review article assessing and inducing neuroplasticity with
TRANSCRIPT

R
AMM
auR
dnp
rftdp
ut
dTuv
utcamidloNadr
oifrm
(NC
(
so
3
S59
EVIEW ARTICLE
ssessing and Inducing Neuroplasticity With Transcranialagnetic Stimulation and Robotics for Motor Function
arcia K. O’Malley, PhD, Tony Ro, PhD, Harvey S. Levin, PhD
pi
h
M
Tmbschcotllesltctmbtppos
n(fiedvRpacemoifratpdrp
ABSTRACT. O’Malley MK, Ro T, Levin HS. Assessingnd inducing neuroplasticity with transcranial magnetic stim-lation and robotics for motor function. Arch Phys Medehabil 2006;87(12 Suppl 2):S59-66.
Objectives: To describe 2 new ways of assessing and in-ucing neuroplasticity in the human brain—transcranial mag-etic stimulation (TMS) and robotics—and to investigate andromote the recovery of motor function after brain damage.
Data Sources: We identified recent articles and books di-ectly bearing on TMS and robotics. Articles using these toolsor purposes other than rehabilitation were excluded. Fromhese studies, we emphasize the methodologic and technicaletails of these tools as applicable for assessing and inducinglasticity.Study Selection: Because both tools have only recently been
sed for rehabilitation, the majority of the articles selected forhis review have been published only within the last 10 years.
Data Extraction: We used the PubMed and Compendexatabases to find relevant peer-reviewed studies for this review.he studies were required to be relevant to rehabilitation and tose TMS or robotics methodologies. Guidelines were appliedia independent extraction by multiple observers.Data Synthesis: Despite the limited amount of research
sing these procedures for assessing and inducing neuroplas-icity, there is growing evidence that both TMS and roboticsan be very effective, inexpensive, and convenient ways forssessing and inducing rehabilitation. Although TMS has pri-arily been used as an assessment tool for motor function, an
ncreasing number of studies are using TMS as a tool toirectly induce plasticity and improve motor function. Simi-arly, robotic devices have been used for rehabilitation becausef their suitability for delivery of highly repeatable training.ew directions in robotics-assisted rehabilitation are taking
dvantage of novel measurements that can be acquired via theevices, enabling unique methods of assessment of motorecovery.
Conclusions: As refinements in technology and advances inur knowledge continue, TMS and robotics should play anncreasing role in assessing and promoting the recovery ofunction. Ongoing and future studies combining TMS andobotics within the same populations may prove fruitful for aore detailed and comprehensive assessment of the central and
From the Departments of Mechanical Engineering and Materials ScienceO’Malley) and Psychology (Ro), Rice University, Houston, TX; and Cognitiveeuroscience Laboratory, Department of Physical Medicine & Rehabilitation, Baylorollege of Medicine, Houston, TX (Levin).Supported in part by the National Institute of Neurological Disorders and Stroke
grant nos. 21772, 21889, NS42772).No commercial party having a direct financial interest in the results of the research
upporting this article has or will confer a benefit upon the author(s) or upon anyrganization with which the author(s) is/are associated.Reprint requests to Marcia K. O’Malley, PhD, Rice University, 6100 Main St, MS
21, Houston, TX 77005-1892, e-mail: [email protected].
o0003-9993/06/8712S-10978$32.00/0doi:10.1016/j.apmr.2006.08.332
eripheral changes in the nervous system during preciselynduced recovery.
Key Words: Brain; Motor cortex; Neuronal plasticity; Re-abilitation; Robotics.© 2006 by the American Congress of Rehabilitationedicine
HE ADULT BRAIN’S potential for reorganization offunction has been supported by experiments using animal
odels to study use-dependent neuroplasticity,1,2 by functionalrain imaging studies of patients undergoing training afterustaining focal brain lesions,3,4 and by imaging of changes inortical representation associated with acquisition of skills inealthy human subjects.5 Extrapolation of neuroplasticity prin-iples from research laboratories to rehabilitation settings isngoing, but several obstacles continue to impede progress. Inhe case of recovery and reorganization of motor function, oneimitation of functional magnetic resonance imaging (fMRI), ateast in typical paradigms, is the requirement that the subjectxecute a movement. During early stages of recovery fromtroke, many patients are unable to move their more affectedimb sufficiently for motor mapping by fMRI. Another limita-ion of fMRI is the inability of some patients to tolerateonfinement in the scanner, and the logistics of scheduling andransportation can be problematic, especially when repeatedeasurement is specified by the study design. As described
elow, transcranial magnetic stimulation (TMS) mitigateshese problems because no motor response is required, therocedure can be performed on the rehabilitation unit, and theatient can be seated comfortably during mapping. TMS alsoffers the capability of inducing neuroplasticity via repetitivetimulation, thus facilitating intervention studies.
Clinical trials that apply principles of neuroplasticity, as inovel therapies such as constraint-induced movement therapyCIMT), have also been challenged by logistics and treatmentdelity. These limitations include, among many others, thextensive human resources needed to provide several hours ofaily treatment with an individual therapist, and the potentialariation in treatment technique across different therapists.obotics, although perhaps introducing other limitations forroviding therapy including an initial investment of resourcesnd time for equipment acquisition and training, could over-ome or at least mitigate these limitations by economically,fficiently, and precisely providing repetition of guided move-ent while preserving oversight by a therapist. Manipulation
f the parameters of motor training, including repetition, tim-ng, stimulus displays, and the distance and resistance requiredor the patient’s movement can all be better controlled byobotics than with a therapist. Feedback systems, which uselgorithms for changing response requirements depending onhe patient’s performance, can also be more consistently im-lemented and flexibly changed through robotics. Similarly,ata generated by the patient’s movement can be more reliablyecorded by the device than through human interaction. De-ending on the goals and design of a study, some combination
f robotics and therapist interaction may be specified. In anyArch Phys Med Rehabil Vol 87, Suppl 2, December 2006

ceut
dratvssTfn
tiatabigfhcthadiwcprwbnm
Tuachbnqofihcflaf1ctmci
vf
pfTrtIeciebwdewlrctco
T
ldsthsttmmt
Fssc
S60 NEUROPLASTICITY WITH TRANSCRANIAL MAGNETIC STIMULATION AND ROBOTICS, O’Malley
A
ase, the initial studies reviewed below lend support to thexpectation that both TMS and robotics will increasingly besed in translational and clinical intervention studies designedo enhance neuroplasticity and improve patient outcomes.
TRANSCRANIAL MAGNETIC STIMULATIONTMS is a relatively new, noninvasive technique that pro-
uces transient disruptions in brain activity.6-9 Although itsoots date back to over a century ago when several scientiststtempted to stimulate the brain with a magnetic pulse,10-13
hese early attempts of magnetic stimulation generated througharious different types of devices were for the most part un-uccessful. In 1980 and 1985, however, the first reports ofuccessful cortical stimulation using TMS were published.14,15
oday, TMS is being routinely used to investigate human brainunction and also particularly for assessing as well as inducingeuroplasticity noninvasively.The technique of TMS complements other neuroscientific
echniques for examining plasticity, such as fMRI, by provid-ng high temporal as well as spatial precision for studying,ssessing, and altering brain function. Furthermore, like tradi-ional patient lesion studies in neurology and neuropsychology,nd unlike functional imaging studies that measure correlationsetween brain activation and function, TMS allows for exam-nation of whether a particular brain area is necessary for aiven function. In this regard, TMS frequently has been re-erred to as producing “virtual lesions,” inducing similar be-avioral manifestations as naturally occurring lesions. (For aomparison of natural vs TMS-induced lesions on visual func-ion, see Ro and Rafal.16) Unlike naturally occurring lesions,owever, TMS can only influence surface brain structures thatre close to the scalp because the strength of the magnetic fluxrops off rapidly with increases in distance from the stimulat-ng coil. In addition, TMS can be safely applied to humans inays similar to the direct stimulation of cortical neurons often
onducted in presurgical mapping procedures and in nonhumanrimate neurophysiology studies, albeit with far less spatialesolution. This allows for a more direct comparative approachith previous neurophysiologic studies investigating brain-ehavior relations. It therefore provides one of the strongestew tools for human neuroscience investigation and affordsany potential ways for assessing and inducing neuroplasticity.The physical principles and technologic requirements of
MS are reasonably simple and straightforward. In brief, TMSses a small but strong and focused magnetic pulse that isdministered through a stimulating coil, usually composed ofopper strips with a plastic casing, held on the surface of theead (fig 1). The magnetic flux is generated by passing a veryrief electric current through the stimulating coil. This mag-etic pulse, which travels through the scalp and skull, conse-uently induces current into the brain. Thus, the size and extentf the magnetic pulse is highly dependent on the spatial con-guration of the stimulating coil and the position in which it iseld. Many commercially available coils in different sizes andonfigurations are available, but most studies typically use aocal figure-8 coil with 45- or 70-mm circular components or aarger, less focal circular coil. In terms of cortical volumeffected by these coils, some estimates have suggested that theocal figure-8 coils can stimulate as little as approximatelycm3, but the true extent and depth of stimulation from inducedurrent spread remains unknown. Nonetheless, we have shownhat subcentimeter resolution can be obtained by systematicallyoving the focus of the figure-8 coils in 1-cm steps to demar-
ate borders of cortical regions.17 Furthermore, when stimulat-
ng with 45-mm figure-8 coils, twitches restricted to an indi- rrch Phys Med Rehabil Vol 87, Suppl 2, December 2006
idual finger can frequently be evoked, further suggesting aairly restricted site of action of the TMS on cortex.
TMS can also be administered with repetitive trains of TMSulses at varying intensities and frequencies. Because the ef-ects on neuronal activity are short lived with single-pulseMS, on the order of tens to only a few hundred milliseconds,
epetitive transcranial magnetic stimulation (rTMS) ensureshat the neuronal disruptions occur for longer periods of time.t has also been shown that rTMS at certain frequencies forxtended periods of time can induce longer-lasting changes inortical function. For example, with rTMS delivered at approx-mately 1Hz for 15 minutes, it has been shown that corticalxcitability decreases for at least 15 minutes after the rTMS,ut curiously it has no effect on motor behavior as assessedith finger tapping speed measurements.18 Conversely, rTMSelivered at higher frequencies (eg, 10Hz) can increase corticalxcitability for up to 3 or 4 minutes.19 These frequencies relateell to the known neurophysiologic properties for inducing
ong-term potentiation and long-term depression.20 WhetherTMS is used during a task or to induce lasting changes inortical function, the temporal resolution is sacrificed becausehe precise timing of when neural events might be occurringannot be determined. Thus, high temporal resolution can bebtained only when using single-pulse TMS.
MS for Assessing NeuroplasticitySingle-pulse TMS has been shown to reliably and efficiently
ocalize the hand area of the motor cortex,17,21 as well as toetect changes in cortical motor representation.4,22,23 Whentimulating over the hand area of the motor cortex, in additiono observable twitches that are induced in the contralateraland, motor-evoked potentials can be reliably recorded, andeveral criteria have been established to determine the motorhreshold intensity for a given subject.24 Because there isremendous variability in the effective TMS intensities (ie,otor thresholds) across subjects,25,26 it is essential that theotor threshold intensity be established in each subject. Using
hese and other measures for examining motor function, several
ig 1. TMS is administered to a patient. TMS uses a small buttrong and focused magnetic pulse that is administered through atimulating coil, usually composed of copper strips with a plasticasing, held on the surface of the head.
ecent studies have taken advantage of the noninvasive, effi-
cmImnatmts
eipimtF
semu
uwpaucwmpmmw
FmtchamlmTmtdtttA
S61NEUROPLASTICITY WITH TRANSCRANIAL MAGNETIC STIMULATION AND ROBOTICS, O’Malley
ient, and highly effective technique of TMS for assessingotor neuroplasticity after extensive practice or brain damage.
n one of the first studies showing rapidly induced changes inotor representations with TMS, it was elegantly shown in
eurologically normal participants that the implicit learning ofmotor sequence can enlarge the cortical output representa-
ions for movement of the hand that is performing the move-ent sequence.22 Classen et al27 have further shown that prac-
ice and performance of a given movement can transiently alterubsequent motor representations as assessed with TMS.
It has also been shown that single-pulse TMS can be usedffectively and safely to map changes in motor representationsn patients with motor deficits consequent to stroke. For exam-le, several studies have shown that CIMT is effective fornducing central nervous system (CNS) reorganization andotor recovery, as assessed by changes in motor representa-
ions of the more affected limb with single-pulse TMS.4,28,29
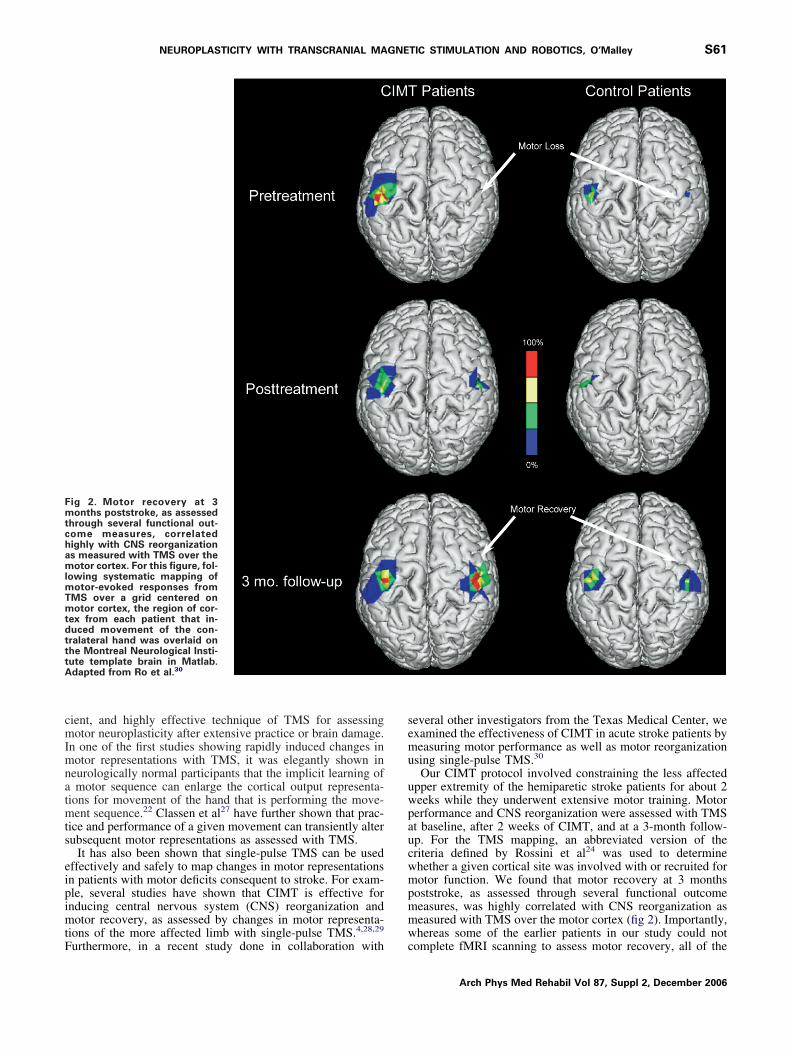
ig 2. Motor recovery at 3onths poststroke, as assessed
hrough several functional out-ome measures, correlatedighly with CNS reorganizations measured with TMS over theotor cortex. For this figure, fol-
owing systematic mapping ofotor-evoked responses from
MS over a grid centered onotor cortex, the region of cor-
ex from each patient that in-uced movement of the con-ralateral hand was overlaid onhe Montreal Neurological Insti-ute template brain in Matlab.dapted from Ro et al.30
urthermore, in a recent study done in collaboration with c
everal other investigators from the Texas Medical Center, wexamined the effectiveness of CIMT in acute stroke patients byeasuring motor performance as well as motor reorganization
sing single-pulse TMS.30
Our CIMT protocol involved constraining the less affectedpper extremity of the hemiparetic stroke patients for about 2eeks while they underwent extensive motor training. Motorerformance and CNS reorganization were assessed with TMSt baseline, after 2 weeks of CIMT, and at a 3-month follow-p. For the TMS mapping, an abbreviated version of theriteria defined by Rossini et al24 was used to determinehether a given cortical site was involved with or recruited forotor function. We found that motor recovery at 3 months
oststroke, as assessed through several functional outcomeeasures, was highly correlated with CNS reorganization aseasured with TMS over the motor cortex (fig 2). Importantly,hereas some of the earlier patients in our study could not
omplete fMRI scanning to assess motor recovery, all of the
Arch Phys Med Rehabil Vol 87, Suppl 2, December 2006

peTiFsan
T
tcaspchtocsrpcppop
atafsascsicstt
fafalhTtptpc
attRi
rth
R
cIothttmitpmles
cfionotucsrdorppotaiociacttds
rurasoptdrepTc
S62 NEUROPLASTICITY WITH TRANSCRANIAL MAGNETIC STIMULATION AND ROBOTICS, O’Malley
A
atients tolerated TMS well and could be conveniently tested,ven at bedside in some cases. These results highlight thatMS can provide a very effective, low-cost means for assess-
ng the effects of rehabilitation and neuroplasticity over time.urthermore, with the portability of some of the available TMSystems, repetitive testing can easily be done even at bedsidend therefore it may be more feasible than many other tech-iques at assessing plasticity.
MS for Inducing NeuroplasticitySeveral investigators have also taken advantage of the po-
ential short- and long-term changes associated with the appli-ation of TMS of the cerebral cortex. Thus, in addition to beingble to map changes in brain organization with TMS, recenttudies have been showing that it may be possible to inducelasticity or recovery of function by selective stimulation of theerebral cortex. A series of studies conducted in patients withemispatial neglect after parietal cortex damage have shownhat either single-pulse31 or low-frequency repetitive TMS32,33
f the unimpaired, contralesional hemisphere may restore per-eptual processing of contralesional (ie, ipsilateral to the TMS)pace. These results are consistent with earlier suggestions of aole of imbalanced interhemispheric inhibition between thearietal cortices in hemispatial neglect34,35 and extend andomplement the related results of a study showing that single-ulse TMS of the right parietal cortex can enhance perceptualrocessing on the ipsilateral side.36 Thus, by disrupting anveractive contralesional hemisphere with TMS, orienting anderceptual imbalances can effectively be restored.The potentially restorative effects from repetitive TMS have
lso been tested in patients with motor cortex damage. As inhe previous studies that were attempting to restore functionnd induce plasticity in patients with neglect, a recent study hasocused on repetitively stimulating the contralesional hemi-phere in attempts to restore interhemispheric inhibitory bal-nces and consequently motor function and behavior.37 In thistudy, Mansur et al37 showed that repetitively stimulating theontralesional motor cortex with low frequencies leads to sub-equently improved motor functions. Importantly, this rTMS-nduced improvement occurred only when stimulating over theontralesional motor cortex and not with premotor cortex orham stimulation. Research establishing the optimal parame-ers for the most effectively and efficiently induced neuroplas-icity remains to be completed.
Khedr et al38 at the Assiut University Hospital in Egypt haveurther shown that higher frequency rTMS over the moreffected motor cortex itself can also lead to improved motorunction compared with sham rTMS. Thus, motor plasticitynd improved outcome with rTMS can be induced either byow-frequency rTMS over the less affected hemisphere origh-frequency rTMS over the more affected hemisphere.aken together, these findings using TMS show the vast po-
ential that this relatively new technology has on assessing andromoting neuroplasticity and rehabilitation. With modifica-ions and extensions of its applications, the use of TMS hasrogressed from an assessment and diagnostic tool to one thatan also be used to directly induce changes within the CNS.
ROBOTICS FOR REHABILITATIONConcurrent with development of TMS as a technology for
ssessment and intervention in rehabilitation-related research,he potential of robotics for training motor skills and studyinghe effects of novel treatment protocols has been recognized.ecent developments in rehabilitation engineering suggest that
t is timely to investigate the use of robotics as a means to s
rch Phys Med Rehabil Vol 87, Suppl 2, December 2006
educe the resources required to implement intensive motorraining of impaired limbs in stroke patients and to facilitateome-based treatment.39-41
obotics-Assisted RehabilitationClinical studies have shown that the injured motor system is
apable of reorganization in the setting of motor practice.42
ndeed, stroke recovery may continue for months after initialnset because of cortical plasticity. In light of such implica-ions, therapeutic exercise has become the cornerstone of re-abilitation efforts after stroke. The goals of classical armherapy in neurorehabilitation include recovery of motor func-ion, improvement of movement coordination, training of newotion strategies, and prevention of secondary complications
ncluding, but not limited to, spasticity. In order to deliverherapy, physical treatment strategies have taken several ap-roaches. Examples include repetitive training of isolatedovements, CIMT to overcome learned nonuse of the paretic
imb,43 bilateral practice to facilitate movement of the pareticxtremity,44,45 and robot-aided rehabilitation to increase inten-ity and/or duration of therapy.39,46-49
Although several studies have shown improved motor out-ome with short and distributed therapy schedules, clinicalndings also indicate that increases in either training intensityr training duration can yield moderate positive effects oneuromuscular function and the patient’s execution of activitiesf daily living (ADLs).50 Because treatment duration and in-ensity can have such a profound effect on motor recovery, these of robotics is well suited to improve rehabilitation out-omes. Robotics, as an assistive technology, can be used toupport and enhance the productivity of clinicians and facilitateecovery of patients because of the controllable, repetitiveelivery and variable intensity (via assistive or resistive action)f the devices. Other potential benefits of the introduction ofobotics include new sensing capabilities for monitoringrogress of the patient, increased accessibility to therapy foratients, and increased therapy efficiency with the possibilityf group therapy. Robotics for rehabilitation has the potentialo automate labor-intensive therapy procedures, bringing ther-py to new venues including rehabilitation hospitals and clin-cs, subacute skilled nursing facilities, acute care hospitals withutpatient services, and even the home. Furthermore, withontinued research and a better understanding of neuroplastic-ty and rehabilitation, more optimal and efficient robotic ther-py procedures may be introduced and further developed. Thisapability comes at an opportune time, given the pressures onhe health care systems of the United States and other nationshat have resulted in a decrease in the amount of therapyelivered to patients due primarily to decreases in length oftay after medical rehabilitation.51
This section will discuss the state of the art in rehabilitationobotics for stroke, focusing on therapeutic robotics and thepper extremity. The technical requirements for therapeuticobotics will be discussed, along with the control approachesnd clinical outcomes (where applicable) of various devices. Ithould be noted that, unlike TMS, robotic technologies wereriginally developed as intervention tools, delivering therapy atotentially higher intensities than could be delivered by aherapist with traditional techniques. It was only after suchevices were used in clinical trials as intervention tools thatesearchers began to investigate uses of robotics for patientvaluation. Indeed, many systems were developed to assessatient progress and adapt the intervention protocols online.herefore, robotic systems will be discussed without specifi-ally separating those intended for assessment from those de-
igned to deliver therapy.
ttrOsadoa
fscatbap
C
seicatmmmtarrmautaltousmgsm
S
fddTcastrpup
a
(apurpawgdrrc
fdcsctwl
A
eeewdatsctstdrttooard
ahfceitd
estCet
S63NEUROPLASTICITY WITH TRANSCRANIAL MAGNETIC STIMULATION AND ROBOTICS, O’Malley
The design of robotic devices for therapy inherently defineshe potential applications of a particular system.52 For example,he degrees of freedom of the robotic device will dictate theanges and types of movement therapies that can be delivered.ften, robotic devices are designed with particular movement
trategies in mind, for example, reaching movements with therm involving primarily the shoulder and elbow, or devicesesigned specifically for repetitive grasping of real or virtualbjects. The control methodology for the robotic device willlso affect its design and implementation.
The reader is referred to extensive reviews of robotic therapyor the upper and lower extremity for a more complete discus-ion of the state of the field.39,46-49 To date, 3 randomizedontrolled studies of robotic therapy for the upper extremityfter stroke have been published.53-55 Several studies of roboticherapy used chronic stroke or spinal cord injury patients as theaseline control.56,57 The reader is directed to these articles formore thorough presentation of clinical results from these
ublicized trials.
ontrol Methodologies for Robotic TherapyA review of control algorithms for robotic therapy is pre-
ented by Reinkensmeyer et al.47 Specifically, for the upperxtremity, a variety of control techniques have been presentedn the literature, including passive,53,54 active-constrained,54
ounterpoise,58 resistive,56 error-amplifying,59 bimanual,54,60,61
nd active assistance.53-57 The active assistance approach is by farhe most used in robotic therapy, in which the patient attempts aovement and the robot assists with the completion of the move-ent through its sensing and actuation. The active assistanceethodology is derived from traditional clinical settings where the
herapist assists the patient to complete a motion if the patientttempts the movement but is unable. The approach may improveecovery by enhancing proprioceptive input, reducing spasticity,estoring soft-tissue suppleness, improving self-confidence, oraking exercise psychologically more tolerable because the ther-
pist manually helps to complete the movement if the patient isnable to do so. The drawbacks of active assistance in the tradi-ional clinical sense are that it is labor intensive and that thepproach has not been validated in clinical trials. Therefore, aogical solution for active assistance, specifically for weak pa-ients, is to deliver therapy with force-generating robots. Robotsffer several advantages over traditional devices that have beensed to provide assistance therapy (eg, mobile arm supports, armkateboards, or overhead slings) in that they can provide program-able levels of assistance, the robotic device can do work against
ravity because of its actuation, and the algorithms can be de-igned so that the output of the robotic device is automaticallyodified based on sensing of the patient’s progress and abilities.
ummary of Clinical FindingsThe first robotic therapy device to be used in clinical trials
or stroke therapy was the MIT-MANUS, a 2 degree-of-free-om back-driveable device that allows planar pointing andrawing movements, targeting the elbow and shoulder joints.62
he robot uses an impedance controller so that a programmableompliance is maintained between the patient’s arm locationnd the desired position along a programmed trajectory. Thetudy concluded that supplemental robot therapy, in addition toraditional physical and/or occupational therapy, can improveecovery in acute and chronic (shown in later studies) strokeatients. However, this work failed to address what features ornique advantages robotic therapy may provide when com-ared with traditional clinical intervention techniques.The mirror image motion enabler (MIME) took a different
pproach by using a 6 degree-of-freedom industrial robot O
PUMA 560) to provide 4 interaction paradigms for shouldernd elbow reaching motions and orientations.63 The robotrovides passive, active assist, active constrained, and biman-al modes of interaction for the patient. The study found thatobotic therapy, delivered via MIME, resulted in greater im-rovements in Fugl-Meyer Assessment (FMA) score, strength,nd reach extent at the conclusion of the trials as comparedith conventional therapy. Six months after the trial, the robotroup still had greater improvements in functional indepen-ence in ADLs, although the FMA scores were equal for theobot and conventional therapy groups. The results suggest thatobotic therapy is at least as effective, possibly more so, thanonventional therapy.
There are a few other clinical studies57,64 of robotic therapyor the upper extremity, along with numerous other roboticevices that are under development or have not undergonelinical testing. Clearly the potential benefits of robotic-as-isted rehabilitation have been recognized by the researchommunity, and future research will address unanswered ques-ions such as the unique contributions of the robotics comparedith therapy delivered by humans directly, appropriate dosage
evel, and treatment protocols for robotic rehabilitation.
ssessment With Therapeutic RoboticsRobotic devices developed to deliver therapy for upper-
xtremity motor deficit can also be used for assessment. Forxample, if the device is back-driveable, meaning that thendpoint of the robot can be easily translated through theorkspace when no power is supplied to the system, then theevice can be used as a motion capture device. This allows forssessment of the smoothness of movements, determined byhe kinematic features of the paths tracked through the work-pace. Additionally, directional error can be assessed by re-ording position data from the robotic device and comparinghat with the desired paths or trajectories through the work-pace. If the device is non–back-driveable, movement proper-ies can also be quantified by tracking reaction force patterns inirections of high impedance, such as lateral forces duringeaching. Because the availability of precise evaluation tools tohe clinical population has been limited, robotic devices withheir suite of sensors (eg, position, velocity, force) offer anpportunity to gain insight into motor processes and the effectsf rehabilitation on the recovery of motor function. Addition-lly, patient progress can be quantified with data from theobotic therapy sessions and associated evaluations, and suchata can be used to show the need for continued intervention.39
CURRENT AND FUTURE TRENDSThis review has presented 2 recent therapeutic tools for
ssessment and therapy intervention of stroke patients. TMSas been shown to be a valuable tool for assessment of motorunction, and rehabilitation robotics can provide repeatable,ontrolled motion input for reaching motions of the upperxtremity. These tools are slowly transitioning to multifacetedmplementation, with TMS being investigated as an interven-ion tool, and robotics being used for combined rehabilitationelivery and patient assessment.Current and future trends in stroke rehabilitation include
xtensions of the techniques mentioned here. For example,ome groups are attempting to combine automated delivery ofherapy, guided by a computer but not necessarily robotic, withIMT, in a project dubbed AutoCITE.41 Other groups arextending upper-extremity robotic-assisted rehabilitation dis-ally, to include movement therapies for wrist and hand.52,65,66
ne example is a robotic exoskeleton that we have designed
Arch Phys Med Rehabil Vol 87, Suppl 2, December 2006

aflrtmettt
afsbwfwiavsssflmm
nwbiibsdtvemn
mmd
1
1
1Fat
Fisttm
S64 NEUROPLASTICITY WITH TRANSCRANIAL MAGNETIC STIMULATION AND ROBOTICS, O’Malley
A
nd fabricated that can provide force assistance for elbowexion and extension, wrist pronation and supination, andadial and ulnar deviation (fig 3).52 The RiceWrist is intendedo provide robotic therapy via force feedback during range-of-otion (ROM) tasks.66 Joint ROM and torque output of the
lectric motor-driven device are matched to human capabili-ies. Passive, triggered, and active-constrained modes, such ashose developed for MIME, allow for therapist control ofherapy protocols based on patient capability and progress.
In studies that we are currently conducting, robotic devicesre being used to induce neuroplasticity and recovery, anduture studies will use TMS to assess it. There is also aignificant research thrust toward using virtual reality in reha-ilitation applications. Although there are too many individualorks to cite, the reader is encouraged to review proceedings
rom the International Workshop on Virtual Rehabilitation,hich has been held annually since 2002 (http://www.
wvr.org). The utilization of virtual reality for rehabilitation hasllowed researchers to investigate interesting theories, such asisual feedback distortion67 assistance forces in virtual realityystems that use haptic feedback58,62,63,68,69 (eg, the systemhown in figure 4) and home-based telerehabilitation.70,71 Withuch advances in technologies and the combination of highlyexible tools, not only will assessments of neuroplasticity beore feasible, accurate, and cost effective, but so will theagnitude of induced plasticity and recovery of function.
CONCLUSIONSThis review presents a review of TMS and robotics as 2
ovel technologies for assessing and inducing neuroplasticity,ith a focus on motor recovery. Although TMS has primarilyeen used as an assessment tool for motor function, an increas-ng number of studies are using TMS as a tool to directlynduce plasticity and improve motor function. Similarly, ro-otic devices have been used for rehabilitation because of theiruitability for the delivery of highly repeatable training. Newirections in robotics-assisted rehabilitation are taking advan-age of novel measurements that can be acquired via the de-ices, enabling unique methods of assessment of motor recov-ry. Although the 2 technologies are presented individually,uch could be gained in terms of understanding the mecha-
isms of robotic-assisted rehabilitation with TMS as an assess-
ig 3. A robotic lower-arm exoskeleton provides sensing and actu-
tion for elbow flexion and extension, wrist pronation and supina-ion, and radial-ulnar deviation.52rch Phys Med Rehabil Vol 87, Suppl 2, December 2006
ent tool, just as coupling TMS and robotics as interventionethodologies may result in improved gains for patients un-
ergoing therapy.
References1. Feeney D, Gonzalez A, Law W. Amphetamine, haloperidol and
experience interact to affect rate of recovery after motor cortexinjury. Science 1982;217:855-7.
2. Nudo R, Wise B, SiFuentes F, Milliken G. Neural substrates forthe effects of rehabilitative training on motor recovery after isch-emic infarct. Science 1996;272:1791-4.
3. Musso M, Weiller C, Keibel S, Muller S, Bulau P, Rijntjes M.Training-induced brain plasticity in aphasia. Brain 1999;122:1781-90.
4. Liepert J, Bauder H, Wolfgang HR, Miltner WH, Taub E, WeillerC. Treatment-induced cortical reorganization after stroke in hu-mans. Stroke 2000;31:1210-6.
5. Karni A, Meyer G, Jezzard P, Adams M, Turner R, Ungerlelder L.Functional MRI evidence for adult motor cortex plasticity duringmotor skill learning. Nature 1995;377:155-8.
6. Jahanshahi M, Rothwell J. Transcranial magnetic stimulationstudies of cognition: an emerging field. Exp Brain Res 2000;131:1-9.
7. Pascual-Leone A, Walsh V, Rothwell J. Transcranial magneticstimulation in cognitive neuroscience—virtual lesion, chronome-try, and functional connectivity. Curr Opin Neurobiol 2000;10:232-7.
8. Hallett M. Transcranial magnetic stimulation and the human brain.Nature 2000;406:147-50.
9. Walsh V, Cowey A. Transcranial magnetic stimulation and cog-nitive neuroscience. Nat Rev Neurosci 2000;1:73-9.
0. d’Arsonval A. Dispositifs pour la mesure des courants alternatifsde toutes fréquences. C R Soc Biol 1896;2:450-1.
1. Magnuson CE, Stevens HC. Visual sensations caused by thechanges in the strength of a magnetic field. Am J Physiol 1911;29:124-36.
2. Magnuson CE, Stevens HC. Visual sensations created by a mag-
ig 4. A haptic (force-feedback) joystick can allow for therapeuticnteractions with virtual environments, displayed via a computercreen.69 Position data recorded via the robotic joystick are moni-ored by the computer, and resultant force commands are displayedo the patient. In such a system, assistance forces can be imple-ented via the actuators of the robotic device.
netic field. Philosoph Mag 1914;28:188-207.

1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
S65NEUROPLASTICITY WITH TRANSCRANIAL MAGNETIC STIMULATION AND ROBOTICS, O’Malley
3. Thompson SP. A physiological effect of an alternating magneticfield. Proc R Soc London 1910;B82:396-9
4. Merton PA, Morton HB. Stimulation of the cerebral cortex in theintact human subject. Nature 1980;285:227.
5. Barker AT, Jalinous R, Freeston IL. Noninvasive magnetic stim-ulation of human motor cortex. Lancet 1985;11:1106-7.
6. Ro T, Rafal R. Visual restoration in cortical blindness: insightsfrom natural and TMS-induced blindsight. Neuropsychol Rehabil2006;16:377-96.
7. Ro T, Cheifet S, Ingle H, Shoup R, Rafal R. Localization of thehuman frontal eye fields and motor hand area with transcranialmagnetic stimulation and magnetic resonance imaging. Neuropsy-chologia 1999;37:225-31.
8. Chen R, Classen J, Gerloff C, et al. Depression of motor cortexexcitability by low-frequency transcranial magnetic stimulation.Neurology 1997;48:1398-403.
9. Pascual-Leone A, Valls-Sole J, Wassermann EM, Hallett M. Re-sponses to rapid-rate transcranial magnetic stimulation of thehuman motor cortex. Brain 1994;117(Pt 4):847-58.
0. Bear MF, Malenka RC. Synaptic plasticity. LTP and LTD. CurrOpin Neurobiol 1994;4:289-99.
1. Boroojerdi B, Foltys H, Krings T, Spetzger U, Thron A, Topper R.Localization of the motor hand area using transcranial magneticstimulation and functional magnetic resonance imaging. Clin Neu-rophysiol 1999;110:699-704.
2. Pascual-Leone A, Grafman J, Hallett M. Modulation of corticalmotor output maps during development of implicit and explicitknowledge. Science 1994;263:1287-9.
3. Rossini P, Caltagirone C, Castriota-Scanderbeg A, et al. Handmotor cortical area reorganization in stroke: a study with fMRI,MEG and TCS maps. Neuroreport 1998;9:2141-6.
4. Rossini PM, Barker AT, Berardelli A, et al. Non-invasive electri-cal and magnetic stimulation of the brain, spinal cord and roots:basic principles and procedures for routine clinical application.Report of an IFCN committee. Electroencephalogr Clin Neuro-physiol 1994;91:79-92.
5. Mills KR, Nithi KA. Corticomotor threshold to magnetic stimu-lation: normal values and repeatability. Muscle Nerve 1997;20:570-6.
6. Ferbert A, Caramia D, Priori A, Bertolasi L, Rothwell JC. Corticalprojection to erector spinae muscles in man as assessed by focaltranscranial magnetic stimulation. Electroencephalogr Clin Neu-rophysiol 1992;85:382-7.
7. Classen J, Liepert J, Wise SP, Hallett M, Cohen LG. Rapidplasticity of human cortical movement representation induced bypractice. J Neurophysiol 1998;79:1117-23.
8. Park SW, Butler AJ, Cavalheiro V, Alberts JL, Wolf SL. Changesin serial optical topography and TMS during task performanceafter constraint-induced movement therapy in stroke: a case study.Neurorehabil Neural Repair 2004;18:95-105.
9. Wittenberg GF, Chen R, Ishii K, et al. Constraint-induced therapyin stroke: magnetic-stimulation motor maps and cerebral activa-tion. Neurorehabil Neural Repair 2003;17:48-57.
0. Ro T, Noser E, Boake C, et al. Functional reorganization andrecovery after constraint-induced movement therapy in subacutestroke: case reports. Neurocase 2006;12:50-60.
1. Oliveri M, Rossini PM, Cicinelli P, et al. Neurophysiologicalevaluation of tactile space perception deficits through transcranialmagnetic stimulation. Brain Res Brain Res Protoc 2000;5:25-9.
2. Brighina F, Bisiach E, Oliveri M, et al. 1 Hz repetitive transcranialmagnetic stimulation of the unaffected hemisphere amelioratescontralesional visuospatial neglect in humans. Neurosci Lett 2003;2003:131-3.
3. Oliveri M, Bisiach E, Brighina F, et al. rTMS of the unaffectedhemisphere transiently reduces contralesional visuospatial hemi-
neglect. Neurology 2001;57:1338-40.4. Kinsbourne M. Hemi-neglect and hemisphere rivalry. Adv Neurol1977;8:41-9.
5. Kinsbourne M. Orientational bias model of unilateral neglect:evidence from attentional gradients within hemispace. In: Robert-son IH, Marshall JC, editors. Unilateral neglect: clinical andexperimental studies. Hillsdale: Lawrence Erlbaum; 1993. p 63-86.
6. Seyal M, Ro T, Rafal RD. Increased sensitivity to ipsilateralcutaneous stimuli following transcranial magnetic stimulation ofthe parietal lobe. Ann Neurol 1995;38:264-7.
7. Mansur CG, Fregni F, Boggio PS, et al. A sham stimulation-controlled trial of rTMS of the unaffected hemisphere in strokepatients. Neurology 2005;64:1802-4.
8. Khedr E, Ahmed M, Fathy N, Rothwell J. Therapeutic trial ofrepetitive transcranial magnetic stimulation after acute ischemicstroke. Neurology 2005;65:466-8.
9. Fasoli SE, Krebs HI, Hogan N. Robotic technology and strokerehabilitation: translating research into practice. Top Stroke Re-habil 2004;11:11-9.
0. Krebs HI, Volpe BT, Aisen ML, Hogan N. Increasing productivityand quality of care: robot-aided neuro-rehabilitation. J RehabilRes Dev 2000;37:639-52.
1. Lum PS, Taub E, Schwandt D, Postman M, Hardin P, Uswatte G.Automated Constraint-Induced Therapy Extension (autoCITE) formovement deficits after stroke. J Rehabil Res Dev 2004;41:249-58.
2. Ward NS. Functional reorganization of the cerebral motor systemafter stroke. Curr Opin Neurol 2004;17:725-30.
3. Taub E, Miller N, Novack T, et al. Technique to improve chronicmotor deficit after stroke. Arch Phys Med Rehabil 1993;74:347-54.
4. Whitall J, McCombe Waller S, Silver KH, Macko RF. Repetitivebilateral arm training with rhythmic auditory cueing improvesmotor function in chronic hemiparetic patients. Stroke 2000;31:2390-8.
5. Mudie M, Matayas T. Upper extremity retraining followingstroke: effects of bilateral practice. J Neurol Rehabil 1996;10:167-84.
6. Hogan N, Krebs HI. Interactive robots for neuro-rehabilitation.Restor Neurol Neurosci 2004;22:349-58.
7. Reinkensmeyer DJ, Emken JL, Cramer SC. Robotics, motor learn-ing, and neurologic recovery. Annu Rev Biomed Eng 2004;6:497-525.
8. Riener R, Nef T, Colombo G. Robot-aided neurorehabilitation ofthe upper extremities. Med Biol Eng Comput 2005;43:2-19.
9. Stein J. Motor recovery strategies after stroke. Top Stroke Rehabil2004;11:12-22.
0. Kwakkel G, Kollen BJ, Wagenaar RC. Long term effects ofintensity of upper and lower limb training after stroke: a random-ised trial. J Neurol Neurosurg Psychiatry 2002;72:473-9.
1. Ottenbacher KJ, Smith PM, Illig SB, Linn RT, Ostir GV, GrangerCV. Trends in length of stay, living setting, functional outcome,and mortality following medical rehabilitation. JAMA 2004;292:1687-95.
2. Gupta A, O’Malley MK. Design of a haptic arm exoskeleton fortraining and rehabilitation. ASME/IEEE Trans Mechatronics2006;11:280-9.
3. Volpe BT, Krebs HI, Hogan N, Edelsteinn L, Diels CM, AisenML. Robot training enhanced motor outcome in patients withstroke maintained over 3 years. Neurology 1999;53:1874-6.
4. Lum PS, Burgar CG, Shor PC, Majmundar M, Van der Loos M.Robot-assisted movement training compared with conventionaltherapy techniques for the rehabilitation of upper-limb motorfunction after stroke. Arch Phys Med Rehabil 2002;83:952-9.
5. Kahn LE, Zygman M, Rymer WZ, Reinkensmeyer D. Effect of
robot-assisted and unassisted exercise on functional reaching inArch Phys Med Rehabil Vol 87, Suppl 2, December 2006

5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
S66 NEUROPLASTICITY WITH TRANSCRANIAL MAGNETIC STIMULATION AND ROBOTICS, O’Malley
A
chronic hemiparesis. In: Engineering in Medicine and BiologySociety, 2001. Proceedings of the 23rd Annual InternationalConference of the IEEE. Vol 2. New York: IEEE; 2001. p 1344-7.
6. Fasoli SE, Krebs HI, Stein J, Frontera WR, Hogan N. Effects ofrobotic therapy on motor impairment and recovery in chronicstroke. Arch Phys Med Rehabil 2003;84:477-82.
7. Hesse S, Schulte-Tigges G, Konrad M, Bardeleben A, Werner C.Robot-assisted arm trainer for the passive and active practice ofbilateral forearm and wrist movements in hemiparetic subjects.Arch Phys Med Rehabil 2003;84:915-20.
8. Reinkensmeyer DJ, Takahashi CD, Timoszyk WK, Reinkens-meyer AN, Kahn LE. Design of robot assistance for arm move-ment therapy following stroke. Adv Robotics 2000;14:625-37.
9. Patton JL, Mussa-Ivaldi FA, Rymer WZ. Altering movementpatterns in healthy and brain-injured subjects via custom designedrobotic forces. In: Engineering in Medicine and Biology Society,2001. Proceedings of the 23rd Annual International Conference ofthe IEEE. Vol 2. New York: IEEE; 2001. p 1356-9.
0. Lum P, Lehman S, Reinkensmeyer D. The bimanual lifting reha-bilitator: a device for rehabilitating bimanual control in strokepatients. IEEE Trans Rehabil Eng 1995;3:166-74.
1. Lum P, Reinkensmeyer D, Lehman S. Robotic assist devices forbimanual physical therapy: preliminary experiments. IEEE TransRehabil Eng 1993;1:185-91.
2. Krebs HI, Hogan N, Aisen ML, Volpe BT. Robot-aided neurore-habilitation. IEEE Trans Rehabil Eng 1998;6:75-87.
3. Burgar CG, Lum PS, Shor PC, Van der Loos HF. Development ofrobots for rehabilitation therapy: The Palo Alto VA/Stanford
experience. J Rehabil Res Dev 2000;37:663-73.rch Phys Med Rehabil Vol 87, Suppl 2, December 2006
4. Reinkensmeyer DJ, Schmit BD, Rymer WZ. Assessment of activeand passive restraint during guided reaching after chronic braininjury. Ann Biomed Eng 1999;27:805-14.
5. Charles SK, Krebs HI, Volpe BT, Lynch D, Hogan N. Wristrehabilitation following stroke: Initial clinical results. In: ICORR2005: 9th International Conference on Rehabilitation Robotics.New York: IEEE; 2005. p 13-6.
6. O’Malley MK, Sledd AM, Gupta A, Patoglu V, Huegel J, BurgarC. The RW: a distal upper extremity rehabilitation robot for stroketherapy. ASME International Mechanical Engineering Congressand Exposition; 2006 Nov 7-11; Chicago (IL).
7. Brewer BR, Fagan M, Klatzky R, Matsuoka Y. Perceptual limitsfor a robotic rehabilitation environment using visual feedbackdistortion. IEEE Trans Neural Syst Rehabil Eng 2005;13:1-11.
8. Mussa-Ivaldi FA, Patton JL. Robots can teach people how tomove their arm. In: ICRA 2000: IEEE International Conferenceon Robotics and Automation. Vol 1. New York: IEEE; 2000. p300-5.
9. O’Malley MK, Gupta A, Gen M, Li Y. Shared control in hapticsystems for performance enhancement and training. ASME JDynamic Syst Meas Control 2006;128:75-85.
0. Popescu VG, Burdea GC, Bouzit M, Hentz VR. A virtual-reality-based telerehabilitation system with force feedback. IEEE TransInform Technol Biomed 2000;4:45-51.
1. Reinkensmeyer DJ, Pang CT, Nessler JA, Painter CC. Java ther-apy: Web-based robotic rehabilitation. In: Integration of AssistiveTechnology in the Information Age: Proceedings 7th InternationalConference on Rehabilitation Robotics. Amsterdam: IOS Pr;
2001. p 66-71.