resistance to dapsone and rifampin in mycobacterium leprae...
TRANSCRIPT

CIENTIFICAL INVESTlGATION ARTICICLES
Resistance to dapsone and rifampin in Mycobacterium leprae isolated from leprosy patients of São Paulo State
Resistência a dapsona e rifampicina em Mycobacterium leprae isolado de pacientes portadores de hanseníase no Estado de São Paulo
Abstract In 1981, reports of resistance to dapsone and rifampin led W HO to reçommend multidrugtherapy in leprosy (realment . Doe of its main goa ls is preventing lhe selection of drug-resistant slrains of mulan! bacleria. Dapsone was lhe fi rs! drug wh ich was experimenlally proved la induce resistance; Ihis became possible only afier lhe mQu$e footpad inoculalion technique was standardized, in 1960. There are some importanl criteria to $uspect lhe existence of resistance, $uch as: relapses in multibacillal)' palients already ,trealed ar undergoing tll::dlrmml or unsatisfaclOry cl inicai response. Our study aimed aI detcction of dapsone and rifampin resislant strains among 40 Irealed patients with cl inicai signs of relapse, from different cilies ofSão Paulo Slale and its capital, employing the mouse foolpad inoculalion. We delecled dapsone resistant bdcilli in " cases. Among Ihem, 5 showed 10lal resislance, 1 inlermediary resistance and 5 partial resistance. Rifampin resistanl bacilli were detected in only IwO cases. We did nOI detect any case of multiple resistance. The high levei of resistance to dapsone is probably a consequence of many years of sulfone and sulfone derivalive monotherapy. As for the rifampin, lhe drug was probably irregul arly used in mo nolherapy; or the patient may have used it previously to treal another d isease. The detection of resiSlanl bilôlli in patients who do not s"how ,:my clinicai improvement, or relapse after trealmenl, is an important malter to be conside red in the future prevention of new cases of resistance. lhe emergence of resistant slrains, especially to rifampin, as well as its dissemination, may cause difficu lties la lhe patients's treatmenl and jeop<lrdize the leprosy control programs.
J(ey words: Mycobacterium leprae; resistance; dapsone; rifampin
B Sunn. Madeir. Oi6<io. InRiMO Lauro dr Sou .. U""'. Rod. Cmte. I0Io R. 8.,ros. km 216. 8.uru/SP _ 8' ... 1. CEP 170Jo·971. microlii l".b,
, Traboolno ~. I i~>do <om .poio fi,,",n(~iro d. Fur>d.ç~o P.uli". COI111 •• H.;rn_I.~.
18io1ogiSl. Sdenlifoc Re.e.rche< IV. Chiei" o( Inslilulo l'uro do; Sou .. lim'" Mic'objology Technic.1 Tum. Ma""" in TR"lfliCal ni_ .....
1M.D., Derm,noIogôSl. Lo-prology ar><! !..on i ... y Do-rmolology Oivi,ionI SP. ~"",nin i@terr •. com.bt.
<Biologi;r.. InSlirulO L.um dr SoYn Li"",. S 8101''lli'' ln\litutO L""'" dr SoY .. Li"",. &M.D .• Oo!rm. tologi .... LepwlogiSl. E_riM R ....... n:he< 01 InSlirutO l.uro dr Souza
l ima.
Suzana Madeira Di6riD 2 Marl i Izabel Penteado Manini 3
Lazara Moreira Trino 4 Beatriz Gomes Carreira Sanori 5
Diltor Vladimi r Araújo Opromolla 6'11'
Introduction Several reports of secondary and primary
resistance lo dapsone (DOS) and also to rifampin (RMP) led lhe World Heahh Organization (WHO) lo recommend, in ' 981, a new therapeulic scheme: lhe multidrugtherapy (MOT). This scheme should nol only cure lhe palient and avoid lhe developmenl of incapac ilies, bul also preveni lhe selection of drug resistant mulant slrains, especially among mu ltibacillary patients (MB)'. With a partially supervised scheme and fixed doses, MDl has conlributed in a remarkable way do the disease's cure, reducing prevalence rales in almosl 90%. In the beginning of 2004, there were 460,000 patients under Ireatmenl ali over lhe world1 . Despile the demonstrated efficacy of this scheme, il could nol avoid the appearance Df slrains resislant lo some of its drugs, even many years after qf ils inlroduction.
In respect lo epidemiology, Ihere are two cases of resislance: secondary or acquired resistance, resulting from inadequale Ireatmenl and generally accompanied of initial clinicai improvemenl, and subsequent worsening, and primary resistance, Ihal manifesls itself in p<llienls who didn'l received any previous Irealmenl. In this case, infeclion has probably been caused by baciJli o riginary from a patient with 5econdary resislance3 .
Early observalions about cases of resislance were raiseel in lhe late 40'S4 . AI this time, sulfonamide drugs as promin, diasone and DOS (4,4'-diaminodiphenylsulfone), were already used to Ireat lhe disease.
DOS was lhe first drug experimenlally proven to induce bacillary resistance. lhal was possible only after Shepard standardized the footpad inoculalion of isogenic mice, in 19605. Following this melhod, Pelil et af>. were able to prove experimentally, in 1964, lhe first cases of bacilli resislance lo DOS. When we discuss resistance, Ihis is the mosl important anli-Ieprosy drug because it was largely used as monolherapy, for more Ihan 30 years. lhe panern of resiSlance is classified as partial lIowl. intermediary or tOlal (high), according to lhe bacilli's abilily to reproduce in mouse lreated wilh O,ooolg%, O,OO1g%

Hansenologia Internationalis
or 0,01 g% of DDS, respectively, in their feed. The concentration Df 0,01 g% corresponds to a dose Df 100 mg to human beings3 .
'Many years later, even with the introduction of MDT, severa I reporls of primary and secondary resistance, not only to DOS but al50 to RMP, clofazimine (CLO) and ofloxacin (OFLOl, were described in various countries7-11.
lhe Instituto Lauro de Souza Lima has been doing experimental studies using lhe Shepard's mouse foot pad technique, since 1986. Analyzing 30 lepromatous patients from Bauru (SPl, who constituted a risk group to sulfone resistance, Costa et aI. 13
obtained a 2,86'% resistance rale to DOS. Ahhough significant, this figure does nol express our epidemiologic reality, probably because the techniques for resistant bacilli detection - mouse footpad inoculation and molecular biology - are expensive and nol available in most Df laboratories.
There are important cri teria to suspect resistance, such as relapses in multibacillary patients already treated or undergoing treatment, or unsatisfactory clinicai response that calls the clinician's attention. The aim of our study was to detect DDS ann RMP resistant strains among treated patients with clinicai signs Df relapse. lhese individuais came from various cities of the São Paulo State. In this study we used Shepard's mouse footpad technique.
Patients and Methods Patient.: from 1994 to 2002, we evaluated 40 treated patienls (n = 40) of both sexes, clinically diagnosed with lepromatous (30) or borderline lepromatous (10) leprosy. Ali patients had bacilloscopic index (BI) > 3+, with clinicai suspicion of relapse. Only 29 patients had their diagnosis confirmed by hislopathology. In 22 cases, skin biopsy showed the disease in activity; in one case with type 2 reaction and in another case, with reversal reaction. lhere were also five cases af regression. lhe patients were from São Paulo State and capital. They were referred to the ILSL by lhe SUS public health system. Nine cases were seen at lhe Divisão de Hansenologia e Dermatologia Sanitãria/SP, and 31 atthe ILSL. Ali ofthese patients reported having undergone some kind Df treatment (promin, diasone, dapsone, MDT-MB/ WHO); two patients could not inform which medicatian they had used. At clinicai dermatological evaluation, none of these patients were receiving treatment. lhe study included only those patients whose treatment had been concluded at least five years before, and who showed new lesions and positive 81 14. lhey were ali examined by a dermatologist for clinicai evaluation, biopsy collection and badlloscopic examination.
16
Biopsy: two fragments of lesion were collected. One was sent to histopathological examination, and the other was inoculated in a mouse's left footpad to test susceptibility to drugs. Biopsy processing for inoculation: baci/Ws DDS and RMP susceptibility tests were done according to Shepard's technique15. lhe biopsy was minced in a tissue homogenizer containing 2 ml of Hanks' balanced salt solution (HBSS Gibco BRl ®), to obtain the bacilli suspension. Afterwards, an amount Df 30 ml of the suspension was laid on microscopy slides, fixed and stained with the ZiehlNeelsen staining. Ali the procedures were carried out in antiseptic conditions, in laminar flow chamber.
Inoculation: 40 young BAlB/c mice of both sexes were inoculated by intradermal injection in the left hind footpad, with 104 baci/li/O,03 ml. The 0:';00015 were divided in five groups: control (diet without drugs), DDS 0,01 g%, DDS 0,001 g%, DDS 0,0001 g% and RMF 10 mgl kg. DDS (Sigma"') was added to dai Iy feed and RMF (Merck®) was administrated by gavage, once a week, for six months. lhe animais were kept in controlled environment, with an average temperature of 222(, receiving water and feed ad libitum.
Period of inoculation: the animais were anaesthetized and sacrificed by cervical dislocation ten months after inoculation; the footpad tissue was excised and processed following the protocol in use for the patient's biopsy, with subsequent counting of baci/li.
Results evaluation: the index of = 105 bacilli/footpad I b
was considered as significant bacillary multiplication. lhe results were interpreted as sensitive only when there was bacillary multiplication in the control group; resistant, when the multiplication occurred in the control group and also in any animal which had received DOS or RMP; inconclusive, whenever there wasn't bacillary multiplication among the animais of the control group and the treated animais. The interpretation of results for the cases of DDS resistance is exposed in Charl 1 .
Chart 1. Results interpretation of Mycobacterium leprae's resistance to dapsone
•• dll"l' IIIliripüonioo (dict wiI!J OIJS)
O,OI~% o,OOIr.". O,OOOlg%
"
• : • +
Dóório SM. ManiAi MlP, Trino lM. Sanori BCC,Op<omoU .. DVA Resi~e lo tbpK>nt anel rif ..... pin in MycobKlerium ~~ i~ated fmm Ifprosy p;llienlS ofSlo P.u lo Süle
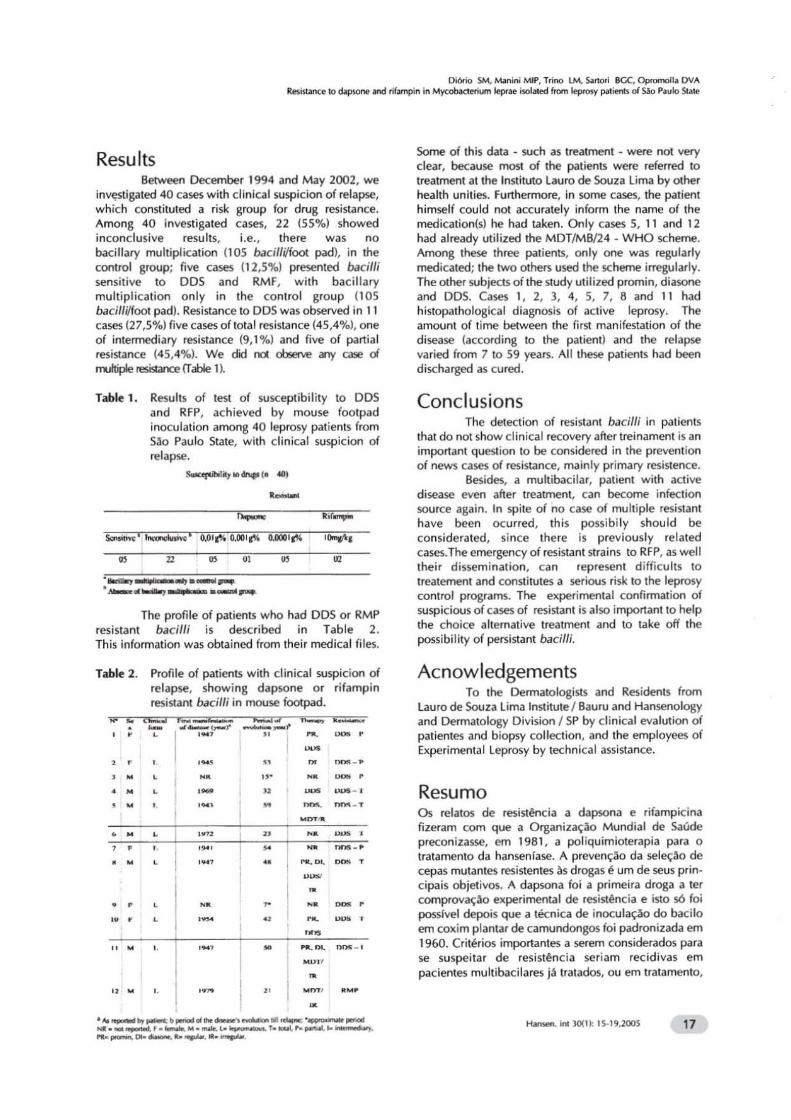
Results Between December 1994 and May 2002, we
i nv~tigated 40 cases with clinicai suspicion of relapse, which consliluled a risk group for drug resislance. Among 40 investigaled cases, 22 (55%) showed inconclusive resu lts, i.e. , there was no bacillary multiplication (lOS bacillVfoot pad), in lhe control group; five cases (12,5%) presenled bacilli sensitive to DOS and RMF, with bacillary multiplication only in the control group 1105 bacilfi/foot pad). Resistance to DOS was observed in 11 cases (27,5%) five casesoftOlal resistance (45,4%). one of intermediary resiSlance (9, 1 'fo) anel five o f partial resistance (45,4%). We did rd observe aTr( case c:i m.J~ resistance (T abre 1 ,.
l able 1. Results of test of susceplibilily 10 DOS and RFP, achieved by mo use foolpad inoculation among 40 leprosy patients from Solo Paulo State, with clinicai suspicion of relapse.
S-<fdoi:iI,. ... ~I. 40)
" " " " . .....,....-..,._._ .. .....,. ......... --. lhe profile of patients who had DOS or RMP
resi stant bacilli is described in Table 2. l his information was obtained from their medicai fi les.
Table 2. Profile of patients with clinicai suspicion of relapse, showing dapsone o r rifampin resistant bacilfi in mouse footpad.
, " " ,
, "
• 0 ,-,~,
,~ ,
,~,
. 0
........... --, " " " .
" .,
,..,. "
,- .-~ ~ .. .0 - , - _ ., - nI'>!\ . T
.~.
'0 ~ , - _ .. ~~. ~ • u_
• .0 ~ , ~ -,~
~~ _ . ,
...... ,., • . ~, o ••
."" __ .... poIoOOt bporiod ..... '"-.......... .. ~ • __ """'""
.. . ... --.'.-. ... ...... 1o~1 ....... ............. --..,.,
.... _DOo_Ilo ....... IIt . ....... .
Some of this data - such as lreatment - were no( very dear, because most of the patients were referred to Ireatment at the Instituto Lauro de Souza lima by o(her health unities. Furthermore, in some cases, lhe palienl himself could not accurately inform lhe name of lhe medication(s) he had taken. Only cases 5, 11 and 12 had already ut ilized lhe MDT/MB/24 • WHO scheme. Among these three patients, only one was regularly medicaled; lhe IwO olners used the scheme irregularly. lhe oIher subjects of the study utilized promin, diasone and 005. Cases " 2, 3, 4, 5, 7, 6 and 11 had hislopalhological diagnosis of aClive leprosy. The amounl o f time between the first man ifestation of lhe disease (according to the pa.tient) and the re lapse varied from 7 to 59 years. Ali these patients had been discharged as cured.
Conclusions The detection of resistant bacilli in palief'lts
that do not show cl inicai recovery after treinament is an important question to be considered in the prevention o f news cases of resislance, mainly primary resistence.
Besides, a multibacilar, palient with active disease even after treatment, can become infeclion source again. In spite of no case of multi pIe resistant have been ocurred, thi s possi bi1y should be considerated , since there is previously related cases.lhe emergency of resistant strains to RFP, as well Iheir dissemination, can represenl difficuhs to treatement and constitutes a serious risk to the leprosy conlrol programs. lhe experimental confi rmation of suspic ious of cases of resistant is also importanllo help the choice altemative treatment and lo take off the possibi lity of persistant bacilfi.
Acnowledgements To the Dermatologisls and ResidenlS from
Lauro de Souza l ima Institule I Bauru anel Hanseno logy and Dermal010gy Oivision I 5P by clinicai eva lution of patientes and b iopsy collOOlon, and lhe employees of Experimental leprosy by technical assistance.
Resumo Os relalOS de resistência a dapsona e rifampicina fizeram com que a Organizaçolo Mundial de Saúde preconizasse, em 1961 , a pol iquimioterapia para o tratamento da hansenlase. A prevençolo da seleçolo de cepas mutanles resistentes às drogas é um de seus principais objetivos. A dapsona foi a primeira droga a ter comprovaçolo experimental de resistência e isto só foi posslvel depois que a técnica de inoculação do bacilo em coxim plantar de camundongos foi padronizada em 1960. Critérios importantes a serem considerados para se suspei tar de resistência seriam recidivas em pacientes multibacilares já tratados, o u em tratamento,
H-. inI )()( I): IS· I,.2OOS 17

ou resposta clínica insatisfatória. Nosso estudo teve por objetivo detectar cepas resistentes à dapsona e rifampicina entre 40 pacientes tratados, com sinais clínicos de recidiva, procedentes de cidades do Estado de São Paulo e capital, utilizando a técnica de inoculação do bacilo em coxim plantar de camundongos. Foram observados bacilos resistentes à dapsona em 11 casos, sendo 05 de resistência total, 01 intermediária e 05 parcial. Bacilos resistentes à rifampicina foram observados em apenas 02 casos. Não se observou nenhum caso de resistência múltipla. O alto índice obtido de resistência à dapsona, provavelmente é decorrência de muitos anos de monoterapia sulfônica ou de seus derivados. No caso da rifampicina, provavelmente a droga foi utilizada de forma irregular, em monoterapia ou ainda, o paciente pode ter utilizado-a previamente para tratar outra moléstia. A detecção de bacilos resistentes entre pacientes que não melhoram clinicamente ou que recidivam após o tratamento, é uma questão importante a ser considerada na prevenção futura de novos casos de resistência. A emergência de cepas resistentes, especialmente à rifampicina, bem como a sua disseminação, pode trazer dificuldades ao tratamento do paciente e se constituir em ameaça aos programas de controle da hanseníase.
Palavras-chave: Mycobacterium lepra e; resistência; dapsona; rifampicina
References
2
3
4
World Health Organization Study Group. Chemotherapy 01 leprosy lor control programs. WHO Geneva; 1982. ( Technical Report Series,675).
World Health Organization. [homepage internet]: Elimination 01 Leprosy as a Public Health [updated 2005 Marchl. Disponível hltp://www.who.int/lep/
Ji B. Drug resistence in leprosy - a review. Lepr rev 265-78.
on the Problem
em:
1985; 56:
Floch H. La sullono-résistance du Bacille de Hansen. Archives de L ' InstituI Pasteur de la Guyane Française et de L' lnini 1957; 18: 1-9, publicação nO 429.
5 Shepard Cc. The experimental disease that lollows the
6
7
8
18
injection 01 human leprosy bacilli into lootpads 01 mice. J exp med 1960; 112: 445-57.
Pettit JHS, Rees RJW. Sullone resistance in leprosy. An experimental and clinicai study. Lancet 1964; 2: 673-4.
Guinto RS, Cellona RV, Fajardo, TI, Cruz EC. Primary dapsone-resistant leprosy in Cebu, Philippines. Int lepr other mycobact dis 1981; 49(4): 427-30.
Matsuoka M, Kashiwabara Y, Namisato Mycobacterium lepra e isolate resistant to rilampin, olloxacin and sparfloxacin. Int other mycobact dis 2000; 68 (4): 452-55 .
M. A dapsone,
j lepr
9
10
11
12
13
14
15
16
17
18
Gillis TP, Williams DL. Dapsone resistance in Mycobacterium leprae. Lepr rev, Workshop Proceedings 2000; 71(1), Suppl S91-5 .
Cambau E, Bonnalous P, Perani E, Sougakoff W, Ji B, Jarlier V. Molecular detection 01 rilampin and olloxacin resistance lor patients who experience relapse 01 multibacillary leprosy. Clin inlect dis 2002; 34: 39-45 .
Sekar B et aI. Drug susceptibility 01 Mycobacterium leprae: a retrospective analysis 01 mouse loot pad inoculation results from 1983 to 1997. Lepr rev 2002; 73: 239-44.
Shelty VP, Wakade AV, Ghate S, Pai W, Ganapati R, Antia NH. Viability and drug susceplibilily lesting of Mycobacterium leprae using mouse loolpad in 37 relapse cases 01 leprosy. Inl j lepr olher mycobacl dis 2002; 71(3): 210-1 7.
Cosia HC, Opromolla DVA, Madeira S, Marques FB, Martelli ACC, Ura S. Prevalência de sulfono resislência em pacienles hansenianos do município de Bauru, Eslado de São Paulo. Hansen inl 1993; 18(1/2): 5-10.
World Health Organization leprosy - The THELEP Approach. mycobact dis 1981; 49(4): 421-25.
Dapsone-resistant Inl j lepr olher
World Heallh Organization. Laboratory Techniques for Leprosy. Geneva: WHO; 1987.
Ji B. Drug susceplibility testing of Mycobacterium leprae. Inl j lepr other mycobact dis 1987; 55(4) Suppl 830-35.
Opromolla DVA, Cosia HC, Oliveira PRD. Resislência medicamenlosa múltipla secundária na hanseníase. Hansen inl 1993; 18(1 /2): 11-6.
Dallas WS, et aI. Cloning, sequencing and enhanced expression of the dihydropteroate syn Ihase gene 01 Escherichia coli MC 4100. J bacteriol 1992; 174(18): 5961-70.
19 Fermer C, Swedberg G. Adaptation lo sulfonamide resistance in Neisseria meningitidis may have required compensatory changes lo retain enzyme function: kinetic analysis of Dihydropleroate syn thase Irom Neisseriã menir.gitidis expressed in aknockoul mutant 01 Escherichia coli. J bacteriol 1997; 179(3): 831-37.
20 Lopez P, Espinosa M, Greenberg B, Sacks, 5 A. Sullonamide resistance in Streptococcus pneumo niae: DNA sequence 01 the gene encoding dihy dropteroate synthase and characterization 01 the enzyme. bacteriol 1987; 169(9): 4320-26.
21 Jacobson RR, Hastings RC. Rilampin resistant lep rosy. (Lelter) Lancet 1976; ii:1304-5.
22
23
24
25
Jacobson RR. Final report 01 the WHO regional working group on drug policy and operational research in the leprosy Philippines; 1981 ; 10.
Guelpa-Lauras M, Brucker leprosy. Int ' 52:101-2.
CC, Grossel G. Nine cases
lepr other
programme; ManHa,
JH, Constant-Deportes 01 rilampicin-resistant
mycobact dis 1984;
Grosset JH et aI. Study 01 39 documented relapses 01 multi bacillary leprosy after treatment with rilampin. Int j lepr other mycobact dis 1989; 57:607-14.
Honoré N, Cole 5T. Molecular basis resistance in Mycobacterium leprae.
agents chemother 1993; 37: 414-18.
01 rilampin Antimicrob
Diório SM. N\;lnini MIP, T,ino LM, SilnOf; BGe, Opfomolla OVA l!esist3nc~ lo dopsonoe an<! nfampin in My<:obactl"rium Iep,..., i~la!ed lrom ieptosy p,Uients 01 SAo Paulo Sla!e
26 Levy L. Mulliplicalion 01 MycobaclerilJm leprae in nQ<mal miee. Inl j lep' OIher my.:ob.1el dis 1987; 55(4) Suppl 814·1 8.
27 GlJptil UO, Kaloch K. Singh H8. Assessmenl 01 viabi li ty by no, . mal MfP aOO badllary ATP biolumi ne~ence assay in mull ibadU .. ry nse5 Ilealed wilh an MOT using eonventional as well as newer drugs like minocycline .. OO oAox .. dn. IOOian j lepr 2000; 72: 437_ 42.
28 Subç()mminee On clinicai trials 01 lhe ehemolherapy of lep'osy (THELEP). Scienlifie wo,king g'oup 01 lhe UNOP{lNorld 8ank.M/HO sped .. 1 programme for .esea,eh and t.aining in tropical disease. lhe THELEP conl'olled clinicai d.ug '.ials. Int j lepr other mycobael dis 1987; 55: 864-71.
29 Almeida JG, Chacko CjG. Christian M. l he signifinnce 01 dapsone (DOS)- resistanl Myc~clerilJm leprae in unlrealed p.llients. Inl j lep. olher mycobact dis 1983; 51: 374-77.
Gupla UO. Kaloch VM. Underslanding lhe phe nomenon 01 pe.sisteroce in mycobdCte,ial infeclions. Indian j lepr 1997; 69(4): 385-93.
31 Levy L. Trealmenl failures in leprosy. In! lepr OIher mycobact dis 1976; 44:177_82.
Han-..intlOlO:1S·19.2005 19