results from the 2014-2015 national antimicrobial ... · results from the 2014-2015 national...
TRANSCRIPT
Results from the 2014-2015
National Antimicrobial
Prescribing Survey (NAPS)
Dr Rod James
National Centre of Antimicrobial Stewardship
at the Peter Doherty Institute
Outline
• Introduction
– Background
– Development of data collection tools and
website
• Results
– Participating hospitals
– Data analysis – focus on NSW
• Future directions

Introduction to
the NAPS

Background
• Antimicrobial Prescribing Survey (APS)
• Developed by Melbourne Health AMS
research team
• Aim – to develop a tool for qualitative and
quantitative assessment of antimicrobial
prescribing at an individual hospital
level

Background
• Flexible, practical and generalisable
• Suit needs of a variety of auditors
• The act of auditing – associated with
reflection and improved practice

Aims and limitations
• Aims
1. Quality improvement tool to help assess own
practice
2. Provide data to allow some simple
comparisons to be made between hospitals
3. Provide feedback on utilisation of guidelines
as well as gaps

Aims and limitations
• Limitations
1. Sampling
• Not always a randomised sample
• Only ‘keen’ hospitals participate
• ? better prescribers
2. ‘Benchmarking’
• Difficult to provide completely accurate
comparisons
• Need to disclose limitations

The results described in the report were obtained from a pilot of a new, web-based National
Antimicrobial Prescribing Survey implemented during Antibiotic Awareness Week in November
2013.
The authors advise caution in the interpretation and extrapolation of these data, and the
results should be interpreted in the context of several limitations:
1. Sampling and selection bias: hospitals included were not a randomised sample. Any
health care facility was able to participate if they wished to, hence these results may be
skewed by selection bias.
2. Survey methodology – participating facilities were able to choose their own method of
data collection (eg point-prevalence survey, random sample, targeted patient types)
and we did not ask them to nominate which they had used. Therefore, we were unable
to determine an accurate denominator in all cases.
3. Validation of audit tool and the assessment of appropriateness: individual auditors at
each participating facility were responsible for determining the appropriateness of each
antimicrobial prescription. An algorithm and detailed instructions were provided,
however this tool has not yet been validated. An inter-rater correlation study is
currently underway to determine consistency of assessment between assessor types.

Data collection
• For more consistent data collection, also
developed a set of training tools:
– definitions for each data entry field
– a unique indication list
– guidelines to assist with the assessment of
appropriateness
– a set of worked case examples

Data Collection Form

Guidelines

Indications List

Website – www.naps.org.au
Reporting
• 5 main components: 1. Dashboard
• Display key indicators
2. Filterable reports
• Antimicrobial usage
• Detailed assessment of prescription
3. ‘Benchmarking’ comparisons
• Needed approval from facilities
• De-identified
4. Time series analysis
5. Data Export

Dashboard

Filterable Reports

Benchmarking

Benchmarking

Time Series

Participation
Rates

Participating hospitals
APS 2011
32 hospitals
APS 2012
76 hospitals
NAPS 2013
152 hospitals
NAPS 2014
248 hospitals
Funding type Public Private Public Private Public Private Public Private
30 2 66 10 133 19 197 51
Location
major city 22 35 65 87
inner regional 6 14 46 62
outer regional 2 14 14 34
remote 0 3 6 10
very remote 0 0 2 4
Number of prescriptions 2, 523 5, 185 13, 111 19, 944

Participating hospitals
State Funding type Number State total
ACT Public 1
2 Private 1
NSW Public 71
79 Private 8
NT Public 2
2 Private 0
QLD Public 26
36 Private 10
SA Public 9
15 Private 6
VIC Public 63
80 Private 17
WA Public 25
34 Private 9
Total Public 197
248 Private 51

Participating hospitals

Public Hospitals
Peer Group Number of hospitals Total number
in each category
Percent of all hospitals in
category, 2014
Percent change from 2013
2013 2014 Absolute Relative
Principle referral 48 61 93 65.6 +14.0 +27.1
Specialist women’s and children’s 6 8 11 72.7 +18.2 +33.3
Large hospitals- Major city 11 18 23 78.3 +30.4 +63.6
Large hospitals - Regional and remote 9 11 20 55.0 +10.0 +22.2
Large hospitals - Group 1 12 17 30 56.7 +16.7 +41.7
Large hospitals - Group 2 13 22 58 37.9 +15.5 +69.2
Small acute hospitals - Regional 9 25 117 21.4 +13.7 +177.8
Sub-acute and non-acute hospitals 6 7 65 10.8 +1.5 +16.7
Small acute hospitals - Remote 7 10 41 24.4 +7.3 +42.9
Multi-purpose services 5 5 79 6.3 0.0 0.0
Rehabilitation 2 2 8 25.0 0.0 0.0
Other non-acute 3 3 12 25.0 0.0 0.0
Psychiatric hospital 0 1 19 5.3 +5.3c nac
Un-peered and other 2 7 201 3.5 +2.5 +250.0
Total 133 197 777 25.4 +8.2 +48.1
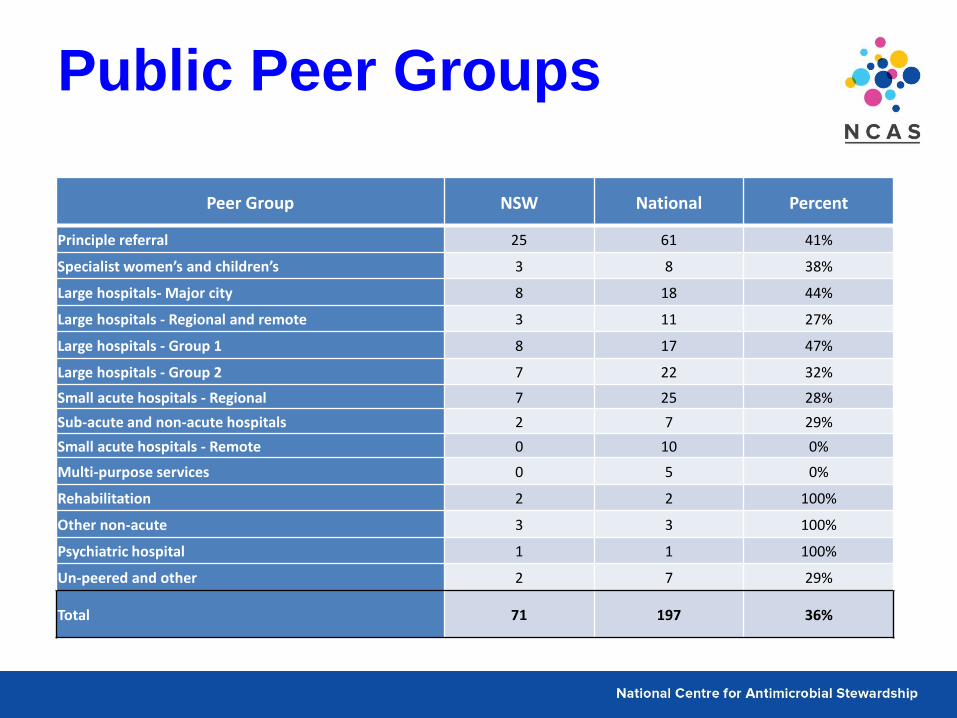
Public Peer Groups
Peer Group NSW National Percent
Principle referral 25 61 41%
Specialist women’s and children’s 3 8 38%
Large hospitals- Major city 8 18 44%
Large hospitals - Regional and remote 3 11 27%
Large hospitals - Group 1 8 17 47%
Large hospitals - Group 2 7 22 32%
Small acute hospitals - Regional 7 25 28%
Sub-acute and non-acute hospitals 2 7 29%
Small acute hospitals - Remote 0 10 0%
Multi-purpose services 0 5 0%
Rehabilitation 2 2 100%
Other non-acute 3 3 100%
Psychiatric hospital 1 1 100%
Un-peered and other 2 7 29%
Total 71 197 36%
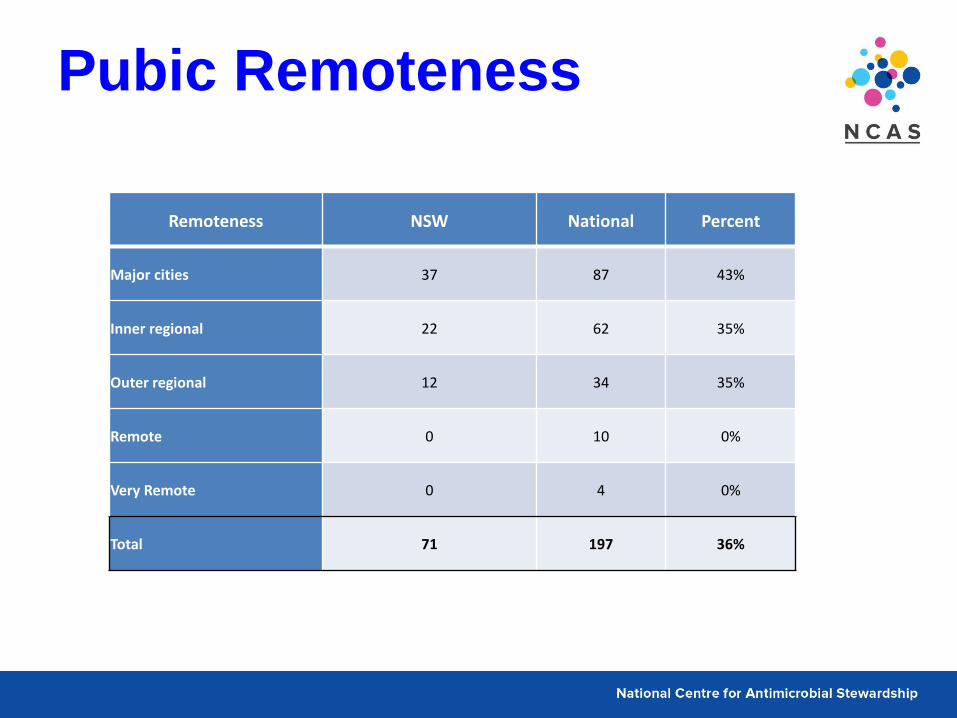
Pubic Remoteness
Remoteness NSW National Percent
Major cities 37 87 43%
Inner regional 22 62 35%
Outer regional 12 34 35%
Remote 0 10 0%
Very Remote 0 4 0%
Total 71 197 36%

NSW Data

Key Performance Indicators
Key Indicator NSW 2013 NSW 2014 National
2013
National
2014
Indication documented (Best practice >95%)
71% 76% 71% 74%
Surgical prophylaxis given >24hrs (Best practice <5%)
48%* 50%* 42%* 36%*
Compliance with
guidelines
Compliant
(Therapeutic Guidelines
& local guidelines)
59% 52% 60% 56%
Directed Therapy - 11% - 10%
Non-compliant 26% 27% 23% 24%
No guideline available 9% 5% 11% 5%
Not assessable 6% 4% 6% 5%
Appropriateness
Appropriate
(optimal & adequate) 69% 70% 71% 72%
Inappropriate
(suboptimal & inadequate) 26% 26% 23% 23%
Not assessable 5% 4% 6% 5% * where surgical prophylaxis was selected as the indication
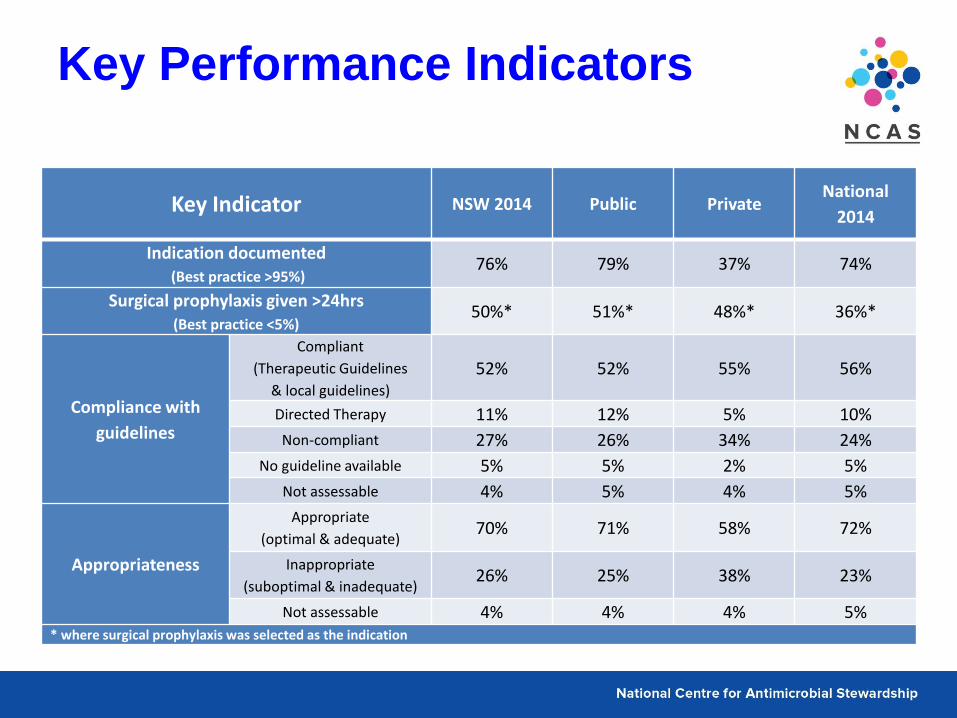
Key Performance Indicators
Key Indicator NSW 2014 Public Private National
2014
Indication documented (Best practice >95%)
76% 79% 37% 74%
Surgical prophylaxis given >24hrs (Best practice <5%)
50%* 51%* 48%* 36%*
Compliance with
guidelines
Compliant
(Therapeutic Guidelines
& local guidelines)
52% 52% 55% 56%
Directed Therapy 11% 12% 5% 10%
Non-compliant 27% 26% 34% 24%
No guideline available 5% 5% 2% 5%
Not assessable 4% 5% 4% 5%
Appropriateness
Appropriate
(optimal & adequate) 70% 71% 58% 72%
Inappropriate
(suboptimal & inadequate) 26% 25% 38% 23%
Not assessable 4% 4% 4% 5% * where surgical prophylaxis was selected as the indication

Inappropriateness by
Remoteness
Remoteness Inappropriate Total prescriptions Percent
Major cities 1064 4449 24%
Inner regional 341 1337 26%
Outer regional 110 371 30%
Remote 0 0 0%
Very remote 0 0 0%
Grand Total 1515 6157 25%

Top 15 indications
106
107
116
131
182
196
198
199
203
213
249
266
493
693
814
0 100 200 300 400 500 600 700 800 900
Osteomyelitis - Bacterial
Sepsis: directed therapy (Gram positive bacteraemia includes…
Febrile neutropaenia - Bacterial
Pneumonia: hospital acquired (HAP) - Bacterial
Wound infection: surgical - Bacterial
Medical prophylaxis - Fungal
Pneumonia: aspiration - Bacterial
Medical prophylaxis - Bacterial
Sepsis: empirical therapy (organism unknown) - Bacterial
Indication Unknown - Pathogen Unknown
Chronic obstructive pulmonary disease (COPD): infective exacerbation -…
Cellulitis/Erysipelas - Bacterial
Urinary tract infection (UTI) - Bacterial
Surgical prophylaxis - Bacterial
Pneumonia: community acquired (CAP) - Bacterial

Top 15 Inappropriate
Indications
18
20
27
28
30
34
43
44
48
68
74
103
133
197
371
0 50 100 150 200 250 300 350 400
Osteomyelitis - Bacterial
Bronchitis - Bacterial
Wound infection: non-surgical - Bacterial
Cholecystitis - Bacterial
Medical prophylaxis - Bacterial
Pneumonia: hospital acquired (HAP) - Bacterial
Pneumonia: aspiration - Bacterial
Sepsis: empirical therapy (organism unknown) - Bacterial
Wound infection: surgical - Bacterial
Indication Unknown - Pathogen Unknown
Cellulitis/Erysipelas - Bacterial
Chronic obstructive pulmonary disease (COPD): infective exacerbation -…
Urinary tract infection (UTI) - Bacterial
Pneumonia: community acquired (CAP) - Bacterial
Surgical prophylaxis - Bacterial

Top 15 Antimicrobials
150
169
184
185
189
212
220
270
272
389
395
408
439
571
752
0 100 200 300 400 500 600 700 800
Nystatin
Trimethoprim-sulfamethoxazole (Bactrim)
Ciprofloxacin
Gentamicin
Doxycycline
Benzylpenicillin
Vancomycin
Flucloxacillin
Azithromycin
Cephalexin
Piperacillin-tazobactam (Tazocin)
Amoxycillin-clavulanic acid (Augmentin or Augmentin Duo Forte)
Metronidazole
Cephazolin
Ceftriaxone

Top 15 Inappropriate
Antimicrobials
31
31
36
36
37
41
52
53
77
108
122
132
182
226
227
0 50 100 150 200 250
Amoxycillin
Ampicillin
Benzylpenicillin
Vancomycin
Doxycycline
Gentamicin
Ciprofloxacin
Flucloxacillin
Piperacillin-tazobactam (Tazocin)
Azithromycin
Metronidazole
Amoxycillin-clavulanic acid (Augmentin or Augmentin Duo Forte)
Cephalexin
Cephazolin
Ceftriaxone

Antimicrobials for CAP by
inappropriateness
1
1
1
1
1
1
2
2
2
2
2
2
3
4
6
6
7
10
14
16
27
41
45
0 5 10 15 20 25 30 35 40 45 50
Cefepime
Erythromycin
Gentamicin
Lincomycin
Moxifloxacin
Vancomycin
Cefaclor
Cephazolin
Ciprofloxacin
Clindamycin
Metronidazole
Ticarcillin-clavulanic acid (Timentin)
Ampicillin
Cephalexin
Amoxycillin
Benzylpenicillin
Piperacillin-tazobactam (Tazocin)
Clarithromycin
Doxycycline
Roxithromycin
Amoxycillin-clavulanic acid (Augmentin or Augmentin Duo Forte)
Azithromycin
Ceftriaxone

Antimicrobials for SAP by
inappropriateness
1
1
1
1
2
3
4
4
5
5
6
10
10
10
19
26
30
86
147
0 20 40 60 80 100 120 140 160
Benzylpenicillin
Piperacillin-tazobactam (Tazocin)
Ticarcillin-clavulanic acid (Timentin)
Trimethoprim-sulfamethoxazole (Bactrim)
Chloramphenicol
Trimethoprim
Cefaclor
Clindamycin
Ampicillin
Ciprofloxacin
Flucloxacillin
Amoxycillin-clavulanic acid (Augmentin or Augmentin Duo Forte)
Gentamicin
Vancomycin
Cefalothin
Ceftriaxone
Metronidazole
Cephalexin
Cephazolin

Reasons for inappropriate
SAP prescribing
3
4
8
16
25
60
81
172
0 20 40 60 80 100 120 140 160 180 200
Allergy mismatch
Microbiology mismatch
Spectrum too narrow
Spectrum too broad
Incorrect route
Incorrect dose/fequency
Antimicrobial not indicated
Incorrect duration

Future
Directions

Future Directions
• Further improvements to the NAPS
website and database
• User training and credentialing
• Sharing, reporting and ownership of data
• More comprehensive reporting and
benchmarking functionality
• Further recruitment of hospitals

Aged Care NAPS

Aged Care NAPS
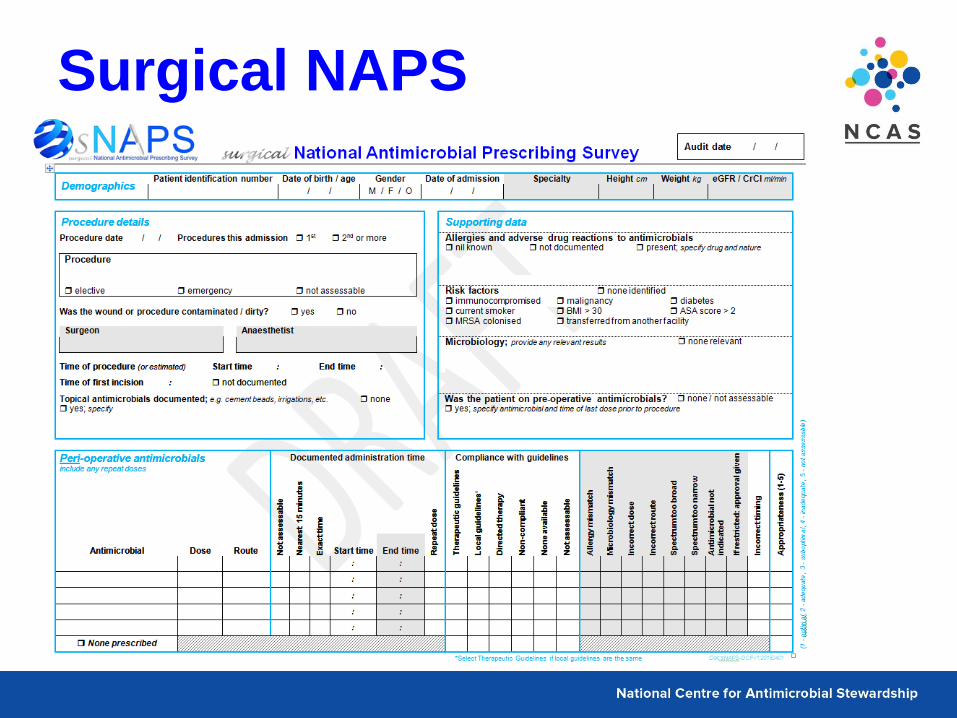
Surgical NAPS

Surgical NAPS

Further NAPS
• Veterinary NAPS
• General Practice NAPS
• Modules
– Indication / antimicrobial audits
– Vancomycin / gentamicin dosage
– IV to oral switch
– Quick NAPS

Acknowledgements
• Melbourne Health, Peter Doherty Institute for Infection and Immunity – A/Prof Karin Thursky – Director National Centre for Antimicrobial Stewardship
– A/Prof Kirsty Buising – Deputy Director National Centre for Antimicrobial Stewardship
– Ms Caroline Chen – Project Manager, Antimicrobial pharmacist
– Dr Noleen Bennett – Project Officer, Infection control consultant
– Ms Sonia Koning – Project Officer, Antimicrobial pharmacist
– Mr Simon Burrell – Database Manager
– Mr Roland Laguitan – IT Analyst
– Mr Xuebing Yang – Software developer
– Mr Danish Sultan – Software developer
• Australian Commission on Safety and Quality in Health Care – Ms Kathy Meleady – Director, Commonwealth Programs
– Ms Liz Metelovski – Senior Project Officer
– Prof John Turnidge – Senior Medical Advisor


Thank You