPi =systolic pulmonary artery pressure – diastolic
pulmonary artery pressure)/central venous pressure
The physiological basis for PAPi as an indicator of
right heart function is predicated on PASP as an
indirect indicator of RV contractile function against
a given afterload, and high CVP as a sign of failing
right ventricle
Normal PAPi is > 1
Guson. K., Richard. H., & Dipanjan., B. (2016). Pulmonary artery pulsatility index predicts right ventricular failure after left ventricular assist device implantation. The Journal of Heart and Lung Transplantation

Three Types of Right Heart Failure
1. Preload problem – Volume overload
2. Contractility problem – RV failure with
normal afterload
3. Afterload problem – RV failure with
increased afterload

Ventetuolo C, Klinger J; Management of Acute Right Ventricular Failure in the Intensive Care Unit; Annals ATS; 2014;11:811-22

Treatment
Based on Which Problem??? Optimize
hemodynamics1. Preload problem – Volume overload-DIURESIS, Ultrafiltration
2. Contractility problem – RV failure with normal afterload-Inotropes
Milrinone + Vaso, Epinephrine
3. Afterload problem – RV failure with increased afterload. Correct
hypercapnia, acidosis, and hypoxia. Pulmonary vasodilators-iFlolan,
iNO
4. VA ECMO

Common Misconception: Volume
Administration RV can physiologically accommodate large variations in preload
Some patients with RV failure are preload dependent-be gentle!!
Delicate balance
A substantial amount RV failure is caused, associated with or aggravated by RV volume overload.
Volume administration → RV overdistention →Increased wall tension → Decreased RV contractility → Worsening tricuspid regurgitation → Decreased LV filling → Reduced systemic cardiac output → End organ malperfusion →Cardiogenic shock
Ventetuolo, C. & Klinger J. Management of Acute Right Ventricular Failure in the Intensive Care Unit. (2014). Annals ATS. June; 2014; 11 (5), 811-822.

Cardiorenal syndrome
In patients with RV dysfunction, you
have decreased arterial perfusion to
kidneys, compounded by increased
venous congestion, which further
decreases renal blood flow.
Both partially responsible for AKI in
decompensated heart failure

Fundamentals of Veno-Venous
(VV) and Veno-Arterial (VA)
Extracorporeal Membrane
Oxygenation (ECMO)

Objectives:
1. List the indications for ECMO in
management of severe respiratory or
circulatory failure.
2. Basics of cannulation techniques and sites
3. Describe basic physiology during ECMO
4. Common complications of the patient on
ECMO

What is ECMO?
ECMO is a form of cardiopulmonary life-
support, where blood is drained from the
vascular system, circulated outside the
body by a mechanical pump, and then
returned into the circulation.
Brief History
1916-Heparin discovered
1944-discovered that blood became oxygenated as it passed through the cellophane chambers of an artificial kidney
1953-Gibbon used artificial oxygenation and perfusion support (cardiopulmonary bypass) for the first successful open-heart operation
1972- Long-term ECMO as support for severe respiratory failure in an adult patient with post-traumatic respiratory failure
1989-ELSO Founded-Best Practices
2009-H1N1 flu pandemic and CESAR Trial-clearly showed an improvement in the death rate and severe disability 6 months after randomization of patients with severe respiratory failure treated with ECMO in an expert high-case-volume center compared with no specialized hospital care.
Makdisi, G. & Wang, I. (2015). Extra Corporeal Membrane Oxygenation (ECMO) review of a lifesaving technology. Journal of Thoracic Disease, Jul; 7(7): E166–E176

Jewish Hospital Data-2020
Multi-disciplinary Team-Surgeon, Cardiologists, Pulmonologists, Perfusionists, Intensivists, APPs, RNs, RTs.
Higher success rate in weaning patients from VV ECMO verses VA ECMO
In 2020 we placed a total of 50 patients on ECMO.
56% patients were successfully weaned off
44% patients were discharged from the facility

ECMO Indications for cardiac support (VA ECMO only)
1. Cardiogenic shock: Severe cardiac failure due to almost any cause:
▪ acute coronary syndrome
▪ cardiac arrhythmic storm refractory to other measures
▪ sepsis with profound cardiac depression
▪ drug overdose/toxicity with profound cardiac depression
▪ myocarditis
▪ pulmonary embolism
▪ isolated cardiac trauma
▪ acute anaphylaxis
2. Post cardiotomy: inability to wean from cardiopulmonary bypass after cardiac surgery
3. Post heart transplant: primary graft failure after heart or heart-lung transplantation
4. Chronic cardiomyopathy:
▪ as a bridge to longer term VAD support
▪ or as a bridge to decision
5. Periprocedural support for high-risk percutaneous cardiac interventions
6. Bridge to transplant
Makdisi, G. & Wang, I. (2015). Extra Corporeal Membrane
Oxygenation (ECMO) review of a lifesaving technology.
Journal of Thoracic Disease, Jul; 7(7): E166–E176

ECMO indications for respiratory support
1. Acute respiratory distress syndrome:
▪ severe bacterial or viral pneumonia
▪ aspiration syndromes
▪ alveolar proteinosis
2. Extracorporeal assistance to provide lung rest:
▪ airway obstruction
▪ pulmonary contusion
▪ smoke inhalation
3. Lung transplant:
▪ primary graft failure after lung transplantation
▪ bridge to lung transplant
▪ intaroperative ECMO
4. Lung hyperinflation:
▪ status asthmaticus
5. Pulmonary hemorrhage or massive hemoptysis
Makdisi, G. & Wang, I. (2015). Extra Corporeal Membrane
Oxygenation (ECMO) review of a lifesaving technology.
Journal of Thoracic Disease, Jul; 7(7): E166–E176

Contrain
dications
to ECMO
Absolute: among these futile treatment without exit strategy in case
of
-Unrecoverable heart and not a candidate for transplant or
destination therapy of VAD support
-Disseminated malignancy
-Known severe brain injury
-Unwitnessed cardiac arrest
-Prolonged CPR without adequate tissue perfusion
-Unrepaired aortic dissection
-Severe aortic regurgitation
-Severe chronic organ dysfunction (emphysema, cirrhosis, renal
failure)
-Compliance (financial, cognitive, psychiatric, or social limitations
in patient without social support)
-Peripheral vascular disease is contraindicated in peripheral VA
ECMO
-VV ECMO is contraindicated in cardiogenic failure and in Severe
chronic pulmonary hypertension (mean pulmonary artery pressure
>50 mmHg)
Relative: contraindication for anticoagulation, advanced age,
obesityAnnich, G., Lynch, W., MacLaren, G., Wilson, J., and Bartlett, R. (2012). Extracorporeal Cardiopulmonary Support in Critical Care 4th Ed

ECMO Physiology-What is going
On? ECMO support is initiated when the patient is
connected to the ECMO circuit. The deoxygenated blood will be drained from the patient through a drainage cannula under negative pressure created by a centrifugal pump, then entering the oxygenator, where gas exchange occurs. Then, blood is returned back to the patient through the return cannula.
Goal is to supply oxygenated blood to meet the metabolic requirements and remove metabolic waste.



Oxygenator Specification: Provides oxygenation AND ventilation
Flow in Oxygenation controlled by FiO2
Ventilation controlled inversely by “Sweep Rate”
Sweep rate is analogous to minute ventilation
Max Blood flow: 7 LPM
Minimum Sweep rate: 1 LPM, unless weaning
Max Sweep rate: 15 LPM

VV ECMO Goals:
1. Support oxygenation and ventilation (gas exchange)
when lungs can’t
2. Lung Protective Ventilation “10/10/10”
• Rate: 10 BPM
• FiO2 : 40-60%
• Inspiratory Pressure 10
• PEEP: preferably 10 cmH2O
• Tidal Volume: 6-8 mL/kg of ideal body weight
HEART FUNCTION MUST BE PRESERVED!!
Must Monitor for Right Ventricular Failure

VV ECMO Cannulation Dual Lumen Bicaval cannulation
Right Internal Jugular
Both drainage and return lumens in one cannula
Requires precise placement. Drainage ports in SVC/IVC and return to
tricuspid valve and returns oxygenated blood to right ventricle
Two separate cannulas
Femoral Vein/Femoral Vein
Drainage cannula tip at IVC/RA junction
Right Internal Jugular Vein/Femoral Vein
Return cannula tip at SVC/RA junction
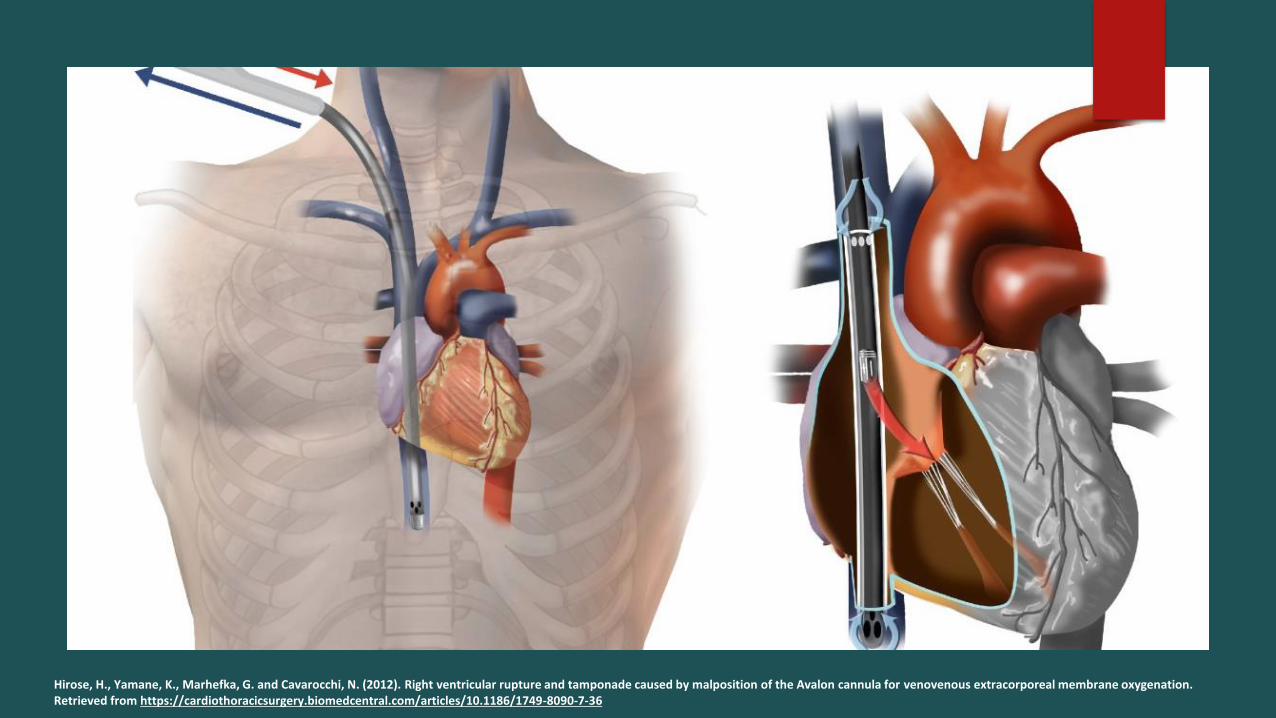
Hirose, H., Yamane, K., Marhefka, G. and Cavarocchi, N. (2012). Right ventricular rupture and tamponade caused by malposition of the Avalon cannula for venovenous extracorporeal membrane oxygenation. Retrieved from https://cardiothoracicsurgery.biomedcentral.com/articles/10.1186/1749-8090-7-36

Dual Lumen Bicaval cannulation in patient with femorally inserted
Impella + Pulmonary Artery Catheter

Image from MC3 Cardiopulmonary. The ECMO Company.
VV ECMO-
Bicaval,
dual-lumen
cannula
Hypercapnic Respiratory Failure
VV ECMO support due to
hypercapnic respiratory failure, avoid
rapid corrections of hypercapnia
when initiating ECMO support. Failing
to do so might promote alkalemia, as
well as cerebral vasoconstriction.
Annich, G., Lynch, W., MacLaren, G., Wilson, J., and Bartlett, R. (2012). Extracorporeal Cardiopulmonary Support in Critical Care 4th Ed.

Troubleshooting Problems encountered
with VV ECMO: Recirculation
Recirculation- reinfused oxygenated blood is withdrawn through the
drainage cannula without passing through the systemic circulation
Decreases level of support provided
Identification: Increase in pre-oxygenator saturation and arterial
saturations, notice similar blood color in cannulas
Causes:
Cannula position are too close together
Higher flow rate and cannula size
Changes in intrathoracic pressure
Ptx, tamponade, anything that impedes venous return
Annich, G., Lynch, W., MacLaren, G., Wilson, J., and Bartlett, R. (2012). Extracorporeal Cardiopulmonary Support in Critical Care 4th Ed.



VA ECMO
Goal:
To restore organ blood flow and
prevent end organ mal-perfusion

VA ECMO Cannulation Sites
Central Cannulation
Open chest-Post cardiotomy failure
Drainage cannula directly in right atrium
Return cannula in ascending aorta
Peripheral
Femoral Vein-Drainage tip at level of RA
Opposite Femoral Artery-Return tip in common iliac artery
Provides flow down opposite extremity and retrograde flow
up the aorta
Distal perfusion cannula to provide

Troubleshooting: Harlequin
Syndrome VA ECMO-perfusate blood from ECMO mixes in the aorta with the
blood ejected from the left ventricle
Content of oxygen and carbon dioxide in the patient’s arterial
blood represents a combination of blood from the above sources
Severe myocardial dysfunction
Mixing zone will be in proximal ascending aorta or aortic root
As myocardial function improves the mixing point moves distally into
the descending aorta
With significant pulmonary edema, hypoxic blood will perfuse the upper body. Thus, the patient’s upper body will appear blue, while
the lower body will appear pink
Short, B. and Williams, L. (2010). ECMO Specialist Training Manual 3rd Ed.

Left Ventricular Unloading in VA-
ECMO
LV Distention: LV Thrombus, Pulmonary
hemorrhage
Preload Reduction-Impella in conjunction
with VA ECMO
Afterload Reduction with Intra Aortic
Balloon Pump
Therapeutic anti-coagulation is essential

Bleeding and Thrombotic
Considerations & Complications
-Inflammatory Response
-Procoagulant mechanisms are activated
-Consumptive coagulopathy
-ECMO therapy leads to thrombocytopenia,
factor XIII and fibrinogen deficiency as well as
acquired von Willebrand syndrome.
Quantitative and qualitative platelet
dysfunction due to activation and
consumption

Anti-coagulation
ECMO circuit contains heparin
Requires systemic anti-coagulation with Heparin or Argatroban.
10% and 33% of patients on ECMO support experience thrombotic or bleeding events.
Fibrin/Clot identification
check pre/post oxygenator
Trend ABGs
Pressures in lines

APP Roles & Responsibilities Patient Preparation:
All necessary lines should be inserted prior to ECMO cannulation
Right Radial Aline-preferable for peripheral VA ECMO
“Prep” patient appropriately
Ensure the patient is adequately sedated and paralyzed
Have inotropes and vasopressor infusions
4 units of blood ordered to maintain a “post-ECMO initiation” Hgb of 8.0 g/L
Notify Blood Bank to keep 4 units pRBC on hold at all times during ECMO
Have anestheisa with TEE ready to ensure correct guidewire and cannula
placement
“ECMO” Bed with mapping system (pre-ECMO, time permitting)

Ethical Considerations:
“Just because we can, doesn’t mean we should”
Discussions with family
Time frame
Realistic Expectations
Palliative (Family Support Team) Care

Up and Coming
ECMO Transport Team

References: Annich, G., Lynch, W., MacLaren, G., Wilson, J., and Bartlett, R. (2012). Extracorporeal Cardiopulmonary Support in Critical Care 4th Ed.
Cresent cannula image from mc3corp.com
Guson. K., Richard. H., & Dipanjan., B. (2016). Pulmonary artery pulsatility index predicts right ventricular failure after left ventricular assist device implantation. The Journal of Heart and Lung Transplantation. January; 35(1), 67-73. Retrieved July 1, 2021 from Science Direct database.
Hirose, H., Yamane, K., Marhefka, G. and Cavarocchi, N. (2012). Right ventricular rupture and tamponade caused by malposition of the Avalon cannula for venovenous extracorporeal membrane oxygenation. Retrieved from https://cardiothoracicsurgery.biomedcentral.com/articles/10.1186/1749-8090-7-36
Makdisi, G. & Wang, I. (2015). Extra Corporeal Membrane Oxygenation (ECMO) review of a lifesaving technology. Journal of Thoracic Disease,
July; 7(7): E166–E176. Retrieved June 20, 2021.
Meineri. M., Rensburg, A., and Vegas. A. (2012). Right ventricular failure after LVAD implantation: prevention and treatment. Retrieved from: https://pubmed.ncbi.nlm.nih.gov/22910091/.
Schmid, L., Hilbreth, J., Blumenstock.G, Shekar, P., King, S., Sherman. S., Rosenberger. P., & Nowak-Machen. M. (2015). Tricuspid annular plane
systolic excursion (TAPSE) predicts poor outcome in patients undergoing acute pulmonary embolectomy. Heart Lung And Vessels 7(2), 151–
158. Retrieved from: https://ubpem.files.wordpress.com/2020/06/tapse.pdf
Short, B. and Williams, L. (2010). ECMO Specialist Training Manual 3rd Ed.
Ventetuolo, C. & Klinger J. Management of Acute Right Ventricular Failure in the Intensive Care Unit. (2014). Annals ATS. June; 2014; 11 (5), 811-822.