review article pauci-immune crescentic glomerulonephritis...
TRANSCRIPT
Review ArticlePauci-Immune Crescentic GlomerulonephritisAn ANCA-Associated Vasculitis
Rafeel Syed Amina Rehman Gautam Valecha and Suzanne El-Sayegh
Division of Nephrology Staten Island University Hospital 475 Seaview Avenue Staten Island NY 10305 USA
Correspondence should be addressed to Rafeel Syed rafeel syedhotmailcom
Received 3 September 2015 Revised 15 November 2015 Accepted 17 November 2015
Academic Editor Monica Carmosino
Copyright copy 2015 Rafeel Syed et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Rapidly progressive glomerulonephritis (RPGN) is a syndrome signified by a precipitous loss of renal function with features ofglomerulonephritis including dysmorphic erythrocyturia and glomerular proteinuria RPGN is associated with extensive crescentformation and thus the clinical term RPGN is often used interchangeably with the pathologic term crescentic glomerulonephritis(CGN) From an immunopathologic standpoint primary RPGN is divided into pauci-immune GN (PICG) anti-GBM GN andimmune complex GN PICG the most common etiology of primary RPGN refers to a necrotizing glomerulonephritis with fewor no immune deposits by immunofluorescence (IF) or electron microscopy (EM) In most patients pauci-immune CGN is acomponent of a systemic small vessel vasculitis such as granulomatosis with polyangiitis (GPA) Approximately 90 of patientswith PICG have circulating ANCA antibodies leading to the nomenclature ANCA-associated vasculitis (AAV) Recent researchhas identified several other antibodies associated with PICG which is now understood to be a complex spectrum of disease withconsiderable overlap in terms of clinical phenotype and outcomes In addition several genetic and environmental factors haverecently been implicated in the pathogenesis of this disorder With new prognostic classifications enhanced understanding ofimmunopathologic mechanisms and novel treatment paradigms clinical and experimental interest in PICG remains high
1 Introduction Epidemiology andClinical Outcomes
At a population level little is known about the epidemiologyand outcome of pauci-immune GN PICG represents up to80 of cases of RPGN the incidence of which is estimatedto be 7ndash10 cases per million people per year in the UnitedStates [1] Pauci-immune GN (PICG) has a predilection forwhites compared to blacks with roughly equal representationin men and women [1] Interestingly GPA is more commonin cooler climates whereas MPA is more frequent in warmerclimates AAV in Asia is more often associated with MPO-ANCA than with PR3-ANCA [2] Without treatment PICGhas a 1-year mortality of 80 With aggressive immuno-suppression however the 5-year survival is up to 75 [3]Older age dialysis dependency and pulmonary hemorrhageall worsen the chances of survival For instance irreversibledialysis-dependent renal failure lowers the 5-year survivalrate to 35 From a renal outcome standpoint about 25of patients progress to ESRD [4] The best predictor of renal
outcomes is the initial serum creatinine as well as the extentof renal injury and fibrosis on biopsy Although remissioncan be induced in most patients about 40 of patientsrelapse indicating the need for closemonitoring [1] Here wepresent a case of renal-limited PICG presenting with dialysis-dependent renal failureThe ensuing discussion aims to detailthe pathophysiology of PICG while highlighting possibleavenues for future scientific inquiry
2 Nomenclature and Classification
Though descriptive and current the classification ldquopauci-immunerdquo glomerulonephritis can be somewhat incompleteand misleading Historically the term was coined to charac-terize the lack of linear immunoglobulin (type I) or immunecomplex (type II) deposition on immunofluorescence [1]This however does not imply that the immune system isnot involved in the pathogenesis of the disease process ONthe contrary pauci-immune GN is a classically autoimmunerenal disease and is thus treated as such
Hindawi Publishing CorporationBioMed Research InternationalVolume 2015 Article ID 402826 8 pageshttpdxdoiorg1011552015402826
2 BioMed Research International
Despite efforts to simplify the classification system theterm ldquopauci-immune glomerulonephritisrdquo represents intri-cate and overlapping ldquospectrumrdquo of disease processes Weknow that about 10of the cases in the pathologic continuumof PICG are ANCA negative despite similar clinical featuresand renal biopsy findings as compared to ANCA-positivecases [1] In addition although pauci-immune necrotizingGN typically occurs in association with involvement of otherorgans in both GPA and MPA some patients present with arenal-limited ANCA-positive vasculitis Up to 80 of thesepatients have MPO-ANCA positivity while the remaininghave anti-PR3-ANCA antibodies [5] The patient presentedin this review has anti-PR3-ANCA which upon remissioncarries a higher relapse rate and an overall worse prognosisRenal-limited vasculitis is considered to be part of thespectrum of GPA and MPA because the histopathologicfindings of the two conditions are often indistinguishable[6] Clinically patients with renal-limited vasculitis are morelikely to have glomerulosclerosis on renal biopsy than thosewith GPA or MPA since patients without extrarenal mani-festations probably present later in the course of their disease[6] Adding to the complexity of the clinical phenotypesome patients have small dispersed immune deposits inthe mesangium and glomerular capillary wall when assessedby electron microscopy This in the proper clinical set-ting and positive ANCA antibodies is still classified asldquopauci-immunerdquo glomerulonephritis [7] Lastly the entity ofldquodouble-antibodyrdquo positive disease must also be mentionedas it includes patients with features of both ANCA-positiveRPGN and anti-GBM disease [8]
3 Case
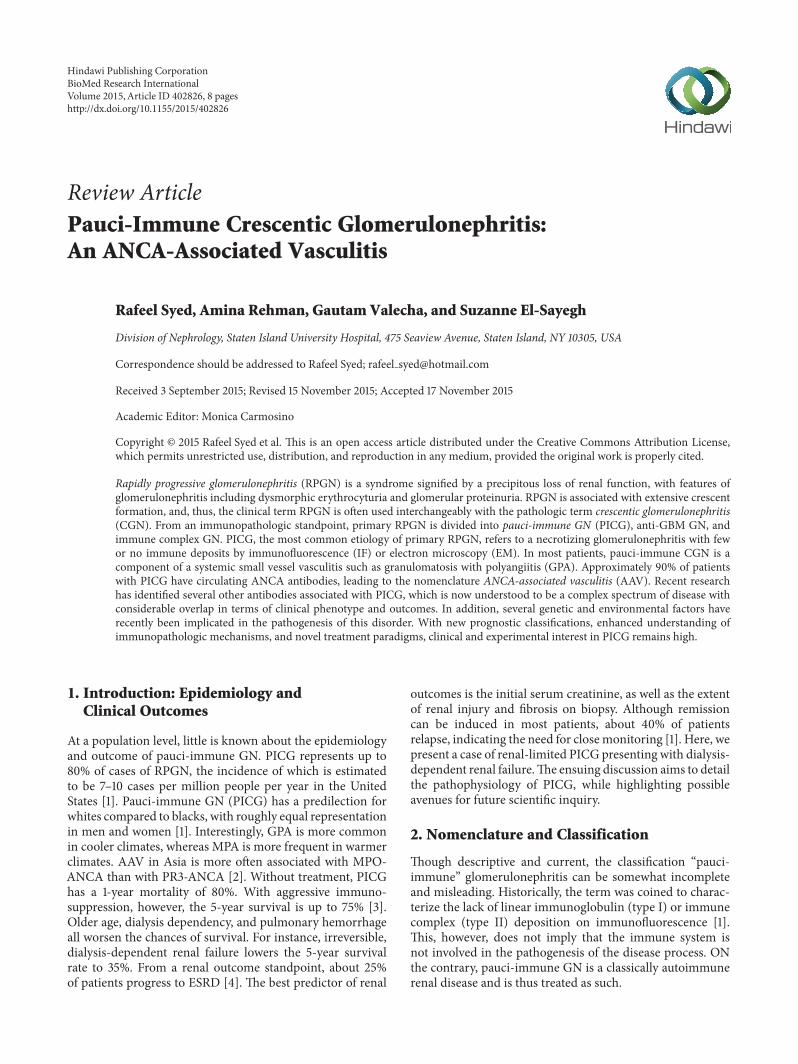
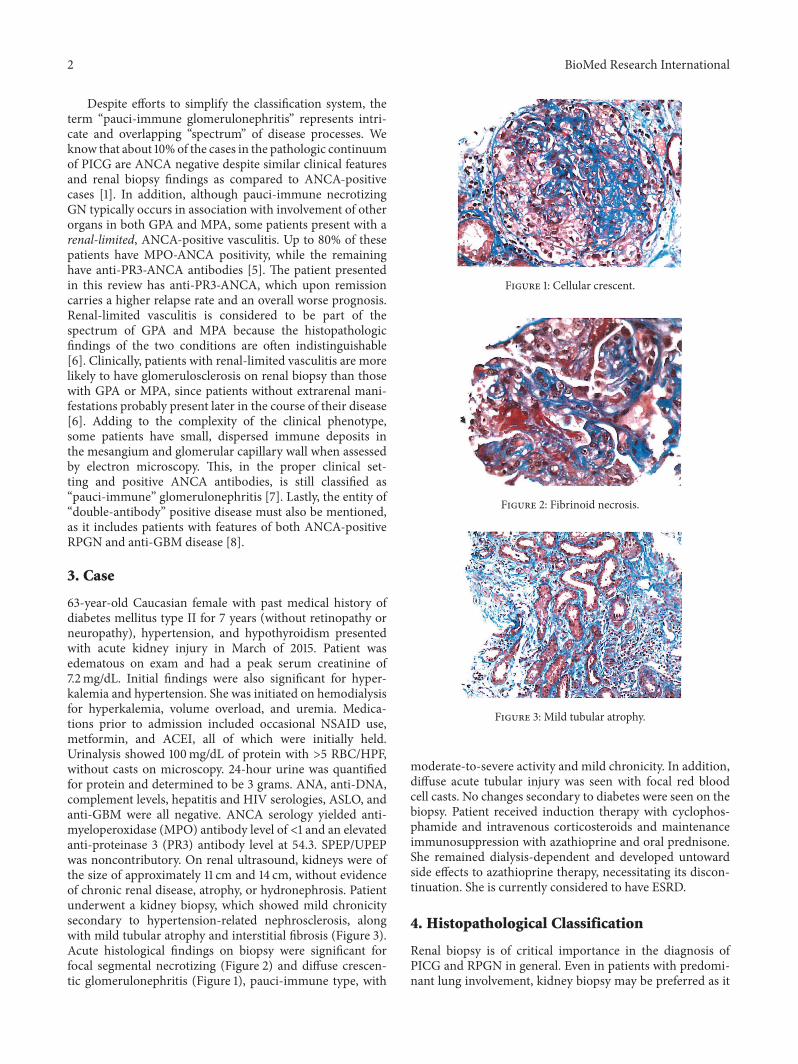
63-year-old Caucasian female with past medical history ofdiabetes mellitus type II for 7 years (without retinopathy orneuropathy) hypertension and hypothyroidism presentedwith acute kidney injury in March of 2015 Patient wasedematous on exam and had a peak serum creatinine of72mgdL Initial findings were also significant for hyper-kalemia and hypertension She was initiated on hemodialysisfor hyperkalemia volume overload and uremia Medica-tions prior to admission included occasional NSAID usemetformin and ACEI all of which were initially heldUrinalysis showed 100mgdL of protein with gt5 RBCHPFwithout casts on microscopy 24-hour urine was quantifiedfor protein and determined to be 3 grams ANA anti-DNAcomplement levels hepatitis and HIV serologies ASLO andanti-GBM were all negative ANCA serology yielded anti-myeloperoxidase (MPO) antibody level of lt1 and an elevatedanti-proteinase 3 (PR3) antibody level at 543 SPEPUPEPwas noncontributory On renal ultrasound kidneys were ofthe size of approximately 11 cm and 14 cm without evidenceof chronic renal disease atrophy or hydronephrosis Patientunderwent a kidney biopsy which showed mild chronicitysecondary to hypertension-related nephrosclerosis alongwith mild tubular atrophy and interstitial fibrosis (Figure 3)Acute histological findings on biopsy were significant forfocal segmental necrotizing (Figure 2) and diffuse crescen-tic glomerulonephritis (Figure 1) pauci-immune type with
Figure 1 Cellular crescent
Figure 2 Fibrinoid necrosis
Figure 3 Mild tubular atrophy
moderate-to-severe activity and mild chronicity In additiondiffuse acute tubular injury was seen with focal red bloodcell casts No changes secondary to diabetes were seen on thebiopsy Patient received induction therapy with cyclophos-phamide and intravenous corticosteroids and maintenanceimmunosuppression with azathioprine and oral prednisoneShe remained dialysis-dependent and developed untowardside effects to azathioprine therapy necessitating its discon-tinuation She is currently considered to have ESRD
4 Histopathological Classification
Renal biopsy is of critical importance in the diagnosis ofPICG and RPGN in general Even in patients with predomi-nant lung involvement kidney biopsy may be preferred as it
BioMed Research International 3
is associated with a higher diagnostic yield and lower proce-dural risk [9]The distinctive pathological features associatedwith PICG are necrosis of the capillary loops extracapillaryproliferation with crescent formation periglomerular andinterstitial infiltrates necrotizing arteritis and absence orpaucity of immune deposits [10]
A crescent is characterized by extracapillary proliferationwithin a glomerulus either partially or completely fillingup Bowmanrsquos space It is composed of proliferating parietalepithelial cells podocytes macrophages and fibroblastsCrescent formation is stimulated by the entry of fibrin andother plasma proteins from the capillary lumens followingthe rupture of the glomerular basement membrane (GBM)This is followed by the migration of T cells macrophagesand other inflammatory cells to the site of injury acceleratingcytokine release and tissue injury These ldquocellularrdquo crescentsmay finally evolve into fibrocellular or fibrous crescents withincreased extracellular matrix and collagen depositionThusthe presence of GBM rupture in a sclerosed glomerulusshould raise suspicion for previous crescentic glomerularinjury
The arrangement and the degree of crescent formationas well as the presence of sclerosis play a significant rolein determining the clinical course of PICG [11 12] Berdenet al recently presented a histopathologic classification sys-tem developed by the international working group of renalpathologists They performed a validation study on 100 renalbiopsies from patients with clinically and histopathologicallyconfirmed diagnosis of ANCA-associated glomerulonephri-tis The authors divided renal biopsies into four histologicalcategories as seen under light microscopy focal crescenticmixed and sclerotic based on the proportion of normalcellular crescentic and sclerotic glomeruli present Theiranalysis showed that this classification system has goodprognostic value in terms of renal outcome at 1 and 5 yearsRenal survival at 1 year was 93 for patients whose renalbiopsies were classified as focal at the time of diagnosis 84for patients whose biopsies were classified as crescentic 69for patients whose biopsies were classified as mixed and50 for patients whose biopsies were classified as scleroticRenal survival percentages at 5 years were 93 (focal) 76(crescentic) 61 (mixed) and 50 (sclerotic) In the scleroticcategory renal survival at 7 years was only 25 Severalvalidation studies out of Japan China Australia UnitedStates Netherlands and Turkey have further confirmedthat the outlined histopathological classification of ANCA-associated glomerulonephritis is of predictive value in termsof renal outcome [13ndash15] This was especially true for theoutlier categories of focal and sclerotic glomerular injuries
Although in PICG by definition there is a paucity ofimmune deposits on immunofluorescence microscopy andelectron microscopy a significant proportion of cases mayindeed show Ig deposits on histopathological examination[7 16 17] Neumann et al [17] showed that the presence of Igdeposits resulted in significantly more proteinuria and maybe associated with worse prognosis This can be explainedby the hypothesis that ANCA and immune complexes mayact synergistically to produce a more severe injury at theglomerulus It is also important to note that experimental
animal models have not convincingly ruled out the presenceof immune deposits in ANCA-associated glomerulonephritis[18 19] Rats preimmunized with human MPO-ANCA thatwere subsequently perfused with lysosomal extracts andH2O2 developed CGN and also showed IgG and C3 deposi-tion early in the course of the disease process Moreover thedegree of histologic injury was proportional to the amountof IgG immune deposits Interestingly the Ig deposits couldnot be detected later in the disease course suggesting that thepresence of immune complexes may be time dependent andnot seen by the time most patients are biopsied Finally thereare also reports of ANCA-associated glomerulonephritiscomplicating immune complex related diseases such as IgAnephropathy membranous glomerulonephritis and postin-fectious glomerulonephritis [7 20ndash22] Thus it is importantto test forANCAeven in caseswith immune deposits on renalhistology (type II lesions)
5 Pathophysiology
Despite the paucity of immune deposits PICG is a classicallyimmune mediated disease process Most of the in vitro invivo and clinical studies point to the involvement of ANCAin the pathogenesis of this disease [23ndash26] One example ofdirect evidence implicating the role of ANCA comes from acase report of neonatal microscopic polyangiitis secondaryto the transplacental transfer of MPO-ANCA [24] Thisfinding though interesting needs further substantiation infuture studies In addition several animal models of ANCA-associated renal disease have also been described Xiao et al[25] injected splenocytes from MPO-immunized mice intobothB andT cell depletedmice andwild typemiceThe recip-ient mice developed pauci-immune necrotizing crescenticglomerulonephritis and hemorrhagic pulmonary capillaritisalmost identical to the histopathology and phenotype ofhuman MPO-ANCA-associated vasculitis Transfer of IgGalone fromMPO-immunizedmice resulted in pauci-immunefocal necrotizing CGN in the recipient clearly demonstratingthe role of anti-MPO antibodies Although in vivo evidencesupporting the role of MPO-ANCA is well documented theresults have not yet been convincingly replicated for PR3-ANCAdisease in animalmodels [27] Some experts have thusquestioned the role of PR3 antibodies in the induction ofANCA disease and have instead proposed other mechanismssuch as T cell mediated inflammation
Anti-neutrophil cytoplasmic autoantibodies (ANCA) arespecific for proteins in the cytoplasm of neutrophils andmonocytes The major target antigens in patients with vas-culitis and glomerulonephritis are myeloperoxidase (MPO)and proteinase 3 (PR3) After binding with the target antigensPR3 or MPO ANCA results in the activation of neutrophilsand monocytes once the cells are primed with low dosesof cytokines such as tumor necrosis factor alpha (TNF-120572) interleukin-1 and interleukin-18 [26 28 29] There arepriming results in the surface expression of PR3 and MPOallowing interaction with ANCA Neutrophil activation ismediated by the engagement of both Fc120574 and Fab10158402 receptors[30 31] In particular the Fc120574 IIa and IIIb receptors areinvolved ANCA-mediated activation of neutrophils results
4 BioMed Research International
in the production of reactive oxygen species and the releaseof lytic enzymes such as elastase that are injurious to theendothelial cells [28 32 33] ANCAalso stimulates the releaseof neutrophil extracellular traps (NETs) that are composedof chromatin fibers and autoantigens including MPO andPR3 [34 35] NETs can damage endothelial cells and entireglomeruli andmay also be involved in propagating theANCAautoimmune response [34] In addition it has become clearthat the alternative pathway of complement activation playsa role in mediating tissue injury in PICG [36 37] Activatedneutrophils release various factors such as properdin whichactivate the alternate pathway with the generation of C3Properdin a molecule stored in neutrophilic granules isreleased when C5a primes the activation of neutrophils Thisoptimizes the interaction with ANCA and helps activate thealternate complement pathway All this sets off a cascade ofevents that augment neutrophil recruitment and activationresulting in the widespread necrotizing lesions seen in AAV[37] It is important to note that ANCA antigen specificityappears to be more closely associated with disease phenotypeand prognosis than with the clinical diagnosis of GPA orMPA [38 39] PR3-ANCA is associated with granulomatousinflammation more extensive extrarenal involvement and ahigher relapse rate In contrastMPO-ANCA ismore frequentin renal-limited disease displays more kidney scarring andcarries an overall worse renal prognosis
Antibodies other than ANCA have also been studiedin patients with PICG Kain et al demonstrated that anew subtype of ANCA lysosomal membrane protein 2(LAMP-2) antibodies are more prevalent than MPO andPR3 antibodies in patients with biopsy proven pauci-immunefocal necrotizing glomerulonephritis (FNGN) [40] Theyalso showed the development of characteristic lesions in thekidneys of rats after injecting them with LAMP-2 antibodiesand apoptosis of human endothelium in vitro by monoclonalantibody to human LAMP-2 (H4B4) A subsequent studyperformed by the same group not only showed the highprevalence of LAMP-2 antibodies in patients with PICGbut also demonstrated that they become undetectable withtreatment and frequently detectable during a relapse [41]which has obvious clinical implications However anotherstudy could not establish a relationship between LAMP-2antibodies and PICG [42] Some investigators have suggestedthat this difference in the results can be attributed to thepatient selection criteria and the assays used [43] Regardlessthese observations are intriguing and merit further studyFinally anti-plasminogen antibodies found in some patientswith AAV have been linked to increased susceptibility tothromboembolic events and greater severity of renal andsystemic disease [44 45]
Several environmental factors have now been associatedwith the pathogenesis of PICG Microbial factors play a rolein initiating the autoimmune response via their mimicryof host antigens [40] Previous studies have demonstratedthat patients with GPA are often chronic nasal carriers ofStaphylococcus aureus and that antimicrobial therapy maydecrease relapses [46 47] S aureus infection may alsoenhance the ability of the neutrophils to form NETs in smallvessel vasculitis [34] More recent evidence has identified
LAMP-2 epitope with 100 homology to fimbrial adhesin(FimH) seen in Gram-negative bacteria [48] It has beenhypothesized that immune response to FimH as seen inurosepsis triggers anti-LAMP-2 antibodies due to molecularmimicry
Another line of evidence implicating the role of microbialfactors comes from in vivo animal studies evaluating the roleof toll-like receptors (TLRs) in the pathogenesis of PICG[49 50] TLRs are a class of receptors present on leuko-cytes that are capable of recognizing infectious organismsand play an important role in generating innate immuneresponse TLR4 ligation has been found to play a role in AAVinduction It results in stimulation of T helper 17 (Th17) andTh1 responses via TLR2 and TLR9 activation respectively[49]
Several nonmicrobial environmental factors have alsobeen linked to PICG Silica is a known risk factor for ANCA[51 52] Certain drugs such as propylthiouracil hydralazineD-penicillamine cefotaxime minocycline anti-TNF agentsphenytoin and certain psychoactive agents are also known tocause ANCA-associated disease [53ndash56]
The role of autoimmune mechanisms in pauci-immuneCGN is also supported by another theory that states that theinitial immune response is generated against the complemen-tary PR3 (cPR3) peptide (generated by antisense DNA strandof PR3) or a mimic of cPR3 rather than against PR3 peptide[57ndash59] Patients with PR3-ANCA disease harbor not onlycirculating antibodies against sense PR3 peptides but also aseparate set of antibodies against antisense complementaryPR3 peptides (anti-cPR3) The immune response againstcPR3 results in the production of anti-cPR3 antibodies whichin turn generate anti-idiotypic antibodies that recognize notonly the idiotope on the anti-cPR3 antibodies but also theepitope on the sense PR3 peptide (original autoantigen)Interestingly a number of pathogens such as S aureus RossRiver virus and Entamoeba histolytica have sequences similarto cPR3 peptide thus making them capable of generatingthe autoimmune response [58] This provides another linkbetween infection and autoimmunity in PICG
The role of genetic factors in the pathogenesis of PICG isevident from the fact that not every individual with environ-mental risk factors develops the disease It is also observedthat AAV is more common in Caucasian population Theunderstanding of genetics in AAV has greatly improvedafter the publication of two genome-wide association studies(GWASs) [60 61]The goal of GWASs is to interrogate a largenumber of single-nucleotide polymorphisms (SNPs) thatcover a big portion of the human genome Interestingly thethree main AAV subtypes are associated with distinct HLAvariants that is granulomatosis with polyangiitis (Wegenerrsquos)GPA with HLA-DP1 microscopic polyangiitis (MPA) withHLA-DQ and eosinophilic GPA (Churg-Strauss) with HLA-DRB4 Patients with GPA are also known to have a higherproportion of neutrophils with increased surface expressionof PR3 [62] GWASs also revealed that polymorphic vari-ants of genes encoding PR3 and its main inhibitor alpha-1antitrypsin are highly associated with GPA especially withPR3-ANCA positivity regardless of the clinical diagnosisCandidate gene approach studies have shown associations
BioMed Research International 5
with other variants involved in AAV such as those belongingto the CTLA-4 and PTPN22 genes These results have not yetbeen replicated in larger studies [63ndash65]
Also it is important to discuss the role of T cell mediatedimmune response in PICG It is widely known that CD4+helper T cells with interferon-gamma secretion are involvedin granuloma formation Granulomas are seen mainly inPR3 AAV and not in MPO AAV TH17 cells play a majorrole in causing granulomatous inflammation and vascularinjury in PR3 AAV [66] Morgan et al have also showndiminished number and functional impairment of regulatoryT cells (Tregs) inGPA [67] Finally according to some studiespatients with ANCA-mediated vasculitis have impaired func-tioning of Tregs alongwith the presence of effector T cells thatare resistant to suppression by Tregs [68]
In addition to autoantibody production B cells also havethe ability to present antigens to T cells and may modulateT cell responses in small vessel vasculitis Regulatory B cells(Bregs) are a distinct B cell subset cells that regulate theaction of the T cell population by secreting IL-10 Wilde etal demonstrated that there is a reduction in the numberof Bregs in both active and quiescent AAV [69] The studyalso revealed a positive correlation between Breg and Treg inquiescent AAV and that Th1 cell suppression by Breg may beinadequate in active AAV
Recently the pathogenic mechanisms of tissue damagein GPA resulting in saddle nose deformity and orbitaldestruction have been further elucidated [38 70] Fibroblastslining bone and cartilage have been acknowledged to playthe role of activated effector cells of tissue destruction inGPA In the first in vivo model of GPA Kesel et al subcu-taneously coimplanted the biopsy specimens from patientswith activeGPAor sinusitis (controls) with healthy allogeneichuman nasal cartilage into immunodeficient mice [70] GPAimplants showed massive destruction of the coimplantedhuman cartilage whereas cartilage destruction was onlymarginal in control samples Further cartilage destructionwas mediated by human fibroblasts and could be controlledsimilar to GPA in humans with corticosteroids In additionin fibrotic lung disease NETs were shown to promote differ-entiation and function of fibroblasts indicating that NETs areinvolved not only in inflammation but also in the resultingfibrosis [38 71]
6 Clinical Manifestations and Natural History
Notwithstanding a slightly higher specificity ANCA is topauci-immune RPGN as anti-DNA is to systemic lupuserythematosus Microscopic polyangiitis (MPA) granulo-matosis with polyangiitis (GPA) eosinophilic granulomatosiswith polyangiitis (EGPA or Churg-Strauss syndrome) andrenal-limited pauci-immune crescentic GN (PICG) are allassociated with ANCA The term ldquopauci-immunerdquo RPGNencapsulates all of these conditions Generalized nonspecificmanifestations of systemic inflammatory disease such asfever malaise anorexia weight loss myalgia and arthralgiacan be seen in any of these diseases The clinical manifesta-tions of each entity vary based on the chronicity and sitesof involvement Patients without systemic involvement may
present later in the course of their disease Granulomatousinvolvement particularly of the upper respiratory tract is acharacteristic feature of GPA but not of MPA eosinophiliaasthma and atopy typically occur in EGPA In each of theseconditions patients can have pulmonary hemorrhage causedby hemorrhagic alveolar capillaritis which has treatmentand prognostic implications [2] As mentioned previouslythe renal failure seen in PICG usually presents clinicallyas RPGN It should be noted though that patients withGPA or MPA could also present with subacute or chronicnephritis In one study assessing the clinical characteristicsof pauci-immune crescentic GN a cohort of more than 300patients evaluated at renal biopsy had a mean age of 56 plusmn 20years (range 2 to 92 years) male-to-female ratio of 10 09mean serum creatinine concentration of 65 plusmn 40mgdL(range 08 to 221mgdL) and proteinuria of 19 plusmn 30 gday(range 01 to 18 gday) [2] Older age higher serum creatinineconcentration at presentation pulmonary hemorrhage anddialysis-dependent renal failure correlate with an overallpoor prognosis Respiratory tract disease and PR3-ANCAare predictors of higher relapse rates [2] Regardless of thecategory of ANCA disease though the best clinical predictorof renal outcome is the glomerular filtration rate (GFR)at the time of diagnosis [1] Interestingly in one of therecent studies the presence of ear nose and throat (ENT)involvement in AAV patients was found to be associatedwith lesser degree of interstitial fibrosis and tubular atrophyon kidney biopsy and better renal function These resultsindicate that there may be different phenotypes of AAVdefined by ENT involvement [71]
7 Conclusion
Despite significant advances in our understanding of theimmune system issues of incomplete efficacy treatmenttoxicity and infectious complications persist With targetedapproaches to immunosuppression andnewer biologic agentsmodulating B and T cell function the future holds promisein terms of greater treatment efficacy with an improved sideeffect profile We believe that future studies will highlight theintricacies of the clinical and pathological spectrum of PICGwhile proposing novel mechanisms for inducing and main-taining remission Based on current guidelines for patientsin complete remission and without extrarenal manifestationsfor at least 12 months renal transplant should not be delayedANCA positivity is not considered a contraindication fortransplantation However no prospective data are availableto assess the likelihood of recurrent ANCA vasculitis afterkidney transplantation In addition the impact of diseaseactivity or ANCA positivity at the time of transplantationon patient outcome is unclear Future studies must bedesigned to gather prospective data that helps answer thesequestions
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
6 BioMed Research International
References
[1] R J Glassock S G Adler H JWard et al ldquoPrimary glomerulardiseasesrdquo inTheKidney BM Brenner and F C Rector Eds pp1182ndash1279 Saunders Philadelphia Pa USA 4th edition 1991
[2] J Charles Jennette R J Falk and J G McGregor ldquoRenaland systemic valculitisrdquo in Comprehensive Clinical NephrologyElsevier 5th edition 2015
[3] S Watnick and T Dirkx ldquoKidney diseaserdquo in Current MedicalDiagnosis amp Treatment 2015 M A Papadakis S J McPhee andM W Rabow Eds McGraw-Hill New York NY USA 2014
[4] J C Jennette J L Olson M M Schwartz and F G SilvaldquoPauci-immune and ANCA-mediated crescentic glomeru-lonephritis and vasculitisrdquo in Heptinstallrsquos Pathology of theKidney vol 1 chapter 14 6th edition 2007
[5] P Seo and J H Stone ldquoThe antineutrophil cytoplasmicantibody-associated vasculitidesrdquo The American Journal ofMedicine vol 117 no 1 pp 39ndash50 2004
[6] U Eisenberger F Fakhouri P Vanhille et al ldquoANCA-negative pauci-immune renal vasculitis histology and out-comerdquo Nephrology Dialysis Transplantation vol 20 no 7 pp1392ndash1399 2005
[7] M Haas and J A Eustace ldquoImmune complex deposits inANCA-associated crescentic glomerulonephritis a study of 126casesrdquo Kidney International vol 65 no 6 pp 2145ndash2152 2004
[8] J B Levy T Hammad A Coulthart T Dougan and C DPusey ldquoClinical features and outcome of patients with bothANCA and anti-GBMantibodiesrdquoKidney International vol 66no 4 pp 1535ndash1540 2004
[9] N Kambham ldquoCrescentic glomerulonephritis an update onpauci-immune and anti-GBM diseasesrdquo Advances in AnatomicPathology vol 19 no 2 pp 111ndash124 2012
[10] F Ferrario A Vanzati and F Pagni ldquoPathology of ANCA-associated vasculitisrdquo Clinical and Experimental Nephrologyvol 17 no 5 pp 652ndash658 2013
[11] A E Berden F Ferrario E C Hagen et al ldquoHistopathologicclassification of ANCA-associated glomerulonephritisrdquo Journalof the American Society of Nephrology vol 21 no 10 pp 1628ndash1636 2010
[12] S L Ford K R Polkinghorne A Longano et al ldquoHistopatho-logic and clinical predictors of kidney outcomes in ANCA-associated vasculitisrdquo American Journal of Kidney Diseases vol63 no 2 pp 227ndash235 2014
[13] T Iwakiri S Fujimoto K Kitagawa et al ldquoValidation of anewly proposed histopathological classification in Japanesepatients with anti-neutrophil cytoplasmic antibody-associatedglomerulonephritisrdquo BMC Nephrology vol 14 article 125 2013
[14] E Nohr L Girard M James and H Benediktsson ldquoValidationof a histopathologic classification scheme for antineutrophilcytoplasmic antibody-associated glomerulonephritisrdquo HumanPathology vol 45 no 7 pp 1423ndash1429 2014
[15] D-Y Chang L-H Wu G Liu M Chen C G M Kallenbergand M-H Zhao ldquoRe-evaluation of the histopathologic classifi-cation of ANCA-associated glomerulonephritis a study of 121patients in a single centerrdquoNephrology Dialysis Transplantationvol 27 no 6 pp 2343ndash2349 2012
[16] M El-Ters U Muthyala M D Philipneri F A Hussein andK L Lentine ldquoImmune-complex deposits in lsquopauci-immunersquoglomerulonephritis a case report and brief review of recentliteraturerdquoArchives of Medical Science vol 6 no 4 pp 633ndash6372010
[17] I Neumann H Regele R Kain R Birck and F T MeislldquoGlomerular immune deposits are associated with increasedproteinuria in patients with ANCA-associated crescenticnephritisrdquo Nephrology Dialysis Transplantation vol 18 no 3pp 524ndash531 2003
[18] E Brouwer M G Huitema P A Klok et al ldquoAntimye-loperoxidase-associated proliferative glomerulonephritis ananimal modelrdquo Journal of Experimental Medicine vol 177 no4 pp 905ndash914 1993
[19] J J Yang J C Jennette and R J Falk ldquoImmune complexglomerulonephritis is induced in rats immunizedwith heterolo-gous myeloperoxidaserdquo Clinical and Experimental Immunologyvol 97 no 3 pp 466ndash473 1994
[20] M Haas J Jafri S M Bartosh S L Karp S G Adler and S MMeehan ldquoANCA-associated crescentic glomerulonephritis withmesangial IgA depositsrdquo American Journal of Kidney Diseasesvol 36 no 4 pp 709ndash718 2000
[21] M Haas ldquoIncidental healed postinfectious glomerulonephritisa study of 1012 renal biopsy specimens examined by electronmicroscopyrdquo Human Pathology vol 34 no 1 pp 3ndash10 2003
[22] R Jimbo Y Ubara T Tagami et al ldquoA pediatric occurrenceof crescentic glomerulonephritis associated with antineutrophilcytoplasmic antibodies and mesangial IgA depositsrdquo ClinicalNephrology vol 68 no 2 pp 104ndash108 2007
[23] J C Jennette ldquoRapidly progressive crescentic glomerulonephri-tisrdquo Kidney International vol 63 no 3 pp 1164ndash1177 2003
[24] P J Bansal andM C Tobin ldquoNeonatal microscopic polyangiitissecondary to transfer of maternal myeloperoxidase-antineutrophil cytoplasmic antibody resulting in neonatalpulmonary hemorrhage and renal involvementrdquo Annals ofAllergy Asthma and Immunology vol 93 no 4 pp 398ndash4012004
[25] H Xiao P Heeringa P Hu et al ldquoAntineutrophil cytoplasmicautoantibodies specific for myeloperoxidase cause glomeru-lonephritis and vasculitis in micerdquo Journal of Clinical Investiga-tion vol 110 no 7 pp 955ndash963 2002
[26] C G M Kallenberg ldquoPathogenesis of ANCA-associated vas-culitis an updaterdquo Clinical Reviews in Allergy and Immunologyvol 41 no 2 pp 224ndash231 2011
[27] H Pfister M Ollert L F Frohlich et al ldquoAntineutrophilcytoplasmic autoantibodies against the murine homolog ofproteinase 3 (Wegener autoantigen) are pathogenic in vivordquoBlood vol 104 no 5 pp 1411ndash1418 2004
[28] R J Falk R S Terrell L A Charles and J C Jennette ldquoAnti-neutrophil cytoplasmic autoantibodies induce neutrophils todegranulate and produce oxygen radicals in vitrordquo Proceedingsof the National Academy of Sciences of the United States ofAmerica vol 87 no 11 pp 4115ndash4119 1990
[29] L A Charles M L R Caldas R J Falk R S Terrell andJ C Jennette ldquoAntibodies against granule proteins activateneutrophils in vitrordquo Journal of Leukocyte Biology vol 50 no6 pp 539ndash546 1991
[30] A J Porges P B Redecha W T Kimberly E Csernok W LGross and R P Kimberly ldquoAnti-neutrophil cytoplasmic anti-bodies engage and activate human neutrophils via Fc gammaRIIardquoThe Journal of Immunology vol 153 no 3 pp 1271ndash12801994
[31] A H Mulder P Heeringa E Brouwer P C Limburg and CG Kallenberg ldquoActivation of granulocytes by anti-neutrophilcytoplasmic antibodies (ANCA) a Fc gamma RII-dependentprocessrdquoClinical amp Experimental Immunology vol 98 no 2 pp270ndash278 1994
BioMed Research International 7
[32] R Kettritz J C Jennette andR J Falk ldquoCrosslinking of ANCA-antigens stimulates superoxide release by human neutrophilsrdquoJournal of the American Society of Nephrology vol 8 no 3 pp386ndash394 1997
[33] B H Ewert J C Jennette and R J Falk ldquoAnti-myeloperoxidaseantibodies stimulate neutrophils to damage human endothelialcellsrdquo Kidney International vol 41 no 2 pp 375ndash383 1992
[34] K Kessenbrock M Krumbholz U Schonermarck et al ldquoNet-ting neutrophils in autoimmune small-vessel vasculitisrdquoNatureMedicine vol 15 no 6 pp 623ndash625 2009
[35] A K Gupta M B Joshi M Philippova et al ldquoActivatedendothelial cells induce neutrophil extracellular traps and aresusceptible to NETosis-mediated cell deathrdquo FEBS Letters vol584 no 14 pp 3193ndash3197 2010
[36] O O Rowaiye M Kusztal and M Klinger ldquoThe kidneys andANCA-associated vasculitis from pathogenesis to diagnosisrdquoClinical Kidney Journal vol 8 no 3 pp 343ndash350 2015
[37] H Xiao A Schreiber P Heeringa R J Falk and J C JennetteldquoAlternative complement pathway in the pathogenesis of dis-ease mediated by anti-neutrophil cytoplasmic autoantibodiesrdquoAmerican Journal of Pathology vol 170 no 1 pp 52ndash64 2007
[38] U Schonermarck E Csernok and W L Gross ldquoPathogenesisof anti-neutrophil cytoplasmic antibody-associated vasculitischallenges and solutions 2014rdquo Nephrology Dialysis Transplan-tation vol 30 supplement 1 pp i46ndashi52 2015
[39] C Franssen R Gans C Kallenberg C Hageluken and SHoorntje ldquoDisease spectrum of patients with antineutrophilcytoplasmic autoantibodies of defined specificity distinct dif-ferences between patients with anti-proteinase 3 and anti-myeloperoxidase autoantibodiesrdquo Journal of Internal Medicinevol 244 no 3 pp 209ndash216 1998
[40] R Kain M Exner R Brandes et al ldquoMolecular mimicry inpauci-immune focal necrotizing glomerulonephritisrdquo NatureMedicine vol 14 no 10 pp 1088ndash1096 2008
[41] R Kain H Tadema E F McKinney et al ldquoHigh prevalenceof autoantibodies to hLAMP-2 in anti-neutrophil cytoplasmicantibody-associated vasculitisrdquo Journal of the American Societyof Nephrology vol 23 no 3 pp 556ndash566 2012
[42] A J Roth M C Brown R N Smith et al ldquoAnti-LAMP-2antibodies are not prevalent in patients with antineutrophilcytoplasmic autoantibody glomerulonephritisrdquo Journal of theAmerican Society of Nephrology vol 23 no 3 pp 545ndash555 2012
[43] R Kain and A J Rees ldquoWhat is the evidence for antibodies toLAMP-2 in the pathogenesis of ANCA associated small vesselvasculitisrdquo Current Opinion in Rheumatology vol 25 no 1 pp26ndash34 2013
[44] J Hao C Wang S-J Gou M-H Zhao and M Chen ldquoTheassociation between anti-plasminogen antibodies and diseaseactivity in ANCA-associated vasculitisrdquo Rheumatology vol 53no 2 pp 300ndash306 2014
[45] A E Berden S L Nolan H L Morris et al ldquoAnti-plasminogenantibodies compromise fibrinolysis and associatewith renal his-tology in ANCA-associated vasculitisrdquo Journal of the AmericanSociety of Nephrology vol 21 no 12 pp 2169ndash2179 2010
[46] C A Stegeman J W Cohen Tervaert W J Sluiter W LManson P E De Jong and C G M Kallenberg ldquoAssociationof chronic nasal carriage of Staphylococcus aureus and higherrelapse rates in Wegener granulomatosisrdquo Annals of InternalMedicine vol 120 no 1 pp 12ndash17 1994
[47] K Zycinska K A Wardyn T M Zielonka R Krupa andW Lukas ldquoCo-trimoxazole and prevention of relapses of PR3-ANCA positive vasculitis with pulmonary involvementrdquo Euro-pean Journal ofMedical Research vol 14 supplement 4 pp 265ndash267 2009
[48] A D Salama and C D Pusey ldquoShining a LAMP on pauci-immune focal segmental glomerulonephritisrdquo Kidney Interna-tional vol 76 no 1 pp 15ndash17 2009
[49] MMVanTimmeren andPHeeringa ldquoPathogenesis ofANCA-associated vasculitis recent insights from animal modelsrdquoCurrent Opinion in Rheumatology vol 24 no 1 pp 8ndash14 2012
[50] A M Coughlan S J Freeley and M G Robson ldquoAnimalmodels of anti-neutrophil cytoplasmic antibody-associated vas-culitisrdquo Clinical and Experimental Immunology vol 169 no 3pp 229ndash237 2012
[51] S L Hogan K K Satterly M A Dooley P H Nachman JC Jennette and R J Falk ldquoSilica exposure in anti-neutrophilcytoplasmic autoantibody-associated glomerulonephritis andlupus nephritisrdquo Journal of the American Society of Nephrologyvol 12 no 1 pp 134ndash142 2001
[52] Z Rihova D Maixnerova E Jancova et al ldquoSilica andasbestos exposure in ANCA-associated vasculitis with pul-monary involvementrdquo Renal Failure vol 27 no 5 pp 605ndash6082005
[53] T Kanda H Tanio CWu H Nishihara F Nogaki and T OnoldquoChurg-Strauss syndrome with severe granulomatous angiitisand crescentic glomerulonephritis which developed duringtherapy with a leukotriene receptor antagonistrdquo Clinical andExperimental Nephrology vol 14 no 6 pp 602ndash607 2010
[54] M Suneja S Baiswar and S A Vogelgesang ldquoHydralazineassociated pauci-immune glomerulonephritisrdquo Journal of Clin-ical Rheumatology vol 20 no 2 pp 99ndash102 2014
[55] S Morita Y Ueda and K Eguchi ldquoAnti-thyroid drug-inducedANCA-associated vasculitis a case report and review of theliteraturerdquo Endocrine Journal vol 47 no 4 pp 467ndash470 2000
[56] H K Choi P A Merkel A M Walker and J L NilesldquoDrug-associated antineutrophil cytoplasmic antibody-positivevasculitis prevalence among patients with high titers ofantimyeloperoxidase antibodiesrdquo Arthritis and Rheumatismvol 43 no 2 pp 405ndash413 2000
[57] J C Jennette R J Falk and A H Gasim ldquoPathogenesis ofantineutrophil cytoplasmic autoantibody vasculitisrdquo CurrentOpinion in Nephrology andHypertension vol 20 no 3 pp 263ndash270 2011
[58] W F Pendergraft III G A Preston R R Shah et al ldquoAutoim-munity is triggered by cPR-3(105ndash201) a protein complemen-tary to human autoantigen proteinase-3rdquo Nature Medicine vol10 no 1 pp 72ndash79 2004
[59] P Hewins F Belmonte J C Jennette R J Falk and G APreston ldquoLongitudinal studies of patients with ANCA vasculi-tis demonstrate concurrent reactivity to complementary PR3protein segments cPR3m and cPR3C and with no reactivity tocPR3Nrdquo Autoimmunity vol 44 no 2 pp 98ndash106 2011
[60] P A Lyons T F Rayner S Trivedi et al ldquoGenetically distinctsubsets within ANCA-associated vasculitisrdquo The New EnglandJournal of Medicine vol 367 no 3 pp 214ndash223 2012
[61] G Xie D Roshandel R Sherva et al ldquoAssociation of granulo-matosis with polyangiitis (Wegenerrsquos) with HLA-DPB1lowast04 andSEMA6A gene variants evidence from genome-wide analysisrdquoArthritis amp Rheumatism vol 65 no 9 pp 2457ndash2468 2013
[62] V Witko-Sarsat P Lesavre S Lopez et al ldquoA large subset ofneutrophils expressing membrane proteinase 3 is a risk factor
8 BioMed Research International
for vasculitis and rheumatoid arthritisrdquo Journal of the AmericanSociety of Nephrology vol 10 no 6 pp 1224ndash1233 1999
[63] P Jagiello P Aries L Arning et al ldquoThe PTPN22 620W alleleis a risk factor for Wegenerrsquos granulomatosisrdquo Arthritis andRheumatism vol 52 no 12 pp 4039ndash4043 2005
[64] D Martorana F Maritati G Malerba et al ldquoPTPN22 R620Wpolymorphism in the ANCA-associated vasculitidesrdquo Rheuma-tology vol 51 no 5 Article ID ker446 pp 805ndash812 2012
[65] R Giscombe X Wang D Huang and A K Lefvert ldquoCodingsequence 1 and promoter single nucleotide polymorphismsin the CTLA-4 gene in Wegenerrsquos granulomatosisrdquo Journal ofRheumatology vol 29 no 5 pp 950ndash953 2002
[66] P Lamprecht S Wieczorek J T Epplen P Ambrosch and CG M Kallenberg ldquoGranuloma formation in ANCA-associatedvasculitidesrdquo APMIS vol 117 supplement s127 no 127 pp 32ndash36 2009
[67] M D Morgan C J Day K P Piper et al ldquoPatients withWegenerrsquos granulomatosis demonstrate a relative deficiency andfunctional impairment of T-regulatory cellsrdquo Immunology vol130 no 1 pp 64ndash73 2010
[68] M E Free D O Bunch J A McGregor et al ldquoPatients withantineutrophil cytoplasmic antibody-associated vasculitis havedefective Treg cell function exacerbated by the presence ofa suppression-resistant effector cell populationrdquo Arthritis andRheumatism vol 65 no 7 pp 1922ndash1933 2013
[69] B Wilde M Thewissen J Damoiseaux et al ldquoRegulatory Bcells in ANCA-associated vasculitisrdquo Annals of the RheumaticDiseases vol 72 no 8 pp 1416ndash1419 2013
[70] N Kesel D Khler L Herich et al ldquoCartilage destruction ingranulomatosis with polyangiitis (Wegenerrsquos granulomatosis)is mediated by human fibroblasts after transplantation intoimmunodeficientmicerdquoTheAmerican Journal of Pathology vol180 no 5 pp 2144ndash2155 2012
[71] C Rahmattulla R A de Lind van Wijngaarden A E Berdenet al ldquoRenal function and ear nose throat involvement in anti-neutrophil cytoplasmic antibody-associated vasculitis prospec-tive data from the European Vasculitis Society clinical trialsrdquoRheumatology vol 54 no 5 pp 899ndash907 2015
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
2 BioMed Research International
Despite efforts to simplify the classification system theterm ldquopauci-immune glomerulonephritisrdquo represents intri-cate and overlapping ldquospectrumrdquo of disease processes Weknow that about 10of the cases in the pathologic continuumof PICG are ANCA negative despite similar clinical featuresand renal biopsy findings as compared to ANCA-positivecases [1] In addition although pauci-immune necrotizingGN typically occurs in association with involvement of otherorgans in both GPA and MPA some patients present with arenal-limited ANCA-positive vasculitis Up to 80 of thesepatients have MPO-ANCA positivity while the remaininghave anti-PR3-ANCA antibodies [5] The patient presentedin this review has anti-PR3-ANCA which upon remissioncarries a higher relapse rate and an overall worse prognosisRenal-limited vasculitis is considered to be part of thespectrum of GPA and MPA because the histopathologicfindings of the two conditions are often indistinguishable[6] Clinically patients with renal-limited vasculitis are morelikely to have glomerulosclerosis on renal biopsy than thosewith GPA or MPA since patients without extrarenal mani-festations probably present later in the course of their disease[6] Adding to the complexity of the clinical phenotypesome patients have small dispersed immune deposits inthe mesangium and glomerular capillary wall when assessedby electron microscopy This in the proper clinical set-ting and positive ANCA antibodies is still classified asldquopauci-immunerdquo glomerulonephritis [7] Lastly the entity ofldquodouble-antibodyrdquo positive disease must also be mentionedas it includes patients with features of both ANCA-positiveRPGN and anti-GBM disease [8]
3 Case
63-year-old Caucasian female with past medical history ofdiabetes mellitus type II for 7 years (without retinopathy orneuropathy) hypertension and hypothyroidism presentedwith acute kidney injury in March of 2015 Patient wasedematous on exam and had a peak serum creatinine of72mgdL Initial findings were also significant for hyper-kalemia and hypertension She was initiated on hemodialysisfor hyperkalemia volume overload and uremia Medica-tions prior to admission included occasional NSAID usemetformin and ACEI all of which were initially heldUrinalysis showed 100mgdL of protein with gt5 RBCHPFwithout casts on microscopy 24-hour urine was quantifiedfor protein and determined to be 3 grams ANA anti-DNAcomplement levels hepatitis and HIV serologies ASLO andanti-GBM were all negative ANCA serology yielded anti-myeloperoxidase (MPO) antibody level of lt1 and an elevatedanti-proteinase 3 (PR3) antibody level at 543 SPEPUPEPwas noncontributory On renal ultrasound kidneys were ofthe size of approximately 11 cm and 14 cm without evidenceof chronic renal disease atrophy or hydronephrosis Patientunderwent a kidney biopsy which showed mild chronicitysecondary to hypertension-related nephrosclerosis alongwith mild tubular atrophy and interstitial fibrosis (Figure 3)Acute histological findings on biopsy were significant forfocal segmental necrotizing (Figure 2) and diffuse crescen-tic glomerulonephritis (Figure 1) pauci-immune type with
Figure 1 Cellular crescent
Figure 2 Fibrinoid necrosis
Figure 3 Mild tubular atrophy
moderate-to-severe activity and mild chronicity In additiondiffuse acute tubular injury was seen with focal red bloodcell casts No changes secondary to diabetes were seen on thebiopsy Patient received induction therapy with cyclophos-phamide and intravenous corticosteroids and maintenanceimmunosuppression with azathioprine and oral prednisoneShe remained dialysis-dependent and developed untowardside effects to azathioprine therapy necessitating its discon-tinuation She is currently considered to have ESRD
4 Histopathological Classification
Renal biopsy is of critical importance in the diagnosis ofPICG and RPGN in general Even in patients with predomi-nant lung involvement kidney biopsy may be preferred as it
BioMed Research International 3
is associated with a higher diagnostic yield and lower proce-dural risk [9]The distinctive pathological features associatedwith PICG are necrosis of the capillary loops extracapillaryproliferation with crescent formation periglomerular andinterstitial infiltrates necrotizing arteritis and absence orpaucity of immune deposits [10]
A crescent is characterized by extracapillary proliferationwithin a glomerulus either partially or completely fillingup Bowmanrsquos space It is composed of proliferating parietalepithelial cells podocytes macrophages and fibroblastsCrescent formation is stimulated by the entry of fibrin andother plasma proteins from the capillary lumens followingthe rupture of the glomerular basement membrane (GBM)This is followed by the migration of T cells macrophagesand other inflammatory cells to the site of injury acceleratingcytokine release and tissue injury These ldquocellularrdquo crescentsmay finally evolve into fibrocellular or fibrous crescents withincreased extracellular matrix and collagen depositionThusthe presence of GBM rupture in a sclerosed glomerulusshould raise suspicion for previous crescentic glomerularinjury
The arrangement and the degree of crescent formationas well as the presence of sclerosis play a significant rolein determining the clinical course of PICG [11 12] Berdenet al recently presented a histopathologic classification sys-tem developed by the international working group of renalpathologists They performed a validation study on 100 renalbiopsies from patients with clinically and histopathologicallyconfirmed diagnosis of ANCA-associated glomerulonephri-tis The authors divided renal biopsies into four histologicalcategories as seen under light microscopy focal crescenticmixed and sclerotic based on the proportion of normalcellular crescentic and sclerotic glomeruli present Theiranalysis showed that this classification system has goodprognostic value in terms of renal outcome at 1 and 5 yearsRenal survival at 1 year was 93 for patients whose renalbiopsies were classified as focal at the time of diagnosis 84for patients whose biopsies were classified as crescentic 69for patients whose biopsies were classified as mixed and50 for patients whose biopsies were classified as scleroticRenal survival percentages at 5 years were 93 (focal) 76(crescentic) 61 (mixed) and 50 (sclerotic) In the scleroticcategory renal survival at 7 years was only 25 Severalvalidation studies out of Japan China Australia UnitedStates Netherlands and Turkey have further confirmedthat the outlined histopathological classification of ANCA-associated glomerulonephritis is of predictive value in termsof renal outcome [13ndash15] This was especially true for theoutlier categories of focal and sclerotic glomerular injuries
Although in PICG by definition there is a paucity ofimmune deposits on immunofluorescence microscopy andelectron microscopy a significant proportion of cases mayindeed show Ig deposits on histopathological examination[7 16 17] Neumann et al [17] showed that the presence of Igdeposits resulted in significantly more proteinuria and maybe associated with worse prognosis This can be explainedby the hypothesis that ANCA and immune complexes mayact synergistically to produce a more severe injury at theglomerulus It is also important to note that experimental
animal models have not convincingly ruled out the presenceof immune deposits in ANCA-associated glomerulonephritis[18 19] Rats preimmunized with human MPO-ANCA thatwere subsequently perfused with lysosomal extracts andH2O2 developed CGN and also showed IgG and C3 deposi-tion early in the course of the disease process Moreover thedegree of histologic injury was proportional to the amountof IgG immune deposits Interestingly the Ig deposits couldnot be detected later in the disease course suggesting that thepresence of immune complexes may be time dependent andnot seen by the time most patients are biopsied Finally thereare also reports of ANCA-associated glomerulonephritiscomplicating immune complex related diseases such as IgAnephropathy membranous glomerulonephritis and postin-fectious glomerulonephritis [7 20ndash22] Thus it is importantto test forANCAeven in caseswith immune deposits on renalhistology (type II lesions)
5 Pathophysiology
Despite the paucity of immune deposits PICG is a classicallyimmune mediated disease process Most of the in vitro invivo and clinical studies point to the involvement of ANCAin the pathogenesis of this disease [23ndash26] One example ofdirect evidence implicating the role of ANCA comes from acase report of neonatal microscopic polyangiitis secondaryto the transplacental transfer of MPO-ANCA [24] Thisfinding though interesting needs further substantiation infuture studies In addition several animal models of ANCA-associated renal disease have also been described Xiao et al[25] injected splenocytes from MPO-immunized mice intobothB andT cell depletedmice andwild typemiceThe recip-ient mice developed pauci-immune necrotizing crescenticglomerulonephritis and hemorrhagic pulmonary capillaritisalmost identical to the histopathology and phenotype ofhuman MPO-ANCA-associated vasculitis Transfer of IgGalone fromMPO-immunizedmice resulted in pauci-immunefocal necrotizing CGN in the recipient clearly demonstratingthe role of anti-MPO antibodies Although in vivo evidencesupporting the role of MPO-ANCA is well documented theresults have not yet been convincingly replicated for PR3-ANCAdisease in animalmodels [27] Some experts have thusquestioned the role of PR3 antibodies in the induction ofANCA disease and have instead proposed other mechanismssuch as T cell mediated inflammation
Anti-neutrophil cytoplasmic autoantibodies (ANCA) arespecific for proteins in the cytoplasm of neutrophils andmonocytes The major target antigens in patients with vas-culitis and glomerulonephritis are myeloperoxidase (MPO)and proteinase 3 (PR3) After binding with the target antigensPR3 or MPO ANCA results in the activation of neutrophilsand monocytes once the cells are primed with low dosesof cytokines such as tumor necrosis factor alpha (TNF-120572) interleukin-1 and interleukin-18 [26 28 29] There arepriming results in the surface expression of PR3 and MPOallowing interaction with ANCA Neutrophil activation ismediated by the engagement of both Fc120574 and Fab10158402 receptors[30 31] In particular the Fc120574 IIa and IIIb receptors areinvolved ANCA-mediated activation of neutrophils results
4 BioMed Research International
in the production of reactive oxygen species and the releaseof lytic enzymes such as elastase that are injurious to theendothelial cells [28 32 33] ANCAalso stimulates the releaseof neutrophil extracellular traps (NETs) that are composedof chromatin fibers and autoantigens including MPO andPR3 [34 35] NETs can damage endothelial cells and entireglomeruli andmay also be involved in propagating theANCAautoimmune response [34] In addition it has become clearthat the alternative pathway of complement activation playsa role in mediating tissue injury in PICG [36 37] Activatedneutrophils release various factors such as properdin whichactivate the alternate pathway with the generation of C3Properdin a molecule stored in neutrophilic granules isreleased when C5a primes the activation of neutrophils Thisoptimizes the interaction with ANCA and helps activate thealternate complement pathway All this sets off a cascade ofevents that augment neutrophil recruitment and activationresulting in the widespread necrotizing lesions seen in AAV[37] It is important to note that ANCA antigen specificityappears to be more closely associated with disease phenotypeand prognosis than with the clinical diagnosis of GPA orMPA [38 39] PR3-ANCA is associated with granulomatousinflammation more extensive extrarenal involvement and ahigher relapse rate In contrastMPO-ANCA ismore frequentin renal-limited disease displays more kidney scarring andcarries an overall worse renal prognosis
Antibodies other than ANCA have also been studiedin patients with PICG Kain et al demonstrated that anew subtype of ANCA lysosomal membrane protein 2(LAMP-2) antibodies are more prevalent than MPO andPR3 antibodies in patients with biopsy proven pauci-immunefocal necrotizing glomerulonephritis (FNGN) [40] Theyalso showed the development of characteristic lesions in thekidneys of rats after injecting them with LAMP-2 antibodiesand apoptosis of human endothelium in vitro by monoclonalantibody to human LAMP-2 (H4B4) A subsequent studyperformed by the same group not only showed the highprevalence of LAMP-2 antibodies in patients with PICGbut also demonstrated that they become undetectable withtreatment and frequently detectable during a relapse [41]which has obvious clinical implications However anotherstudy could not establish a relationship between LAMP-2antibodies and PICG [42] Some investigators have suggestedthat this difference in the results can be attributed to thepatient selection criteria and the assays used [43] Regardlessthese observations are intriguing and merit further studyFinally anti-plasminogen antibodies found in some patientswith AAV have been linked to increased susceptibility tothromboembolic events and greater severity of renal andsystemic disease [44 45]
Several environmental factors have now been associatedwith the pathogenesis of PICG Microbial factors play a rolein initiating the autoimmune response via their mimicryof host antigens [40] Previous studies have demonstratedthat patients with GPA are often chronic nasal carriers ofStaphylococcus aureus and that antimicrobial therapy maydecrease relapses [46 47] S aureus infection may alsoenhance the ability of the neutrophils to form NETs in smallvessel vasculitis [34] More recent evidence has identified
LAMP-2 epitope with 100 homology to fimbrial adhesin(FimH) seen in Gram-negative bacteria [48] It has beenhypothesized that immune response to FimH as seen inurosepsis triggers anti-LAMP-2 antibodies due to molecularmimicry
Another line of evidence implicating the role of microbialfactors comes from in vivo animal studies evaluating the roleof toll-like receptors (TLRs) in the pathogenesis of PICG[49 50] TLRs are a class of receptors present on leuko-cytes that are capable of recognizing infectious organismsand play an important role in generating innate immuneresponse TLR4 ligation has been found to play a role in AAVinduction It results in stimulation of T helper 17 (Th17) andTh1 responses via TLR2 and TLR9 activation respectively[49]
Several nonmicrobial environmental factors have alsobeen linked to PICG Silica is a known risk factor for ANCA[51 52] Certain drugs such as propylthiouracil hydralazineD-penicillamine cefotaxime minocycline anti-TNF agentsphenytoin and certain psychoactive agents are also known tocause ANCA-associated disease [53ndash56]
The role of autoimmune mechanisms in pauci-immuneCGN is also supported by another theory that states that theinitial immune response is generated against the complemen-tary PR3 (cPR3) peptide (generated by antisense DNA strandof PR3) or a mimic of cPR3 rather than against PR3 peptide[57ndash59] Patients with PR3-ANCA disease harbor not onlycirculating antibodies against sense PR3 peptides but also aseparate set of antibodies against antisense complementaryPR3 peptides (anti-cPR3) The immune response againstcPR3 results in the production of anti-cPR3 antibodies whichin turn generate anti-idiotypic antibodies that recognize notonly the idiotope on the anti-cPR3 antibodies but also theepitope on the sense PR3 peptide (original autoantigen)Interestingly a number of pathogens such as S aureus RossRiver virus and Entamoeba histolytica have sequences similarto cPR3 peptide thus making them capable of generatingthe autoimmune response [58] This provides another linkbetween infection and autoimmunity in PICG
The role of genetic factors in the pathogenesis of PICG isevident from the fact that not every individual with environ-mental risk factors develops the disease It is also observedthat AAV is more common in Caucasian population Theunderstanding of genetics in AAV has greatly improvedafter the publication of two genome-wide association studies(GWASs) [60 61]The goal of GWASs is to interrogate a largenumber of single-nucleotide polymorphisms (SNPs) thatcover a big portion of the human genome Interestingly thethree main AAV subtypes are associated with distinct HLAvariants that is granulomatosis with polyangiitis (Wegenerrsquos)GPA with HLA-DP1 microscopic polyangiitis (MPA) withHLA-DQ and eosinophilic GPA (Churg-Strauss) with HLA-DRB4 Patients with GPA are also known to have a higherproportion of neutrophils with increased surface expressionof PR3 [62] GWASs also revealed that polymorphic vari-ants of genes encoding PR3 and its main inhibitor alpha-1antitrypsin are highly associated with GPA especially withPR3-ANCA positivity regardless of the clinical diagnosisCandidate gene approach studies have shown associations
BioMed Research International 5
with other variants involved in AAV such as those belongingto the CTLA-4 and PTPN22 genes These results have not yetbeen replicated in larger studies [63ndash65]
Also it is important to discuss the role of T cell mediatedimmune response in PICG It is widely known that CD4+helper T cells with interferon-gamma secretion are involvedin granuloma formation Granulomas are seen mainly inPR3 AAV and not in MPO AAV TH17 cells play a majorrole in causing granulomatous inflammation and vascularinjury in PR3 AAV [66] Morgan et al have also showndiminished number and functional impairment of regulatoryT cells (Tregs) inGPA [67] Finally according to some studiespatients with ANCA-mediated vasculitis have impaired func-tioning of Tregs alongwith the presence of effector T cells thatare resistant to suppression by Tregs [68]
In addition to autoantibody production B cells also havethe ability to present antigens to T cells and may modulateT cell responses in small vessel vasculitis Regulatory B cells(Bregs) are a distinct B cell subset cells that regulate theaction of the T cell population by secreting IL-10 Wilde etal demonstrated that there is a reduction in the numberof Bregs in both active and quiescent AAV [69] The studyalso revealed a positive correlation between Breg and Treg inquiescent AAV and that Th1 cell suppression by Breg may beinadequate in active AAV
Recently the pathogenic mechanisms of tissue damagein GPA resulting in saddle nose deformity and orbitaldestruction have been further elucidated [38 70] Fibroblastslining bone and cartilage have been acknowledged to playthe role of activated effector cells of tissue destruction inGPA In the first in vivo model of GPA Kesel et al subcu-taneously coimplanted the biopsy specimens from patientswith activeGPAor sinusitis (controls) with healthy allogeneichuman nasal cartilage into immunodeficient mice [70] GPAimplants showed massive destruction of the coimplantedhuman cartilage whereas cartilage destruction was onlymarginal in control samples Further cartilage destructionwas mediated by human fibroblasts and could be controlledsimilar to GPA in humans with corticosteroids In additionin fibrotic lung disease NETs were shown to promote differ-entiation and function of fibroblasts indicating that NETs areinvolved not only in inflammation but also in the resultingfibrosis [38 71]
6 Clinical Manifestations and Natural History
Notwithstanding a slightly higher specificity ANCA is topauci-immune RPGN as anti-DNA is to systemic lupuserythematosus Microscopic polyangiitis (MPA) granulo-matosis with polyangiitis (GPA) eosinophilic granulomatosiswith polyangiitis (EGPA or Churg-Strauss syndrome) andrenal-limited pauci-immune crescentic GN (PICG) are allassociated with ANCA The term ldquopauci-immunerdquo RPGNencapsulates all of these conditions Generalized nonspecificmanifestations of systemic inflammatory disease such asfever malaise anorexia weight loss myalgia and arthralgiacan be seen in any of these diseases The clinical manifesta-tions of each entity vary based on the chronicity and sitesof involvement Patients without systemic involvement may
present later in the course of their disease Granulomatousinvolvement particularly of the upper respiratory tract is acharacteristic feature of GPA but not of MPA eosinophiliaasthma and atopy typically occur in EGPA In each of theseconditions patients can have pulmonary hemorrhage causedby hemorrhagic alveolar capillaritis which has treatmentand prognostic implications [2] As mentioned previouslythe renal failure seen in PICG usually presents clinicallyas RPGN It should be noted though that patients withGPA or MPA could also present with subacute or chronicnephritis In one study assessing the clinical characteristicsof pauci-immune crescentic GN a cohort of more than 300patients evaluated at renal biopsy had a mean age of 56 plusmn 20years (range 2 to 92 years) male-to-female ratio of 10 09mean serum creatinine concentration of 65 plusmn 40mgdL(range 08 to 221mgdL) and proteinuria of 19 plusmn 30 gday(range 01 to 18 gday) [2] Older age higher serum creatinineconcentration at presentation pulmonary hemorrhage anddialysis-dependent renal failure correlate with an overallpoor prognosis Respiratory tract disease and PR3-ANCAare predictors of higher relapse rates [2] Regardless of thecategory of ANCA disease though the best clinical predictorof renal outcome is the glomerular filtration rate (GFR)at the time of diagnosis [1] Interestingly in one of therecent studies the presence of ear nose and throat (ENT)involvement in AAV patients was found to be associatedwith lesser degree of interstitial fibrosis and tubular atrophyon kidney biopsy and better renal function These resultsindicate that there may be different phenotypes of AAVdefined by ENT involvement [71]
7 Conclusion
Despite significant advances in our understanding of theimmune system issues of incomplete efficacy treatmenttoxicity and infectious complications persist With targetedapproaches to immunosuppression andnewer biologic agentsmodulating B and T cell function the future holds promisein terms of greater treatment efficacy with an improved sideeffect profile We believe that future studies will highlight theintricacies of the clinical and pathological spectrum of PICGwhile proposing novel mechanisms for inducing and main-taining remission Based on current guidelines for patientsin complete remission and without extrarenal manifestationsfor at least 12 months renal transplant should not be delayedANCA positivity is not considered a contraindication fortransplantation However no prospective data are availableto assess the likelihood of recurrent ANCA vasculitis afterkidney transplantation In addition the impact of diseaseactivity or ANCA positivity at the time of transplantationon patient outcome is unclear Future studies must bedesigned to gather prospective data that helps answer thesequestions
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
6 BioMed Research International
References
[1] R J Glassock S G Adler H JWard et al ldquoPrimary glomerulardiseasesrdquo inTheKidney BM Brenner and F C Rector Eds pp1182ndash1279 Saunders Philadelphia Pa USA 4th edition 1991
[2] J Charles Jennette R J Falk and J G McGregor ldquoRenaland systemic valculitisrdquo in Comprehensive Clinical NephrologyElsevier 5th edition 2015
[3] S Watnick and T Dirkx ldquoKidney diseaserdquo in Current MedicalDiagnosis amp Treatment 2015 M A Papadakis S J McPhee andM W Rabow Eds McGraw-Hill New York NY USA 2014
[4] J C Jennette J L Olson M M Schwartz and F G SilvaldquoPauci-immune and ANCA-mediated crescentic glomeru-lonephritis and vasculitisrdquo in Heptinstallrsquos Pathology of theKidney vol 1 chapter 14 6th edition 2007
[5] P Seo and J H Stone ldquoThe antineutrophil cytoplasmicantibody-associated vasculitidesrdquo The American Journal ofMedicine vol 117 no 1 pp 39ndash50 2004
[6] U Eisenberger F Fakhouri P Vanhille et al ldquoANCA-negative pauci-immune renal vasculitis histology and out-comerdquo Nephrology Dialysis Transplantation vol 20 no 7 pp1392ndash1399 2005
[7] M Haas and J A Eustace ldquoImmune complex deposits inANCA-associated crescentic glomerulonephritis a study of 126casesrdquo Kidney International vol 65 no 6 pp 2145ndash2152 2004
[8] J B Levy T Hammad A Coulthart T Dougan and C DPusey ldquoClinical features and outcome of patients with bothANCA and anti-GBMantibodiesrdquoKidney International vol 66no 4 pp 1535ndash1540 2004
[9] N Kambham ldquoCrescentic glomerulonephritis an update onpauci-immune and anti-GBM diseasesrdquo Advances in AnatomicPathology vol 19 no 2 pp 111ndash124 2012
[10] F Ferrario A Vanzati and F Pagni ldquoPathology of ANCA-associated vasculitisrdquo Clinical and Experimental Nephrologyvol 17 no 5 pp 652ndash658 2013
[11] A E Berden F Ferrario E C Hagen et al ldquoHistopathologicclassification of ANCA-associated glomerulonephritisrdquo Journalof the American Society of Nephrology vol 21 no 10 pp 1628ndash1636 2010
[12] S L Ford K R Polkinghorne A Longano et al ldquoHistopatho-logic and clinical predictors of kidney outcomes in ANCA-associated vasculitisrdquo American Journal of Kidney Diseases vol63 no 2 pp 227ndash235 2014
[13] T Iwakiri S Fujimoto K Kitagawa et al ldquoValidation of anewly proposed histopathological classification in Japanesepatients with anti-neutrophil cytoplasmic antibody-associatedglomerulonephritisrdquo BMC Nephrology vol 14 article 125 2013
[14] E Nohr L Girard M James and H Benediktsson ldquoValidationof a histopathologic classification scheme for antineutrophilcytoplasmic antibody-associated glomerulonephritisrdquo HumanPathology vol 45 no 7 pp 1423ndash1429 2014
[15] D-Y Chang L-H Wu G Liu M Chen C G M Kallenbergand M-H Zhao ldquoRe-evaluation of the histopathologic classifi-cation of ANCA-associated glomerulonephritis a study of 121patients in a single centerrdquoNephrology Dialysis Transplantationvol 27 no 6 pp 2343ndash2349 2012
[16] M El-Ters U Muthyala M D Philipneri F A Hussein andK L Lentine ldquoImmune-complex deposits in lsquopauci-immunersquoglomerulonephritis a case report and brief review of recentliteraturerdquoArchives of Medical Science vol 6 no 4 pp 633ndash6372010
[17] I Neumann H Regele R Kain R Birck and F T MeislldquoGlomerular immune deposits are associated with increasedproteinuria in patients with ANCA-associated crescenticnephritisrdquo Nephrology Dialysis Transplantation vol 18 no 3pp 524ndash531 2003
[18] E Brouwer M G Huitema P A Klok et al ldquoAntimye-loperoxidase-associated proliferative glomerulonephritis ananimal modelrdquo Journal of Experimental Medicine vol 177 no4 pp 905ndash914 1993
[19] J J Yang J C Jennette and R J Falk ldquoImmune complexglomerulonephritis is induced in rats immunizedwith heterolo-gous myeloperoxidaserdquo Clinical and Experimental Immunologyvol 97 no 3 pp 466ndash473 1994
[20] M Haas J Jafri S M Bartosh S L Karp S G Adler and S MMeehan ldquoANCA-associated crescentic glomerulonephritis withmesangial IgA depositsrdquo American Journal of Kidney Diseasesvol 36 no 4 pp 709ndash718 2000
[21] M Haas ldquoIncidental healed postinfectious glomerulonephritisa study of 1012 renal biopsy specimens examined by electronmicroscopyrdquo Human Pathology vol 34 no 1 pp 3ndash10 2003
[22] R Jimbo Y Ubara T Tagami et al ldquoA pediatric occurrenceof crescentic glomerulonephritis associated with antineutrophilcytoplasmic antibodies and mesangial IgA depositsrdquo ClinicalNephrology vol 68 no 2 pp 104ndash108 2007
[23] J C Jennette ldquoRapidly progressive crescentic glomerulonephri-tisrdquo Kidney International vol 63 no 3 pp 1164ndash1177 2003
[24] P J Bansal andM C Tobin ldquoNeonatal microscopic polyangiitissecondary to transfer of maternal myeloperoxidase-antineutrophil cytoplasmic antibody resulting in neonatalpulmonary hemorrhage and renal involvementrdquo Annals ofAllergy Asthma and Immunology vol 93 no 4 pp 398ndash4012004
[25] H Xiao P Heeringa P Hu et al ldquoAntineutrophil cytoplasmicautoantibodies specific for myeloperoxidase cause glomeru-lonephritis and vasculitis in micerdquo Journal of Clinical Investiga-tion vol 110 no 7 pp 955ndash963 2002
[26] C G M Kallenberg ldquoPathogenesis of ANCA-associated vas-culitis an updaterdquo Clinical Reviews in Allergy and Immunologyvol 41 no 2 pp 224ndash231 2011
[27] H Pfister M Ollert L F Frohlich et al ldquoAntineutrophilcytoplasmic autoantibodies against the murine homolog ofproteinase 3 (Wegener autoantigen) are pathogenic in vivordquoBlood vol 104 no 5 pp 1411ndash1418 2004
[28] R J Falk R S Terrell L A Charles and J C Jennette ldquoAnti-neutrophil cytoplasmic autoantibodies induce neutrophils todegranulate and produce oxygen radicals in vitrordquo Proceedingsof the National Academy of Sciences of the United States ofAmerica vol 87 no 11 pp 4115ndash4119 1990
[29] L A Charles M L R Caldas R J Falk R S Terrell andJ C Jennette ldquoAntibodies against granule proteins activateneutrophils in vitrordquo Journal of Leukocyte Biology vol 50 no6 pp 539ndash546 1991
[30] A J Porges P B Redecha W T Kimberly E Csernok W LGross and R P Kimberly ldquoAnti-neutrophil cytoplasmic anti-bodies engage and activate human neutrophils via Fc gammaRIIardquoThe Journal of Immunology vol 153 no 3 pp 1271ndash12801994
[31] A H Mulder P Heeringa E Brouwer P C Limburg and CG Kallenberg ldquoActivation of granulocytes by anti-neutrophilcytoplasmic antibodies (ANCA) a Fc gamma RII-dependentprocessrdquoClinical amp Experimental Immunology vol 98 no 2 pp270ndash278 1994
BioMed Research International 7
[32] R Kettritz J C Jennette andR J Falk ldquoCrosslinking of ANCA-antigens stimulates superoxide release by human neutrophilsrdquoJournal of the American Society of Nephrology vol 8 no 3 pp386ndash394 1997
[33] B H Ewert J C Jennette and R J Falk ldquoAnti-myeloperoxidaseantibodies stimulate neutrophils to damage human endothelialcellsrdquo Kidney International vol 41 no 2 pp 375ndash383 1992
[34] K Kessenbrock M Krumbholz U Schonermarck et al ldquoNet-ting neutrophils in autoimmune small-vessel vasculitisrdquoNatureMedicine vol 15 no 6 pp 623ndash625 2009
[35] A K Gupta M B Joshi M Philippova et al ldquoActivatedendothelial cells induce neutrophil extracellular traps and aresusceptible to NETosis-mediated cell deathrdquo FEBS Letters vol584 no 14 pp 3193ndash3197 2010
[36] O O Rowaiye M Kusztal and M Klinger ldquoThe kidneys andANCA-associated vasculitis from pathogenesis to diagnosisrdquoClinical Kidney Journal vol 8 no 3 pp 343ndash350 2015
[37] H Xiao A Schreiber P Heeringa R J Falk and J C JennetteldquoAlternative complement pathway in the pathogenesis of dis-ease mediated by anti-neutrophil cytoplasmic autoantibodiesrdquoAmerican Journal of Pathology vol 170 no 1 pp 52ndash64 2007
[38] U Schonermarck E Csernok and W L Gross ldquoPathogenesisof anti-neutrophil cytoplasmic antibody-associated vasculitischallenges and solutions 2014rdquo Nephrology Dialysis Transplan-tation vol 30 supplement 1 pp i46ndashi52 2015
[39] C Franssen R Gans C Kallenberg C Hageluken and SHoorntje ldquoDisease spectrum of patients with antineutrophilcytoplasmic autoantibodies of defined specificity distinct dif-ferences between patients with anti-proteinase 3 and anti-myeloperoxidase autoantibodiesrdquo Journal of Internal Medicinevol 244 no 3 pp 209ndash216 1998
[40] R Kain M Exner R Brandes et al ldquoMolecular mimicry inpauci-immune focal necrotizing glomerulonephritisrdquo NatureMedicine vol 14 no 10 pp 1088ndash1096 2008
[41] R Kain H Tadema E F McKinney et al ldquoHigh prevalenceof autoantibodies to hLAMP-2 in anti-neutrophil cytoplasmicantibody-associated vasculitisrdquo Journal of the American Societyof Nephrology vol 23 no 3 pp 556ndash566 2012
[42] A J Roth M C Brown R N Smith et al ldquoAnti-LAMP-2antibodies are not prevalent in patients with antineutrophilcytoplasmic autoantibody glomerulonephritisrdquo Journal of theAmerican Society of Nephrology vol 23 no 3 pp 545ndash555 2012
[43] R Kain and A J Rees ldquoWhat is the evidence for antibodies toLAMP-2 in the pathogenesis of ANCA associated small vesselvasculitisrdquo Current Opinion in Rheumatology vol 25 no 1 pp26ndash34 2013
[44] J Hao C Wang S-J Gou M-H Zhao and M Chen ldquoTheassociation between anti-plasminogen antibodies and diseaseactivity in ANCA-associated vasculitisrdquo Rheumatology vol 53no 2 pp 300ndash306 2014
[45] A E Berden S L Nolan H L Morris et al ldquoAnti-plasminogenantibodies compromise fibrinolysis and associatewith renal his-tology in ANCA-associated vasculitisrdquo Journal of the AmericanSociety of Nephrology vol 21 no 12 pp 2169ndash2179 2010
[46] C A Stegeman J W Cohen Tervaert W J Sluiter W LManson P E De Jong and C G M Kallenberg ldquoAssociationof chronic nasal carriage of Staphylococcus aureus and higherrelapse rates in Wegener granulomatosisrdquo Annals of InternalMedicine vol 120 no 1 pp 12ndash17 1994
[47] K Zycinska K A Wardyn T M Zielonka R Krupa andW Lukas ldquoCo-trimoxazole and prevention of relapses of PR3-ANCA positive vasculitis with pulmonary involvementrdquo Euro-pean Journal ofMedical Research vol 14 supplement 4 pp 265ndash267 2009
[48] A D Salama and C D Pusey ldquoShining a LAMP on pauci-immune focal segmental glomerulonephritisrdquo Kidney Interna-tional vol 76 no 1 pp 15ndash17 2009
[49] MMVanTimmeren andPHeeringa ldquoPathogenesis ofANCA-associated vasculitis recent insights from animal modelsrdquoCurrent Opinion in Rheumatology vol 24 no 1 pp 8ndash14 2012
[50] A M Coughlan S J Freeley and M G Robson ldquoAnimalmodels of anti-neutrophil cytoplasmic antibody-associated vas-culitisrdquo Clinical and Experimental Immunology vol 169 no 3pp 229ndash237 2012
[51] S L Hogan K K Satterly M A Dooley P H Nachman JC Jennette and R J Falk ldquoSilica exposure in anti-neutrophilcytoplasmic autoantibody-associated glomerulonephritis andlupus nephritisrdquo Journal of the American Society of Nephrologyvol 12 no 1 pp 134ndash142 2001
[52] Z Rihova D Maixnerova E Jancova et al ldquoSilica andasbestos exposure in ANCA-associated vasculitis with pul-monary involvementrdquo Renal Failure vol 27 no 5 pp 605ndash6082005
[53] T Kanda H Tanio CWu H Nishihara F Nogaki and T OnoldquoChurg-Strauss syndrome with severe granulomatous angiitisand crescentic glomerulonephritis which developed duringtherapy with a leukotriene receptor antagonistrdquo Clinical andExperimental Nephrology vol 14 no 6 pp 602ndash607 2010
[54] M Suneja S Baiswar and S A Vogelgesang ldquoHydralazineassociated pauci-immune glomerulonephritisrdquo Journal of Clin-ical Rheumatology vol 20 no 2 pp 99ndash102 2014
[55] S Morita Y Ueda and K Eguchi ldquoAnti-thyroid drug-inducedANCA-associated vasculitis a case report and review of theliteraturerdquo Endocrine Journal vol 47 no 4 pp 467ndash470 2000
[56] H K Choi P A Merkel A M Walker and J L NilesldquoDrug-associated antineutrophil cytoplasmic antibody-positivevasculitis prevalence among patients with high titers ofantimyeloperoxidase antibodiesrdquo Arthritis and Rheumatismvol 43 no 2 pp 405ndash413 2000
[57] J C Jennette R J Falk and A H Gasim ldquoPathogenesis ofantineutrophil cytoplasmic autoantibody vasculitisrdquo CurrentOpinion in Nephrology andHypertension vol 20 no 3 pp 263ndash270 2011
[58] W F Pendergraft III G A Preston R R Shah et al ldquoAutoim-munity is triggered by cPR-3(105ndash201) a protein complemen-tary to human autoantigen proteinase-3rdquo Nature Medicine vol10 no 1 pp 72ndash79 2004
[59] P Hewins F Belmonte J C Jennette R J Falk and G APreston ldquoLongitudinal studies of patients with ANCA vasculi-tis demonstrate concurrent reactivity to complementary PR3protein segments cPR3m and cPR3C and with no reactivity tocPR3Nrdquo Autoimmunity vol 44 no 2 pp 98ndash106 2011
[60] P A Lyons T F Rayner S Trivedi et al ldquoGenetically distinctsubsets within ANCA-associated vasculitisrdquo The New EnglandJournal of Medicine vol 367 no 3 pp 214ndash223 2012
[61] G Xie D Roshandel R Sherva et al ldquoAssociation of granulo-matosis with polyangiitis (Wegenerrsquos) with HLA-DPB1lowast04 andSEMA6A gene variants evidence from genome-wide analysisrdquoArthritis amp Rheumatism vol 65 no 9 pp 2457ndash2468 2013
[62] V Witko-Sarsat P Lesavre S Lopez et al ldquoA large subset ofneutrophils expressing membrane proteinase 3 is a risk factor
8 BioMed Research International
for vasculitis and rheumatoid arthritisrdquo Journal of the AmericanSociety of Nephrology vol 10 no 6 pp 1224ndash1233 1999
[63] P Jagiello P Aries L Arning et al ldquoThe PTPN22 620W alleleis a risk factor for Wegenerrsquos granulomatosisrdquo Arthritis andRheumatism vol 52 no 12 pp 4039ndash4043 2005
[64] D Martorana F Maritati G Malerba et al ldquoPTPN22 R620Wpolymorphism in the ANCA-associated vasculitidesrdquo Rheuma-tology vol 51 no 5 Article ID ker446 pp 805ndash812 2012
[65] R Giscombe X Wang D Huang and A K Lefvert ldquoCodingsequence 1 and promoter single nucleotide polymorphismsin the CTLA-4 gene in Wegenerrsquos granulomatosisrdquo Journal ofRheumatology vol 29 no 5 pp 950ndash953 2002
[66] P Lamprecht S Wieczorek J T Epplen P Ambrosch and CG M Kallenberg ldquoGranuloma formation in ANCA-associatedvasculitidesrdquo APMIS vol 117 supplement s127 no 127 pp 32ndash36 2009
[67] M D Morgan C J Day K P Piper et al ldquoPatients withWegenerrsquos granulomatosis demonstrate a relative deficiency andfunctional impairment of T-regulatory cellsrdquo Immunology vol130 no 1 pp 64ndash73 2010
[68] M E Free D O Bunch J A McGregor et al ldquoPatients withantineutrophil cytoplasmic antibody-associated vasculitis havedefective Treg cell function exacerbated by the presence ofa suppression-resistant effector cell populationrdquo Arthritis andRheumatism vol 65 no 7 pp 1922ndash1933 2013
[69] B Wilde M Thewissen J Damoiseaux et al ldquoRegulatory Bcells in ANCA-associated vasculitisrdquo Annals of the RheumaticDiseases vol 72 no 8 pp 1416ndash1419 2013
[70] N Kesel D Khler L Herich et al ldquoCartilage destruction ingranulomatosis with polyangiitis (Wegenerrsquos granulomatosis)is mediated by human fibroblasts after transplantation intoimmunodeficientmicerdquoTheAmerican Journal of Pathology vol180 no 5 pp 2144ndash2155 2012
[71] C Rahmattulla R A de Lind van Wijngaarden A E Berdenet al ldquoRenal function and ear nose throat involvement in anti-neutrophil cytoplasmic antibody-associated vasculitis prospec-tive data from the European Vasculitis Society clinical trialsrdquoRheumatology vol 54 no 5 pp 899ndash907 2015
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
is associated with a higher diagnostic yield and lower proce-dural risk [9]The distinctive pathological features associatedwith PICG are necrosis of the capillary loops extracapillaryproliferation with crescent formation periglomerular andinterstitial infiltrates necrotizing arteritis and absence orpaucity of immune deposits [10]
A crescent is characterized by extracapillary proliferationwithin a glomerulus either partially or completely fillingup Bowmanrsquos space It is composed of proliferating parietalepithelial cells podocytes macrophages and fibroblastsCrescent formation is stimulated by the entry of fibrin andother plasma proteins from the capillary lumens followingthe rupture of the glomerular basement membrane (GBM)This is followed by the migration of T cells macrophagesand other inflammatory cells to the site of injury acceleratingcytokine release and tissue injury These ldquocellularrdquo crescentsmay finally evolve into fibrocellular or fibrous crescents withincreased extracellular matrix and collagen depositionThusthe presence of GBM rupture in a sclerosed glomerulusshould raise suspicion for previous crescentic glomerularinjury
The arrangement and the degree of crescent formationas well as the presence of sclerosis play a significant rolein determining the clinical course of PICG [11 12] Berdenet al recently presented a histopathologic classification sys-tem developed by the international working group of renalpathologists They performed a validation study on 100 renalbiopsies from patients with clinically and histopathologicallyconfirmed diagnosis of ANCA-associated glomerulonephri-tis The authors divided renal biopsies into four histologicalcategories as seen under light microscopy focal crescenticmixed and sclerotic based on the proportion of normalcellular crescentic and sclerotic glomeruli present Theiranalysis showed that this classification system has goodprognostic value in terms of renal outcome at 1 and 5 yearsRenal survival at 1 year was 93 for patients whose renalbiopsies were classified as focal at the time of diagnosis 84for patients whose biopsies were classified as crescentic 69for patients whose biopsies were classified as mixed and50 for patients whose biopsies were classified as scleroticRenal survival percentages at 5 years were 93 (focal) 76(crescentic) 61 (mixed) and 50 (sclerotic) In the scleroticcategory renal survival at 7 years was only 25 Severalvalidation studies out of Japan China Australia UnitedStates Netherlands and Turkey have further confirmedthat the outlined histopathological classification of ANCA-associated glomerulonephritis is of predictive value in termsof renal outcome [13ndash15] This was especially true for theoutlier categories of focal and sclerotic glomerular injuries
Although in PICG by definition there is a paucity ofimmune deposits on immunofluorescence microscopy andelectron microscopy a significant proportion of cases mayindeed show Ig deposits on histopathological examination[7 16 17] Neumann et al [17] showed that the presence of Igdeposits resulted in significantly more proteinuria and maybe associated with worse prognosis This can be explainedby the hypothesis that ANCA and immune complexes mayact synergistically to produce a more severe injury at theglomerulus It is also important to note that experimental
animal models have not convincingly ruled out the presenceof immune deposits in ANCA-associated glomerulonephritis[18 19] Rats preimmunized with human MPO-ANCA thatwere subsequently perfused with lysosomal extracts andH2O2 developed CGN and also showed IgG and C3 deposi-tion early in the course of the disease process Moreover thedegree of histologic injury was proportional to the amountof IgG immune deposits Interestingly the Ig deposits couldnot be detected later in the disease course suggesting that thepresence of immune complexes may be time dependent andnot seen by the time most patients are biopsied Finally thereare also reports of ANCA-associated glomerulonephritiscomplicating immune complex related diseases such as IgAnephropathy membranous glomerulonephritis and postin-fectious glomerulonephritis [7 20ndash22] Thus it is importantto test forANCAeven in caseswith immune deposits on renalhistology (type II lesions)
5 Pathophysiology
Despite the paucity of immune deposits PICG is a classicallyimmune mediated disease process Most of the in vitro invivo and clinical studies point to the involvement of ANCAin the pathogenesis of this disease [23ndash26] One example ofdirect evidence implicating the role of ANCA comes from acase report of neonatal microscopic polyangiitis secondaryto the transplacental transfer of MPO-ANCA [24] Thisfinding though interesting needs further substantiation infuture studies In addition several animal models of ANCA-associated renal disease have also been described Xiao et al[25] injected splenocytes from MPO-immunized mice intobothB andT cell depletedmice andwild typemiceThe recip-ient mice developed pauci-immune necrotizing crescenticglomerulonephritis and hemorrhagic pulmonary capillaritisalmost identical to the histopathology and phenotype ofhuman MPO-ANCA-associated vasculitis Transfer of IgGalone fromMPO-immunizedmice resulted in pauci-immunefocal necrotizing CGN in the recipient clearly demonstratingthe role of anti-MPO antibodies Although in vivo evidencesupporting the role of MPO-ANCA is well documented theresults have not yet been convincingly replicated for PR3-ANCAdisease in animalmodels [27] Some experts have thusquestioned the role of PR3 antibodies in the induction ofANCA disease and have instead proposed other mechanismssuch as T cell mediated inflammation
Anti-neutrophil cytoplasmic autoantibodies (ANCA) arespecific for proteins in the cytoplasm of neutrophils andmonocytes The major target antigens in patients with vas-culitis and glomerulonephritis are myeloperoxidase (MPO)and proteinase 3 (PR3) After binding with the target antigensPR3 or MPO ANCA results in the activation of neutrophilsand monocytes once the cells are primed with low dosesof cytokines such as tumor necrosis factor alpha (TNF-120572) interleukin-1 and interleukin-18 [26 28 29] There arepriming results in the surface expression of PR3 and MPOallowing interaction with ANCA Neutrophil activation ismediated by the engagement of both Fc120574 and Fab10158402 receptors[30 31] In particular the Fc120574 IIa and IIIb receptors areinvolved ANCA-mediated activation of neutrophils results
4 BioMed Research International
in the production of reactive oxygen species and the releaseof lytic enzymes such as elastase that are injurious to theendothelial cells [28 32 33] ANCAalso stimulates the releaseof neutrophil extracellular traps (NETs) that are composedof chromatin fibers and autoantigens including MPO andPR3 [34 35] NETs can damage endothelial cells and entireglomeruli andmay also be involved in propagating theANCAautoimmune response [34] In addition it has become clearthat the alternative pathway of complement activation playsa role in mediating tissue injury in PICG [36 37] Activatedneutrophils release various factors such as properdin whichactivate the alternate pathway with the generation of C3Properdin a molecule stored in neutrophilic granules isreleased when C5a primes the activation of neutrophils Thisoptimizes the interaction with ANCA and helps activate thealternate complement pathway All this sets off a cascade ofevents that augment neutrophil recruitment and activationresulting in the widespread necrotizing lesions seen in AAV[37] It is important to note that ANCA antigen specificityappears to be more closely associated with disease phenotypeand prognosis than with the clinical diagnosis of GPA orMPA [38 39] PR3-ANCA is associated with granulomatousinflammation more extensive extrarenal involvement and ahigher relapse rate In contrastMPO-ANCA ismore frequentin renal-limited disease displays more kidney scarring andcarries an overall worse renal prognosis
Antibodies other than ANCA have also been studiedin patients with PICG Kain et al demonstrated that anew subtype of ANCA lysosomal membrane protein 2(LAMP-2) antibodies are more prevalent than MPO andPR3 antibodies in patients with biopsy proven pauci-immunefocal necrotizing glomerulonephritis (FNGN) [40] Theyalso showed the development of characteristic lesions in thekidneys of rats after injecting them with LAMP-2 antibodiesand apoptosis of human endothelium in vitro by monoclonalantibody to human LAMP-2 (H4B4) A subsequent studyperformed by the same group not only showed the highprevalence of LAMP-2 antibodies in patients with PICGbut also demonstrated that they become undetectable withtreatment and frequently detectable during a relapse [41]which has obvious clinical implications However anotherstudy could not establish a relationship between LAMP-2antibodies and PICG [42] Some investigators have suggestedthat this difference in the results can be attributed to thepatient selection criteria and the assays used [43] Regardlessthese observations are intriguing and merit further studyFinally anti-plasminogen antibodies found in some patientswith AAV have been linked to increased susceptibility tothromboembolic events and greater severity of renal andsystemic disease [44 45]
Several environmental factors have now been associatedwith the pathogenesis of PICG Microbial factors play a rolein initiating the autoimmune response via their mimicryof host antigens [40] Previous studies have demonstratedthat patients with GPA are often chronic nasal carriers ofStaphylococcus aureus and that antimicrobial therapy maydecrease relapses [46 47] S aureus infection may alsoenhance the ability of the neutrophils to form NETs in smallvessel vasculitis [34] More recent evidence has identified
LAMP-2 epitope with 100 homology to fimbrial adhesin(FimH) seen in Gram-negative bacteria [48] It has beenhypothesized that immune response to FimH as seen inurosepsis triggers anti-LAMP-2 antibodies due to molecularmimicry
Another line of evidence implicating the role of microbialfactors comes from in vivo animal studies evaluating the roleof toll-like receptors (TLRs) in the pathogenesis of PICG[49 50] TLRs are a class of receptors present on leuko-cytes that are capable of recognizing infectious organismsand play an important role in generating innate immuneresponse TLR4 ligation has been found to play a role in AAVinduction It results in stimulation of T helper 17 (Th17) andTh1 responses via TLR2 and TLR9 activation respectively[49]
Several nonmicrobial environmental factors have alsobeen linked to PICG Silica is a known risk factor for ANCA[51 52] Certain drugs such as propylthiouracil hydralazineD-penicillamine cefotaxime minocycline anti-TNF agentsphenytoin and certain psychoactive agents are also known tocause ANCA-associated disease [53ndash56]
The role of autoimmune mechanisms in pauci-immuneCGN is also supported by another theory that states that theinitial immune response is generated against the complemen-tary PR3 (cPR3) peptide (generated by antisense DNA strandof PR3) or a mimic of cPR3 rather than against PR3 peptide[57ndash59] Patients with PR3-ANCA disease harbor not onlycirculating antibodies against sense PR3 peptides but also aseparate set of antibodies against antisense complementaryPR3 peptides (anti-cPR3) The immune response againstcPR3 results in the production of anti-cPR3 antibodies whichin turn generate anti-idiotypic antibodies that recognize notonly the idiotope on the anti-cPR3 antibodies but also theepitope on the sense PR3 peptide (original autoantigen)Interestingly a number of pathogens such as S aureus RossRiver virus and Entamoeba histolytica have sequences similarto cPR3 peptide thus making them capable of generatingthe autoimmune response [58] This provides another linkbetween infection and autoimmunity in PICG
The role of genetic factors in the pathogenesis of PICG isevident from the fact that not every individual with environ-mental risk factors develops the disease It is also observedthat AAV is more common in Caucasian population Theunderstanding of genetics in AAV has greatly improvedafter the publication of two genome-wide association studies(GWASs) [60 61]The goal of GWASs is to interrogate a largenumber of single-nucleotide polymorphisms (SNPs) thatcover a big portion of the human genome Interestingly thethree main AAV subtypes are associated with distinct HLAvariants that is granulomatosis with polyangiitis (Wegenerrsquos)GPA with HLA-DP1 microscopic polyangiitis (MPA) withHLA-DQ and eosinophilic GPA (Churg-Strauss) with HLA-DRB4 Patients with GPA are also known to have a higherproportion of neutrophils with increased surface expressionof PR3 [62] GWASs also revealed that polymorphic vari-ants of genes encoding PR3 and its main inhibitor alpha-1antitrypsin are highly associated with GPA especially withPR3-ANCA positivity regardless of the clinical diagnosisCandidate gene approach studies have shown associations
BioMed Research International 5
with other variants involved in AAV such as those belongingto the CTLA-4 and PTPN22 genes These results have not yetbeen replicated in larger studies [63ndash65]
Also it is important to discuss the role of T cell mediatedimmune response in PICG It is widely known that CD4+helper T cells with interferon-gamma secretion are involvedin granuloma formation Granulomas are seen mainly inPR3 AAV and not in MPO AAV TH17 cells play a majorrole in causing granulomatous inflammation and vascularinjury in PR3 AAV [66] Morgan et al have also showndiminished number and functional impairment of regulatoryT cells (Tregs) inGPA [67] Finally according to some studiespatients with ANCA-mediated vasculitis have impaired func-tioning of Tregs alongwith the presence of effector T cells thatare resistant to suppression by Tregs [68]
In addition to autoantibody production B cells also havethe ability to present antigens to T cells and may modulateT cell responses in small vessel vasculitis Regulatory B cells(Bregs) are a distinct B cell subset cells that regulate theaction of the T cell population by secreting IL-10 Wilde etal demonstrated that there is a reduction in the numberof Bregs in both active and quiescent AAV [69] The studyalso revealed a positive correlation between Breg and Treg inquiescent AAV and that Th1 cell suppression by Breg may beinadequate in active AAV
Recently the pathogenic mechanisms of tissue damagein GPA resulting in saddle nose deformity and orbitaldestruction have been further elucidated [38 70] Fibroblastslining bone and cartilage have been acknowledged to playthe role of activated effector cells of tissue destruction inGPA In the first in vivo model of GPA Kesel et al subcu-taneously coimplanted the biopsy specimens from patientswith activeGPAor sinusitis (controls) with healthy allogeneichuman nasal cartilage into immunodeficient mice [70] GPAimplants showed massive destruction of the coimplantedhuman cartilage whereas cartilage destruction was onlymarginal in control samples Further cartilage destructionwas mediated by human fibroblasts and could be controlledsimilar to GPA in humans with corticosteroids In additionin fibrotic lung disease NETs were shown to promote differ-entiation and function of fibroblasts indicating that NETs areinvolved not only in inflammation but also in the resultingfibrosis [38 71]
6 Clinical Manifestations and Natural History
Notwithstanding a slightly higher specificity ANCA is topauci-immune RPGN as anti-DNA is to systemic lupuserythematosus Microscopic polyangiitis (MPA) granulo-matosis with polyangiitis (GPA) eosinophilic granulomatosiswith polyangiitis (EGPA or Churg-Strauss syndrome) andrenal-limited pauci-immune crescentic GN (PICG) are allassociated with ANCA The term ldquopauci-immunerdquo RPGNencapsulates all of these conditions Generalized nonspecificmanifestations of systemic inflammatory disease such asfever malaise anorexia weight loss myalgia and arthralgiacan be seen in any of these diseases The clinical manifesta-tions of each entity vary based on the chronicity and sitesof involvement Patients without systemic involvement may
present later in the course of their disease Granulomatousinvolvement particularly of the upper respiratory tract is acharacteristic feature of GPA but not of MPA eosinophiliaasthma and atopy typically occur in EGPA In each of theseconditions patients can have pulmonary hemorrhage causedby hemorrhagic alveolar capillaritis which has treatmentand prognostic implications [2] As mentioned previouslythe renal failure seen in PICG usually presents clinicallyas RPGN It should be noted though that patients withGPA or MPA could also present with subacute or chronicnephritis In one study assessing the clinical characteristicsof pauci-immune crescentic GN a cohort of more than 300patients evaluated at renal biopsy had a mean age of 56 plusmn 20years (range 2 to 92 years) male-to-female ratio of 10 09mean serum creatinine concentration of 65 plusmn 40mgdL(range 08 to 221mgdL) and proteinuria of 19 plusmn 30 gday(range 01 to 18 gday) [2] Older age higher serum creatinineconcentration at presentation pulmonary hemorrhage anddialysis-dependent renal failure correlate with an overallpoor prognosis Respiratory tract disease and PR3-ANCAare predictors of higher relapse rates [2] Regardless of thecategory of ANCA disease though the best clinical predictorof renal outcome is the glomerular filtration rate (GFR)at the time of diagnosis [1] Interestingly in one of therecent studies the presence of ear nose and throat (ENT)involvement in AAV patients was found to be associatedwith lesser degree of interstitial fibrosis and tubular atrophyon kidney biopsy and better renal function These resultsindicate that there may be different phenotypes of AAVdefined by ENT involvement [71]
7 Conclusion
Despite significant advances in our understanding of theimmune system issues of incomplete efficacy treatmenttoxicity and infectious complications persist With targetedapproaches to immunosuppression andnewer biologic agentsmodulating B and T cell function the future holds promisein terms of greater treatment efficacy with an improved sideeffect profile We believe that future studies will highlight theintricacies of the clinical and pathological spectrum of PICGwhile proposing novel mechanisms for inducing and main-taining remission Based on current guidelines for patientsin complete remission and without extrarenal manifestationsfor at least 12 months renal transplant should not be delayedANCA positivity is not considered a contraindication fortransplantation However no prospective data are availableto assess the likelihood of recurrent ANCA vasculitis afterkidney transplantation In addition the impact of diseaseactivity or ANCA positivity at the time of transplantationon patient outcome is unclear Future studies must bedesigned to gather prospective data that helps answer thesequestions
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
6 BioMed Research International
References
[1] R J Glassock S G Adler H JWard et al ldquoPrimary glomerulardiseasesrdquo inTheKidney BM Brenner and F C Rector Eds pp1182ndash1279 Saunders Philadelphia Pa USA 4th edition 1991
[2] J Charles Jennette R J Falk and J G McGregor ldquoRenaland systemic valculitisrdquo in Comprehensive Clinical NephrologyElsevier 5th edition 2015
[3] S Watnick and T Dirkx ldquoKidney diseaserdquo in Current MedicalDiagnosis amp Treatment 2015 M A Papadakis S J McPhee andM W Rabow Eds McGraw-Hill New York NY USA 2014
[4] J C Jennette J L Olson M M Schwartz and F G SilvaldquoPauci-immune and ANCA-mediated crescentic glomeru-lonephritis and vasculitisrdquo in Heptinstallrsquos Pathology of theKidney vol 1 chapter 14 6th edition 2007
[5] P Seo and J H Stone ldquoThe antineutrophil cytoplasmicantibody-associated vasculitidesrdquo The American Journal ofMedicine vol 117 no 1 pp 39ndash50 2004
[6] U Eisenberger F Fakhouri P Vanhille et al ldquoANCA-negative pauci-immune renal vasculitis histology and out-comerdquo Nephrology Dialysis Transplantation vol 20 no 7 pp1392ndash1399 2005
[7] M Haas and J A Eustace ldquoImmune complex deposits inANCA-associated crescentic glomerulonephritis a study of 126casesrdquo Kidney International vol 65 no 6 pp 2145ndash2152 2004
[8] J B Levy T Hammad A Coulthart T Dougan and C DPusey ldquoClinical features and outcome of patients with bothANCA and anti-GBMantibodiesrdquoKidney International vol 66no 4 pp 1535ndash1540 2004
[9] N Kambham ldquoCrescentic glomerulonephritis an update onpauci-immune and anti-GBM diseasesrdquo Advances in AnatomicPathology vol 19 no 2 pp 111ndash124 2012
[10] F Ferrario A Vanzati and F Pagni ldquoPathology of ANCA-associated vasculitisrdquo Clinical and Experimental Nephrologyvol 17 no 5 pp 652ndash658 2013
[11] A E Berden F Ferrario E C Hagen et al ldquoHistopathologicclassification of ANCA-associated glomerulonephritisrdquo Journalof the American Society of Nephrology vol 21 no 10 pp 1628ndash1636 2010
[12] S L Ford K R Polkinghorne A Longano et al ldquoHistopatho-logic and clinical predictors of kidney outcomes in ANCA-associated vasculitisrdquo American Journal of Kidney Diseases vol63 no 2 pp 227ndash235 2014
[13] T Iwakiri S Fujimoto K Kitagawa et al ldquoValidation of anewly proposed histopathological classification in Japanesepatients with anti-neutrophil cytoplasmic antibody-associatedglomerulonephritisrdquo BMC Nephrology vol 14 article 125 2013
[14] E Nohr L Girard M James and H Benediktsson ldquoValidationof a histopathologic classification scheme for antineutrophilcytoplasmic antibody-associated glomerulonephritisrdquo HumanPathology vol 45 no 7 pp 1423ndash1429 2014
[15] D-Y Chang L-H Wu G Liu M Chen C G M Kallenbergand M-H Zhao ldquoRe-evaluation of the histopathologic classifi-cation of ANCA-associated glomerulonephritis a study of 121patients in a single centerrdquoNephrology Dialysis Transplantationvol 27 no 6 pp 2343ndash2349 2012
[16] M El-Ters U Muthyala M D Philipneri F A Hussein andK L Lentine ldquoImmune-complex deposits in lsquopauci-immunersquoglomerulonephritis a case report and brief review of recentliteraturerdquoArchives of Medical Science vol 6 no 4 pp 633ndash6372010
[17] I Neumann H Regele R Kain R Birck and F T MeislldquoGlomerular immune deposits are associated with increasedproteinuria in patients with ANCA-associated crescenticnephritisrdquo Nephrology Dialysis Transplantation vol 18 no 3pp 524ndash531 2003
[18] E Brouwer M G Huitema P A Klok et al ldquoAntimye-loperoxidase-associated proliferative glomerulonephritis ananimal modelrdquo Journal of Experimental Medicine vol 177 no4 pp 905ndash914 1993
[19] J J Yang J C Jennette and R J Falk ldquoImmune complexglomerulonephritis is induced in rats immunizedwith heterolo-gous myeloperoxidaserdquo Clinical and Experimental Immunologyvol 97 no 3 pp 466ndash473 1994
[20] M Haas J Jafri S M Bartosh S L Karp S G Adler and S MMeehan ldquoANCA-associated crescentic glomerulonephritis withmesangial IgA depositsrdquo American Journal of Kidney Diseasesvol 36 no 4 pp 709ndash718 2000
[21] M Haas ldquoIncidental healed postinfectious glomerulonephritisa study of 1012 renal biopsy specimens examined by electronmicroscopyrdquo Human Pathology vol 34 no 1 pp 3ndash10 2003
[22] R Jimbo Y Ubara T Tagami et al ldquoA pediatric occurrenceof crescentic glomerulonephritis associated with antineutrophilcytoplasmic antibodies and mesangial IgA depositsrdquo ClinicalNephrology vol 68 no 2 pp 104ndash108 2007
[23] J C Jennette ldquoRapidly progressive crescentic glomerulonephri-tisrdquo Kidney International vol 63 no 3 pp 1164ndash1177 2003
[24] P J Bansal andM C Tobin ldquoNeonatal microscopic polyangiitissecondary to transfer of maternal myeloperoxidase-antineutrophil cytoplasmic antibody resulting in neonatalpulmonary hemorrhage and renal involvementrdquo Annals ofAllergy Asthma and Immunology vol 93 no 4 pp 398ndash4012004
[25] H Xiao P Heeringa P Hu et al ldquoAntineutrophil cytoplasmicautoantibodies specific for myeloperoxidase cause glomeru-lonephritis and vasculitis in micerdquo Journal of Clinical Investiga-tion vol 110 no 7 pp 955ndash963 2002
[26] C G M Kallenberg ldquoPathogenesis of ANCA-associated vas-culitis an updaterdquo Clinical Reviews in Allergy and Immunologyvol 41 no 2 pp 224ndash231 2011
[27] H Pfister M Ollert L F Frohlich et al ldquoAntineutrophilcytoplasmic autoantibodies against the murine homolog ofproteinase 3 (Wegener autoantigen) are pathogenic in vivordquoBlood vol 104 no 5 pp 1411ndash1418 2004
[28] R J Falk R S Terrell L A Charles and J C Jennette ldquoAnti-neutrophil cytoplasmic autoantibodies induce neutrophils todegranulate and produce oxygen radicals in vitrordquo Proceedingsof the National Academy of Sciences of the United States ofAmerica vol 87 no 11 pp 4115ndash4119 1990
[29] L A Charles M L R Caldas R J Falk R S Terrell andJ C Jennette ldquoAntibodies against granule proteins activateneutrophils in vitrordquo Journal of Leukocyte Biology vol 50 no6 pp 539ndash546 1991
[30] A J Porges P B Redecha W T Kimberly E Csernok W LGross and R P Kimberly ldquoAnti-neutrophil cytoplasmic anti-bodies engage and activate human neutrophils via Fc gammaRIIardquoThe Journal of Immunology vol 153 no 3 pp 1271ndash12801994
[31] A H Mulder P Heeringa E Brouwer P C Limburg and CG Kallenberg ldquoActivation of granulocytes by anti-neutrophilcytoplasmic antibodies (ANCA) a Fc gamma RII-dependentprocessrdquoClinical amp Experimental Immunology vol 98 no 2 pp270ndash278 1994
BioMed Research International 7
[32] R Kettritz J C Jennette andR J Falk ldquoCrosslinking of ANCA-antigens stimulates superoxide release by human neutrophilsrdquoJournal of the American Society of Nephrology vol 8 no 3 pp386ndash394 1997
[33] B H Ewert J C Jennette and R J Falk ldquoAnti-myeloperoxidaseantibodies stimulate neutrophils to damage human endothelialcellsrdquo Kidney International vol 41 no 2 pp 375ndash383 1992
[34] K Kessenbrock M Krumbholz U Schonermarck et al ldquoNet-ting neutrophils in autoimmune small-vessel vasculitisrdquoNatureMedicine vol 15 no 6 pp 623ndash625 2009
[35] A K Gupta M B Joshi M Philippova et al ldquoActivatedendothelial cells induce neutrophil extracellular traps and aresusceptible to NETosis-mediated cell deathrdquo FEBS Letters vol584 no 14 pp 3193ndash3197 2010
[36] O O Rowaiye M Kusztal and M Klinger ldquoThe kidneys andANCA-associated vasculitis from pathogenesis to diagnosisrdquoClinical Kidney Journal vol 8 no 3 pp 343ndash350 2015
[37] H Xiao A Schreiber P Heeringa R J Falk and J C JennetteldquoAlternative complement pathway in the pathogenesis of dis-ease mediated by anti-neutrophil cytoplasmic autoantibodiesrdquoAmerican Journal of Pathology vol 170 no 1 pp 52ndash64 2007
[38] U Schonermarck E Csernok and W L Gross ldquoPathogenesisof anti-neutrophil cytoplasmic antibody-associated vasculitischallenges and solutions 2014rdquo Nephrology Dialysis Transplan-tation vol 30 supplement 1 pp i46ndashi52 2015
[39] C Franssen R Gans C Kallenberg C Hageluken and SHoorntje ldquoDisease spectrum of patients with antineutrophilcytoplasmic autoantibodies of defined specificity distinct dif-ferences between patients with anti-proteinase 3 and anti-myeloperoxidase autoantibodiesrdquo Journal of Internal Medicinevol 244 no 3 pp 209ndash216 1998
[40] R Kain M Exner R Brandes et al ldquoMolecular mimicry inpauci-immune focal necrotizing glomerulonephritisrdquo NatureMedicine vol 14 no 10 pp 1088ndash1096 2008
[41] R Kain H Tadema E F McKinney et al ldquoHigh prevalenceof autoantibodies to hLAMP-2 in anti-neutrophil cytoplasmicantibody-associated vasculitisrdquo Journal of the American Societyof Nephrology vol 23 no 3 pp 556ndash566 2012
[42] A J Roth M C Brown R N Smith et al ldquoAnti-LAMP-2antibodies are not prevalent in patients with antineutrophilcytoplasmic autoantibody glomerulonephritisrdquo Journal of theAmerican Society of Nephrology vol 23 no 3 pp 545ndash555 2012
[43] R Kain and A J Rees ldquoWhat is the evidence for antibodies toLAMP-2 in the pathogenesis of ANCA associated small vesselvasculitisrdquo Current Opinion in Rheumatology vol 25 no 1 pp26ndash34 2013
[44] J Hao C Wang S-J Gou M-H Zhao and M Chen ldquoTheassociation between anti-plasminogen antibodies and diseaseactivity in ANCA-associated vasculitisrdquo Rheumatology vol 53no 2 pp 300ndash306 2014
[45] A E Berden S L Nolan H L Morris et al ldquoAnti-plasminogenantibodies compromise fibrinolysis and associatewith renal his-tology in ANCA-associated vasculitisrdquo Journal of the AmericanSociety of Nephrology vol 21 no 12 pp 2169ndash2179 2010
[46] C A Stegeman J W Cohen Tervaert W J Sluiter W LManson P E De Jong and C G M Kallenberg ldquoAssociationof chronic nasal carriage of Staphylococcus aureus and higherrelapse rates in Wegener granulomatosisrdquo Annals of InternalMedicine vol 120 no 1 pp 12ndash17 1994
[47] K Zycinska K A Wardyn T M Zielonka R Krupa andW Lukas ldquoCo-trimoxazole and prevention of relapses of PR3-ANCA positive vasculitis with pulmonary involvementrdquo Euro-pean Journal ofMedical Research vol 14 supplement 4 pp 265ndash267 2009
[48] A D Salama and C D Pusey ldquoShining a LAMP on pauci-immune focal segmental glomerulonephritisrdquo Kidney Interna-tional vol 76 no 1 pp 15ndash17 2009
[49] MMVanTimmeren andPHeeringa ldquoPathogenesis ofANCA-associated vasculitis recent insights from animal modelsrdquoCurrent Opinion in Rheumatology vol 24 no 1 pp 8ndash14 2012
[50] A M Coughlan S J Freeley and M G Robson ldquoAnimalmodels of anti-neutrophil cytoplasmic antibody-associated vas-culitisrdquo Clinical and Experimental Immunology vol 169 no 3pp 229ndash237 2012
[51] S L Hogan K K Satterly M A Dooley P H Nachman JC Jennette and R J Falk ldquoSilica exposure in anti-neutrophilcytoplasmic autoantibody-associated glomerulonephritis andlupus nephritisrdquo Journal of the American Society of Nephrologyvol 12 no 1 pp 134ndash142 2001
[52] Z Rihova D Maixnerova E Jancova et al ldquoSilica andasbestos exposure in ANCA-associated vasculitis with pul-monary involvementrdquo Renal Failure vol 27 no 5 pp 605ndash6082005
[53] T Kanda H Tanio CWu H Nishihara F Nogaki and T OnoldquoChurg-Strauss syndrome with severe granulomatous angiitisand crescentic glomerulonephritis which developed duringtherapy with a leukotriene receptor antagonistrdquo Clinical andExperimental Nephrology vol 14 no 6 pp 602ndash607 2010
[54] M Suneja S Baiswar and S A Vogelgesang ldquoHydralazineassociated pauci-immune glomerulonephritisrdquo Journal of Clin-ical Rheumatology vol 20 no 2 pp 99ndash102 2014
[55] S Morita Y Ueda and K Eguchi ldquoAnti-thyroid drug-inducedANCA-associated vasculitis a case report and review of theliteraturerdquo Endocrine Journal vol 47 no 4 pp 467ndash470 2000
[56] H K Choi P A Merkel A M Walker and J L NilesldquoDrug-associated antineutrophil cytoplasmic antibody-positivevasculitis prevalence among patients with high titers ofantimyeloperoxidase antibodiesrdquo Arthritis and Rheumatismvol 43 no 2 pp 405ndash413 2000
[57] J C Jennette R J Falk and A H Gasim ldquoPathogenesis ofantineutrophil cytoplasmic autoantibody vasculitisrdquo CurrentOpinion in Nephrology andHypertension vol 20 no 3 pp 263ndash270 2011
[58] W F Pendergraft III G A Preston R R Shah et al ldquoAutoim-munity is triggered by cPR-3(105ndash201) a protein complemen-tary to human autoantigen proteinase-3rdquo Nature Medicine vol10 no 1 pp 72ndash79 2004
[59] P Hewins F Belmonte J C Jennette R J Falk and G APreston ldquoLongitudinal studies of patients with ANCA vasculi-tis demonstrate concurrent reactivity to complementary PR3protein segments cPR3m and cPR3C and with no reactivity tocPR3Nrdquo Autoimmunity vol 44 no 2 pp 98ndash106 2011
[60] P A Lyons T F Rayner S Trivedi et al ldquoGenetically distinctsubsets within ANCA-associated vasculitisrdquo The New EnglandJournal of Medicine vol 367 no 3 pp 214ndash223 2012
[61] G Xie D Roshandel R Sherva et al ldquoAssociation of granulo-matosis with polyangiitis (Wegenerrsquos) with HLA-DPB1lowast04 andSEMA6A gene variants evidence from genome-wide analysisrdquoArthritis amp Rheumatism vol 65 no 9 pp 2457ndash2468 2013
[62] V Witko-Sarsat P Lesavre S Lopez et al ldquoA large subset ofneutrophils expressing membrane proteinase 3 is a risk factor
8 BioMed Research International
for vasculitis and rheumatoid arthritisrdquo Journal of the AmericanSociety of Nephrology vol 10 no 6 pp 1224ndash1233 1999
[63] P Jagiello P Aries L Arning et al ldquoThe PTPN22 620W alleleis a risk factor for Wegenerrsquos granulomatosisrdquo Arthritis andRheumatism vol 52 no 12 pp 4039ndash4043 2005
[64] D Martorana F Maritati G Malerba et al ldquoPTPN22 R620Wpolymorphism in the ANCA-associated vasculitidesrdquo Rheuma-tology vol 51 no 5 Article ID ker446 pp 805ndash812 2012
[65] R Giscombe X Wang D Huang and A K Lefvert ldquoCodingsequence 1 and promoter single nucleotide polymorphismsin the CTLA-4 gene in Wegenerrsquos granulomatosisrdquo Journal ofRheumatology vol 29 no 5 pp 950ndash953 2002
[66] P Lamprecht S Wieczorek J T Epplen P Ambrosch and CG M Kallenberg ldquoGranuloma formation in ANCA-associatedvasculitidesrdquo APMIS vol 117 supplement s127 no 127 pp 32ndash36 2009
[67] M D Morgan C J Day K P Piper et al ldquoPatients withWegenerrsquos granulomatosis demonstrate a relative deficiency andfunctional impairment of T-regulatory cellsrdquo Immunology vol130 no 1 pp 64ndash73 2010
[68] M E Free D O Bunch J A McGregor et al ldquoPatients withantineutrophil cytoplasmic antibody-associated vasculitis havedefective Treg cell function exacerbated by the presence ofa suppression-resistant effector cell populationrdquo Arthritis andRheumatism vol 65 no 7 pp 1922ndash1933 2013
[69] B Wilde M Thewissen J Damoiseaux et al ldquoRegulatory Bcells in ANCA-associated vasculitisrdquo Annals of the RheumaticDiseases vol 72 no 8 pp 1416ndash1419 2013
[70] N Kesel D Khler L Herich et al ldquoCartilage destruction ingranulomatosis with polyangiitis (Wegenerrsquos granulomatosis)is mediated by human fibroblasts after transplantation intoimmunodeficientmicerdquoTheAmerican Journal of Pathology vol180 no 5 pp 2144ndash2155 2012
[71] C Rahmattulla R A de Lind van Wijngaarden A E Berdenet al ldquoRenal function and ear nose throat involvement in anti-neutrophil cytoplasmic antibody-associated vasculitis prospec-tive data from the European Vasculitis Society clinical trialsrdquoRheumatology vol 54 no 5 pp 899ndash907 2015
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
in the production of reactive oxygen species and the releaseof lytic enzymes such as elastase that are injurious to theendothelial cells [28 32 33] ANCAalso stimulates the releaseof neutrophil extracellular traps (NETs) that are composedof chromatin fibers and autoantigens including MPO andPR3 [34 35] NETs can damage endothelial cells and entireglomeruli andmay also be involved in propagating theANCAautoimmune response [34] In addition it has become clearthat the alternative pathway of complement activation playsa role in mediating tissue injury in PICG [36 37] Activatedneutrophils release various factors such as properdin whichactivate the alternate pathway with the generation of C3Properdin a molecule stored in neutrophilic granules isreleased when C5a primes the activation of neutrophils Thisoptimizes the interaction with ANCA and helps activate thealternate complement pathway All this sets off a cascade ofevents that augment neutrophil recruitment and activationresulting in the widespread necrotizing lesions seen in AAV[37] It is important to note that ANCA antigen specificityappears to be more closely associated with disease phenotypeand prognosis than with the clinical diagnosis of GPA orMPA [38 39] PR3-ANCA is associated with granulomatousinflammation more extensive extrarenal involvement and ahigher relapse rate In contrastMPO-ANCA ismore frequentin renal-limited disease displays more kidney scarring andcarries an overall worse renal prognosis
Antibodies other than ANCA have also been studiedin patients with PICG Kain et al demonstrated that anew subtype of ANCA lysosomal membrane protein 2(LAMP-2) antibodies are more prevalent than MPO andPR3 antibodies in patients with biopsy proven pauci-immunefocal necrotizing glomerulonephritis (FNGN) [40] Theyalso showed the development of characteristic lesions in thekidneys of rats after injecting them with LAMP-2 antibodiesand apoptosis of human endothelium in vitro by monoclonalantibody to human LAMP-2 (H4B4) A subsequent studyperformed by the same group not only showed the highprevalence of LAMP-2 antibodies in patients with PICGbut also demonstrated that they become undetectable withtreatment and frequently detectable during a relapse [41]which has obvious clinical implications However anotherstudy could not establish a relationship between LAMP-2antibodies and PICG [42] Some investigators have suggestedthat this difference in the results can be attributed to thepatient selection criteria and the assays used [43] Regardlessthese observations are intriguing and merit further studyFinally anti-plasminogen antibodies found in some patientswith AAV have been linked to increased susceptibility tothromboembolic events and greater severity of renal andsystemic disease [44 45]
Several environmental factors have now been associatedwith the pathogenesis of PICG Microbial factors play a rolein initiating the autoimmune response via their mimicryof host antigens [40] Previous studies have demonstratedthat patients with GPA are often chronic nasal carriers ofStaphylococcus aureus and that antimicrobial therapy maydecrease relapses [46 47] S aureus infection may alsoenhance the ability of the neutrophils to form NETs in smallvessel vasculitis [34] More recent evidence has identified
LAMP-2 epitope with 100 homology to fimbrial adhesin(FimH) seen in Gram-negative bacteria [48] It has beenhypothesized that immune response to FimH as seen inurosepsis triggers anti-LAMP-2 antibodies due to molecularmimicry
Another line of evidence implicating the role of microbialfactors comes from in vivo animal studies evaluating the roleof toll-like receptors (TLRs) in the pathogenesis of PICG[49 50] TLRs are a class of receptors present on leuko-cytes that are capable of recognizing infectious organismsand play an important role in generating innate immuneresponse TLR4 ligation has been found to play a role in AAVinduction It results in stimulation of T helper 17 (Th17) andTh1 responses via TLR2 and TLR9 activation respectively[49]
Several nonmicrobial environmental factors have alsobeen linked to PICG Silica is a known risk factor for ANCA[51 52] Certain drugs such as propylthiouracil hydralazineD-penicillamine cefotaxime minocycline anti-TNF agentsphenytoin and certain psychoactive agents are also known tocause ANCA-associated disease [53ndash56]
The role of autoimmune mechanisms in pauci-immuneCGN is also supported by another theory that states that theinitial immune response is generated against the complemen-tary PR3 (cPR3) peptide (generated by antisense DNA strandof PR3) or a mimic of cPR3 rather than against PR3 peptide[57ndash59] Patients with PR3-ANCA disease harbor not onlycirculating antibodies against sense PR3 peptides but also aseparate set of antibodies against antisense complementaryPR3 peptides (anti-cPR3) The immune response againstcPR3 results in the production of anti-cPR3 antibodies whichin turn generate anti-idiotypic antibodies that recognize notonly the idiotope on the anti-cPR3 antibodies but also theepitope on the sense PR3 peptide (original autoantigen)Interestingly a number of pathogens such as S aureus RossRiver virus and Entamoeba histolytica have sequences similarto cPR3 peptide thus making them capable of generatingthe autoimmune response [58] This provides another linkbetween infection and autoimmunity in PICG
The role of genetic factors in the pathogenesis of PICG isevident from the fact that not every individual with environ-mental risk factors develops the disease It is also observedthat AAV is more common in Caucasian population Theunderstanding of genetics in AAV has greatly improvedafter the publication of two genome-wide association studies(GWASs) [60 61]The goal of GWASs is to interrogate a largenumber of single-nucleotide polymorphisms (SNPs) thatcover a big portion of the human genome Interestingly thethree main AAV subtypes are associated with distinct HLAvariants that is granulomatosis with polyangiitis (Wegenerrsquos)GPA with HLA-DP1 microscopic polyangiitis (MPA) withHLA-DQ and eosinophilic GPA (Churg-Strauss) with HLA-DRB4 Patients with GPA are also known to have a higherproportion of neutrophils with increased surface expressionof PR3 [62] GWASs also revealed that polymorphic vari-ants of genes encoding PR3 and its main inhibitor alpha-1antitrypsin are highly associated with GPA especially withPR3-ANCA positivity regardless of the clinical diagnosisCandidate gene approach studies have shown associations
BioMed Research International 5
with other variants involved in AAV such as those belongingto the CTLA-4 and PTPN22 genes These results have not yetbeen replicated in larger studies [63ndash65]
Also it is important to discuss the role of T cell mediatedimmune response in PICG It is widely known that CD4+helper T cells with interferon-gamma secretion are involvedin granuloma formation Granulomas are seen mainly inPR3 AAV and not in MPO AAV TH17 cells play a majorrole in causing granulomatous inflammation and vascularinjury in PR3 AAV [66] Morgan et al have also showndiminished number and functional impairment of regulatoryT cells (Tregs) inGPA [67] Finally according to some studiespatients with ANCA-mediated vasculitis have impaired func-tioning of Tregs alongwith the presence of effector T cells thatare resistant to suppression by Tregs [68]
In addition to autoantibody production B cells also havethe ability to present antigens to T cells and may modulateT cell responses in small vessel vasculitis Regulatory B cells(Bregs) are a distinct B cell subset cells that regulate theaction of the T cell population by secreting IL-10 Wilde etal demonstrated that there is a reduction in the numberof Bregs in both active and quiescent AAV [69] The studyalso revealed a positive correlation between Breg and Treg inquiescent AAV and that Th1 cell suppression by Breg may beinadequate in active AAV
Recently the pathogenic mechanisms of tissue damagein GPA resulting in saddle nose deformity and orbitaldestruction have been further elucidated [38 70] Fibroblastslining bone and cartilage have been acknowledged to playthe role of activated effector cells of tissue destruction inGPA In the first in vivo model of GPA Kesel et al subcu-taneously coimplanted the biopsy specimens from patientswith activeGPAor sinusitis (controls) with healthy allogeneichuman nasal cartilage into immunodeficient mice [70] GPAimplants showed massive destruction of the coimplantedhuman cartilage whereas cartilage destruction was onlymarginal in control samples Further cartilage destructionwas mediated by human fibroblasts and could be controlledsimilar to GPA in humans with corticosteroids In additionin fibrotic lung disease NETs were shown to promote differ-entiation and function of fibroblasts indicating that NETs areinvolved not only in inflammation but also in the resultingfibrosis [38 71]
6 Clinical Manifestations and Natural History
Notwithstanding a slightly higher specificity ANCA is topauci-immune RPGN as anti-DNA is to systemic lupuserythematosus Microscopic polyangiitis (MPA) granulo-matosis with polyangiitis (GPA) eosinophilic granulomatosiswith polyangiitis (EGPA or Churg-Strauss syndrome) andrenal-limited pauci-immune crescentic GN (PICG) are allassociated with ANCA The term ldquopauci-immunerdquo RPGNencapsulates all of these conditions Generalized nonspecificmanifestations of systemic inflammatory disease such asfever malaise anorexia weight loss myalgia and arthralgiacan be seen in any of these diseases The clinical manifesta-tions of each entity vary based on the chronicity and sitesof involvement Patients without systemic involvement may
present later in the course of their disease Granulomatousinvolvement particularly of the upper respiratory tract is acharacteristic feature of GPA but not of MPA eosinophiliaasthma and atopy typically occur in EGPA In each of theseconditions patients can have pulmonary hemorrhage causedby hemorrhagic alveolar capillaritis which has treatmentand prognostic implications [2] As mentioned previouslythe renal failure seen in PICG usually presents clinicallyas RPGN It should be noted though that patients withGPA or MPA could also present with subacute or chronicnephritis In one study assessing the clinical characteristicsof pauci-immune crescentic GN a cohort of more than 300patients evaluated at renal biopsy had a mean age of 56 plusmn 20years (range 2 to 92 years) male-to-female ratio of 10 09mean serum creatinine concentration of 65 plusmn 40mgdL(range 08 to 221mgdL) and proteinuria of 19 plusmn 30 gday(range 01 to 18 gday) [2] Older age higher serum creatinineconcentration at presentation pulmonary hemorrhage anddialysis-dependent renal failure correlate with an overallpoor prognosis Respiratory tract disease and PR3-ANCAare predictors of higher relapse rates [2] Regardless of thecategory of ANCA disease though the best clinical predictorof renal outcome is the glomerular filtration rate (GFR)at the time of diagnosis [1] Interestingly in one of therecent studies the presence of ear nose and throat (ENT)involvement in AAV patients was found to be associatedwith lesser degree of interstitial fibrosis and tubular atrophyon kidney biopsy and better renal function These resultsindicate that there may be different phenotypes of AAVdefined by ENT involvement [71]
7 Conclusion
Despite significant advances in our understanding of theimmune system issues of incomplete efficacy treatmenttoxicity and infectious complications persist With targetedapproaches to immunosuppression andnewer biologic agentsmodulating B and T cell function the future holds promisein terms of greater treatment efficacy with an improved sideeffect profile We believe that future studies will highlight theintricacies of the clinical and pathological spectrum of PICGwhile proposing novel mechanisms for inducing and main-taining remission Based on current guidelines for patientsin complete remission and without extrarenal manifestationsfor at least 12 months renal transplant should not be delayedANCA positivity is not considered a contraindication fortransplantation However no prospective data are availableto assess the likelihood of recurrent ANCA vasculitis afterkidney transplantation In addition the impact of diseaseactivity or ANCA positivity at the time of transplantationon patient outcome is unclear Future studies must bedesigned to gather prospective data that helps answer thesequestions
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
6 BioMed Research International
References
[1] R J Glassock S G Adler H JWard et al ldquoPrimary glomerulardiseasesrdquo inTheKidney BM Brenner and F C Rector Eds pp1182ndash1279 Saunders Philadelphia Pa USA 4th edition 1991
[2] J Charles Jennette R J Falk and J G McGregor ldquoRenaland systemic valculitisrdquo in Comprehensive Clinical NephrologyElsevier 5th edition 2015
[3] S Watnick and T Dirkx ldquoKidney diseaserdquo in Current MedicalDiagnosis amp Treatment 2015 M A Papadakis S J McPhee andM W Rabow Eds McGraw-Hill New York NY USA 2014
[4] J C Jennette J L Olson M M Schwartz and F G SilvaldquoPauci-immune and ANCA-mediated crescentic glomeru-lonephritis and vasculitisrdquo in Heptinstallrsquos Pathology of theKidney vol 1 chapter 14 6th edition 2007
[5] P Seo and J H Stone ldquoThe antineutrophil cytoplasmicantibody-associated vasculitidesrdquo The American Journal ofMedicine vol 117 no 1 pp 39ndash50 2004
[6] U Eisenberger F Fakhouri P Vanhille et al ldquoANCA-negative pauci-immune renal vasculitis histology and out-comerdquo Nephrology Dialysis Transplantation vol 20 no 7 pp1392ndash1399 2005
[7] M Haas and J A Eustace ldquoImmune complex deposits inANCA-associated crescentic glomerulonephritis a study of 126casesrdquo Kidney International vol 65 no 6 pp 2145ndash2152 2004
[8] J B Levy T Hammad A Coulthart T Dougan and C DPusey ldquoClinical features and outcome of patients with bothANCA and anti-GBMantibodiesrdquoKidney International vol 66no 4 pp 1535ndash1540 2004
[9] N Kambham ldquoCrescentic glomerulonephritis an update onpauci-immune and anti-GBM diseasesrdquo Advances in AnatomicPathology vol 19 no 2 pp 111ndash124 2012
[10] F Ferrario A Vanzati and F Pagni ldquoPathology of ANCA-associated vasculitisrdquo Clinical and Experimental Nephrologyvol 17 no 5 pp 652ndash658 2013
[11] A E Berden F Ferrario E C Hagen et al ldquoHistopathologicclassification of ANCA-associated glomerulonephritisrdquo Journalof the American Society of Nephrology vol 21 no 10 pp 1628ndash1636 2010
[12] S L Ford K R Polkinghorne A Longano et al ldquoHistopatho-logic and clinical predictors of kidney outcomes in ANCA-associated vasculitisrdquo American Journal of Kidney Diseases vol63 no 2 pp 227ndash235 2014
[13] T Iwakiri S Fujimoto K Kitagawa et al ldquoValidation of anewly proposed histopathological classification in Japanesepatients with anti-neutrophil cytoplasmic antibody-associatedglomerulonephritisrdquo BMC Nephrology vol 14 article 125 2013
[14] E Nohr L Girard M James and H Benediktsson ldquoValidationof a histopathologic classification scheme for antineutrophilcytoplasmic antibody-associated glomerulonephritisrdquo HumanPathology vol 45 no 7 pp 1423ndash1429 2014
[15] D-Y Chang L-H Wu G Liu M Chen C G M Kallenbergand M-H Zhao ldquoRe-evaluation of the histopathologic classifi-cation of ANCA-associated glomerulonephritis a study of 121patients in a single centerrdquoNephrology Dialysis Transplantationvol 27 no 6 pp 2343ndash2349 2012
[16] M El-Ters U Muthyala M D Philipneri F A Hussein andK L Lentine ldquoImmune-complex deposits in lsquopauci-immunersquoglomerulonephritis a case report and brief review of recentliteraturerdquoArchives of Medical Science vol 6 no 4 pp 633ndash6372010
[17] I Neumann H Regele R Kain R Birck and F T MeislldquoGlomerular immune deposits are associated with increasedproteinuria in patients with ANCA-associated crescenticnephritisrdquo Nephrology Dialysis Transplantation vol 18 no 3pp 524ndash531 2003
[18] E Brouwer M G Huitema P A Klok et al ldquoAntimye-loperoxidase-associated proliferative glomerulonephritis ananimal modelrdquo Journal of Experimental Medicine vol 177 no4 pp 905ndash914 1993
[19] J J Yang J C Jennette and R J Falk ldquoImmune complexglomerulonephritis is induced in rats immunizedwith heterolo-gous myeloperoxidaserdquo Clinical and Experimental Immunologyvol 97 no 3 pp 466ndash473 1994
[20] M Haas J Jafri S M Bartosh S L Karp S G Adler and S MMeehan ldquoANCA-associated crescentic glomerulonephritis withmesangial IgA depositsrdquo American Journal of Kidney Diseasesvol 36 no 4 pp 709ndash718 2000
[21] M Haas ldquoIncidental healed postinfectious glomerulonephritisa study of 1012 renal biopsy specimens examined by electronmicroscopyrdquo Human Pathology vol 34 no 1 pp 3ndash10 2003
[22] R Jimbo Y Ubara T Tagami et al ldquoA pediatric occurrenceof crescentic glomerulonephritis associated with antineutrophilcytoplasmic antibodies and mesangial IgA depositsrdquo ClinicalNephrology vol 68 no 2 pp 104ndash108 2007
[23] J C Jennette ldquoRapidly progressive crescentic glomerulonephri-tisrdquo Kidney International vol 63 no 3 pp 1164ndash1177 2003
[24] P J Bansal andM C Tobin ldquoNeonatal microscopic polyangiitissecondary to transfer of maternal myeloperoxidase-antineutrophil cytoplasmic antibody resulting in neonatalpulmonary hemorrhage and renal involvementrdquo Annals ofAllergy Asthma and Immunology vol 93 no 4 pp 398ndash4012004
[25] H Xiao P Heeringa P Hu et al ldquoAntineutrophil cytoplasmicautoantibodies specific for myeloperoxidase cause glomeru-lonephritis and vasculitis in micerdquo Journal of Clinical Investiga-tion vol 110 no 7 pp 955ndash963 2002
[26] C G M Kallenberg ldquoPathogenesis of ANCA-associated vas-culitis an updaterdquo Clinical Reviews in Allergy and Immunologyvol 41 no 2 pp 224ndash231 2011
[27] H Pfister M Ollert L F Frohlich et al ldquoAntineutrophilcytoplasmic autoantibodies against the murine homolog ofproteinase 3 (Wegener autoantigen) are pathogenic in vivordquoBlood vol 104 no 5 pp 1411ndash1418 2004
[28] R J Falk R S Terrell L A Charles and J C Jennette ldquoAnti-neutrophil cytoplasmic autoantibodies induce neutrophils todegranulate and produce oxygen radicals in vitrordquo Proceedingsof the National Academy of Sciences of the United States ofAmerica vol 87 no 11 pp 4115ndash4119 1990
[29] L A Charles M L R Caldas R J Falk R S Terrell andJ C Jennette ldquoAntibodies against granule proteins activateneutrophils in vitrordquo Journal of Leukocyte Biology vol 50 no6 pp 539ndash546 1991
[30] A J Porges P B Redecha W T Kimberly E Csernok W LGross and R P Kimberly ldquoAnti-neutrophil cytoplasmic anti-bodies engage and activate human neutrophils via Fc gammaRIIardquoThe Journal of Immunology vol 153 no 3 pp 1271ndash12801994
[31] A H Mulder P Heeringa E Brouwer P C Limburg and CG Kallenberg ldquoActivation of granulocytes by anti-neutrophilcytoplasmic antibodies (ANCA) a Fc gamma RII-dependentprocessrdquoClinical amp Experimental Immunology vol 98 no 2 pp270ndash278 1994
BioMed Research International 7
[32] R Kettritz J C Jennette andR J Falk ldquoCrosslinking of ANCA-antigens stimulates superoxide release by human neutrophilsrdquoJournal of the American Society of Nephrology vol 8 no 3 pp386ndash394 1997
[33] B H Ewert J C Jennette and R J Falk ldquoAnti-myeloperoxidaseantibodies stimulate neutrophils to damage human endothelialcellsrdquo Kidney International vol 41 no 2 pp 375ndash383 1992
[34] K Kessenbrock M Krumbholz U Schonermarck et al ldquoNet-ting neutrophils in autoimmune small-vessel vasculitisrdquoNatureMedicine vol 15 no 6 pp 623ndash625 2009
[35] A K Gupta M B Joshi M Philippova et al ldquoActivatedendothelial cells induce neutrophil extracellular traps and aresusceptible to NETosis-mediated cell deathrdquo FEBS Letters vol584 no 14 pp 3193ndash3197 2010
[36] O O Rowaiye M Kusztal and M Klinger ldquoThe kidneys andANCA-associated vasculitis from pathogenesis to diagnosisrdquoClinical Kidney Journal vol 8 no 3 pp 343ndash350 2015
[37] H Xiao A Schreiber P Heeringa R J Falk and J C JennetteldquoAlternative complement pathway in the pathogenesis of dis-ease mediated by anti-neutrophil cytoplasmic autoantibodiesrdquoAmerican Journal of Pathology vol 170 no 1 pp 52ndash64 2007
[38] U Schonermarck E Csernok and W L Gross ldquoPathogenesisof anti-neutrophil cytoplasmic antibody-associated vasculitischallenges and solutions 2014rdquo Nephrology Dialysis Transplan-tation vol 30 supplement 1 pp i46ndashi52 2015
[39] C Franssen R Gans C Kallenberg C Hageluken and SHoorntje ldquoDisease spectrum of patients with antineutrophilcytoplasmic autoantibodies of defined specificity distinct dif-ferences between patients with anti-proteinase 3 and anti-myeloperoxidase autoantibodiesrdquo Journal of Internal Medicinevol 244 no 3 pp 209ndash216 1998
[40] R Kain M Exner R Brandes et al ldquoMolecular mimicry inpauci-immune focal necrotizing glomerulonephritisrdquo NatureMedicine vol 14 no 10 pp 1088ndash1096 2008
[41] R Kain H Tadema E F McKinney et al ldquoHigh prevalenceof autoantibodies to hLAMP-2 in anti-neutrophil cytoplasmicantibody-associated vasculitisrdquo Journal of the American Societyof Nephrology vol 23 no 3 pp 556ndash566 2012
[42] A J Roth M C Brown R N Smith et al ldquoAnti-LAMP-2antibodies are not prevalent in patients with antineutrophilcytoplasmic autoantibody glomerulonephritisrdquo Journal of theAmerican Society of Nephrology vol 23 no 3 pp 545ndash555 2012
[43] R Kain and A J Rees ldquoWhat is the evidence for antibodies toLAMP-2 in the pathogenesis of ANCA associated small vesselvasculitisrdquo Current Opinion in Rheumatology vol 25 no 1 pp26ndash34 2013
[44] J Hao C Wang S-J Gou M-H Zhao and M Chen ldquoTheassociation between anti-plasminogen antibodies and diseaseactivity in ANCA-associated vasculitisrdquo Rheumatology vol 53no 2 pp 300ndash306 2014
[45] A E Berden S L Nolan H L Morris et al ldquoAnti-plasminogenantibodies compromise fibrinolysis and associatewith renal his-tology in ANCA-associated vasculitisrdquo Journal of the AmericanSociety of Nephrology vol 21 no 12 pp 2169ndash2179 2010
[46] C A Stegeman J W Cohen Tervaert W J Sluiter W LManson P E De Jong and C G M Kallenberg ldquoAssociationof chronic nasal carriage of Staphylococcus aureus and higherrelapse rates in Wegener granulomatosisrdquo Annals of InternalMedicine vol 120 no 1 pp 12ndash17 1994
[47] K Zycinska K A Wardyn T M Zielonka R Krupa andW Lukas ldquoCo-trimoxazole and prevention of relapses of PR3-ANCA positive vasculitis with pulmonary involvementrdquo Euro-pean Journal ofMedical Research vol 14 supplement 4 pp 265ndash267 2009
[48] A D Salama and C D Pusey ldquoShining a LAMP on pauci-immune focal segmental glomerulonephritisrdquo Kidney Interna-tional vol 76 no 1 pp 15ndash17 2009
[49] MMVanTimmeren andPHeeringa ldquoPathogenesis ofANCA-associated vasculitis recent insights from animal modelsrdquoCurrent Opinion in Rheumatology vol 24 no 1 pp 8ndash14 2012
[50] A M Coughlan S J Freeley and M G Robson ldquoAnimalmodels of anti-neutrophil cytoplasmic antibody-associated vas-culitisrdquo Clinical and Experimental Immunology vol 169 no 3pp 229ndash237 2012
[51] S L Hogan K K Satterly M A Dooley P H Nachman JC Jennette and R J Falk ldquoSilica exposure in anti-neutrophilcytoplasmic autoantibody-associated glomerulonephritis andlupus nephritisrdquo Journal of the American Society of Nephrologyvol 12 no 1 pp 134ndash142 2001
[52] Z Rihova D Maixnerova E Jancova et al ldquoSilica andasbestos exposure in ANCA-associated vasculitis with pul-monary involvementrdquo Renal Failure vol 27 no 5 pp 605ndash6082005
[53] T Kanda H Tanio CWu H Nishihara F Nogaki and T OnoldquoChurg-Strauss syndrome with severe granulomatous angiitisand crescentic glomerulonephritis which developed duringtherapy with a leukotriene receptor antagonistrdquo Clinical andExperimental Nephrology vol 14 no 6 pp 602ndash607 2010
[54] M Suneja S Baiswar and S A Vogelgesang ldquoHydralazineassociated pauci-immune glomerulonephritisrdquo Journal of Clin-ical Rheumatology vol 20 no 2 pp 99ndash102 2014
[55] S Morita Y Ueda and K Eguchi ldquoAnti-thyroid drug-inducedANCA-associated vasculitis a case report and review of theliteraturerdquo Endocrine Journal vol 47 no 4 pp 467ndash470 2000
[56] H K Choi P A Merkel A M Walker and J L NilesldquoDrug-associated antineutrophil cytoplasmic antibody-positivevasculitis prevalence among patients with high titers ofantimyeloperoxidase antibodiesrdquo Arthritis and Rheumatismvol 43 no 2 pp 405ndash413 2000
[57] J C Jennette R J Falk and A H Gasim ldquoPathogenesis ofantineutrophil cytoplasmic autoantibody vasculitisrdquo CurrentOpinion in Nephrology andHypertension vol 20 no 3 pp 263ndash270 2011
[58] W F Pendergraft III G A Preston R R Shah et al ldquoAutoim-munity is triggered by cPR-3(105ndash201) a protein complemen-tary to human autoantigen proteinase-3rdquo Nature Medicine vol10 no 1 pp 72ndash79 2004
[59] P Hewins F Belmonte J C Jennette R J Falk and G APreston ldquoLongitudinal studies of patients with ANCA vasculi-tis demonstrate concurrent reactivity to complementary PR3protein segments cPR3m and cPR3C and with no reactivity tocPR3Nrdquo Autoimmunity vol 44 no 2 pp 98ndash106 2011
[60] P A Lyons T F Rayner S Trivedi et al ldquoGenetically distinctsubsets within ANCA-associated vasculitisrdquo The New EnglandJournal of Medicine vol 367 no 3 pp 214ndash223 2012
[61] G Xie D Roshandel R Sherva et al ldquoAssociation of granulo-matosis with polyangiitis (Wegenerrsquos) with HLA-DPB1lowast04 andSEMA6A gene variants evidence from genome-wide analysisrdquoArthritis amp Rheumatism vol 65 no 9 pp 2457ndash2468 2013
[62] V Witko-Sarsat P Lesavre S Lopez et al ldquoA large subset ofneutrophils expressing membrane proteinase 3 is a risk factor
8 BioMed Research International
for vasculitis and rheumatoid arthritisrdquo Journal of the AmericanSociety of Nephrology vol 10 no 6 pp 1224ndash1233 1999
[63] P Jagiello P Aries L Arning et al ldquoThe PTPN22 620W alleleis a risk factor for Wegenerrsquos granulomatosisrdquo Arthritis andRheumatism vol 52 no 12 pp 4039ndash4043 2005
[64] D Martorana F Maritati G Malerba et al ldquoPTPN22 R620Wpolymorphism in the ANCA-associated vasculitidesrdquo Rheuma-tology vol 51 no 5 Article ID ker446 pp 805ndash812 2012
[65] R Giscombe X Wang D Huang and A K Lefvert ldquoCodingsequence 1 and promoter single nucleotide polymorphismsin the CTLA-4 gene in Wegenerrsquos granulomatosisrdquo Journal ofRheumatology vol 29 no 5 pp 950ndash953 2002
[66] P Lamprecht S Wieczorek J T Epplen P Ambrosch and CG M Kallenberg ldquoGranuloma formation in ANCA-associatedvasculitidesrdquo APMIS vol 117 supplement s127 no 127 pp 32ndash36 2009
[67] M D Morgan C J Day K P Piper et al ldquoPatients withWegenerrsquos granulomatosis demonstrate a relative deficiency andfunctional impairment of T-regulatory cellsrdquo Immunology vol130 no 1 pp 64ndash73 2010
[68] M E Free D O Bunch J A McGregor et al ldquoPatients withantineutrophil cytoplasmic antibody-associated vasculitis havedefective Treg cell function exacerbated by the presence ofa suppression-resistant effector cell populationrdquo Arthritis andRheumatism vol 65 no 7 pp 1922ndash1933 2013
[69] B Wilde M Thewissen J Damoiseaux et al ldquoRegulatory Bcells in ANCA-associated vasculitisrdquo Annals of the RheumaticDiseases vol 72 no 8 pp 1416ndash1419 2013
[70] N Kesel D Khler L Herich et al ldquoCartilage destruction ingranulomatosis with polyangiitis (Wegenerrsquos granulomatosis)is mediated by human fibroblasts after transplantation intoimmunodeficientmicerdquoTheAmerican Journal of Pathology vol180 no 5 pp 2144ndash2155 2012
[71] C Rahmattulla R A de Lind van Wijngaarden A E Berdenet al ldquoRenal function and ear nose throat involvement in anti-neutrophil cytoplasmic antibody-associated vasculitis prospec-tive data from the European Vasculitis Society clinical trialsrdquoRheumatology vol 54 no 5 pp 899ndash907 2015
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
with other variants involved in AAV such as those belongingto the CTLA-4 and PTPN22 genes These results have not yetbeen replicated in larger studies [63ndash65]
Also it is important to discuss the role of T cell mediatedimmune response in PICG It is widely known that CD4+helper T cells with interferon-gamma secretion are involvedin granuloma formation Granulomas are seen mainly inPR3 AAV and not in MPO AAV TH17 cells play a majorrole in causing granulomatous inflammation and vascularinjury in PR3 AAV [66] Morgan et al have also showndiminished number and functional impairment of regulatoryT cells (Tregs) inGPA [67] Finally according to some studiespatients with ANCA-mediated vasculitis have impaired func-tioning of Tregs alongwith the presence of effector T cells thatare resistant to suppression by Tregs [68]
In addition to autoantibody production B cells also havethe ability to present antigens to T cells and may modulateT cell responses in small vessel vasculitis Regulatory B cells(Bregs) are a distinct B cell subset cells that regulate theaction of the T cell population by secreting IL-10 Wilde etal demonstrated that there is a reduction in the numberof Bregs in both active and quiescent AAV [69] The studyalso revealed a positive correlation between Breg and Treg inquiescent AAV and that Th1 cell suppression by Breg may beinadequate in active AAV
Recently the pathogenic mechanisms of tissue damagein GPA resulting in saddle nose deformity and orbitaldestruction have been further elucidated [38 70] Fibroblastslining bone and cartilage have been acknowledged to playthe role of activated effector cells of tissue destruction inGPA In the first in vivo model of GPA Kesel et al subcu-taneously coimplanted the biopsy specimens from patientswith activeGPAor sinusitis (controls) with healthy allogeneichuman nasal cartilage into immunodeficient mice [70] GPAimplants showed massive destruction of the coimplantedhuman cartilage whereas cartilage destruction was onlymarginal in control samples Further cartilage destructionwas mediated by human fibroblasts and could be controlledsimilar to GPA in humans with corticosteroids In additionin fibrotic lung disease NETs were shown to promote differ-entiation and function of fibroblasts indicating that NETs areinvolved not only in inflammation but also in the resultingfibrosis [38 71]
6 Clinical Manifestations and Natural History
Notwithstanding a slightly higher specificity ANCA is topauci-immune RPGN as anti-DNA is to systemic lupuserythematosus Microscopic polyangiitis (MPA) granulo-matosis with polyangiitis (GPA) eosinophilic granulomatosiswith polyangiitis (EGPA or Churg-Strauss syndrome) andrenal-limited pauci-immune crescentic GN (PICG) are allassociated with ANCA The term ldquopauci-immunerdquo RPGNencapsulates all of these conditions Generalized nonspecificmanifestations of systemic inflammatory disease such asfever malaise anorexia weight loss myalgia and arthralgiacan be seen in any of these diseases The clinical manifesta-tions of each entity vary based on the chronicity and sitesof involvement Patients without systemic involvement may
present later in the course of their disease Granulomatousinvolvement particularly of the upper respiratory tract is acharacteristic feature of GPA but not of MPA eosinophiliaasthma and atopy typically occur in EGPA In each of theseconditions patients can have pulmonary hemorrhage causedby hemorrhagic alveolar capillaritis which has treatmentand prognostic implications [2] As mentioned previouslythe renal failure seen in PICG usually presents clinicallyas RPGN It should be noted though that patients withGPA or MPA could also present with subacute or chronicnephritis In one study assessing the clinical characteristicsof pauci-immune crescentic GN a cohort of more than 300patients evaluated at renal biopsy had a mean age of 56 plusmn 20years (range 2 to 92 years) male-to-female ratio of 10 09mean serum creatinine concentration of 65 plusmn 40mgdL(range 08 to 221mgdL) and proteinuria of 19 plusmn 30 gday(range 01 to 18 gday) [2] Older age higher serum creatinineconcentration at presentation pulmonary hemorrhage anddialysis-dependent renal failure correlate with an overallpoor prognosis Respiratory tract disease and PR3-ANCAare predictors of higher relapse rates [2] Regardless of thecategory of ANCA disease though the best clinical predictorof renal outcome is the glomerular filtration rate (GFR)at the time of diagnosis [1] Interestingly in one of therecent studies the presence of ear nose and throat (ENT)involvement in AAV patients was found to be associatedwith lesser degree of interstitial fibrosis and tubular atrophyon kidney biopsy and better renal function These resultsindicate that there may be different phenotypes of AAVdefined by ENT involvement [71]
7 Conclusion
Despite significant advances in our understanding of theimmune system issues of incomplete efficacy treatmenttoxicity and infectious complications persist With targetedapproaches to immunosuppression andnewer biologic agentsmodulating B and T cell function the future holds promisein terms of greater treatment efficacy with an improved sideeffect profile We believe that future studies will highlight theintricacies of the clinical and pathological spectrum of PICGwhile proposing novel mechanisms for inducing and main-taining remission Based on current guidelines for patientsin complete remission and without extrarenal manifestationsfor at least 12 months renal transplant should not be delayedANCA positivity is not considered a contraindication fortransplantation However no prospective data are availableto assess the likelihood of recurrent ANCA vasculitis afterkidney transplantation In addition the impact of diseaseactivity or ANCA positivity at the time of transplantationon patient outcome is unclear Future studies must bedesigned to gather prospective data that helps answer thesequestions
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
6 BioMed Research International
References
[1] R J Glassock S G Adler H JWard et al ldquoPrimary glomerulardiseasesrdquo inTheKidney BM Brenner and F C Rector Eds pp1182ndash1279 Saunders Philadelphia Pa USA 4th edition 1991
[2] J Charles Jennette R J Falk and J G McGregor ldquoRenaland systemic valculitisrdquo in Comprehensive Clinical NephrologyElsevier 5th edition 2015
[3] S Watnick and T Dirkx ldquoKidney diseaserdquo in Current MedicalDiagnosis amp Treatment 2015 M A Papadakis S J McPhee andM W Rabow Eds McGraw-Hill New York NY USA 2014
[4] J C Jennette J L Olson M M Schwartz and F G SilvaldquoPauci-immune and ANCA-mediated crescentic glomeru-lonephritis and vasculitisrdquo in Heptinstallrsquos Pathology of theKidney vol 1 chapter 14 6th edition 2007
[5] P Seo and J H Stone ldquoThe antineutrophil cytoplasmicantibody-associated vasculitidesrdquo The American Journal ofMedicine vol 117 no 1 pp 39ndash50 2004
[6] U Eisenberger F Fakhouri P Vanhille et al ldquoANCA-negative pauci-immune renal vasculitis histology and out-comerdquo Nephrology Dialysis Transplantation vol 20 no 7 pp1392ndash1399 2005
[7] M Haas and J A Eustace ldquoImmune complex deposits inANCA-associated crescentic glomerulonephritis a study of 126casesrdquo Kidney International vol 65 no 6 pp 2145ndash2152 2004
[8] J B Levy T Hammad A Coulthart T Dougan and C DPusey ldquoClinical features and outcome of patients with bothANCA and anti-GBMantibodiesrdquoKidney International vol 66no 4 pp 1535ndash1540 2004
[9] N Kambham ldquoCrescentic glomerulonephritis an update onpauci-immune and anti-GBM diseasesrdquo Advances in AnatomicPathology vol 19 no 2 pp 111ndash124 2012
[10] F Ferrario A Vanzati and F Pagni ldquoPathology of ANCA-associated vasculitisrdquo Clinical and Experimental Nephrologyvol 17 no 5 pp 652ndash658 2013
[11] A E Berden F Ferrario E C Hagen et al ldquoHistopathologicclassification of ANCA-associated glomerulonephritisrdquo Journalof the American Society of Nephrology vol 21 no 10 pp 1628ndash1636 2010
[12] S L Ford K R Polkinghorne A Longano et al ldquoHistopatho-logic and clinical predictors of kidney outcomes in ANCA-associated vasculitisrdquo American Journal of Kidney Diseases vol63 no 2 pp 227ndash235 2014
[13] T Iwakiri S Fujimoto K Kitagawa et al ldquoValidation of anewly proposed histopathological classification in Japanesepatients with anti-neutrophil cytoplasmic antibody-associatedglomerulonephritisrdquo BMC Nephrology vol 14 article 125 2013
[14] E Nohr L Girard M James and H Benediktsson ldquoValidationof a histopathologic classification scheme for antineutrophilcytoplasmic antibody-associated glomerulonephritisrdquo HumanPathology vol 45 no 7 pp 1423ndash1429 2014
[15] D-Y Chang L-H Wu G Liu M Chen C G M Kallenbergand M-H Zhao ldquoRe-evaluation of the histopathologic classifi-cation of ANCA-associated glomerulonephritis a study of 121patients in a single centerrdquoNephrology Dialysis Transplantationvol 27 no 6 pp 2343ndash2349 2012
[16] M El-Ters U Muthyala M D Philipneri F A Hussein andK L Lentine ldquoImmune-complex deposits in lsquopauci-immunersquoglomerulonephritis a case report and brief review of recentliteraturerdquoArchives of Medical Science vol 6 no 4 pp 633ndash6372010
[17] I Neumann H Regele R Kain R Birck and F T MeislldquoGlomerular immune deposits are associated with increasedproteinuria in patients with ANCA-associated crescenticnephritisrdquo Nephrology Dialysis Transplantation vol 18 no 3pp 524ndash531 2003
[18] E Brouwer M G Huitema P A Klok et al ldquoAntimye-loperoxidase-associated proliferative glomerulonephritis ananimal modelrdquo Journal of Experimental Medicine vol 177 no4 pp 905ndash914 1993
[19] J J Yang J C Jennette and R J Falk ldquoImmune complexglomerulonephritis is induced in rats immunizedwith heterolo-gous myeloperoxidaserdquo Clinical and Experimental Immunologyvol 97 no 3 pp 466ndash473 1994
[20] M Haas J Jafri S M Bartosh S L Karp S G Adler and S MMeehan ldquoANCA-associated crescentic glomerulonephritis withmesangial IgA depositsrdquo American Journal of Kidney Diseasesvol 36 no 4 pp 709ndash718 2000
[21] M Haas ldquoIncidental healed postinfectious glomerulonephritisa study of 1012 renal biopsy specimens examined by electronmicroscopyrdquo Human Pathology vol 34 no 1 pp 3ndash10 2003
[22] R Jimbo Y Ubara T Tagami et al ldquoA pediatric occurrenceof crescentic glomerulonephritis associated with antineutrophilcytoplasmic antibodies and mesangial IgA depositsrdquo ClinicalNephrology vol 68 no 2 pp 104ndash108 2007
[23] J C Jennette ldquoRapidly progressive crescentic glomerulonephri-tisrdquo Kidney International vol 63 no 3 pp 1164ndash1177 2003
[24] P J Bansal andM C Tobin ldquoNeonatal microscopic polyangiitissecondary to transfer of maternal myeloperoxidase-antineutrophil cytoplasmic antibody resulting in neonatalpulmonary hemorrhage and renal involvementrdquo Annals ofAllergy Asthma and Immunology vol 93 no 4 pp 398ndash4012004
[25] H Xiao P Heeringa P Hu et al ldquoAntineutrophil cytoplasmicautoantibodies specific for myeloperoxidase cause glomeru-lonephritis and vasculitis in micerdquo Journal of Clinical Investiga-tion vol 110 no 7 pp 955ndash963 2002
[26] C G M Kallenberg ldquoPathogenesis of ANCA-associated vas-culitis an updaterdquo Clinical Reviews in Allergy and Immunologyvol 41 no 2 pp 224ndash231 2011
[27] H Pfister M Ollert L F Frohlich et al ldquoAntineutrophilcytoplasmic autoantibodies against the murine homolog ofproteinase 3 (Wegener autoantigen) are pathogenic in vivordquoBlood vol 104 no 5 pp 1411ndash1418 2004
[28] R J Falk R S Terrell L A Charles and J C Jennette ldquoAnti-neutrophil cytoplasmic autoantibodies induce neutrophils todegranulate and produce oxygen radicals in vitrordquo Proceedingsof the National Academy of Sciences of the United States ofAmerica vol 87 no 11 pp 4115ndash4119 1990
[29] L A Charles M L R Caldas R J Falk R S Terrell andJ C Jennette ldquoAntibodies against granule proteins activateneutrophils in vitrordquo Journal of Leukocyte Biology vol 50 no6 pp 539ndash546 1991
[30] A J Porges P B Redecha W T Kimberly E Csernok W LGross and R P Kimberly ldquoAnti-neutrophil cytoplasmic anti-bodies engage and activate human neutrophils via Fc gammaRIIardquoThe Journal of Immunology vol 153 no 3 pp 1271ndash12801994
[31] A H Mulder P Heeringa E Brouwer P C Limburg and CG Kallenberg ldquoActivation of granulocytes by anti-neutrophilcytoplasmic antibodies (ANCA) a Fc gamma RII-dependentprocessrdquoClinical amp Experimental Immunology vol 98 no 2 pp270ndash278 1994
BioMed Research International 7
[32] R Kettritz J C Jennette andR J Falk ldquoCrosslinking of ANCA-antigens stimulates superoxide release by human neutrophilsrdquoJournal of the American Society of Nephrology vol 8 no 3 pp386ndash394 1997
[33] B H Ewert J C Jennette and R J Falk ldquoAnti-myeloperoxidaseantibodies stimulate neutrophils to damage human endothelialcellsrdquo Kidney International vol 41 no 2 pp 375ndash383 1992
[34] K Kessenbrock M Krumbholz U Schonermarck et al ldquoNet-ting neutrophils in autoimmune small-vessel vasculitisrdquoNatureMedicine vol 15 no 6 pp 623ndash625 2009
[35] A K Gupta M B Joshi M Philippova et al ldquoActivatedendothelial cells induce neutrophil extracellular traps and aresusceptible to NETosis-mediated cell deathrdquo FEBS Letters vol584 no 14 pp 3193ndash3197 2010
[36] O O Rowaiye M Kusztal and M Klinger ldquoThe kidneys andANCA-associated vasculitis from pathogenesis to diagnosisrdquoClinical Kidney Journal vol 8 no 3 pp 343ndash350 2015
[37] H Xiao A Schreiber P Heeringa R J Falk and J C JennetteldquoAlternative complement pathway in the pathogenesis of dis-ease mediated by anti-neutrophil cytoplasmic autoantibodiesrdquoAmerican Journal of Pathology vol 170 no 1 pp 52ndash64 2007
[38] U Schonermarck E Csernok and W L Gross ldquoPathogenesisof anti-neutrophil cytoplasmic antibody-associated vasculitischallenges and solutions 2014rdquo Nephrology Dialysis Transplan-tation vol 30 supplement 1 pp i46ndashi52 2015
[39] C Franssen R Gans C Kallenberg C Hageluken and SHoorntje ldquoDisease spectrum of patients with antineutrophilcytoplasmic autoantibodies of defined specificity distinct dif-ferences between patients with anti-proteinase 3 and anti-myeloperoxidase autoantibodiesrdquo Journal of Internal Medicinevol 244 no 3 pp 209ndash216 1998
[40] R Kain M Exner R Brandes et al ldquoMolecular mimicry inpauci-immune focal necrotizing glomerulonephritisrdquo NatureMedicine vol 14 no 10 pp 1088ndash1096 2008
[41] R Kain H Tadema E F McKinney et al ldquoHigh prevalenceof autoantibodies to hLAMP-2 in anti-neutrophil cytoplasmicantibody-associated vasculitisrdquo Journal of the American Societyof Nephrology vol 23 no 3 pp 556ndash566 2012
[42] A J Roth M C Brown R N Smith et al ldquoAnti-LAMP-2antibodies are not prevalent in patients with antineutrophilcytoplasmic autoantibody glomerulonephritisrdquo Journal of theAmerican Society of Nephrology vol 23 no 3 pp 545ndash555 2012
[43] R Kain and A J Rees ldquoWhat is the evidence for antibodies toLAMP-2 in the pathogenesis of ANCA associated small vesselvasculitisrdquo Current Opinion in Rheumatology vol 25 no 1 pp26ndash34 2013
[44] J Hao C Wang S-J Gou M-H Zhao and M Chen ldquoTheassociation between anti-plasminogen antibodies and diseaseactivity in ANCA-associated vasculitisrdquo Rheumatology vol 53no 2 pp 300ndash306 2014
[45] A E Berden S L Nolan H L Morris et al ldquoAnti-plasminogenantibodies compromise fibrinolysis and associatewith renal his-tology in ANCA-associated vasculitisrdquo Journal of the AmericanSociety of Nephrology vol 21 no 12 pp 2169ndash2179 2010
[46] C A Stegeman J W Cohen Tervaert W J Sluiter W LManson P E De Jong and C G M Kallenberg ldquoAssociationof chronic nasal carriage of Staphylococcus aureus and higherrelapse rates in Wegener granulomatosisrdquo Annals of InternalMedicine vol 120 no 1 pp 12ndash17 1994
[47] K Zycinska K A Wardyn T M Zielonka R Krupa andW Lukas ldquoCo-trimoxazole and prevention of relapses of PR3-ANCA positive vasculitis with pulmonary involvementrdquo Euro-pean Journal ofMedical Research vol 14 supplement 4 pp 265ndash267 2009
[48] A D Salama and C D Pusey ldquoShining a LAMP on pauci-immune focal segmental glomerulonephritisrdquo Kidney Interna-tional vol 76 no 1 pp 15ndash17 2009
[49] MMVanTimmeren andPHeeringa ldquoPathogenesis ofANCA-associated vasculitis recent insights from animal modelsrdquoCurrent Opinion in Rheumatology vol 24 no 1 pp 8ndash14 2012
[50] A M Coughlan S J Freeley and M G Robson ldquoAnimalmodels of anti-neutrophil cytoplasmic antibody-associated vas-culitisrdquo Clinical and Experimental Immunology vol 169 no 3pp 229ndash237 2012
[51] S L Hogan K K Satterly M A Dooley P H Nachman JC Jennette and R J Falk ldquoSilica exposure in anti-neutrophilcytoplasmic autoantibody-associated glomerulonephritis andlupus nephritisrdquo Journal of the American Society of Nephrologyvol 12 no 1 pp 134ndash142 2001
[52] Z Rihova D Maixnerova E Jancova et al ldquoSilica andasbestos exposure in ANCA-associated vasculitis with pul-monary involvementrdquo Renal Failure vol 27 no 5 pp 605ndash6082005
[53] T Kanda H Tanio CWu H Nishihara F Nogaki and T OnoldquoChurg-Strauss syndrome with severe granulomatous angiitisand crescentic glomerulonephritis which developed duringtherapy with a leukotriene receptor antagonistrdquo Clinical andExperimental Nephrology vol 14 no 6 pp 602ndash607 2010
[54] M Suneja S Baiswar and S A Vogelgesang ldquoHydralazineassociated pauci-immune glomerulonephritisrdquo Journal of Clin-ical Rheumatology vol 20 no 2 pp 99ndash102 2014
[55] S Morita Y Ueda and K Eguchi ldquoAnti-thyroid drug-inducedANCA-associated vasculitis a case report and review of theliteraturerdquo Endocrine Journal vol 47 no 4 pp 467ndash470 2000
[56] H K Choi P A Merkel A M Walker and J L NilesldquoDrug-associated antineutrophil cytoplasmic antibody-positivevasculitis prevalence among patients with high titers ofantimyeloperoxidase antibodiesrdquo Arthritis and Rheumatismvol 43 no 2 pp 405ndash413 2000
[57] J C Jennette R J Falk and A H Gasim ldquoPathogenesis ofantineutrophil cytoplasmic autoantibody vasculitisrdquo CurrentOpinion in Nephrology andHypertension vol 20 no 3 pp 263ndash270 2011
[58] W F Pendergraft III G A Preston R R Shah et al ldquoAutoim-munity is triggered by cPR-3(105ndash201) a protein complemen-tary to human autoantigen proteinase-3rdquo Nature Medicine vol10 no 1 pp 72ndash79 2004
[59] P Hewins F Belmonte J C Jennette R J Falk and G APreston ldquoLongitudinal studies of patients with ANCA vasculi-tis demonstrate concurrent reactivity to complementary PR3protein segments cPR3m and cPR3C and with no reactivity tocPR3Nrdquo Autoimmunity vol 44 no 2 pp 98ndash106 2011
[60] P A Lyons T F Rayner S Trivedi et al ldquoGenetically distinctsubsets within ANCA-associated vasculitisrdquo The New EnglandJournal of Medicine vol 367 no 3 pp 214ndash223 2012
[61] G Xie D Roshandel R Sherva et al ldquoAssociation of granulo-matosis with polyangiitis (Wegenerrsquos) with HLA-DPB1lowast04 andSEMA6A gene variants evidence from genome-wide analysisrdquoArthritis amp Rheumatism vol 65 no 9 pp 2457ndash2468 2013
[62] V Witko-Sarsat P Lesavre S Lopez et al ldquoA large subset ofneutrophils expressing membrane proteinase 3 is a risk factor
8 BioMed Research International
for vasculitis and rheumatoid arthritisrdquo Journal of the AmericanSociety of Nephrology vol 10 no 6 pp 1224ndash1233 1999
[63] P Jagiello P Aries L Arning et al ldquoThe PTPN22 620W alleleis a risk factor for Wegenerrsquos granulomatosisrdquo Arthritis andRheumatism vol 52 no 12 pp 4039ndash4043 2005
[64] D Martorana F Maritati G Malerba et al ldquoPTPN22 R620Wpolymorphism in the ANCA-associated vasculitidesrdquo Rheuma-tology vol 51 no 5 Article ID ker446 pp 805ndash812 2012
[65] R Giscombe X Wang D Huang and A K Lefvert ldquoCodingsequence 1 and promoter single nucleotide polymorphismsin the CTLA-4 gene in Wegenerrsquos granulomatosisrdquo Journal ofRheumatology vol 29 no 5 pp 950ndash953 2002
[66] P Lamprecht S Wieczorek J T Epplen P Ambrosch and CG M Kallenberg ldquoGranuloma formation in ANCA-associatedvasculitidesrdquo APMIS vol 117 supplement s127 no 127 pp 32ndash36 2009
[67] M D Morgan C J Day K P Piper et al ldquoPatients withWegenerrsquos granulomatosis demonstrate a relative deficiency andfunctional impairment of T-regulatory cellsrdquo Immunology vol130 no 1 pp 64ndash73 2010
[68] M E Free D O Bunch J A McGregor et al ldquoPatients withantineutrophil cytoplasmic antibody-associated vasculitis havedefective Treg cell function exacerbated by the presence ofa suppression-resistant effector cell populationrdquo Arthritis andRheumatism vol 65 no 7 pp 1922ndash1933 2013
[69] B Wilde M Thewissen J Damoiseaux et al ldquoRegulatory Bcells in ANCA-associated vasculitisrdquo Annals of the RheumaticDiseases vol 72 no 8 pp 1416ndash1419 2013
[70] N Kesel D Khler L Herich et al ldquoCartilage destruction ingranulomatosis with polyangiitis (Wegenerrsquos granulomatosis)is mediated by human fibroblasts after transplantation intoimmunodeficientmicerdquoTheAmerican Journal of Pathology vol180 no 5 pp 2144ndash2155 2012
[71] C Rahmattulla R A de Lind van Wijngaarden A E Berdenet al ldquoRenal function and ear nose throat involvement in anti-neutrophil cytoplasmic antibody-associated vasculitis prospec-tive data from the European Vasculitis Society clinical trialsrdquoRheumatology vol 54 no 5 pp 899ndash907 2015
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
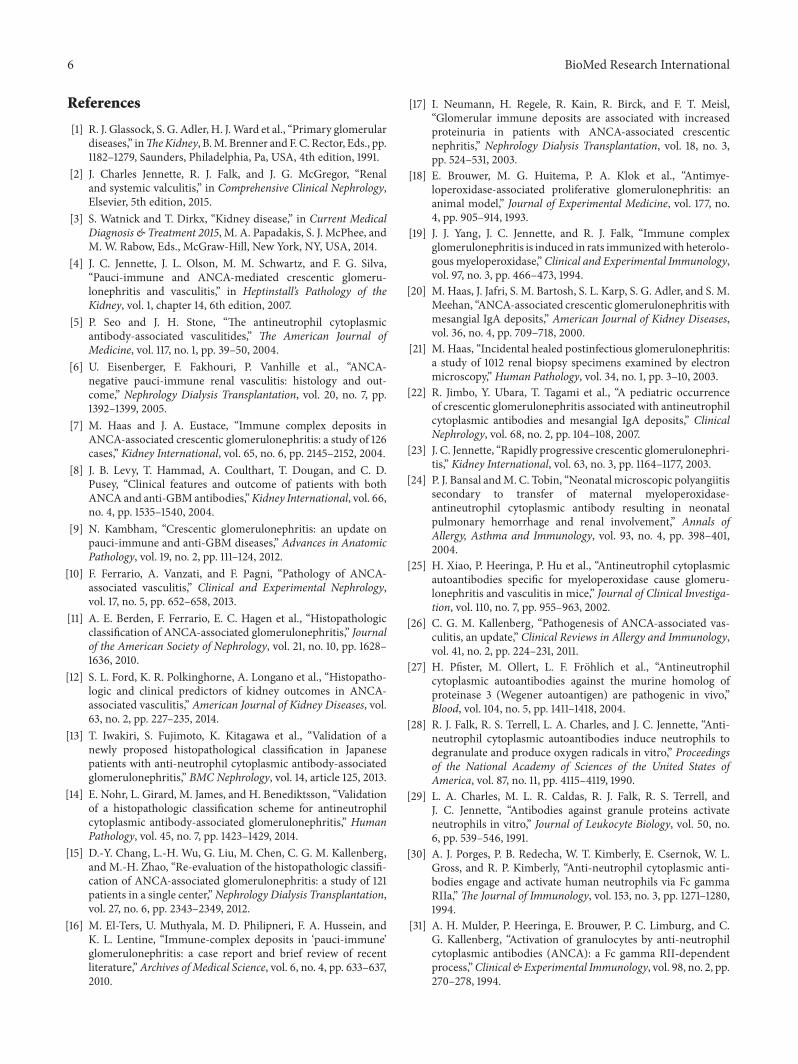
6 BioMed Research International
References
[1] R J Glassock S G Adler H JWard et al ldquoPrimary glomerulardiseasesrdquo inTheKidney BM Brenner and F C Rector Eds pp1182ndash1279 Saunders Philadelphia Pa USA 4th edition 1991
[2] J Charles Jennette R J Falk and J G McGregor ldquoRenaland systemic valculitisrdquo in Comprehensive Clinical NephrologyElsevier 5th edition 2015
[3] S Watnick and T Dirkx ldquoKidney diseaserdquo in Current MedicalDiagnosis amp Treatment 2015 M A Papadakis S J McPhee andM W Rabow Eds McGraw-Hill New York NY USA 2014
[4] J C Jennette J L Olson M M Schwartz and F G SilvaldquoPauci-immune and ANCA-mediated crescentic glomeru-lonephritis and vasculitisrdquo in Heptinstallrsquos Pathology of theKidney vol 1 chapter 14 6th edition 2007
[5] P Seo and J H Stone ldquoThe antineutrophil cytoplasmicantibody-associated vasculitidesrdquo The American Journal ofMedicine vol 117 no 1 pp 39ndash50 2004
[6] U Eisenberger F Fakhouri P Vanhille et al ldquoANCA-negative pauci-immune renal vasculitis histology and out-comerdquo Nephrology Dialysis Transplantation vol 20 no 7 pp1392ndash1399 2005
[7] M Haas and J A Eustace ldquoImmune complex deposits inANCA-associated crescentic glomerulonephritis a study of 126casesrdquo Kidney International vol 65 no 6 pp 2145ndash2152 2004
[8] J B Levy T Hammad A Coulthart T Dougan and C DPusey ldquoClinical features and outcome of patients with bothANCA and anti-GBMantibodiesrdquoKidney International vol 66no 4 pp 1535ndash1540 2004
[9] N Kambham ldquoCrescentic glomerulonephritis an update onpauci-immune and anti-GBM diseasesrdquo Advances in AnatomicPathology vol 19 no 2 pp 111ndash124 2012
[10] F Ferrario A Vanzati and F Pagni ldquoPathology of ANCA-associated vasculitisrdquo Clinical and Experimental Nephrologyvol 17 no 5 pp 652ndash658 2013
[11] A E Berden F Ferrario E C Hagen et al ldquoHistopathologicclassification of ANCA-associated glomerulonephritisrdquo Journalof the American Society of Nephrology vol 21 no 10 pp 1628ndash1636 2010
[12] S L Ford K R Polkinghorne A Longano et al ldquoHistopatho-logic and clinical predictors of kidney outcomes in ANCA-associated vasculitisrdquo American Journal of Kidney Diseases vol63 no 2 pp 227ndash235 2014
[13] T Iwakiri S Fujimoto K Kitagawa et al ldquoValidation of anewly proposed histopathological classification in Japanesepatients with anti-neutrophil cytoplasmic antibody-associatedglomerulonephritisrdquo BMC Nephrology vol 14 article 125 2013
[14] E Nohr L Girard M James and H Benediktsson ldquoValidationof a histopathologic classification scheme for antineutrophilcytoplasmic antibody-associated glomerulonephritisrdquo HumanPathology vol 45 no 7 pp 1423ndash1429 2014
[15] D-Y Chang L-H Wu G Liu M Chen C G M Kallenbergand M-H Zhao ldquoRe-evaluation of the histopathologic classifi-cation of ANCA-associated glomerulonephritis a study of 121patients in a single centerrdquoNephrology Dialysis Transplantationvol 27 no 6 pp 2343ndash2349 2012
[16] M El-Ters U Muthyala M D Philipneri F A Hussein andK L Lentine ldquoImmune-complex deposits in lsquopauci-immunersquoglomerulonephritis a case report and brief review of recentliteraturerdquoArchives of Medical Science vol 6 no 4 pp 633ndash6372010
[17] I Neumann H Regele R Kain R Birck and F T MeislldquoGlomerular immune deposits are associated with increasedproteinuria in patients with ANCA-associated crescenticnephritisrdquo Nephrology Dialysis Transplantation vol 18 no 3pp 524ndash531 2003
[18] E Brouwer M G Huitema P A Klok et al ldquoAntimye-loperoxidase-associated proliferative glomerulonephritis ananimal modelrdquo Journal of Experimental Medicine vol 177 no4 pp 905ndash914 1993
[19] J J Yang J C Jennette and R J Falk ldquoImmune complexglomerulonephritis is induced in rats immunizedwith heterolo-gous myeloperoxidaserdquo Clinical and Experimental Immunologyvol 97 no 3 pp 466ndash473 1994
[20] M Haas J Jafri S M Bartosh S L Karp S G Adler and S MMeehan ldquoANCA-associated crescentic glomerulonephritis withmesangial IgA depositsrdquo American Journal of Kidney Diseasesvol 36 no 4 pp 709ndash718 2000
[21] M Haas ldquoIncidental healed postinfectious glomerulonephritisa study of 1012 renal biopsy specimens examined by electronmicroscopyrdquo Human Pathology vol 34 no 1 pp 3ndash10 2003
[22] R Jimbo Y Ubara T Tagami et al ldquoA pediatric occurrenceof crescentic glomerulonephritis associated with antineutrophilcytoplasmic antibodies and mesangial IgA depositsrdquo ClinicalNephrology vol 68 no 2 pp 104ndash108 2007
[23] J C Jennette ldquoRapidly progressive crescentic glomerulonephri-tisrdquo Kidney International vol 63 no 3 pp 1164ndash1177 2003
[24] P J Bansal andM C Tobin ldquoNeonatal microscopic polyangiitissecondary to transfer of maternal myeloperoxidase-antineutrophil cytoplasmic antibody resulting in neonatalpulmonary hemorrhage and renal involvementrdquo Annals ofAllergy Asthma and Immunology vol 93 no 4 pp 398ndash4012004
[25] H Xiao P Heeringa P Hu et al ldquoAntineutrophil cytoplasmicautoantibodies specific for myeloperoxidase cause glomeru-lonephritis and vasculitis in micerdquo Journal of Clinical Investiga-tion vol 110 no 7 pp 955ndash963 2002
[26] C G M Kallenberg ldquoPathogenesis of ANCA-associated vas-culitis an updaterdquo Clinical Reviews in Allergy and Immunologyvol 41 no 2 pp 224ndash231 2011
[27] H Pfister M Ollert L F Frohlich et al ldquoAntineutrophilcytoplasmic autoantibodies against the murine homolog ofproteinase 3 (Wegener autoantigen) are pathogenic in vivordquoBlood vol 104 no 5 pp 1411ndash1418 2004
[28] R J Falk R S Terrell L A Charles and J C Jennette ldquoAnti-neutrophil cytoplasmic autoantibodies induce neutrophils todegranulate and produce oxygen radicals in vitrordquo Proceedingsof the National Academy of Sciences of the United States ofAmerica vol 87 no 11 pp 4115ndash4119 1990
[29] L A Charles M L R Caldas R J Falk R S Terrell andJ C Jennette ldquoAntibodies against granule proteins activateneutrophils in vitrordquo Journal of Leukocyte Biology vol 50 no6 pp 539ndash546 1991
[30] A J Porges P B Redecha W T Kimberly E Csernok W LGross and R P Kimberly ldquoAnti-neutrophil cytoplasmic anti-bodies engage and activate human neutrophils via Fc gammaRIIardquoThe Journal of Immunology vol 153 no 3 pp 1271ndash12801994
[31] A H Mulder P Heeringa E Brouwer P C Limburg and CG Kallenberg ldquoActivation of granulocytes by anti-neutrophilcytoplasmic antibodies (ANCA) a Fc gamma RII-dependentprocessrdquoClinical amp Experimental Immunology vol 98 no 2 pp270ndash278 1994
BioMed Research International 7
[32] R Kettritz J C Jennette andR J Falk ldquoCrosslinking of ANCA-antigens stimulates superoxide release by human neutrophilsrdquoJournal of the American Society of Nephrology vol 8 no 3 pp386ndash394 1997
[33] B H Ewert J C Jennette and R J Falk ldquoAnti-myeloperoxidaseantibodies stimulate neutrophils to damage human endothelialcellsrdquo Kidney International vol 41 no 2 pp 375ndash383 1992
[34] K Kessenbrock M Krumbholz U Schonermarck et al ldquoNet-ting neutrophils in autoimmune small-vessel vasculitisrdquoNatureMedicine vol 15 no 6 pp 623ndash625 2009
[35] A K Gupta M B Joshi M Philippova et al ldquoActivatedendothelial cells induce neutrophil extracellular traps and aresusceptible to NETosis-mediated cell deathrdquo FEBS Letters vol584 no 14 pp 3193ndash3197 2010
[36] O O Rowaiye M Kusztal and M Klinger ldquoThe kidneys andANCA-associated vasculitis from pathogenesis to diagnosisrdquoClinical Kidney Journal vol 8 no 3 pp 343ndash350 2015
[37] H Xiao A Schreiber P Heeringa R J Falk and J C JennetteldquoAlternative complement pathway in the pathogenesis of dis-ease mediated by anti-neutrophil cytoplasmic autoantibodiesrdquoAmerican Journal of Pathology vol 170 no 1 pp 52ndash64 2007
[38] U Schonermarck E Csernok and W L Gross ldquoPathogenesisof anti-neutrophil cytoplasmic antibody-associated vasculitischallenges and solutions 2014rdquo Nephrology Dialysis Transplan-tation vol 30 supplement 1 pp i46ndashi52 2015
[39] C Franssen R Gans C Kallenberg C Hageluken and SHoorntje ldquoDisease spectrum of patients with antineutrophilcytoplasmic autoantibodies of defined specificity distinct dif-ferences between patients with anti-proteinase 3 and anti-myeloperoxidase autoantibodiesrdquo Journal of Internal Medicinevol 244 no 3 pp 209ndash216 1998
[40] R Kain M Exner R Brandes et al ldquoMolecular mimicry inpauci-immune focal necrotizing glomerulonephritisrdquo NatureMedicine vol 14 no 10 pp 1088ndash1096 2008
[41] R Kain H Tadema E F McKinney et al ldquoHigh prevalenceof autoantibodies to hLAMP-2 in anti-neutrophil cytoplasmicantibody-associated vasculitisrdquo Journal of the American Societyof Nephrology vol 23 no 3 pp 556ndash566 2012
[42] A J Roth M C Brown R N Smith et al ldquoAnti-LAMP-2antibodies are not prevalent in patients with antineutrophilcytoplasmic autoantibody glomerulonephritisrdquo Journal of theAmerican Society of Nephrology vol 23 no 3 pp 545ndash555 2012
[43] R Kain and A J Rees ldquoWhat is the evidence for antibodies toLAMP-2 in the pathogenesis of ANCA associated small vesselvasculitisrdquo Current Opinion in Rheumatology vol 25 no 1 pp26ndash34 2013
[44] J Hao C Wang S-J Gou M-H Zhao and M Chen ldquoTheassociation between anti-plasminogen antibodies and diseaseactivity in ANCA-associated vasculitisrdquo Rheumatology vol 53no 2 pp 300ndash306 2014
[45] A E Berden S L Nolan H L Morris et al ldquoAnti-plasminogenantibodies compromise fibrinolysis and associatewith renal his-tology in ANCA-associated vasculitisrdquo Journal of the AmericanSociety of Nephrology vol 21 no 12 pp 2169ndash2179 2010
[46] C A Stegeman J W Cohen Tervaert W J Sluiter W LManson P E De Jong and C G M Kallenberg ldquoAssociationof chronic nasal carriage of Staphylococcus aureus and higherrelapse rates in Wegener granulomatosisrdquo Annals of InternalMedicine vol 120 no 1 pp 12ndash17 1994
[47] K Zycinska K A Wardyn T M Zielonka R Krupa andW Lukas ldquoCo-trimoxazole and prevention of relapses of PR3-ANCA positive vasculitis with pulmonary involvementrdquo Euro-pean Journal ofMedical Research vol 14 supplement 4 pp 265ndash267 2009
[48] A D Salama and C D Pusey ldquoShining a LAMP on pauci-immune focal segmental glomerulonephritisrdquo Kidney Interna-tional vol 76 no 1 pp 15ndash17 2009
[49] MMVanTimmeren andPHeeringa ldquoPathogenesis ofANCA-associated vasculitis recent insights from animal modelsrdquoCurrent Opinion in Rheumatology vol 24 no 1 pp 8ndash14 2012
[50] A M Coughlan S J Freeley and M G Robson ldquoAnimalmodels of anti-neutrophil cytoplasmic antibody-associated vas-culitisrdquo Clinical and Experimental Immunology vol 169 no 3pp 229ndash237 2012
[51] S L Hogan K K Satterly M A Dooley P H Nachman JC Jennette and R J Falk ldquoSilica exposure in anti-neutrophilcytoplasmic autoantibody-associated glomerulonephritis andlupus nephritisrdquo Journal of the American Society of Nephrologyvol 12 no 1 pp 134ndash142 2001
[52] Z Rihova D Maixnerova E Jancova et al ldquoSilica andasbestos exposure in ANCA-associated vasculitis with pul-monary involvementrdquo Renal Failure vol 27 no 5 pp 605ndash6082005
[53] T Kanda H Tanio CWu H Nishihara F Nogaki and T OnoldquoChurg-Strauss syndrome with severe granulomatous angiitisand crescentic glomerulonephritis which developed duringtherapy with a leukotriene receptor antagonistrdquo Clinical andExperimental Nephrology vol 14 no 6 pp 602ndash607 2010
[54] M Suneja S Baiswar and S A Vogelgesang ldquoHydralazineassociated pauci-immune glomerulonephritisrdquo Journal of Clin-ical Rheumatology vol 20 no 2 pp 99ndash102 2014
[55] S Morita Y Ueda and K Eguchi ldquoAnti-thyroid drug-inducedANCA-associated vasculitis a case report and review of theliteraturerdquo Endocrine Journal vol 47 no 4 pp 467ndash470 2000
[56] H K Choi P A Merkel A M Walker and J L NilesldquoDrug-associated antineutrophil cytoplasmic antibody-positivevasculitis prevalence among patients with high titers ofantimyeloperoxidase antibodiesrdquo Arthritis and Rheumatismvol 43 no 2 pp 405ndash413 2000
[57] J C Jennette R J Falk and A H Gasim ldquoPathogenesis ofantineutrophil cytoplasmic autoantibody vasculitisrdquo CurrentOpinion in Nephrology andHypertension vol 20 no 3 pp 263ndash270 2011
[58] W F Pendergraft III G A Preston R R Shah et al ldquoAutoim-munity is triggered by cPR-3(105ndash201) a protein complemen-tary to human autoantigen proteinase-3rdquo Nature Medicine vol10 no 1 pp 72ndash79 2004
[59] P Hewins F Belmonte J C Jennette R J Falk and G APreston ldquoLongitudinal studies of patients with ANCA vasculi-tis demonstrate concurrent reactivity to complementary PR3protein segments cPR3m and cPR3C and with no reactivity tocPR3Nrdquo Autoimmunity vol 44 no 2 pp 98ndash106 2011
[60] P A Lyons T F Rayner S Trivedi et al ldquoGenetically distinctsubsets within ANCA-associated vasculitisrdquo The New EnglandJournal of Medicine vol 367 no 3 pp 214ndash223 2012
[61] G Xie D Roshandel R Sherva et al ldquoAssociation of granulo-matosis with polyangiitis (Wegenerrsquos) with HLA-DPB1lowast04 andSEMA6A gene variants evidence from genome-wide analysisrdquoArthritis amp Rheumatism vol 65 no 9 pp 2457ndash2468 2013
[62] V Witko-Sarsat P Lesavre S Lopez et al ldquoA large subset ofneutrophils expressing membrane proteinase 3 is a risk factor
8 BioMed Research International
for vasculitis and rheumatoid arthritisrdquo Journal of the AmericanSociety of Nephrology vol 10 no 6 pp 1224ndash1233 1999
[63] P Jagiello P Aries L Arning et al ldquoThe PTPN22 620W alleleis a risk factor for Wegenerrsquos granulomatosisrdquo Arthritis andRheumatism vol 52 no 12 pp 4039ndash4043 2005
[64] D Martorana F Maritati G Malerba et al ldquoPTPN22 R620Wpolymorphism in the ANCA-associated vasculitidesrdquo Rheuma-tology vol 51 no 5 Article ID ker446 pp 805ndash812 2012
[65] R Giscombe X Wang D Huang and A K Lefvert ldquoCodingsequence 1 and promoter single nucleotide polymorphismsin the CTLA-4 gene in Wegenerrsquos granulomatosisrdquo Journal ofRheumatology vol 29 no 5 pp 950ndash953 2002
[66] P Lamprecht S Wieczorek J T Epplen P Ambrosch and CG M Kallenberg ldquoGranuloma formation in ANCA-associatedvasculitidesrdquo APMIS vol 117 supplement s127 no 127 pp 32ndash36 2009
[67] M D Morgan C J Day K P Piper et al ldquoPatients withWegenerrsquos granulomatosis demonstrate a relative deficiency andfunctional impairment of T-regulatory cellsrdquo Immunology vol130 no 1 pp 64ndash73 2010
[68] M E Free D O Bunch J A McGregor et al ldquoPatients withantineutrophil cytoplasmic antibody-associated vasculitis havedefective Treg cell function exacerbated by the presence ofa suppression-resistant effector cell populationrdquo Arthritis andRheumatism vol 65 no 7 pp 1922ndash1933 2013
[69] B Wilde M Thewissen J Damoiseaux et al ldquoRegulatory Bcells in ANCA-associated vasculitisrdquo Annals of the RheumaticDiseases vol 72 no 8 pp 1416ndash1419 2013
[70] N Kesel D Khler L Herich et al ldquoCartilage destruction ingranulomatosis with polyangiitis (Wegenerrsquos granulomatosis)is mediated by human fibroblasts after transplantation intoimmunodeficientmicerdquoTheAmerican Journal of Pathology vol180 no 5 pp 2144ndash2155 2012
[71] C Rahmattulla R A de Lind van Wijngaarden A E Berdenet al ldquoRenal function and ear nose throat involvement in anti-neutrophil cytoplasmic antibody-associated vasculitis prospec-tive data from the European Vasculitis Society clinical trialsrdquoRheumatology vol 54 no 5 pp 899ndash907 2015
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
BioMed Research International 7
[32] R Kettritz J C Jennette andR J Falk ldquoCrosslinking of ANCA-antigens stimulates superoxide release by human neutrophilsrdquoJournal of the American Society of Nephrology vol 8 no 3 pp386ndash394 1997
[33] B H Ewert J C Jennette and R J Falk ldquoAnti-myeloperoxidaseantibodies stimulate neutrophils to damage human endothelialcellsrdquo Kidney International vol 41 no 2 pp 375ndash383 1992
[34] K Kessenbrock M Krumbholz U Schonermarck et al ldquoNet-ting neutrophils in autoimmune small-vessel vasculitisrdquoNatureMedicine vol 15 no 6 pp 623ndash625 2009
[35] A K Gupta M B Joshi M Philippova et al ldquoActivatedendothelial cells induce neutrophil extracellular traps and aresusceptible to NETosis-mediated cell deathrdquo FEBS Letters vol584 no 14 pp 3193ndash3197 2010
[36] O O Rowaiye M Kusztal and M Klinger ldquoThe kidneys andANCA-associated vasculitis from pathogenesis to diagnosisrdquoClinical Kidney Journal vol 8 no 3 pp 343ndash350 2015
[37] H Xiao A Schreiber P Heeringa R J Falk and J C JennetteldquoAlternative complement pathway in the pathogenesis of dis-ease mediated by anti-neutrophil cytoplasmic autoantibodiesrdquoAmerican Journal of Pathology vol 170 no 1 pp 52ndash64 2007
[38] U Schonermarck E Csernok and W L Gross ldquoPathogenesisof anti-neutrophil cytoplasmic antibody-associated vasculitischallenges and solutions 2014rdquo Nephrology Dialysis Transplan-tation vol 30 supplement 1 pp i46ndashi52 2015
[39] C Franssen R Gans C Kallenberg C Hageluken and SHoorntje ldquoDisease spectrum of patients with antineutrophilcytoplasmic autoantibodies of defined specificity distinct dif-ferences between patients with anti-proteinase 3 and anti-myeloperoxidase autoantibodiesrdquo Journal of Internal Medicinevol 244 no 3 pp 209ndash216 1998
[40] R Kain M Exner R Brandes et al ldquoMolecular mimicry inpauci-immune focal necrotizing glomerulonephritisrdquo NatureMedicine vol 14 no 10 pp 1088ndash1096 2008
[41] R Kain H Tadema E F McKinney et al ldquoHigh prevalenceof autoantibodies to hLAMP-2 in anti-neutrophil cytoplasmicantibody-associated vasculitisrdquo Journal of the American Societyof Nephrology vol 23 no 3 pp 556ndash566 2012
[42] A J Roth M C Brown R N Smith et al ldquoAnti-LAMP-2antibodies are not prevalent in patients with antineutrophilcytoplasmic autoantibody glomerulonephritisrdquo Journal of theAmerican Society of Nephrology vol 23 no 3 pp 545ndash555 2012
[43] R Kain and A J Rees ldquoWhat is the evidence for antibodies toLAMP-2 in the pathogenesis of ANCA associated small vesselvasculitisrdquo Current Opinion in Rheumatology vol 25 no 1 pp26ndash34 2013
[44] J Hao C Wang S-J Gou M-H Zhao and M Chen ldquoTheassociation between anti-plasminogen antibodies and diseaseactivity in ANCA-associated vasculitisrdquo Rheumatology vol 53no 2 pp 300ndash306 2014
[45] A E Berden S L Nolan H L Morris et al ldquoAnti-plasminogenantibodies compromise fibrinolysis and associatewith renal his-tology in ANCA-associated vasculitisrdquo Journal of the AmericanSociety of Nephrology vol 21 no 12 pp 2169ndash2179 2010
[46] C A Stegeman J W Cohen Tervaert W J Sluiter W LManson P E De Jong and C G M Kallenberg ldquoAssociationof chronic nasal carriage of Staphylococcus aureus and higherrelapse rates in Wegener granulomatosisrdquo Annals of InternalMedicine vol 120 no 1 pp 12ndash17 1994
[47] K Zycinska K A Wardyn T M Zielonka R Krupa andW Lukas ldquoCo-trimoxazole and prevention of relapses of PR3-ANCA positive vasculitis with pulmonary involvementrdquo Euro-pean Journal ofMedical Research vol 14 supplement 4 pp 265ndash267 2009
[48] A D Salama and C D Pusey ldquoShining a LAMP on pauci-immune focal segmental glomerulonephritisrdquo Kidney Interna-tional vol 76 no 1 pp 15ndash17 2009
[49] MMVanTimmeren andPHeeringa ldquoPathogenesis ofANCA-associated vasculitis recent insights from animal modelsrdquoCurrent Opinion in Rheumatology vol 24 no 1 pp 8ndash14 2012
[50] A M Coughlan S J Freeley and M G Robson ldquoAnimalmodels of anti-neutrophil cytoplasmic antibody-associated vas-culitisrdquo Clinical and Experimental Immunology vol 169 no 3pp 229ndash237 2012
[51] S L Hogan K K Satterly M A Dooley P H Nachman JC Jennette and R J Falk ldquoSilica exposure in anti-neutrophilcytoplasmic autoantibody-associated glomerulonephritis andlupus nephritisrdquo Journal of the American Society of Nephrologyvol 12 no 1 pp 134ndash142 2001
[52] Z Rihova D Maixnerova E Jancova et al ldquoSilica andasbestos exposure in ANCA-associated vasculitis with pul-monary involvementrdquo Renal Failure vol 27 no 5 pp 605ndash6082005
[53] T Kanda H Tanio CWu H Nishihara F Nogaki and T OnoldquoChurg-Strauss syndrome with severe granulomatous angiitisand crescentic glomerulonephritis which developed duringtherapy with a leukotriene receptor antagonistrdquo Clinical andExperimental Nephrology vol 14 no 6 pp 602ndash607 2010
[54] M Suneja S Baiswar and S A Vogelgesang ldquoHydralazineassociated pauci-immune glomerulonephritisrdquo Journal of Clin-ical Rheumatology vol 20 no 2 pp 99ndash102 2014
[55] S Morita Y Ueda and K Eguchi ldquoAnti-thyroid drug-inducedANCA-associated vasculitis a case report and review of theliteraturerdquo Endocrine Journal vol 47 no 4 pp 467ndash470 2000
[56] H K Choi P A Merkel A M Walker and J L NilesldquoDrug-associated antineutrophil cytoplasmic antibody-positivevasculitis prevalence among patients with high titers ofantimyeloperoxidase antibodiesrdquo Arthritis and Rheumatismvol 43 no 2 pp 405ndash413 2000
[57] J C Jennette R J Falk and A H Gasim ldquoPathogenesis ofantineutrophil cytoplasmic autoantibody vasculitisrdquo CurrentOpinion in Nephrology andHypertension vol 20 no 3 pp 263ndash270 2011
[58] W F Pendergraft III G A Preston R R Shah et al ldquoAutoim-munity is triggered by cPR-3(105ndash201) a protein complemen-tary to human autoantigen proteinase-3rdquo Nature Medicine vol10 no 1 pp 72ndash79 2004
[59] P Hewins F Belmonte J C Jennette R J Falk and G APreston ldquoLongitudinal studies of patients with ANCA vasculi-tis demonstrate concurrent reactivity to complementary PR3protein segments cPR3m and cPR3C and with no reactivity tocPR3Nrdquo Autoimmunity vol 44 no 2 pp 98ndash106 2011
[60] P A Lyons T F Rayner S Trivedi et al ldquoGenetically distinctsubsets within ANCA-associated vasculitisrdquo The New EnglandJournal of Medicine vol 367 no 3 pp 214ndash223 2012
[61] G Xie D Roshandel R Sherva et al ldquoAssociation of granulo-matosis with polyangiitis (Wegenerrsquos) with HLA-DPB1lowast04 andSEMA6A gene variants evidence from genome-wide analysisrdquoArthritis amp Rheumatism vol 65 no 9 pp 2457ndash2468 2013
[62] V Witko-Sarsat P Lesavre S Lopez et al ldquoA large subset ofneutrophils expressing membrane proteinase 3 is a risk factor
8 BioMed Research International
for vasculitis and rheumatoid arthritisrdquo Journal of the AmericanSociety of Nephrology vol 10 no 6 pp 1224ndash1233 1999
[63] P Jagiello P Aries L Arning et al ldquoThe PTPN22 620W alleleis a risk factor for Wegenerrsquos granulomatosisrdquo Arthritis andRheumatism vol 52 no 12 pp 4039ndash4043 2005
[64] D Martorana F Maritati G Malerba et al ldquoPTPN22 R620Wpolymorphism in the ANCA-associated vasculitidesrdquo Rheuma-tology vol 51 no 5 Article ID ker446 pp 805ndash812 2012
[65] R Giscombe X Wang D Huang and A K Lefvert ldquoCodingsequence 1 and promoter single nucleotide polymorphismsin the CTLA-4 gene in Wegenerrsquos granulomatosisrdquo Journal ofRheumatology vol 29 no 5 pp 950ndash953 2002
[66] P Lamprecht S Wieczorek J T Epplen P Ambrosch and CG M Kallenberg ldquoGranuloma formation in ANCA-associatedvasculitidesrdquo APMIS vol 117 supplement s127 no 127 pp 32ndash36 2009
[67] M D Morgan C J Day K P Piper et al ldquoPatients withWegenerrsquos granulomatosis demonstrate a relative deficiency andfunctional impairment of T-regulatory cellsrdquo Immunology vol130 no 1 pp 64ndash73 2010
[68] M E Free D O Bunch J A McGregor et al ldquoPatients withantineutrophil cytoplasmic antibody-associated vasculitis havedefective Treg cell function exacerbated by the presence ofa suppression-resistant effector cell populationrdquo Arthritis andRheumatism vol 65 no 7 pp 1922ndash1933 2013
[69] B Wilde M Thewissen J Damoiseaux et al ldquoRegulatory Bcells in ANCA-associated vasculitisrdquo Annals of the RheumaticDiseases vol 72 no 8 pp 1416ndash1419 2013
[70] N Kesel D Khler L Herich et al ldquoCartilage destruction ingranulomatosis with polyangiitis (Wegenerrsquos granulomatosis)is mediated by human fibroblasts after transplantation intoimmunodeficientmicerdquoTheAmerican Journal of Pathology vol180 no 5 pp 2144ndash2155 2012
[71] C Rahmattulla R A de Lind van Wijngaarden A E Berdenet al ldquoRenal function and ear nose throat involvement in anti-neutrophil cytoplasmic antibody-associated vasculitis prospec-tive data from the European Vasculitis Society clinical trialsrdquoRheumatology vol 54 no 5 pp 899ndash907 2015
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 BioMed Research International
for vasculitis and rheumatoid arthritisrdquo Journal of the AmericanSociety of Nephrology vol 10 no 6 pp 1224ndash1233 1999
[63] P Jagiello P Aries L Arning et al ldquoThe PTPN22 620W alleleis a risk factor for Wegenerrsquos granulomatosisrdquo Arthritis andRheumatism vol 52 no 12 pp 4039ndash4043 2005
[64] D Martorana F Maritati G Malerba et al ldquoPTPN22 R620Wpolymorphism in the ANCA-associated vasculitidesrdquo Rheuma-tology vol 51 no 5 Article ID ker446 pp 805ndash812 2012
[65] R Giscombe X Wang D Huang and A K Lefvert ldquoCodingsequence 1 and promoter single nucleotide polymorphismsin the CTLA-4 gene in Wegenerrsquos granulomatosisrdquo Journal ofRheumatology vol 29 no 5 pp 950ndash953 2002
[66] P Lamprecht S Wieczorek J T Epplen P Ambrosch and CG M Kallenberg ldquoGranuloma formation in ANCA-associatedvasculitidesrdquo APMIS vol 117 supplement s127 no 127 pp 32ndash36 2009
[67] M D Morgan C J Day K P Piper et al ldquoPatients withWegenerrsquos granulomatosis demonstrate a relative deficiency andfunctional impairment of T-regulatory cellsrdquo Immunology vol130 no 1 pp 64ndash73 2010
[68] M E Free D O Bunch J A McGregor et al ldquoPatients withantineutrophil cytoplasmic antibody-associated vasculitis havedefective Treg cell function exacerbated by the presence ofa suppression-resistant effector cell populationrdquo Arthritis andRheumatism vol 65 no 7 pp 1922ndash1933 2013
[69] B Wilde M Thewissen J Damoiseaux et al ldquoRegulatory Bcells in ANCA-associated vasculitisrdquo Annals of the RheumaticDiseases vol 72 no 8 pp 1416ndash1419 2013
[70] N Kesel D Khler L Herich et al ldquoCartilage destruction ingranulomatosis with polyangiitis (Wegenerrsquos granulomatosis)is mediated by human fibroblasts after transplantation intoimmunodeficientmicerdquoTheAmerican Journal of Pathology vol180 no 5 pp 2144ndash2155 2012
[71] C Rahmattulla R A de Lind van Wijngaarden A E Berdenet al ldquoRenal function and ear nose throat involvement in anti-neutrophil cytoplasmic antibody-associated vasculitis prospec-tive data from the European Vasculitis Society clinical trialsrdquoRheumatology vol 54 no 5 pp 899ndash907 2015
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom