report on health care workers training for...
TRANSCRIPT

REPORT ON HEALTH CARE WORKERS TRAINING FOR NUTRITIONAL ASSESSMENT
OF TUBERCULOSIS (TB) PATIENTS
FOR KAKAMEGA COUNTY
DATES: 6th
to 10TH
SEPTEMBER, 2015
ACTIVITY …….5.1………..
VENUE: WESTGATE INN BUNGOMA
Florence Emali - CNC, KAKAMEGA
9/14/2015
Email: [email protected] When replying, please quote Ref. No: TR. 1 VOL. III/012
County Director for Health Services
Kakamega County, P.O. Box 359,
Kakamega.
Date: 14th September, 2015
MINISTRY OF HEALTH

Group photo of the participants outside Westgate Inn
Participants performing a role play of a nutrition counseling session

EXECUTIVE SUMMARY
The Nutrition in TB training was supported by NEPHAK. It was held for four days i.e. 7th
to 10th
September 2015. Participants were drawn from all the twelve sub counties of Kakamega County.
National training guidelines were used for the training. The goal of the training was to equip
health care workers with nutrition knowledge and skills needed to prevent and intervene on
uncomplicated nutrition problems.
Various teaching methodologies were used including lecture, discussion, demonstration role
plays e.t.c. The topics covered were :- background information and basics of TB, Leprosy, PAL
and lung disease burden in Kenya, Nutrition assessment, Nutrition care process in TB Leprosy
and lung disease, and Nutritional management of COPD, Key definitions, Food security, Food
and Drug interactions among others. Practical were done in class for assessments and
demonstrations of data tools. Field visit was also organized for the participants to Bugoma
County Hospital. The post test results showed that learning had taken place among the
participants as there was marked improvement. Participants then made an action plan. Some of
the activities done are captured in photos within this report.
INTRODUCTION/ BACKGROUND
Kakamega County has a projected population of 1,660651 and a population growth rate of 2.54%
(KNBS 2009) annually with the population density of 3,050.3 per square km. It is located in
Western part of Kenya that is predominantly Luhya tribe, and it borders Trans Nzioa County to
the North, Nandi County to the East, Vihiga County to the South and Busia County to the West.
It is made up of twelve sub counties which are as follows:- Likuyani, Lugari, Malava,
Navakholo, Lurambi, Shinyalu, Ikolomani, Khwisero, Butere, Mumias East, Mumias west and
Matungu.
County Health Indicators
Among the top ten causes of morbidity and mortality among children under five are
ARI/Pneumonia, and severe acute malnutrition. Among adults, the top ten causes of morbidity
and mortality are Diseases of the respiratory system, ARI/Pneumonia/TB, and malnutrition.
Major risk factors causing morbidity and mortality in County
Micronutrient deficiencies, sub optimal feeding practices, unsafe deliveries, malnutrition are
some of the top ten risk factors causing morbidity and mortality in the County.
Nutrition and TB indicators
There is a lot of under nutrition in Kakamega County. Stunting among children under five is at
28.4%. KDHS 2014, 10.3% of them were underweight
There has been a knowledge gap among health workers attending to TB and malnourished
clients. Some clients would be put on food supplements but not as per the standard guidelines.
This would mean that though the client responded on treatment and became smear negative, he
or she would still be wasted.

Table 1: Status of TB and Nutrition Related MDGs for Kakamega County
Goal Status
Goal 4:
To reduce child mortality
95/1000
Goal 5:
To improve maternal health
Maternal Mortality 531/100,000
Goal 6:
To combat HIV/AIDS, TB Malaria and
other diseases
HIV Prevalence (5.7%)
PMTCT Prevalence (8.2%)
TB cure rate (86.3%)
TB Case detection rate (46%)
Source: Kakamega County Nutrition Action Plan 2013/2014- 2017/2018
Introduction to the Training
Under nutrition increases the risk of tuberculosis and in turn tuberculosis can lead to
malnutrition. Under nutrition is therefore highly prevalent among people with tuberculosis. It has
been demonstrated that under nutrition is a risk factor for progression from tuberculosis infection
to active tuberculosis disease and that under nutrition at the time of diagnosis of active
tuberculosis is a predictor of increased risk of death and tuberculosis relapse.
The training was supported by NEPHAK and was held in Westgate Inn, Bungoma County. A
total of twenty-five participants attended the meeting. The cadres were: Clinical Officers, Nurses
and nutritionists as per the attendance list. Four facilitators were used at county and sub county
level, 2 NEPHAK officer- Olivia Khakasa and Arnold Otieno
The training used the standard guidelines that were sent from National office. A pre and posttest
was administered to determine the level of knowledge gained.
The meeting started at 9.00am with a word of prayer form Nancy Muyeka. Introductions were
done using a standardized format. Norms set, leaders from among the participants were elected
and rapporteurs for the various days were also identified.
Leaders/roles
The leaders selected were as follows:
Chairman Nancy Muyeka
Timekeeper Bernard Kinara
Energizer Tatuli Simwa

Spiritual Leader Leah Aliela
Norms
Norms established by the class to guide them for the four days were:
Phones on silent mode
Start and end with a word of prayer
Punctuality: start at 8.30 am and end at 5.00pm
Respect each other’s opinion
Active participation
Goal
The goal of the training was to equip health care workers with nutrition knowledge and skills
needed to prevent and intervene on uncomplicated nutrition problems.
Carry out the nutrition care process during a field visit
Identify available linkages and referral systems in existence
Monitor and evaluate nutrition activities in the program
Specific Objectives
At the end of this course participants were be able to:
Understand TB in terms of epidemiology, patho physiology, classification, diagnosis and
treatment/intervention
Identify clients with Leprosy
Understand the nutrition care process for in and out patients and its integration in TB
management
Identify available linkages and the referral systems in existence
Monitor and evaluate nutrition activities in the program
Carry out the nutrition care process during a field visit
Methodology
Various training methodologies were used with the participants. The sessions were very
interactive and the participants participated actively. These methods were:
Lecture: For majority of the session especially when giving new information

Discussion: Issues were discussed based on the actual events happening in the facilities
guided by the facilitator.
Participatory: Clients were involved in the presentations
Field Visit: Participants were divided into 2 groups and went to Bugoma County Hospital
where they visited the TB clinic, CCC and Nutrition department.
Practicals: Participants were divided into 4 groups of which they worked in throughout
the training Topics Covered
Day 1
Topics covered included Background information and basics of TB including the history, how it
is spread and the associated risk factors. This included prevalence. Classification, Diagnosis and
treatment of TB then followed in children, specialized areas,. Participants were then taken
through the relationship between TB and HIV. Drug resistance TB was then discussed including
its epidemiology, classification, diagnosis and medications. Practical Approach to Lung health
approach was then introduced. Lastly, participants were taken through how to identify a leprosy
case and medications to give.
Day 2
Introduction to nutrition. Various definitions and aspects of nutrition were covered. Macro and
micronutrients requirements including examples and sources were addressed using both the plate
model and food guide pyramid. Categories of malnutrition, pathophysiology of malnutrition,
relationship between TB and Malnutrition and the Nutrition care process were tackled. After tea
break nutrition assessment methods were done. This was followed by classification of nutritional
status based on the findings and how to write a PES statement under nutrition diagnosis. The
session also tackled various types of interventions and the recommended intervention for each
situation based on the cut off points. There was a counseling session role play by the participants.
Lastly participants took measurements for weight height MUAC waist and hip Circumference,
and calculated Waist Hip ratios, BMI and Z scores.
Day 3
During the morning session, food and drug interactions were covered. Various terminologies
were defined, metabolism of drugs, risks of food drug interactions, benefits of minimizing risks,
patients at risk and drug related risk factors, drugs that increase/decrease appetite, cause diarrhea,
raise blood sugar, how food and drugs interact including for those on enteral feeding using
specific examples of drugs available in facilities. Food and Nutrition security were defined, and
methods of assessing them explained including ways and actions to improve food security.
Follow up, types and its importance, importance and reasons for referral, linkages, networking,
how to net work and who to network with were also covered. The participants were taken
through the commodities available for management of malnutrition and what to give based on
the classifications and quantities including entry and exit criteria.
Day 4

Management of Asthma and COPD were covered. This focused on locally available foods that
alleviate and those that trigger. Monitoring and evaluation was introduced. Participants were
taken through all the tools and how to fill them. They were then taken through the nutrition
reporting tools including those that capture nutrition in TB management data. Participants were
taken to Bungoma County referral hospital in two groups. They visited the TB clinic and CCC to
ascertain the actual practices on the ground based on what they had learned in class. Feedback of
the visit was then done in class including group work for other assignments
ANNEX
LIST OF PARTICIPANTS
Name Sex Age Id /no. Phone no. Desgn Station
1 Mourine Ndombi F 28 24639859 0724151140 KRHN Mumias H/C
2 Lucy W. Kinuthia F 35 21722243 0723220117 NUT. O Malava C. Hosp
3 Grace N. Githuku F 30 24255055 0720238556 KRHN Bukaya H/C
4 Maureen Ndanyo F 40 12846130 0724445009 N.O Malava C.Hosp
5 Jackline S. Isuluti F 25 28625101 0719832497 NUT. O CGH
6 Irene Muhande F 30 22475587 0722998611 NUT. O Likuyani
SC/Hosp
7 Moreen Nandwa F 34 22472808 0723442635 NUT. O Lumakanda C.
Hosp.
8 Reuben Chivini M 43 1103269 0710640405 N.O Lumakanda C.
Hosp.
9 Priscillah M. Sheri F 42 13007817 0724956325 KECHN Khwisero H/C
10 Leah M. Aliela F 28 24748256 0720043126 NUT. O Matungu C. Hosp
11 Julia N. Wenani F 35 22385367 0710519573 N.O Navakholo SC.H
12 Anjelyne Were F 33 23356025 0705080832 KECHN Iguhu C. Hosp
13 Rose Cherop F 31 23109259 0727325242 R.C.O CGH
14 Rebeccah Tsalwa F 52 0933143 0720272919 N.O CGH
15 Benard Kinara M 31 24122228 0725354071 N.O Navakholo SCH
16 Musungu K. Lydia F 28 26631495 0715785951 NUT. O Matungu C. Hosp
17 Renson L. Bulinya M 53 7956787 0711228298 KRN Shinyalu H/C
18 Linda Litunya F 28 25185785 0729872675 NUT.O Khwisero H/C

19 Nancy M. Muchuta F 30 23912383 0727944684 NUT.O Butere CH
20 Vincent O. Oronyi M 29 24799252 0710484389 N.O Ileho H/C
21 Noel Khatiala F 34 22073227 0722278768 NUT.O Butere CH
22 Tatuli Simwa M 25 27864696 0723601188 RCO Lusheya H/C
23 Odhiambo Collin M 26 276813 0719822558 RCO Makunga H/C
24 Florence N. Mutura F 54 3857378 0712317549 N.O Likuyani SCH
25 Milcah Onzere F 28 24606897 0726089540 NUT.O Iguhu CH
26 Emilly Vuguza F 40 21619545 0712984762 SCTLC CGH Lurambi
27 Josina Sikolia F 44 11041465 0712799063 SC.NUT.O Iguhu CH
Ikolomani
28 Andole L. Mwale M 58 2573150 0722446868 CTLC CGH Kakamega
29 Florence E. Amakobe F 45 9625418 0724389904 CNUT.O CDH Kakamega
30 Olivia Khakasa F 30 24100864 0725315860 P.A NEPHAK
Kakamega
31 Arnold Otieno M 32 23147262 0721808523 P.O NEPHAK
Pre and Post Test Results
All the sessions had 100% attendance since the participants had earlier been prepared and
advices to avoid missing sessions.
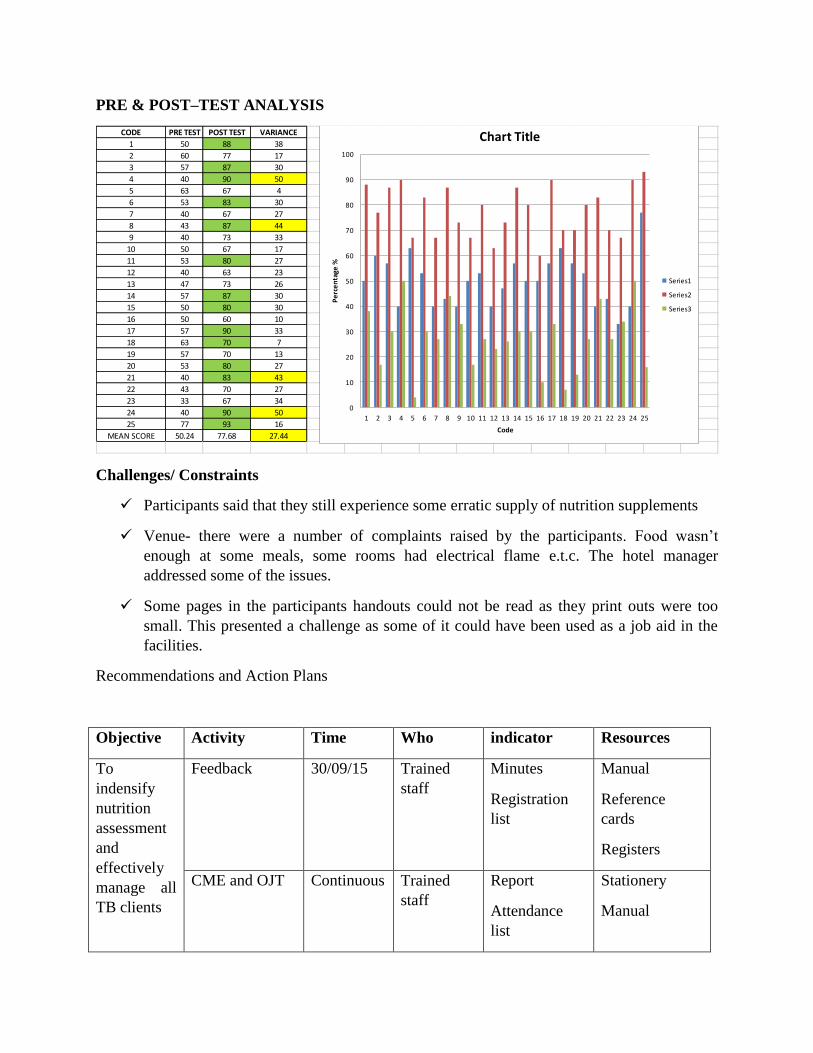
PRE & POST–TEST ANALYSIS
CODE PRE TEST POST TEST VARIANCE
1 50 88 38
2 60 77 17
3 57 87 30
4 40 90 50
5 63 67 4
6 53 83 30
7 40 67 27
8 43 87 44
9 40 73 33
10 50 67 17
11 53 80 27
12 40 63 23
13 47 73 26
14 57 87 30
15 50 80 30
16 50 60 10
17 57 90 33
18 63 70 7
19 57 70 13
20 53 80 27
21 40 83 43
22 43 70 27
23 33 67 34
24 40 90 50
25 77 93 16
MEAN SCORE 50.24 77.68 27.44
0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Pe
rce
nta
ge %
Code
Chart Title
Series1
Series2
Series3
Challenges/ Constraints
Participants said that they still experience some erratic supply of nutrition supplements
Venue- there were a number of complaints raised by the participants. Food wasn’t
enough at some meals, some rooms had electrical flame e.t.c. The hotel manager
addressed some of the issues.
Some pages in the participants handouts could not be read as they print outs were too
small. This presented a challenge as some of it could have been used as a job aid in the
facilities.
Recommendations and Action Plans
Objective Activity Time Who indicator Resources
To
indensify
nutrition
assessment
and
effectively
manage all
TB clients
Feedback 30/09/15 Trained
staff
Minutes
Registration
list
Manual
Reference
cards
Registers
CME and OJT Continuous Trained
staff
Report
Attendance
list
Stationery
Manual

Improve and
Intensify taking
of
anthropometric
measurements
in patients
Continuous Focal
Person
Reporting
tools
No. assessed
as per tally
and nutrition
registers
Anthropometric
equipment
Human
resource
Manage the
malnourished
clients as per
the guidelines
Continuous Focal
Person
No.
adequately
managed
Nutrition
supplements
Reporting tools
Monitoring and
Evaluation
Continuous Focal
Person
No. of reports Registers
Reporting
forms
Annex 3: Training evaluation form
Please tell us how satisfied or dissatisfied you were with the following.
1) How satisfied were you with the registration process?
Very Dissatisfied
Dissatisfied 4
Satisfied 14
Very Satisfied 6
2) How satisfied were you with the training materials provided?
Very Dissatisfied
Dissatisfied
Satisfied 16
Very Satisfied 8
3) Overall, how satisfied were you with the speakers / presenters?
Very Dissatisfied

Dissatisfied
Satisfied 6
Very Satisfied 18
4) Overall, how satisfied were you with the conference facilities?
Very Dissatisfied
Dissatisfied 17
Satisfied 6
Very Satisfied 1
5) How many sessions did you attend? 24
6) Did you feel the length of conference sessions were too long, just about right, or too short?
Too long 1
Just about right 19
Too short 4
Please tell us how much you agree or disagree with the following statements.
7) The content of conference sessions was appropriate and informative.
Strongly Disagree
Disagree
Agree 18
Strongly Agree 6
8) The conference was well organized.
Strongly Disagree
Disagree 3
Agree 17

Strongly Agree 4
9) Conference staff was helpful and courteous.
Strongly Disagree 2
Disagree 2
Agree 15
Strongly Agree 5
10) What kinds of sessions would you like to see included at future conferences? -------------------
allocate more time 5days 15
No response 4
Perdiem/half board 3
More practical 2
ANNEX 5: PRE AND POST TEST
Code: _________________________________________
Pre and Post -course questionnaire
Circle the correct answer
1. Which one is not the aim of treating is TB?
A. To cure patient of TB
B. To prevent death from TB
C. To decrease TB transmission
D. To prolong life
2. Apart from one all the following are roles of nutrition service provider at the TB clinic
A. Weight monitoring
B. HIV testing for all TB patients
C. Counseling on nutrition and TB
D. Meal-drug planning
3. Name the factors that contribute to DR TB
Provider risk factors Patient risk factors
Programmatic risk factors
4. List the 3 hierarchy’s of TB infection prevention and control

Administrative controls
Environmental (engineering) controls
Respiratory protection
5. Name the two groups of WHO classification for Leprosy
Pauci-bacillary leprosy Multi-bacillary leprosy (MB)
6. Nutrition as an essential complementary intervention to anti-Tb therapy will NOT
enhance
A. Food drug interactions
B. Patient rehabilitation
C. The immunity
D. Adherence anti-Tb drugs
7. All TB patients with BMI <16kg/m2 should be put on.
A. Therapeutic feeds
B. High protein diet
C. Supplementary feeds
D. General food ration
8. These are some of actions that improve food insecurity, which one is not?
A. Promote production and consumption of indigenous foods
B. Provide short term food assistance
C. Provision of anti Tb drugs
D. Link households to programs and organizations (CBOs, FBOs, NGOs, GOK) that
provide services on food/nutrition security
TRUE (T) or FALSE (F)
1. Monthly nutritional assessment is a critical nutrition action to people with Tb. T
2. Tb patients should carry out vigorous physical activity or exercises to strengthen or build
muscles, increase appetite and health. F
3. Those on medication should be informed about managing the drug-food interactions and
side effects that can be managed by food and nutrition interventions. T
4. Loss of body weight may also be a side effect of anti-Tb therapy. T
5. Individuals with a BMI less than 18.5 kg/m², indicates under-nutrition and a high risk of
illness and require hospitalization. F
6. Monitoring and evaluation of nutrition interventions for TB patients helps to assess the
degree to which progress is made T
Short answers

7. Explain the relationship between Tb and malnutrition (4marks)
8. Outline steps in nutrition care process for TB patients (4marks)
a. Nutrition Assessment b. Nutrition Diagnosis c. Nutrition Intervention d. Monitoring and Evaluation
9. List different ways of nutrition assessments ( 6marks)
a) Anthropometric measurements b) Biochemical assessments c) Clinical assessment (signs of deficiencies) d) Dietary ( 24 hour recall, food diary,) e) Economic and social status f) Functional
ANNEX 6: TIMETABLE
NUTRITION IN TB TRAINING PROGRAMME
DAY ONE
TIME PRESENTATION/ GROUOP TIME FACILITATOR ACTIVITIES
8.00-8.15 am Registration 15 minutes
8.15-8.45 am Introduction
Participants expectations, norms, group leaders for each day
30 minutes
8.45-9:15 am Opening Remarks Course overview, Objectives of the course,
30 minutes
9:15-9:45 pretest 30minutes
9:45-10:30 • Background information and Basics of TB
45 minutes
TEA BREAK
10:30- 10:45am Classification, diagnosis and treatment of TB 1hour
10.45 -11.15am TB/ HIV relationship 30 minutes
11.15- 11:45am Drug resistance TB 30minutes
11:45-1:00pm PAL 1hour 15 minutes

LEPROSY
1.00-2.00 pm LUNCH
2.00 – 2.25pm Infection prevention and control 25 minutes
2.25- 2:55pm 30 minutes
3:00 – 3:30pm 30 minutes
3:30-4:00pm Introduction to nutrition 30 minutes
4.00-4.30 TEA BREAK
DAY TWO
TIME PRESENTATION TIME FACILITATOR ACTIVITIES
8.00-8.15 am Prayer, Recap 15 minutes
8:15-8:45am Introduction to nutrition and definitions 30minutes
8.45-9:15am Patho physiology of malnutrition 30minutes
9:15-10:00am Relationship between nutrition, leprosy, TB and lung
disease
45minutes
10:00-
10:15am
The link between nutrition and TB 15Minutes
10:15-
10:30am
The consequences of malnutrition in TB 15Minutes
10.30-11.00
am TEA BREAK
11.00 -
11:20am
Role of nutrition in leprosy 20 minutes
11;20-12-
05pm
Introduction to nutrition care process in TB
management
45minutes
12:05-1:00pm Nutrition assessment 55minutes
1.00-2.00 pm LUNCH
2:00 –5;00 pm Nutrition assessment practical 3hours
DAY THREE
TIME PRESENTATION FACILITATOR ACTIVITIES
8.00-8.15 am Prayer, Recap 15 minutes
8.15-9:15am Food- drug interactions 1 hour
9:15-10:00am Food and nutrition security in relation to TB 45Minutes
10.00-10.30 am
TEA BREAK
10.30-11.45 am Nutrition commodities in relation to TB 1 hour 15 min

11.45-1.00 pm Dietary management of lung disease 1 hour 15 min
1.00-2.00 pm LUNCH
2.00-3.00 pm Monitoring and Evaluation in Nutrition and TB 1 hour
3.00-4.00pm Identification, accuracy and completion of M&E
tools in DLTLD
1 hour
4.00 –5.00 pm Discussions
4.30 – 5.00 pm TEA BREAK
DAY FOUR
TIME PRESENTATION FACILITATOR ACTIVITIES
8.00-8.30 am Prayer and Recap 30 min
8.30-10.00 am Preparation steps 1 hour 15 min
TEA BREAK
10.30 -1.00pm Field Visit 2 hours 30 min
1.00-2.00 pm LUNCH
2.00 – 4.00 pm Post-test and Closing 2 hours
4.00-4.30 TEA BREAK
One of the participants receives her certificate from the CNC

Energizer session
Report by:
Florence Emali, CNC, Kakamega County
Signed:__________________________ Stamped:___________________________________
Andole Mwale, CTLC Kakamega County
Signed:______________________________Stamped:_________________________________
Report Received by NEPHAK