remodeling of suspended small intestinal submucosa venous valve: an experimental study in sheep to...
TRANSCRIPT

Remodeling of Suspended Small IntestinalSubmucosa Venous Valve: An ExperimentalStudy in Sheep to Assess the Host Cells’ OriginElias Brountzos, MD, Dusan Pavcnik, MD, PhD, Hans A. Timmermans, BFA, Christopher Corless, MD, PhD,Barry T. Uchida, BS, Edith S. Nihsen, BA, Manabu Nakata, MD, PhD, Maria Schoder, MD,John A. Kaufman, MD, Frederick S. Keller, MD, and Josef Rösch, MD
PURPOSE: To investigate the origin of host cells during remodeling of small intestinal submucosa (SIS) squarestent–based bicuspid venous valves (VVs).
MATERIALS AND METHODS: Suspended VVs (SVVs) were developed by suspending VVs within bare squarestents so the valve elements would not contact the vein wall after deployment. Eight SVVs were placed within theintrahepatic and infrahepatic inferior venae cavae (IVCs) of four adult female sheep. Eight standard VVs wereimplanted in the external jugular veins of these animals for comparison. At 5 weeks after placement, the devices wereexamined for stability and patency and the animals were killed. Gross, histologic, and scanning electron microscopic(SEM) examinations were performed.
RESULTS: Follow-up spot radiographs and venography showed no migration of the devices, venous occlusion, orthrombus formation. All SVVs were intact without contact with the IVC wall. Six VVs were competent and two wereslightly tilted with some reflux. Histologic study showed remodeling of SVVs and VVs with newly formed collagenfibers; fibroblasts and inflammatory cells were found penetrating the SIS leaflets and endothelial cells on the surface.SIS neovascularization was also present. There was no difference regarding SIS remodeling between SVVs and thefree part of VV leaflets. The VV leaflets’ bases were thicker compared to their free parts (P < .01). SEM examinationshowed endothelial cells on both sides of the SVVs and VVs. Endothelialization of the SVV central leaflet surfacesand both surfaces of the VV leaflets was more complete than that of the peripheral surfaces of the SVV leaflets.
CONCLUSION: SIS-based valve remodeling occurs independently of vessel wall contact by recruitment of cellsdirectly from the circulation.
Index terms: Endothelial cells • Endovascular stent-grafts
J Vasc Interv Radiol 2003; 14:349–356
Abbreviations: EJV � external jugular vein, IVC � inferior vena cava, SEM � scanning electron microscopy, SIS � small intestinal submucosa, SVV � sus-pended venous valve, VV � venous valve
SMALL intestinal submucosa (SIS) hasbeen shown to serve as a scaffold forconstructive remodeling of several tis-
sues (1–5), including tissues in the car-diovascular system (6–10). As a coverfor intravascular devices, SIS provides
a framework with a three-dimensionalstructure for the ingrowth of cells(11,12). Our previous experimentalwork with square stent–based SIS bi-cuspid venous valves (VVs) demon-strated remodeling of SIS with hostcells on both sides of valve leaflets.Early endothelialization and remodel-ing of the valve leaflets was found tooccur simultaneously at the free partsof the VV and at its base attached tothe vein wall (13). This finding sug-gests that endothelialization of the freepart of the VV occurs independently ofdirect extension of endothelial cellsfrom the attached valve base (14). To
From the Dotter Interventional Institute (E.B., D.P.,H.A.T., B.T.U., M.N., M.S., J.A.K., F.S.K., J.R.) and De-partment of Pathology (C.C.), Oregon Health and Sci-ences University, Portland, Oregon; Cook Biotech In-corporated (E.S.N.), West Lafayette, Indiana; andSecond Department of Radiology (E.B.), Athens Uni-versity Medical School, Athens, Greece. Received June10, 2002; revision requested August 15; revision re-ceived September 24; accepted September 26. Addresscorrespondence to D.P., Dotter Interventional Insti-tute, Oregon Health and Sciences University, L342,3181 SW Sam Jackson Park Rd., Portland, OR 97201;
E-mail: [email protected]
D.P., F.S.K., and J.R. have patent agreements withCook, Inc., and H.A.T. is a paid consultant of Cook,Inc.
None of the other authors has identified a potentialconflict of interest.
© SIR, 2003
DOI: 10.1097/01.RVI.0000058410.01661.62
349

explore the remodeling of the SIS VV,a suspended VV (SVV) model inside alarge square stent was developed. Thismodel allows intravascular deploy-ment of a valve without any contactwith the vein wall. We tested the SVVin the sheep inferior vena cava (IVC)and compared results of its cell re-modeling with remodeling of VVs im-planted into sheep external jugularveins (EJVs).
MATERIALS AND METHODS
Animals
The study involved four adult fe-male sheep weighing 54.5–75.9 kg(mean, 62.4 kg). The study was ap-proved by the Institutional AnimalCare and Use Committee of OregonHealth and Sciences University.
Devices
SIS.—SIS is an almost acellular,nonimmunogenic, biodegradable, xe-nogenic, collagen-based biomaterialderived from the submucosal layer ofporcine small intestine. Because of itsproperties, SIS is conducive to tissueremodeling. It becomes remodeled byhost tissue while degrading and re-absorbing over time. SIS is obtainedfrom the intestine by removing thesuperficial layers of the mucosa andthe external muscular layer. SIScomes in two forms, wet and dry. Inits wet form, SIS contains approxi-mately 90% water and is pliable, soft,and slick. In its dehydrated (or ly-ophilized) form, it contains approxi-mately 90% collagen and is paper-like and more fragile. The majority ofits collagen is type I, but other colla-gen types are also present. It containsnatural extracellular matrix moleculessuch as fibronectin, hyaluronic acid,heparin, chondroitin sulfates A andB, heparan sulfate, and several typesof growth factors including fibroblastgrowth factor, transforming growthfactor beta, and vascular endothelialcell growth factor (1–13). Recently,the United States Food and Drug Ad-ministration has approved SIS as abiomaterial for soft tissue repair andskin wound dressing.
SVVs.—For construction of SVVs,10-mm-diameter VVs were madefrom SIS sheets (100 �m; Cook Bio-tech, Lafayette, IN) sutured with 7–0
Prolene monofilament suture (Ethi-con; Johnson & Johnson, Somerville,NJ) to barbless square stents (0.0075-inch stainless-steel wire) as previ-ously described (13–15) (Fig 1a). The10-mm-diameter VVs were then sus-pended with 5–0 Prolene suture fromthe four corners of 20- or 25-mm-di-ameter barbed square stents (0.012-inch stainless-steel wire) (Cook,Bloomington, IN) (Fig 1b,c). This de-sign positions the VV in the center ofthe blood stream while preventingcontact with the IVC wall.
VVs.—Standard VVs were con-structed from barbed square stents(0.0075-inch stainless-steel wire;Cook) and laser-welded SIS as de-scribed elsewhere (13–15). The VVswere constructed in three sizes(10–11 mm, 12–13 mm, and 14–16mm) for insertion into EJVs of corre-sponding diameters.
SVVs and VVs were sterilizedwith gas. The SVVs were folded andfront-loaded into 9-F, 100-cm-longTeflon sheaths (Cook). A 8-F Teflonpusher catheter was used for theirdelivery. The VVs were folded in an8-F delivery catheter and deliveredcoaxially through a 9-F, 40-cm Teflonsheath (Cook) (14). Fifteen minutesbefore delivery, SVVs and VVs wererehydrated with injection of 10 mL ofsterile saline solution into the sheath.
Animal Experiment
Each animal was tranquilized witha 5–8-mg/kg intramuscular injectionof Telazol (Tiletamine HCL and Zolaz-epam HCL; Fort Dodge AnimalHealth, Fort Dodge, IA) and maskedwith 5% isoflurane until intubationwas possible. Atropine sulfate (6 mg;American Regent Laboratories,Shirley, NY) was administered intra-venously. Animals were allowed tobreathe spontaneously at 2%–2.5%isoflurane (Iso-thesia; Burns Veteri-nary Supply, Rockville Center, NY)mixed with 2 L O2 unless mechanicalventilation was required. Antibiotics(10 mg/kg oxytetracycline) were ad-ministrated as a single dose. A GE/OEC 9800 cardiac mobile system withdigital imaging (GE Medical Systems/OEC, Salt Lake City, UT) was used forimaging.
An 11-F, 40-cm-long Teflon sheathwas introduced percutaneously intoEJVs bilaterally. After administration
of 6,000 IU of heparin, a 100-cm Grad-uate measuring pigtail catheter (Cook)was placed through the sheath into theIVC distal to the renal veins.
Venograms were obtained beforeand after SVV and VV implantation intwo planes at 90° to properly estimatethe size of the target segments of thevessel and to assess VV function, po-sition, and degree of tilting relative tothe vein wall. IVC and EJV diameterswere measured with use of OECsoftware.
Two SVVs in square stents approx-imately the same diameter (20 or 25mm) as the IVC segment were selectedfor implantation. A 260-cm-long stiff0.035-inch guide wire (Cook) was thenintroduced in one EJV and the 40-cmsheath was exchanged for a 100-cmTeflon sheath of the same diameterand advanced into the peripheral IVC.The guide wire was removed and the9-F sheath containing a preloaded, re-hydrated SVV was coaxially intro-duced into the IVC. Each animal re-ceived two SVVs; one into theintrahepatic IVC and one into the in-frahepatic IVC. The SVV was deliv-ered by withdrawing both sheathswhile holding the pusher. As the SVVwas deployed, its square stent self-at-tached to the IVC wall. Altogether,eight SVVs were placed in fouranimals.
Subsequently, the 100-cm sheath wasexchanged for the 40-cm sheath. Simul-taneous bilateral jugular venogramswere obtained and the diameter of eachEJV was measured with the use of a0.035-inch Graduate measuring guidewire (Cook).
One VV of approximately the samediameter as the EJV was then deliv-ered across the native valve in eachanimal’s EJV as described previously(14). Function and stability of the VVswere immediately evaluated byvenography performed with a 6-Fstraight multihole catheter placed cen-tral and peripheral to the VV (14). Mi-gration was defined as movement ofthe implanted device from one ana-tomic position inside the vein toanother.
The catheters and sheaths were re-moved and the animals were allowedto recover from anesthesia. Two daysafter the procedure, the animals weresent to roam freely in a pasture.
350 • Remodeling of Suspended SIS Venous Valves in Ovine Model March 2003 JVIR
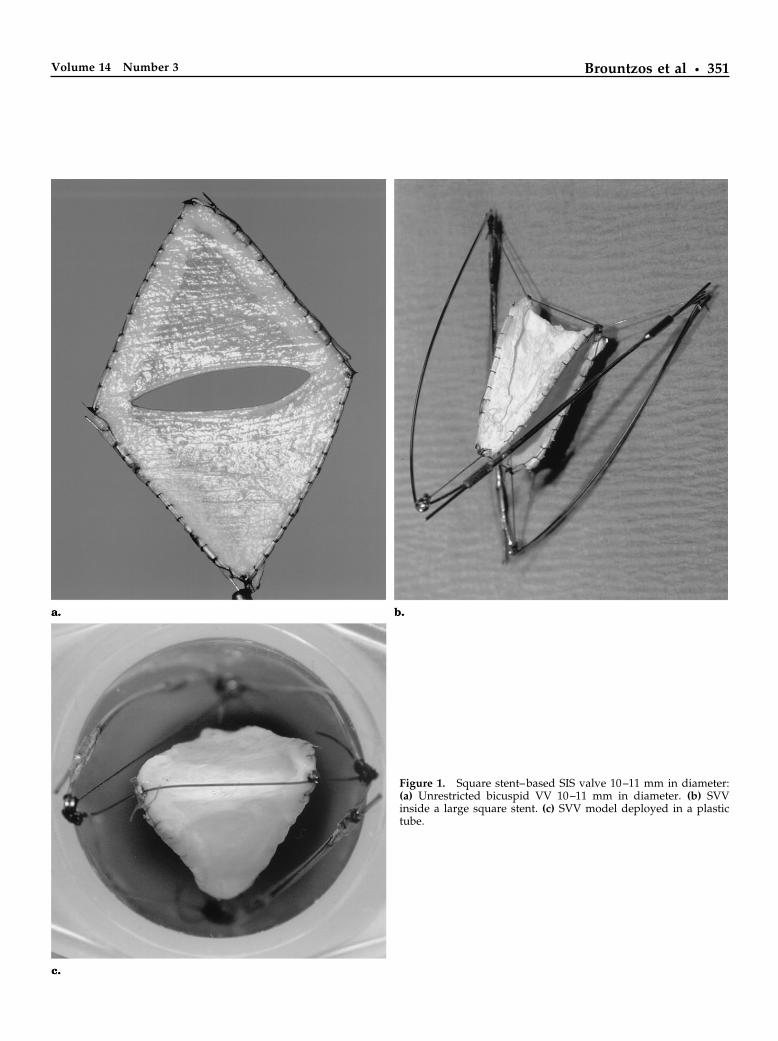
Figure 1. Square stent–based SIS valve 10–11 mm in diameter:(a) Unrestricted bicuspid VV 10–11 mm in diameter. (b) SVVinside a large square stent. (c) SVV model deployed in a plastictube.
Brountzos et al • 351Volume 14 Number 3

Follow-up
All animals were studied undergeneral anesthesia 5 weeks after de-vice implantation. The devices wereexamined for stability with use of flu-oroscopic spot radiographs. Patencyand function of the VVs was studiedby venography performed with directcatheterization of the external jugularveins as described herein. To test com-petency of the VVs, a 6-F sideholecatheter with two markers (Cook) wasintroduced from the distal EJV acrossthe VV for a high-volume (20 mL/secfor 2 sec) injection of contrast mediumcentral to the VV. Competency wasdefined by no leakage of contrast me-dium through the VV during high-flow injection. Minimal and moderatereflux were defined as minimal andmoderate leakage of contrast agentthrough the VV during high-flow in-jection. Patency was defined as thecondition of the vein and the VV ofbeing open with flow.
The patency of the SVVs was stud-ied with IVC venograms performedwith use of percutaneous catheteriza-tion of the right common femoral vein.
The animals were then killed with in-travenous injection of 0.1/kg of pento-barbital and phenytoin sodium (Eu-thasol; Delmarva Lab, Midlothian,VA).
Gross and Histologic Studies
Gross examination focused on theEJV, IVC, and surrounding structures.Veins containing VVs or SVVs werephotographed in situ and then har-vested. After harvesting, all SVVs andVVs were bisected longitudinally sothat each half contained one leaflet.One half from each device was ran-domly selected and fixed in 10% buff-ered formalin for histologic evaluation(in total, eight SVVs and eight VVs).After the wires were removed, thefixed leaflet was processed for paraf-fin-embedding and 5-�m sectionswere cut and stained with hematoxy-lin and eosin or with Massontrichrome stain. The remaining halvesof the harvested SVVs and VVs wereprocessed for electron microscopy ac-cording to a previously described pro-tocol (7).
Statistical Analysis
Vein diameters and VV and SVVthicknesses are reported as ranges andmeans � SD. Differences between VVand SVV thicknesses at different loca-tions were examined for statistical sig-nificance with the Student paired ttest. A P value of less than .05 wasconsidered to represent a significantdifference.
RESULTS
Intrahepatic IVC diameters rangedfrom 17.9 to 26.6 mm (mean: 20.9 mm� 3.4) and infrahepatic IVC diametersranged from 18.4 to 22.3 mm (mean:19.9 mm � 1.6). EJV diameters rangedbetween 11.2 and 16.7 mm (mean: 14.9mm � 2.2). Placement of all 16 deviceswas successful. There were no proce-dure-related complications. FourSVVs were well centered and fourwere slightly tilted on the postimplan-tation venograms. However, in allcases, the SVVs were not in contactwith the IVC wall. Six VVs were wellcentered in EJVs and two were slightlytilted; nevertheless, postplacementvenograms depicted good patencyand competency in all cases.
Follow-up spot radiographs andvenography at 5 weeks before sacrificedemonstrated no device migration. Alldevices were patent, without evidenceof thrombus or increase in tilt angle.All SVVs were intact. Barb penetrationof the IVC wall and minimal intimalthickening at the square stent’s attach-ment points were seen in all SVVs (Fig2a). Six VVs were competent; minimalto moderate reflux was noted in alltilted and one well-centered VV (Fig3a,b).
Gross Examination
The square-stent frames of all SVVsand VVs were anchored against theIVC and the EJV wall, respectively.With SVVs, total or partial incorpora-tion of the square-stent frame into theIVC wall was found in all specimens.Nevertheless, there was no contact be-tween the valve portion of the SVVand the IVC wall in any instance (Fig2b). The suspended valves were easilyharvested by cutting the suspensory5–0 Prolene sutures. Glistening leafletsurfaces were seen in all eight speci-mens. The square-stent base of the VV
Figure 2. SVV model in the sheep intrahepatic IVC at 5 weeks follow-up: (a) Cavogramdemonstrates no SVV contact with the IVC wall; note the SVV’s central (white arrow) andperipheral (black arrow) sides. (b) Axial view from above shows SVV specimen (whitearrow) avoiding IVC wall (black arrow).
352 • Remodeling of Suspended SIS Venous Valves in Ovine Model March 2003 JVIR

was similarly incorporated into theEJV wall, forming valves approximat-ing the architecture and anatomy ofnative valves (Fig 3c).
In the case of one tilted VV, tiltingwas caused by inadvertent partialplacement of the VV in a venousbranch. The leaflets of another VV,which was oversized, were fused withthe vein wall; this valve exhibited re-flux on the follow-up venogram.
Histology
In cross-section, all SVVs displayedremodeling by fibroblasts with newcollagen fibers on both outer surfacesof the leaflets with a layer of residualSIS material in the center (Fig 4a,b).Numerous spindle-shaped fibroblastswere interspersed among the collagenfibers. Endothelial cells were found onboth sides of all SVV leaflets; inflam-matory cells (lymphocytes, plasmacells, histiocytes) were also found pen-etrating the SIS leaflets. New capillar-ies were identified within the extracel-lular matrix (neovascularization).Thicknesses of the remodeled SIS ofthe SVVs measured 30–140 �m (mean:86.5 �m � 37.6). No differences werenoted between SVVs in the infrarenalversus intrahepatic IVC.
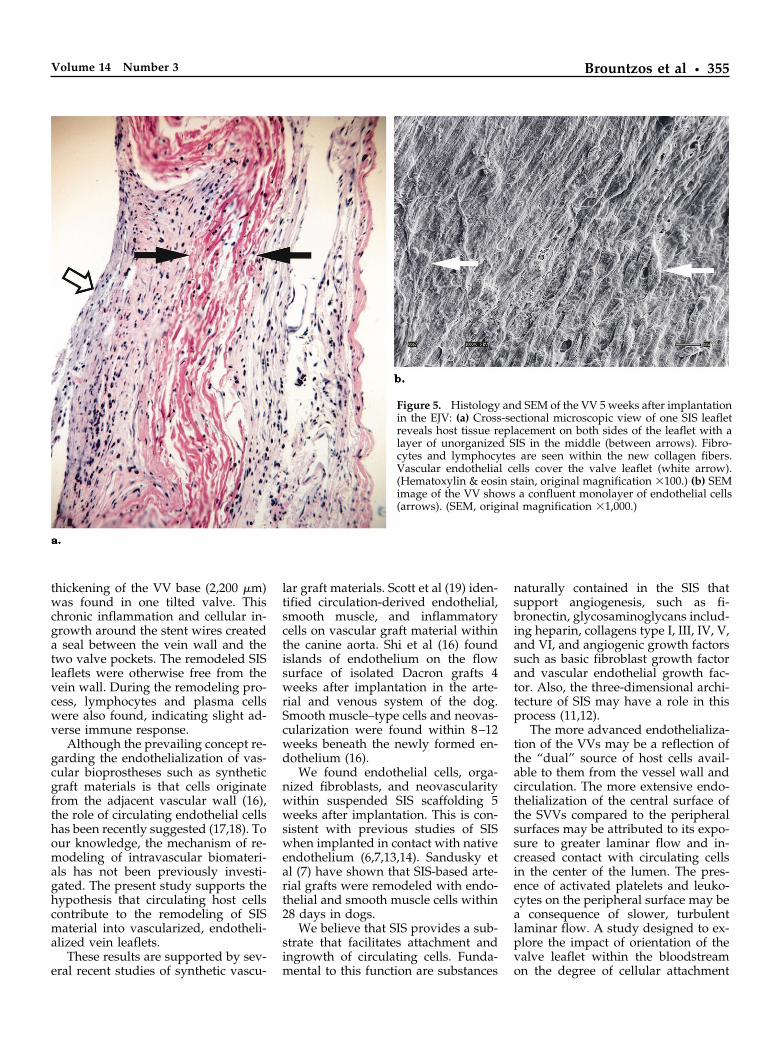
Similar host cellular ingrowth andneovascularization was found in theVVs (Fig 5a). Only the leaflet of thetilted VV was found to have unilateralremodeling; the contralateral side wasfused with the vein wall. A significantdifference (P � .01) was found be-tween the thickness of the SIS mem-brane at the base and at the free part ofthe VV leaflet; the bases of the VVsmeasured 600–2,200 �m (mean: 1,390�m � 496.6), whereas the free parts ofthe VVs measured 160–600 �m (mean:318.3 �m � 169.2). This is a consistentfinding (14) and is attributed to cellu-lar ingrowth around sutures and thestent wires creating a seal between thevein wall and the valve pockets.
There was no difference in the ex-tent of SIS remodeling between theSVVs and the free part of the VVs.Thicknesses of the remodeled SIS ofthe VVs’ free parts measured 20–180�m (mean: 78.7 �m � 43.8).
SEM
Host cell ingrowth was observed bySEM in SVVs and VVs. A difference
Figure 3. The VV placed into the EJV at 5 weeks: (a) Jugular venogram with injectionperipheral to the VV demonstrates valve patency. (b) Venogram with injection central to thevalve demonstrates closure of the VV with no reflux. (c) Jugular vein specimen shows smoothincorporation of the VV into the vein wall. Forceps are inserted into the VV’s pockets.
Brountzos et al • 353Volume 14 Number 3

between the two surfaces of the SVVleaflets was observed. The central (to-ward the lumen) side appeared tohave a more organized layer of endo-thelial cells (Fig 4c) whereas, on theperipheral (toward the vein wall) side,only individual endothelial cells werenoted, as were leukocytes and acti-vated and nonactivated platelets (Fig4d). There was no difference betweenSVVs situated in the infrahepatic andintrahepatic IVC.
The VVs exhibited a confluentmonolayer of endothelial cells on bothsides of the valve leaflets. The direc-tion of the blood flow through the
valve could be determined based onthe pattern of the endothelial cells.Leukocytes were absent on both sur-faces of the VV. Platelets were seenadhered to both surfaces, but they didnot appear activated (Fig 5b).
DISCUSSION
SIS is a unique biomaterial that hasserves as a scaffold for tissue growth.The mechanism of cellular migrationis poorly understood, but is presumedthat cells migrate from adjacent tissueswhen SIS is used—as in mostcases—as a scaffolding for skin, blad-
der, and bone (1–4,11,12). The mecha-nism of remodeling of SIS in the vas-cular system has not been previouslyevaluated. The objective of this studywas to investigate whether valve SISremodeling and endothelializationmay occur independently of vesselwall contact.
We have shown that endothelialcell growth at 5 weeks occurs on bothsides of the SIS valve leaflets whensuspended midstream in the IVC. Thisoccurred even though the SIS had nodirect contact with the endothelium ofthe venous wall. In addition, there wasasymmetry of the degree of endotheli-alization: the endothelial cells on thecentral surfaces of the suspended leaf-lets were greater in number and moreorganized than those on the peripheralsurfaces. There was no apparent in-creased endothelialization near the at-tachment points of the four suspen-sory sutures. This pattern suggeststhat the origin of the endothelial cellswas primarily the bloodstream ratherthan migration from the wall of theIVC.
SEM demonstrated that the degreeof endothelialization of both surfaces(central and peripheral) of the VVswere similar to that of the central sur-face of the SVVs. The base of the VVwas in direct contact with the nativeendothelium, which would permit di-rect migration of cells. The pattern ofendothelialization possibly resultingfrom migration from adjacent veinwall was not observed in the SVVs; thegreatest degree of endothelializationwas on the surface of the valve thatwas furthest from the vein wall. Thissuggests that endothelialization ofVVs may occur by severalmechanisms.
There was no difference in the ex-tent of SIS remodeling between SVVsand the free part of the VVs whencomparing the thickness of remodeledSIS material. Residual unremodeledSIS layer was present in the middle ofthe cross-section of the SVV valve leaf-lets. Similar remodeling process wasfound in the VVs in this experimentand was identical to that observed inour previous long-term valve study(14).
At the VV base (bottom of thecusp), the SIS membrane with its flapwas thickened (mean: 1,390 �m � 496)and attached to the vein wall. Severe
Figure 4. Histology and SEM of the SVV 5 weeks after implantation in the IVC: (a)Cross-sectional microscopic view of the leaflets shows remodeled SIS on both sides withunorganized SIS in the middle (between arrows). (Hematoxylin & eosin stain, originalmagnification �200.) (b) High magnification of the remodeled layer of the SIS showsformation of microvessels (open arrow) inside fully penetrated and reorganized layer byhost cells, including fibrocytes, lymphocytes, and endothelial cells. Vascular endothelialcells cover the valve leaflet (arrow). (Hematoxylin & eosin stain, original magnification�400.) (c) SEM image of the SVV’s central side shows an organized layer of endothelialcells (arrows). (SEM, original magnification �1,000.) (d) SEM image of the peripheral sideof the same SVV. Arrows point to endothelial cells among white cells and thrombocytes.(SEM, original magnification �1,000.)
354 • Remodeling of Suspended SIS Venous Valves in Ovine Model March 2003 JVIR
thickening of the VV base (2,200 �m)was found in one tilted valve. Thischronic inflammation and cellular in-growth around the stent wires createda seal between the vein wall and thetwo valve pockets. The remodeled SISleaflets were otherwise free from thevein wall. During the remodeling pro-cess, lymphocytes and plasma cellswere also found, indicating slight ad-verse immune response.
Although the prevailing concept re-garding the endothelialization of vas-cular bioprostheses such as syntheticgraft materials is that cells originatefrom the adjacent vascular wall (16),the role of circulating endothelial cellshas been recently suggested (17,18). Toour knowledge, the mechanism of re-modeling of intravascular biomateri-als has not been previously investi-gated. The present study supports thehypothesis that circulating host cellscontribute to the remodeling of SISmaterial into vascularized, endotheli-alized vein leaflets.
These results are supported by sev-eral recent studies of synthetic vascu-
lar graft materials. Scott et al (19) iden-tified circulation-derived endothelial,smooth muscle, and inflammatorycells on vascular graft material withinthe canine aorta. Shi et al (16) foundislands of endothelium on the flowsurface of isolated Dacron grafts 4weeks after implantation in the arte-rial and venous system of the dog.Smooth muscle–type cells and neovas-cularization were found within 8–12weeks beneath the newly formed en-dothelium (16).
We found endothelial cells, orga-nized fibroblasts, and neovascularitywithin suspended SIS scaffolding 5weeks after implantation. This is con-sistent with previous studies of SISwhen implanted in contact with nativeendothelium (6,7,13,14). Sandusky etal (7) have shown that SIS-based arte-rial grafts were remodeled with endo-thelial and smooth muscle cells within28 days in dogs.
We believe that SIS provides a sub-strate that facilitates attachment andingrowth of circulating cells. Funda-mental to this function are substances
naturally contained in the SIS thatsupport angiogenesis, such as fi-bronectin, glycosaminoglycans includ-ing heparin, collagens type I, III, IV, V,and VI, and angiogenic growth factorssuch as basic fibroblast growth factorand vascular endothelial growth fac-tor. Also, the three-dimensional archi-tecture of SIS may have a role in thisprocess (11,12).
The more advanced endothelializa-tion of the VVs may be a reflection ofthe “dual” source of host cells avail-able to them from the vessel wall andcirculation. The more extensive endo-thelialization of the central surface ofthe SVVs compared to the peripheralsurfaces may be attributed to its expo-sure to greater laminar flow and in-creased contact with circulating cellsin the center of the lumen. The pres-ence of activated platelets and leuko-cytes on the peripheral surface may bea consequence of slower, turbulentlaminar flow. A study designed to ex-plore the impact of orientation of thevalve leaflet within the bloodstreamon the degree of cellular attachment
Figure 5. Histology and SEM of the VV 5 weeks after implantationin the EJV: (a) Cross-sectional microscopic view of one SIS leafletreveals host tissue replacement on both sides of the leaflet with alayer of unorganized SIS in the middle (between arrows). Fibro-cytes and lymphocytes are seen within the new collagen fibers.Vascular endothelial cells cover the valve leaflet (white arrow).(Hematoxylin & eosin stain, original magnification �100.) (b) SEMimage of the VV shows a confluent monolayer of endothelial cells(arrows). (SEM, original magnification �1,000.)
Brountzos et al • 355Volume 14 Number 3

and SIS remodeling would be useful tounderstand this process.
The question regarding the specificidentities of the circulating cells thatultimately remodeled the SIS of theSVV was not explored in our study.There is increasing evidence in the lit-erature supporting the existence of acirculating bone marrow–derived en-dothelial precursor cell (20–22). Thiscirculating endothelial precursor cir-culates, proliferates, and differentiatesinto mature vascular endothelial cellsfundamental to the endothelializationof vascular prostheses. Circulating en-dothelial precursors may also have adominant role in a variety of physio-logic and pathologic processes involv-ing angiogenesis such as wound heal-ing or tumor growth. Other studiessuggest that circulating fibrocytes ormyofibroblast precursors may be re-cruited in sites of vascular healing(23,24). More recently, a pluripotentstem cell capable of differentiatinginto several cell types was described innormal adult human blood (25).
There are several potential limita-tions of this study, foremost of whichis that the SIS of the SVVs could not becompletely isolated from the veinwalls. The suspensory sutures at thecorners of the valves could haveserved as a conduit for migratory en-dothelial and other cells originatingfrom the wall of the IVC. However,there was no evidence of focal deposi-tion of endothelial cells or remodelingat the corners of the valves (where thesutures attached) compared to anyother portion of the valves. In addi-tion, this would not explain the differ-ence in endothelial cells noted be-tween the central and peripheralsurfaces of the suspended SIS. Otherlimitations include the single timepoint for harvesting the valves ratherthan serial evaluation. This was neces-sitated by the use of a large animalmodel. Last, the results in the sheepIVC may not be applicable to SIS inhuman veins and arteries.
In conclusion, this study indicatesthat circulating cells are a likely sourceof origin for cell deposition on SIS inthe sheep IVC.
Acknowledgments: The authors thankSheri Imai-Swiggart, BS, Lisa Buckley, BS,and Hua Xie, MD, for their assistance.
References1. Badylak SF. Small intestinal submu-
cosa (SIS): a biomaterial conducive tosmart tissue remodeling. In: Bell E, ed.Tissue engineering: current perspec-tives. Cambridge, MA: Burkhauser,1993;179–189.
2. Aiken SW, Badylak SF, Toombs JP, etal. Small intestine submucosa as anintra-articular ligamentous graft mate-rial: a pilot study in dogs. Vet CompOrthoped Trauma 1994; 7:124–128.
3. Peel SF, Chen H, Renlund R, BadylakSF, Kandel RA. Formation of a SIS-cartilage composite graft in vitro andits use in the repair of articular carti-lage defect. Tissue Eng 1998; 4:143–153.
4. Prevel CD, Eppley BI, Summerlin DJ,Jackson JR, McCarthy M, Badylak SF.Small intestinal submucosa (SIS): utili-zation for repair of rodent abdominalwall defect. Ann Plast Surg 1995; 35:347–380.
5. Park JW, Pavcnik D, Uchida BT, et al.Small intestinal submucosa covered ex-pandable Z stents for treatment of tra-cheal injury: an experimental pilotstudy in swine. J Vasc Interv Radiol2000; 11:1325–1330.
6. Lantz GC, Badylak SF, Hiles MC, et al.Small-intestinal submucosa as a vascu-lar graft: a review. J Invest Surg 1993;6:297–310.
7. Sandusky GE Jr, Badylak SF, Morff RJ,Johnson WD, Lantz G. Histologicfindings after in vivo placement ofsmall intestinal submucosa vasculargrafts and saphenous vein grafts in thecarotid artery in dogs. Am J Pathol1992; 140:317–324.
8. Hiles MC, Badylak JF, Lantz GC, Ko-kini K, Geddes LA, Morff RJ. Me-chanical properties of xenogenic small-intestinal submucosa when used as anaortic graft in the dog. J Biomed MaterRes 1995; 29:883–895.
9. Yamada K, Pavcnik D, Uchida BT, et al.Endoluminal treatment of ruptured ab-dominal aortic aneurysm with smallintestinal submucosa sandwich en-dografts: a pilot study in sheep. Car-diovasc Intervent Radiol 2001; 24:99–105.
10. Toyota N, Pavcnik D, VanAlstine W, etal. Experimental comparison of thesmall intestinal submucosa covered-and noncovered nitinol stents in thesheep iliac arteries: a pilot study. J VascInterv Radiol 2002; 13:489–498.
11. Badylak SF, Record R, Lindberg K,Hodde J, Park K. Small intestinal sub-mucosa: a substrate for in vitro cellgrowth. J Biomater Sci Polym Ed 1998;9:863–878.
12. Badylak S, Liang A, Record R, TulliusR, Hodde J. Endothelial cell adher-
ence to small intestinal submucosa: anacellular bioscaffold. Biomaterials1999; 20:2257–2263.
13. Pavcnik D, Uchida B, Timmermans H,Keller FS, Rösch J. Square stent: anew self-expandable endoluminal de-vice and its applications. CardiovascIntrevent Radiol 2001; 24:207–217.
14. Pavcnik D, Uchida BT, TimmermansHA, et al. Percutaneous bioprostheticvenous valve: a long-term study insheep. J Vasc Surg 2002; 35:598–602.
15. Pavcnik D, Uchida B, TimmermansHA, Corless C, Keller FS, Rosch J.Square stent based large vessel oc-cluder. J Vasc Interv Radiol 2000; 11:1227–1234.
16. Shi Q, Wu MD, Hayashida N,Wechezak AR, Clowes AW, SauvageLR. Proof of fallout endothelializa-tion of impervious Dacron grafts in theaorta and the inferior vena cava in thedog. J Vasc Surg 1994; 20:546–557.
17. Stump MM, Jordan GL Jr, DeBakeyME, Halpert B. Endothelium grownfrom circulating blood on isolated in-travascular Dacron hub. Am J Pathol1963; 43:361–367.
18. Frazier OH, Baldwin RT, Eskin SG,Duncan JM. Immunochemical identi-fication of human endothelial cells onthe lining of a ventricular assist device.Tex Heart Inst J 1993; J2:78–82.
19. Scott SM, Barth MG, Gaddy LR, AhlET. The role of circulating cells in thehealing of vascular prostheses. J VascSurg 1994; 19:585–593.
20. Shi Q, Rafii S, Wu MHD, et al. Evi-dence for circulating bone marrow-de-rived endothelial cells. Blood 1998; 92:362–367.
21. Shahin R. Circulating endothelialprecursor: mystery, reality, and prom-ise. J Clin Invest 2000; 105:17–19.
22. Lin Y, Weisdorf DJ, Solovey A, HebbelRP. Origins of circulating endothelialcells and endothelial outgrowth fromblood. J Clin Invest 2000; 105:71–77.
23. Abe R, Donnelly SC, Peng T, Bucala R,Metz CN. Peripheral blood fibro-cytes: differentiation pathway and mi-gration to wound sites. J Immunol2001; 166:7556–7562.
24. Wilcox JN, Okamoto EI, Nakahara KI,Vinten-Johansen J. Perivascular re-sponses after angioplasty which maycontribute to post angioplasty resteno-sis: a role for circulating myofibroblastprecursors? Ann N Y Acad Sci 2001;947:68–90.
25. Milhaud G. A human pluripotentstem cell in the blood of adults: to-wards a new cellular therapy for tissuerepair. Bull Acad Natl Med 2001;185:567–577.
356 • Remodeling of Suspended SIS Venous Valves in Ovine Model March 2003 JVIR