renovascular disease daniel shoskes md, msc, frcsc professor of surgery/urology glickman urological...
TRANSCRIPT

Renovascular Disease
Daniel Shoskes MD, MSc, FRCSC
Professor of Surgery/Urology
Glickman Urological and Kidney Institute
Cleveland Clinic

• Pathophysiology
• Classification of Lesions
• Clinical Evaluation
• Medical and Surgical Management
• Renal Artery Aneurysm
Overview

Goldblatt Dog Models
ARB/ACE inhibitors help Only help when Na depleted

Ischemic Nephropathy
• Does not correlate with hypertension
• Progressive azotemia in pt with risk factors
for atherosclerotic disease
• Progresses through nephrosclerosis and
atheroemboli
• Treatment of hypertension will not improve
renal function, may actually exacerbate

Diameter and Blood Flow

• Atherosclerotic (70%)
• Fibromuscular Disease (30%)
Classification

Fibromuscular Disease
Medial Fibroplasia: 77%
Perimedial Fibroplasia: 10%
Intimal Fibroplasia: 10%
Fibromuscular Hyperplasia: 3%

Atherosclerosis
• typically a systemic disease
• involves proximal 2 cm of artery
• may only be seen on oblique views
• progression common, at least 50% in 2 years
• 10-15% progress to occlusion
• can cause hypertension and Renal Failure

Medial Fibroplasia
• most common fibrous
• women 25-50
• commonly bilateral
• "string of beads"
• involves distal 2/3 and
branches
• progression less
common

Clinical Clues to RVH
• HTN onset < 30 yrs or > 55
• sudden onset, short duration
• lack of family history
• difficult to control
• malignant crisis
• bruits
• disseminated atherosclerotic disease
• renal size disparity

Key Diagnostic Points• Captopril provocation
– reduction of GFR detected by nuclear scan• best predictor of surgical cure (spec 93-98%)
– increased PRA (off most drugs)• Renal Vein Renins
– ipsilateral hypersecretion, contralateral suppression– best for bilateral disease
• Ultrasound– operator dependent, independent of renal function
• MRA – poor images beyond main renal artery

Investigation of Ischemic Nephropathy
• High suspicion
– straight to angiography
• Mild to Moderate suspicion
– non-invasive imaging (local preference)
– if significant azotemia, US rather than MRA or
spiral CT

Investigation of RVH
• High suspicion– angiography and Renal Vein Renins if bilateral
• Moderate suspicion– captopril nuclear renography (can do "post"
study first)– positive -> angio– equivocal -> non-invasive imaging– negative -> stop

Treatment of RVH
• Select medical management based on risk of ischemic nephropathy and lesion progression
– medial fibroplasia and atherosclerotic (without ischemic nephropathy) best for medical
• angioplasty +/- stents usually procedure of choice unless
– branch vessel disease
– renal artery aneurysm
• Nephrectomy if small and non-functioning

Treatment of Ischemic Nephropathy
• No benefit with unilateral disease• Signs of reversibility
– progressive occlusion– collaterals– retrograde arterial filling– size > 9 cm– Cr < 4.0– preservation of glomeruli on biopsy
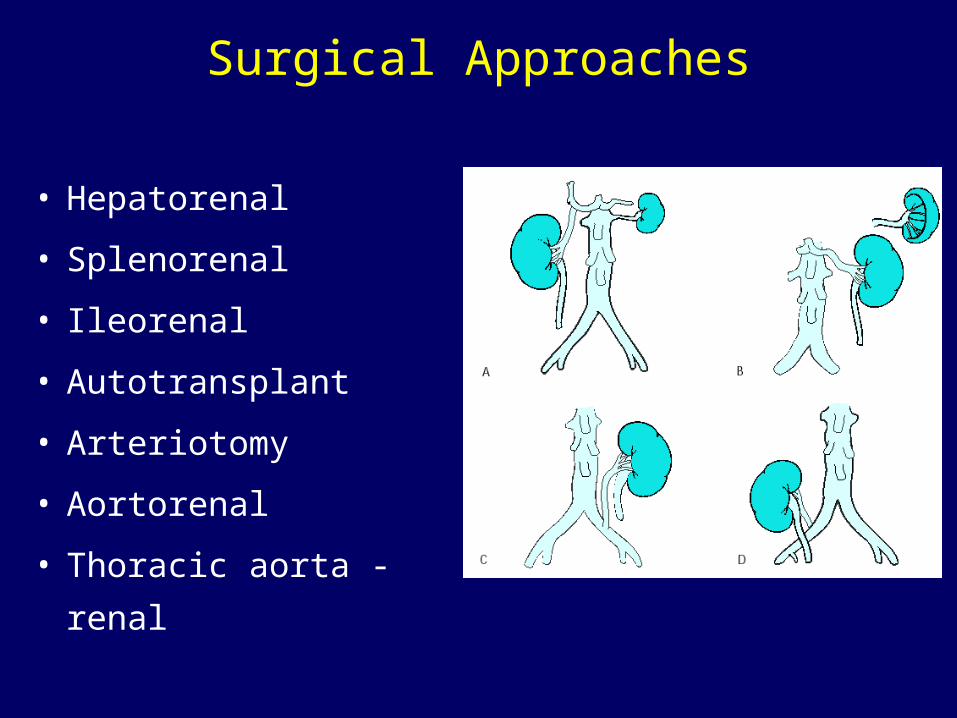
Surgical Approaches
• Hepatorenal
• Splenorenal
• Ileorenal
• Autotransplant
• Arteriotomy
• Aortorenal
• Thoracic aorta - renal
Renal Artery Aneurysms
• most small and asymptomatic• pathology
– saccular (most common), fusiform, dissecting, intrarenal
• risk of rupture– absent/incomplete calcification, >2cm diameter,
expanding, hypertension, pregnancy
• other complications– pain, hematuria, dissection, emboli